Cardiorespiratory Fitness

Cardiorespiratory
Fitness
Cardiorespiratory Fitness
Assessment
• Purpose
–
Determine level of fitness & set goals
– Develop safe & effective exercise prescription
– Document improvements
– Motivation
–
Provide info concerning health status
Cardiorespiratory Fitness
• Health Related
– Low levels
• ↑ d risk of premature death
–
↑ s
• reduction of death from all causes
– High levels
• high levels of PA & better health
Cardiorespiratory Fitness
• Related to the ability to perform large muscle, dynamic, moderate-to-high intensity exercise for prolonged periods.
Performance depends on
Respiratory
Cardiovascular
Skeletal muscles
Measuring Cardiovascular
Endurance (Aerobic Capacity)
• Best Measure?
• VO
2max
– O
2 uptake – Pulmonary
– O
2
–
O
2 transport – Cardiac utilization - Muscular
Measuring Cardiovascular
Endurance (Aerobic Capacity)
•
VO
2max
– Measure
– Estimate
–
Laboratory Tests
– Field Tests
1
Measuring Aerobic Capacity
Laboratory Methods
Measures of Maximal Exercise Capacity
• Maximal Oxygen Consumption
Submaximal estimations
•
Astrand Rhyming Nomogram
• YMCA Cycle Protocol
Linear Relationships Among
VO
2
.
Measuring Aerobic Capacity
Field Methods
Distance runs
• 1 Mile Run
•
1.5 Mile Run
•
12 Minute Run
• 6 Minute Walk
• Rockport 1-Mile Walk Test
Measuring Aerobic Capacity
Field Methods
Step tests
• YMCA 3-Minute Step Test
Predicting VO
2max w/o exercise
VO
2max
= 50.513 + 1.589 * self-reported physical activity –
.0289 * age in yrs - .552 & %Fat + 5.836 * gender
(female = 0; male = 1)
Measuring Aerobic Capacity
Laboratory Tests
Vs
.
Field Methods
Advantages/Disadvantages??
2
Cardiorespiratory Fitness
• Which test?
– Time demands
–
Expense or costs
– Personnel needed (i.e., qualifications)
– Equipment & facilities needed
–
Physician supervision needed
– Population tested (safety concerns)
–
Need for accuracy of data
Cardiorespiratory Fitness
• Field or Submaximal Tests advantages
– Less expensive
–
Does not need same level of clinical supervision
–
Lower risk
– Less sensitive & specific for disease detection
– Less equipment
– Generally shorter
– In lab tests can assess a workload progression
– Estimates of VO
2
Cardiorespiratory Fitness
• Field or Submaximal Tests disadvantages
– Maximum measures estimated
– VO
2max prediction error can be 10-20%
–
Limited diagnostic capabilities
– Limited for exercise prescription
Standard Procedures
(must be followed)
• Standard testing protocol
• Same modality & protocol – repeat testing
• Constant pedal rate
• Seat height
• Time of day
• Data collection standardized & consistent
• Subjects free of infection – normal sinus rhythm
• Pre test instructions
• Room Temperature (64-68 O ) – air flow
Assumptions of Submax
Tests
• Measurements made in steady state
• Linear relationship b/n HR & VO
2
• HR max similar at same age
• Mechanical efficiency same
Indications for Stopping an Exercise
Test in Low-Risk Adults
•
Angina-like symptoms
• Drop (20 mmHg) in systolic BP or a failure to rise
• Excessive rise in BP
– systolic pressure > 260 mmHg
– diastolic pressure > 115 mmHg
• Signs of poor perfusion
– light-headedness, confusion, ataxia, pallor, cyanosis, nausea, or cold & clammy skin
3
Indications for Stopping an Exercise
Test in Low-Risk Adults
• Failure of heart rate to ↑
• Noticeable ∆ in heart rhythm
• Subject requests to stop
• Physical or verbal manifestations of severe fatigue
• Failure of the testing equipment
Measuring Aerobic Capacity
Criterion Based Reference
Minimal levels of aerobic capacity associated with a reduced risk of disease & death
• Females = VO
2max
•
Males = VO
2max of 31.5 ml/kg/min of 35.0 ml/kg/min
Norm Based Reference
Cardiorespiratory Fitness
•
Field Tests
– Complete a measured distance
– Distance covered in a certain time
• Submaximal Tests
–
Step test
– Single or multiple stage cycle test
– HR measure
• Maximal Exertion
– Graded or progressive exertion to volitional fatigue (measure)
Pre-Test Considerations
1. Abstain from eating prior (>4 hrs)
2. Abstain from strenuous exercise (> 24 hrs)
3. Abstain form caffeine (>12-24 hrs)
4. Abstain from nicotine (> 3 hrs)
5. Abstain from alcohol (> 24 hrs)
6. Medications
Step Tests
Queens College or McArdle Step Test
• Step: ht = 16.25 in for 3 min
• Men: 24 steps/min;
– Women: 22 steps/min
• Radial pulse in 1st-5 sec, for 15 sec
• Men: VO
2max
= 111.33 – (0.42 * HR)
• Women: VO
2max
= 65.81 – (0.1847 * HR)
1.5 Mile Run
• Record total time to complete 1.5 miles
• VO
2max
= 3.5 + 483/time
– Time in nearest hundredth of min
4
12 Min Walk/Run
• Cover maximum distance in 12 min
• VO
2max
= (3.126 * meters) - 11.3
Submaximal Cycle
Ergometer Advantages
• Non-weight bearing
• Accurate workloads
• Easy to measure HR & BP
• Cost is lower than treadmill
• Requires smaller space
• No electricity needed
Submaximal Cycle
Ergometer Disadvantages
• Non-familiar work mode
• Must maintain cadence
• Leg fatigue
Submaximal Prediction of
CRF - Assumptions
• B/n HR of 110-150
• HR max
= 220-age
• Steady State
• Constant cadence
Submaximal Prediction of
CRF – Sources of Error
• HR max
• Efficiency
• Calibration
• Accurate measurement of HR
• HR at steady state
Cycle Ergometer Protocols (other)
Astrand-Rhyming Cycle Ergometer Test
•
Single Stage Test – 6 minutes
• Males – unconditioned: 300 or 600 kgm/min
(50 or 100 watts)
• Males – conditioned: 600 or 900 kgm/min (100 or 150 watts)
•
Females – unconditioned: 300 or 450 kgm/min
(50 or 75 watts)
•
Females – conditioned: 450 or 600 kgm/min
(75 or 100 watts)
5
Cycle Ergometer Protocols (other)
Astrand-Rhyming Cycle Ergometer Test
(cont)
•
50 rpm
• Goal – HR b/n 125 to 170 – measured during
5 th & 6th minutes – average the 2 HRs for nomogram
• Nomogram – page 73 (Figure 4-1)
•
Age adjustment – page 72
Treadmill Testing
• Not usually used for submaximal testing
• Range of efficiencies is so high
• Would not recommend – but can be done
Step Tests
• Astrand-Rhyming
– Single step height – 33 cm for women, 40 cm for men
– Rate = 22.5 steps/min for 6 minutes
• YMCA Protocol
– 12 in – 24 steps/min
– 1 min - Recovery heart rate
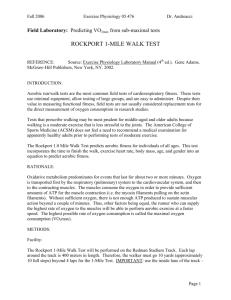
Field Tests
• Rockport 1-mile walk Test
–
HR at end
– VO
2max
(ml/kg/min) = 132.9 – 0.17 (body mass in kg) – 0.39 (age in yrs) + 6.3 (gender) - 3.26
(time in min) – 0.16 (HR)
• 1.5-mile run test
– VO
2max
(ml/kg/min) = 3.5 + 483/(time in min)
6