Effects of cardiac rehabilitation 1085
advertisement

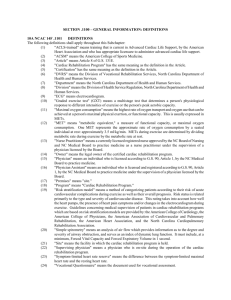
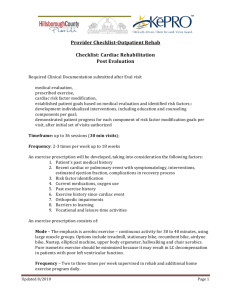
Effects of cardiac rehabilitation P5796 | BEDSIDE Low disparity and high attendance rate to out-patient cardiac rehabilitation after systematic referral H. Rasmusen, M. Frederiksen, A. Holdgaard, E. Prescott. Bispebjerg Hospital of the Copenhagen University Hospital, Department of Cardiology, Copenhagen, Denmark Purpose: Outpatient Cardiac Rehabilitation (CR) improves prognosis in coronary heart disease (CHD) but remains underutilized, especially among women, ethnic minorities, and the elderly. We hypothesized that automatized early referral will increase attendance and reduce disparities. Methods: All consecutive patients discharged from our hospital with acute coronary syndrome (ACS) or stable CHD in a 24-months period from February 2011 were monitored for referral to and participation in CR after introduction of automatized early referral. Results: 817 patients were included in the study. Index event was STEMI (22%), NSTEMI (26%), unstable angina (18%) and stable CHD (34%). Mean age was 65 (inter quartile range 57-74), 246 (30%) were women and 138 (17%) belonged to an ethnic minority. Overall, 297 (36%) did not participate in CR: 248 (84%) were not referred and 49 declined to participate. Main reasons for non-referral were severe co-morbidity, living in a nursing home or recent participation in CR. The non-referred were older (mean age 69, p for difference compared to referred <0.001), 37% were women (p=0.002), and 16% belonged to an ethnic minority (p=0.81). In a logistic regression younger age (P<0.001) and STEMI versus other index events (OR 2.2, p=0.001) but not gender (p=0.12) or ethnicity (p=0.34) predicted referral after mutual adjustment. Of the 569 patients referred for CR, 49 (9%) declined participation. These nonattendees did not differ from attendees with regard to gender, ethnicity, age or index-event. In relation to traditional cardiovascular risk factors, smokers (p<0.001) and patients with diabetes (p=0.003) were less likely to attend whereas hypertension, hypercholesterolemia, family history of CHD, BMI and physical inactivity did not predict attendance. Conclusion: The study indicate that automatized referral results in very high rates of participation in cardiac rehabilitation with no gender or ethnic disparities. In this unselected sample of consecutive patients discharged with CHD, 74% participated in CR. Main reason for non-participation was non-referral: Among patients deemed eligible to CR only 9% declined participation. P5797 | BEDSIDE Effects of music therapy on endothelial function in patients with coronary artery disease participating in rehabilitation M. Deljanin Ilic 1 , S. Ilic 1 , R. Pavlovic 2 , G. Kocic 2 , D. Kalimanovska Ostric 3 , V. Stoickov 1 , D. Simonovic 1 , V. Ilic 1 . 1 Institute of Cardiology, Medical Faculty University of Nis, Niska Banja, Serbia; 2 Institute of Biochemistry, University of Nis, Nis, Serbia; 3 Clinic of Cardiology, Clinical Center of Serbia, University of Belgrade, Belgrade, Serbia Purpose: To evaluate the effects of listening to favorite music on the endothelial function, assess through changes of circulating blood markers of endothelial function: the stable end product of Nitric Oxide (NOx), Dimethylarginine (ADMA), Symmetric Dimethylarginine (SDMA) and Xanthine Oxidase (XO), in patients (pts) with Coronary Artery Disease (CAD). Methods: 74pts with stable CAD were studied. At baseline and 3 weeks later, in all pts values of NOx, ADMA, SDMA and XO were evaluated and exercise test was performed. After the initial study, pts were randomized to trained (T,n=33), music and trained (MT, n=31) and music (M,n=10) group. Patients in T and MT group underwent a supervised 3 weeks aerobic exercise training at residential center. Additional to exercise training, patients in MT group were listening to their favorite music, for half an hour, every day. Patients in M group received usual community care and were listening to their favorite music for half an hour every day. Results: After 3 weeks NOx increased in T group (from 33.0±13.0 to 42.8±11.0 μmol/l, P< 0.005), MT group (from 34.5±7.1 to 49.6±12.6 μmol/l, P<0.0005) and M group (from 32.8±6.5 to 36.5±7.0 μmol/l, ns). However increase in NOx was higher in MT than in T and M group (P=0.0246 and P<0.005), and in T than in M group (P<0.05). Value of ADMA as well of SDMA decreased in all three groups (ns) after 3 weeks, and this reduction was the most pronounced in MT group. Compared to the baseline, value of XO at the end of the study was significantly lower in T, MT and M group (P<0.0005 for all of them). However at the end of the study value of XO was significantly lower in MT than in T and M group (P<0.005 and P<0.0005) and in T than in M group (P<0.001). After 3 weeks exercise capacity significantly increased in T, MT and M group (P<0.001, P<0.001 and P<0.025), and increase in exercise capacity was higher in MT than in T and M group (39% vs 29% and 19%). Conclusion: In pts with CAD listening to favorite music alone as well as in addition to regular exercise training, improves endothelial function. Combination of music and exercise training leads to more favorable improvement in endothelial function, expressed through higher increased of NOx, decreased of ADMA, SDMA and XO than exercise training alone. This improvement in endothelial function is associated with significant improvement in exercise capacity. P5798 | BEDSIDE Significant residual coronary obstruction: impact on short and long-term outcomes of a cardiac rehabilitation program in coronary heart disease I. Rangel, A. Rocha, C. Sousa, F. Melao, J. Rodrigues, M. Paiva, A.S. Correia, V. Araujo, V. Parada-Pereira, M.J. Maciel. Sao Joao Hospital, Porto, Portugal Introduction: There is evidence that cardiac rehabilitation programs (CRP) exert significant benefits in patients with coronary artery disease (CAD). However, safety and influence of residual significant coronary stenosis on CRP outcomes remain unclear. Methods: We retrospectively analyzed clinical, angiographic and functional data of a total of 287 patients referenced to a CRP after an acute coronary syndrome (ACS), between September 2008 and December 2011. Incomplete revascularization (IR) was defined by the presence of residual structural stenosis in any major epicardial vessels (>70%), consequent to unfavorable anatomy to angioplasty (PCI). Pre and post CRP functional capacity was assessed using exercise stress testing metabolic equivalents (METS). A composite outcome of overall mortality and nonfatal cardiovascular events was evaluated. Furthermore, functional capacity at follow-up evaluation was estimated using the patient-reported Duke Activity Status Index (DASI). Results: We analyzed 280 patients, mostly male (88%), aged 54±10 years. Incomplete revascularization (IR) was found in 61 (23%) patients. IR patients more frequently presented previous diagnosis of coronary heart disease (CHD) (25% vs 12%, p=0.009). They and also tended to be more often women (36% vs 22%, p=0.082) and diabetic (21% vs 14%, p=0.155), although these differences were not statistically significant. Physical training in pts with IR was safe and well tolerated. Exercise capacity increased significantly in both groups (peak MET level: + 0.7±1.7, p=0.013, in IR vs 1,0±1.7, p<0.001, in complete revascularized [CR] patients). Maximum functional capacity at program completion was considerable in both groups (10.2±2.1 [IR] vs 10.7±2.2 METs [CR], p>0.05). The mean follow-up time was 30±13 months. Both groups showed a similar perceived physical performance, using DASI estimated peak METs (8.0±1.6 [IR] vs 8.3±1.6 [CR], p>0.05). Composite endpoints were found in 36 (10%) patients and occurred more in IR patients (19% vs 13%); however, the difference was not statistically significant (p>0.05). Kaplan Meyer showed no difference in the likelihood of a cardiovascular event, between IR and CR patients (p>0.05). Conclusion: IR patients take similar advantage from a CRP and maintain an equivalent long-term functional capacity. Although signficant residual stenosis is frequently regarded as a relative exclusion criteria for cardiac rehabilitation, these patients derive similar benefits both in short and long-term functional capacity, cardiovascular morbidity and mortality. P5799 | BEDSIDE Comprehensive cardiac rehabilitation increases the serum EPA level and EPA/AA ratio in patients with acute myocardial infarction K.K. Kada, N.T. Tsuboi, H.M. Murakami, T.O. Okada, T.O. Ota, T.S. Sumi, H.K. Kojima, S.R. Riku, M.Y. Yosida. Social Insurance Chukyo Hospital, Nagoya, Japan The residual risk of cardiovascular events after statin therapy might be explained, in part, by low levels of serum n-3 Polyunsaturated Fatty Acids (PUFAs), espe- Downloaded from http://eurheartj.oxfordjournals.org/ by guest on March 4, 2016 (METS) achieved during the exercise stress testing. Perception of QoL was estimated through Medical Outcomes Study Short Form 36 (MOS SF-36, physical and mental summary components). Both measurements were assessed at program initiation and completion and at 12 months of follow up. Improvement in FC and QoL perception were measured by the difference between METS and MOS SF-36 values. Results: In our population, 89.5% patients were male, mean age was 54.0±9.6 years. Patients were divided into 2 groups according to LV function: group 1 (83.3%) with left ventricle ejection fraction ≥ 45% and group 2 (16.7%) with left ventricle ejection fraction < 45%. After the CRP, FC improved significantly in both groups: from 9.9±2.1 to 10.8±2.1 METS (p=0.001) in group 1 and from 9.1±2.4 to 10.5±2.3 METS (p=0.001) in group 2. This functional capacity improvement persisted in both groups at 12 month evaluation: 11.7±6.7 METS in group 1 (p=0.042) and 10.2±2.0 METS in group 2 (p=0.001). The same kind of results was observed regarding QoL: CRP achieved a significant increase in physical and mental summary perception components in both groups (p<0.05 for all analysis). However, at 12 month follow up this improvement only reached statistical significance in group 1 (p<0.05). No between-group differences were identified in either initial or final FC, QoL and magnitude of improvement, meaning that the degree of improvement was similar between patients with and without significant systolic dysfunction. Conclusions: FC capacity improvement achieved after completion of a cardiac rehabilitation program is sustained in time and independent of initial left ventricle function. The long term gain in terms of QoL seems only to persist in patients with no significant LV dysfunction. 1085 1086 Effects of cardiac rehabilitation cially Eicosapentaenoic Acid (EPA) and Docosahexiaenoic Acid (DHA). In addition, a recent study has shown that statin therapy reduces the serum n-3 PUFAs levels. Purpose: We investigated whether Comprehensive Cardiac Rehabilitation (CCR) affects the serum PUFA levels in patients with acute myocardial infarction (AMI). Methods: Fifty-six consecutive AMI patients who underwent optimal medical therapy, including statins and CCR (e.g., assessment of risk factors, dietary counseling, exercise training and smoking cessation intervention) were enrolled in this study. Patients taking EPA or DHA supplements were excluded from the study. We compared the data for all patients between the AMI onset and 9.5 months after the onset. Results: The serum LDL-cholesterol level decreased markedly (115.0±36.9 mg/dl to 82.3±25.6 mg/dl, p < 0.001), while the serum HDL-cholesterol level stayed constant (45.4±17.2 mg/dl to 43.5±12.0 mg/dl, p = 0.54). The serum EPA level increased significantly (45.6±20.2 μg/dl to 65.1±31.7 μg/dl, p = 0.004), whereas the serum DHA and arachidonic acid (AA) levels remained unchanged (133.7±40.8 μg/dl to 134.0±51.9 μg/dl, p = 0.98 and 171.0±45.7 μg/dl to 186.0±50.3 μg/dl, p = 0.19, respectively). These changes resulted in a significant elevation in the serum EPA/AA ratio (0.28±0.14 to 0.37±0.28, p = 0.03), but not in the DHA/AA ratio (0.81±0.27 to 0.74±0.28, p = 0.28). Conclusions: In AMI patients, CCR and optimal medical therapy without EPA or DHA supplementation increased the serum EPA level and EPA/AA ratio. Lifestyle modification with CCR might therefore cancel the negative effects of statins on the serum PUFAs levels. whether discharge FIM score at acute phase (phase I) CR can predict subsequent patient discharge to their home (as opposed to another destination at discharge); the FIM cutoff score that best predicted discharge home was calculated. Methods: This study included 1015 patients enrolled during a 24-month period from January 2010 through December 2011. Criteria for participating in CR included acute myocardial infarction, cardiovascular surgery, and others. The measurement items were FIM score at starting of CR and at discharge, length of stay (LS), and CR discharge outcome (discharge to home or other). Furthermore, data on age, sex, and presence of heart failure at admission were also obtained. In a multiple logistic-regression analysis, home discharge was set as a dependent variable. All other data were adopted as independent variables. The FIM cutoff score for discharge home was determined using receiver-operating characteristic (ROC) curve analysis, and the area under the curve (AUC) was calculated using the ROC curve. This research was approved by the Ethics Committee of our institution. Participants provided informed consent in accordance with the principles of the Declaration of Helsinki. Results: Home discharge was possible for 760 people (74.9%); the remaining 255 (25.1%) had other destinations at discharge. After regression analysis, FIM at discharge, LS, and presence of heart failure were extracted as prediction factors (Table). The capability of the regression model to correctly predict discharge home was 88.0%. ROC curve analysis determined the FIM cutoff point to be 100.5 points at discharge, with an AUC of 0.918. Prediction Factors for Home Discharge P5800 | BENCH Experienced fatigue is decreased after cardiac rehabilitation and at one year follow up M.E. Van Geffen 1 , N. Ter Hoeve 1 , M. Sunamura 1 , R.T. Van Domburg 2 , H.J.G. Van Den Berg-Emons 3 . 1 CAPRI Hartrevalidatie Rotterdam, Rotterdam, Netherlands; 2 Erasmus Medical Center, Department of Cardiology, Rotterdam, Netherlands; 3 Erasmus Medical Center, Department of Rehabilitation Medicine and Physical Therapy, Rotterdam, Netherlands Purpose: To explore the short and long term effect of cardiac rehabilitation (CR) on experienced fatigue. Additionally, to explore the effects of CR on physical fitness and social participation and to investigate whether experienced fatigue is influenced by these constructs. Methods: In total, 89 patients (79.8% men, 58 years) that participated in the Capri rehabilitation program were included in this study. The rehabilitation program consists of exercise training twice a week and information modules on risk factors of cardiovascular disease. Primary outcome was experienced fatigue as measured with the Fatigue Severity Scale (FSS) and the Visual Analogue Scale (VAS). Secondary outcomes were physical fitness and social participation. Measurements were taken pre- and post-rehabilitation and at one year follow-up. Results: Experienced fatigue decreased from baseline to post-rehabilitation and sustained till one year follow-up (P<0.05). Physical fitness was improved postrehabilitation (P<0.05), but declined at one year follow-up (P<0.05). Participation scores were improved post-rehabilitation (P<0.05), these improvements sustained till one year follow-up. A significant (P<0.05) correlation of 0.431 was found between the differences in the restrictions domain of USER-P and fatigue (FSS). FIM discharge LS Heart Failure Coefficient (β) Standard Error Wald χ2 −0.59 0.12 −0.449 0.004 0.005 0.229 225.1 6.82 3.85 p Odds Ratio 95% CI <0.001 <0.01 <0.05 0.943 1.012 0.683 0.935–0.950 1.003–1.021 0.408–0.999 CI, confidence Interval; FIM, Functional Independence Measure; LS, Length of Stay. Conclusion: Discharge FIM score at phase I CR may be the strongest predictor of a patient subsequently being discharged home (rather than to another destination); the FIM cutoff score was 101 points. P5802 | BEDSIDE Gender differences in risk profile and response to a cardiac rehabilitation program after an acute coronary syndrome F. De Torres Alba, S. Rosillo Rodriguez, D. Gemma, A. Iniesta Manjavacas, S. Valbuena Lopez, S. Del Prado Diaz, N. Montoro Lopez, A. Castro Conde, R. Dalmau Gonzelez-Gallarza, J.L. Lopez Sendon. University Hospital La Paz, Department of Cardiology, Madrid, Spain Objectives: Women have a different distribution of lifestyle risk factors of coronary artery disease than men. In order to define the priorities of a cardiac rehabilitation program (CRP) for women, we compared the risk profile and the response to a CRP of women vs. men, in a cohort of patients with a recent admission for ACS submitted to our CRP. Material and methods: We studied 694 patients, 96 women (13.5%) and 598 men. We compared the risk profile and the modification of lifestyle related risk factors after an 8-week exercise-based CRP between men and women. Results: Men and women presented a similar distribution of risk factors (Table 1), except for abdominal obesity, which was the most prevalent risk factor in women and was significantly more prevalent in women compared to men, and for overweight. Functional capacity in METs assessed by a symptoms-limited exercise test on admission to CRP was significantly lower in women (6.3 vs. 7.9 METs, p <0.001). Adherence to CRP and usual pharmacological measures for secondary prevention were similar in both men and women. After CRP, both women and men experienced an important improvement in functional capacity (gain in METs 3.6 vs. 3.5, p = NS). However, despite dietary recommendations, only 25% of overweight women lost weight (average loss of 0.5 kg at the end of the program), and abdominal girth loss was modest in general, and significantly lower in women than in men (1.2 vs. 2.2 cm of abbominal girth reduction). At 3 months, only 74% of female smokers remained abstinent compared to 86% of men (p<0.05). This difference became greater at 12 months follow up (59% vs. 80% of abstinence, p<0.001). Figure 1. Experienced fatigue Risk factor distribution among men and women Conclusion: Experienced fatigue was deceased post-rehabilitation and sustained decreased till one year follow-up. The decrease in experienced fatigue was associated with improvements in experienced restrictions domain of social participation domain. P5801 | BEDSIDE Functional independence measure analysis in patients undergoing phase I of cardiac rehabilitation N. Sasanuma, K. Takahashi, T. Tanaka, S. Mabuchi, N. Kodama, M. Ohyanagi, T. Masuyama, Y. Miyamoto, K. Domen. Hyogo College of Medicine, Nishinomiya, Japan Purpose: Previous analysis of the Functional Independence Measure (FIM) scale in patients with chronic heart disease have given little consideration to scores during the acute phase of cardiac rehabilitation (CR). Our objective was to determine Age Hyper- Diabetes Dys- Smoking Inactivity Obesity Over- Abdominal (yrs) tension lipidemia weight obesity Women (n=96) 58.2 52.6% Men (n=598) 57.1 50.8% P value NS NS 19.1% 27.5% NS 54.3% 59.5% NS 51.6% 54.9% NS 66.3% 59.9% NS 29.8% 43.3% 73.6% 30.6% 49.8% 41.1% NS 0.004 <0.0001 Conclusions: Men and women with a recent ACS submitted to our CRP have a similar risk profile in general terms, but show a different response to lifestyle modification interventions. CRP should reinforce smoking cessation, diet and physical exercise interventions in women, to promote adherence to recommendations in these minority group of patients. Downloaded from http://eurheartj.oxfordjournals.org/ by guest on March 4, 2016 Predictor