Understanding & Managing Drug Shortages.
advertisement

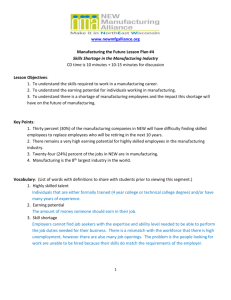
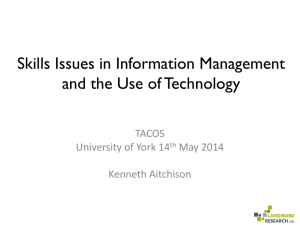
Understanding & Managing Drug Shortages Proceedings of a breakfast symposium held during the 37th ASHP Midyear Clinical Meeting on Monday, December 9, 2002 in Atlanta, Georgia Supported by an educational grant from 1 Understanding & Managing Drug Shortages Presented by Linda S. Tyler, Pharm.D., FASHP Pharmacy Manager, Drug Information Services University of Utah Hospitals and Clinics Salt Lake City, Utah and Scott M. Mark, Pharm.D., M.S. Director of Pharmacy Children’s National Medical Center Washington, D.C. Learning Objectives After studying this article, the reader should be able to: 1. Identify the current and emerging trends in drug shortages. 2. List 3 resources for obtaining up-to-date information on drug shortages. 3. Describe the components of a successful communication strategy within a health system for managing drug shortages. 4. Define the role of the pharmacist in managing drug shortages. The American Society of Health-System Pharmacists is approved by the Accreditation Council for Pharmacy Education as a provider of continuing pharmaceutical education. The program provides 1.5 hours (0.15 CEUs) of continuing education credit (program number 204-00003-417-H04). Official certificates of continuing education will be mailed to attendees within six weeks. This program is provided free of charge. Pharmacists may complete the CE test at the CE Testing Center on the ASHP web site (www.ashp.org). The release date for the program is 11/15/03 and expiration date is 11/15/05. Test code 03417. Disclosure Statements ASHP Advantage requires that faculty members disclose any relationships (e.g., shareholder, recipient of research grant, consultant or member of an advisory committee) that the faculty may have with commercial companies whose products or services may be mentioned in their presentations. The existence of these relationships is provided for the information of attendees and should not be assumed to have an adverse impact on faculty presentations. The faculty reports the following relationships: Linda S. Tyler, Pharm.D., FASHP: Dr. Tyler has no affiliations to disclose. Scott M. Mark, Pharm.D., M.S.: Dr. Mark has no affiliations to disclose. 1. Minor editorial revisions made by Abbott Laboratories. 6-052A Drug Shortages Linda S. Tyler, Pharm.D., FASHP Pharmacy Manager, Drug Information Services University of Utah Hospitals and Clinics Salt Lake City, Utah Introduction Drug shortages are a challenge for the health-care community, particularly since they typically appear with little or no warning and significant resources may be needed to manage patients when a particular therapy is in short supply. Health care professionals define a drug shortage as a change in the drug supply that has the potential to compromise patient care. Changes in drug supply can alter the way medications are prepared in the pharmacy, the way they are administered to patients, and, in some cases, whether patients receive medications at all. When faced with a drug shortage, the ultimate goal is to avoid the situation in which the patient is told that the drug of choice is not available due to a shortage. In this article, Linda S. Tyler, Pharm. D., FASHP will identify current and emerging trends in drug shortages, describe common reasons why shortages occur, and compare available resources for obtaining information on drug shortages. Drug Shortages: A Problem on the Rise Dr. Tyler can vividly remember the first drug shortage she encountered. The pharmacy was down to a one-week supply of vincristine, even though the department had tried to get the drug for six weeks. It got to the point that the department finally had to ask the physicians on staff, a tough question. “Do we ration what [vincristine] we have, or do we use it until it’s gone?” The problem was eventually solved, but Tyler learned a couple of important lessons from the experience. First, prescribers are more constructive and cooperative if they are involved in the process, and second, information regarding the shortage needs to be disseminated to those who will be impacted by it as soon as possible. 6-052A Dr. Tyler has become accustomed to managing drug shortages because there has been a sharp rise in them over the past few years. Dr. Tyler shared data collected at The University of Utah Drug Information Center (UUDIC), and compared it with national data collected over the last five years.1 When data collection began in 1996, there were less than 5 drug shortages a year both nationally and at UUDIC. Between 1997 and 2000, that number crept up to 20 shortages per year both nationally and at UUDIC. It should come as no surprise that drug shortages are expensive. Tyler said her department devoted significant personnel and financial resources to identifying, tracking and resolving supply problems. She estimated that many organizations spend between one-half and three Understanding and Managing Drug Shortages ■ 1 full-time equivalent (FTE) personnel on the management of drug shortages. These extra FTEs spend their time investigating the reason for the shortage, finding alternative agents, working with wholesalers, finding alternative suppliers, compounding a replacement product internally, or communicating with other practitioners. Tyler said the process could be expedited by involving other practitioners (i.e., physicians, pharmacists, nurses) in the decision-making process at the earliest possible moment. She’s had success with disseminating information about specific shortages via a written memorandum to all affected parties. Not only is a memorandum an effective communication vehicle, but it also can be used as a written record of shortages that have had an impact on the institution. Dr. Tyler attributes the pharmacy department’s proactive, problem-solving skills with their success in managing shortages and preventing the shortages from having a negative effect on patient care. Why Drug Shortages Occur The process of delivering medications to patients is much more complex than most people realize, especially patients. By understanding barriers in the medication supply process, health-care practitioners can more effectively use the limited available resources to communicate with each other as well as with patients. In December of 2001, the Healthcare Distribution Management Association reported a 23% back-order situation in the supply of medications.1 For example, for a facility that orders 300-500 items a day, such as the University of Utah Hospital (UUH), this means that approximately 50-100 items will not be delivered each day. Although back-orders typically do not result in shortages, it is evident that good purchasing policies are an important part of monitoring drug shortages. Drug shortages are multi-factorial, and rarely is it possible to pinpoint an exact cause. Tyler explained how industry consolidations and supply chain issues can result in shortages. Some of the factors influencing drug supply are predictable, while others are not. Following is a list and explanation of some of the unpredictable factors that can result in shortages: 2 ■ Understanding and Managing Drug Shortages ■ Natural Disasters. Natural disasters may cause a shortage by affecting the plants involved in the sole production of a product and inflicting unexpected damage to manufacturing facilities (e.g., hurricanes in the Caribbean). ■ Raw Materials. Raw material shortages may have a profound impact on drug supply. This is especially true when multiple manufacturers are producing a drug product from which there is only one source of raw materials. Problems can also arise when the raw materials are difficult to process (e.g., the raw material must be extracted from a natural source, such as tree bark). ■ Non-compliance with Regulatory Standards. Shortages can occur when the primary or sole manufacturer of a product has its production halted by the Food and Drug Administration (FDA) for reasons such as not adhering with Good Manufacturing Practices (GMPs). ■ Voluntary Recalls. A recall may create shortages, particularly when one company manufactures the majority of a product. Complying with voluntary recalls can create ethical dilemmas as well because doing so may result in a shortage. Following is a list of predictable factors: ■ Manufacturer Rationing. Occasionally, manufacturers will temporarily or permanently reduce production of products as they shift production or re-allocate resources. ■ Restricted Distribution. Post marketing surveillance programs can yield drug information that encourages the manufacturer to limit supplies to select patient populations for which the benefits of the product outweigh the risks. ■ Manufacturer Discontinuation. A manufacturer might stop production of a drug product because of lack of financial return, poor demand, or potential safety concerns. When this happens, the FDA will perform a medical necessity evaluation. In addition, the National Organization for Rare Disorders (www.rarediseases.org) will work to find 6-052A ■ ■ ■ ■ ■ another company to manufacture the product in order to protect those patients that rely on or need the medication. Industry Consolidations. Company mergers may result in decisions to discontinue products and narrow the focus of the product line. A subsequent reduction in suppliers can make a particular marketplace vulnerable to shortages, should other factors come into play. Market shifts. Sometimes, the addition of a generic product to the market may precipitate a decrease in the manufacturing of the innovator product and create a temporary reduction in the supply of a particular medication. Military conflict may also create unexpected market shifts. For example, during the Desert Storm conflict, large quantities of albumin were diverted overseas, which significantly diminished the supply in the United States.2 Unexpected Demand. Occasionally demand for a product can far exceed the existing production capacity as can happen when new unlabeled uses, clinical practices, disease outbreaks (e.g., anthrax disaster), changes in a product form or formulation (e.g., sustained release), or other unpredictable increases in demand occur. Such shifts in demand may be further complicated when the manufacturing process for the product is time consuming or raw materials needed to produce it are limited (e.g., blood-based products). “Grey” Market Vendors. The profitability of pharmaceuticals attracts vendors who create artificial shortages by selectively purchasing excessive quantities of products and thereby depleting the available stock. These vendors then re-sell the products back to the users at inflated prices. Prime Vendors and Just-in-Time Inventories. The increased use of prime vendors may have contributed to the drug shortage situation by reducing the amount of product available in the supply chain. It is no longer easy to weather shortages by relying on stockpiled inventories because both wholesalers and health systems maintain minimum levels of stock. As a result, manufacturer 6-052A Figure 1. Drug shortages at UUH by therapeutic categories. Other 28% Antibiotics 17% Autonomic 11% CV 7% Vaccines 11% CNS 15% Hormones 11% Source: UUH Drug Information Center. supply issues are transmitted directly to the user without the benefit of an inventory buffer, thereby increasing the number of short-term shortages that may impact institutions. Reasons often given for shortages include regulatory issues (7%), product discontinuation (20%), raw materials issues (8%), manufacturing problems (28%), and supply and demand problems (10%).1 Interestingly, Tyler noted that approximately 27% of shortages are unexplained. Drug companies may sometimes be reluctant to reveal the details of a shortage because of public relation, legal, and problem-solving issues. Tyler said that even though the exact reasons for shortages may not be known, it is important to investigate the general circumstances behind a shortage as part of the assessment and planning process. For example, knowing that a change in the supply is secondary to a raw material shortage is a sign that the shortage will likely be lengthy. A breakdown of drug shortages at UUH by therapeutic category was provided (Figure 1). Tyler said that this information will vary among institutions because of differences in prescribing patterns and patient populations. However, knowing which therapeutic categories of drugs have been in short supply can provide good insight into those departments within the institution that should have a vested interest in working with the pharmacy to manage a particular shortage. Interestingly, 70-80% of the Understanding and Managing Drug Shortages ■ 3 Duration (days) Figure 2. Duration of Shortages at UUH drugs in short supply nationally have been parenteral drugs.1 Part of this may have to 140 do with the disproportionate amount of 59% 67% 120 oral drugs in the supply chain and the % resolved greater time required to produce inject100 able products. However, it also means that 80 drug shortages are more of an issue for 25% hospitals and acute care settings than they 60 are in community pharmacy practice. 29% 40 It has been difficult to assess how Unresolved long shortages last. Shortages that reach 20 the hospital and patient-care level are 0 often of prolonged duration. Figure 2 Resolved 2001 2001 2002 2002 summarizes some information on (7/02) (7/02) (10/02) (10/02) duration of shortages. Of the 120 shortSource: UUH Drug Information Center. ages identified in 2001, 59% were resolved by July 2002 and 67% by October 2002. When calling the manufacturing company, Tyler explained that setting reasonable expectations Unfortunately, institutions do not get a lot of about what you hope to learn is key. Getting to support from outside organizations in managing the source of the problem can be a challenge shortages. The Food and Drug Administration because many companies do not have a central has limited authority with respect to shortages contact point for shortages. Often, the caller is and only becomes involved if a medication is sent to the customer service group. Often the deemed medically necessary. Professional person taking the call is not aware of the shortage, organizations and associations often learn of a does not have an official statement, and cannot problem from their members, which means they provide a timeline for resolution. Tyler has found do not get involved until late in the game. Drug that asking companies specific questions yields manufacturers may send letters notifying the most useful information. For example, asking practitioners of drug shortages, but these letters the company to quantify the duration of the seldom arrive before the pharmacy is faced with shortage in days, weeks, or months can often managing a particular shortage. Because there is no advance warning system yield more useful information than asking what date the product will become available. Tyler also and formulating an effective management plan takes time, pharmacy practitioners have had to implement their own systems to proactively identify drug shortages. Successful outcomes can be achieved when the shortage is identified in advance, there is time to notify other practitioners and gather information about the shortage, and options for preventing adverse effects on patient care can be investigated. Resources for Managing Drug Shortages Three of the main resources are currently available for assistance with drug shortages: the manufacturing company, the Food and Drug Administration web site, and the American Society of Health-System Pharmacists. 4 ■ Understanding and Managing Drug Shortages Figure 3. Food and Drug Administration’s Web Site (www.fda.gov/cder/drug/shortages/default.htm) 6-052A Figure 4. American Society of Health-System Pharmacist’s Web Site (www.ashp.org/shortage) Figure 5. Example of Drug Shortage Bulletin on ASHP’s Web Site recommends following-up on a regular basis to find out if new information is available. Another source is the Food and Drug Administration’s web site (www.fda.gov/cder/ drug/shortages/default.htm). The site contains information about current and resolved drug shortages as well as information about drugs that are going to be discontinued (Figure 3). The site lists drugs that are in short supply, but does not provide any clinical information about how to deal with a particular shortage. FDA breaks shortage information into two categories: drugs and biologics. The FDA shortages web page just deals with drugs. It is important to also check the biologics section for information on biologics shortages. ASHP has devoted significant resources to the management of drug shortages and has developed several policy positions on the subject. In addition, the University of Utah Drug Information Center, Novation and ASHP partnered to create Drug Product Shortage Bulletins, which are available on the ASHP web site at www.ashp.org/shortage (Figure 4). The bulletins provide information about drug product shortages, implications for patient care, alternative therapies and management, and estimated re-supply dates, when available. A sample bulletin is shown in Figure 5. Pharmacists can also report shortages that have not already been posted on the site. Tyler encouraged practitioners to report shortages, even if they think they may be limited to a particular region of the country. Future enhancements to the site include search features, which will allow visitors to search for drugs by date of last update, trade name, or generic name. Conclusion Drug shortages are a concern to pharmacists and managing them requires significant resources. Key elements to a successful program for managing drug shortages include a good understanding of the reasons behind the shortages, a proven system for involving the entire health care organization quickly, and clear channels for communicating information and plans with all those involved, especially patients, when necessary. References 1. Fox ER, Tyler LS. Managing drug shortages: seven years’ experience at one health system. Am J Health-Syst Pharm. 2003; 60: 245–53. 2. American Society of Health-System Pharmacists. ASHP guidelines on managing drug product shortages. Am J Health-Syst Pharm. 2001; 58:1445–50. 6-052A Understanding and Managing Drug Shortages ■ 5 Understanding and Managing Challenges Posed by Drug Shortages Scott M. Mark, Pharm.D., M.S. Director of Pharmacy Children’s National Medical Center Washington, D.C. Introduction Now more than ever, drug product shortages are posing challenges to pharmacy operations. As a result, pharmacists are being called upon to establish proactive processes for preventing, identifying, assessing, and enduring shortages without compromising patient care. When a shortage occurs, pharmacists are challenged to provide equivalent drug therapy at a comparable cost. Product supply issues are particularly complex in the medical field because of the large number of monotherapies and mono-products available. Not only can drug shortages increase cost and delay patient care, but they can also prevent patients from receiving the medications on which they need and rely. Drug shortages have always been a way of life in health care, but recent increases in the frequency and duration of shortages have forced health care professionals and manufacturers to devote significant resources to resolving them. Said Dr. Mark, “Every health system needs to develop a preparation strategy and awareness campaign for managing shortage issues that goes beyond the pharmacy.” Drug shortages have been receiving more attention lately because they are having a bigger impact on patient care. In the past, when an institution ran out of a medication, it could borrow it from another hospital or work through alternate vendors. Rarely was an institution unable to provide the medication at all. However, today it is becoming more common for practitioners to come up empty, leaving them in the uncomfortable position of having to inform other health care professionals and patients that a particular drug therapy is not available. In this article, Dr. Mark lists factors that can affect the supply and distribution of drugs, explain how stockpiling can contribute to the prolongation of a shortage, and explain how careful assessment and communications can assist in the successful management of a shortage. 6-052A Understanding and Managing Drug Shortages ■ 7 Effects of Manufacturing Companies on Shortages While the increased frequency and longer duration of shortages are burdensome to the health-care community, the problems are often magnified by the absence of advanced warning from the pharmaceutical industry. The industry is not currently required to communicate the availability of products. According to the Food and Drug Administration (FDA), a manufacturer is only required to provide advance notice of plans to discontinue a medication if the manufacturer is the sole producer of a medication (i.e., it manufactures 100% of the product on the market). Mark voiced his position from a practitioner’s perspective, and said that despite not being required to notify health care practitioners and patients of impending shortages, he thinks that companies ought to communicate such information. In fact, this issue is being addressed through discussion among practitioners, manufacturers, and the FDA. Mark is most frustrated by shortages driven by a manufacturer’s bottom line. For example, a company may decide to discontinue one product in favor of another that has a better margin. Manufacturers are typically most familiar with market share and alternate therapies for a particular product, and it would be helpful if the healthcare community received advance notice of corporate decisions affecting the drug supply. Not only is it important to notify health-care practitioners, but it is also essential that manufacturers inform their competitors as well. By giving advance warning, a competitor would have sufficient time to increase production in order to meet potential increases in product demand. With the public so focused on health care, particularly its rising costs, Mark thinks it would behoove the industry to keep the best interest of patients at the forefront. Mark conceded that it would be impossible for pharmaceutical manufacturers to provide advance notice of every single shortage, because of the nature of certain shortages (e.g., lack of raw materials). Given the proper information and warnings, health care providers are reasonable 8 ■ Understanding and Managing Drug Shortages and will work with manufactures whose production is limited because of a shortage of raw material or natural disasters. However, Mark’s opinion is that many of the shortages occurring during the last 10 years were within the manufacturer’s control. As a result, manufacturers have faced animosity from practitioners and patients, and the press and legislators have a heightened level of interest on shortages. As partners in health care, manufacturers have equal responsibility to patients for ensuring continuity of care as do health care professionals. Organizations such as the Health Industry Group Purchasing Association, The Pharmaceutical Research and Manufacturers of America (PhRMA), and Congress have begun to focus on the responsibilities to patient care. The prevailing perception in Congress is that the pharmaceutical industry is profit driven, and this is an area that the industry appears to be doing whatever possible to sway Congress and the public against viewing it as primarily a profit-driven business. Stockpiling Stockpiling is one of the inherent problems that occurs when a drug is in short supply. Stockpiling is the practice of purchasing more product than would typically be required to fulfill an institution’s anticipated monthly needs. Stockpiling can actually prolong a drug shortage because it creates an artificial shortfall by depleting the available product in the supply chain. Mark recommended that institutions purchase sufficient amounts of products to meet their needs. However, he recognized that the fear of paying non-contract prices for medications as well as pressure from administrators and clinicians within the institution may often motivate people to buy more product than they need. Distribution One lesson learned from recent shortages is that larger institutions have an advantage over smaller institutions with respect to product availability. The advantage is not only in terms of learning about shortages sooner, but also in terms of product distribution. 6-052A Often, large institutions are the last to feel the impact of a shortage, but the first to receive shipments when supplies become more plentiful. A similar trend has been observed across larger geographic regions. Mark said that drug shortages rarely affect the health-care industry in a uniform fashion, and recommended networking as one solution to addressing imbalances in drug supplies. Food and Drug Administration’s Web Site. The FDA’s web site (www.fda.gov/drug/shortages/ default.htm) allows the user to sign up for a push news service. By signing up for the service, users receive information about drug shortages via email, can get contact information for manufacturers, as well as get copies of letters sent to physicians regarding shortages. Profiteers and the Grey Market Centers for Disease Control and Prevention Web Site. The CDC’s web site (www.cdc.gov) is a good source of information regarding vaccine shortages and recommendations for modifying immunization schedules. When a shortage of a vaccine occurs, health-care practitioners need to contact patient families and inform them of any changes that may need to be made in the immunization schedule. Being proactive goes a long way to restoring patients’ confidence. Dr. Mark recalled a situation that occurred at the Children’s National Medical Center, which illustrated the importance of good information and networking. Two years ago the Children’s National Medical Center experienced a shortage of influenza vaccine. Explaining the shortage to the parents of the children was difficult, but the situation was made worse because a local pharmacy chain was hosting free vaccination clinics. In addition many of the larger institutions in the area were vaccinating their employees. When fentanyl was in short supply, the staff at Children’s National Medical Center researched the shortage and networked and found sources of the drug well before it became available through their wholesaler. The grey market is another problem resulting from drug shortages that frustrates wholesalers, practitioners, manufactures, and patients. When a drug is in short supply, health care institutions will frequently receive offers to purchase it from secondary suppliers at inflated prices. Congress is investigating how these suppliers learn about shortages before most providers to determine if they might be purposely contributing to and/or prolonging shortages to increase their profits. Resources for Managing Shortages Mark explained how pharmacists can prepare for shortages and highlighted several resources they can tap for help. These are described below: Information and Networking. Getting good information and maintaining a strong network are two of the best ways to minimize the impact of a drug shortage. Product buyers should investigate existing and potential shortages on a daily basis, they should routinely review information on listservs, network with other buyers, and maintain contact with wholesalers. When pharmacists find out about a shortage, they should be sure to get information about the reason for it. American Society of Health-System Pharmacists. The American Society of Health-System Pharmacists (ASHP) is a good source of information. Their web site (www.ashp.org/shortage) includes information about drug product availability, information about alternative agents and the respective references, links to other resources, and a mechanism for reporting an emerging drug shortage. ASHP has developed Guidelines for Managing Product Shortages, and these are also included on the site. 6-052A Tips for Managing a Drug Shortage Dr. Mark gave an overview of things health-care practitioners to prepare for and manage drug shortages. Descriptions of these recommendations follow: Develop Policies and Teams. Policies within a hospital that identify which governing body can mandate practice changes across medical disciplines need to be developed. It is also important to determine how communication and medical education will be managed. Mark recommended that such policies be medical Understanding and Managing Drug Shortages ■ 9 policies rather than pharmacy department policies in order to get the support of the institution and deflect attention from the pharmacy. Forming ad hoc committees can aid in assessing the potential impact of a shortage, approving alternatives, prioritizing patients, and rallying support within the institution. Such committees can be stand-alone committees or subcommittees of the pharmacy and therapeutics committee. Mark recommended giving anesthesia, pediatrics, and emergency medicine departments prominent representation on these committees because of the disproportional effect drug shortages tend to have on these disciplines. individual should be available and prepared to provide accurate, timely, and consistent information to practitioners who have questions. The drug shortage coordinator should be charged with managing all information and products related to shortages and communicating to staff information related to supply, policy, alternative products, and decisions made by the institution. Mark said that during an intravenous immunoglobulin (IVIG) shortage physicians worked closely with the drug shortage coordinator to verify product availability, ensuring that the appropriate amount of product was set aside so that patients could receive their course of therapy. Educate the Staff. When a drug shortage results in the use of an alternative product, health care professionals and patients need to be educated about any differences between the unavailable product and the alternative product. If not properly educated, patient care can be compromised because of medication errors. Examples of the types of errors that can be made include prescribing errors, dispensing and/or selection errors (particularly with automated machines), compliance errors (e.g., patients have to change the way they take medications), and preparation errors (e.g., pharmacy personnel must adapt to new preparation procedures). Mark, who is affiliated with a pediatric hospital, said practitioners at his institution are particularly sensitive to the potential for errors, because so many of the drugs they use are dosed according to patient weight. Mark said his facility relies heavily on education when a new product is introduced. The pharmacy department also minimizes to the extent possible variation in vial sizes and concentrations, and avoids purchasing products that look alike. Developing Long- and ShortTerm Strategies Communicate. Communication is the key to surviving any medication shortage. Mark said that the top priority during a shortage is to establish and maximize communication channels. Staff must get up-to-the minute information about the problem, proposed solutions, and progress. Mark recommended designating someone in the department (e.g., a drug shortage coordinator) as the primary contact. This 10 ■ Understanding and Managing Drug Shortages Both long- and short-term strategies need to be developed to deal with shortages effectively. Short-term Strategies. Finding out how long a shortage may last needs to be determined early in the process. Mark said to start with the manufacturers, even if you may not get a definitive answer. As was discussed in the previous article, finding out the cause of the shortage can often provide clues about its duration. Wholesalers should also be contacted to determine if the supply chain is sufficient to withstand the shortage. Mark said that, in some cases, through the course of investigating a shortage he will determine that no such shortage exists. Mark said some wholesalers will report that the “manufacturer is unable to supply” a product, but the problem may be the result of a temporary outage at the wholesaler, a contract dispute, or outstanding invoices. Mark recommended including language in wholesaler contracts that impose penalties for drug outages. He also advised pharmacists to contact the manufacturer directly to confirm the outage and to compare wholesaler “stock-outs” with other institutions. After a shortage has been confirmed, a comprehensive evaluation of how the drug shortages will affect patient care should be conducted (i.e., a threat analysis). A threat analysis takes into account factors such as prescribing trends, 6-052A clinical pathways, or protocols involving the medication, the location of the medication within the institution, and other data to determine which patients are likely to suffer most, which medical services are at greatest risk, and how long the existing medication supply will last. Internal medication supplies should be sequestered for more effective management, which means locating all of the medications within your health-system. If the institution employs automated dispensing cabinets, a “hospital wide summary” report can be used to locate the drugs. Code carts should be searched and pharmacists should be on the lookout for medications with short expiration dates that may have been pulled prematurely. Mark suggested working with the institution’s Information Technology department to streamline data and create customized reports. Long-term Strategies. If the short-term assessment determines that a drug shortage exists, the next step is to formulate a long-term strategy aimed at protecting the interests of patients. All the options should be evaluated, including alternative therapies, contract compounding, priority-driven dispensing, and rationing. These strategies should be re-evaluated regularly because circumstances will likely change during the shortage. Determining which alternative therapies to use during a shortage can be difficult, especially if the alternative is not equally effective for all of the indications for which the drug in short supply would have been used. Mark recommended contacting regional and local drug information centers for assistance in assembling a list of alternatives and the supporting literature. The University of Utah provides alternative therapy guides for the Drug Shortage Bulletins posted on ASHP’s web site, but this information might be available more quickly through a local or regional drug information center. Mark said other good sources of information include the manufacturer, in-house clinical staff, and the ad hoc committees. Pathway committees and regional protocol groups can also be a good source of information if it becomes necessary to modify the institution’s pathways and protocols. 6-052A Some pharmacies use contract-compounding firms to provide substitutions for medications that are in short supply. In addition, Mark said there have been reports that groups within some health systems have ordered compounded formulations without knowledge or oversight of the pharmacy department. Staff need to be reminded periodically on the institution’s policies regarding how drugs are ordered and received. Although out-sourcing compounding has been a viable option for some pharmacies, Mark emphasized the substantial risks assumed by pharmacies that use these services. Formulations for compounding are typically not reviewed by the FDA, which means FDA has no control over the quality and consistency of the preparation process used. The potential dangers were illustrated last when three patients in California died last year from bacterial meningitis that they contracted from contaminated betamethasone that had been purchased from a compounding pharmacy.1 Mark said that any facility that uses contract compounding services should consult with its Investigational Review Board (IRB) who can provide assistance in informed consent with respect to educating patients about associated risks. Both, ASHP and the Joint Commission on Accreditation of Health Care Organizations (JCAHO) have guidelines and requirements on the matter. According to ASHP’s Guidelines on Outsourcing Pharmaceutical Services, “an organization’s pharmacy director must take complete responsibility for patient outcomes for all medication-related activities performed at or for the organization.”2 Pharmacy directors are also responsible for any preparations obtained from outside pharmacies and have the right to monitor the quality of medications used in a hospital. This responsibility, according to ASHP, should be explicitly stated in all outsourcing contracts. The JCAHO requirement is more specific. According to JCAHO’s Standard L.D.3.50,3 services provided by consultation, contractual arrangements, or other agreements must be provided safely and effectively. The elements of performance also state that leaders approve sources for the organization’s services that are Understanding and Managing Drug Shortages ■ 11 provided by consultation, contractual arrangements or other agreements.3 The organization also retains overall responsibility and authority for services furnished under a contract.3 Mark’s advice was that it is much better to use an alternative therapy than a potentially bad-quality product. During a severe shortage it is sometimes necessary to prioritize patients to ensure that the available medication is dispensed appropriately. Patient prioritization is one of the most challenging parts of managing a drug shortage. Patients can be prioritized based on diseases for which an alternative therapy is available, the acuity of their condition, or whether the patients have already received therapy with the drug in short supply. Mark said it is critical to involve the public relations and legal departments in the prioritization process. It is important to keep in mind that no matter how the prioritization is performed, the potential for patients to disagree with methods and take legal action exists. Knowing when to release supplies is also difficult and should be decided by the P&T committee. Mark’s institution experienced this problem when the supply of phenobarbital was unpredictable. To ensure that supply would always be available for patients with status epilepticus, the institution decided to maintain two separate stocks. Although this created some animosity with the medical staff, having a central coordinator, previously established policies, and support of the P&T committee kept the hard feelings to a minimum. Some manufacturers have developed rationing programs for products they know will be in a short supply. It is worth contacting manufacturers to learn about the programs that might be available. Conclusion Communication is a key component to any strategy for managing drug shortages. Practitioners can effectively deal with shortages by establishing a proactive system, developing institution-wide policies, opening channels for quick and clear communication, minimizing liability, and remembering the end goal of protecting patients. References 1. California Department of Consumer Affairs. Pharmacy operation restricted by action from the California State Board of Pharmacy. http://www.dca.ca.gov/press_releases/20010717a. htm. Accessed 2003 Aug 14. 2. American Society of Health-System Pharmacists. ASHP Guidelines on outsourcing pharmaceutical services. Am J Health-Syst Pharm. 1998; 55:1611–7. 3. Anon. Accreditation Standards for Hospitals (Prepublication version). Joint Commission on Accreditation of Healthcare Organizations, 2003 (www.jcaho.org). 12 ■ Understanding and Managing Drug Shortages 6-052A Continuing-Education Test Identify the current and emerging trends in drug shortages. 1. Which of the following statements is TRUE? a. The primary reason the incidence drug shortages has increased drastically since 1996 is the merging of manufacturing companies. b. Drug shortages have a bigger impact on community pharmacy practice than hospital and acute care practice. c. The reason for approximately 27% of drug shortages is unknown. d. Greater than 60% of drug shortages are due to reduced supply of raw material. 2. Which of the following is NOT considered a valid reason for drug shortages? a. Increased demand due to stockpiling. b. Stricter guidelines imposed on manufacturers by the FDA in 1999. c. Regulatory violations by manufacturers. d. Imbalances in product distribution. 3. According to Dr. Tyler’s presentation, drug shortages have the biggest impact on drug supply in which of the following therapeutic areas? a. b. c. d. Central Nervous System Hormone Therapies Antibiotics Vaccines List 3 resources for obtaining up-to-date information on drug shortages. 4. Of the three drug shortage resources reviewed in the program, which is considered the best source to find the appropriate contact at a manufacturer? a. Food and Drug Administration’s Web Site b. American Society of Health-System Pharmacy’s Web site c. Centers for Disease Control and Prevention’s Web site d. Wholesaler 5. The best source for clinical guidelines for dealing with a drug shortage is: a. Food and Drug Administration’s Web Site b. American Society of Health-System Pharmacy’s Web site c. Manufacturer d. Wholesaler 6. Which of the following resources includes a mechanism for reporting drug shortages: a. Food and Drug Administration’s Web Site b. American Society of Health-System Pharmacy’s Web site c. Manufacturer d. Wholesaler 7. Which of the following statements is FALSE a. The letters practitioners receive from drug manufacturers are a timely source of information about drug shortages. b. The Centers for Disease Control and Prevention’s web site is the best source of information regarding vaccine shortages. c. ASHP’s web site includes clinical guidelines for dealing with drug shortages. d. The FDA’s web site offers a push-news service regarding drug shortages. Describe the components of a successful communication strategy within a health system for managing drug shortages. 8. According to Dr. Mark’s presentation, which of the following is the most important part of a drug shortage management program? a. Educating patients about drug shortages. b. Implementing a pharmacy department policy for managing drug shortages. c. Communication practices. d. Forming ad hoc committees that consist of anesthesia, pediatrics, and neurology disciplines. 9. Which of the following is NOT considered a part of an effective communication plan? a. Remind departments within the institution about appropriate practices for ordering and receiving products. b. Provide educational materials to alert practitioners to differences between the alternative therapies and the drug in short supply. c. Establishing a pharmacy-based committee to manage drug shortages. d. Use a written memo to communicate facts with practitioners. 10. Which of the following statements about external compounding companies is FALSE? a. Formulations are not reviewed by the FDA. b. The FDA requires that products provided by external compounding companies are done so with the approval of the Pharmacy and Therapeutics Committee. c. JCAHO requires that the institution demonstrate efficacy, toxicity, bioequivalence, and pharmaceutical equivalence of compounds. d. According to JCAHO and ASHP, the pharmacy director is personally responsible for the quality of contract services. 11. Components of a long-term strategy for dealing with drug shortages include all the following EXCEPT: a. Identify and evaluate alternative drug regimens for the agent in short supply. b. Identify and centralize the supply of the drug in short supply. c. Confirm and evaluate the duration of a drug shortage. d. Distribute educational materials to teach staff about the differences between the alternative drugs and the drug in short supply. Describe the role of pharmacists in managing drug shortages 12. Which of the following is NOT considered an acceptable means for managing drug shortages? a. Implement systems to proactively identify drug shortages. b. Stockpile medications to prevent a shortage. c. Ration medications based on a prioritization plan developed by a multidisciplinary team. d. Purchase the product from an external compounding facility. 13. All of these methods for prioritizing patients to determine who receives drugs in short supply are recommended EXCEPT: a. By disease state for which alternative therapies are available. b. Using a lottery system. c. Based on the acuity of each patient’s condition. d. Whether a patient has already received therapy or not. 14. The goals of a “threat analysis” include all of the following EXCEPT: a. Identify patients at the biggest risk. b. Identify medical services at the biggest risk. c. Determine how long the existing medication supply will last. d. Identify secondary suppliers as sources of medication. 15. All of the following statements describe a good approach to dealing with wholesalers, EXCEPT: a. Contact the wholesaler weekly to inquire about drug shortages. b. Ensure that the wholesaler contract includes language that imposes penalties for drug outages. c. Contact the manufacturer directly to confirm outages. d. Benchmark the number of stock-outs at your institution against other institutions. 6-052A ASHP Advantage 7272 Wisconsin Avenue Bethesda, Maryland 20814 6-052A-5-Jun., 03