P219 A rationale for the wider use of plasma exchange in the
advertisement

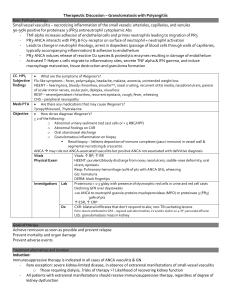
P219 A rationale for the wider use of plasma exchange in the management of ANCA vasculitis Andrew Saunders, Neeraj Dhaun, David C Kluth. Royal Infirmary of Edinburgh Introduction Systemic vasculitis associated with autoantibodies to neutrophil cytoplasmic antigens (ANCA) is the most frequent cause of rapidly progressive glomerulonephritis. Data suggest a role for plasma exchange (PEX) on top of standard immunosuppression in improving disease outcomes. We aimed to define a rationale for which patients presenting with ANCA disease may benefit from PEX. Methods Patients presenting with ANCA vasculitis between September 2006 and April 2013 were prospectively allocated to treatment with PEX (8 centrifugal exchanges) alongside standard of care if they fulfilled any of the following criteria at presentation: 1. serum creatinine >500µmol/l or dialysis-requiring renal failure, 2. alveolar haemorrhage, 3. renal disease with ≥30% focal and necrotising lesions ± cellular crescents on renal biopsy. Patients were followed up for the time period of the study with study endpoints including disease remission and relapse, cumulative immunosuppressive burden at 3 months, and all-cause mortality. Results 104 patients presented with a new diagnosis of ANCA vasculitis within the study period. Comparisons between the two groups are shown below (mean ± SD, ns, not significant). Characteristic Age Male /female ANCA status: PR3+ vs. MPO+ vs. negative Renal involvement Lung involvement At presentation Creatinine (µmol/l) CRP (mg/l) Haemoglobin (g/l) Dialysis-requiring Induction period (~3 months) Number receiving Glucocorticoids Cyclophosphamide MMF Rituximab Cumulative glucocorticoid dose (g) Cumulative cyclophosphamide dose (g) Number entering remission Time to remission (days) At 12 months Creatinine (µmol/l) Dialysis-requiring Number of patients with disease relapses (%) Number of patients died (%) No PEX (n=46) 61 ± 15 26/20 26 vs. 15 vs. 4 35 26 140 ± 90 48 ± 61 116 ± 21 1 PEX (n=58) 60 ± 17 27/31 25 vs. 30 vs. 3 57 30 370 ± 259 105 ± 82 94 ± 18 20 p value ns ns ns ns p = 0.000 p = 0.001 p = 0.000 p = 0.000 46 23 8 10 2.5 ± 0.4 8.0 ± 3.6 44 118 ± 200 120 ± 46 0 12 (26) 5 (11) 58 45 16 7 2.3 ± 0.2 5.4 ± 3.0 57 83 ± 39 191 ± 172 5 8 (14) 3 (5) ns p = 0.005 ns ns p = 0.000 p = 0.002 ns ns p = 0.02 p = 0.04 ns ns Conclusion Despite more severe disease at presentation, those patients receiving PEX had similar disease outcomes to those not receiving it. PEX treatment was associated with a lower cumulative dose of glucocorticoid and cyclophosphamide. Extent of histological injury should be considered alongside current suggested criteria for treatment of patients with ANCA vasculitis with PEX.