Pneumonia Admission Orders (All Forms)
advertisement
")
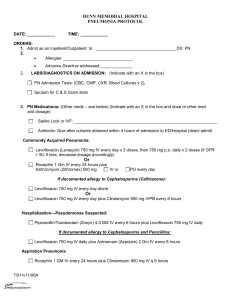
Name:______________________________ DOB:______________________________ Generic equivalents are utilized unless checked. l CORE MEASURE REQUIREMENTS Physician Name(s) Status Admit to Dr.______________________________ Inpatient Observation Code Status Code Status:________________________________________________________ Location _________________________________________________________________ ICU Telemetry Medical Other Old chart to floor with patient. Diagnosis Community Acquired Pneumonia ( CAP ) Healthcare Associated Pneumonia ( HAP ) Condition Good Serious Fair Critical Nursing Interventions Vital Signs Per unit Protocol Other:_______________________ Activity Bed Rest with bedside commode with bathroom privileges Out of bed with assistance Ambulation Fall Prevention Monitor Pulse oximetry per unit routine and record Interventions Strict Recording of Intake and Output record Daily weights (chart results) Aspiration Precautions Transcribed Noted / Acknowledged Signature Telephone Order(TOR) Date / Time Signature PHYSICIAN INITIALS Date / Time DATE / TIME Originated 2010 rev Pneumonia Admission Orders Pg 1 of 4 public Revised 5/12/11 Name:______________________________ DOB:______________________________ Generic equivalents are utilized unless checked. l CORE MEASURE REQUIREMENTS Respiratory Therapy Respiratory Therapy per protocol Oxygen ______________ Liters Atrovent 0.5 mg nebulizer every ______ hours Albuterol 2.5mg nebulizer every ______ hours Atrovent 0.5 mg nebulizer every ______ hours PRN Shortness of Breath / Wheezing Albuterol 2.5mg nebulizer every ______ hours PRN Shortness of Breath / Wheezing Diet Regular Nothing by mouth except for medications Cardiac Diet American Diabetes Association_________kCal IV Fluids Saline lock with 3 mL Normal Saline flush every 12 hours IVF:________________________ with __________ milliequivalents Potassium Chloride (KCL) / liter at ___________mL / hour times __________ hours Any other IV fluids:______________________________________________ Medications Protocols l Smoking Cessation Education Materials Scheduled CAP Non - ICU Antibiotics PCN allergy: (may choose one) l Rocephin ( cefTRIAXone ) 1 gram IV piggyback every 24 hours PLUS Zithromax (azithromycin) 500 mg PO every 24 hours l Rocephin ( cefTRIAXone ) 1 gram IV piggyback every 24 hours PLUS Doxycycline 100mg PO every 12 hours l Levaquin ( levofloxacin ) 750 mg IV piggyback every 24 hours ( may change to PO when tolerating diet ) CAP ICU Admission (may choose one) l Rocephin (cefTRIAXone) 1 gram IV piggyback every 24 hours PLUS Zithromax (azithromycin) 500 mg IV piggyback every 24 hours l Rocephin (cefTRIAXone) 1 gram IV piggyback every 24 hours PLUS Levaquin (levofloxacin) 750 mg IV piggyback every 24 hours Send blood cultures times 2 if not collected in ER Transcribed Noted / Acknowledged Signature Telephone Order(TOR) Date / Time Signature PHYSICIAN INITIALS Date / Time DATE / TIME Originated 2010 rev Pneumonia Admission Orders Pg 2 of 4 public Revised 5/12/11 Name:______________________________ Generic equivalents are utilized unless checked. l CORE MEASURE REQUIREMENTS Aspiration Pneumonia DOB:______________________________ (may choose one) Zosyn ( Piperacillin and Tazobactam ) 3.375 grams IV piggyback every 6 hours Cleocin ( Clindamycin ) 600mg IV every 6 hours PCN allergy: Healthcare Associated Pneumonia (may choose one) Zosyn ( Piperacillin and Tazobactam ) 4.5 grams IV piggyback every 6 hours PLUS Levaquin ( Levofloxacin ) 750 mg IV piggyback every 24 hours ( Pharmacy to adjust renal dosing ) Doripenem ( Doribax ) 500mg IV piggyback every 8 hours PLUS Levaquin (levofloxacin) 750mg IV piggyback every 24 hours ( Pharmacy to adjust renal dosing ) PCN allergy: MRSA Suspected Vancomycin ( Vancocin ) 15mg / kg IV every 12 hours ( Pharmacy to adjust ) VTE Prophylaxis Lovenox (enoxaparin) 40 mg Subcutaneous every day OR if Creatinine Clearance less than 30 mL / min Lovenox (enoxaparin) 30 mg Subcutaneous every day Anti-embolism Hose (TED) to bilateral lower extremeties Sequential compression devices to bilateral lower extremeties Anti-Inflammatory (may choose one) Solu-MEDROL (methyIPREDNISolone) _______ mg IV every _________ hours PredniSONE _________ mg PO every ______ hours Expectorant GuaiFENesin 600 mg ______tab(s) PO every 12 hours Ulcer Prophylaxis ( may choose one ) Pepcid ( famotidine ) 20 mg PO every 12 hours Protonix ( pantaprazole ) 40 mg PO every 24 hours Pepcid ( famotidine ) 20 mg IV push every 12 hours Protonix ( pantaprazole ) 40 mg IV push every 24 hours Vaccines l l Other Medicines Pneumococcal Vaccine 0.5 mL IM 1 time only ( age 65 and over or high risk: *assess year-round* ) Influenza Vaccine 0.5 mL IM 1 time only ( age 50 and over or high risk: *assess from October through end of March flu season* ) Other: ________________________________________________________ ________________________________________________________ Transcribed Noted / Acknowledged Signature Telephone Order(TOR) Date / Time Signature PHYSICIAN INITIALS Date / Time DATE / TIME Originated 2010 rev Pneumonia Admission Orders Pg 3 of 4 public Revised 5/12/11 Name:______________________________ DOB:______________________________ Generic equivalents are utilized unless checked. l CORE MEASURE REQUIREMENTS PRN Adult Insulin Sliding Scale Protocol Low High Pain Severe ( 7 - 10 ) Morphine Sulphate 2 mg IV push every 2 hours PRN severe pain Moderate ( 4 - 6 ) HYDROcodone / APAP 5 / 325 mg 2 tabs PO every 6 hours PRN moderate pain Mild ( 1 - 3 ) HYDROcodone / APAP 5 / 325 mg 1 tab PO every 4 hours PRN mild pain PRN Temperature Constipation Tylenol (Acetaminophen) 650 mg PO every 4 hours PRN temperature over 101.3 degrees Fahrenheit Colace (Ducosate Sodium) 100 mg PO two times per day PRN constipation Milk of Magnesia (magnesium hydroxide) 30 mL PO daily PRN constipation Nausea Zofran (ondansetron) 4 mg IV every 3 hours PRN Nausea / Vomiting Diagnostics Lab In AM Basic Metabolic Panel Magnesium Complete Blood Count with differential Comprehensive Metabolic Panel Radiology Chest X-ray _________________________________________ Other _______________________________________________________________ Consults Other: Speech Therapy Notify Physician Temperature greater than ____________ Heart Rate greater than ___________ or less than _________ Oxygen Saturation less than ____________________________% Systolic Blood Pressure less than _______________________ Diastolic Blood Pressure greater than _____________________ Change of patient condition Transcribed Noted / Acknowledged Signature Telephone Order(TOR) Date / Time Signature PHYSICIAN SIGNATURE Date / Time DATE / TIME Originated 2010 rev Pneumonia Admission Orders Pg 4 of 4 public Revised 5/12/11