SBAR Clinical report on Maternity situation
advertisement

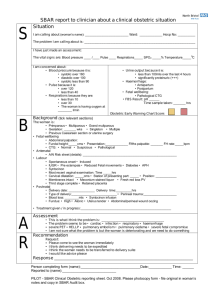
Maternal and Perinatal Morbidity and Mortality Review Committee Ministry of Health and Family SBAR Clinical report on Maternity situation SITUATION S B A R I am calling about (name of women)………………………………….Ward………………………Hosp. No The problem I am calling about is I just made an assessment of the patient: Vital signs: BP………… / Pulse………………..rep. rate…………….oxygen saturation…..% oxygen at……./min temperature………….C I am concerned about Blood Pressure because: Urine output: Systolic pressure greater than 160mmHg - output less than 100ml over last 4 hrs Diastolic pressure more than 100mmHg - Significant protein uria (+++/++++) Systolic pressure less than 90mmHg Haemorrhage Pulse because: - Antepartum Pulse rare more than 120 - Postpartum Pulse rate less than 40 Fetal well being Pulse rate greater than systolic BP - Fetal heart rate Respiration rate because: - Fetal movement Rate less than 10/min - NST Rate more than 30/min BACKGROUND (tick relevant sections) The women is: Parity (primiparous / multiparous / granmultiparous) with gestation……..weeks & a (singleton/ multiple pregnancy) The present fetal assessment is: Fundal height……wk/cm Presentation……….with……..fiths above brim: Fetal heart rate……..bron Antenatal risks Risk identified on antenatal card / period……………………………… Labour Not in labour / spontaneous onset of labour/induced labour IUGR/ Pre-eclampsia/reduced fetal movements / Diabetes / Antepartum haemorrhage On sysntocinon infusion(……..IU/…………….ml fluid given at……………….ml / hour) Most recent vaginal examination done at………………..h. Dialated……………cm with effacement……………% at saturation Membranes: Intact / ruptured at………..h with currently clear /meconium stained liquor /blood stained liquor rd Delivered…………………..at………………h with 3 stage complete / retained placenta Post natal Delivery date………………at…………….h………………type of delivery…………….with/without perineal trauma Blood loss………………..ml Syntocinon infusion………………IU/…………………ml at……………..ml/hour Fundal height: High/ Atonic/ Tender/ Abdominal- perineal wound oozing Treatment given / in progress Rx………………………………………………………………………………………………………………………………………………………………….. ASSESMENT I think the problem is……………………………………………………………………………………………………………………………………. The problem may be related to: Cardiac/ infection/ respiratory/hemorrhage/PET/HELP/Embolism/Plum oedema/Fetal distress I am not sure what the problem is, but the woman is deteriorating and we need to do something RECOMMENDATION Request I think delivery need to be expedited I think the patient need to be transferred I would like advice on management of the patient Response …………………………………………………………………………………………………………………………………………………………….. Person completing form(Name)…………………………………….Designation………………………………..Date……………………Time…………………Signature Person reported to (Name)……………………………………. Designation………………………………Institution………………….. NB! After completing and consultation, place this form in the patient file as proof of communication and response IGMH contact numbers: 331 5502 7874298