Handout
advertisement

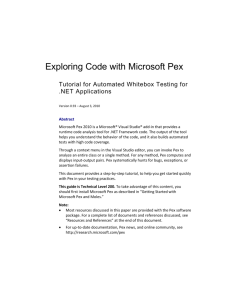
The Physical Examination: We appreciate the art… What is the evidence? Ricardo José Gonzalez-Rothi MD Department of Clinical Sciences The Art: Reasons for examining the patient… Reason # 1: “ To impress the patient.” Reason # 2 “To impress, not the patient, but anyone watching you…” The Ritual… “Examining the patient…has the ingredients of a ritual: performed in a special space; involves one person baring soul…body.. allowing another the privilege of touch… the person examining wearing a special uniform… performs a systematic examination… steps are mysterious to the patient… using instruments that are the tokens and talismans of the profession.” Dr. A Verghese What I wish to share today: • Provide a historical trajectory of the Physical Examination (PEX) • Discuss how PEX as a “diagnostic test” can be subjected to rigorous evidence base regarding reliability and accuracy • Discuss PEX findings in light of their diagnostic accuracy in ascertaining/excluding certain conditions Physical Examination: a historical trajectory • 35001500 BC • 460 BC • 200 AD Egyptians describe pulse and heart palpation “Hippocratic” physicians describe inspection, direct auscultation of organs, palpation, examine bodily secretions “Galenic” period: pulse, nerves and muscles, followed by stagnation through Medieval and Post-Renaissance periods Hales, Auenbrugger, Laennec, Stokes, Adams, Pasteur, McKenzie, Traube et al… • 1700-1800’s • 1980’s,90’s “i-Patients” A radical proposition… Physical Exam findings should be looked on as individual “diagnostic tests”. We subject serum potassium measurements to scientific exactitude, demanding accuracy and reliability in measurement and interpretation. Should we not do the same with the PEX? Empiric generalizations about Physical findings • A PEX* finding characteristic of a suspected diagnosis when present, makes the diagnosis more likely. • Absence of the characteristic finding makes the suspected diagnosis less likely. • Positive/Negative PEX findings shift the probability of detecting disease (diagnostic accuracy). * If objectively validated against “gold standard” “Time-honored” PEX findings may be of poor/no diagnostic value… • Nailbed pallor for anemia • Barrel Chest for airway obstruction • Diaphragmatic excursion “A good clinician must know the limitations of the physical examination…” D. Harry, in Magnum Force What Determines how good the PEX is? Is it based on sound anatomic/physiologic principle(s)? Does it measure what it claims to measure? Orthostatic Blood Pressure and Pulse in Hypovolemia Jugular Vein Distention in Volume overload states and/or diminished cardiac Ventricular function PEX: Orthostatic BP and Pulse in detecting hypovolemia from acute blood loss* Procedure: 1) measure BP, Pulse after 2 min. supine 2) measure (1 min? 2 min? after standing) 3) record endpoint(s) (BP, Pulse) Results: a) A drop in SBP> 20mm Hg has NO proven value b) A postural increase in 30 bpm correlates with “large volume loss” (630-1150 ml blood phlebotomy) * Baraff and Schriger, Am J. Emerg Med 1992 Vol 10 p 99, Witting et al Ann Emerg. Med 1994 Vol 23 p 1320 CALibratedFingerRubAuditoryScreeningTest D. Torres-Rusotto et al. Neurology 2009 Vol 72 p 1595 442 ears tested Sound intensity of Finger Rub and subjects Assessed by audiometry ~70 cm ~35cm Sensitivity, specificity, LR’s and interobserver reliability assessed Factors influencing Diagnostic Accuracy of a test • Reliability • Pre-test probability • Sensitivity • Specificity What Determines how good the PEX is? Reliability: extent of agreement among multiple clinicians examining the same patients of the absence/presence of PEX findings in those patients(inter-observer agreement).* * Not that simple… Concurrence by chance alone… Dr. “A” and Dr “B” examine 100 patients with dyspnea. “Gonzo maneuver” is present in 10, and absent in 70. (present in 10+ absent in 70=80) or 80% “Simple Agreement” But: Simple Agreement can be influenced CHANCE ALONE Especially when Drs A and B both agree on the finding as very “Uncommon” (near to 0%) or very “Common”(near 100%). There is a STATISTIC that accounts for CHANCE ALONE in assessing reliability (К) kappa Statistic К Statistic and interobserver agreement (Range 0-1) К Value Degree of Agreement 0 CHANCE ALONE 0-0.2 Slight 0.2-0.4 Fair 0.4-0.6 Moderate 0.6-0.8 Substantial 0.8-1.0 Near Perfect Lack of agreement: PEX • Physical sign ambiguous and/or vague (“normal” vs “diminished”) • Flawed technique • Biologic variation (intermittent friction rubs, etc) • Examiner carelessness • Clinician Bias (loud P2) Interobserver agreement (К) PEX Finding Tachycardia (>100/bpm) Normal bowel sounds Peripheral pulse (absent/present) (normal/diminished) CALFRAST Abdominal rigidity Liver span >9cm (percussion) Increased tactile fremitus Diaphragmatic excursion (percussion) К Value 0.85 0.36 0.52-0.92 0.01-0.15 0.83 0.14 0.11 0.01 -0.04!!! Interobserver agreement (К) Technology Chest X ray (Cardiomegaly) (Interstitial edema) Cardiac Cath (extent CAD stenosis) К Value 0.48 0.83 0.33 MRI (lumbar root compression) 0.83 Pathology, Liver biopsy (ETOH cirrhosis) (Cholestasis) 0.49 0.40 Factors influencing Diagnostic Accuracy of a test • Reliability • Pre-test probability • Sensitivity • Specificity Pre-test Probability (PTP): Diagnostic Accuracy • Refers to the probability of the disease (prevalence) before a diagnostic test (PEX) is applied • Generally PTP is used as first step in clinical decision-making Pre-Test Probability Clinical Situation Diagnosis Pre-Test Probability Cough, fever Pneumonia 12-30%* Acute Abdominal pain Cholecystitis 5% Dysuria, inc. frequency Urinary tract Infection 50% Clinician’s Gestalt? Chunilal et el JAMA 2003 Vol 290 p 2849 Pre-Test Probabilities for Pulmonary Embolism Clinician Gestalt Clinical Prediction Rule Low 8-19% 3-28% Moderate 26-47% 16-46% High 46-91% 38-98% The Pre-Test Probability is a start of the diagnostic processs…but it is not good enough. Factors influencing Diagnostic Accuracy of a test • Reliability • Pre-test probability • Sensitivity • Specificity Sensitivity refers to the proportion of patients with a diagnosis who have the particular PEX finding Specificity is the proportion of patients without the diagnosis who don’t have the particular PEX finding Sensitivity and Specificity describe the discriminatory strength of PEX findings. BIOSTATSPEAK “ A test is valid if it detects most people with the target disorder (high sensitivity) and excludes most people without the disorder (high specificity) and if a positive test usually indicates that the disorder is present (high positive predictive value).” Greenhalgh, BMJ 1997 Vol 315 p540 “ Lies, damned lies and statistics…” not Disraeli While sensitivity and specificity of a test are virtually constant, the positive(PPV) and negative (NPV) predictive values when calculated depend crucially on prevalence ( e.g.pre-test probability). * * Effect prevalence change on PPV with a test which is 95% Sensitive and Specific Towards a more rapid and robust measure of accuracy… The Likelihood Ratio is a statistical expression which provides the likelihood of a particular PEX finding occurring in someone with a disorder relative to the likelihood of the same finding occurring in someone without the disorder Likelihood Ratios (LR) describe discriminatory power of PEX findings • A SINGLE number, unaffected by prevalence • Simple to use, calculated from Sensitivity and Specificity values • Accurate • Can be applied to PEX findings of continuous scale (BP), or ordinate scale (e.g. 1+, 2+) • Can be used to combine PEX findings* Likelihood Ratios (LR) • Expressed as LR “+” (PEX finding present) or LR “-” (PEX finding absent) • LR’s > 1 increase probability of presence of disease* • The higher the LR the greater the compelling power that the PEX confirms a disease • LR=(0-1) decrease the probability of presence of disease* * Assuming the 95% Confidence intervals appropriate LR: rule of thumb… LR +/- change in post-test probability 2.0 + 5.0 + 10.0 + + 15% + 30% + 45% 0.5 0.2 0.1 - - 15% - 30% - 45% EXAMPLE: PRE=TEST PROB= 20%, LR=10.0 POST-TEST PROB 20+45= 65% Bayesian Thinking The probability of diagnosing a disease following the interpretation of a diagnostic test (post-test probability) is based on 2 factors: 1) The Pre-test probability (prevalence of disease) 2) How accurate (and reliable) the diagnostic test itself is* • VS “Gold Standard” Rinne Test: Hearing loss vs Audiometry=gold standard BC> AC= CONDUCTIVE LOSS Likelihood Ratio (+) = 16.8 * Likelihood Ratio (-) = 0.2 *Burkey et. al. Am J. Otol 1993 Vol 19 p 59, Chole et al. Arch Otolaryngol Head Neck Surg 1988 Vol 114 p 399 FAGAN NOMOGRAM Condition: Unilateral hearing loss Rinne Test: A: Pretest Prob=20% LR+ B: Pretest Prob=40% A LR + = 16.8 BC>AC LR - = 0.2 AC>BC B LR - Cardiac PEX: Jugular Venous Distention Exam Maneuver (vs Gold Standard) LR + LR- (CVP > 8 cm H2O) 9.0 NS (ELEVATED LVEDP) 3.9 NS (LOW EJECTION FRACTION) 7.9 NS JVD > 3cm ABDOMINOJUGULAR TEST (aka HJR) (ELEVATED LVEDP) 8.0 0.3 Chest PEX and airway obstruction PEX FINDING LIKELIHOOD RATIO Early Inspiratory coarse crackles 14.6 Absence of Cardiac Dullness LSB 11.2 Breath sound score < 9 10.2 Snider Test (blow out match) 9.6 Subxyphoid Cardiac Impulse 7.4 Hyperresonance RU Anterior chest 5.1 Reduced Diaphragmatic Excursion NS What I shared today: • Historical trajectory of the Physical Examination (PEX) • How PEX as a “diagnostic test” can be subjected to rigorous evidence base regarding reliability and accuracy • Discussed PEX findings in light of their diagnostic accuracy in ascertaining/excluding certain conditions Additional Resources “on papyrus”: • Simel DL and Rennie D. The Rational Clinical Examination JAMA evidence, McGraw Hill Medical Press, 2009. (mcgraw-hillmedical.com) • McGee S. Evidence Based Physical Diagnosis, Saunders Elsevier, second edition 2007. “on line” : • Essential Evidence Plus (available to FSUCOM Library, PDA’s) • Statistical Calculators: www.mclibrary.duke.edu/subject/ebm/ratios.html Smartphone Apps: upcoming www.medicinetoolkit.com (?)