Clinical Review Article
Metastatic Disease to Bone
David J. Jacofsky, MD
Deborah A. Frassica, MD
Frank J. Frassica, MD
he skeleton, after the lungs and liver, is the
third most common site of metastatic disease,1,2
and metastatic disease is the most common
malignancy of bone. Half of the nearly 1.4 million cases of newly diagnosed cancers each year involve
tumors that frequently metastasize to bone (Table 1).3
Prostate, breast, lung, kidney, and thyroid cancers
account for 80% of skeletal metastases.1 A predilection
for the axial skeleton is seen, perhaps owing to the
venous blood flow in Batson’s plexus. Overall, the most
common sites of bony metastases are the spine, pelvis,
ribs, skull, and proximal femur. When rare acral (ie, distal) metastases to the hands and feet occur, they most
commonly originate from a lung primary.4,5
As postcancer survival has increased with improvements in treatment, the numbers of patients developing
metastatic disease during their lifetime has also
increased. In careful postmortem studies of patients who
succumbed to malignancy, rates of skeletal metastases
approached 70%.2 This number increased to 85% when
only breast, lung, kidney, thyroid, and prostate primary
cancers were considered. This article reviews the presentation and evaluation of patients with metastatic bone
disease and discusses the management of these patients.
T
CLINICAL EVALUATION
Presentation
The presentation of metastatic bone disease is variable, but pain is the most common complaint. The pain
of metastatic disease is usually insidious in onset and is
present in 75% of patients at presentation.6 Painless
lesions usually are diagnosed during staging or routine
follow-up (eg, technetium bone scan) in patients with a
known history of carcinoma. Night pain and pain incompletely relieved by rest are not specific for metastasis
alone, but they are typical symptoms. Weightbearing
bones may become symptomatic early in the course of
disease, whereas bones such as the flat bones of ribs or
sternum may remain asymptomatic until late in the disease, often until pathologic fracture occurs.
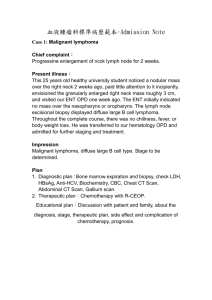
Figures 1 and 2 show the algorithms used for evaluation of the patient with suspected metastatic bone dis-
www.turner-white.com
ease. The use of a schema such as these will diagnose
85% of suspected metastatic malignancies and their
primary malignancies.7
History
The history in a patient with suspected malignancy
should be more thorough than is often required for
other orthopaedic conditions. Risk factors for carcinoma, such as tobacco abuse, alcohol abuse,8 chronic infections (especially viral), exposure to ionizing radiation, exposure to carcinogens, and family history of
cancer, must be thoroughly explored and specifically
questioned. Many patients will not know, for example,
that chronic hepatitis is a strong risk factor for hepatocellular carcinoma, or that ulcerative colitis portends a
markedly increased risk for colon cancer. Past medical
history should be carefully discussed and reviewed.
Patients may not recall the removal of a small mole on
their back unless specifically asked.
A review of symptoms should go beyond simply a
question regarding malaise or weight loss. Inquiries
about cough, dyspnea, hematuria, flank pain, urinary
hesitancy and/or painful urination, endocrine symptoms, and the noticing of any “lumps or bumps” are
only some of the required queries in this patient population. If not specifically addressed, the patient with
undiagnosed metastatic prostate cancer, for example,
may make no connection between his frequent urination and his hip pain.
Physical Examination
The physical examination should be comprehensive.
Examination of the musculoskeletal system in isolation
is inadequate in this patient population if one wishes to
diagnose a yet undetermined primary malignancy or
Dr. Jacofsky is an assistant professor, Department of Orthopaedics, Mayo
Clinic, Rochester, MN. Dr. Deborah Frassica is an associate professor of
radiation oncology and Dr. Frank Frassica is chairman, Department of
Orthopaedic Surgery, and Robert A. Robinson Professor of Orthopaedic
Surgery, Johns Hopkins University School of Medicine, Baltimore, MD.
Hospital Physician November 2004
21
Jacofsky et al : Metastatic Disease to Bone : pp. 21 – 28, 39
Table 1. Incidence of Primary Cancers that Frequently
Metastasize to Bone (United States, 2004)
Primary Site
Estimated Cases Diagnosed
Prostate
230,110
Breast
217,440
Lung
173,770
Kidney
35,710
Thyroid
23,600
Data from Cancer facts and figures—2004. Atlanta: American Cancer
Society; 2004. Available at www.cancer.org. Accessed 27 Sep 2004.
locate additional sites of metastatic disease. In addition
to a focused examination in the symptomatic area,
examination of the breasts, thyroid, prostate, and skin
should be performed when appropriate. Lymphadenopathy should be sought by palpation of the
major lymph node chains (axillary, supraclavicular,
and inguinal). A stool guaiac study may be helpful if a
gastrointestinal primary malignancy is suspected.
Hyperreflexia (eg, Chovstek’s sign) may be a sign of
hypercalcemia, a risk in patients with bone malignancy.
Additionally, careful examination for deep vein thrombosis is prudent in this high-risk group.
LABORATORY STUDIES
A complete blood count, erythrocyte sedimentation
rate, C -reactive protein level, blood chemistries, and
liver function tests should be ordered as deemed appropriate to rule out other diagnoses such as infection,
hyperparathyroidism, or metabolic bone disease. A urinalysis to search for occult blood should be performed,
as occult hematuria may be the only early finding in
renal or bladder carcinoma. Additionally, a urine and
serum protein electrophoresis to rule out multiple
myeloma, and a prostate-specific antigen test to rule
out prostate carcinoma, may be wise in some patients.
Subtle findings of anemia, thrombocytopenia,
leukopenia, or abnormal liver function tests should
not be dismissed without further evaluation, as these
may support systemic findings of metastatic disease. An
ionized calcium level is helpful in the identification of
hypercalcemia, as low albumin levels may make total
calcium values difficult to interpret. One should also
remember that many carcinomas can cause fever and
elevated acute-phase proteins (eg, C -reactive protein)
in the absence of infection. Therefore, these findings
in isolation do not rule out metastatic disease, nor do
they empirically confirm the diagnosis of infection.
Although tumor markers such as carcinoembryonic
antigen, CA-125, and CA 19-9 are extremely helpful in
22 Hospital Physician November 2004
monitoring the response of certain cancers to treatment, they are of little, if any, value in the initial workup of metastatic disease with an unknown primary.
IMAGING STUDIES
Radiographs
Radiographs of the symptomatic area are the first step
in the imaging evaluation of suspected bone metastases.
In addition, radiographs are important for the interpretation of abnormal findings on the technetium bone
scan. The clinician should correlate the technetium
bone scan with the plain radiographs prior to confirming
the diagnosis of metastatic bone disease with the patient.
Up to 30% of benign enostoses (bone islands) and most
enchondromas exhibit increased uptake on technetium
scans. Technetium scans are very sensitive but nonspecific in distinguishing malignant and nonmalignant abnormalities. Radiographs are often diagnostic for enchondromas, bone islands, bone infarcts, and other incidental
findings in the cancer patient. Up to 40% of metastatic
lesions may be missed on radiographic survey, because
30% to 50% of mineral loss or a lesion size of greater
than 1.5 cm is typically required for consistent detection.9
One’s ability to see less dramatic findings is certainly
enhanced if a positive bone scan localizes an area of
interest for scrutiny. One must carefully inspect all the
cortices to detect subtle bone destruction.
The radiographic appearance of metastatic disease
may be purely lytic, purely blastic (sclerotic), or mixed.
Metastases from prostate, bladder, medulloblastoma, and
bronchial carcinoid tumors are most likely to be blastic in
nature (Figure 3). Purely lytic metastases are usually secondary to renal, pulmonary, thyroid, uterine, adrenal,
melanoma, or gastrointestinal cancers (Figure 4). Mixed
lesions are typically due to primary cancers of the breast,
ovary, testicle, cervix, or lymphatic tissues.10,11 It is important to remember, however, that any cancer can appear
in any pattern. Traditionally, primary sarcomas are associated with periosteal reactions (eg, Codman’s triangle,
sunburst reactions), but one must avoid the temptation
to definitively diagnose metastatic disease from a radiographic impression alone. Misdiagnosis of a primary
mesenchymal sarcoma of bone as metastatic disease,
with subsequent internal fixation rather than resection,
can compromise limb-salvage options and even the life
of the patient.
Technetium Bone Scan
Technetium Tc 99m methylene diphosphonate
scanning is a very useful adjunct study in the work-up
for metastatic bone disease in a patient with known or
suspected cancer. Tumor osteolysis (directly caused by
www.turner-white.com
Jacofsky et al : Metastatic Disease to Bone : pp. 21 – 28, 39
Bone pain/history of cancer
Plain films: hip & pelvis
Chest radiograph
Laboratory tests
Suspicious lesion/normal radiograph
Nonmalignant diagnosis
Bone scan
Appropriate work-up
Single focus
MRI scan locally
Restaging evaluation
Multiple lesions
Possible sarcoma
Restaging evaluation
± biopsy, ± fixation
Referral as indicated for
CTX/XRT
Probable metastatic
disease
Biopsy
Nonrenal, nonthyroid
primary cancer
Fixation, CTX, XRT,
as indicated
Renal or thyroid
primary cancer
Referral to orthopaedic
oncologist
Figure 1. Evaluation of patient with known primary cancer. CTX = cytotoxic chemotherapy; MRI = magnetic resonance imaging;
XRT = radiation therapy. (Adapted from Hage W, Aboulafia A, Aboulafia D. Incidence, location, and diagnostic evaluation of metastatic bone disease. Orth Clin North Am 2000;31:523 with permission from Elsevier.)
osteoclastic resorption) causes a compensatory hyperemic and coupled osteoblastic response of varying
degrees; this activity is responsible for the deposition of
radioisotope tracer and, therefore, a positive finding
on the test (Figure 5).
Tracer uptake on technetium bone scanning is not
specific for metastatic bone disease. Monostotic lesions
identified by technetium scanning in patients with
known cancer will be proven to be metastases in only
50% of cases, underscoring the importance of a biopsy
for confirmation, even in a patient with a known primary malignancy.10 Benign lesions such as enchondroma, infection, Paget’s disease, stress fracture, and
enostoses also may cause increased tracer uptake. Additionally, second primary cancers of mesenchymal origin (eg, chondrosarcoma) are rare but do occur. Multi-
www.turner-white.com
ple positive polyostotic findings in a patient with a
known cancer are most likely to be metastatic disease,
but a biopsy of a readily accessible site is still wise in the
absence of visceral metastases.
A false-negative bone scan may occur despite the presence of single or multiple lesions from multiple myeloma
(or solitary plasmacytoma), melanoma, Langerhans cell
histiocytosis, lymphoma, leukemia, thyroid carcinoma,
neuroblastoma, purely lytic lung carcinoma, or, rarely,
breast cancer. Some authors argue against the use of routine bone scanning for staging of squamous cell cancer
of the head and neck,12 bladder cancer, and melanoma
because of the very low incidence of bony metastases in
these cancers. The presence of bone pain, however,
should prompt such an evaluation.
In the setting of diffuse metastatic disease, the
Hospital Physician November 2004
23
Jacofsky et al : Metastatic Disease to Bone : pp. 21 – 28, 39
Bone pain
Plain films: hip & pelvis
Chest radiograph
Laboratory tests
Multiple myeloma
Unknown primary cancer
Skeletal survey
Referral to oncologist
Technetium Tc 99m
bone scan
CT: chest, abdomen, pelvis
Primary cancer
elucidated
Go to Figure 1
Unknown primary
monostotic disease
Unknown primary
polyostotic disease
Assume sarcoma
Referral to orthopaedic
oncologist
Biopsy
A
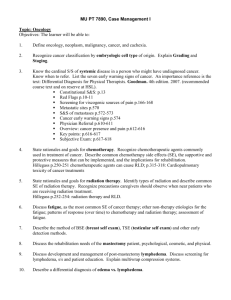
Figure 2. Evaluation of patient with no
prior cancer history. CT = computed tomography. (Adapted from from Hage W,
Aboulafia A, Aboulafia D. Incidence, location, and diagnostic evaluation of metastatic bone disease. Orth Clin North Am
2000;31:524 with permission from
Elsevier.)
B
Figure 3. Radiographic appearance of blastic metastases. (A) Anterior-posterior view of the pelvis shows diffuse blastic lesions in the
sacral ala on both the left and right sides. In addition, a blastic lesion is visible in the right supra acetabula area. (B) Anterior-posterior
view of the proximal humerus shows a dense sclerotic lesion in the metaphysis with no cortical bone destruction.
increased uptake may be so diffuse and marked that no
single area appears intense; this can result in the bone
scan appearing normal. This phenomenon, termed a
superscan, can be diagnosed by looking for “renal steal,”
which is the absence of the normal renal uptake pattern
that results from the excretion of excess isotopes. This
pattern may also be seen in patients with poor renal
clearance, however, and should not alone lead to the
diagnosis of diffuse metastatic disease. Bone scanning
24 Hospital Physician November 2004
for metastatic thyroid carcinoma can be improved with
the use of technetium-99m methoxyisobutyl isonitrile.13
Computed Tomographic Scan
A computed tomographic (CT) scan of the chest,
abdomen, and pelvis can be studied to search for primary
disease, as well as to look for lymphadenopathy or
metastatic disease in the lungs or liver. A CT scan of the
local site of metastasis is occasionally performed and may
www.turner-white.com
Jacofsky et al : Metastatic Disease to Bone : pp. 21 – 28, 39
Figure 4. Anterior-posterior radiograph of the proximal
humerus showing a lytic destructive lesion in the proximal diaphysis. The lesion is poorly marginated. There is no reactive
bone. This is a very common appearance of metastatic renal
cell carcinoma.
Figure 5. Technetium bone
scan of a patient with metastatic prostate carcinoma. Notice
the intense uptake in the sacral
ala on both sides. There is intense uptake in the right supra acetabula area and the left
lesser trochanteric area.
Notice the marked increase
activity in the left proximal
humerus and the right sixth
rib. There is also metastasis in
the upper lumbar spine.
provide excellent osseous detail. This may be useful in the
evaluation of subtle cortical irregularities or mineralized
lesions in the medullary cavity or soft tissues.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is often performed at the site of metastatic disease. MRI is often
useful in cases in which the bone scan is negative but
localized symptoms are present. In addition, MRI is
more sensitive than technetium bone scanning in the
detection of bone metastases because earlier marrow
abnormalities may be identified14 (Figure 6). MRI is
the gold standard for evaluation of soft tissue masses.
In the spine, MRI is valuable in assessing the extent
of involvement as well as evaluating for spinal cord
or nerve root compression. Additionally, MRI can occasionally be helpful in determining the extent of disease and marrow involvement in patients requiring
radiotherapy postoperatively or for palliation.
Positron Emission Tomography
Positron emission tomography (PET) utilizing flu-
www.turner-white.com
R Anterior
orodeoxyglucose is becoming more widely available.
PET scans have the potential of both high sensitivity
and high specificity. In some malignancies, such as thyroid cancer, the results of the PET scan may be positive
while results of all other diagnostic modalities (ie,
radiograph, bone scan, MRI, CT) are negative. As clinical trials of PET scanning in the orthopaedic setting
continue, the use and understanding of this diagnostic
modality is certain to increase.
Hospital Physician November 2004
25
Jacofsky et al : Metastatic Disease to Bone : pp. 21 – 28, 39
A
C
B
BIOPSY
It is generally prudent to confirm the diagnosis of
bone metastases with biopsy. A solitary bone lesion in a
patient with cancer should not be assumed to be from
the patient’s cancer. In addition, in cancer patients who
develop bone lesions without the presence of visceral
metastases, biopsy should be considered to confirm the
diagnosis. A biopsy should be viewed as a confirmatory
study of metastatic disease—in only a minority of patients can the primary site of the malignancy be diagnosed by biopsy alone.15 In polyostotic lesions, the
26 Hospital Physician November 2004
Figure 6. (A) Anterior-posterior radiograph of the hip of a
patient with metastatic breast carcinoma. A poorly marginated
lesion in the greater trochanter is visible, with thinning of the cortex. (B) Coronal T1-weighted magnetic resonance imaging scan of
the pelvis. A low-signal lesion can be seen occupying the entire
greater trochanter and extending down to the subtrochanteric
level. On the opposite (left) hip, multiple round, low-density,
low-signal lesions are visible in both the proximal femur and the
acetabulum, consistent with metastatic bone disease. (C) A coronal inversion recovery sequence shows high-signal activity in the
greater trochanter extending to the subtrochanteric level, masking the area of involvement seen on the T1-weighted image.
most easily accessible lesion should be chosen for biopsy. If, however, there exists an area of impending fracture, this site may be biopsied at the time of surgical
stabilization if frozen section confirmation of metastatic disease is available at the institution.
Biopsy may be performed via fine needle aspiration,
CT-guided needle or core sampling, or via open techniques. Open techniques typically require operative time
and often the risk of anesthesia. The choice of biopsy
technique must be based on the lesion size and location, the surgeon’s experience, the experience of the
www.turner-white.com
Jacofsky et al : Metastatic Disease to Bone : pp. 21 – 28, 39
radiologist, and the preferences of the musculoskeletal
pathologist who will be making the histologic diagnosis.
If a primary sarcoma is a possibility, the biopsy must
be performed in a manner that will not complicate or
compromise future oncologic resection or possible
limb-salvage procedures. In most cases, if a primary
sarcoma is suspected (eg, no primary cancer is found
after work-up, or a patient with a distant history of cancer has a solitary lesion and no other evidence of active
disease), the patient should be referred for biopsy to
an orthopaedic oncologist who can perform the definitive procedure.
In cases of an isolated renal or thyroid metastasis,
oncologic resection with wide margins may be indicated because of the possibility of cure in isolated metastatic lesions with these diagnoses. These patients
should be considered for referral to an orthopaedic
oncologist as well.
Histologic examination of bone biopsy specimens
can differentiate metastatic disease from multiple
myeloma, lymphoma, or primary sarcoma. Metastatic
bone lesions show a consistent pattern of clusters of
epithelial cells grouped in a glandular pattern in a
fibrous stroma (Figure 7).
TREATMENT
There are 4 basic tenets in the orthopaedic treatment of metastatic disease to bone: pain control, prevention and treatment of fractures, maintenance of
patient independence, and prevention of tumor progression.
Pain Control
Pain from bony metastases can be caused by tumor
biology and the local effects of bone destruction or by
the resultant structural insufficiency. Bone pain without structural insufficiency is often effectively treated
with narcotic analgesics and radiation therapy, usually
external-beam irradiation. Patients often benefit from
hormonal therapy (eg, in metastatic prostate carcinoma), cytotoxic therapy, and/or bisphosphonate therapy. Bisphosphonates have been shown to improve pain
and reconstitute bone stock. Some bisphosphonates
may decrease tumor cell burden through induction of
tumor apoptosis.16
Prevention and Treatment of Fractures
Prediction of fracture risk. Surgical stabilization to
prevent pathologic fracture can immediately improve
pain, mobility, and independence. Clinicians are often
required to determine the appropriateness of surgical
intervention in patients referred for “impending frac-
www.turner-white.com
ture.” The criteria for impending fracture are in no
way absolute, and the clinician must consider the patient’s surgical risk stratification, estimated life expectancy, and previous level of function when making
decisions regarding the appropriateness of surgery as
well as the implant type to be recommended. Many criteria exist in the literature for prediction of fracture
risk,17 – 21 but none have been decisively supported in
clinical trials. Important factors include the amount
and pattern of bone destruction, the location of the
lesion (or lesions), and the quality of associated pain.
The amount of bone destruction is the most important variable to be considered. The amount of involvement requires assessment of 2 orthogonal radiographs,
through which 4 cortices are assessed and their involvement summed. Fidler20 has shown that fractures are
highly unlikely (2.3% risk) when less than 50% of the
cortical bone is involved, but very likely to occur (80%
risk) if 75% of the cortical bone is involved. Eccentric
lesions are more worrisome than similarly sized lesions
that are located centrally. The pattern of bone destruction is also significant. Purely blastic lesions are least
likely to fracture. Purely lytic lesions are the most likely
to cause bone failure and the least likely to heal. Mixed
lesions are of intermediate risk.22,23 Location of the
lesion is also of paramount importance. Areas of high
stress, such as the femoral neck and subtrochanteric
regions, or the humeri in patients using walkers, are
most likely to be exposed to forces in excess of the
bone’s ultimate strength.
Weightbearing pain is another important predictor
of fracture. When patients experience pain with every
step that decreases with rest, structural insufficiency is
likely present during normal physiologic loading. If,
however, pain is present at night and at rest, then this
pain may be due to tumor biology rather than structural osseous insufficiency.
Serial radiographs are often helpful in monitoring
disease progression. Certainly, all patients treated conservatively for metastatic disease should have follow-up
radiographs to evaluate progression of disease.
Surgical options. A complete discussion of surgical
options for metastatic disease is beyond the scope of
this review. Plates, intramedullary devices, and prosthetics all have their specific places in the orthopaedist’s
armamentarium. Plates with methylmethacrylate augmentation are quite useful for metaphyseal and epiphyseal fixation but require an intact articular surface and
sufficient nearby bone stock for fixation. At least 1 intact cortex is typically required to achieve rigid fixation
and allow full weightbearing postoperatively if plate fixation is utilized. Reamed intramedullary nails have a
Hospital Physician November 2004
27
Jacofsky et al : Metastatic Disease to Bone : pp. 21 – 28, 39
A
B
Figure 7. (A) Photomicrograph of bone tissue in a patient with metastatic breast carcinoma. Clusters of round epithelial cells arranged
in an organoid fashion are visible in a background of fibrous tissue. This histologic appearance is consistent with metastatic carcinoma
(hematoxylin and eosin stain). (B) Photomicrograph of bone tissue of a different patient with metastatic renal cell carcinoma. Clear cells
grouped in clusters are visible. This histologic appearance is consistent with clear cell carcinoma of the kidney (metastatic hypernephroma) (hematoxylin and eosin stain).
neutral axis almost identical to that of the bone in
which they are placed. This load-sharing device, with a
small-moment arm and low transmission of torque,
confers excellent implant survival despite immediate
full weightbearing. Large destructive lesions, intra- or
peri-articular lesions, and lesions not permitting rigid
fixation may require prosthetic replacement. Modular
and custom complex prostheses are available.
One useful adjunctive procedure to be considered in
the treatment of metastatic disease is preoperative
tumor embolization. Most, if not all, metastatic lesions
are hypervascular. Some lesions, especially renal metastases and myeloma, are notorious for the rich vascular
network associated with them. This hypervascularity can
be a source of markedly increased perioperative risk, as
massive intraoperative blood loss can cause death, especially in patients with chronic illness and minimal physiologic reserve. Significant decreases in blood loss are
seen with preoperative embolization.24 Embolization
can be expected to be successful in up to 90% of
cases.25,26 Metallic coils, polyvinyl alcohol beads, or gelatinous sponges may be used. With coils or polyvinyl
alcohol, a 24- to 36-hour delay before surgery will not
have a detrimental effect.24 Surgery should take place
within 24 hours if gelatin is used to minimize loss of
effectiveness via resorption of gelatin and recanalization
of vessels. Embolization is especially helpful if reaming
through a tumor is to be performed. Embolization may
also be used as a method of pain control in patients
who are not candidates for surgery.27–29
Prevention of Tumor Progression
In virtually all patients undergoing prophylactic fixation for metastatic disease, postoperative external-beam
irradiation is warranted. Townsend et al30 found that
15% of patients treated with surgery alone required a
second surgical procedure because of increasing pain
or subsequent loss of fixation. In comparison, only 3%
of patients who received postoperative radiation therapy needed additional surgical procedures.
Radiation therapy should be initiated after fixation
and usually is begun 2 to 4 weeks postoperatively. The
dose administered is 20 to 30 Gy divided into 5 to
10 fractions. The radiation field should include the
original site of disease and the entire implant or fixation device, along with an adequate margin.31 In patients with life expectancies greater than 12 months
(eg, those with solitary breast or renal metastases with
no active primary disease) larger doses (eg, 45 Gy
divided into 1.8-Gy fractions) may be warranted.
PROGNOSIS
Unfortunately, virtually all patients with bony metastatic disease eventually succumb to cancer. Median survival
ranges from 6 to 48 months, but it is difficult to predict
an individual patient’s prognosis. The median survival
after the development of bony metastases is 48 months
for thyroid carcinoma, 40 months for prostate cancer,
24 months for breast cancer, and 6 months for melanoma, kidney, and lung cancers.32 However, these are averages. For example, a patient with renal cell carcinoma, a
2-year disease-free interval, no visceral disease, and a
nonaxial metastasis may live for many years. Discussion of
the variety of positive and negative prognostic factors for
each disease is beyond the scope of this review.
CONCLUSION
The management of metastatic bone disease is
(continued on page 39)
28 Hospital Physician November 2004
www.turner-white.com
Jacofsky et al : Metastatic Disease to Bone : pp. 21 – 28, 39
(from page 28)
complex and requires a multidisciplinary approach.
The evaluation must be thorough regardless of
whether the patient has a previously diagnosed cancer.
The treatment is geared toward controlling pain, preventing and treating fracture, maintaining the patient’s
independence, and preventing progression of the
tumor. Surgeons, radiation and medical oncologists,
radiologists, physiatrists, therapists, nutritionists, and
pain clinicians must collaborate to maximize the patient’s longevity and quality of life and to coordinate
care in an expeditious and logical manner.
HP
REFERENCES
16.
17.
18.
19.
1. Buckwalter JA, Brandser EA. Metastatic disease of the
skeleton. Am Fam Physician 1997;55:1761–8.
2. Jaffe HL. Tumors metastatic to the skeleton. In: Jaffe
HL, editor. Tumors and tumorous conditions of the
bones and joints. Philadelphia: Lea & Febiger; 1958.
3. Cancer facts and figures—2004. Atlanta: American
Cancer Society; 2004. Available at www.cancer.org.
Accessed 27 Sep 2004.
4. Healey JH, Turnbull AD, Miedema B, Lane JM. Acrometastases. A study of twenty-nine patients with osseous
involvement of the hands and feet. J Bone Joint Surg
Am 1986;68:743–6.
5. Libson E, Bloom RA, Husband JE, Stoker DJ. Metastatic
tumours of bones of the hand and foot. A comparative
review and report of 43 additional cases. Skeletal Radiol
1987;16:387–92.
6. Wagner G. Frequency of pain in patients with cancer.
Recent Results Cancer Res 1984;89:64–71.
7. Simon MA, Finn HA. Diagnostic strategy for bone and
soft-tissue tumors. J Bone Joint Surg Am 1993;75:622–31.
8. Seitz HK, Stickel F, Homann N. Pathogenetic mechanisms of upper aerodigestive tract cancer in alcoholics.
Int J Cancer 2004;108:483–7.
9. Bunker SR, Kleiner BC. Bone imaging. In: Harrington
KD, editor. Orthopaedic management of metastatic
bone disease. St. Louis: Mosby; 1988:35–52.
10. Rosenthal DI. Radiologic diagnosis of bone metastases.
Cancer 1997;80(8 Suppl):1595–607.
11. Rouleau P, Wenger D. Radiologic evaluation of metastatic bone disease. J Am Acad Orthop Surg 2002;10:
313–22.
12. Brown DH, Leakos M. The value of a routine bone scan
in a metastatic survey. J Otolaryngol 1998;27:187–9.
13. Alam MS, Kasagi K, Misaki T, et al. Diagnostic value of
technetium - 99m methoxyisobutyl isonitrile (99m
Tc-MIBI) scintigraphy in detecting thyroid cancer metastases: a critical evaluation. Thyroid 1998;8:1091–100.
14. Traill ZC, Talbot D, Golding S, Gleeson FV. Magnetic
resonance imaging versus radionuclide scintigraphy in
screening for bone metastases. Clin Radiol 1999;54:
448–51.
15. Rougraff BT, Kneisl JS, Simon MA. Skeletal metastases of
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
unknown origin. A prospective study of a diagnostic
strategy. J Bone Joint Surg Am 1993;75:1276–81.
Shipman CM, Rogers MJ, Apperley JF, et al. Bisphosphonates induce apoptosis in human myeloma cell
lines: a novel anti-tumor activity. Br J Haematol 1997;98:
665–72.
Hipp JA, Springfield DS, Hayes WC. Predicting pathologic fracture risk in the management of metastatic
bone defects. Clin Orthop 1995;(312):120–35.
Landis SH, Murray T, Bolden S, Wingo PA. Cancer
statistics, 1998 [published errata appear in CA Cancer J
Clin 1998;48:192 and 1998;48:329]. CA Cancer J Clin
1998;48:6–29.
Mirels H. Metastatic disease in long bones. A proposed
scoring system for diagnosing impending pathologic
fractures. Clin Orthop 1989;(249):256–64.
Fidler M. Incidence of fracture of metastases in long
bones. Acta Orthop Scand 1981;52:623–7.
Fidler M. Prophylactic internal fixation of secondary
neoplastic deposits in long bones. Br Med J 1973;10:
341–3.
Harrington KD. Orthopaedic management of extremity
and pelvic lesions. Clin Orthop 1995;(312):136–47.
Harrington KD. Impending pathologic fractures from
metastatic malignancy: evaluation and management.
Instr Course Lect 1986;35:351–81.
Varma J, Huben RP, Wajsman Z, Pontes JE. Therapeutic
embolization of pelvic metastases of renal cell carcinoma. J Urol 1984;131:647–9.
Sun S, Lang EV. Bone metastases from renal cell carcinoma: preoperative embolization. J Vasc Interv Radiol
1998;9:263–9.
Layalle I, Flandroy P, Trotteur G, Dondelinger RF.
Arterial embolization of bone metastases: is it worthwhile? J Belge Radiol 1998;81:223–5.
Bowers TA, Murray JA, Charnsangavej C, et al. Bone
metastases from renal carcinoma. The preoperative use
of transcatheter arterial occlusion. J Bone Joint Surg Am
1982;64:749–54.
Breslau J, Eskridge JM. Preoperative embolization of
spinal tumors. J Vasc Interv Radiol 1995;6:871–5.
Chuang VP, Wallace S, Swanson D, et al. Arterial occlusion in the management of pain from metastatic renal
carcinoma. Radiology 1979;133(3 Pt 1):611–4.
Townsend PW, Rosenthal HG, Smalley SR, et al. Impact
of postoperative radiation therapy and other perioperative factors on outcome after orthopedic stabilization of
impending or pathologic fractures due to metastatic disease. J Clin Oncol 1994;12:2345–50.
British Association of Surgical Oncology guidelines. The
management of metastatic bone disease in the United
Kingdom. The Breast Specialty Group of the British
Association of Surgical Oncology. Eur J Surg Oncol
1999;25:3–23.
Coleman RE. Skeletal complications of malignancy.
Cancer 1997;80(8 Suppl):1588–94.
Copyright 2004 by Turner White Communications Inc., Wayne, PA. All rights reserved.
www.turner-white.com
Hospital Physician November 2004
39