Outline
advertisement

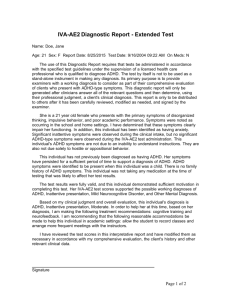
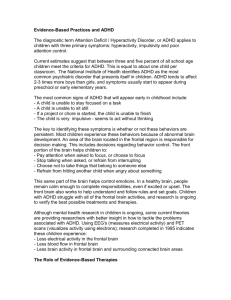
Attention Deficit Hyperactivity Disorder: Neurodevelopmental Perspectives on Current Research and Treatment Development JJeffreyy M. Halperin, p , Ph.D. Department of Psychology Queens College, City University of New York Department of Psychiatry The Mount Sinai School of Medicine Outline Neurodevelopmental Perspectives on ADHD Re--thinking the Neural Substrates of ADHD Re from a Lifespan Perspective Queens College Preschool Project (QCPP) Relations between neuropsychological and behavioral functioning over time Implications for understanding ADHD Implications for Treatment and Future Research ADHD Across the Lifespan Adults Adolescents School-age Preschoolers 1 What Causes ADHD? Genetic Determinants Environmental Factors Brain Dysfunction Hypothesized Neural Anomalies in ADHD Prefrontal (PFC)/Executive Impairments? Subcortical state regulation anomalies? Dopaminergic insufficiencies? Poor alpha 2a receptor functioning? Behavioral and neurocognitive heterogeneity suggest that it may not be the same in all with the disorder ADHD is a developmental disorder, but most models do not consider development! 2 ADHD is Likely Related to Catecholaminergic Innervation of the Frontal Lobe and Basal Ganglia Developmental Considerations PFC and the EFs it mediates develop relatively late in ontogeny Synaptic pruning: 5 – 16 years years--old Myelination:: through early adulthood Myelination EFs develop into at least early adulthood Yet ADHD is always present in early childhood ADHD tends to get better with age Developmental trajectories of behavioral deficits associated with ADHD and early frontal lobe lesions ADHD Early PFC Lesion* Preschool Later in Childhood Present in Childhood Always Sometimes Adolescent Trajectory Improve or remain the same Worsen Onset of Symptoms *Anderson et al. 1999; Trauner et al. 2001 3 Corresponding trajectories for A) the remission of ADHD, B) the development of EFs, and C) the maturation of white matter in the DLPFC. Figures from A) Hill & Schoener, 1996; B) Paus, 2005; and C) Barnea-Goraly et al., 2005. Note: FA = fractional anisotrophy; SSRT = Stop-signal reaction time. A Developmental Model of ADHD Pathophysiology* Distinct neural and cognitive mechanisms are involved in the etiology of and recovery from ADHD ADHD is due to non-cortical neural dysfunction that is present early in ontogeny and remains static throughout the lifetime PFC circuitry is not linked to the cause of ADHD, but is involved in recovery The diminution of symptoms with age is accounted for by the degree to which the development of the PFC/EFs are able to compensate through the implementation of ‘top down’ regulatory control. *Halperin & Schulz (2006). Psychological Bulletin. Predictions from Model Improvements in behavior over time should be differentially linked to distinct types of neurocognitive functioning M Measures off hi higher h cortical ti l ““recovery”” mechanisms h i should parallel later status; effortful/goal effortful/goal--directed Measures of subcortical “causal” mechanisms persist irrespective of later clinical status; less conscious control/stimulus--driven control/stimulus 4 Preliminary Support from Longitudinal Study of Adolescents with Childhood ADHD Irrespective of followfollow-up status, those with childhood ADHD are impaired on less consciously controlled measures (e.g., RTSD, ankle movements)1,2 ADHD--p ADHD persisters are most impaired p on measures requiring effortful control (e.g., working memory, CPT errors, conflict resolution) 1,2 Prefrontal activation obtained during effortful processing (i.e., conflict resolution), parallels severity of adult symptomatology 3,4 1Halperin 3Schulz 2 Bedard 4Schulz et al. (2008) JCPP. et al., In review. et al. (2005a) Neuropsychology et al. (2005b) JAACAP Longitudinal Study of Urban Youth with ADHD: Baseline Assessment Initially recruited 1990 – 1997 Clinically--referred sample Clinically Age g at initial assessment 7 – 11 yyears Teacher ratings: IOWA Conners Parent ratings: CBCL Parent Interview: DISC Comorbidity in Childhood Diagnosis N = 98 % ODD 49.0 % CD 32.7 % Anxiety 31.6 % Mood 10.2 5 Adolescent Characteristics of Probands and Matched Control Group Childhood ADHD N Mean Age (years) Mean WAISWAISIII FSIQ % Male Controls 98 85 18.4 18.5 93.3 96.8 88.8 87.1 Axis I Diagnoses in patients with childhood ADHD and never-ADHD controls ADHD Controls ADHD (%) 49.5 0 <.001 Depression (%) 4.7 .001 Anxiety (%) 21.6 19 6 19.6 82 8.2 < 05 <.05 ODD (%) CD (%) 22.7 26.8 1.2 1.3 <.001 <.001 Alcohol Abuse/Dep. (%) 15.5 7.1 Drug Abuse/Dep. (%) 44.3 27.1 .08 <.05 Adolescents Diagnosed with ADHD During Childhood 35 ADHD D-RS 30 25 20 Controls Remitters Persisters 15 10 5 0 Parent* Self* *All groups differ, p < .05 6 Working Memory and ADHD Outcome* Controls (n=85) ADHD (n=98) Remitters (n=29) 100 100 WAIS-III WM MI Controls (n=85) Persisters (n=44) 95 95 90 90 85 85 80 Controls vs. ADHD: p=.007; d=.41 80 Controls vs. Remit: p>.30; d=.20 Controls vs. Persist: p=.03; d=.43 *Halperin et al. 2008 Perceptual Inhibition Never‐ADHD ADHD‐partial remitters ADHD‐persisters 190 550 SDR RT (ms) Mean RT (ms) 650 450 160 130 100 350 70 Compatible Incompatible Compatible Incompatible Main effect Condition: p < .001 Main effect Group: p = .004 GxC Interaction: p = .04 Main effect Condition: p < .001 Main effect Group: p = .08 GxC Interaction: p > .10 Bedard et al. In Review. Continuous Performance Test (CPT(CPT-IP) Errors, which reflect effortful processing, processing, as a Function of Adolescent/Adult Status 16 80 14 78 12 76 10 74 Controls Remitters Persisters 72 8 Controls Remitters Persisters 6 70 4 68 2 0 66 Percent Hits* Percent False Alarms* *Controls differ from Persisters, p < .05 Halperin et al. 2008 7 Less Conscious Reaction Time Measures as a Function of ADHD Persistence Controls Remitters Persisters 250 650 600 550 200 500 450 150 400 350 100 300 250 200 Hit RT (in msec.)* *Persisters < Controls, p = .045 50 RT SD (in msec.)** **Persisters = Remitters > Controls, p < .001 Activity Level in Adolescents as a Function of Persistence of ADHD Persisters 100 90 80 70 60 50 40 30 20 10 0 Ankle* Remitters Controls Waist *Persisters = Remitters > Controls Halperin et al. 2008 Activation During Go/No Go/No--go Task Schulz et al. 2005; JAACAP 8 Stimulus and Response Conflict Task BLOCKED DESIGN Location Control + + 0 30 Stimulus Characteristic + 90 60 Prepotent Motor Response Control + + 150 120 Time (seconds) 180 Combined + 210 240 270 Block 1 Control A Block 2 + Location TRIALS + + C + Control B + + Block 4 Block 3 Stimulus Characteristic c + Prepotent Motor Response C + C + Block 5 Block 6 Combined C + C + + C 0 1500 Time (milliseconds) 2000 Activation During Conflict Task Schulz et al. 2005; Neuropsychology The Preschooler 9 Queens College Preschool Project (QCPP) Overview of Methodology Gather parent and teacher ADHD ratings on a g sample p of 3 and 4 yearyear y -old children large Comprehensive inin-lab assessment of identified children/parents Semi--annual parent and teacher behavior ratings Semi In--lab reIn re-evaluation annually Identify “at risk” and “control” children QCPP: Classification Criteria At Risk (AR) Group: At least 6 Hyperactivity/Impulsivity or Inattention symptoms rated 2 or greater (0 – 3 scale) by parent, teacher,, or a combination of the two Typically--developing (TD) Group Typically Group:: Fewer than 3 Hyperactivity/Impulsivity and Inattention symptoms rated 2 or greater by both parent and teacher QCPP: Sample Characteristics TD (N=76) At--Risk At (N=140) t p Age (in years) 4.20 (.48) 4.36 (.46) 2.46 <.05 % Boys B 67 1 67.1 75 7 75.7 1.84* 1 84* > .10 10 WPPSI FSIQ 112.63 (12.0) 101.96 (12.8) 5.96 ADHD--RSADHD RS-P 8.74 (4.9) 27.6 9 (10.9) 17.57 < .001 ADHD--RSADHD RS-T 4.63 (4.3) 30.32 (13.5) <.001 20.64 < .001 *Chi Square 10 ADHD and ODD Diagnoses in AtAt-Risk Group (N = 140) Primary Measures (for this presentation) Parent and Teacher Ratings ADHD-RS ((DuPaul ADHDDuPaul et al. 1998) Children’s Problem Checklist (CPC; Healey et al. 2008) NEPSY Attention/Executive Function Language Sensorimotor Visuospatial Memory QCPP: Solid State Actigraph Recordings Ankle* Waist* 1400 600 1200 500 1000 400 800 300 600 400 200 200 0 100 Boys Controls Girls At-risk 0 Boys Girls *Main Effect Group, p < .001 11 QCPP: NEPSY Domain Scores (Baseline)* Typically-developing At-risk 115 110 105 100 95 90 85 80 75 70 Exec/Att Lang. Sen/Mot Vis/Sp Mem * All p < .001 NEPSY Subtest Scores in Hyperactive Preschoolers Typically-developing At-risk on Ph Bo dy Pa r t* Pr oc Co m p. D es .C op Bl . k. C on . Vi s. At t. St a I m t ue .H an d Vi sm N ot ar .M em Se . nt .R ep . 13 12 11 10 9 8 7 6 *p > .05 QCPP Timeline ADHD-RS CPC NEPSY ADHD-RS CPC NEPSY ADHD-RS ADHD RS CPC 0 6 12 ADHD-RS ADHD RS CPC ADHD-RS CPC NEPSY 18 24 ADHD-RS ADHD RS CPC 30 Time in Months 12 Are Changes in ADHD Severity Over Time Related to Improved Neuropsychological Functioning in AtAt Risk Children? ADHD severity assessed via a single latent variable Symptoms Impairment Parent ADHD-RS Parent CPC ADHD Severity Teacher ADHD-RS Teacher CPC Individual Trajectories for ADHD Severity in At--Risk Children At 3.0 ADHD factor z-score 2.0 1.0 0 -1.0 -2.0 -3.0 0 6 12 18 24 30 Time in months 13 Change in Neuropsychological Functioning Assessed via a Single Latent Variable (Baseline to 24 Month) Attention/ Executive Memory Change in Neuropsych. Functioning Visuospatial Language Sensorimotor Distribution of NEPSY Change Scores Mean = -0.07 SD = 1.00 N = 101 Change in NEPSY Associated with improved ADHD trajectory 1.0 <20%ile (n=21, 91% ADHD dx at 24m) 20-40%ile (n=19, 68% ADHD dx at 24m) 40-60%ile (n=20, 75% ADHD dx at 24m) ADHD factor zz-score 60-80%ile (n=21, 57% ADHD dx at 24m) 0.5 Fixed Effects: Intercept: p=.058 p p p=.007 Linear Slope: Quadratic Slope: p=.54 >80%ile (n=20, 45% ADHD dx at 24m) 0 -0.5 -1.0 0 6 12 18 24 30 Time in months 14 Percentage of Cases Meeting Criteria for ADHD at 24--month Follow 24 Follow--up as a Function of Change in NEPSY Score Less improvement More improvement Chi Square = 11.18, p = .025 Do Changes in ADHD Severity Over Time Precede or Follow Changes in Neuropsychological Functioning? At-risk children N-1 N-2 .24* N-3 .99* N-4 N-5 N-1 .21 .20* NeuroPsychological Functioning Baseline N-2 .34*** .59*** .99* N-3 .52*** N-4 N-5 .20* .42** ADHD parent .21* ADHD teacher .42*** CPC parent .19* CPC teacher ADHD parent N-5 .27* -.19 -.40** Attention Deficit & Impairment at Time 2 .82*** N-4 .66*** NeuroPsychological Functioning at Time 3 .99*** -.07 .76 N-3 48** -.02 Attention Deficit & Impairment Baseline N-2 .49** .52*** NeuroPsychological Functioning at Time 2 .33* N-1 .63*** .15* .34** ADHD teacher Attention Deficit & Impairment at Time 3 .81*** .99*** .56*** CPC parent CPC teacher ADHD parent .38* .65*** ADHD teacher CPC parent .21* CPC teacher 15 Typically-developing children N-1 56** N-2 .40** N-3 99** N-4 .99** N-5 N-1 .37** NeuroPsychological Functioning Baseline .55*** N-2 N-3 .49*** .74*** N-4 .67*** N-5 NeuroPsychological Functioning at Time 2 .60 N-1 .25** ADHD parent .16** ADHD teacher .14* .13* CPC parent CPC teacher ADHD parent N-5 .58*** -.08* Attention Deficit & Impairment at Time 2 .73*** N-4 .68*** -.17 -0.04 .73 N-3 .46** NeuroPsychological Functioning at Time 3 87*** -0.19 Attention Deficit & Impairment Baseline N-2 .49** .66*** .54*** .57** ADHD teacher .49* CPC parent Attention Deficit & Impairment At Time 3 .72** .43*** CPC teacher .87** ADHD parent .75*** ADHD teacher .94*** CPC parent .63*** CPC teacher RMSEA = .067; 90% CI, .061-.072; CFI = .78 Summary of Preschool Data Behavioral impairment related to ADHD symptoms is clearly apparent during the preschool years Behavioral difficulties are accompanied p by a wide array of cognitive deficits Improved behavioral functioning is related to and may be preceded by improved neuropsychological functioning Implications for Conceptualizing ADHD ADHD is a lifespan disorder that must be conceptualized within the context of a developmental framework Within the framework of o ourr model model, ADHD might have a unitary cause; behavioral and cognitive heterogeneity should increase with age Although we might not be able to “cure” ADHD, the trajectory should be susceptible to positive and negative influences 16 Implications for Treatment If ADHD is due to subcortical disorder that is relatively permanent, can we develop lasting treatments? Must take advantage of early cortical neurodevelopment, that may be linked to clinical/behavioral /b improvement across the lifespan. f Perhaps, environmental manipulations targeted at facilitating experience experience--dependent neurodevelopmental processes such as synaptic pruning, dendritic arborization and mylenation could be employed to facilitate recovery TEAMS Training Executive, Attention and Motor Skills TEAMS is based on these ideas: 1) ADHD is associated with deficient neural networks that: • affect a wide array of neurocognitive and behavioral processes • may not be identical in all children with the disorder; 2) Neurodevelopment is sensitive to and can be positively affected by appropriate environmental influences; 3) Effective environmental stimulation will be best achieved within a social context; 4) Core activities of the treatment must be intrinsically rewarding (i.e., fun) rather than extrinsically reinforced (e.g., parental praise or tokens). This will: • facilitate self-imposed continuation of the intervention • lead to generalization over time and across settings. 17 How Do We Think TEAMS Will Work? • ‘Exercise the brain’ using game-like activities which employ neurocognitive and motor skills. • Small group setting (4-5 children) • Parent P t education d ti about b t ADHD and d support • Encourage parents to engage their children in these game-like and exercise activities at home. Directions for Future Research Need to develop and apply better measures of stimulus--driven or “bottomstimulus “bottom-up” processes Need to add neuroimaging to the mix in developmental studies st dies Does cognitive/behavioral improvement relate to measurable changes in brain structure and function? Do genes moderate ADHD trajectory? Development of interventions to alter the trajectory over the lifespan Preschool Studies Acknowledgements David Marks, Ph.D. Dione Healey, Ph.D. Olga Berwid Berwid,, Ph.D. Elizabeth Kera, Kera, Ph.D. Amita Santra Santra,, Ph.D. Chaya Gopin A i k Mlodnicka Agnieszka Ml d i k Beth Rabinovitz Katya Staikova Michelle Bubnik Katia Castelli Bipasha Basu NIMH Adolescent Studies Jeffrey Newcorn, Newcorn, M.D. Carlin Miller, Ph.D. Joey Trampush Virginia Fresiello Seth Harty Tobey Busch Dana Barowsky Neuroimaging Kurt Schulz, Ph.D. Jin Fan. Ph.D. Chuck Tang, Ph.D. Suzanne Clerkin, Clerkin, Ph.D RO1 MH060698 RO1 MH068286 1R21MH085898 18 Thank you. you 19