From www.bloodjournal.org by guest on March 5, 2016. For personal use only.
HEMOSTASIS, THROMBOSIS, AND VASCULAR BIOLOGY
Brief report
Familial essential thrombocythemia associated with a dominant-positive
activating mutation of the c-MPL gene, which encodes for the receptor
for thrombopoietin
Jianmin Ding, Hirokazu Komatsu, Atsushi Wakita, Miyuki Kato-Uranishi, Masato Ito, Atsushi Satoh, Kazuya Tsuboi, Masakazu Nitta,
Hiroshi Miyazaki, Shinsuke Iida, and Ryuzo Ueda
One Japanese pedigree of familial essential thrombocythemia (FET) inherited in
an autosomal-dominant manner is presented. A unique point mutation, serine
505 to asparagine 505 (Ser505Asn), was
identified in the transmembrane domain
of the c-MPL gene in all of the 8 members
with thrombocythemia, but in none of the
other 8 unaffected members in this FET
family. The Ba/F3 cells expressing the
mutant Asn505 acquired interleukin 3
(IL-3)–independent survival capacity,
whereas those expressing wild-type
Ser505 did not. The autonomous phosphorylation of Mek1/2 and Stat5b was
observed in the mutant Ba/F3 cells in
the absence of IL-3. The former was
also found in platelets derived from the
affected individual in the absence of
thrombopoietin. These results show
that the Asn505 is an activating mutation with respect to the intracellular signaling and survival of the cells. This is
the first report of FET deriving from a
dominant-positive activating mutation
of the c-MPL gene. (Blood. 2004;103:
4198-4200)
© 2004 by The American Society of Hematology
Introduction
Familial essential thrombocythemia (FET) is a rare hereditary
chronic myeloproliferative disorder, which is characterized by
autonomously activated megakaryocytopoiesis with the excessive
production of platelets. The c-MPL gene and its ligand, thrombopoietin (TPO), regulate the proliferation and differentiation of
megakaryocytes and platelets. The germline mutations in the
promoter region of the TPO gene, which produce the aberrantly
stable TPO mRNA resulting in FET, have been reported.1,2
Germline mutations in the c-MPL gene have been also reported to
cause congenital amegakaryocytic thrombocytopenia,3-6 which is
characterized by defective proliferation of megakaryocytes in bone
marrow. In the present study, we found one Japanese pedigree of
FET in which affected members showed autosomal-dominant
inheritance, and investigated the underlying molecular mechanisms.
Study design
Mutation analysis of c-MPL and TPO genes
Supplemental Table link at the top of the online article on the Blood
website.
Cell survival assay using stably transfected Ba/F3 cells with
wild and mutant types of c-MPL
The Humplpas12 plasmid carrying a full length of the wild-type c-MPL
cDNA was provided by Amgen (Thousand Oaks, CA). The mutant
c-MPL cDNA was generated by reverse transcription–polymerase chain
reaction (RT-PCR) using platelet-derived RNA of patient ‘b’ in Figure
1A. The coding region of each c-MPL cDNA fragment was ligated into
the pCI-Neo expression vector (Promega, Madison, WI) and transfected
into Ba/F3 cells by electroporation (1040 F and 0.3 kV). The resistant
clones against 1 mg/mL G418 were selected and maintained in RPMI
1640 with 10% fetal bovine serum (FBS), 10% supernatant from WEHI
cells, as a source of interleukin 3 (IL-3). Immunoblotting was performed
using anti–c-Mpl polyclonal antibody (Upstate Biotechnology, Lake
Placid, NY), as previously reported.8 Methylthiotetrazole (MTT) assays
were used to evaluate viable cell numbers in the presence and absence
of IL-3.9
We amplified all of the exons and splice sites of TPO and c-MPL genes and
then performed direct sequencing using an automated sequencer (model
ABI377; Applied Biosystems, Foster City, CA) to find the germline
mutations in gDNAs derived from peripheral blood mononuclear cells.7
Primer sequences are given in the Supplemental Materials: see the
Phosphorylation analysis of the downstream signaling in
Mek1/2 and Stat5b status
From the Department of Internal Medicine and Molecular Science, Nagoya City
University Graduate School of Medical Science, Nagoya, Japan; Division of
Hematology, Department of Internal Medicine, Aichi Medical University School
of Medicine, Aichi-gun, Japan; and Kirin Brewery Company Ltd, Tokyo, Japan.
The online version of the article contains a data supplement.
Submitted October 10, 2003; accepted January 20, 2004. Prepublished online
as Blood First Edition Paper, February 5, 2004; DOI 10.1182/blood-2003-10-3471.
Supported by grants from the Ministry of Education Science, Sports and
Culture, Japan (S.I., A.W., and R.U.), grants-in aid for research from Nagoya
City University (H.K.), and by the Ministry of Education, Culture, Sports,
Science and Technology “Honors Scholarship for privately financed
International Student” (J.D.).
4198
Exponentially growing cells were cultured at 2 ⫻ 107/mL in the absence
of IL-3 for 6 hours, followed by incubation for 90 minutes with or
An Inside Blood analysis of this article appears in the front of this issue.
Reprints: Hirokazu Komatsu, Department of Internal Medicine and Molecular
Science, Nagoya City University Graduate School of Medical Science,
1-Kawasumi, Mizuho-cho, Mizuho-Ku, Nagoya 467-8601, Japan; e-mail:
komatsu@med.nagoya-cu.ac.jp.
The publication costs of this article were defrayed in part by page charge
payment. Therefore, and solely to indicate this fact, this article is hereby
marked ‘‘advertisement’’ in accordance with 18 U.S.C. section 1734.
© 2004 by The American Society of Hematology
BLOOD, 1 JUNE 2004 䡠 VOLUME 103, NUMBER 11
From www.bloodjournal.org by guest on March 5, 2016. For personal use only.
BLOOD, 1 JUNE 2004 䡠 VOLUME 103, NUMBER 11
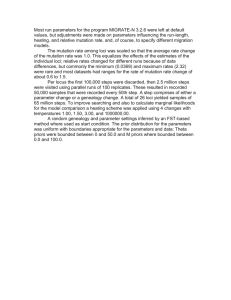
Figure 1. Results of study of family affected with FET. (A) Pedigree of FET.
Members of the family, designated as ‘a’ through ‘h’ and ‘1’ through ‘8’, were
examined clinically; solid symbols (a-h) indicate ET-affected members, and numbers
1-8 indicate unaffected members. Square symbols denote men; circles, women; and
symbols with a slash, deceased members. This pedigree shows the autosomaldominant inheritance of disease penetration. (B) Sequence of the Asn505 mutation of
the c-MPL gene detected in ET-affected members of the family. Upper sequence
indicates the wild type, and the lower sequence indicates the point mutation detected
in the affected members. The nucleotide change from guanine to adenine caused an
amino acid substitution from Ser505 to Asn505. (C) Platelet counts for the family
members and the association with the status of the Asn505 mutation of the c-MPL
gene. f indicates platelet counts of the members carrying the Asn505 mutation of the
c-MPL gene; 䡺, platelet counts of the members with wild-type alleles of the
homozygous Ser505, showing that the Asn505 mutation is unique in affected
members; 1-8 and a-h correspond to the designations in panel A.
without 10% WEHI cells’ supernatant. The cells were dissolved in lysis
buffer containing a protease-inhibitor cocktail (Complete mini; Roche
Diagnostics, Mannheim, Germany). Anti–phospho-Mek1/2 and anti–
whole-Mek1/2 (Phospho Plus ser 217/221 antibody kit; Cell Signaling
Technology, Beverly, MA) were used to evaluate the phosphorylation
status using immunoblot analysis. Immunoprecipitation was performed
using Stat5b antibody (c-17) followed by immunoblotting with anti–pTyr antibody (PY-99; Santa Cruz Biotechnology, Santa Cruz, CA) for
the detection of the phosphorylation status of Stat5b. The platelets
isolated from patient ‘a’ shown in Figure 1A and one healthy volunteer
were stimulated with 200 ng/mL recombinant human TPO (IM-25A;
Invitrogen, Carlsbad, CA) for 10 minutes at 37°C10 and evaluated for the
phosphorylation status of Mek1/2. Study approval was obtained from
the institutional review board of the Nagoya City University Graduate
School of Medical Science. Informed consent was provided according to
the Declaration of Helsinki.
Results and discussion
We used the revised criteria of the Polycythemia Vera Study Group
for the diagnosis of essential thrombocythemia (ET), which include
a platelet count more than 600 ⫻ 109/L (600 000/L).11 Eight of 16
members examined in 3 generations of this pedigree were found to
be affected with ET in an autosomal-dominant manner (Figure 1A).
The individuals with FET showed normocellular and normoplastic
marrows except for increased megakaryocytes.
To clarify the genetic alterations responsible for this hereditary thrombocythemia, we investigated if germline mutations in
TPO and c-MPL genes were present in the affected members.
Interestingly, a unique variant of c-MPL was identified in all of
c-MPL MUTATION IN FET
4199
the 8 affected members but not in any of the 8 unaffected
members, whereas no unique nucleotide variants could be
detected in TPO. This unique variant presented as a heterozygous G⬎A nucleotide substitution at position 1073 in exon 10 of
c-MPL (GenBank accession no. U68161), which results in an
amino acid exchange from serine to asparagine (Ser505Asn;
GenBank accession no. NP_005364; Figure 1B-C). RT-PCR
followed by direct sequencing confirmed that the mutant c-MPL
mRNA encoding Asn505 was expressed in the platelets (data not
shown), suggesting that this mutant c-Mpl plays a crucial role in
the pathogenesis of FET.
To investigate the mechanisms contributing to the cellular
growth and survival of the mutant c-MPL, we performed an MTT
assay using stably transfected Ba/F3 cell clones containing wildtype or mutant c-MPL. Although the mock and Ba/F3 cells
expressing wild-type c-Mpl are completely dependent on the
presence of IL-3 and die immediately after withdrawal of IL-3,
Ba/F3 cells expressing mutant c-Mpl could survive for at least 6
days even in the absence of IL-3 (Figure 2A). This suggests that the
mutant c-Mpl (Asn505) provides megakaryocytic progenitors with
a cell survival capacity.
Next, because the downstream signaling pathways including
Shc-Ras-Raf-Mek1/2-Mapk (Erk) and Jak-Stat cascades have
been reported to be associated with the Tpo-c-Mpl system in
megakaryopoiesis,12 we examined the phosphorylation status of
Mek1/2 and Stat5b in the c-Mpl–expressing Ba/F3 cells in the
presence and absence of IL-3 to determine if the mutant c-Mpl
can activate those signaling molecules. In wild-type c-Mpl–
expressing cells, tyrosine phosphorylation of Mek1/2 and Stat5b
was detected only in the presence of IL-3, whereas mutant
c-Mpl–expressing cells harbored constitutively phosphorylated
Mek1/2 even in the absence of IL-3. Constitutive but faint
phosphorylation of Stat5b was also detected in mutant c-Mpl–
expressing cells, although it was never seen in wild-type
c-Mpl–expressing cells in the absence of IL-3 (Figure 2B).
Moreover, constitutive phosphorylation of Mek1/2 was observed in the platelets of the ET-affected individual even in the
absence of TPO stimulation (Figure 2C). These observations
show that mutant c-Mpl with Asn505 activates the downstream
signals involved in the Tpo-c-Mpl pathway with factor independence in vitro and in vivo, suggesting that the mutant c-Mpl–
expressing megakaryocytes acquire promoted cell survival
capacity in bone marrow, leading to the excessive production of
platelets. The mechanism underlying how c-Mpl with Asn505
induces constitutive phosphorylation of Mek1/2 and Stat5b
remains unknown. However, it is assumed that the dimerization
of c-Mpl molecules, which is believed to be a requisite step for
activation of c-Mpl, may be constitutive as a result of this
specific mutation, as in the cases of mutations of c-kit and Neu at
their transmembrane domains.9,13 Further investigation is needed
to elucidate the mechanism.
The same Asn505 mutation of c-MPL, which had been prepared
artificially by PCR-driven random mutagenesis in vitro, was
previously reported by Onishi et al to be an activating mutation that
manifests higher sensitivity to very low doses of TPO and
tumorigenicity in mice.14 However, we have not yet found any
ET-affected individuals in this family who have developed malignancies including leukemia.
Finally, we attempted to analyze whether the same mutation,
Asn505, is found in the sporadic ET cases. Platelet-derived
RNAs of 19 sporadic ET patients were screened for the c-MPL
mutations, but none were found (data not shown). This is
From www.bloodjournal.org by guest on March 5, 2016. For personal use only.
4200
BLOOD, 1 JUNE 2004 䡠 VOLUME 103, NUMBER 11
DING et al
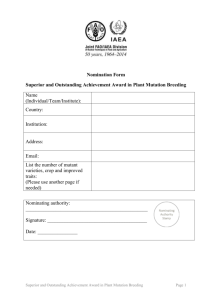
Figure 2. MTT and Western blotting analyses. (A) (Left) MTT assay of mutant-type c-Mpl. W1 and W2 are the transfectants with the wild-type allele (Ser505), and M1 and M2
are those with the mutant type (Asn505). The x-axis indicates time of culture after withdrawal of IL-3. The y-axis shows the relative value of cell viability (OD, 580-630 nm). Half
the culture medium was exchanged with IL-3–free medium every other day. Mutant cells (Asn505) exhibited survival capacity in the absence of IL-3 (each experiment was
repeated 3 times). (Right) Western blot with the c-Mpl antibody. Arrow shows the c-Mpl products (82 kDa). The FDCP2 cells transfected with the wild-type c-MPL were used as
a positive control. The lysate of Ba/F3 cells and the plasmid PCI-neo carrying no foreign gene were analyzed as negative controls. The same filter was stripped and blotted with
-actin antibody. (B) Western blot with the Mek1/2 antibody of Ba/F3 transfectants and immunoprecipitation–Western blot with p-Tyr and Stat5b antibodies. Phosphorylated
Mek1/2 signals (45 kDa) were detected in M1 and M2 after 6 hours culture with the IL-3–free medium. The same filter was stripped and blotted with anti-Mek1/2 antibody. The
phosphorylated Stat5b signals of 96-kDa products were observed in M1 and M2 in the IL-3–free condition. The same filters were stripped and blotted with anti-Stat5b antibody.
This experiment was repeated twice and the results were reproducible. (C) Western blot with the Mek1/2 antibody of the platelets from the ET-affected member. The
constitutively phosphorylated Mek1/2 was detected in the platelets of the ET-affected individual (patient ‘a’ in Figure 1A) even in the absence of the stimulation of TPO.
consistent with the study of Horikawa et al who demonstrated
that the c-Mpl–mediated signaling pathway is not constitutively
activated in platelets derived from sporadic ET patients in the
absence of TPO.15 Also, the somatic mutations of the c-MPL
gene have not been identified in sporadic ET patients yet.16 This
indicates that the FET pedigree reported here is an exceptional
case, but one that provides novel insights into ET and the
operation of the Tpo-c-Mpl system.
References
1. Kondo T, Okabe M, Sanada M, et al. Familial essential thrombocythemia associated with onebase deletion in the 5⬘-untranslated region of the
thrombopoietin gene. Blood. 1998;92:1091-1096.
2. Ghilardi N, Wiestner A, Kikuchi M, Ohsaka A,
Skoda RC. Hereditary thrombocythaemia in a
Japanese family is caused by a novel point mutation in the thrombopoietin gene. Br J Haematol.
1999;107:310-316.
3. Ihara K, Ishii E, Eguchi M, et al. Identification of
mutations in the c-mpl gene in congenital
amegakaryocytic thrombocytopenia. Proc Natl
Acad Sci U S A. 1999;96:3132-3136.
4. Ballmaier M, Germeshausen M, Schulze H, et al.
c-mpl mutations are the cause of congenital
amegakaryocytic throbocytopenia. Blood. 2001;
97:139-146.
5. Tonelli R, Scardovi AL, Pession A, et al. Compound heterozygosity for two different amino-acid
substitution mutations in the thrombopoietin receptor (c-mpl gene) in congenital amegakaryocytic thrombocytopenia (CAMT). Hum Genet.
2000;107:225-233.
6. van den Oudenrijn S, Bruin M, Folman CC, et al.
Mutations in the thrombopoietin receptor, Mpl, in
children with congenital amegakaryocytic thrombocytopenia. Br J Haematol. 2000;110:441-448.
7. Migliazza A, Bosch F, Komatsu H, et al. Nucleotide sequence, transcription map, and mutation
analysis of the 13q14 chromosomal region deleted in B-cell chronic lymphocytic leukemia.
Blood. 2001;97:2098-2104.
8. Kato M, Iida S, Komatsu H, Ueda R. Lack of Ku80
alteration in multiple myeloma. Jpn J Cancer Res.
2002;93:359-362.
9. Kitayama H, Kanakura Y, Furitsu T, et al. Constitutively activating mutations of c-kit receptor tyrosine kinase confer factor-independent growth
and tumorigenicity of factor-dependent hematopoietic cell lines. Blood. 1995;85:790-798.
10. Miyakawa Y, Oda A, Druker BJ, et al. Recombinant thrombopoietin induces rapid protein tyrosine phosphorylation of Janus kinase 2 and
Shc in human blood platelets. Blood. 1995;86:
23-27.
11. Michiels JJ, Juvonen E. Proposal for revised diagnostic criteria of essential thrombocythemia
and polycythemia vera by the thrombocythemia
vera study group. Semin Thromb Hemost. 1997;
23:339-347.
12. Abe M, Suzuki K, Inagaki O, Sassa S, Shikama H. A
novel MPL point mutation resulting in thrombopoietin-independent activation. Leukemia. 2002;16:
1500-1506.
13. Weiner DB, Liu J, Cohen JA, Villiams WY, Greene
MI. A point mutation in the neu oncogene mimics
ligand induction of receptor aggregation. Nature.
1989;339:230-231.
14. Onishi M, Mui AL, Morikawa Y, et al. Identification
of an oncogenic form of the thrombopoietin receptor MPL using retrovirus-mediated gene transfer. Blood. 1996;88:1399-1406.
15. Horikawa Y, Matsumura I, Hashimoto K, et al.
Markedly reduced expression of platelet c-mpl
receptor in essential thrombocythemia. Blood.
1997;90:4031-4038.
16. Taksin AL, Couedic JP, Dusanter-Fourt I, et al.
Autonomous megakaryocyte growth in essential
thrombocythemia and idiopathic myelofibrosis is
not related to a c-mpl mutation or to an autocrine
stimulation by Mpl-L. Blood. 1999;93:125-139.
AQ0: Changed the short running head so it would
have fewer than 50 characters, per journal limit.
From www.bloodjournal.org by guest on March 5, 2016. For personal use only.
2004 103: 4198-4200
doi:10.1182/blood-2003-10-3471 originally published online
February 5, 2004
Familial essential thrombocythemia associated with a dominant-positive
activating mutation of the c-MPL gene, which encodes for the receptor
for thrombopoietin
Jianmin Ding, Hirokazu Komatsu, Atsushi Wakita, Miyuki Kato-Uranishi, Masato Ito, Atsushi Satoh,
Kazuya Tsuboi, Masakazu Nitta, Hiroshi Miyazaki, Shinsuke Iida and Ryuzo Ueda
Updated information and services can be found at:
http://www.bloodjournal.org/content/103/11/4198.full.html
Articles on similar topics can be found in the following Blood collections
Brief Reports (1868 articles)
Clinical Trials and Observations (4268 articles)
Hematopoiesis and Stem Cells (3359 articles)
Hemostasis, Thrombosis, and Vascular Biology (2494 articles)
Signal Transduction (1930 articles)
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society
of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.