Critical Care Medicine Congress Abstracts 2015
advertisement

December 2014
OFFICIAL JOURNAL
Supplement to
OF THE
SOCIETY
OF
Volume 42, Number 12
CRITICAL CARE MEDICINE
CONGRESS ABSTRACTS
▲ January 17-21, 2015
▲ Phoenix Convention Center
▲ Phoenix, Arizona, USA
Supplement to Critical Care Medicine
December 2014/Volume 42/Number 12/Abstracts A1–A1304
2014–2014 SCCM EXECUTIVE COMMITTEE AND COUNCIL
Executive Committee
SCCM Council
Heatherlee Bailey, MD, FCCM
President
J. Christopher Farmer, MD, FCCM
Heidi L. Frankel, MD, FCCM
Sandra L. Kane-Gill, PharmD, MS, FCCM
Lewis J. Kaplan, MD, FCCM
President-Elect
Craig M. Coopersmith, MD, FCCM
Lynn A. Kelso, MSN, ACNP, FCCM
Greg S. Martin, MD, MSc, FCCM
Treasurer
Steven J. Martin, PharmD, BCPS, FCCM
Todd Dorman, MD, FCCM
M. Michele Moss, MD, FCCM
Vinay M. Nadkarni, MD, FCCM
Secretary
Ruth M. Kleinpell, RN-CS, PhD, FCCM
Amdrew J. Patterson, MD, PhD, FCCM
Beth Taylor, MD, RD, FCCM
Michael H. Wall, MD, FCCM
Past President
Carol Thompson, PhD, CCRN, FCCM
Jerry J. Zimmerman, MD, PhD, FCCM
44TH CRITICAL CARE CONGRESS PROGRAM PLANNING COMMITTEE
Greg S. Martin, MD, MSc, FCCM, Co-Chair
Lauren R. Sorce, ACNP, CCRN, MSN,
Co-Chair
Daniel R. Brown, MD, PhD, FCCM,
Past Co-Chair
Vinay M. Nadkarni, MD, FCCM, Past
Co-Chair
Jeffrey Barletta, PharmD, FCCM
Katherine V. Biagas, MD, FCCM
Kent D. Blad, DNP, ACNP-BC, FCCM
Benjamin Brainard, VMD
Richard D. Branson, MS, RRT, FCCM
Diane Byrum, CCRN, MSN, RN, FCCM
Cherylee W. Chang, MD, FCCM
Paul A. Checchia, MD, FACC, FCCM
Gail Cresci, PhD, RD, LD
Dennis Tim Crowe, DVM, DACVS, FCCM
William E. Dager, BCPS, PharmD, FCCM
David J. Dries, MD, MSE, FCCM
Michael A. Dubick, PhD
Clarence G. Finch, MBA, RRT, FCCM
Wendy Ricketts Greene, MD, FACS, FCCM
Judith Hellman, MD
Jorge Luis Hidalgo, MD, MACP, FCCM
Marilyn Hravnak, ACNP, PhD, RN, FCCM
Robert C. Hyzy, MD, Professor, FCCM
John A. Kellum, MD, MCCM
Kristine A.K. Lombardozzi, FCCM
Maureen A. Madden, MSN, PCCNP, CCRN
Mark E. Mikkelsen, MD, MSCE
Rahul Nanchal, MD
Mark Edwin Nunnally, MD, FCCM
John Papadopoulos, PharmD, FCCM
Pauline K. Park, MD, FCCM
Steven E. Pass, PharmD, FCCM
Michael A. Rie, MD
Sophia C. Rodgers, ACNP, FCCM
Gloria M. Rodriguez-Vega, MD, FCCM
Tuhin K. Roy, MD, PhD
Richard H. Savel, MD, FCCM
Aryeh Shander, MD, FCCP, FCCM
Corinna Sicoutris, ACNP, CCRN, FCCM
Eric Siegal, MD
Antoinette Spevetz, MD, FACP, FCCM
Ram M. Subramanian, MD
Dan R. Thompson, MD, MCCM, MA, FACP
Christine C. Toevs, MD, FCCM
Michel Torbey, MD, MPH, FAHA, FCCM
Michael H. Wall, MD, FCCM
Chris Winkelman, ACNP, FCCM
Michael B. Yaffe, MD, PhD
Timothy S. Yeh, MD, FCCM
Sergio L. Zanotti-Cavazzoni, MD, FCCM
Janice L. Zimmerman, MD, FCCM
Basilia Zingarelli, MD, PhD
44TH CRITICAL CARE CONGRESS ABSTRACT REVIEWERS
Fernando Jose Abelha, PhD
Prasad E. Abraham, PharmD
Adeyinka Adebayo, MD
Adebola O. Adesanya, MB, MPH
Hemant Agarwal, MBBS
Suresh Agarwal, MD, FCCM
Ritwick Agrawal, MS, MD, FCCP
Naoki Aikawa, MD, DMSc, FACS
Samuel J. Ajizian, MD, FCCM
Ozan Akca, MD, FCCM
Cesar Alaniz, PharmD
Dr. Martin Albert, MD
Sheila A. Alexander, BSN, PhD, RN
Veerajalandhar Allareddy, MD
Gilman B. Allen, MD
Theodore A. Alston, PhD
Rajesh K Aneja MD
Shoshana Arai, RN, CCRN, PhD
Lee M. Arcement, MD, MPH
Ayse A. Arikan, MD
Grace M. Arteaga, MD, FAAP
Rebecca A. Aslakson, MD, PhD
Michael L. Ault, MD, FCCM
Edgar Avalos Herrera, MD, MSc
Ruben Jose Azocar, MD, FCCM
Ahmed E. Badr, MD, FACS
Amado Alejandro Baez, MD, MPH, FCCM
Aranya Bagchi, MBBS
James M. Bailey, MD
Jonathan Bain, BCPS, PharmD
Jose A. Baltazar-Torres, MD
Arvind Bansal, MD
Jeffrey Barletta, PharmD, FCCM
Sangita Basnet, MD, FAAP
Adel M. Bassily-Marcus, MD, FCCM
Angel Carlos Bassols Ricardez, MD
Rajit Basu, MD
Sonali Basu, MD
Michael L. Bentley, PharmD, FCCM
Utpal S. Bhalala, MD
Rahul Bhatia, MD
Katherine V. Biagas, MD, FCCM
Dr. Patrick Biston, MD
Edward A. Bittner, MD, PhD, FCCM
Steven A. Blau, MD
John J. Bon, BCPS, PharmD
Sara J.D. Bork, PharmD, MBA
William M. Bowling, MBA, MD
David Bracco, MD, FCCM
Ludwik K. Branski, MD
Richard D. Branson, MSc, RRT, FCCM
Ronald A. Bronicki, MD
William T. Browne, MD, FCCM
Marilyn N. Bulloch, PharmD
Diane Byrum, CCRN, MSN, RN, FCCM
Luis A. Camputaro, MD, MSc, MSc, FCCM
Charles C. Canver, MBA, MD, CPE, FACHE
Gerardo P. Carino, MD, PhD
David L. Carpenter, PA-C
Todd C. Carpenter, MD
Christopher L. Carroll, MD, MS, FCCM
Jorge A. Castanon-Gonzalez, MD, MSc,
FCCM
Pelin Cengiz, MD
Jean G. Charchaflieh, MD, MPH, DrPH,
FCCM
Sanjay Chawla, BS, MD
Ira M. Cheifetz, MD, FCCM
Sanjeev V. Chhangani, MBA, MD, FCCM
Linda L. Chlan, BSN, PhD, RN, FAAN
Jill Marie Cholette, MD
John Chow, MD
Kenneth B. Christopher, MD
Sai Ho Jason Chui, BCPS, PharmD
Michael Joshua Cisco, MD
Amalia Cochran, MD, FCCM
Panna Codner, MD
Liziamma George, FCCM
Thomas J. Johnson, MBA, PharmD, FCCM
Michael T. Meyer, MD
Jason Cohen, DO
Anthony T. Gerlach, BCPS, PharmD, FCCM
Robert L. Joyner, Jr., PhD, RRT, FAARC
Mark E. Mikkelsen, MD, MSCE
Michael A. Cole, MD
Rik Th. Gerritsen, MD, FCCM
Paul Juang, BCPS, PharmD
Russell R. Miller, III, MD, MPH
Gary R. Collin, MD, FACS, FCCM
Hayley Gershengorn, MD
Deven Juneja, MD, FNB, EDIC
Eduardo Mireles-Cabodevila, MD
Brad E. Cooper, PharmD, FCCM
Shekhar Ghamande, MD
Jason M. Kane, MD, MS, FCCM
Ronald P. Mlcak, PhD
Christiane O. Corriveau, MD, MEd
Santhosh Gheevarghese John, MD, FACP
Sandra L. Kane-Gill, MSc, PharmD, FCCM
Alicia Mohr, BA, MD
Kevin G. Couloures, DO, MPH
Ian C. Gilchrist, MD, FCCM
Dr. Menelaos Karanikolas, MD, MPH
Majid Mokhtari, MD, FCCP
Angel Coz-Yataco, MD
Jason M. Golbin, DO, MS
Jennifer Kaplan, MD, MS
Stefania Mondello, MD, MPH, PhD
Kelli L. Crowley, BCPS, PharmD, RPh
Jeffrey P. Gonzales, BCPS, PharmD,
Markos G. Kashiouris, MD, MPH
Rafael Montecino, MD
Jason N. Katz, MD, MHS
Hiroshi Morimatsu, MD, PhD
Cleon W. Goodwin, MD
Larry J. Kaufman, MD, FCCP, FCCM
Benjamin D. Mosher, MD
Brian M Cummings, MD
Deepak Govil, MD, EDIC, FCCM
Kevin P. Keating, MD
Oussayma Moukhachen, PharmD
Quinn A. Czosnowski, PharmD
Ana Lia Graciano, MD, FAAP, FCCM
Mark T. Keegan, MB, MSc
Eric W. Mueller, PharmD, RPh, FCCM
Anahita Dabo-Trubelja, MD
Loreta Grecu, MD
Ashish K. Khanna, MD, FCCP
Srinivas Reddy Mummadi, MD
Brian J. Daley, MBA, MD
Steven Greenberg, MD
Mehdi Khosravi, MD
Claire V. Murphy, PharmD
Heidi J. Dalton, MD, MCCM, MCCM
Bruce M. Greenwald, MD, FAAP, FCCM
Felix Khusid, RRT- ACCS-NPS, RPFT
Vinay M. Nadkarni, MD, FCCM
Ehab G. Daoud, MD
Phil Grgurich, PharmD, BCPS
Hyung Kook Kim, MD
Silvio A. Ñamendys-Silva, MD, DHCA,
Kshama M. Daphtary, MD
Ioana Grigoras, MD, PhD
Kyuseok Kim, MD, PhD
Saqib I. Dara, MD, PGDipEcho, CPHQ
Colin K. Grissom, MD, FCCM
Tyree H. Kiser, PharmD, BCPS, FCCM
Rahul Nanchal, MD
Luis A. De La Cruz, MBA, MD
A Kendall Gross BCPS, PharmD
Martin CJ Kneyber, MD, PhD
Lama Nazer, PharmD, BCPS
Jonas P. DeMuro, MD
Maritza L. Groth, MD, FCCM
Patrick M. Kochanek, MD, MCCM
Noureddine Nciri, MD, PhD
Rajat Dhar, MD
W Alan Guo, MD
Lisa Kohr, ACNP, FCCM
Kristoffer P. Neu, MD, BS
Kush R. Dholakia, MD
Mohan Gurjar, MD, PDCC, FICCM
Patricia A. Kountz, MSN, CNP
Christopher D. Newman, PA-C
Deepali Dixit, BCPS, PharmD
Jorge A. Guzman, MD, FCCM
David J. Kramer, MD
Masaji Nishimura, MD, PhD
Chaoxuan Dong, MD, PhD
Fahim Habib, MPH
Sundar Krishnan, MD
Akira Nishisaki, MD
Marcus J. Dortch, PharmD, BCPS, FCCM
Mehrnaz Hadian, MD, MS, FCCM
Yi-Chen Lai, MD
Mark Edwin Nunnally, MD, FCCM
David J. Dries, MD, MCCM, MSE
Kaye E. Hale, MD
Manoj Lalu, MD
Paul Alan Nyquist, MD, MPH, FCCM
Michael A. Dubick, PhD
Mark W. Hall, MD, FCCM
David M. Landsberg, MD
Fola Odetola, MD, MPH
Marc J. Dubois, MD
Lisa Hall Zimmerman, PharmD, BCPS,
James R. Langdon, MD
Sandro Vieira De Oliveira, MBA, MD, MS
A. Joseph Layon, MD, FACP
Keith M. Olsen, PharmD, FCCM
Salvador Cruz-Flores, MD, MPH, FAHA,
FCCM
Mark Duffett, MSc, RPh
FCCM
FCCM
MSc
Yves Durandy, MD, PhD
Susan E. Hamblin, PharmD, BCPS
H. Thomas Lee, MD, PhD
James P. Orlowski, MD, FCCM
Stephanie B. Edwin, PharmD
Leslie A. Hamilton, BCPS, PharmD
Jong O. Lee, MD, FACS, FCCM
Dr. Norio Otani, MD
Linda S. Efferen, MBA, MD, FCCM
Raja A. Hanania, RPh, BCPS
Charlene Leonard, ACNP, PCCNP
Charles W. Otto, MD, FCCM
Philip A. Efron, MD, FCCM
Robert W. Hand, MS, FCCM
Klaus-Dieter K. Lessnau, MD
Lavi Oud, MD
Sally A.F. El Sahrigy, MD
Sheila J. Hanson, MD
Jennifer L. LeTourneau, DO, MCR, FACP
Yves Ouellette, MD, PhD
Evert A. Eriksson, MD, FACS
Reza Seyed Mohammad Hashemian,
Andrew Levinson, MD, MPH
Christopher Paciullo, BCPS, PharmD
Jennifer L. Liedel, MD
Sheela Pai Cole MD
Raffo Escalante, MD
MD, FCCM
Mario E. Eyzaguirre, MD
Kevin W. Hatton, MD
Pamela A. Lipsett, MD, MHPE, FCCM
Charu Paranjape, MD
Barbara E. Faircloth, PharmD
Gabriel J. Hauser, MD, FCCM
Matthew E. Lissauer, MD
Linda A. Park, BCPS, PharmD
P Jane Faris, BCPS, PharmD
Stephen O. Heard, MD, FCCM
Patricia R. Louzon, PharmD, BCPS
Margaret M. Parker, MD, MCCM
Megan Farraj, PharmD
Alan C. Heffner, MD
Lia H. Lowrie, MD
Melissa J. Parker, MD, MS
Nadia Ferguson, BCPS, PharmD
Jorge Luis Hidalgo, MD, MACP, FCCM
Robert E. Lynch, MD, PhD, FCCM
Robert I. Parker, MD
Christopher K. Finch, BCPS, FCCM
Archana P. Hinduja, MD
Elizabeth H. Mack
Stephen M. Pastores, MD, FCCM
Ericka L. Fink, MD
Hitoshi Hirose, MD, PhD
Robert MacLaren, MPH, PharmD, FCCM
Namrata Patil, MD, MPH
Kevin Finkel, MD, FCCM
Tudy Hodgman, PharmD, BCPS, FCCM
Ivan L. Maldonado, MD, FCCM
Herbert Patrick, MD, MSEE, FCCM
Jeff J. Fletcher, MD, MS
Meredith Hollinger, BCPS, PharmD
Mark A Malesker, BCPS, PharmD, FCCP
Thomas E. Paulson, MD
Jeffrey J. Fong, PharmD
Caron M. Hong, MD
Fern M. Malila, BSN, MS
Ronald G. Pearl, MD, PhD, FCCM
Michael L. Forbes, MD, FAAP, FCCM
Jane Marie Hughes, PharmD, BCNSP
Dr. Jihad Mallat, MD
Daleen Aragon Penoyer, PhD, RN, CCRP,
Daniel G. Ford, PharmD
Jimmy W. Huh, MD
Nikolaos Maniatis, MD
James D. Fortenberry, MD, MCCM
David F. Hunt, MD
Janice E. Manjuck, MD
Toni M. Petrillo-Albarano, MD, FCCM
Michael A. Frakes, CCRN, CNS, MS, RN
Lynn J. Hydo, MBA, RN, FCCM
Christopher W. Mastropietro, MD, MD
Nga B. Pham, MD, FAAP
Yaakov Friedman, MD
Robert C. Hyzy, MD, Professor, FCCM
John E. Mazuski, MD, PhD, FCCM
Tam N. Pham, MD
Stuart Howard Friess, MD
Eiji Isotani, MD, PhD
Karen McAllen, PharmD, FCCM
Christina M. Phelps, MD
Brian Fuller, MD, MSc
Judith Jacobi, BCPS, PharmD, FCCM
Kevin W. McConnell, MD
Louisdon Pierre, MD, MBA, FCCM
Andrea Gabrielli, MD, FCCM
Michael Luke James, MD
Kari Anne McCracken, BCPS, PharmD
Murray M. Pollack, MD, MCCM, MBA
Samuel M. Galvagno, DO, MS, PhD
Mouhamad G. Jamil, MD
Barbara McLean, ACNP, CCRN, FCCM
Dr. Vivekananthan Poogavanam, MD
Ricardo Luis Garcia-De Jesus, MD
Randeep S. Jawa, MD, FCCM
Wesley D. McMillian, BCPS, PharmD,
Marc J. Popovich, MD, FCCM
Jeremy S. Garrett, MD
Xiaofeng Jia, MD, MS, PhD
Rainer G. Gedeit, MD
Victor C. Joe, MD, FACS
Nathaniel McQuay, Jr., MD, FACS
Heitor P. Povoas, MD
Douglas M. Geehan, MD, FCCM
Peter N. Johnson, BCPS, PharmD
Shivanand Medar, MD
Karen S. Powers, MD, FCCM
FCCM
FCCM
David T. Porembka, DO, FCCM
Donald S. Prough, MD
Ava M. Puccio, PhD
Tyler Putnam, II, MD, FCCM
Sadeq A. Quraishi, MD, MD, MHA, MMSc
Jean-Sebastien Rachoin, MD
Patricia A. Radovich, CNS, PhD, RN, FCCM
Hamideh Raeisi, ACNP, MSN
Venkatakrishna Rajajee, MD
Joseph F. Rappold, MD
Robert S. Ream, MD
Kyle Rehder, MD
Mohammed F. Rehman, DO
Harvey S. Reich, MD, FACP FCCP
Roger W. Reichenbach, RRT, BS
Marc G. Reichert, PharmD, BCPS
Maggy Riad, MD
Michael Rie, MD
Mark R. Rigby, MD, PhD, FCCM
Dr. Giuseppe Ristagno, MD
Emanuel P. Rivers, BS, MD, MPH, IOM
Pamela R. Roberts, MD, FCCM
Russel J. Roberts, PharmD
Michael Rodgers
William Rodriguez-Cintron, MD, FCCM
Gloria M. Rodriguez-Vega, MD, FCCM
Jamie M. Rosini, PharmD
Alan Roth, MBA, MS, RRT, FAARC
Alexandre T. Rotta, MD, FAAP, FCCM
Ranna A. Rozenfeld, MD, FCCM
Kelli Rumbaugh, PharmD
Leif Saager, MD, FCCP
Farid Sadaka, MD
Nicholas Sadovnikoff, MD, FCCM
Nahel N. Saied, MD, MB, BCh
Javier L. Sanchez, MD
Richard H. Savel, MD, FCCM
Miren A. Schinco-Schaffer, MD, FCCM
Charles L. Schleien, MD, MBA, FCCM
David M. Schreck, MD, MS
Kevin M Schuster, MD, FCCM
Elizabeth A. Scruth, CCRN, CNS, PhD, FCCM
David B. Seder, MD, FCCM
Hariharan Seetharaman, MD, FCCM
Edward G. Seferian, MD, MS
Aleksander Shalshin, MD
David Scott Shapiro, MD, FCCM
Michael GS Shashaty, MD
David K. Shellington, MD
Hsiu-Nien Shen, MD
Eric K. Shepard, MD, FCCM
Joseph R. Shiber, MD, FCCM
Lori A. Shutter, MD, FNCS, FCCM
Peter C. Silver, BA, MD, FCCM
Balwinder Singh, MD, MS
Neil M. Skjodt, MD, MSc FRCP(C) D
Todd L. Slesinger, MD, FCCM
Norma Michelle Smalls-Mantey, MD,
FCCM
Lincoln S. Smith, MD
Sean G. Smith, BS, BSN, CCRN, RN
Pamela L. Smithburger, MS, PharmD, BCPS
Guy W. Soo Hoo, MD
Lauren R. Sorce, ACNP, CCRN, FCCM
Ben Speelberg, MD, PhD
Charles L. Sprung, MD, MCCM, JD
Vijay Srinivasan, MD
Neeraj Srivastava, MD
Jana A. Stockwell, MD, FCCM
John P. Straumanis, MD, FCCM
Erik Su, MD
Maja Surbatovic, MD, PhD
Alexander O. Sy, MBA, MD, FCCP, FACP
James E. Szalados, MBA, MD, FCCM
Danny M. Takanishi, Jr., MD
Oleg Tarabrin
M. Hossein Tcharmtchi, MD
Ken Tegtmeyer, MD, FAAP, FCCM
Ravi R. Thiagarajan, MD, MPH
Neal J. Thomas, MD, MSc, FCCM
Richard G. Thomas, PharmD, PharmD
Zachariah Thomas, PharmD, BCPS
Dan R. Thompson, MD, MCCM, MA, FACP
Naveen V. Thuramalla, MS
Samuel A. Tisherman, MD, FCCM
Christine C. Toevs, MD, FCCM
Michel Torbey, MD, MPH, FAHA, FCCM
Randi Trope, MD
David A. Turner, MD
Sebastian Ugarte, MD
Aristeidis Vakalos, PhD
Atul Vats, MD, FCCM
Philip A. Verhoef, MD, PhD
Stacy Alan Voils, BCPS, MS, PharmD
Kathryn T. Von Rueden, MS, FCCM
Rade B. Vukmir, MD, JD
Katja E. Wartenberg, MD
Eizo Watanabe, MD, PhD
Charles Weissman, MD
Jason A. Werner, MD
Arthur P. Wheeler, MD
Derek S. Wheeler, MD, FCCM
John J. Whitcomb, CCRN, PhD, RN, FCCM
Craig B. Whitman, BCPS, PharmD
Charles E. Wiles, III, MD, FCCM
Kristine Willett, PharmD
Eric A. Williams, MD
Sharon Wilson, BCPS, PharmD
Arino Yaguchi, MD, PhD
Kuang-Yao Yang, MD, PhD
Siu Yan Amy Yeung, BCPS, PharmD
Mihae Yu, MD
Arno L. Zaritsky, MD
Jack E. Zimmerman, MD, FCCM
Jerry J. Zimmerman, MD, PhD, FCCM
2015 Abstract-Based Awards
2015 ABSTRACT-BASED AWARDS
In-Training Award
6 Melatonin Inhibits Hemorrhagic Shock Induced Fluid Leak and Microvascular Endothelial
Derangements—Katie Wiggins-Dohlvik, Himakarnika Alluir, Chinchusha Anasooya Shaji, Vivayak
Govande, Madhava Beeram, Amin Mohammad, Matthew Davis, Binu Tharakan
Young Investigator Award
3 Mortality Risk Factors with Carbapenem-Resistant Bacteremia: Impact of Combination Therapy—
Stephanie Bass, Elizabeth Neuner, Seth Bauer, Simon Lam
Annual Scientific Awards
19 Epidemiology of Acute Kidney Injury and Fluid Overload in Critically Ill Children—Priyank Yagnik,
Vinai Modem
20 Heterogeneous Treatment Effect of Red Blood Cell Transfusion (RBCT) in the Critically Ill
Patients—Xinggang Liu, Omar Badawi, Christine Franey, Ilene Zuckerman, Craig Lilly
27 Benefits of Levetiracetam After Controlled Cortical Impact in Rats: Studies from the OBTT
Consortium—Megan Browning, Samuel Poloyac, Edward Dixon, Philip Empey, Travis Jackson,
Erik Brockman, Jeremy Henchir, Patrick Kochanek
42 Random Forest Models Separate Vital Sign Events as Real or Artifact in Continuous Monitoring
Data—Marilyn Hravnak, Lujie Chen, Artur Dubrawski, Donghan Wang, Eliezer Bose, Gilles Clermont,
Michael Pinsky
48 Osteopontin Induces Neutrophil Migration in Sepsis-Induced Acute Lung Injury via ERK
Activation—Yohei Hirano, Monowar Aziz, Weng-Lang Yang, Zhimin Wang, Mian Zhou, Mahendar
Ochani, Adam Khader, Ping Wang
49 ICU Outcomes of Physician Assistants and Acute Care Nurse Practitioners Compared to Resident
Teams—Joseph Keller, Harrison Reed, Xiaofeng Wang, Jorge Guzman
63 REWS: Real-time Early Warning Score for Septic Shock—Katharine Henry, Chris Paxton, Kwang
Sik Kim, Julius Pham, Suchi Saria
225 Physiological Monitoring of CPR Quality is Associated with Improved Survival from Cardiac
Arrest—Peter Meaney, Benjamin French, Christopher Parshuram, Stephen Schexnayder, Dana Edelson,
Benjamin Abella, Raina Merchant, Robert Sutton
534 Efficacy of an Erythropoietin? Mimetic Peptide ( ARA290) In Experimental Traumatic Brain
Injury—Leela Cherian, Carlos Estevez-Castillo, Roberto Garcia, Carla Hand, Lamin Mbye, Charles
Minard, J. Clay Goodman, Claudia Robertson
940 Pharmacological Activation of AMPK Improves Cardiac Dysfunction in Experimental Sepsis in
Mice—Yu Inata, Paul Hake, Giovanna Piraino, John Ledford, Christine Schulte, Victoria Moore, Jeanne
James, Basilia Zingarelli
2015 Abstract-Based Awards
Specialty Awards
Administration
1007 Development of Tele-ICU Multidimensional Severity Adjusted PIRO Sepsis Model—Donna
Armaignac, Carlos Valle, Julie Lamoureux, Louis Gidel, Xiaorong Mei, Emir Veledar
Cardiovascular
1 Correlation of CHADS2 with New Onset Atrial Fibrillation in Thoracic and Vascular Surgical
Patients—Kirstin Kooda, Benjamin Dreesman, Ross Dierkhising, James Onigkeit, Arun Subramanian
CPR/Resuscitation
17 Epidemiology And Outcomes Of In-Hospital Cardiac Arrest Across Hospitals Of Varied Center
Volume—Punkaj Gupta, Casey Lauer, Xinyu Tang, Christine Gall, Thomas Rice, Randall Wetzel
Education
13 Teaching Situation Awareness During Cardiac Arrests and Rapid Responses - A Simulation Study—
Akiva Andrew Dym, Carla Venegas-Borsellino, Maneesha Bangar, Dmitry Lisenenkov, Adam Keene,
Lewis Eisen
Endocrine/Nutrition
44 Nutrition Status and Outcomes in Noncardiogenic Acute Respiratory Failure: A Cohort Study—
Kenneth Christopher, James Rawn, Kris Mogensen
Epidemiology/Outcomes
22 Predictors of Home Discharge among Survivors of Necrotizing Fasciitis: A Population-Based
StudyLavi Oud, Phillip Watkins
Ethics/End of Life/Palliative Care
25 Differences in End of Life Care for Intensive Care Unit (ICU) Patients With vs. Without Cancer—
Geoffrey Koff, Edward Len, David Oxman, MD, Urvashi Vaid
GI/Hepatic
410 Proton Pump Inhibitors and the Risk for Hospital-Acquired Clostridium Difficile in ICU Patients—
Jeffrey Barletta, David Sclar
Hematology
45 Acute Respiratory Distress Syndrome Following Hematopoietic Stem Cell Transplantation—
Hermang Yadav, Matthew Nolan, John Bohman, Steve Peters, Rodrigo Cartin-Ceba, Ognjen Gajic,
Daryl Kor
Immunology/Transplant
26 Effect of Steroids Administration on Brain Dead Organ Donors and Recipients: A Systematic
Review—Frederick D'Aragon, Arnav Agarwal, Maureen Meade, Emilie Belley-Cote, Anne Julie Frenette,
Francois Lamontagne, Sonny Dhanani
Infectious Disease
37 Performance of Interleukin 27 as a Sepsis Diagnostic Biomarker in Critically Ill Children—William
Hanna, Hector Wong
Neuroscience
30 The Effect of Aneurysmal Subarachnoid Hemorrhage on Work Productivity—Elizabeth Crago,
Thomas Price, Catherine Bender, Dianxu Ren, Samuel Poloyac, Paula Sherwood
2015 Abstract-Based Awards
Patient and Family Support
32 Giving your patients M.O.R.E: Implementing of a Non-Pharmacologic Protocol to Prevent ICU
Delirium—Ryan Rivosecchi, Sandra Kane-Gill, Shauna Campbell, Sue Svec, Pamela Smithburger
Pharmacology
460 Elevated risk of Thomboembolic Events after Novel Anticoagulation Reversal Protocol—Cassie
Barton, Jon Case, Melissa Ferguson, Nathan Johnson, Gregory Roberti, Jason Zimmerman, Wesley
McMillian, Martin Schreiber
Professional Development
324 Transition to First Job: An In Training Section Research Survey—Laura Watkins, Krzysztof
Laudanski
Pulmonary
46 Chylothorax is Associated with an Increased Risk of Thrombosis in Adults—Sumedh Hoskote,
Hemang Yadav, Prashant Jagtap, Craig Daniels
Quality and Safety
769 Improving glucose control in Intensive and Intermediate Care units using a Lean Six Sigma
approach—Ian Cohen, Mark Calabretta, Ruth Jamieson-Cohen, Ananda Dharshan, Singh Jatinder,
Bonnie Gleason
Renal
914 Early AKI is Associated with Persistence of Other Organ Dysfunction and Late Death in the
PICU—Lazaro Sanchez-Pinto, Robinder Khemani
Sepsis
59 Effect of Cholecalciferol Supplementation on Vitamin D Status and Cathelicidin in Sepsis—
Sadeq Quraishi, Gennaro DePascale, Joseph Needleman, Carlos Camargo, Jr., Ednan Bajwa, Ishir Bhan
Surgery/Trauma/Burns
1028 Disparity in Trauma and Critical Care for Traumatic Brain Injury in Arizona—Lynn Munoz, Irada
Ibrahim-zada, Terence O'Keeffe, Randall Friese, Peter Rhee
Research Citation Finalists
101 Pharmacokinetics of Micafungin in Plasma and Burn Eschares in Critically Ill Burned Patients—
Maria Jose Asensio, Manuel Sanchez, Beatriz Galván, Eva Herrero, Lucia Cachafeiro, Alexander
Agrifolio, Sonia Luque, Abelardo Garcìa-de-Lorenzo
102 Adherence to Guidelines Based Antibiotic Therapy in the Treatment of Community Acquired
Pneumonia—Mahmoud Nour, Ayman Gaber, Mohamed Momtaz
103 Evaluation of Sepsis Treatment Outcomes in Port-au-Prince, Haiti—Alfred Papali, Marc Augustin,
Lovely Colas, Carl Jean-Francois, Avelino Verceles, Nevins Todd
104 A Potential Novel Role for Olfactomedin 4 in Sepsis—Matthew Alder, Patrick Lahni, Hector Wong,
David Hildeman
105 Comparing Accuracy of 2 Phases of a Pediatric Electronic Severe Sepsis Screening Algorithm—
Peter Michael Mangubat, Samir Shah
2015 Abstract-Based Awards
106 Does PICC Insertion in Bacteremic Patients Increase CLABSI Rate?—F. Maguire, Russell Acevedo,
David Landsberg, Daniel Polacek, Todd Olrich, David Martin, Lynette Johnson
107 Combining EEG and Serum Brain Biomarkers to Classify Mortality after Pediatric Cardiac
Arrest—Katherine Anetakis, Satyanarayana Gedela, Patrick Kochanek, Yoshimi Sogawa, Ericka Fink
108 The Role of Branched Chain Amino Acids in the Functional Recovery From Traumatic Brain
Injury—Matthew Kirschen, Jaclynn Elkind, Miranda Lim, Brendan Putnam, Akiva Cohen
109 Plasma High-Mobility Group Box-1 (HMGB1) Concentration in Pediatric Sepsis and Multi-Organ
Failure—Diana Pang, Ronald Aaron Bola, Alicia Au, Joseph Carcillo, Eric Halstead, Robert Clark,
Rajesh Aneja
110 High-Dose Erythropoietin Improves Survival in a Swine Model of Ventricular Fibrillation—
Raul Gazmuri, Herbert Whitehouse, Vesna Borovnik-Lesjak, Kruti Shah, Alvin Baetiong, Jeejabai
Radhakrishnan
111 Variation of Central Venous Catheter Usage in Three ICUs Managed by the Same Intensivist
Group—Richard Woerndle, Alex Hoyt, John Hoyt
112 Using Indirect Calorimetry Data to Assess the Impact of Sedatives on REE in the ICU—Mary
McCarthy, Janet Fabling, Christopher Poprawski, Cristin Mount
113 Epidemiology and Outcomes of New-Onset Atrial Fibrillation in the ICU: A 6-year Retrospective
Study—Perliveh Carrera, Charat Thongprayoon, Wisit Cheungpasitporn, Vivek Iyer, Teng Moua
114 Validation of the SWIFT Score for Intensive Care Unit (ICU) Readmissions in an Asian
Population—Eric Heymann, Liv Maier, Amartya Mukhopadhyay
115 Cerebral Perfusion Pressure in Patients Undergoing Hypothermia after Cardiac Arrest—Fabio Silvio
Taccone, Katia Donadello, Antonio Dell'Anna, Sabino Scolletta, Jean-Louis Vincent
116 Ceftazidime-avibactam Tested Against Gram-Negative Bacteria From Intensive Care Unit (ICU)
Patients—Helio Sader, Mariana Castanheira, David Farrell, Robert Flamm, Rodrigo Mendes
117 Impact of Macrolide Antibiotics on Outcomes in ICU Patients with Acute Exacerbations of
COPD—Tyree Kiser, Richard Allen, Kavita Nair, R. Vandivier
118 Prehospital Hypotension Correlates with Injury Severity and Outcomes—Clayton Damme, Jiangtao
Luo, Keely Buesing
119 The Evaluation of Cerebral Function after Hypothermia in a Pig Model of CPR—Ziren Tang,
Peng Peng, Jiang Tao, Ping Gong, Wanchun Tang
120 Patterns of Deterioration in Hospitalized Pediatric Oncology Patients Requiring ICU Admission—
Asya Agulnik, Peter Forbes, Nicole Stenquist, Carlos Rodriguez-Galindo, Monica Kleinman
2015 Abstract-Based Awards
121 Feasibility of a Non-Invasive Sensor for Measuring ICU Patient Mobility—Andy J Ma, Andong
Zhan, Gunnar Sigurdsson, Nishi Rawat, Dale Needham, Suchi Saria
122 Culture Algorithm to Reduce Urine Culture and Catheter-Associated Urinary Tract Infection
Rates—Ashok Cattamanchi, Lindsay Stevenson, Priscilla Jang, Laith Altaweel, Svetolik Djurkovic, Nitin
Puri, Sujata Ambardar, Jason Vourlekis
123 Pediatric Procedural Sedation Using Dexmedetomidine: Provider Specialty and Complication
Rates—Carmen Sulton, Courtney McCracken, Kiran Hebbar, Harold Simon, Jason Reynolds, Joseph
Cravero, Pradip Kamat
124 Predictors of PTSD and Depression among Family and Friends of Patients Admitted To the ICU—
Ann Marie Warren, Megan Reynolds, Monica Bennett, Michael Foreman, Evan Rainey, Rebecca Weddle
125 Use of a Pediatric Traumatic Brain Injury Pathway Is Associated With Improved Outcomes—
Natalie Tillman, Wei Dong, Andrew Reisner, Tracie Walton, Karen Walson, Toni Petrillo-Albarano, Joshua
Chern, Atul Vats
126 Glycemic Variability With Temperature Changes During Therapeutic Hypothermia After Cardiac
Arrest—Krystal Haase, Jennifer Grelle, Faisal Khasawneh, Chiamaka Ike
127 In-Hospital Arrests, Anoxic/Hypoxic Ischemic Encephalopathy, And G Tube/Tracheostomy
Estimates—Veerajalandhar Allareddy, Sankeerth Rampa, Romesh Nalliah, Karen Lidsky, Veerasathpurush
Allareddy, Alexandre Rotta
128 Pediatric Delirium Prevalence and Motoric Subtypes in Critically Ill Infants and Young Children—
Christina Goben, Maalobeeka Gangopadhyay, Mary Hamilton Chestnut, Natalie Jacobowski, Catherine
Fuchs, E. Wesley Ely, Pratik Pandharipande, Heidi Smith
129 Family Presence During Tracheal Intubations in Pediatric ICUs—Ronald Sanders, G. Bysani,
Margaret Parker, Sholeen Nett, Vinay Nadkarni, Akira Nishisaki
130 Post-Resuscitation Reduction of Hepatic Microcirculation Reflects Cardiac but Not Liver
Dysfunction—Jie Qian, Shen Zhao, Jiangang Wang, Ping Gong, Zhengfei Yang, Xiaobo Wu, Jena
Cahoon, Wanchun Tang
Editorial Board
Critical Care Medicine
EDITOR-IN-CHIEF
ASSOCIATE EDITORS
Joseph E. Parrillo, MD, MCCM
Edwin A. Deitch, MD, FACS
Professor of Medicine
Chairman, Heart and Vascular Hospital
Hackensack University Medical Center
Hackensack, New Jersey
USA
Professor and Chairman
Department of Surgery
University of Medicine and Dentistry
of New Jersey Medical School
Newark, New Jersey
R. Phillip Dellinger, MD, MCCM
Mitchell P. Fink, MD, MCCM
Lynn J. Retford
Editorial Assistant:
Bethany Fresen
Editorial Associates:
Lin Rizzuto
Delphine Sayeed
SCCM
500 Midway Drive
Mount Prospect, IL 60056
Phone: (847) 827-6869
Fax: (847) 827-6886
E-mail: journals@sccm.org
www.sccm.org
NEUROLOGIC CRITICAL CARE
SENIOR EDITOR
SCIENTIFIC EDITORS
Director of Publications:
Professor, Anesthesiology and Pediatrics
Phoenix Children’s Hospital
Phoenix, Arizona
Henry Masur, MD, FCCM
Professor, Pediatrics
State University of New York
at Stony Brook
Stony Brook, New York
Sophie M. Tosta
Murray M. Pollack, MD, FCCM
Thomas P. Bleck, MD, FCCM
Margaret M. Parker, MD, MCCM
Managing Editor:
PEDIATRIC CRITICAL CARE
Professor, Medicine
Section of Critical Care Medicine
Cooper Health System
Camden, New Jersey
Chief, Critical Care Medicine Department
NIH-Clinical Center, NIH
Clinical Professor of Medicine
George Washington University
School of Medicine
Attending Physician, Washington
Hospital Center
Washington, D.C.
EDITORIAL OFFICE
SECTION EDITORS
Ronald Reagan University of California
Los Angeles Medical Center
Los Angeles, California
Patrick M. Kochanek, MD, MCCM
Vice Chairman, Department of Critical
Care Medicine
Director, Safar Center for Resuscitation
Research
University of Pittsburgh School of Medicine
and Children’s Hospital of Pittsburgh of
UPMC
Pittsburgh, Pennsylvania
Neil R. MacIntyre, MD
Professor, Medicine
Duke University Medical Center
Durham, North Carolina
Donald S. Prough, MD
Professor and Chairman
Department of Anesthesiology
University of Texas Medical Branch at Galveston
Galveston, Texas
Professor
Rush Medical College
Chicago, Illinois
Jean-Louis Vincent, MD, PhD, FCCM
Professor, Intensive Care
Erasme University Hospital
Brussels, Belgium
BOOK REVIEW EDITOR
Jerry J. Zimmerman, MD, PhD, FCCM
Director, Pediatric Critical Care Medicine
Seattle Children’s Hospital
University of Washington
Seattle, Washington
EDITOR EMERITUS
Bart Chernow, MD, FCCM
FOUNDING EDITOR
William C. Shoemaker, MD, MCCM
CONCISE DEFINITIVE
REVIEW SERIES EDITOR
Jonathan E. Sevransky, MD, MHS, FCCM
Director, Medical ICU
Emory University Hospital
Assistant Director for Medicine
Emory Center for Critical Care
Atlanta, Georgia
EDITORIAL BOARD
MEMBERS
Department of Surgery
Emory University School of Medicine
Atlanta, Georgia
Edward Abraham, MD, FCCM
Joseph A. Carcillo, MD
Professor and Dean
Wake Forest School of Medicine
Winston-Salem, North Carolina
Hasan B. Alam, MD, FACS
Professor, Critical Care Medicine and Pediatrics
Children’s Hospital of Pittsburgh of UPMC
University of Pittsburgh School of Medicine
Pittsburgh, Pennsylvania
Professor of Surgery
Harvard Medical School
Program Director, Surgical Critical
Care Fellowship Program
Massachusetts General Hospital
Boston, Massachusetts
Davide Chiumello, MD
Theodore A. Alston, MD, PhD
David A. Cook, FANZCA, FCICM, PhD
Department of Anesthesia, Critical Care,
and Pain Medicine
Massachusetts General Hospital
Harvard Medical School
Boston, Massachusetts
John H. Arnold, MD
Dipartimento di Anestesia, Rianimazione
Emergenza Urgenza
Fondazione IRCCS Ca’ Granda
Ospedale Maggiore Policlinico
Milan, Italy
Professor of Anaethesia and Critical Care
University of Queensland
Princess Alexandra Hospital
Brisbane, Queensland, Australia
Craig Coopersmith, MD, FCCM
Associate Professor, Anaesthesia (Pediatrics)
Harvard Medical School
Boston, Massachusetts
Professor of Surgery
Emory Center for Critical Care
Emory University School of Medicine
Atlanta, Georgia
Philip S. Barie, MD, MBA, FCCM
Douglas B. Coursin, MD
Anish Bhardwaj, MD, MBA, CPE,
FAHA, FCCM
Elliott Crouser, MD
Professor of Surgery and Public Health
Weil Cornell Medical College
New York, New York
Chairman, Department of Neurology
John Sealy Chair of Neurology
Professor of Neurology, Neurosurgery,
Neuroscience and Cell Biology
Assistant Dean for Faculty Affairs
University of Texas Medical Branch
Galveston, Texas
Luca Bigatello, MD
Director, Surgical Critical Care
St. Elizabeth’s Medical Center
Professor of Anesthesiology
Tufts University School of Medicine
Boston, Massachusetts
Bruce R. Bistrian, MD, MPH, PhD
Professor of Medicine
Beth Israel Deaconess Medical Center
Harvard Medical School
Boston, Massachusetts
Roy G. Brower, MD
Professor of Medicine
Johns Hopkins University
School of Medicine
Baltimore, Maryland
Timothy G. Buchman, PhD,
MD, MCCM
Professor of Surgery
Professor, Anesthesiology and Medicine
University of Wisconsin School of Medicine
and Public Health
Madison, Wisconsin
Associate Professor of Medicine
Division of Pulmonary and Critical
Care Medicine
Director, Medical Intensive Care Unit
University Hospital East
Associate Director, Center for Critical Care
Ohio State University Medical Center
Columbus, Ohio
Mary Dahmer, PhD
Associate Professor of Pediatrics
and Communicable Diseases
Division of Pediatric Critical Care Medicine
University of Michigan Health System
Ann Arbor, Michigan
Marion Danis, MD
Chief, Bioethics Consultation Service
Head, Section of Ethics and Health Policy
Department of Bioethics
National Institutes of Health
Bethesda, Maryland
Joseph F. Dasta, MSc (PharmD),
FCCM, FCCP
Professor Emeritus
Ohio State University
Austin, Texas
Adjunct Professor of Pharmacy
University of Texas College of Pharmacy
Austin, Texas
Bennett deBoisblanc, MD
Fred Allison, Jr, MD Professor of Medicine
and Physiology
Section of Pulmonary/Critical Care Medicine
LSU Health Sciences Center, New Orleans
New Orleans, Louisiana
Clifford S. Deutschman, MS, MD, FCCM
Professor of Anesthesiology and Critical Care
Perlman School of Medicine at the
University of Pennsylvania
Philadelphia, Pennsylvania
John W. Devlin, PharmD, FCCM, FCCP
Professor, Department of Pharmacy Practice
Bouve College
Northeastern University
Special and Scientific Staff
Division of Pulmonary, Critical Care
and Sleep Medicine
Critical Care Pharmacist
Tufts Medical Center
Boston, Massachusetts
Todd Dorman, MD
Associate Dean and Director
Vice Chair, Critical Care
Associate Professor
Department of Anesthesiology/Critical Care
Medicine/Surgery
The Johns Hopkins University School
of Medicine
Baltimore, Maryland
David J. Dries, MSE, MD, MCCM
Assistant Medical Director for Surgical Care
Health Partners Medical Group,
Regions Hospital
Professor of Surgery and Anesthesiology
University of Minnesota
Saint Paul, Minnesota
Jay L. Falk, MD, FCCM
Clinical Professor of Medicine and
Emergency Medicine
University of Florida College of Medicine
Vice-President, Medical Education
Orlando Regional Healthcare
Orlando, Florida
J. Christopher Farmer, MD, FCCM
Professor and Chair
Department of Critical Care Medicine
Mayo Clinic
Phoenix, Arizona
Laurent G. Glance, MD
Professor and Vice Chairman for Research
Department of Anesthesiology
University of Rochester School of Medicine
Rochester, New York
Roy D. Goldfarb, PhD
Department of Medicine
Section of Cardiology
Cooper University Hospital
Camden, New Jersey
Editorial Board
A. B. Johan Groeneveld, MD, PhD,
FCCP, FCCM
Professor of Intensive Care
Erasmus MC
Rotterdam, The Netherlands
Jesse Hall, MD
Professor of Medicine, Anesthesia and
Critical Care
University of Chicago Hospitals
The Pritzker School of Medicine
Chicago, Illinois
Neil A. Halpern, MD, MCCM
Professor, Anesthesiology and Medicine
Weil Medical College of Cornell University
Chief, Critical Care Medicine
Memorial Sloan Kettering Cancer Center
New York, New York
Maurene A. Harvey, RN, MPH, MCCM
Critical Care Educator and Consultant
Glenbrook, Nevada
Mark A. Helfaer, MD, FCCM
Professor, Anesthesiology and Critical Care,
Pediatrics and Nursing
University of Pennsylvania School of Medicine
Philadelphia, Pennsylvania
Thomas L. Higgins, MD, MCCM
Professor of Medicine, Surgery,
and Anesthesiology
Tufts University School of Medicine
Vice-Chairman of Clinical Affairs
Department of Medicine
Baystate Medical Center
Springfield, Massachusetts
Steven M. Hollenberg, MD, FCCM
Professor of Medicine
Cooper Medical School of Rowan University
Camden, New Jersey
Judith Jacobi, PharmD, FCCM, BCPS
Critical Care Pharmacy Specialist
Indiana University Health Methodist Hospital
Indianapolis, Indiana
Marc G. Jeschke, MD, PhD, FACS,
FCCM, FRCSC
Director, Ross Tilley Burn Centre
Sunnybrook Health Sciences Centre
Senior Scientist
Sunnybrook Research Institute
Associate Professor
Department of Surgery, Division
of Plastic Surgery
Department of Immunology
Toronto, Ontario, Canada
Robert M. Kacmarek, PhD, FCCM
Professor of Anesthesiology
Harvard Medical School
Director of Respiratory Care
Massachusetts General Hospital
Boston, Massachusetts
Critical Care Medicine
Sandra L. Kane-Gill, PharmD,
MSc, FCCM
Michael S. Niederman, MD, FCCM
Associate Professor
University of Pittsburgh
School of Pharmacy and Clinical Translational
Science Institute
Pittsburgh, Pennsylvania
Professor of Medicine
State University of New York
at Stony Brook
Chairman, Department of Medicine
Winthrop-University Hospital
Mineola, New York
Niranjan “Tex” Kissoon, MD
John M. Oropello, MD, FCCM
Professor in Critical Care Medicine—
Global Child Health
British Columbia Children’s Hospital
University of British Columbia
Vancouver, British Columbia, Canada
Ruth M. Kleinpell, PhD, RN, FCCM
Director, Center for Clinical Research
and Scholarship
Rush University Medical Center
Professor
Rush University College of Nursing
Nurse Practitioner
Mercy Hospital and Medical Center
Chicago, Illinois
Marin H. Kollef, MD
Virginia E. and Sam J. Golman Chair
in Respiratory Intensive Care Medicine
Professor of Medicine
Division of Pulmonary and Critical Care
Medicine
Washington University School of Medicine
Director, Critical Care Research
Director, Respiratory Care Services
Barnes-Jewish Hospital
St. Louis, Missouri
George C. Kramer, PhD
Professor, Department of Anesthesiology
and Physiology
Director, Resuscitation Research Laboratory
University of Texas Medical Branch, Galveston
Galveston, Texas
Matthias Majetschak, MD, PhD
Associate Professor
Departments of Surgery and Molecular
Pharmacology and Therapeutics
Loyola University Chicago
Stritch School of Medicine
Maywood, Illinois
John J. Marini, MD
Professor, Medicine
University of Minnesota–St. Paul
Saint Paul, Minnesota
Georg Mols, MD
Program Director, Critical Care Medicine
Icahn School of Medicine at Mount Sinai
New York, New York
Luis Ostrosky-Zeichner, MD, FACP, FIDSA
Professor of Medicine and Epidemiology
University of Texas Medical School of Houston
Houston, Texas
Robert I. Parker, MD
Professor and Vice Chairman for Academic Affairs
Director, Pediatric Hematology/Oncology
Department of Pediatrics
Associate Director
Stony Brook University Cancer Center
State University of New York at Stony Brook
School of Medicine
Stony Brook, New York
David T. Porembka, DO, FCCM
Professor of Surgery and Anesthesiology
Case Western Reserve University School
of Medicine
MetroHealth Medical Center
Cleveland, Ohio
Kenneth G. Proctor, PhD
Professor of Surgery and Anesthesiology
Divisions of Trauma and Surgical
Critical Care
Daughtry Family Department of Surgery
University of Miami Miller School of
Medicine
Miami, Florida
Krishnan Raghavendran, MD
Associate Professor of Surgery
University of Michigan
Ann Arbor, Michigan
Richard A. Proctor, MD
Emeritus Professor
Departments of Medicine and Medical
Microbiology/Immunology
University of Washington School of
Medicine and Public Health
Madison, Wisconsin
Department Head
Department of Anaesthesia and Critical
Care Medicine
Hospital Lahr-Ettenheim,
Lahr, Germany
Stanley H. Rosenbaum, MA, MD
Stanley A. Nasraway, MD, FCCM
Kathy L. Ryan, PhD
Professor of Surgery, Medicine, and Anesthesia
Tufts University School of Medicine
Boston, Massachusetts
Professor of Anesthesiology, Internal
Medicine and Surgery
Yale University School of Medicine
New Haven, Connecticut
Research Physiologist
U. S. Army Institute of Surgical Research
Fort Sam Houston, Texas
Richard H. Savel, MD, FCCM
Professor of Clinical Medicine and Neurology
Albert Einstein College of Medicine
Bronx, New York
Andrew Shorr, MD
Associate Professor of Medicine
Washington Hospital Center
Washington, DC
Mark D. Siegel, MD, FCCP, FACP
Professor of Internal Medicine
Pulmonary, Critical Care, and Sleep
Medicine
Co-Chair, Bioethics Committee
Yale-New Haven Hospital
Program Director
Traditional Internal Medicine Residency
Yale University School of Medicine
New Haven, Connecticut
Zoltan Spolarics, MD, PhD
Professor, Department of Surgery
University of Medicine and Dentistry
of New Jersey Medical School
Newark, New Jersey
Charles L. Sprung, MD, JD, MCCM
Professor of Medicine and Critical
Care Medicine
Hadassah Hebrew University
Medical Center
Jerusalem, Israel
Paul Steendijk, PhD
Associate Professor of Cardiovascular
Physiology
Department of Cardiology
Leiden University Medical Center
Leiden, The Netherlands
Wolfgang Steudel, MD
Newton, Massachusetts
Daniel Talmor, MD, FCCM
Department of Anesthesia, Critical Care,
and Pain Medicine
Beth Israel Deaconess Medical Center
Associate Professor of Anesthesia
Harvard Medical Center
Boston, Massachusetts
Wanchun Tang, MD, MCCM
Professor, President, and Chief Scientific Officer
Weil Institute of Critical Care Medicine
Clinical Professor of Anesthesiology
Keck School of Medicine of the University
of Southern California
Rancho Mirage, California
Richard Teplick, MD
Theodore, Alabama
Samuel Tisherman, MD, FCCM
Professor
Departments of Critical Care Medicine
and Surgery
University of Pittsburgh School of Medicine
Pittsburgh, Pennsylvania
Antoni Torres, MD, PhD
Professor of Medicine
University of Barcelona
Hospital Clinic of Barcelona
Ciber, Idibaps
Barcelona, Spain
Luis Ulloa, PhD
Associate Professor
University of Medicine and Dentistry
of New Jersey Medical School
Newark, New Jersery
Paul M. Vespa, MD, FCCM
Director of Neurocritical Care
Professor of Neurosurgery and Neurology
University of California Los Angeles
Geffen School of Medicine
Los Angeles, California
Robert J. Weber, PharmD, MD,
BCPS, FSHP, FNAP
Senior Director of Pharmaceutical Services
Wexner Medical Center at the Ohio State
University
Assistant Dean
Ohio State University College of Pharmacy
Columbus, Ohio
Robert A. Weinstein, MD
Chairman, Department of Medicine
Cook County Health and Hospital Systems
Chief Operating Officer
Ruth M. Rothstein CORE Center
The C. Anderson Hedberg, MD
Professor of Internal Medicine
Rush Medical College
Chicago, Illinois
Lawrence S. Weisberg, MD
Professor of Medicine
Cooper Medical School of Rowan University
Head, Division of Nephrology
Cooper University Hospital
Camden, New Jersey
Michaela A. West, MD, PhD, FCCM
Professor of Surgery
University of California San Francisco
San Francisco, California
Martin Westphal, MD, PhD
Department of Anesthesiology, Intensive Care,
and Pain Medicine
University of Muenster
Muenster, Germany
Marya Zilberberg, MD, MPH, FCCP
President and CEO
Evi Med Research Group, LLC
School of Public Health and Health Sciences
University of Massachusetts
Worcester, Massachusetts
SOCIETY OF CRITICAL CARE MEDICINE
44TH CRITICAL CARE CONGRESS
PHOENIX, ARIZONA
JANUARY 17–21, 2015
ORAL PRESENTATIONS
Oral Abstract Session: Acute Care Surgery
PUBLISHING NUMBER
1 CORRELATION OF CHADS2 WITH NEW ONSET ATRIAL FIBRILLATION IN THORACIC AND
VASCULAR SURGICAL PATIENTS
2 FLUID OVERLOAD COSTS IN CARDIOVASCULAR PATIENTS: ARE SMALL VOLUME INFUSIONS
A PROACTIVE SOLUTION?
3 MORTALITY RISK FACTORS WITH CARBAPENEM-RESISTANT BACTEREMIA: IMPACT OF
COMBINATION THERAPY
4 RCT OF CHLORHEXIDINE VS. SOAP & WATER BATHING FOR PREVENTION OF HOSPITALACQUIRED INFECTIONS IN SICU
5 IMMUNOMODULTAING DIET CONTANING WHEY PROTEIN AND EPA SUPPRESSED REACTIVE
OXYGEN SPECIES PRODUCTION
6 MELATONIN INHIBITS HEMORRHAGIC SHOCK INDUCED FLUID LEAK AND
MICROVASCULAR ENDOTHELIAL DERANGEMENTS
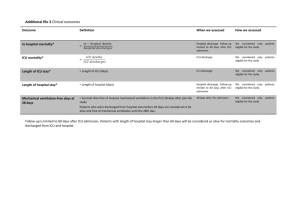
7 PHYSICAL THERAPY CONSULTATION AND ITS EFFECT ON SURGICAL TRAUMA ICU LENGTH
OF STAY.
8 SIMPLE, RELIABLE SEPSIS SCREENING TOOL IMPROVES MORTALITY IN TRAUMA PATIENTS
Oral Abstract Session: CPR/Resuscitation
PUBLISHING NUMBER
9 ADAMTS13 IS ASSOCIATED WITH NEUROLOGICAL OUTCOME IN PATIENTS WITH OUT-OFHOSPITAL CARDIAC ARREST
10 CPR IN ADULT PATIENTS UNDERGOING MAJOR SURGICAL PROCEDURES IN USA: PROFILE
AND PREDICTORS.
11 LOWER OXYGEN CONCENTRATION REDUCED SYSTEMIC INFLAMMATORY RESPONSE AND
IMPROVED THE OUTCOME OF CPR
12 PRO-INFLAMMATORY CYTOKINES ARE ELEVATED IN THE RAT HIPPOCAMPUS DURING
CARDIOPULMONARY RESUSCITATION
13 TEACHING SITUATION AWARENESS DURING CARDIAC ARRESTS AND RAPID RESPONSES - A
SIMULATION STUDY
14 VIDEO LARYNGOSCOPY IMPROVES ODDS OF FIRST ATTEMPT SUCCESS AT INTUBATION IN
THE INTENSIVE CARE UNIT
15 ZONIPORIDE COMBINED WITH-MNE OPTIMIZES THE HEMODYNAMIC EFFICACY OF CHEST
COMPRESSION
16 CENTRAL VENOUS PRESSURE: IS IT AN ACCURATE REFLECTION OF INTRAVASCULAR
VOLUME STATUS?
Oral Abstract Session: Epidemiology
PUBLISHING NUMBER
17 EPIDEMIOLOGY AND OUTCOMES OF IN-HOSPITAL CARDIAC ARREST ACROSS HOSPITALS
OF VARIED CENTER VOLUME
18 ADR SURVEILLANCE USING A MULTICENTER CLINICAL DATABASE: PROPOFOL RELATED
INFUSION SYNDROME INCIDENCE
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
19 EPIDEMIOLOGY OF ACUTE KIDNEY INJURY AND FLUID OVERLOAD IN CRITICALLY ILL
CHILDREN
20 HETEROGENEOUS TREATMENT EFFECT OF RED BLOOD CELL TRANSFUSION (RBCT) IN THE
CRITICALLY ILL PATIENTS
21 HOSPITALIZATIONS & OUTCOMES ATTRIBUTED TO EPIDERMAL NECROLYSIS IN USA:
PREDICTORS OF MORTALITY
22 PREDICTORS OF HOME DISCHARGE AMONG SURVIVORS OF NECROTIZING FASCIITIS: A
POPULATION-BASED STUDY
23 THE OBESITY PARADOX IS NOT OBSERVED IN CRITICALLY ILL PATIENTS ON EARLY
ENTERAL NUTRITION
24 EPIDEMIOLOGIC FEATURES AND OUTCOME OF SEPSIS IN NEUROLOGIC INTENSIVE CARE
UNIT PATIENTS
Oral Abstract Session: Neuroscience
PUBLISHING NUMBER
25 DIFFERENCES IN END OF LIFE CARE FOR ICU PATIENTS WITH VS. WITHOUT CANCER
26 EFFECT OF STEROIDS ADMINISTRATION ON BRAIN DEAD ORGAN DONORS AND
RECIPIENTS: A SYSTEMATIC REVIEW
27 BENEFITS OF LEVETIRACETAM AFTER CONTROLLED CORTICAL IMPACT IN RATS: STUDIES
FROM THE OBTT CONSORTIUM
28 PLATELET DYSFUNCTION ON THROMBOELASTOGRAM IS ASSOCIATED WITH INCREASED
MORTALITY IN HEAD TRAUMA
29 SEIZURES AND STATUS EPILEPTICUS EXACERBATE VENTRICULAR INSTABILITY IN
CHILDREN WITH EPILEPSY
30 THE EFFECT OF ANEURYSMAL SUBARACHNOID HEMORRHAGE ON WORK PRODUCTIVITY
31 TRAUMATIC BRAIN INJURY LEADS TO ALTERED BRAIN DRUG TRANSPORTER EXPRESSION
32 GIVING YOUR PATIENTS M.O.R.E: IMPLEMENTING OF A NON-PHARMACOLOGIC PROTOCOL
TO PREVENT ICU DELIRIUM
Oral Abstract Session: Pediatrics
PUBLISHING NUMBER
33 ACCURATELY IDENTIFYING DEGREE OF LUNG INJURY IN PEDIATRIC ACUTE RESPIRATORY
DISTRESS SYNDROME
34 ALVEOLAR DEAD SPACE FRACTION DISCRIMINATES SURVIVAL IN PEDIATRIC ACUTE
RESPIRATORY DISTRESS SYNDROME
35 DIFFERENTIAL REGULATION OF INFLAMMATORY BIOMARKERS BY
METHYLPREDNISOLONE IN EARLY PEDIATRIC ARDS
36 IMPACT OF KETAMINE COADMINISTRATION DURING DEXMEDETOMIDINE SEDATION FOR
PEDIATRIC MRI.
37 PERFORMANCE OF INTERLEUKIN-27 AS A SEPSIS DIAGNOSTIC BIOMARKER IN CRITICALLY
ILL CHILDREN
38 PHYSIOLOGICAL VARIABLES OF BURN INJURY IN INFANTS: AN OVERVIEW
39 RED BLOOD CELL DISTRIBUTION WIDTH IS ASSOCIATED WITH INCREASED MORTALITY IN
CRITICALLY ILL CHILDREN
40 RICHMOND AGITATION SEDATION SCALE INTER-RATER RELIABILITY IN CRITICALLY ILL
PEDIATRIC PATIENTS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Oral Abstract Session: Pulmonary and Monitoring
PUBLISHING NUMBER
41 FORECASTING CARDIO-RESPIRATORY INSTABILITY IN MONITORED PATIENTS: A MACHINE
LEARNING APPROACH
42 RANDOM FOREST MODELS SEPARATE VITAL SIGN EVENTS AS REAL OR ARTIFACT IN
CONTINUOUS MONITORING DATA
43 VOLUMETRIC CAPNOGRAPHY IN THE ASSESSMENT OF HEMODYNAMIC STATUS IN INFANTS
WITH CARDIAC DISEASE
44 NUTRITION STATUS AND OUTCOMES IN NONCARDIOGENIC ACUTE RESPIRATORY FAILURE:
A COHORT STUDY
45 ACUTE RESPIRATORY DISTRESS SYNDROME FOLLOWING HEMATOPOIETIC STEM CELL
TRANSPLANTATION
46 CHYLOTHORAX IS ASSOCIATED WITH AN INCREASED RISK OF THROMBOSIS IN ADULTS
47 LIPOPOLYSACCHARIDE PRIMES THE INFLAMMASOME BY INCREASING LEVELS OF
IMMUNOREACTIVE NALP3
48 OSTEOPONTIN INDUCES NEUTROPHIL MIGRATION IN SEPSIS-INDUCED ACUTE LUNG
INJURY VIA ERK ACTIVATION
Oral Abstract Session: Quality, Safety, and Outcomes
PUBLISHING NUMBER
49 ICU OUTCOMES OF PHYSICIAN ASSISTANTS AND ACUTE CARE NURSE PRACTITIONERS
COMPARED TO RESIDENT TEAMS
50 A PICU SEDATION PROTOCOL FOR MECHANICALLY VENTILATED PATIENTS NEEDS
SUSTENANCE BEYOND IMPLEMENTATION
51 ARCHETYPING ARTIFACTS IN MONITORED NONINVASIVE VITAL SIGNS DATA
52 ASSOCIATIONS BETWEEN SEDATIVES, VENTILATOR-ASSOCIATED EVENTS, LENGTH OF
STAY, AND MORTALITY
53 BIG DATA, OPEN SOURCE TOOLS, AND CLINICAL DECISION SUPPORT IN A PEDIATRIC ICU
54 COST SAVINGS FROM REAL TIME PRESSURE MAPPING ON HOSPITAL ACQUIRED PRESSURE
ULCERS IN A MEDICAL ICU
55 EFFICACY OF SIMPLE SCAVENGING SYSTEM APPLIED FOR VOLATILE-BASED, LONG-TERM
ICU SEDATION
56 PREDICTING PICU ADMISSION AND TEAM COMPOSITION FROM TRANSPORT RISK
ASSESSMENT IN PEDIATRICS SCORE
Oral Abstract Session: Sepsis
PUBLISHING NUMBER
57 IMPACT OF ORAL HEALTH ON INFECTIOUS COMPLICATIONS IN ADULTS HOSPITALIZED
DUE TO LEUKEMIAS IN THE USA
58 EBI3 GENETIC DEFICIENCY INCREASES LUNG AND SYSTEMIC INFLAMMATION IN MICE
SUBJECTED TO SEPSIS
59 EFFECT OF CHOLECALCIFEROL SUPPLEMENTATION ON VITAMIN D STATUS AND
CATHELICIDIN IN SEPSIS
60 PERSISTENTLY HIGH ALBUMIN LEAK IS ASSOCIATED WITH MORTALITY.
61 PRE-ADMISSION ORAL STEROIDS ARE ASSOCIATED WITH A DECREASED RISK OF ARDS IN
ICU PATIENTS WITH SEPSIS
62 RECOMBINANT HUMAN THROMBOMODULIN INHIBITS NEUTROPHIL EXTRACELLULAR
TRAPS FORAMATION IN VITRO
63 REWS: REAL-TIME EARLY WARNING SCORE FOR SEPTIC SHOCK
64 SHOCK INDEX TO ASSESS OUTCOMES ON PEDIATRIC INTERFACILITY TRANSPORT
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
POSTER PRESENTATIONS
Poster Session: Research Citation Finalists
PUBLISHING NUMBER
101 PHARMACOKINETICS OF MICAFUNGIN IN PLASMA AND BURN ESCHARES IN CRITICALLY
ILL BURNED PATIENTS
102 ADHERENCE TO GUIDELINES BASED ANTIBIOTIC THERAPY IN THE TREATMENT OF
COMMUNITY ACQUIRED PNEUMONIA
103 EVALUATION OF SEPSIS TREATMENT OUTCOMES IN PORT-AU-PRINCE, HAITI
104 A POTENTIAL NOVEL ROLE FOR OLFACTOMEDIN 4 IN SEPSIS
105 COMPARING ACCURACY OF 2 PHASES OF A PEDIATRIC ELECTRONIC SEVERE SEPSIS
SCREENING ALGORITHM
106 DOES PICC INSERTION IN BACTEREMIC PATIENTS INCREASE CLABSI RATE?
107 COMBINING EEG AND SERUM BRAIN BIOMARKERS TO CLASSIFY MORTALITY AFTER
PEDIATRIC CARDIAC ARREST
108 THE ROLE OF BRANCHED CHAIN AMINO ACIDS IN THE FUNCTIONAL RECOVERY FROM
TRAUMATIC BRAIN INJURY
109 PLASMA HIGH-MOBILITY GROUP BOX-1 (HMGB1) CONCENTRATION IN PEDIATRIC SEPSIS
AND MULTIORGAN FAILURE
110 HIGH-DOSE ERYTHROPOIETIN IMPROVES SURVIVAL IN A SWINE MODEL OF
VENTRICULAR FIBRILLATION
111 VARIATION OF CENTRAL VENOUS CATHETER USAGE IN THREE ICUS MANAGED BY THE
SAME INTENSIVIST GROUP
112 USING INDIRECT CALORIMETRY DATA TO ASSESS THE IMPACT OF SEDATIVES ON REE IN
THE ICU
113 EPIDEMIOLOGY AND OUTCOMES OF NEW-ONSET ATRIAL FIBRILLATION IN THE ICU:
A 6-YEAR RETROSPECTIVE STUDY
114 VALIDATION OF THE SWIFT SCORE FOR INTENSIVE CARE UNIT (ICU) READMISSIONS IN
AN ASIAN POPULATION
115 CEREBRAL PERFUSION PRESSURE IN PATIENTS UNDERGOING HYPOTHERMIA AFTER
CARDIAC ARREST
116 CEFTAZIDIME-AVIBACTAM TESTED AGAINST GRAM-NEGATIVE BACTERIA FROM ICU
PATIENTS
117 IMPACT OF MACROLIDE ANTIBIOTICS ON OUTCOMES IN ICU PATIENTS WITH ACUTE
EXACERBATIONS OF COPD
118 PREHOSPITAL HYPOTENSION CORRELATES WITH INJURY SEVERITY AND OUTCOMES
119 THE EVALUATION OF CEREBRAL FUNCTION AFTER HYPOTHERMIA IN A PIG MODEL
OF CPR
120 PATTERNS OF DETERIORATION IN HOSPITALIZED PEDIATRIC ONCOLOGY PATIENTS
REQUIRING ICU ADMISSION
121 FEASIBILITY OF A NON-INVASIVE SENSOR FOR MEASURING ICU PATIENT MOBILITY
122 CULTURE ALGORITHM TO REDUCE URINE CULTURE AND CATHETER-ASSOCIATED
URINARY TRACT INFECTION RATES
123 PEDIATRIC PROCEDURAL SEDATION USING DEXMEDETOMIDINE: PROVIDER SPECIALTY
AND COMPLICATION RATES
124 PREDICTORS OF PTSD AND DEPRESSION AMONG FAMILY AND FRIENDS OF PATIENTS
ADMITTED TO THE ICU
125 USE OF A PEDIATRIC TRAUMATIC BRAIN INJURY PATHWAY IS ASSOCIATED WITH
IMPROVED OUTCOMES
126 GLYCEMIC VARIABILITY WITH TEMPERATURE CHANGES DURING THERAPEUTIC
HYPOTHERMIA AFTER CARDIAC ARREST
127 IN-HOSPITAL ARRESTS, ANOXIC/HYPOXIC ISCHEMIC ENCEPHALOPATHY, AND G TUBE/
TRACHEOSTOMY ESTIMATES.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
128 PEDIATRIC DELIRIUM PREVALENCE AND MOTORIC SUBTYPES IN CRITICALLY ILL
INFANTS AND YOUNG CHILDREN
129 FAMILY PRESENCE DURING TRACHEAL INTUBATIONS IN PEDIATRIC ICUS
130 POST-RESUSCITATION REDUCTION OF HEPATIC MICROCIRCULATION REFLECTS CARDIAC
BUT NOT LIVER DYSFUNCTION
Poster Session: Administration 1
PUBLISHING NUMBER
131 EFFECT OF ENVIRONMENT OF CARE WITHIN PIRO SEPSIS MODEL: IS TELE-HEALTH THE
ANSWER FOR HEALTH POLICY?
132 A SURVEY ASSESSING PICU PROVIDERS’ KNOWLEDGE OF THE COST OF CARE
133 CLINICAL PREDICTORS OF RESOURCE UTILIZATION IN SEVERE PEDIATRIC TRAUMATIC
BRAIN INJURY
134 PHYSICIAN ASSISTANT BILLING AND PROCEDURES IN THE INTENSIVE CARE UNIT
135 DEMAND FORECAST AND OPTIMAL PLANNING OF ICU BEDS: A CASE STUDY IN RIO DE
JANEIRO (RJ)
136 LESSONS LEARNED IN THE EVOLUTION OF PEDIATRIC CRITICAL CARE: APPLICABILITY IN
DEVELOPING COUNTRIES
137 HOSPITAL COSTS ASSOCIATED WITH SIGNIFICANT PEDIATRIC BRAIN INJURIES
138 FREQUENT FLYERS TO AN ONCOLOGIC ICU: CHARACTERISTICS AND OUTCOMES
139 PHYSICIAN ASSISTANT DEMOGRAPHICS IN THE INTENSIVE CARE UNIT
140 THE IMPACT OF A HOME HEALTH, NURSE-DRIVEN TELEMONITORING PROGRAM ON
HEART FAILURE READMISSIONS
141 EFFECT OF DELIRIUM MOTORIC SUBTYPES ON ICD-9 DOCUMENTATION OF DELIRIUM IN
THE INTENSIVE CARE UNIT
Poster Session: Administration 2
PUBLISHING NUMBER
142 CRITICAL CARE CAPACITY IN LOW-INCOME COUNTRIES: A SYSTEMATIC REVIEW
143 CURRENT PRACTICE OF MECHANICALLY VENTILATED PATIENTS TREATED OUTSIDE THE
ICU IN JAPAN
144 LESSONS LEARNED FROM A PICU SURGE CAPACITY EXERCISE IN A NEW YORK CITY
CHILDREN’S HOSPITAL
145 A COMMUNITY HOSPITAL TELEMEDICINE PROGRAM- INCREASING UTILIZATION OVER A 4
YEAR PERIOD
146 COMPARISON OF PROVIDER TYPES WHO PERFORMED PREHOSPITAL LIFESAVING
INTERVENTIONS: A PROSPECTIVE STUDY
147 OPTIMAL THRESHOLDS FOR A PICU VENTILATOR ALLOCATION ALGORITHM IN A
PANDEMIC
148 INTERHOSPITAL TRANSFER OF CHILDREN IN RESPIRATORY FAILURE: A CLINICIAN
INTERVIEW QUALITATIVE STUDY
149 INTERHOSPITAL TRANSFER OF CHILDREN IN SEPTIC SHOCK: A CLINICIAN INTERVIEW
QUALITATIVE STUDY
150 STRESS ULCER PROPHYLAXIS PROTOCOL COMPLIANCE IN A MICU MANAGED BY ACNPS
VERSUS MEDICAL RESIDENTS
151 IMPACT OF COMPUTERIZED PHYSICIAN ORDER ENTRY ON SEDATION DEPTH AND
RELATED OUTCOMES IN THE ICU
152 EVALUATION OF SAS-BASED SYMPTOM-TRIGGERED TREATMENT OF ALCOHOL
WITHDRAWAL IN CRITICALLY ILL PATIENTS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Cardiovascular 1
PUBLISHING NUMBER
153 CORRELATION BETWEEN INVASIVE AND NON-INVASIVE CARDIAC OUTPUT ASSESSMENT
IN HEART TRANSPLANT PATIENTS
154 ASSOCIATION OF PARP-1 ACTIVITY WITH MYOCARDIAL DYSFUNCTION IN PATIENT WITH
SEPTIC SHOCK
155 CARDIAC FUNCTION INDEX PREDICTS OUTCOME OF TAKOTSUBO CARDIOMYOPATHY
AFTER SUBARACHNOID HEMORRHAGE
156 WHAT IS ASSOCIATED WITH THE DISCREPANCY BETWEEN NIBP AND IBP?
157 THE SLUSCORETM: A NOVEL METRIC QUANTIFYING THE ADVERSE IMPACT OF
INTRAOPERATIVE HYPOTENSIVE EXPOSURE
158 IMPACT OF ORAL HEALTH ON OUTCOMES IN PATIENTS HAVING HEART VALVE
REPLACEMENT PROCEDURES IN USA.
159 POOR ORAL HEALTH IN CABG SURGERY RECIPIENTS INCREASES THE RISK OF
INFECTIOUS COMPLICATIONS
160 ANTICOAGULATION INDICES IN EXTRACORPOREAL MEMBRANE OXYGENATION PATIENTS
Poster Session: Cardiovascular 2
PUBLISHING NUMBER
161 PREDICTION OF MAJOR ADVERSE CARDIOVASCULAR EVENTS BY PLASMA NGAL AT CCU
DISCHARGE
162 ALTERATIONS IN PROTEINASE-ACTIVATED RECEPTOR-1 EXPRESSION WITH INCREASED
PULMONARY BLOOD FLOW
163 PERIOPERATIVE ANTICOAGULATION SPECIFIC TO CARDIAC INTERVENTIONAL
PROCEDURES
164 THE PROGNOSTIC VALUE OF SERUM 25- HYDROXY VITAMIN D LEVEL IN PATIENTS WITH
ST-SEGMENT ELEVATION MI
165 GOAL-DIRECTED THERAPY DOES NOT REVERSE AKI IN CRITICALLY ILL PATIENTS BUT
DECREASES MORTALITY.
166 THE IMPACT OF VASOPRESSIN ADMINISTRATION ON ACUTE KIDNEY INJURY FOLLOWING
OPEN HEART SURGERY
167 ARTERIAL CATHETER FAILURE IN CRITICALLY ILL PATIENTS
168 LOW CARDIAC OUTPUT SYNDROME SCORE–THE NEW COMPANION TO THE VASOACTIVEINOTROPIC SCORE?
169 NON-INVASIVE MEASURE OF MUSCLE PH CORRELATES WITH SPLANCHNIC PERFUSION
DURING SHOCK
Poster Session: Cardiovascular 3
PUBLISHING NUMBER
170 NASAL ALAR BLOOD FLOW IS MAINTAINED WITH OCCLUSION OF THE FACIAL AND/OR
OPHTHALMIC ARTERIES
171 ADVANCING ICU TELEMEDICINE: REAL TIME FOCUSED CRITICAL CARE MEDICINE
TELE-ECHOCARDIOGRAM
172 COMPARISON OF UNCALIBRATED, CALIBRATED AND THERMODILUTION-DERIVED
CARDIAC INDEX: A PROSPECTIVE STUDY
173 NON-INVASIVE MEASURE OF TISSUE PERFUSION, SMO2, COMPARED WITH STANDARD
INVASIVE ASSESSMENTS OF SHOCK
174 PROPHYLACTIC AMIODARONE AND MAGNESIUM FOR POSTOPERATIVE ATRIAL
FIBRILLATION IN CARDIAC SURGERY
175 CARDIAC DYSFUNCTION IN ADULT HEART DONORS & TEMPORAL CHANGES OF LV
SYSTOLIC FUNCTION OVER TIME
176 SPECKLE TRACKING IMAGING FOR EVALUATION OF EFFECTS OF PEEP LEVEL ON RIGHT
VENTRICULAR FUNCTION
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
177 A NONPHARMACOLOGICAL APPROACH TO DECREASE RESTRAINT USE IN A TRAUMA
INTENSIVE CARE UNIT
178 CONTINUATION OF AMIODARONE AT DISCHARGE FOR NEW-ONSET ATRIAL FIBRILLATION
IN CRITICALLY ILL PATIENTS
Poster Session: Cardiovascular 4
PUBLISHING NUMBER
179 EFFICACY OF CHEMICAL PLEURODESIS WITH DOXYCYCLINE FOR CHYLOUS PLEURAL
EFFUSION AFTER CARDIAC SURGERY
180 SEVERE PULMONARY HYPERTENSION AND RHF TREATED WITH ECMO PRIOR TO DOUBLE
LUNG TRANSPLANT
181 TRANSFUSION RELATED PULMONARY COMPLICATIONS IN CARDIOVASCULAR SURGICAL
PATIENTS
182 CORRELATION BETWEEN P WAVE DURATION ON ADMISSION AND NURSING AND
SEVERITY INDEXES IN ICU PATIENTS.
183 THE RELATION BETWEEN INTERLEUKIN-18 AND ACUTE CORONARY SYNDROME
184 EVOLUTION OF LIVER FUNCTION AFTER INITIATION OF VENO-ARTERIAL
EXTRACORPOREAL MEMBRANE OXYGENATION
185 GOAL DIRECTED ECHOCARDIOGRAPHY BY NON-CARDIOLOGIST IN CRITICALLY ILL
PATIENTS; EGYPTIAN EXPERIENCE
186 ASSESSING HEMORRHAGE SEVERITY WITH CONTINUOUS AUTOMATIC HEART-RATECOMPLEXITY MONITORING IN SWINE
187 ECG STUDY IN ICU PATIENTS: QTC INTERVAL
Poster Session: Cardiovascular 5
PUBLISHING NUMBER
188 THE PREVALENCE OF CHRONIC ATRIAL FIBRILLATION: PRE-OPERATIVE FACTORS
ASSOCIATED
189 CORRELATION OF INTRACELLULAR HISTAMINE AND CLINICAL SYMPTOMS IN
ANAPHYLACTIC PATIENTS
190 SHORT-COURSE OF RANOLAZINE PREVENTS POST-OPERATIVE ATRIAL FIBRILLATION
FOLLOWING CARDIAC SURGERIES
191 EFFECT OF DEXMEDETOMIDINE ON POSTOPERATIVE TACHYARRHYTHMIAS AFTER
VALVULAR SURGERY
192 EFFECT OF V-V ECMO FLOW RATES ON IVC DIAMETER VARIATION ON TRANS-THORACIC
ECHOCARDIOGRAPHY
193 DATA DRIVEN PERSONALIZED RISK PREDICTION IN PEDIATRIC INTENSIVE CARE UNITS
194 RISK FACTORS FOR DEXMEDETOMIDINE-ASSOCIATED HEMODYNAMIC INSTABILITY IN
NON-CARDIAC ICU PATIENTS
195 RESULTS OF A RESTRICTIVE V. LIBERAL TRANSFUSION STRATEGY IN NEONATAL AND
INFANT CARDIAC SURGERY
196 USING ABDOMINAL NIRS TO PREDICT GASTROINTESTINAL MORBIDITY IN NEONATES
AFTER CARDIAC SURGERY
Poster Session: Cardiovascular 6
PUBLISHING NUMBER
197 IMAGE ACQUISITION AND INTERPRETATION OF BEDSIDE ULTRASOUND BY PEDIATRIC
CRITICAL CARE PROVIDERS
198 PREDICTORS OF THE UTILIZATION OF TEMPORARY PACING WIRES IN PEDIATRIC
PATIENTS AFTER CARDIAC SURGERY
199 EARLY DETECTION OF CRITICAL CONGENITAL HEART DISEASE IN THE NEWBORNS BY
PULSE OXIMETRY
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
200 EVALUATION OF PULMONARY VASODILATORS IN PEDIATRIC CONGENITAL
CARDIOVASCULAR CARE
201 THE INCIDENCE OF LEFT VENTRICULAR DIASTOLIC DYSFUNCTION IN PEDIATRIC
PATIENTS WITH SEPSIS
202 EXTUBATION FAILURE IN POSTOPERATIVE SINGLE-VENTRICLE INFANTS WITH PARALLEL
CIRCULATION
203 BOUND AND FREE CORTISOL RESPONSE AND THE RELATION TO OUTCOMES AFTER
INFANT CARDIOPULMONARY BYPASS
204 RELATIONSHIP OF COPEPTIN AND ARGININE VASOPRESSIN MEASUREMENTS AFTER
PEDIATRIC CARDIAC SURGERY
205 HEMODYNAMIC SAFETY OF PROLONGED DEXMEDETOMIDINE USE IN PEDIATRIC
CARDIAC CRITICAL CARE PATIENTS
Poster Session: Cardiovascular 7
PUBLISHING NUMBER
206 FRACTURES RELATED TO METABOLIC BONE DISEASE IN WITH CONGENITAL HEART
DISEASE
207 OUTCOMES ASSOCIATED WITH USE OF DIALYSIS IN CHILDREN RECEIVING ECMO AFTER
HEART SURGERY
208 INFERIOR VENA CAVA COLLAPSIBILITY AND VASCULAR REACTIVITY IN PEDIATRIC
PATIENTS.
209 ASSOCIATION BETWEEN SERUM CORTISOL LEVELS AND HYDROCORTISONE THERAPY
AFTER PEDIATRIC CARDIAC SURGERY
210 DEXAMETHASONE LEVELS AND THE ASSOCIATION WITH CLINICAL OUTCOMES AFTER
INFANT CARDIOPULMONARY BYPASS
211 RELATIONSHIP OF ECMO DURATION WITH OUTCOMES AFTER PEDIATRIC CARDIAC
SURGERY
212 IMPACT OF TIMING OF ECMO INITIATION ON OUTCOMES AFTER PEDIATRIC HEART
SURGERY
213 INTERMEDIATE TERM RESULTS AFTER EXTRA CARDIAC CONDUIT FONTAN SURGERY IN
CHILDREN AND YOUNG ADULTS
214 ARE COMPLICATIONS OF SURGICAL VENTRICULAR SEPTAL DEFECT CLOSURE, AGE OR
WEIGHT DEPENDENT ?
Poster Session: Cardiovascular 8
PUBLISHING NUMBER
215 OUTCOMES ASSOCIATED WITH PREOPERATIVE USE OF ECMO IN CHILDREN UNDERGOING
HEART OPERATION
216 KETOROLAC USE FOR PAIN CONTROL IN PEDIATRIC PATIENTS AFTER CARDIAC SURGERY
217 A RETROSPECTIVE EVALUATION OF RECRUITMENT MANEUVERS IN A CARDIAC
PEDIATRIC INTENSIVE CARE UNIT
218 PULSE PRESSURE VARIATION SHOWS CONSISTENT AND ROBUST CHANGE IN RESPONSE
TO FLUID BOLUS IN CHILDREN
219 EARLY CELL SAVER TRANSFUSION DECREASES THE NEED FOR ALLOGENEIC BLOOD
AFTER PEDIATRIC CARDIAC SURGERY
220 PRESERVED FETAL RIGHT VENTRICULAR NO SIGNALING IN AN OVINE MODEL OF
CONGENITAL HEART DISEASE
221 HYPOALBUMINEMIA PREDICTS THE CLINICAL COURSE IN PEDIATRIC PATIENTS AFTER
OPEN HEART SURGERY
222 VARIATION OF VENTILATION PRACTICES WITH CENTER VOLUME AFTER PEDIATRIC
HEART SURGERY
223 CEREBRAL OXYGENATION AND HEMODYNAMICS IN NEONATES AFTER CARDIAC SURGERY
224 DATA DRIVEN MATHEMATICAL MODELING OF THE SINGLE VENTRICLE ANATOMY AND
PHYSIOLOGY
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: CPR/Resuscitation 1
PUBLISHING NUMBER
225 PHYSIOLOGICAL MONITORING OF CPR QUALITY IS ASSOCIATED WITH IMPROVED
SURVIVAL FROM CARDIAC ARREST
226 DEFINING HEAD-TILT POSITION OF RESUSCITATION
227 CARDIOPULMONARY RESUSCITATION IN CHILDREN ONBOARD COMMERCIAL AIRLINE
FLIGHTS
228 DELIRIUM IN SURVIVORS OF CARDIAC ARREST TREATED WITH MILD THERAPEUTIC
HYPOTHERMIA
229 METHOD OF COOLING IS NOT ASSOCIATED WITH CHANGES IN SURVIVAL FOR
THERAPEUTIC HYPOTHERMIA PATIENTS
230 DEVELOPMENT OF AN INNOVATIVE IN SITU CARDIAC ARREST SIMULATION TRAINING
PROGRAM
231 EFFECT OF HYPOTHERMIA ON POST-RESUSCITATION CEREBRAL MICROCIRCULATION IN
A RAT MODEL OF CPR
232 EVALUATION OF POST-INTUBATION HYPOTENSION USING PRE-INTUBATION SHOCK
INDEX AND MODIFIED SHOCK INDEX
Poster Session: CPR/Resuscitation 2
PUBLISHING NUMBER
233 OUTCOMES OF DELAYED RRT ACTIVATION IN PATIENTS TRANSFERRING TO THE ICU
234 EXPRESSION OF SUPEROXIDE DISMUTASE AND NF-ΚB IS AUGMENTED IN THE
HIPPOCAMPUS OF RATS DURING CPR
235 HOW WELL DO WE DOCUMENT NEONATAL RESUSCITATION? AMEND (ASSESSMENT OF
NEONATAL DOCUMENTATION) STUDY
236 BLOOD LACTATE LEVELS AFTER CARDIAC ARREST
237 EFFECTS OF PROGESTERONE ON NEUROLOGICAL OUTCOMES IN A RAT MODEL OF
CARDIAC ARREST AND RESUSCITATION
238 RETROSPECTIVE USE OF AN ELECTRONIC CHECKLIST AT RAPID RESPONSE TEAM
ACTIVATIONS: A CERTAIN STUDY
239 PROGNOSTIC VALUE OF MR DIFFUSION IMAGING IN CARDIAC ARREST PATIENTS
TREATED WITH HYPOTHERMIA THERAPY
240 UNDERSTANDING HOW BASIC LIFE SUPPORT TRAINING IS UTILIZED BY OUR MEDICAL
STUDENTS ON CLINICAL ROTATI
241 TIME TO TARGET TEMPERATURE DURING THERAPEUTIC HYPOTHERMIA AFTER CARDIAC
ARREST: EFFECT ON OUTCOME
Poster Session: CPR/Resuscitation 3
PUBLISHING NUMBER
242 EXPRESSION OF HIF-1A AND NF-ΚB IN THE HIPPOCAMPUS OF RATS INDUCED BY
CARDIOPULMONARY RESUSCITATION
243 COMBINATION THERAPY OF NIACIN AND SELENIUM ATTENUATES BRAIN INJURY AND
IMPROVES NEUROLOGICAL OUTCOME
244 THE NEUROPROTECTIVE EFFECT OF VALPROATE COMBINED WITH HYPOTHERMIA ON
ASPHYXIAL CARDIAC ARREST MODEL
245 COMPARISON OF SURVIVAL HOSPITAL DISCHARGE FOR PATIENTS RECEIVING ECPR IN
WEEKEND VERSUS WEEKDAYS
246 PATIENT AND PROVIDER CHARACTERISTICS IN TRACHEAL INTUBATION ASSOCIATED
CARDIAC ARREST EVENTS
247 SEIZURE INCIDENCE IN THERAPEUTIC HYPOTHERMIA PATIENTS POST CARDIAC ARREST
248 RESUSCITATIVE ENDOVASCULAR BALLOON OCCLUSION OF THE AORTA IMPROVES
SURVIVAL IN LETHAL HEMORRHAGE
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
249 CODE TEAM TRAINING: IMPROVING TEAM DYNAMICS AND ADHERENCE TO AHA
GUIDELINES
250 EVALUATION OF A THERAPEUTIC HYPOTHERMIA PROTOCOL AT A COMMUNITY HOSPITAL
IN ALABAMA
Poster Session: CPR/Resuscitation 4
PUBLISHING NUMBER
251 WHOLE BLOOD TRANSFUSION VIA IO ACCESS DOES NOT RESULT IN GROSS HEMOLYSIS IN
A PRE-CLINICAL STUDY
252 NEUROMUSCULAR BLOCKING AGENTS DO NOT IMPACT TIME TO TARGET TEMPERATURE
WITH THERAPEUTIC HYPOTHERMIA
253 THE EFFECTS OF TEMPERATURE VARIABILITY ON THE OUTCOME OF COMATOSE
SURVIVORS AFTER CARDIAC ARREST
254 INCORPORATION OF POINT OF CARE ULTRASONOGRAPHY INTO ACLS PROTOCOLS
255 SERUM CYTOCHROME C IS ASSOCIATED WITH OUTCOME AND CARDIAC DYSFUNCTION
AFTER PEDIATRIC CARDIAC ARREST
256 TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST:33°C VS 36°C,
SHIVERING AND HYPERTHERMIA CONTROL
257 THE IMPACT OF VASOPRESSOR SUPPORT ON SURVIVAL IN PATIENTS UNDERGOING
THERAPEUTIC HYPOTHERMIA
258 SUBLINGUAL MICROCIRCULATION IS RELATED WITH BULBAR CONJUNCTIVA
MICROCIRCULATION IN A RAT MODEL
Poster Session: CPR/Resuscitation 5
PUBLISHING NUMBER
259 COMPARISON OF PERFORMANCE OF AED BETWEEN TRAINED AND UNTRAINED RESCUERS
IN A MANIKIN STUDY
260 SURVIVAL FOLLOWING AKI IN ADULTS WHO RECEIVED EXTRACORPOREAL
CARDIOPULMONARY RESUSCITATION.
261 UTILITY OF LEFT VENTRICULAR EJECTION FRACTION AS A PREDICTOR OF SURVIVAL
AFTER CARDIAC ARREST
262 MAGNETIC RESONANCE AND ELECTROENCEPHALOGRAPHIC CORRELATES OF
MYOCLONUS IN CARDIAC ARREST SURVIVORS
263 IMPACT OF INDUCED HYPOTHERMIA ON CARDIAC ARREST SURVIVAL AND ASSOCIATED
INITIAL RHYTHM
264 PROMPTING WITH ELECTRONIC CHECKLIST IMPROVES CLINICIAN PERFORMANCE IN
MEDICAL EMERGENCIES: HIGH FIDE
265 “TEAM CODE”: COUNTING ON DEBRIEFS: IMPROVING TEAM PERFORMANCE AT AN
UNIVERSITY MEDICAL CENTER
266 THE VALUE OF AEEG AND RSO2 ASSESSMENT OF POST-CARDIAC ARREST SYNDROME WITH
THERAPEUTIC HYPOTHERMIA
267 I-FABP IS AN INTESTINAL INJURY MARKER IN SIRS FOLLOWING CARDIAC ARRESTS
Poster Session: CPR/Resuscitation 6
PUBLISHING NUMBER
268 ASSOCIATION OF BODY MASS INDEX WITH TIME TO TARGET TEMPERATURE IN
THERAPEUTIC HYPOTHERMIA PATIENTS
269 THE USE OF ULTRASOUND GUIDANCE FOR EMERGENCY INTUBATIONS IN THE ICU.
270 ROLE-BASED RESUSCITATION AND INTERDISCIPLINARY CODE BLUE TEAM TRAINING
271 IMPACT OF CARDIO PULMONARY RESUSCITATION(CPR) ON OUTCOMES IN ADULT STEM
CELL TRANSPLANT RECIPIENTS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
272 INCREASED SURVIVAL IN SMOKERS TREATED WITH THERAPEUTIC HYPOTHERMIA
FOLLOWING CARDIAC ARREST.
273 BALANCED RESUSCITATION IN POST-OPERATIONAL PATIENTS AFTER DIGESTIVE
SURGERY IN ICU
274 COMPARISON BETWEEN TWO METHODS OF TARGETED TEMPERATURE MANAGEMENT IN
PATIENTS WITH CARDIAC ARREST
275 PREDICTION FOR NEED OF VASOPRESSORS BY VITALS AND PHYSICAL EXAMINATION
FINDINGS IN EARLY SHOCK
276 DEVELOPMENT OF A CARDIOPULMONARY RESUSCITATION NON-TECHNICAL SKILLS
SCORING TOOL (CPR-NTS)
Poster Session: CPR/Resuscitation 7
PUBLISHING NUMBER
277 INTRAVASCULAR GAS OF POST CPR MAY ASSOCIATE WITH HYPERCAPNIA DURING CHEST
COMPRESSION.
278 THE STATE OF CARDIOPULMONARY ARREST WITH SEVERE HYPOTHERMIA
279 SHIVERING IN CARDIAC ARREST PATIENTS UNDERGOING THERAPEUTIC HYPOTHERMIA
IS ASSOCIATED WITH SURVIVAL
280 EXTERNAL VERSUS INTERNAL COOLING FOR THERAPEUTIC HYPOTHERMIA: DOES THE
METHOD MATTER?
281 MONITORING OF CIRCULATING WATER TEMPERATURE CAN DETECT FEVER DURING
THERAPEUTIC HYPOTHERMIA
282 ANTI-SHIVERING MEDICATION REQUIREMENTS IN THERAPEUTIC NORMOTHERMIA:
SURFACE VS. ENDOVASCULAR COOLING
283 VECTOR AUTO-REGRESSIVE (VAR) MODEL FOR EXPLORING CAUSAL DYNAMICS OF
CARDIORESPIRATORY INSTABILITY
284 DONOR TISSUE OXYGEN SATURATION CORRELATES WITH THE NUMBER OF ORGANS
TRANSPLANTED PER DONOR
285 OUTCOMES ASSOCIATED WITH CPR IN STEM CELL TRANSPLANT RECIPIENT CHILDREN
IN USA
Poster Session: Education 1
PUBLISHING NUMBER
286 IMPACT OF INTERPROFESSIONAL COLLABORATION ON DELIRIUM SCREENING AND
TREATMENT IN A PICU
287 HIGH-FIDELITY SIMULATION RESOLVES KNOWN AND UNKNOWN MILESTONE GAPS IN
SURGICAL CRITICAL CARE
288 HIGH-FIDELITY SIMULATION IMPROVES RESIDENT LEARNING FOR THE PECARN HEAD
TRAUMA RULE
289 EFFICACY OF A STREAMLINED EDUCATION PROGRAM FOR NURSING TRANSITION INTO
CRITICAL CARE AREAS
290 ASSESSING KNOWLEDGE AND CONFIDENCE OF THE NURSE PRACTITIONER AND
PHYSICIAN ASSISTANT RESIDENT
291 EFFECT OF VIDEO LARYNGOSCOPY WITH SUPERVISOR FEEDBACK ON TRAINEE
INTUBATION EDUCATION
292 CAN YOU INTUBATE BETTER THAN A 5TH GRADER: THE VALUE OF VIDEO LARYNGOSCOPY
IN MED STUDENT TEACHING
293 EVALUATION OF KEY WORDS CITED IN CRITICAL CARE MEDICINE PUBLICATIONS
294 IMPLEMENTATION AND EXPANSION OF AN ONLINE CRITICAL CARE PHARMACY JOURNAL
CLUB
295 USING AN AUDIENCE RESPONSE SYSTEM SMARTPHONE APP TO IMPROVE RESIDENT
EDUCATION IN THE PICU
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Education 2
PUBLISHING NUMBER
296 EVIDENCE-BASED ICU FELLOW TRACHEAL INTUBATION SKILL MILESTONES
297 EFFECT OF SIMULATION BASED CURRICULUM ON THE UTILIZATION OF RAPID RESPONSE
TEAM ACTIVATIONS (RRT)
298 ANNUAL FIELD EPIDEMIOLOGY COURSE: A SIMULATED INVESTIGATION OF A FEBRILE
ILLNESS IN TUMBES, PERU
299 INTERN PERCEPTION OF CODE BLUE SIMULATION TRAINING IN RESIDENCY
300 DEVELOPMENT OF INTERNATIONAL PEDIATRIC FUNDAMENTALS OF CRITICAL CARE
SUPPORT (PFCCS) INSTRUCTORS
301 NURSING PERCEPTIONS AND ASSOCIATION WITH APPROACH RATES IN THE THAPCA
TRIALS
302 SIMULATION TRAINING FOR ICU TEAMS FOR APPROACH TO DONATION AFTER CARDIAC
DEATH
303 ACHIEVING COMPETENCY IN ULTRASOUND GUIDED CENTRAL VENOUS CATHETER
INSERTION FOR INCOMING HOUSE STAFF
304 COMPUTER SOFTWARE DEPICTS DYNAMIC SHIFTING OF THE OXYHEMOGLOBIN
DISSOCIATION CURVE VIDEOGRAPHICALLY
305 USING A “FLIPPED CLASSROOM” MODEL TO TEACH BEDSIDE ECHOCARDIOGRAPHY IN A
SURGICAL ICU
Poster Session: Education 3
PUBLISHING NUMBER
306 VALIDATING PEDIATRIC CRITICAL CARE TRAINING WITH KNOWLEDGE, CONFIDENCE,
AND SIMULATION COMPETENCY
307 DESIGNING & IMPLEMENTING A WEB-BASED “QUESTION OF THE DAY” MODULE IN A BUSY
CRITICAL CARE FELLOWSHIP
308 REINFORCING ABCDE BUNDLE CONCEPTS THROUGH INTERPROFESSIONAL SIMULATION
AND TEAM STEPPS TRAINING
309 EVALUATION OF FCCS IN CRITICAL CARE EDUCATION IN JAPAN: A SURVEY OF
INSTRUCTORS AND PARTICIPANTS
310 SIMULATION-BASED CENTRAL VENOUS CATHETER PLACEMENT TRAINING PROGRAM FOR
INTERNAL MEDICINE RESIDENTS
311 ASSESSMENT OF DISASTER-PREPAREDNESS AMONGST PEDIATRICIANS
312 COMMUNICATION & PROFESSIONALISM: VALIDATION OF AN ASSESSMENT TOOL IN A
PEDIATRIC FELLOWSHIP PROGRAM
313 RISE AND SHINE EVERYONE: HOSPITAL WIDE EARLY MOBILITY PROGRAM
314 IMPLEMENTATION OF A SUCCESSFUL INTENSIVE CARE NURSING STAFF DEVELOPMENT
PROGRAM IN HAITI
315 TOWARD ECHOCARDIOGRAPHY AND CRITICAL CARE ULTRASOUND INTEGRATION INTO
CRITICAL CARE FELLOWSHIP
Poster Session: Education 4
PUBLISHING NUMBER
316 ICU ROUNDS AND MENTAL FATIGUE
317 INTRODUCTION OF A DEGREE COURSE IN CRITICAL CARE FOR UNDERGRADUATE
MEDICAL STUDENTS
318 COLLABORATIVE TEACHING OF MEDICAL AND NURSING STUDENTS IN ACUTE CARDIAC
ARREST SIMULATION
319 ASSESSING PARENT UNDERSTANDING OF THE “ASTHMA ACTION PLAN” EDUCATION
USING INTERACTIVE MOBILE APP.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
320 ACCIDENT PREVENTION AND FIRST AID KNOWLEDGE AMONG PRESCHOOL CHILDREN’S
PARENTS
321 QUALITY OF YOUTUBE VIDEOS ON CENTRAL LINE PLACEMENT
322 EVALUATING PALLIATIVE CARE EDUCATION IN PEDIATRIC CRITICAL CARE TRAINING
PROGRAMS
323 KNOWLEDGE AND SKILL GAPS IN HIGH QUALITY CPR ARE PREVALENT IN THE PEDIATRIC
INTENSIVE CARE UNIT
324 TRANSITION TO FIRST JOB: AN IN TRAINING SECTION RESEARCH SURVEY
325 ARE RESIDENTS PREPARED TO ENTER THE “REAL WORLD”? SURVEYING BOTH ATTENDING
AND RESIDENT VIEWPOINTS
Poster Session: Endocrine/Nutrition 1
PUBLISHING NUMBER
326 THE EFFECT OF GUT-ORIENTED COMPREHENSIVE NUTRITIONAL THERAPY ON
NOSOCOMIAL INFECTIONS.
327 IMPLEMENTATION OF AN AGGRESSIVE ENTERAL NUTRITION PROTOCOL AND THE
EFFECT ON CLINICAL OUTCOMES
328 A COMPARISON OF BOLUS VERSUS CONTINUOUS FEEDING METHODS IN MECHANICALLY
VENTILATED CHILDREN
329 COMPARISON OF INSULIN INFUSION METHODS IN CRITICALLY ILL PATIENTS: BASAL/
BOLUS AND MULTIPLIER
330 INSULIN GLARGINE COMPARED TO INSULIN NPH FOR THE MANAGEMENT OF
HYPERGLYCEMIA IN THE CRITICALLY ILL
331 ROUTE OF NUTRITIONAL SUPPORT AFFECTS METABOLIC OUTCOMES IN AN
ENDOTOXEMIA MODEL OF SEPSIS
332 ENTERAL NUTRITION ADMINISTRATION IN THE ICU: ACHIEVING GOALS WITH BETTER
STRATEGIES
333 NUTRITION PRACTICE PATTERNS IN ADULT ECMO PATIENTS: RESULTS OF AN
INTERNATIONAL SURVEY
334 EVALUATION OF A BASAL–BOLUS INSULIN PROTOCOL FOR CONTINUING DOSING
EFFICACY AND SAFETY OPTIMIZATION
335 NUTRITIONAL SUPPORT AND CLINICAL OUTCOMES OF CHILDREN IN A PEDIATRIC
INTENSIVE CARE UNIT
Poster Session: Endocrine/Nutrition 2
PUBLISHING NUMBER
336 EVALUATION OF GLUCOSE MANAGEMENT SOFTWARE IN CRITICALLY ILL PATIENTS WITH
HYPERGLYCEMIC CRISES
337 EFFECTS OF VITAMIN C AND E ON THE OUTCOME OF CRITICALLY ILL PATIENTS
REQUIRED MECHANICAL VENTILATION
338 USE OF PH AS AN INDICATOR OF NASOGASTRIC FEEDING TUBE PLACEMENT IN
CRITICALLY ILL INFANTS
339 EFFECT OF OPIOIDS AND BENZODIAZEPINES ON TOLERANCE OF ENTERAL NUTRITION IN
PICU
340 INCREASING WEIGHT-BASED DOSING OF INSULIN IS ASSOCIATED WITH HYPOGLYCEMIA
IN CRITICALLY ILL PATIENTS
341 ASSOCIATION OF EARLY ENTERAL NUTRITION DELIVERY AND CLINICAL OUTCOME IN
CRITICALLY ILL CHILDREN
342 EVALUATION OF A GLYCEMIC CONTROL PREVENTATIVE MEASURES PROTOCOL IN THE
INTENSIVE CARE UNIT
343 EFFICACY AND SAFETY OF INSULIN GLARGINE VERSUS INSULIN INFUSIONS IN
INTENSIVE CARE UNIT PATIENTS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
344 SYNBIOTICS THERAPY IMPROVES GUT DYSBIOSIS IN SEVERE SEPSIS PATIENTS: A
RANDOMIZED CONTROLLED TRIAL
345 METABOLOME ALTERATION IN CRITICAL ILLNESS ACCORDING TO VITAMIN D STATUS: A
PROSPECTIVE COHORT STUDY
Poster Session: Endocrine/Nutrition 3
PUBLISHING NUMBER
346 EDUCATION AND ALGORITHM IMPROVE NUTRITION OF CRITICALLY ILL PATIENTS IN THE
SURGICAL INTENSIVE CARE
347 ULTRASOUND GUIDED NASOGASTRIC FEEDING TUBE PLACEMENT IN CRITICAL CARE
PATIENTS
348 EFFICACY OF A NURSE-DRIVEN, ELECTRONIC, DIABETIC KETOACIDOSIS PROTOCOL–A
COMPARATIVE ANALYSIS
349 EVALUATION OF HYPOGLYCEMIA WITH 2 DIFFERENT INSULIN PROTOCOLS IN THE
NEUROINTENSIVE CARE UNIT(NICU)
350 RADIOLOGIC INTERPRETATION OF NUTRITION AT BASE OF SPINE (RIBS) - NOVEL MARKER
FOR NUTRITIONAL STATUS
351 EFFECTS OF INSULIN INFUSION RATE CHANGES ON GLUCOSE OSCILLATIONS FOR
STRESS HYPERGLYCEMIA
352 CALORIFIC DEFICIT IN PATIENTS WITH MULTIPLE SEVERE TRAUMA AND MORBIDITY
ASSOCIATED
353 EARLY TRANSITION TO SUBCUTANEOUS INSULIN FOR GLYCEMIC CONTROL IN CARDIAC
SURGERY
354 PARENTERAL NUTRITION IN CRITICAL CARE: OBSERVATIONS AND CHALLENGES IN A
PRACTICE PATTERN ASSESSMENT
355 ENTERAL FEEDING TIMING AND OUTCOMES AFTER SIMULTANEOUS TRACHEOSTOMY
AND PEG PLACEMENT IN THE ICU
Poster Session: Epidemiology 1
PUBLISHING NUMBER
356 ALL-TERRAIN VEHICLE ACCIDENTS: NINE YEARS OF EXPERIENCE AT A LEVEL 1 TRAUMA
CENTER
357 SIZE OF SEPSIS IN WALES: FEASIBILITY PILOT
358 OVERLAP OF COGNITIVE, PHYSICAL AND MENTAL HEALTH IMPAIRMENTS IN THE POSTINTENSIVE CARE SYNDROME
359 CONTEMPORARY TRENDS OF ICU UTILIZATION AMONG PATIENTS WITH DEMENTIA: A
POPULATION-BASED COHORT STUDY
360 LONG-TERM INTENSIVE CARE UNIT (ICU) OUTCOME TRENDS AMONG A NATIONWIDE
COHORT OF TELE-ICU PATIENTS
361 INJURIES DUE TO LEGAL INTERVENTION AND EMERGENCY DEPARTMENT VISITS
362 CHARACTERISTICS AND OUTCOMES OF CANCER PATIENTS ADMITTED TO THE INTENSIVE
CARE UNIT: A 5-YEAR STUDY
363 INCIDENCE AND OUTCOMES OF ARDS IN RWANDA USING MODIFIED BERLIN CRITERIA
FOR RESOURCE-POOR SETTINGS
Poster Session: Epidemiology 2
PUBLISHING NUMBER
364 RACE IS AN INDEPENDENT RISK FACTOR FOR MORTALITY DURING ECMO FOR
RESPIRATORY SUPPORT
365 CHARACTERISTICS OF LONG STAY PATIENTS IN PEDIATRIC INTENSIVE CARE UNITS IN
THE UNITED STATES
366 COST ANALYSIS OF THE PANGEA STUDY
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
367 EPIDEMIOLOGY OF HOSPITAL BASED ED VISITS DUE TO AIR AND SPACE TRANSPORT
ACCIDENTS IN THE USA
368 EPIDEMIOLOGICAL ESTIMATES OF EMERGENCY DEPARTMENT VISITS ATTRIBUTED TO
STORMS & FLOODS
369 DYSNATREMIAS IN CRITICALLY ILL CHILDREN: EPIDEMIOLOGY AND ASSOCIATED
OUTCOMES
370 INTERNATIONAL COLLABORATION IN PEDIATRIC CRITICAL CARE RCTS: A SOCIAL
NETWORK ANALYSIS
371 THE INCIDENCE OF VENTILATOR-ASSOCIATED PNEUMONIA IN THE UNITED STATES
FROM 2008 TO 2011
372 CHANGING TRENDS IN THE USE OF VASOPRESSORS IN INTENSIVE CARE UNIT: A 7-YEAR
STUDY
Poster Session: Epidemiology 3
PUBLISHING NUMBER
373 SIMULTANEOUS PREDICTION OF MORBIDITY (M), MORTALITY (D), AND INTACT SURVIVAL (S)
374 EPIDEMIOLOGICAL ESTIMATES OF HOSPITAL BASED EMERGENCY DEPARTMENT VISITS
ATTRIBUTED TO LIGHTNING
375 EFFECT OF METHODOLOGY: DETERMINING DISPARITIES IN MORTALITY OF TRAUMA
PATIENTS BASED ON PAYER SOURCE
376 THE ASSOCIATION OF AGE WITH SHORT-TERM AND LONG-TERM MORTALITY IN ADULTS
ADMITTED TO THE ICU
377 WITNESSES AND INITIAL RESPONSE ARE CRUCIAL FOR POSITIVE OUTCOMES IN
PATIENTS ASPIRATING FOOD.
378 RBC TRANSFUSION RATES WITHIN MECHANICALLY VENTILATED, MEDICAL ICU SHOCK
PATIENTS REQUIRING CRRT
379 A MODEL TO PREDICT DURATION OF VENTILATION AND 30-DAY MORTALITY IN PATIENTS
WITH TRAUMATIC INJURIES
380 OUTCOME OF BONE MARROW TRANSPLANTATION IN CHILDREN: AN ANALYSIS OF KID’S
INPATIENT DATABASE
Poster Session: Epidemiology 4
PUBLISHING NUMBER
381 NEW PROGNOSTIC PREDICTION SYSTEM IN CRITICAL CARE BASED ON NETWORK
ANALYSIS
382 PATIENT-SPECIFIC RISK MODEL OF BACTERIAL CO-INFECTION IN CHILDREN WITH
SEVERE VIRAL BRONCHIOLITIS
383 PATTERN OF HOSPITAL ADMISSIONS AND OUTCOME OF ACUTE ALUMINIUM PHOSPHIDE
POISONING IN AN INDIAN ICU
384 ELIXHAUSER COMORBIDITY INDEX BETTER PREDICTS ICU MORTALITY THAN CHARLSON
COMORBIDITY INDEX
385 TOXIC COLITIS: SURGICAL OUTCOMES AND RISK FACTORS FOR MORTALITY
386 RETROSPECTIVE MULTICENTER STUDY OF IN-HOSPITAL CARDIOPULMONARY ARREST
(CPA) IN JAPAN
387 HOSPITAL BASED EMERGENCY DEPARTMENT VISITS DUE TO RAPE: A PUBLIC HEALTH
ISSUE.
388 EPIDEMIOLOGICAL STUDY FOR CASES WITH IRREVERSIBLE HYPOXIC ENCEPHALOPATHY
AND BRAIN DEATH
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Ethics/End of Life/Palliative Care 1
PUBLISHING NUMBER
389 VARIABILITY IN END-OF-LIFE PRACTICE AMONG U.S. TERTIARY CARE PEDIATRIC
INTENSIVE CARE UNITS (PICUS)
390 USE OF ICU DURING END-OF-LIFE HOSPITALIZATIONS OF PATIENTS WITH DEMENTIA: A
POPULATION-BASED STUDY
391 THE IMPACT OF ADVANCED DIRECTIVES ON NON-SURVIVORS WHO ARE INTUBATED IN
THE EMERGENCY DEPARTMENT
392 IMPROVING ACCESS TO PALLIATIVE CARE SERVICES IN THE PEDIATRIC ICU
393 IMPACT OF A PEDIATRIC HOSPITAL ORGAN DONATION COMMITTEE ON OPO REFERRAL
AND CONSENT
394 OUTCOME EXPECTATIONS AND GOALS OF CARE AMONG MDS, RNS, AND FAMILY
SURROGATES FOR CCI ADULTS
395 UTILIZATION OF PALLIATIVE CARE CONSULTS IN CIRRHOTIC PATIENTS IN THE MICU
396 RESOURCE UTILIZATION DURING END-OF-LIFE HOSPITALIZATIONS AMONG DEMENTIA
PATIENTS ADMITTED TO ICU
397 IS THE ICU/STEP-DOWN UNIT AN APPROPRIATE TRIAGE LOCATION FOR THE
PRESPECIFIED DNR-DNI PATIENT?
398 NURSES' PERSPECTIVE ON END OF LIFE ISSUES
Poster Session: Ethics/End of Life/Palliative Care 2
PUBLISHING NUMBER
399 THE CRITICAL ILLNESS MORTALITY INFLECTION POINT DURING PROLONGED SURGICAL
ICU LENGTH OF STAY
400 VALIDATION OF A PEDIATRIC BEDSIDE TOOL TO PREDICT TIME TO DEATH AFTER
WITHDRAWAL OF LIFE SUPPORT
401 ORGAN DONATION: A VALUES EXPLORATION EXERCISE
402 EFFICACY OF THE “SURPRISE” QUESTION TO PREDICT 6-MONTH MORTALITY IN ICU
PATIENTS
403 PALLIATIVE CARE CONSULTATION AND END-OF-LIFE CARE IN AN ONCOLOGIC ICU
404 PRE-DEPLOYMENT POST-TRAUMATIC STRESS DISORDER IN MILITARY TRAUMA CARE
PROVIDERS
405 DECISION-MAKING AUTHORITY FOR CPR AND VA-ECMO: PHYSICIAN ATTITUDES AND
ETHICAL IMPLICATIONS
406 THE UNCLEAR TEMPORAL BOUNDARIES OF PEDIATRIC CPR: IMPLICATIONS FOR MORAL
DISTRESS AND INTEGRITY
407 THE PROTECTIVE ROLE OF RELIGIOSITY IN EMERGENCY CARE
408 APRN-LED PRIMARY PALLIATIVE CARE IN THE MEDICAL ICU
409 HAVE A HEART! WHAT MOTIVATES ORGAN DONATION
Poster Session: GI/Hepatic 1
PUBLISHING NUMBER
410 PROTON PUMP INHIBITORS AND THE RISK FOR HOSPITAL-ACQUIRED CLOSTRIDIUM
DIFFICILE IN ICU PATIENTS
411 ALCOHOL RELATED ADMISSIONS TO ICU: AN 18 MONTH PROSPECTIVE COHORT STUDY
412 WARFARIN IN PATIENTS WITH LIVER CIRRHOSIS AND ATRIAL FIBRILLATION WORTH THE
RISK?
413 SERUM IFNΓ INCREASES FOLLOWING ENTERAL IL-23 ADMINISTRATION
414 PREDICTION OF OUTCOME IN ACUTE PANCREATITIS: A PROSPECTIVE STUDY ON SCORES
AND SINGLE PARAMETERS
415 ACUTE KIDNEY INJURY AND MORTALITY IN ACUTE MESENTERIC ISCHEMIA: A COHORT
STUDY
416 EVALUATION OF THE USE OF STEROIDS IN CIRRHOTIC PATIENTS WITH SHOCK
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
417 GASTRIC ACID SUPPRESSANT PROPHYLAXIS: CURRENT PRACTICE IN PEDIATRIC
INTENSIVE CARE
418 IMPACT OF ACUTE HYPERGLYCEMIA IN BRAIN-DEAD DONORS AS A RISK FACTOR FOR
STEATOSIS IN LIVER GRAFTS
419 ROLE OF PLATELET TRANSFUSION IN GASTROINTESTINAL BLEEDING IN PATIENTS ON
ANTI-PLATELET THERAPY
Poster Session: GI/Hepatic 2
PUBLISHING NUMBER
420 ASSOCIATION BETWEEN TRALI AND MASSIVE TRANSFUSION FOR GASTROINTESTINAL
BLEEDING IN A TERTIARY MICU
421 EMERGENCE OF ACUTE GI ILLNESS IN PREDISPOSITION, INSULT, RESPONSE, OUTCOMES
(PIRO) SEPSIS MODEL
422 A SYSTEMATIC REVIEW: CONTINUOUS REGIONAL ARTERIAL INFUSION FOR SEVERE
ACUTE PANCREATITIS
423 USE OF PCC IN PATIENTS WITH VARICEAL BLEEDING REQUIRING MASSIVE TRANSFUSION
424 HISTOPATHOLOGIC ANALYSIS OF AUTOPSY FINDINGS OF CHILDREN WITH ESLD
AWAITING TRANSPLANTATION
425 THE HIGH-THROUGHPUT DNA SEQUENCING REVEALS DYNAMIC CHANGE OF GUT
MICROBIOTA IN ICU PATIENTS
426 IMPACT OF A STRESS ULCER PROPHYLAXIS GUIDELINE AND EDUCATION ON ACID
SUPPRESSIVE THERAPY IN THE ICU
427 ELECTROMAGNETIC GUIDED CONFIRMATION OF NASOGASTRIC TUBE INSERTION
428 SAFETY OF GASTEROINTESTINAL ENDOSCOPIC PROCEDURES IN OCTOGENERIANS AND
NONAGENERIANS—A PILOT STUDY
429 EVALUATION OF RIFAXIMIN THERAPY FOR HEPATIC ENCEPHALOPATHY IN THE MEDICAL
INTENSIVE CARE UNIT
430 THE ECONOMIC IMPACT OF A STRESS ULCER PROPHYLAXIS PHARMACY PROGRAM
TARGETING INAPPROPRIATE THERAPY
Poster Session: Hematology 1
PUBLISHING NUMBER
431 EFFICACY AND SAFETY OF 4-FACTOR PROTHROMBIN COMPLEX CONCENTRATE IN
PATIENTS WITH LIVER DISEASE
432 DIC (DISSEMINATED INTRAVASCULAR COAGULATION) STATUS ON ADMISSION INCREASES
ICU MORTALITY
433 THE ROLE OF NUCLEATED RED BLOOD CELLS AS AN EARLY MARKER FOR INTENSIVE
CARE UNIT ADMISSION
434 RISK-STRATIFIED THROMBOPROPHYLAXIS DECREASES VENOUS THROMBOEMBOLISM IN
LONG GAP ESOPHAGEAL ATRESIA
435 EVALUATION OF IGG VERSUS IGG/IGM/IGA PF4 ELISA FOR DIAGNOSIS OF HIT AND
ARGATROBAN USAGE
436 PROTHROMBIN COMPLEX CONCENTRATE PLUS LOW-DOSE FACTOR VIIA FOR BLEEDING
AND REVERSAL OF COAGULOPATHY
437 A COMPARISON OF INR REVERSAL BETWEEN 4-FACTOR AND 3-FACTOR PROTHROMBIN
COMPLEX CONCENTRATES
438 PROSPECTIVE EVALUATION OF A BIVALIRUDIN DOSING NOMOGRAM FOR HEPARININDUCED THROMBOCYTOPENIA
439 THROMBOCYTOPENIA ASSOCIATED WITH CONTINUOUS RENAL REPLACEMENT THERAPY
IN CRITICALLY ILL PATIENTS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Hematology 2
PUBLISHING NUMBER
440 PREVALENCE ESTIMATES OF CPR AND ASSOCIATED OUTCOMES IN CHILDREN
HOSPITALIZED DUE TO LEUKEMIAS IN USA
441 SAFETY AND EFFECTIVENESS OF 3- VS 4-FACTOR PCC IN PATIENTS REQUIRING
EMERGENT WARFARIN REVERSAL
442 CONSEQUENCES OF TREATING FALSE POSITIVE HEPARIN-INDUCED
THROMBOCYTOPENIA
443 EVALUATION OF HEPARIN RESISTANCE IN PATIENTS OUTSIDE OF THE OPERATING ROOM
444 PERIPHERALLY INSERTED CENTRAL CATHETER (PICC) ASSOCIATED THROMBOSIS IN ICU
VERSUS NON-ICU SETTINGS
445 PREVALENCE, PREDICTORS AND OUTCOMES OF CPR IN HOSPITALIZED ADULT LEUKEMIC
PATIENTS.
446 UPPER EXTREMITY DVT AND PLATELETS: SHOULD THE CLINICAL THRESHOLD FOR
THROMBOCYTOSIS BE REDEFINED?
447 LIBERAL OR RESTRICTIVE BLOOD PRODUCT TRANSFUSION TRIGGERS IN AORTOCORONARY BYPASS SURGERY?
448 EVALUATION OF EPOETIN ALFA FOR PREVENTION OF BLOOD TRANSFUSIONS IN A
PEDIATRIC INTENSIVE CARE UNIT
Poster Session: Hematology 3
PUBLISHING NUMBER
449 OBESITY AND RISK OF THROMBOEMBOLISM IN CRITICALLY ILL MEDICAL PATIENTS
RECEIVING CHEMOPROPHYLAXIS
450 SNAKEBITE DOES CAUSE DISSEMINATED INTRAVASCULAR COAGULATION
451 VENOUS THROMBOSIS IN THE NEONATAL INTENSIVE CARE UNIT
452 IMPACT OF ORAL HEALTH ON OUTCOMES IN CHILDREN HOSPITALIZED DUE TO
LEUKEMIAS
453 MASSIVE BLEEDING ENSUES HYPERFIBRINOLYTIC DISSEMINATED INTRAVASCULAR
COAGULATION IN DROWNING VICTIMS
454 EFFICACY AND SAFETY OF THE NOVEL ORAL ANTICOAGULANTS DABIGATRAN,
RIVAROXABAN AND APIXABAN
455 REVERSAL OF FACTOR XA INHIBITORS-INDUCED ANTICOAGULATION IN HEALTHY
SUBJECTS BY ANDEXANET ALFA
456 PLATELET TRANSFUSION THRESHOLDS AMONG CHILDREN ADMITTED TO A PEDIATRIC
INTENSIVE CARE UNIT
457 TLR4- AND TLR9- MEDIATED IMMUNE TOLERANCE AND CROSS-TOLERANCE IS
ATTENUATED BY IL-7
Poster Session: Hematology 4
PUBLISHING NUMBER
458 VENOUS THROMBOEMBOLISM PROPHYLAXIS QUANDARY: OBESE POPULATION
459 DOSE-ADJUSTED ENOXAPARIN FOR VENOUS THROMBOEMBOLISM PROPHYLAXIS IN
TRAUMA PATIENTS
460 ELEVATED RISK OF THOMBOEMBOLIC EVENTS AFTER NOVEL ANTICOAGULATION
REVERSAL PROTOCOL
461 FOUR FACTOR PROTHROMBIN COMPLEX CONCENTRATE: ONE YEAR EXPERIENCE
462 SAFETY AND EFFICACY OF EARLY VENOUS THROMBOEMBOLISM PROPHYLAXIS IN
PATIENTS WITH ACUTE SPINAL INJURY
463 EVALUATION OF THE USE OF NOVEL ORAL ANTICOAGULANTS IN A MEDICAL INTENSIVE
CARE UNIT
464 VENOUS THROMBOEMBOLISM PROPHYLAXIS IN PATIENTS POST LIVER TRANSPLANT
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
465 HEPARIN INDUCED THROMBOCYTOPENIA IN EXTRACORPOREAL LIFE SUPPORT: A
SYSTEMATIC REVIEW OF ARGATROBAN
466 RED CELL DISTRIBUTION WIDTH (RDW) AS PREDICTOR OF HOSPITAL MORTALITY IN
CRITICALLY ILL PATIENTS
467 EPIDEMIOLOGY OF DEEP VENOUS THROMBOSIS IN A MIXED NEUROSCIENCES INTENSIVE
CARE UNIT
Poster Session: Infectious Disease 1
PUBLISHING NUMBER
468 HIGH-DOSE VERSUS STANDARD DOSE OSELTAMIVIR FOR TREATMENT OF SEVERE
INFLUENZA IN ADULT ICU PATIENTS
469 IMPACT OF ANTIBIOTIC SETTING OF PROCALCITONIN ORDERING ON PROVIDER ACTIONS
IN MEDICAL INTENSIVE CARE
470 CHARACTERISTICS OF INCREASED INCIDENCE OF NECROTIZING ENTEROCOLITIS IN A
CARDIAC INTENSIVE CARE UNIT
471 EFFICACY OF INDUCTION THERAPY OF CRYPTOCOCCAL MENINGITIS IN HIV INFECTED
ADULTS: A META-ANALYSIS
472 TREATMENT COMPARISONS IN CMV INFECTED IMMUNOCOMPROMISED PATIENTS: A
META-ANALYSIS
473 COST-EFFECTIVENESS OF 6 TREATMENTS FOR PRIMARY CLOSTRIDIUM DIFFICILE
INFECTION IN AN ICU POPULATION
474 INVESTIGATION OF A SEASONAL CLUSTER OF ACINETOBACTER BAUMANII INFECTIONS
IN A SURGICAL ICU
475 PROCALCITONIN GUIDED ANTIBIOTIC THERAPY IN THE PICU–A RANDOMIZED
CONTROLLED TRIAL
476 COLISTIN: THE SAFETY AND EFFICACY OF A LOADING DOSE, HIGH DOSE MAINTENANCE
REGIMEN
Poster Session: Infectious Disease 2
PUBLISHING NUMBER
477 IMPACT OF ORAL HEALTH ON OUTCOMES IN PATIENTS HAVING STEM CELL
TRANSPLANTS IN UNITED STATES.
478 FUNCTIONAL CHARACTERISTICS OF CD4+CD25+FOXP3+ REGULATORY T CELLS IN
PATIENTS WITH SAP
479 MRSA-COVERAGE DE-ESCALATION PRACTICES IN PATIENTS WITH VENTILATORASSOCIATED PNEUMONIA
480 VALUE OF MRSA NASAL SWAB SCREENING FOR PREDICTING INVASIVE MRSA
RESPIRATORY INFECTION
481 EVALUATION OF PROCALCITONIN UTILIZATION IN SEPTIC PATIENTS IN AN ACADEMIC
INTENSIVE CARE UNIT
482 ISOLATION OF VIRUSES IN SEVERE COMMUNITY-ACQUIRED PNEUMONIA: A PROSPECTIVE
COHORT STUDY
483 INCIDENCE OF THE NEUROLOGICAL MANIFESTATIONS OF DENGUE FEVER
484 CHARACTERISTICS AND OUTCOMES OF CRITICALLY ILL CANCER PATIENTS INFECTED
WITH ACINETOBACTER BAUMANNII
485 INFECTION WITH MULTIPLE RESPIRATORY VIRUSES MAY INCREASE MORTALITY
Poster Session: Infectious Disease 3
PUBLISHING NUMBER
486 SUSTAINED REDUCTION IN NOSOCOMIAL BLOODSTREAM INFECTIONS IN THE ICU
SETTING
487 REDEFINING FUNGUS IN ECMO: INFECTION AND COLONIZATION DO NOT DIFFER
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
488 CLINICAL MARKERS FOR DIFFERENTIATION OF VIRAL ENCEPHALITIS FROM ACUTE
DISSEMINATED ENCEPHALOMYELITIS
489 MODULATION OF THE ANTIVIRAL RESPONSE THROUGH THE LINEAR UBIQUITIN CHAIN
ASSEMBLY COMPLEX (LUBAC)
490 IMPACT OF THE JOINT COMMISSION PNEUMONIA CORE MEASURES ON ANTIBIOTIC USE
IN THE EMERGENCY DEPARTMENT
491 2009 H1N1 AND SEASONAL INFLUENZA INFECTION: ICU COURSE AND OUTCOMES
492 REAL-WORLD ANTIBIOTIC TREATMENT PATTERNS IN MECHANICALLY VENTILATED
PNEUMONIA PATIENTS
493 HEALTHCARE-ASSOCIATED INFECTIONS AND CHLORHEXIDINE BATHING – A PRAGMATIC
CLUSTER-RANDOMIZED TRIAL
494 PROVIDERS' PERCEPTIONS OF AN ANTIMICROBIAL STEWARDSHIP PROGRAM AT AN
ACADEMIC INSTITUTION
Poster Session: Infectious Disease 4
PUBLISHING NUMBER
495 CASTILE SOAP AS AN INTERVENTION IN CATHETER-ASSOCIATED URINARY TRACT
INFECTION PREVENTION
496 IMPACT OF COMBINATION GRAM-NEGATIVE ANTIBIOTICS ON EMPIRIC ANTIBIOTIC
APPROPRIATENESS IN THE PICU
497 CRITICAL ILLNESS ASSOCIATED WITH PANDEMIC (2009) VS. POST-PANDEMIC (2013)
INFLUENZA A (H1N1)
498 CNS PHARMACOKINETICS OF ANTITUBERCULOUS AGENTS IN TUBERCULOUS
MENINGITIS
499 SEVERE ADENOVIRAL RESPIRATORY INFECTION IN IMMUNOCOMPROMISED CHILDREN
500 MANAGEMENT OF STAPHYLOCOCCUS AUREUS BACTEREMIA THROUGH PHARMACIST
PROSPECTIVE EVALUATION
501 A COMMUNITY HOSPITAL'S EXPERIENCE WITH PROCALCITONIN: REDUCTION IN THE USE
OF ANTIBIOTICS
502 DESIGNING A NEW CANDIDA SCORING SYSTEMS IN PATIENTS ADMITTED TO THE
INTENSIVE CARE UNITES
503 VANCOMYCIN CONTINUOUS VERSUS INTERMITTENT INFUSION DURING CONTINUOUS
VENOVENOUS HEMOFILTRATION
Poster Session: Infectious Disease 5
PUBLISHING NUMBER
504 THE V-PROJECT: VANCOMYCIN DOSING AND THERAPEUTIC MONITORING IN ADULTS
505 CLINICAL PHARMACIST INTERVENTIONS WITH PROCALCITONIN WHILE PERFORMING
ANTIBIOTIC STEWARDSHIP
506 DISPROPORTIONATE RATES OF HIV PREVALENCE DUE TO DEMOGRAPHIC DIFFERENCES;
INPATIENT TRAUMA TESTING.
507 EFFICACY OF EXTENDED-INFUSION CEFEPIME AND MEROPENEM IN TRAUMA AND BURN
INTENSIVE CARE UNIT PATIENTS
508 INFLUENCE OF COLISTIN DOSE ON GLOBAL CURE IN PATIENTS WITH GRAM-NEGATIVE
BACTEREMIA
509 HIGH MELD SCORE AND COMMON ICU PARAMETERS: PREDICTING OUTCOMES WITH
INFECTED CIRRHOTIC PATIENTS
510 QUANTITATIVE POLYMERASE CHAIN REACTION FOR EARLY DIAGNOSIS OF METHICILLINRESISTANT STAPHYLOCOCCUS A
511 DIRECT CSF ANTIMICROBIALS IN THE TREATMENT OF CNS INFECTIONS: A SYSTEMATIC
REVIEW
512 FACTORS INFLUENCING ANTIBIOTIC ACTIONS AFTER PROCALCITONIN RESULT: A CASE
CONTROL STUDY
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Neuroscience 1
PUBLISHING NUMBER
513 SUBARACHNOID HEMORRHAGE AND PUPILLARY ABNORMALITIES ON ADMISSION
514 MANAGEMENT OF SEVERE, RESISTANT ALCOHOL WITHDRAWAL WITH OR WITHOUT THE
ADDITION OF PROPOFOL
515 ACCUMETRICS BASED CLOPIDOGREL DOSING IN ENDOVASCULAR NEUROSURGERY
516 ABCG2 RS2231142 C.421C>A IS ASSOCIATED WITH OUTCOMES FOLLOWING SEVERE
TRAUMATIC BRAIN INJURY
517 ANTI-APOPTOTIC SIGNALING IN BRAIN INDUCED BY PERIODIC ACCELERATION (PGZ)
AFTER HYPOXIC INJURY
518 COGNITIVE TESTING OUTCOMES AFTER MILD TRAUMATIC BRAIN INJURY
519 AN ANIMAL MODEL OF ANEURYSMAL SUBARACHNOID HEMORRHAGE
520 CLINICAL AND LABORATORY PREDICTORS OF OUTCOME IN PATIENTS WITH HERPES
SIMPLEX ENCEPHALITIS
521 ADULT STATUS EPILEPTICUS : EPIDEMIOLOGICAL AND CLINICAL STUDY IN THE MEDICAL
INTENSIVE CARE UNIT
522 OS-1, AN ORAL REHYDRATION SOLUTION, IMPROVES THERMOREGULATION IN A MOUSE
HEATSTROKE MODEL
Poster Session: Neuroscience 2
PUBLISHING NUMBER
523 BRAIN DEATH CONFIRMATION ON EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO):
A NOVEL TECHNIQUE
524 FACTORS ASSOCIATED WITH ELEVATED VANCOMYCIN DOSING IN NEUROCRITICAL CARE
PATIENTS
525 IV TREATMENT WITH ARGININE-VASOPRESSIN RECEPTOR BLOCKER VAPRISOL REDUCES
ISCHEMIA-EVOKED BRAIN EDEMA
526 EFFICACY & SAFETY: INTRAVENOUS SODIUM VALPROATE AND PHENYTOIN IN STATUS
EPILEPTICUS
527 MINOCYCLINE DELAYS RECOVERY IN A MODEL OF PEDIATRIC TRAUMATIC BRAIN INJURY
528 BLOOD PRESSURE ELEVATION AFTER THROMBOLYSIS IN ACUTE ISCHEMIC STROKE
PATIENTS
529 ALTERED CALCIUM HOMEOSTASIS IS ASSOCIATED WITH EKG ABNORMALITIES IN
EXPERIMENTAL STATUS EPILEPTICUS
530 QUANTITATIVE IMAGING BIOMARKERS OF BRAIN EDEMA AFTER 23% SALINE IN LIVER
FAILURE
531 TO PREDICT THE OUTCOME USING BISPECTRAL INDEX IN PATIENTS WITH SEVERE
TRAUMATIC BRAIN INJURY
532 STUDY INTOXICATION AS A PREDICTOR OF MORTALITY IN PATIENTS WITH SEVERE
MULTIPLE TRAUMA
Poster Session: Neuroscience 3
PUBLISHING NUMBER
533 IMPACT OF DELAYED PLASMA STORAGE ON BRAIN INJURY BIOMARKER STABILITY
534 EFFICACY OF AN ERYTHROPOIETIN – MIMETIC PEPTIDE ( ARA290) IN EXPERIMENTAL
TRAUMATIC BRAIN INJURY
535 A THERAPEUTIC PROTOCOL OF ACUTE INTERMITTENT HYPOXIA DOES NOT PROMOTE
INFLAMMATION IN THE RAT CNS
536 SERIAL MEASUREMENTS OF AUDITORY BRAINSTEM RESPONSE CAN PREDICT PATIENT
OUTCOMES WITH MORE PRECISION
537 HEMODYNAMIC SLOPE PLAYS A KEY ROLE IN REVERSING CLINICAL VASOSPASM AFTER
SUBARACHNOID HEMORRHAGE
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
538 PAIN BEHAVIORS IN BRAIN-INJURED ICU PATIENTS AT VARYING LEVELS OF
CONSCIOUSNESS
539 SAFETY FIRST: CARBOGEN AND CAPNOGRAPHY USE MINIMIZES COMPLICATIONS DURING
APNEA TESTING
540 DEPRESSED HEART RATE VARIABILITY PREDICTS OUTCOME IN PATIENTS WITH
SUBARACHNOID HEMORRHAGE
541 PSYCHOLOGICAL PROFILE OF NEUROSCIENCE INTENSIVE CARE UNIT PATIENTS BY
HIGHEST MOBILITY STATUS
542 VASOPRESSORS DOES NOT IMPROVE OUTCOMES OF DELAYED CEREBRAL ISCHEMIA
AFTER SUBARACHNOID HEMORRHAGE
Poster Session: Neuroscience 4
PUBLISHING NUMBER
543 NEUROTELEMETRY: REMOTE CEEG MONITORING AND READING FOR NEUROCRITICAL
CARE PATIENT MANAGEMENT
544 PREDICTORS OF FUNCTIONAL OUTCOME AFTER SUBDURAL HEMATOMA: A PROSPECTIVE
STUDY
545 PREDICTORS OF HIGH HOSPITAL COSTS AFTER SUBDURAL HEMATOMA
546 THE ROLE OF TRANSCRANIAL DOPPLER SONOGRAPHY IN DIAGNOSIS OF BRAIN DEATH: A
SINGLE CENTER STUDY
547 EARLY EFFECTS OF ENTERAL UREA ON INTRACRANIAL PRESSURE IN HYPONATREMIC
PATIENTS WITH BRAIN INJURY
548 THE EFFECT OF PROGESTERONE ON MICROGLIAL ACTIVATION IN A RAT MODEL OF
PEDIATRIC TBI
549 PREDICTORS OF MORTALITY OF IN-HOSPITAL PATIENTS WITH ISQUEMIC STOKE
550 CAN ADJUSTED PHENYTOIN CONCENTRATION ACCURATELY PREDICT FREE
CONCENTRATION?
551 IMPACT OF AGE ON PERFUSION IN PATIENTS WITH MYOCARDIAL INJURY AFTER
SUBARACHNOID HEMORRHAGE
552 THE IMPACT OF DONOR HOSPITAL MANAGEMENT ON ORGAN DONATION OUTCOMES
Poster Session: Neuroscience 5
PUBLISHING NUMBER
553 TREATMENT WITH HYPERTONIC SALINE ALTERNATING WITH MANNITOL IN NEUROLOGIC
EMERGENCIES
554 THE IMPACT OF EMERGENCY ROOM SEDATION ON ICU OUTCOMES
555 SIMPLIFYING THE CALCULATION OF OPTIMAL CEREBRAL PERFUSION PRESSURE
WITHOUT CONTINUOUS WAVEFORMS
556 CLEVIDIPINE VS. NICARDIPINE FOR INTENSIVE BLOOD PRESSURE CONTROL IN
HEMORRHAGIC STROKE
557 CEREBRAL BLOOD FLOW CHANGES WITH INCREASED INTRACRANIAL PRESSURE TO
DETECT CONCUSSION IN ATHLETES
558 CLINICAL UTILITY OF BRAIN INJURY MARKERS IN TBI CLINICAL TRIALS:FINDINGS FROM
THE INTREPID2566 TRIAL
559 A PCC-BASED REVERSAL PROTOCOL IS ASSOCIATED WITH REDUCED MORTALITY IN
WARFARIN-ASSOCIATED ICH
560 IV ACETAMINOPHEN USE AND ASSOCIATED OUTCOMES IN NEUROCRITICAL CARE
PATIENTS
561 RATE OF TRACHEOSTOMY IN PATIENTS WITH INTRAPARENCHYMAL HEMORRHAGE
562 THE EFFECTS OF ASPHYXIA ON CEREBROVASCULAR AUTOREGULATION IN NEWBORN
PIGLETS 24 HOURS AFTER INJURY
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Neuroscience 6
PUBLISHING NUMBER
563 RESPIRATORY MUSCLE CHANGES IN NEUROCRITICAL PATIENTS: EFFECT OF MV, AGE,
OBESITY AND VOLUME STATUS
564 DELAYED INR REVERSAL FOR PATIENT TRANSFER BETWEEN HOSPITALS LEADS TO
INTRACRANIAL HEMATOMA EXPANSION
565 OPTIMIZATION OF CLOPIDOGREL LOADING DOSE IN PATIENTS UNDERGOING CAROTID
STENT PLACEMENT
566 USE OF BISPECTRAL INDEX FOR MONITORING SEDATION IN THERAPEUTICALLY
PARALYZED PATIENTS
567 DATA QUALITY IN NEUROINTENSIVE CARE DATASETS
568 ACUTE NEUROLOGICAL INJURY MONITORING WITH EQUANOX (ANIME) STUDY
569 EFFECT OF SODIUM AND FLUID ON SERUM SODIUM LEVELS IN PATIENTS WITH
INTRACRANIAL HYPERTENSION
570 SEVERE ALCOHOL WITHDRAWAL SYNDROME (AWS): MANAGEMENT OF
167 PATIENTS: IMPACT OF ADJUNCTIVE THERAPY
571 SAFETY PROFILE OF DESMOPRESSIN IN PATIENTS WITH ACUTE INTRACRANIAL
HEMORRHAGE
572 POLYNITROXYLATED PEGYLATED HEMOGLOBIN:A SMALL VOLUME RESUSCITATION
SOLUTION FOR TBI PLUS HS
Poster Session: Neuroscience 7
PUBLISHING NUMBER
573 LONG-TERM SEQUELAE IN PEDIATRIC TRAUMATIC BRAIN INJURY
574 NEUROINFLAMMATION AND MICROGLIAL RESPONSE IN PEDIATRIC CNS TUBERCULOSIS
575 EVALUATION OF PUPILLARY DIAMETER IN THE SETTING OF PEDIATRIC DEATH
576 OUTCOME IS ASSOCIATED WITH TYPE OF NEUROLOGIC DISEASE DURING SPECIALIZED
TRANSPORT OF CHILDREN
577 TRANSCRANIAL DOPPLER MONITORING FOR NEUROLOGIC INJURY IN PEDIATRIC ECMO
578 DEVELOPMENT OF A NOVEL ANIMAL MODEL OF INFLICTED CHILDHOOD NEUROTRAUMA
IN IMMATURE RATS
579 INTRACRANIAL HEMORRHAGE AFTER CARDIOPULMONARY BYPASS FOR CORRECTION OF
CONGENITAL HEART DISEASE
580 SECONDARY BRAIN INSULTS DURING INTERFACILITY TRANSPORT AFTER PEDIATRIC
TRAUMATIC BRAIN INJURY
581 NEUROINFLAMMATION PERSISTS BEYOND ACUTE INJURY AFTER PEDIATRIC HYPOXICASPHYXIC CARDIAC ARREST
Poster Session: Neuroscience 8
PUBLISHING NUMBER
582 AUTOIMMUNE STATUS EPILEPTICUS IN CHILDREN
583 INFANTS WITH TRAUMATIC INTRACRANIAL HEMORRHAGE AT HIGH RISK FOR SEIZURES
584 CONTINUOUS ELECTROENCEPHALOGRAPHY FOR SEIZURE DETECTION IN CHILDREN:
WHO SHOULD WE MONITOR?
585 EVALUATING THE TRANSITION FROM DEXMEDETOMIDINE TO CLONIDINE FOR PAD
MANAGEMENT IN THE ICU
586 PREADMISSION SMOKING AND INFLAMMATION AND DELIRIUM IN ICU PATIENTS
587 DELIRIUM IN MECHANICALLY-VENTILATED INTENSIVE CARE PATIENTS: EFFECT OF
SEDATION AND RISK FACTORS
588 SOCIETAL GUIDELINES EFFECT CHANGE: IMPLEMENTATION OF THE SCCM PAIN,
AGITATION, DELIRIUM (PAD) BUNDLE
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
589 IMPACT OF A COLLABORATIVE MULTIDISCIPLINARY TEAM ON ICU DELIRIUM
590 EVALUATION OF AN ICU PAIN, AGITATION AND DELIRIUM PROTOCOL IN A LARGE
ACADEMIC HEALTH SYSTEM
Poster Session: Neuroscience 9
PUBLISHING NUMBER
591 THE SEDATIVE EFFECT OF PROPRANOLOL ON CRITICALLY ILL PATIENTS
592 SEDATION VARIABILITY INCREASES INCIDENCE OF DELIRIUM IN ADULT MEDICAL
INTENSIVE CARE UNIT PATIENTS
593 QUETIAPINE FOR DELIRIUM PROPHYLAXIS IN HIGH-RISK CRITICALLY ILL PATIENTS
594 SUPPLEMENTAL MELATONIN AND DELIRIUM IN THE INTENSIVE CARE UNIT: A
RETROSPECTIVE STUDY
595 MULTIPLE BENZODIAZEPINES USED IN SEVERE ALCOHOL WITHDRAWAL OR ALCOHOLRELATED DELIRIUM TREMENS
596 DEVELOPING DELIRIUM EXPERTS - AN ALTERNATIVE APPROACH TO NURSING
EDUCATION
597 EVALUATION OF THE EFFECTIVENESS OF TRAINING FOR THE CAM-ICU ASSESSMENT BY
THE NURSES IN THE ICU
598 PHYSICIAN ORDER ENTRY IMPLEMENTATION EFFECTS ON SEDATION/ANALGESIA
ASSESSMENT IN SURGICAL TRAUMA ICU
599 NEAR INFARED SPECTROSCOPY MONITORING DURING PROPOFOL SEDATION
Poster Session: Patient and Family Support 1
PUBLISHING NUMBER
600 IMPROVING THE ICU PATIENT EXPERIENCE: THE C4 (CRITICAL CARE COLLABORATION
AND COMMUNICATION) PROJECT
601 A NOVEL METHOD OF OPTIMIZING PATIENT AND FAMILY CENTERED CARE IN THE ICU
602 COMMUNICATION PRACTICES BETWEEN PEDIATRIC ICU PHYSICIANS AND ENGLISH AND
SPANISH-SPEAKING FAMILIES
603 USABILITY AND ACCEPTABILITY TESTING OF AN IPAD COMMUNICATION APPLICATION IN
THE INTENSIVE CARE UNIT
604 ETHNIC AND CULTURAL DIFFERENCES DO NOT IMPACT ON PARENTAL SATISFACTION IN
THE PICU
605 COMMUNICATION DURING PEDIATRIC INTENSIVE CARE UNIT (PICU) FAMILY
CONFERENCES (FCS)
606 EFFECT OF MOBILE APPLICATION PROVIDING INFORMATION SUPPORT ON SATISFACTION
OF ICU PATIENT FAMILIES
607 DESCRIPTIVE EXPERIENCES OF SURGICAL CRITICAL CARE BY PATIENTS AND
CAREGIVERS FOLLOWING DISCHARGE
Poster Session: Patient and Family Support 2
PUBLISHING NUMBER
608 COMPARING SATISFACTION WITH CARE BETWEEN FAMILIES OF DECEASED AND
SURVIVING PATIENTS IN A NEURO ICU
609 THE IMPACT OF A STRUCTURED ICU DIARY PROGRAM ON REDUCING BARRIERS TO DIARY
UTILIZATION
610 TO COMMUNICATE WITH RELATIVES; AN EVALUATION OF INTERVENTIONS IN THE
INTENSIVE CARE UNIT
611 PACIENTE A SEMI-STRUCTURED INTERVIEW ENHANCES FAMILY COMMUNICATION IN
THE ICU
612 ICU FAMILY ANGER AND ANXIETY: A PILOT PROJECT IN SELF-REPORTED OUTCOMES BY
PATIENT FAMILIES.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
613 DESIGN OF A COMMUNICATION PORTAL IN THE INTENSIVE CARE UNIT: SURVEYS OF
POTENTIAL STAKEHOLDERS
614 DEVELOPING PATIENT AND FAMILY CENTERED CARE THROUGH AN ICU PATIENT AND
FAMILY ADVISORY COUNCIL
615 FAMILY PRESENCE ON ROUNDS DOES NOT IMPACT EFFICIENCY OF ROUNDS IN A
PEDIATRIC INTENSIVE CARE UNIT
616 A QUALITATIVE STUDY EXPLORING THE IMPACT OF ALCOHOL USE DISORDERS ON
RECOVERY FROM ICU
Poster Session: Pharmacology 1
PUBLISHING NUMBER
617 PHARMACOKINETICS (PK) OF DAPTOMYCIN (DAP) IN CRITICALLY ILL TRAUMA PATIENTS
618 INHALED EPOPROSTENOL VS INHALED NITRIC OXIDE FOR ACUTE PULMONARY
HYPERTENSION AFTER CARDIAC SURGERY
619 PROTON PUMP INHIBITORS VERSUS HISTAMINE-2 RECEPTORS BLOCKERS IN
PREVENTING GASTROINTESTINAL BLEEDING
620 ANTIPSYCHOTIC PRESCRIBING PATTERNS DURING AND AFTER CRITICAL ILLNESS IN A
TERTIARY MEDICAL CENTER
621 COMPARATIVE EFFECTS OF NORADRENALINE AND LEVOSIMENDAN IN AN
EXPERIMENTAL HEMORRHAGIC SHOCK MODEL
622 DOES QTC PROLONGATION OCCUR AFTER INITIATION OF HALOPERIDOL OR QUETIAPINE
IN THE CRITICALLY ILL?
623 IMPACT OF A NATIONAL CALCIUM GLUCONATE SHORTAGE IN ICU PATIENTS RECEIVING
PARENTERAL NUTRITION
624 PREVALENCE AND FACTORS ASSOCIATED WITH ABSENCE OF VENOUS
THROMBOEMBOLISM PROPHYLAXIS
625 LOW DOSES OF DEXMEDETOMIDINE PLAY A PROTECTIVE ROLE IN KETAMINE-INDUCED
PROLIFERATION INHIBITION
626 PHARMACOKINETIC ANALYSIS OF ONCE-DAILY VANCOMYCIN DOSING DURING
CONTINUOUS RENAL REPLACEMENT THERAPY
Poster Session: Pharmacology 2
PUBLISHING NUMBER
627 PROBENECID INCREASES N-ACETYLCYSTEINE BRAIN LEVELS: IMPLICATIONS FOR BRAINDIRECTED THERAPEUTICS
628 VANCOMYCIN DOSING NOMOGRAM FOR SURGICAL INTENSIVE CARE PATIENTS
629 EVALUATION OF LIPOSOMAL BUPIVACAINE FOR PAIN MANAGEMENT AFTER TOTAL KNEE
ARTHROPLASTY
630 ASSESSING BLEEDING ASSOCIATED WITH COMBINED USE OF SSRI AND DUAL
ANTIPLATELET THERAPY
631 METHYLNALTREXONE VERSUS NALOXONE FOR OPIOID-INDUCED CONSTIPATION IN THE
MEDICAL INTENSIVE CARE UNIT
632 PHARMACOLOGIC CONTROL OF SUBARACHNOID HEMORRHAGE HEADACHE: ANALYSIS OF
PAIN INTENSITY DIFFERENCE
633 PHARMACOKINETICS OF LEVOFLOXACIN IN CRITICALLY-ILL PATIENTS RECEIVING
CONTINUOUS HEMODIAFILTRATION
634 IMPLICATIONS OF ATYPICAL ANTIPSYCHOTIC PRESCRIBING IN THE INTENSIVE CARE
UNIT
635 CONTINUOUS INFUSION VANCOMYCIN VIA INSTILLATION OF VANCOMYCIN INTO THE
DIALYSATE SOLUTION
636 HEMODYNAMIC DISTURBANCES IN EMERGENT RAPID SEQUENCE INTUBATION USING
PROPOFOL OR ETOMIDATE
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Pharmacology 3
PUBLISHING NUMBER
637 ASSESSMENT OF MEDICATION ASSOCIATED HYPOTENSION REQUIRING INTERVENTION
IN THE PICU.
638 EVALUATION OF THE USE OF KETAMINE FOR ACUTE PAIN IN THE EMERGENCY
DEPARTMENT
639 CLINICAL OUTCOMES OF ADJUNCTIVE KETAMINE FOR MANAGING ALCOHOL
WITHDRAWAL SYNDROME
640 COMPARISON OF CONTINUOUS INFUSIONS OF MIDAZOLAM AND PENTOBARBITAL FOR
REFRACTORY STATUS EPILEPTICUS
641 COMPARISON OF TWO GUIDELINE BASED PAIN AND AGITATION PROTOCOLS IN
MECHANICALLY VENTILATED PATIENTS
642 NMDA ANTAGONIST INTERFERES WITH DIFFERENTIATION OF MO INTO DC
643 PHARMACOECONOMIC ANALYSIS OF INHALED EPOPROSTENOL VS NITRIC OXIDE FOR
SEVERE, REFRACTORY ARDS
644 THIOCYANATE ACCUMULATION IN CRITICALLY ILL PATIENTS RECEIVING
NITROPRUSSIDE INFUSIONS
645 CONTINUATION OF QUETIAPINE THERAPY AT TRANSITIONS OF CARE IN AN ACADEMIC
ICU
646 A MULTICENTER EVALUATION OF EVIDENCE SUPPORTING ICU OFF-LABEL MEDICATION
USE
Poster Session: Pharmacology 4
PUBLISHING NUMBER
647 IMPACT OF AN ANALGESIA-BASED SEDATION PROTOCOL ON MECHANICALLY
VENTILATED PATIENTS IN A MEDICAL ICU
648 EFFICACY OF REDOSING PROPHYLACTIC ANTIBIOTICS FOR PROLONGED SURGERIES
649 POPULATION PHARMACOKINETICS OF MEROPENEM IN A PEDIATRIC ICU POPULATION
650 RETROSPECTIVE EVALUATION OF DEXMEDETOMIDINE TO FACILITATE MECHANICAL
VENTILATION EXTUBATION
651 PROPOFOL AND DEXMEDETOMIDINE DIFFERENTIALLY IMPACT TLR RESPONSES OF
HUMAN DCS AND MONOCYTES
652 UPLC-MS/MS METHOD FOR ASSESSING PHENYTOIN AND LEVETIRACETAM
CONCENTRATIONS IN PEDIATRIC CA PATIENTS
653 FACTORS AFFECTING VANCOMYCIN USE IN THE PEDIATRIC INTENSIVE CARE UNIT
654 TRANSITION FROM DEXMEDETOMIDINE TO ENTERAL CLONIDINE FOR ICU SEDATION: A
PILOT STUDY
655 EXTENDED INTERVAL FONDAPARINUX FOR VTE PROPHYLAXIS IN CRITICALLY ILL
PATIENTS WITH RENAL FAILURE
Poster Session: Pharmacology 5
PUBLISHING NUMBER
656 RISE AND SHINE: USING A STANDARDIZED SEDATION ORDERSET TO PROMOTE ABCDE
COMPLIANCE
657 RISK FACTORS FOR ADVERSE HEMODYNAMIC EFFECTS WITH DEXMEDETOMIDINE
658 THE PHARMACOKINETICS OF ETOMIDATE IN NEONATES AND INFANTS WITH
CONGENITAL HEART DISEASE
659 PROVIDER USE OF DEXMEDETOMIDINE FOR PEDIATRIC PROCEDURAL SEDATION
660 SEDATION FOR CHILDREN WITH MODERATE TO SEVERE TBI: REMIFENTANIL
661 FASTING FOR PEDIATRIC PROCEDURAL SEDATION AND THE RISK OF COMPLICATIONS.
662 BOLUS VS BOLUS+INFUSION USE OF DEXMEDETOMIDINE FOR PEDIATRIC MRI SEDATION
663 CHARACTERIZATION OF TOLERANCE IN CRITICALLY-ILL CHILDREN RECEIVING
FENTANYL CONTINUOUS INFUSIONS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
664 INTRANASAL DEXMEDETOMIDINE AS A PRIMARY PEDIATRIC PROCEDURAL SEDATION
MEDICATION
665 DEXMEDETOMIDINE IS EFFECTIVE FOR SEDATING YOUNG CHILDREN AND PATIENTS
WITH AUTISM FOR EEG
Poster Session: Pulmonary 1
PUBLISHING NUMBER
666 HYPERBARIC OXYGEN THERAPY: HOW SAFE IS IT FOR CRITICALLY ILL PATIENTS?
667 CORTICOSTEROID USE IN PEDIATRIC ARDS IS ASSOCIATED WITH NON-SURVIVAL AND
FEWER VENTILATOR-FREE DAYS
668 PERFORMANCE OF OXYGEN SATURATION INDEX AMONG ADULTS WITH TYPE I
RESPIRATORY FAILURE
669 PRESSURE ATTENUATION ACROSS AN ETT DURING CHFO WITH THE METANEB® SYSTEM
IN A PEDIATRIC LUNG MODEL
670 CLINICAL EQUIPOISE IN UTILIZATION OF ECLS IN PEDIATRIC CRITICAL CARE
PRACTITIONERS
671 EXTRACORPOREAL CARBON-DIOXIDE REMOVAL IS FEASIBLE USING A ZERO
BICARBONATE DIALYSATE
672 IMPLEMENTATION OF AN ICU EARLY MOBILITY PROGRAM USING THE CUSP MODEL: A
MULTI-DISCIPLINARY APPROACH
673 THE EFFECTS OF EXTRACT FROM JATROPHA CURCAS L. ON FIBROPROLIFERATION AFTER
ALI/ARDS INJRUY
674 SEVERE THINNESS (BMI<16KG/M2) IS ASSOCIATED WITH MORTALITY IN COMMUNITYACQUIRED PNEUMONIA
Poster Session: Pulmonary 2
PUBLISHING NUMBER
675 LUNG DECELLULARIZATION IN A RODENT VENO-ARTERIAL EXTRACORPOREAL
MEMBRANE OXYGENATION (ECMO) MODEL
676 OUTCOMES OF PATIENTS ADMITTED WITH SICKLE CELL CRISIS REQUIRING INVASIVE
MECHANICAL VENTILATION
677 RESPIRATORY VOLUME MONITORING: EARLY WARNING OF RESPIRATORY DEPRESSION &
IDENTIFYING FALSE ALARMS
678 MECHANICS OF IN VITRO HIGH-FREQUENCY OSCILLATORY VENTILATION
679 TAILORED VENTILATION IN MORBID OBESE PATIENTS.
680 RISK FACTORS FOR DEATH FROM VENTILATOR-ASSOCIATED PNEUMONIA IN THE UNITED
STATES FROM 2008-2011
681 NONINVASIVELY DETERMINED WORK OF BREATHING DURING NONINVASIVE PRESSURE
SUPPORT: VALIDATION STUDY
682 DEFINING “FLOW STARVATION” IN VOLUME CONTROL MECHANICAL VENTILATION
683 TISSUE INFLAMMATION IN AWAKE SHEEP SUBJECTED TO EXTRACORPOREAL ACID LOAD
CO2 REMOVAL (ALCO2R)
684 SAFETY AND FEASIBILITY OF PATIENT-CONTROLLED SEDATION (PCS) IN VENTILATED ICU
PATIENTS
Poster Session: Pulmonary 3
PUBLISHING NUMBER
685 ASSESSMENT OF CDC VENTILATOR ASSOCIATED CONDITION CRITERIA IN HIGH RISK
PEDIATRIC PATIENTS
686 WHEN PULMONARY ARTERIAL HYPERTENSION IS NOT ARTERIAL
687 PENTRAXIN 3 AS A NOVEL BIOMARKER OF LUNG INJURY;EVIDENCE FROM A HUMAN ONELUNG VENTILATION MODEL
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
688 IMPACT OF BRONCHOSCOPY ON OUTCOMES IN STEM CELL TRANSPLANT RECIPIENTS
WITH RESPIRATORY FAILURE
689 RETROSPECTIVE ANALYSIS OF SYSTEMIC AND CATHETER-DIRECTED THROMBOLYSIS FOR
PULMONARY EMBOLISM
690 MICROVASCULAR REACTIVITY IS ALTERED IN ARDS PATIENTS
691 CLINICAL OUTCOMES OF RESPIRATORY EXTRACORPOREAL LIFE SUPPORT IN ELDERLY
PATIENTS WITH SEVERE ARDS
692 LIBERATION FROM VENTILATION: A MULTIDISCIPLINARY TEAM STREAMLINES THE
PROCESS FOR EARLIER EXTUBATION
693 INHALED NITRIC OXIDE VERSUS INHALED EPOPROSTENOL FOR THE ACUTE
MANAGEMENT OF PULMONARY HYPERTENSION
694 TRANSFUSION IMPACTS THE ASSOCIATION BETWEEN ABO BLOOD TYPE AND RISK OF
ARDS
Poster Session: Pulmonary 4
PUBLISHING NUMBER
695 SYSTEMIC VERSUS INHALED CORTICOSTEROIDS IN COPD EXACERBATION: A
META-ANALYSIS
696 IMPROVEMENT IN OUTCOMES THROUGH A PROGRESSIVE UPRIGHT MOBILITY PROGRAM
IN CANCER PATIENTS
697 THREE CAPNOGRAPHY METHODS FOR DIAGNOSIS OF PULMONARY EMBOLISM: A
META-ANALYSIS
698 SKELETAL MUSCLE ULTRASOUND AS A TOOL TO ASSESS MUSCLE FUNCTION
699 OUTCOMES IN PATIENTS WITH ACUTE PE AND IVC FILTER PLACEMENT: A CASE-CONTROL
STUDY
700 DIFFUSE ALVEOLAR HEMORRHAGE (DAH) DURING NOVEL ANTICOAGULANT USE AND
POSITIVE AUTOIMMUNE SCREEN
701 A RETROSPECTIVE SINGLE CENTER ANALYSIS OF INHALED EPOPRESTONOL IN ARDS
PATIENTS
702 ANGIOTENSIN-CONVERTING ENZYME INHIBITOR (ACEI) INDUCED ANGIOEDEMA IN THE
INTENSIVE CARE UNIT (ICU)
703 PATIENTS ON ECMO WITH H1N1 HAVE GOOD OUTCOMES DESPITE HIGHER RESOURCE
UTILIZATION
Poster Session: Pulmonary 5
PUBLISHING NUMBER
704 ECMO FOR PEDIATRIC RESPIRATORY FAILURE: FACTORS AFFECTING MORTALITY AMONG
VARYING CENTER VOLUMES
705 NASAL HIGH-FLOW OXYGEN THERAPY VS NON-INVASIVE VENTILATION FOR
POSTOPERATIVE RESPIRATORY FAILURE
706 PEEP DETERMINED BY OPTIMAL STATIC COMPLIANCE IN THE ACUTE RESPIRATORY
DISTRESS SYNDROME (ARDS)
707 OPTOACOUSTIC ASSESSMENT OF ENDOTRACHEAL TUBE POSITIONING
708 DEFINING “FLOW STARVATION” IN VOLUME CONTROL MECHANICAL VENTILATION
709 HIGH TIDAL VOLUME VENTILATION IS EQUALLY INJURIOUS IN THE PEDIATRIC AND
ADULT LUNG
710 USE OF TRANSEOSOPHAGEAL DOPPLER IN GUIDING WEANING FROM MECHANICAL
VENTILATION IN CARDIAC PATIENTS
711 EXOSOMES SECRETED BY MESENCHYMAL STEM CELLS PREVENT HYPEROXIA-INDUCED
LUNG INJURY IN NEWBORN RAT
712 APPLICATION OF AIRWAY PRESSURE RELEASE VENTILATION BEFORE LUNG INJURY
PREVENTS PROGRESSION TO ARDS
713 COMPARISON OF INHALED EPOPROSTENOL TO INHALED NITRIC OXIDE: A NONINFERIORITY STUDY
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Pulmonary 6
PUBLISHING NUMBER
714 PRESSURE VERSUS VOLUME CONTROL VENTILATION: A PHYSIOLOGIC-BASED
SYSTEMATIC REVIEW AND META-ANALYSIS
715 INITIAL DISCHARGE PLANNING IMPACTS THE RATES OF READMISSION TO THE ICU IN
PATIENTS WITH SEVERE COPD
716 IMPROVED OXYGENATION AFTER CRITICAL CARE TRANSPORT IN PATIENTS WITH
HYPOXEMIC RESPIRATORY FAILURE
717 ASSOCIATION OF PULMONARY HYPERTENSION AND MORTALITY IN PATIENTS WITH
VENTILATOR ASSOCIATED EVENTS
718 EFFICACY STUDY OF A NOVEL DEVICE TO CLEAN THE ENDOTRACHEAL TUBE
719 IMPROVEMENT OF MECHANICAL VENTILATION IN OBESE PATIENTS AFTER
PERCUTANEOUS DILATATIONAL TRACHEOSTOMY
720 SUSTAINING RESPIRATORY THERAPIST ENGAGEMENT IN ICU LIBERATION
721 INCIDENCE AND MORTALITY OF POST-LUNG RESECTION LUNG INJURY OVER TIME; A
META-REGRESSION ANALYSIS
722 ANEMIA AND MORTALITY IN COPD PATIENTS REQUIRING INVASIVE MECHANICAL
VENTILATION
Poster Session: Pulmonary 7
PUBLISHING NUMBER
723 HIGH FREQUENCY OSCILLATION VENTILATION IN ACUTE RESPIRATORY DISTRESS
SYNDROME: A META-ANALYSIS
724 TIMING OF TRACHEOSTOMY IN UNSELECTED CRITICAL ILLNESS PATIENTS: FROM A
CHINA HOSPITAL REPORT
725 DYNAMICAL DENSITY PLOTS FOR THE DISPLAY OF RESPIRATORY PATTERNS DURING A
SPONTANEOUS BREATHING TRIAL
726 IDENTIFICATION OF ALPHA-1-ANTITRYPSIN DEFICIENCY BY STANDARDIZED SCREENING
IN A COMMUNITY HOSPITAL
727 SYSTEMIC SARCOIDOSIS AND MULTIPLE MYELOMA, RARE PRESENTATION
728 THE EFFECT OF AN EARLY MOBILITY PROTOCOL IN CRITICALLY ILL, MECHANICALLY
VENTILATED PATIENTS
729 NEUROMUSCULAR BLOCKADE IMPROVES TRACHEAL INTUBATION SUCCESS IN THE
INTENSIVE CARE UNIT
730 PROGNOSTIC FACTORS FOR ACUTE RESPIRATORY FAILURE TREATED WITH HIGHFREQUENCY OSCILLATORY VENTILATION
731 AUTOMATED BEDS FOR PRONE POSITION VENTILATION: NOT ALL IT’S MADE OUT TO BE
Poster Session: Pulmonary 8
PUBLISHING NUMBER
732 SEVERE HYPOXIA IN AN ASYMPTOMATIC PATIENT CAUSED BY PULMONARY
ARTERIOVENOUS MALFORMATION
733 CISATRACURIUM FOR ACUTE RESPIRATORY DISTRESS SYNDROME: PATTERNS OF
UTILIZATION
734 COMPARING THE CHARACTERISTICS AND OUTCOMES OF PATIENTS WITH UNPLANNED
EXTUBATION
735 EFFECT OF SELECTIVE Β BLOCKERS ON PATIENTS WITH NON CARDIAC ACUTE
HYPOXAEMIC RESPIRATORY FAILURE
736 72-HOUR CLINICAL PULMONARY INFECTION SCORE MAY HAVE PROGNOSTIC VALUE IN
TRAUMA PATIENTS WITH VAP
737 A UNIQUE CASE OF RECURRENT DIFFUSE ALVEOLAR DAMAGE (DAD) IN A CHRONIC
NARCOTIC USER
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
738 IMPACT OF SEVERITY OF HYPOXEMIA ON SHORT TERM MORTALITY IN MECHANICALLY
VENTILATED PATIENTS
739 TRYCYCLE: PRELIMINARY RESULTS OF EARLY IN-BED CYCLING WITH MECHANICALLY
VENTILATED PATIENTS
740 LUNG ULTRASOUND IN THE NEUROLOGICALLY DECEASED DONOR
Poster Session: Pulmonary 9
PUBLISHING NUMBER
741 PRETRANSPLANT EXTRACORPOREAL MEMBRANE OXYGENATION APPLICATION IN LUNG
TRANSPLANTATION
742 SILDENAFIL FOR ACUTE PULMONARY HYPERTENSION AFTER CARDIAC SURGERY
743 EFFECT OF EXTRACORPOREAL MEMBRANE OXYGENATION USE ON SEDATIVE
REQUIREMENTS DURING SEVERE ARDS
744 OUTCOMES FOLLOWING MECHANICAL VENTILATION OF SALICYLATE-POISONED
PATIENTS
745 ASSESSMENT OF A SEDATION TITRATION PROTOCOL FOR PATIENTS RECEIVING
MECHANICAL VENTILATION
746 SCAMP® DECREASED NEED FOR ESCALATION OF CRITICAL INTERVENTIONS IN
CHILDREN WITH ASTHMA
747 ASSOCIATION OF NUMBER OF TRACHEAL INTUBATION ATTEMPTS WITH OUTCOME IN
CRITICALLY ILL CHILDREN
748 SAFETY AND EFFICACY OF LUNG RECRUITMENT IN POST-OPERATIVE PEDIATRIC
CARDIAC SURGICAL PATIENTS
749 OUTCOMES FOR A RECENT COHORT OF CHILDREN NEEDING HIGH FREQUENCY
OSCILLATORY VENTILATION
Poster Session: Pulmonary 10
PUBLISHING NUMBER
750 NEBULIZED HYPERTONIC SALINE IN MECHANICALLY VENTILATED CHILDREN: A
RANDOMIZED, BLINDED PILOT STUDY
751 MORTALITY OF CHILDREN UNDERGOING EARLY OR LATE TRACHEOSTOMY VERSUS
PROLONGED MECHANICAL VENTILATION
752 RE-ADMISSION RISK FACTORS TO PICU IN CHILDREN WITH RESPIRATORY TRACT
DISEASES
753 HIGH FLOW NASAL CANNULA THERAPY IN PRETERM INFANTS: A POOLED ANALYSIS
754 USING PLETH VARIABILITY INDEX TO PREDICT ASTHMA SEVERITY IN CHILDREN
PRESENTING TO A PEDIATRIC ED
755 OPTOACOUSTIC DETECTION OF TRACHEAL TUBE DEPTH IN THE PEDIATRIC ICU
756 INEFFECTIVE TRIGGERING IN MECHANICALLY VENTILATED CHILDREN
757 HYPOTONIC FLUIDS AND HYPONATREMIA ARE ASSOCIATED WITH ADVERSE OUTCOMES
IN PEDIATRIC BRONCHIOLITIS
758 OXYGENATION AND VARYING INTERVALS OF FLUID BALANCE IN MECHANICALLY
VENTILATED CHILDREN
Poster Session: Pulmonary 11
PUBLISHING NUMBER
759 INHALED FLOLAN VERSUS INHALED VELETRI FOR REFRACTORY HYPOXEMIA IN
CRITICALLY ILL PATIENTS
760 DETERMINING OUTCOMES AMONG PEDIATRIC SURVIVORS OF RESPIRATORY
EXTRACORPOREAL LIFE SUPPORT
761 FLUID OVERLOAD AND OUTCOMES IN CRITICALLY ILL CHILDREN WITH BRONCHIOLITIS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
762 THE STUDY OF WEANING INFLUENCE FACTORS AND INDEXES IN CHILDREN
763 HIGH FLOW NASAL CANNULA IN CRITICALLY ILL INFANTS AND CHILDREN WITH
BRONCHIOLITIS AND PNEUMONIA
764 IMPLEMENTATION OF A HIGH FLOW NASAL CANNULA WEANING PROTOCOL IN THE
PEDIATRIC INTENSIVE CARE
765 STUDY OF AIRWAY IN NEONATES AND INFANTS UNDERGOING MRI OF HEAD AND NECK
766 CAN THE PULSE-OX VERSUS ARTERIAL SAO2 DIFFERENCE PREDICT MORTALITY IN
CRITICALLY ILL PEDIATRIC BONE
767 SURVEY OF INTENSIVE CARE MANAGEMENT OF RESPIRATORY FAILURE IN CHILDREN
WITH HSCT
Poster Session: Quality and Safety 1
PUBLISHING NUMBER
768 EVALUATION OF FOUR FACTOR PROTHROMBIN CONCENTRATE COMPLEX (PCC) USAGE
AND SAFETY AT A TERTIARY CARE
769 IMPROVING GLUCOSE CONTROL IN INTENSIVE AND INTERMEDIATE CARE UNITS USING A
LEAN SIX SIGMA APPROACH
770 STRESS ULCER PROPHYLAXIS UTILIZATION AND OVERUTILIZATION IN INTENSIVE CARE
UNITS FROM 2008 TO 2012
771 TEAM BASED PERFORMANCE IMPROVEMENT PROTOCOL INCREASED PATIENT
SATISFACTION
772 DISCOVERY & ACTION: BRINGING QUALITY IMPROVEMENT FROM THE CONFERENCE
ROOM TO THE BEDSIDE IN THE PICU
773 A NATIONAL APPROACH FOR MEASURING PERFORMANCE AND QUALITY IN PEDIATRIC
CRITICAL CARE
774 CLINICAL OUTCOMES OF NEUROCRITICAL CARE PATIENTS FOLLOWING A BED TRIAGE
WORKFLOW
775 DANGEROUSLY ELEVATED PEDIATRIC ENDOTRACHEAL CUFF PRESSURES AT ALTITUDE:
AN EX VIVO INVESTIGATION
776 COMPLIANCE WITH SPONTANEOUS BREATHING TRIAL PROTOCOL ASSOCIATED WITH
LOWER VAE RATES
Poster Session: Quality and Safety 2
PUBLISHING NUMBER
777 PHYSICIAN AND NURSE AGREEMENT OF PATIENT ISSUES
778 A MORE RAPID, RAPID RESPONSE.
779 URINARY CATHETER MANAGEMENT CORRELATES WITH CATHETER-ASSOCIATED
URINARY TRACT INFECTION-CAUTI IN ICU
780 IMPACT OF SEDATION AND AGITATION ON UNPLANNED EXTUBATIONS IN THE ICU
781 STRUCTURED ROUNDS IN THE MEDICAL ICU; AN INTERDISCIPLINARY IMPROVEMENT
PROJECT
782 FEASIBILITY OF A SAFE SEDATION CHECKLIST IN A PEDIATRIC SEDATION UNIT
783 AN AIRWAY RISK ASSESSMENT SCORE CAN IDENTIFY PEDIATRIC PATIENTS AT RISK FOR
UNPLANNED EXTUBATION
784 DIFFERENCES IN NURSE AND PHYSICIAN ASSESSED ICU ORGANIZATIONAL
CHARACTERISTICS
785 HIGH COMPLIANCE WITH A CLABSI-PREVENTION BUNDLE IS ASSOCIATED WITH A ZERO
RATE OF CLABSI
786 ADAPTING THE CDC’S NHSN VENTILATOR-ASSOCIATED CONDITION DEFINITION FOR
PEDIATRICS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Quality and Safety 3
PUBLISHING NUMBER
787 SEVERE TRACHEAL INTUBATION ASSOCIATED EVENTS IN PICU ARE INCREASED DURING
WEEKENDS BUT NOT NIGHTTIME
788 IMPLEMENTATION OF CAUTI PREVENTION PROTOCOL IN THE NEURO ICU LOWERS CAUTI
RATES AND LENGTH OF STAY
789 IMPACT OF A PEDIATRIC CHRONIC VENTILATOR UNIT ON A REGIONAL PEDIATRIC
INTENSIVE CARE UNIT
790 PERCEPTIONS OF HOSPITAL MEDICAL PERSONNEL ON DISASTER PREPAREDNESS
791 SAFETY ATTITUDES IN THE ICU: A COMPARISON OF THE PERCEPTIONS OF NURSES AND
PHYSICIANS
792 DEVICE RELATED PRESSURE ULCERS & PERCUTANEOUS TRACHEOSTOMY: TO SUTURE OR
NOT TO SUTURE
793 ROLE OF ADHERENCE TO GLUCOSE CHECK INTERVAL IN THE DEVELOPMENT OF
HYPOGLYCEMIA IN THE CRITICALLY ILL
794 RAPID RESPONSE TEAM TRIGGERS AND OUTCOMES IN ADULT MEDICAL AND SURGICAL
ONCOLOGY PATIENTS
795 THREE YEAR OUTCOMES OF A MEDICAL INTENSIVE CARE UNIT ACUTE CARE NURSE
PRACTITIONER (ACNP) SERVICE
796 CATEGORIZATION IN MECHANICALLY VENTILATED PEDIATRIC PATIENTS: A PROPOSED
METHOD TO IMPROVE QUALITY
Poster Session: Quality and Safety 4
PUBLISHING NUMBER
797 INTERPRETABLE ACTIVE LEARNING IN SUPPORT OF CLINICAL DATA ANNOTATION
798 HOW DOES ACTIGRAPHY CONTRIBUTE TO OUR UNDERSTANDING OF DELIVERED
ACTIVITY IN ICU PATIENTS?
799 STRATEGIES TO REDUCE URINARY CATHETER USAGE AND RATE OF CATHETERASSOCIATED URINARY TRACT INFECTIONS
800 BENCHMARKING ICU PERFORMANCE: THE ROLE OF FAMILY SATISFACTION
801 TELE-ICU INTERDISCIPLINARY CENTRAL LINE PROGRAM IMPROVES RESIDENT
COMPETENCY AND OUTCOMES
802 A PROSPECTIVE STUDY OF CRITICAL INCIDENT REPORTING IN AN INDIAN PEDIATRIC
INTENSIVE CARE UNIT
803 STRESS (SUBJECTIVE TRANSFER RISK EVALUATION SEVERITY SCORE) ACCURATELY
PREDICTS ICU READMISSION
804 NOISE LEVELS IN THE PICU AND STAFF PERCEPTION REGARDING EFFECT OF NOISE
EXPOSURE ON SLEEP QUALITY.
805 PRESSURE ULCER DEVELOPMENT IN ≤7 DAYS: ATTRIBUTABLE TO THE REFERRING
MEDICAL CENTER?
Poster Session: Quality and Safety 5
PUBLISHING NUMBER
806 AN ELECTRONIC ALGORITHM TO IDENTIFY VENTILATOR ASSOCIATED CONDITIONS, AND
REDUCE RN LABOR AND COST
807 DESATURATION DURING TRACHEAL INTUBATION: DOES THAT MATTER?
808 RADIATION EXPOSURE AMONG MEDICAL PROFESSIONALS WORKING IN THE INTENSIVE
CARE UNIT
809 TELEMEDICINE IMPROVES HOSPITAL SYSTEM COMPLIANCE WITH LUNG-PROTECTIVE
VENTILATING STRATEGIES
810 EVALUATING THE EFFECTIVENESS OF AN ABCDE BUNDLE IMPLEMENTATION PROGAM
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
811 AN OVERVIEW OF REGISTERED STUDIES IN CRITICAL CARE MEDICINE: ANALYSIS OF
CLINICALTRIALS.GOV REGISTRY
812 EVALUATION OF MOBILITY PRACTICE PATTERNS AND IDENTIFICATION OF BARRIERS TO
EARLY MOBILIZATION IN ICU
813 ADOLESCENT CARE IN ICU: EUROPEAN SOCIETY OF PAEDIATRIC AND NEONATAL
INTENSIVE CARE (ESPNIC) SURVEY
814 INTRA-TEAM COMMUNICATION OFTEN INTERRUPTS PATIENT CARE IN THE PEDIATRIC
INTENSIVE CARE UNIT
815 REDUCING THREE INFECTIONS AND IMPROVING CULTURE ACROSS CARDIAC SURGERY
UNITS
Poster Session: Quality and Safety 6
PUBLISHING NUMBER
816 DAILY SPONTANEOUS AWAKENING TRIAL IN THE SEDATED MECHANICALLY VENTILATED
PATIENT IN THE SURGICAL ICU
817 ROLE OF EICU TO MODIFY ANTIBIOTIC MISUSE IN THE DEVELOPING WORLD
818 OPTIMIZATION OF INTELLIGENT INFUSION PUMP TECHNOLOGY TO MINIMIZE
VASOPRESSOR PUMP PROGRAMING ERRORS
819 IMPROVING PATIENT INFORMATION TRANSFER FROM OR TO ICU: OBSERVATIONAL
ANALYSIS OF PRESENT PRACTICE.
820 REDUCTION OF NUISANCE ALARMS IN THE ICU
821 IMPLEMENTATION OF A VTE RISK ASSESSMENT TOOL AT A PEDIATRIC HOSPITAL
822 MISSED OPPORTUNITIES FOR INTERVENTION IN THE COMPREHENSIVE MANAGEMENT
OF ALCOHOL WITHDRAWAL SYNDROME
823 REDUCING IATROGENIC PHLEBOTOMY LOSSES IN CRITICALLY ILL CHILDREN
824 DIFFERENCES OF RAPID RESPONSE SYSTEM BETWEEN PATIENTS ADMITTED TO THE
SURGICAL AND MEDICAL SERVICES
825 ADULT ICU ON THE “QUEST FOR ZERO” INTERVENTIONS TO ELIMINATE CENTRAL LINE
BLOODSTREAM INFECTIONS
Poster Session: Quality and Safety 7
PUBLISHING NUMBER
826 A PRELIMINARY PSYCHOMETRIC TESTING OF THE CRITICAL-CARE PAIN OBSERVATION
TOOL IN CHINESE ADULTS
827 EFFECT OF PATIENT CONTROLLED ANALGESIA (PCA) ORDER SET TEMPLATES ON SAFETY
EVENTS REQUIRING NALOXONE
828 DEVELOPMENT AND VALIDATION OF A SKILL ASSESSMENT TOOL FOR MEDICAL
EMERGENCIES IN A SIMULATION CENTER
829 ASSESSMENT OF A HEMODYNAMIC INDICATOR OF IMPENDING OXYGENATOR FAILURE
830 QUALITY OF HAND-OFFS IN A PEDIATRIC INTENSIVE CARE UNIT
831 SAFETY OF A PHARMACY MANAGED INTRAVENOUS VANCOMYCIN LOADING DOSE
PROTOCOL
832 FUNCTIONING OF THE SAPS-3 INDEX IN PATIENTS ADMITTED FOR INTOXICATION IN
INTENSIVE CARE UNITS
833 THE HANDOFF CONTINUITY SCORE (HCS) CORRELATES WITH ROUNDING EFFICIENCY
834 PERIPHERALLY INSERTED CENTRAL CATHETER INSERTION USING VASCULAR
POSITIONING SYSTEMS IN CRITICAL CARE
835 DOES IT MATTER WHO INTUBATES PATIENTS? A COMPARISON OF ENDOTRACHEAL
INTUBATION PRACTICE PATTERNS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Quality and Safety 8
PUBLISHING NUMBER
836 DEVELOPING A COOPERATIVE COMMUNICATION SYSTEM FOR SAFE, EFFECTIVE, AND
EFFICIENT PATIENT CARE
837 IMPROVING PEDIATRIC SEPSIS CARE THROUGH COLLABORATION
838 CHARACTERISTICS OF CHILDREN WITH HOSPITAL ACQUIRED PRESSURE ULCERS IN AN
INTENSIVE CARE UNIT
839 EVALUATION OF VARIOUS VENTILATOR-ASSOCIATED INFECTION CRITERIA IN THE
PEDIATRIC ICU
840 OPTIMIZING CLINICAL DECISION SUPPORT USING PUSH NOTIFICATION OF SHOCK INDEX
IN A PICU
841 HYPOGLYCEMIA AND ADHERENCE TO AN INSULIN INFUSION PROTOCOL IN CARDIAC
SURGERY VS OTHER ICU PATIENTS
842 COST SAVINGS BY BUNDLING ENDOTRACHEAL AND GASTRIC INTUBATION AND AVOIDING
UNNECESSARY IMAGING
843 UNCONSCIOUS BIAS IN TRAUMA CARE PROVIDERS IN A MAJORITY LATIN AMERICAN, US
CITY
844 PATIENT ROUNDING AUDITS: VOLUNTEERS AS MEMBERS OF THE MICU QUALITY
IMPROVEMENT TEAM
845 EVALUATION OF PICU STAFF KNOWLEDGE OF PEDIATRIC DELIRIUM: A SURVEY STUDY
Poster Session: Quality and Safety 9
PUBLISHING NUMBER
846 ADHERENCE TO A NURSE-MANAGED PAIN, AGITATION, AND DELIRIUM PROTOCOL IS
FEASIBLE IN SICU PATIENTS
847 PERCEPTIONS OF UNDERSTANDING AND MEDICAL ERROR IN THE SURGICAL INTENSIVE
CARE UNIT
848 CAN 10$ A DAY SAVE LIVES? EICU IMPLEMENTATION REDUCES MORTALITY IN THE
DEVELOPING WORLD
849 PREVENTING PEDIATRIC VAPS BY PLACING ORAL CARE ON THE MEDICATION
ADMINISTRATION RECORD
850 CHOOSING WISELY: REDUCING CHEST X-RAYS IN THE SICU THROUGH RESIDENT
EDUCATION AND ELECTRONIC ORDERS
851 LEAN THINKING CAN REDUCE PROLONGED VENTILATION IN CARDIAC SURGERY
PATIENTS
852 APPRAISAL OF PEDIATRIC CRITICAL CARE FOR NORTHWESTERN NIGERIA
853 IMPLEMENTING CLINICAL PHARMACY SERVICES IN A MULTIDISCIPLINARY CRITICAL
CARE RECOVERY CENTER
854 VENTILATOR LIBERATION IN AN ICU WITH PERIPHERAL INTENSIVIST COVERAGE: A
QUALITY IMPROVEMENT PROJECT
855 CRISIS OF CRITICAL CARE COSTS IN A GERIATRIC TRAUMA POPULATION: 10-YEAR RURAL
TRAUMA SYSTEM ANALYSIS
Poster Session: Quality and Safety 10
PUBLISHING NUMBER
856 EFFECT OF AN OVERNIGHT “QUIET TIME” PROGRAM ON AMBIENT SOUND LEVELS IN THE
SURGICAL ICU
857 EVALUATION OF ROUNDING STRUCTURE IN A MEDICAL ICU BEFORE AND AFTER
ELECTRONIC ROUNDING TOOL IMPLEMEN
858 HEIGHT ACCURACY IN CRITICALLY ILL PATIENTS
859 RAPID RESPONSE SYSTEM ON MORE CRITICAL CONDITION IN LARGE HOSPITALS
COMPARED WITH SMALL HOSPITALS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
860 A FOCUSED, TIME-SENSITIVE DISCHARGE PROTOCOL FOR PREVENTING ICU
RE-ADMISSIONS IN SURGICAL PATIENTS
861 SAFELY SHIFTING SURGICAL ELECTIVE CASES TO AN INTERMEDIATE CARE UNIT FROM
AN INTENSIVE CARE UNIT
862 MEASURING ETT CARINA DISTANCE USING THE AIRWAVE DEVICE IN PATIENTS
IDENTIFIED AS A DIFFICULT AIRWAY
863 PROCESS TO REDUCE CATHETER ASSOCIATED URINARY TRACT INFECTIONS IN THE ICU
864 LONG TERM OUTCOMES IN A SURGICAL INTENSIVE CARE UNIT
865 EFFECT OF IV PHOSPHATE REPLETION GUIDELINE CHANGES IN VENTILATED PATIENTS
IN AN INTENSIVE CARE UNIT
Poster Session: Quality and Safety 11
PUBLISHING NUMBER
866 ENHANCING SAFETY AND IMPROVING CARE OF TRACHEOSTOMY AND LARYNGECTOMY
PATIENTS
867 PEDIATRIC DENTAL PROCEDURES: IS PROPOFOL A SAFE AND EFFECTIVE OPTION?
868 VENTILATOR ALARM MANAGEMENT–A QUALITY IMPROVEMENT PROJECT
869 MEDICAL READINESS FOR TRANSFER DOES NOT PREDICT ACTUAL PICU LENGTH OF STAY
870 EVALUATION OF PROTHROMBIN COMPLEX CONCENTRATE UTILIZATION AT A LARGE,
URBAN ACADEMIC MEDICAL CENTER
871 RELATIONAL COORDINATION: THE KEY TO ELIMINATING CLABSI IN THE SICU
872 IMPACT OF A DAILY MOBILITY HUDDLE ON PATIENT ACTIVITY LEVEL IN THE ICU
873 ASSESSMENT OF PARENTERAL NUTRITION APPROPRIATENESS AFTER IMPLEMENTATION
OF A QUALIFICATION CHECKLIST
874 IDENTIFYING PALLIATIVE CARE TRIGGERS & REASON FOR NOT CONSULTING SPECIALIST
IN CRITICAL CARE SETTING
875 “CHOOSING WISELY” TO IMPROVE PATIENT OUTCOMES AND HOSPITAL COSTS
Poster Session: Quality and Safety 12
PUBLISHING NUMBER
876 M&M CONFERENCE IN A HIGH VOLUME MICU: A PROCESS FOR TIMELY REVIEW AND
ACCURATE CLASSIFICATION
877 SUCCESSFUL REDUCTION OF CHEST RADIOGRAPHS IN A NEW YORK CITY PICU: RESULTS
OF A QUALITY IMPROVEMENT
878 EARLY GOAL DIRECTED THERAPY IN CRITICALLY ILL PATIENTS DECREASES HOSPITAL
LENGTH OF STAY
879 THE IMPLEMENTATION & IMPACT OF A MODIFIED WHO PROCEDURAL SEDATION SAFETY
CHECKLIST ON RISK REDUCTION
880 SAFETY OUTCOMES IN PATIENTS WHO ARE DEAF OR HAVE LIMITED ENGLISH
PROFICIENCY IN THE ICU
881 EVALUATION OF SEVERITY BY FOUR SCORING SYSTEMS IN CRITICALLY ILL PATIENTS
882 BAL CULTURE RESULTS ARE NOT SPECIFIC TO VAP IN MECHANICALLY VENTILATED
CHILDREN
883 DEVELOPMENT OF AN ICU COMMUNICATION TOOL BASED ON PROVIDER PERCEPTIONS
OF PATIENT SAFETY
884 EVALUATION OF AN UPDATED INSULIN INFUSION PROTOCOL AT A LARGE ACADEMIC
MEDICAL CENTER
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Quality and Safety 13
PUBLISHING NUMBER
885 COMPLICATIONS FROM CENTRAL VENOUS CATHETER PLACEMENT IN TWO LARGE
TERTIARY HOSPITALS
886 ADAPTING THE COMPREHENSIVE UNIT-BASED SAFETY PROGRAM TO IMPROVE PATIENT
OUTCOMES IN THE ICU
887 COHORT STUDY OF A COMPUTERIZED ALERT SYSTEM USED TO DETECT HYPERLACTEMIA
IN HIGH RISK PATIENTS
888 OUTCOMES OF A MULTI-PROFESSIONAL APPROACH TO REDUCING VENTILATOR LENGTH
OF STAY
889 COAPTIVE ULTRASOUND IS A NOVEL PROCEDURAL TECHNIQUE APPLICABLE IN ACUTE
CARE SETTINGS
890 PHYSICIANS’ KNOWLEDGE AND UTILIZATION OF PROCALCITONIN TESTING IN AN URBAN
COMMUNITY HOSPITAL
891 VARIATIONS IN MORNING ROUNDING TASKS AMONG CRITICAL CARE PROVIDERS IN TWO
ICUS
892 NURSE PERCEIVED BARRIERS TO TOPICAL ANALGESIA USE PRIOR TO VENIPUNCTURE
PROCEDURES IN PEDIATRICS
893 FUNCTIONAL ABILITY AFTER ACUTE CORONARY SYNDROME (ACS) WITH ST ELEVATION
894 PICU PROCEDURAL PAIN (PP) CLINICAL PRACTICE GUIDELINES (CPG): NURSING
PERCEPTIONS
Poster Session: Quality and Safety 14
PUBLISHING NUMBER
895 EFFECT OF A VENT WEANING PROTOCOL ON SELF EXTUBATION AND REINTUBATION
RATES IN THE SICU
896 VENOUS THROMBOEMBOLISM PREVENTION: AUTOMATING RISK ASSESSMENT &
CLINICAL DECISION SUPPORT IN THE EHR
897 THE ROCKET PROTOCOL - THE NEXUS OF EMERGENCY MEDICINE, HOSPITALIST
MEDICINE & CRITICAL CARE MEDICINE
898 USING PRE-HEALTH STUDENT VOLUNTEERS TO IMPLEMENT EARLY MOBILIZATION
THROUGH PASSIVE RANGE OF MOTION
899 PHYSICIAN ASSISTANT’S SAFETY ATTITUDES IN THE ICU: A DESCRIPTIVE ANALYSIS
900 SEVERITY-ADJUSTED MORTALITY AND PICU VOLUME: NOT A LINEAR RELATIONSHIP
901 IMPACT OF A SURGICAL INTENSIVIST TEAM ON ICU LENGTH OF STAY AND MORTALITY
902 PATIENT CHARACTERISTICS AND MORTALITY IN A NP-STAFFED ICU VS. A RESIDENT
-STAFFED ICU.
903 STAFFING CONCERNS WITH ADVANCED PRACTICE PROVIDERS IN THE ICU: STARTLING
FACTS
904 IMPLEMENTATION OF DAILY MULTIDISCIPLINARY ABCDE BUNDLE ROUNDS IN A
MEDICAL ICU
Poster Session: Quality and Safety 15
PUBLISHING NUMBER
905 SEDATION AND/OR ANALGESIA FOLLOWING EMERGENCY DEPARTMENT ENDOTRACHEAL
INTUBATION
906 ENGAGING STAFF THROUGH SOCIAL GAMIFICATION: DELIVERY OF MICROLEARNING TO
IMPROVE SAFETY AND QUALITY
907 COULD MORE PHASE 2 TRIALS AND COMPLEX ADAPTIVE TRIAL DESIGN SAVE LIVES IN
CRITICAL CARE TRIALS?
908 THE SIGNIFICANCE OF THE TREATMENT FOR THE ELDERLY EMERGENCY PATIENTS
REQUIRING INTENSIVE CARE
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
909 NURSE AND PATIENT INTERACTION BEHAVIORS AND NURSING CARE QUALITY OF
CRITICALLY ILL, OLDER ADULTS
910 THE EFFECT OF THE MEDICAL EMERGENCY TEAM IN PREVENTING THE DETERIORATION
OF INPATIENTS
911 CARD SORTS HELP “UNPACK” CLINICIAN PERSPECTIVES ON PATIENT CONDITION AND
TREATMENT PRIORITIES
912 INSERTION AND USE OF ARTERIAL CATHETERS: A NATIONAL SURVEY OF CLINICIAN
ANTISEPTIC TECHNIQUE
913 OUTCOMES OF CAUTI BUNDLE OPTIMIZATION: A MULTIDISCIPLINARY APPROACH
Poster Session: Renal 1
PUBLISHING NUMBER
914 EARLY AKI IS ASSOCIATED WITH PERSISTENCE OF OTHER ORGAN DYSFUNCTION AND
LATE DEATH IN THE PICU
915 IMPACT OF FLUID ACCUMULATION AND RENAL FUNCTION ON MORTALITY IN CHILDREN
RECEIVING ECMO
916 PROGNOSTIC VALUE OF NEPHROCHECK (URINARY [TIMP-2]*[IGFBP7]) IN A GENERAL ICU:
A PROSPECTIVE STUDY
917 ABO BLOOD TYPE IS ASSOCIATED WITH ACUTE KIDNEY INJURY IN CRITICALLY ILL
TRAUMA AND SEPSIS PATIENTS
918 EFFECT OF INTRAOPERATIVE ALBUMIN VS HES ON RENAL FUNCTION AFTER
ORTHOTOPIC LIVER TRANSPLANTATION
919 EFFECT OF ACUTE KIDNEY INJURY ON OUTCOMES IN CRITICALLY ILL CHILDREN WITH
BRONCHIOLITIS
920 HES, ANGIOTENSIN CONVERTING ENZYME INHIBITORS (ACEI) AND ACUTE KIDNEY
INJURY IN NON-CARDIAC SURGERY
921 SIMVASTATIN PROTECTS AGAINST OLEIC-ACID MEDIATED RENAL INJURY VIA
ACTIVATION OF THE HO-1 PROMOTER
922 IS RENAL REPLACEMENT THERAPY AN INDEPENDENT PREDICTOR OF LONG TERM
MORTALITY?
Poster Session: Renal 2
PUBLISHING NUMBER
923 EARLY FLUID RESUSCITATION OF END STAGE RENAL DISEASE PATIENTS WITH SEVERE
SEPSIS AND SEPTIC SHOCK
924 ASSOCIATION BETWEEN HIGHER COLISTIN DOSE AND NEPHROTOXICITY
925 ACUTE KIDNEY INJURY ACCORDING TO KDIGO IN CHILDREN UNDERGOING
CARDIOPULMONARY BYPASS
926 UTILITY OF SCREENING ECG IN ACUTE HYPERKALEMIA: LOW SENSITIVITY OF THE
USUAL FINDINGS
927 RENAL EFFECTS OF FENOLDOPAM ADMINISTRATION IN SEPTIC SHOCK
928 POSITIVE FLUID BALANCE IS A RISK FACTOR FOR ACUTE KIDNEY INJURY IN CRITICALLY
ILL PATIENTS
929 EXERCISE-INDUCED ACUTE KIDNEY INJURY IN RENAL HYPOURICEMIA CAUSED BY
NOVEL ALLELIC VARIANTS IN URAT1
930 THE COST OF VARYING DEGREES OF RENAL FAILURE IN A QUATERNARY CARE
UNIVERSITY HOSPITAL.
931 LOOP DIURETIC INFUSIONS WITH AND WITHOUT CONTINUOUS ALBUMIN INFUSIONS IN
ACUTE KIDNEY INJURY PATIENTS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Renal 3
PUBLISHING NUMBER
932 10-YEAR EXPERIENCE OF INFANT RENAL REPLACEMENT THERAPY (RRT) IN A SPECIALIST
CHILDREN’S HOSPITAL
933 NEPHROPATHY BY CONTRAST IN ACUTE CORONARY SYNDROME (ACS)
934 EVALUATION OF VANCOMYCIN DOSING AND CVVH INTENSITY ON VANCOMYCIN TROUGH
CONCENTRATIONS ATTAINMENT
935 HYDRATION FOR CONTRAST-INDUCED ACUTE KIDNEY INJURY PREVENTION: A
META-ANALYSIS
936 EARLY DETECTION OF NGAL IN PLASMA AND URINE TO ASSESS ACUTE RENAL FAILURE
IN PATIENTS AFTER CARDIAC
937 USE OF CONIVAPTAN AND TOLVAPTAN FOR THE TREATMENT OF HYPONATREMIA IN
CRITICALLY ILL ADULTS
938 INCIDENCE AND CHARACTERIZATION OF ACUTE RENAL FAILURE FOLLOWING
ACETAMINOPHEN OVERDOSE
939 INFLUENCE OF 6% HYDROXYETHYL STARCH 130/0.4 ON AKI AND TRANSFUSION
REQUIREMENTS IN CT SURGERY
Poster Session: Sepsis 1
PUBLISHING NUMBER
940 PHARMACOLOGICAL ACTIVATION OF AMPK IMPROVES CARDIAC DYSFUNCTION IN
EXPERIMENTAL SEPSIS IN MICE
941 RED CELL DISTRIBUTION WIDTH AND MICROCIRCULATION IN CRITICALLY ILL SEPTIC
PATIENTS
942 PREDICTIVE VALUE OF EARLY CHANGES OF MICROCIRCULATION IN ORGAN FAILURE OF
SEPTIC SHOCK PATIENTS
943 ECMO IN ARDS DUE TO INFLUENZA A H1N1 PNEUMONIA: A SINGLE-CENTER EXPERIENCE
DURING THE 2013-14 SEASON
944 CAROTID PEAK FLOW VARIATION AS A PREDICTOR OF VOLUME RESPONSIVENESS IN
SEPTIC SHOCK PATIENTS
945 PREVALENCE AND PREDICTORS OF SEPTICEMIA IN PATIENTS WHO UNDERWENT MAJOR
SURGICAL PROCEDURES IN USA
946 IMPACT OF HYDROCORTISONE ON ATRIAL FIBRILLATION IN SEPTIC SHOCK
947 DELIVERY OF SEPSIS 6 BY CRITICAL CARE OUTREACH ON THE GENERAL WARDS: IMPACT
ON OUTCOME
Poster Session: Sepsis 2
PUBLISHING NUMBER
948 FLUID RESUSCITATION IMPROVES SURVIVAL IN MURINE ENDOTOXEMIA
949 HIGHER MELD SCORES ARE ASSOCIATED WITH ELEVATED LACTATE LEVELS IN PATIENTS
WITHOUT SEVERE SEPSIS.
950 INITIAL LACTATE LEVEL AND LACTATE CLEARANCE AS A PREDICTOR OF IN-HOSPITAL
MORTALITY IN SEPTIC SHOCK
951 VASOPRESSOR RESPONSIVENESS TO HYDROCORTISONE SUPPLEMENTATION IN
VASOPRESSOR REFRACTORY SHOCK
952 ASSOCIATION OF LEFT VENTRICULAR STRAIN AND LACTATE AND MORTALITY IN SEPTIC
SHOCK.
953 EFFECT OF AN ELECTRONIC MEDICAL RECORD ALERT FOR SEVERE SEPSIS AMONG
EMERGENCY DEPARTMENT PATIENTS
954 CD4+ LYMPHOCYTES MEDIATE THE BENEFICIAL EFFECT OF EGF IN POLYMICROBIAL
SEPSIS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
955 FLUID BALANCE IN THE ICU–INTERVENTIONS TO MINIMIZE FLUIDS IN PATIENTS WITH
SEPTIC SHOCK
956 OBESITY ALTERS CARDIAC DYSFUNCTION IN SEPTIC MICE THROUGH THE STAT3
PATHWAY
Poster Session: Sepsis 3
PUBLISHING NUMBER
957 ANALYSIS OF OUTCOMES OF AN ALERT SYSTEM IMPLEMENTED TO SHORTEN ED LOS FOR
PATIENTS WITH SEPTIC SHOCK
958 METABOLOMIC ANALYSIS IN SEPSIS AND ARDS FUNDING SOURCE: 1R21HL117705-01,
5 K23 HL103842-03
959 RECOGNIZING INPATIENT SEPSIS EARLY (RISE) ON THE MEDICAL FLOORS
960 PREDICTING THE PROGRESSION TO SEPTIC SHOCK IN PATIENTS WITH A CANDIDA
BLOODSTREAM INFECTION
961 ACTIVATION OF AMP-ACTIVATED PROTEIN KINASE REDUCES LUNG INFLAMMATION IN A
MURINE MODEL OF SEPSIS
962 THE IMPACT OF BRAIN DYSFUNCTION IN SEPTIC PATIENTS: RESULTS FROM THE ICON
STUDY
963 TISSUE DYSOXIA AND MORTALITY IN SEPTIC SHOCK
964 PHARMACIST PRESENCE AND COMPLIANCE WITH THE 3 HOUR SEPSIS BUNDLE IN THE ED
965 IMMUNOSTIMULATORY OLIGODEOXYNUCLEOTIDE IMT504 PROTECTS NEUTROPENIC
ANIMALS FROM P.AERUGINOSA SEPSIS
Poster Session: Sepsis 4
PUBLISHING NUMBER
966 SEPSIS: AN INNOVATIVE ELECTRONIC WARNING SYSTEM FOR IN-HOSPITAL SCREENING
OF SEPSIS
967 EFFECTS OF MEANS OF STEROID DISCONTINUATION ON HYPOTENSION IN RESOLVED
SEPTIC SHOCK
968 ROLE OF MELANOCORTIN RECEPTOR AGONIST ON LPS-INDUCED NEUTROPHIL
ACTIVATION AND ACUTE LUNG INJURY
969 PRE-HOSPITAL IDENTIFICATION OF PATIENTS WITH SEVERE SEPSIS: DEVELOPMENT OF A
NOVEL PREDICTION SCORE
970 ASSOCIATION OF SEPSIS BUNDLE COMPLIANCE WITH IN-HOSPITAL DEATH
CONTROLLING FOR SEVERITY OF ILLNESS
971 PHARMACIST IMPACT ON TIME TO ANTIBIOTIC ADMINISTRATION IN SEPSIS PATIENTS IN
AN EMERGENCY DEPARTMENT
972 IMPACT OF AN IN-PATIENT ELECTRONIC CLINICAL DECISION SUPPORT TOOL ON SEPSISRELATED MORTALITY
973 TRANSCRIPTOME ANALYSIS DEMONSTRATES DIFFERENTIAL MRNA SPLICING PATTERNS
IN RESPONSE TO LPS
974 CHRONIC ALCOHOL INGESTION AFFECTS CD4 T CELL FUNCTION BUT NOT ACTIVATION IN
SEPSIS
Poster Session: Sepsis 5
PUBLISHING NUMBER
975 PLASMA GLUTATHIONE REDUCTASE ACTIVITY IS ASSOCIATED WITH THE PROGNOSIS OF
SEPTIC SHOCK
976 DETECTION OF MYOCARDIAL DYSFUNCTION WITH PRESERVED EJECTION FRACTION IN
SEPTIC SHOCK
977 EARLY LACTATE CLEARANCE CUT OFF AS PREDICTOR OF EARLY MORTALITY IN SEVERE
SEPSIS AND SEPTIC SHOCK
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
978 THE ASSOCIATION BETWEEN BLOOD GLUCOSE AND MATRIX-METALLOPROTEINASE-9 IN
EARLY SEVERE SEPSIS
979 SHOCK INDEX AS A PREDICTOR OF OUTCOMES IN PATIENTS WITH SEPTIC SHOCK
980 PRACTICES AND PERCEPTIONS OF ED AND ICU RNS REGARDING INITIAL IV ANTIBIOTIC
THERAPY FOR SEPTIC SHOCK
981 EVALUATION OF BURN SEPSIS AUTOMATED ALERTS IN AN INTENSIVE CARE UNIT
982 SEPTIC SHOCK-STEROID TREATMENT DECREASES A MARKER OF MICRO VASCULAR
LEAKAGE
Poster Session: Sepsis 6
PUBLISHING NUMBER
983 SENSITIVITY AND POSITIVE PREDICTIVE VALUE OF CERNER EMR BASED SEPSIS
RECOGNITION TOOL
984 REMOVAL OF CYTOMEGALOVIRUS FROM BLOOD BY HEPARIN-FUNCTIONAL
HEMOPERFUSION MEDIA
985 EVALUATION OF ENDOTHELIAL MICROPARTICLES IN SEPSIS INDUCED DIC TREATED BY
RECOMBINANT THROMBOMODULIN
986 OUTCOMES IN SEPTIC SHOCK PATIENTS TREATED WITH CONTINUOUS VERSUS BOLUS
STRESS-DOSE HYDROCORTISONE
987 RELATIONSHIP OF CEREBRAL PERFUSION PRESSURE VARIABILITY TO SEPSISASSOCIATED ENCEPHALOPATHY
988 SICKLE CELL ANEMIA PATIENTS PRESENTING TO AN EMERGENCY DEPARTMENT WITH
SEVERE SEPSIS OR SEPTIC SHOCK
989 ASSOCIATION OF HEMATOLOGIC PARAMETERS AND SEPSIS-INDUCED CARDIOMYOPATHY
990 CELLULAR LOCATION DICTATES THE PROLIFERATIVE RESPONSE OF INTESTINAL
EPITHELIAL CELLS IN SEPSIS
991 EMR-BASED SEPSIS ALERT: IMPROVING EARLY DETECTION
Poster Session: Sepsis 7
PUBLISHING NUMBER
992 ASSOCIATION OF CHANGE IN MEAN ARTERIAL PRESSURE PRE AND POST
RESUSCITATION AND AKI IN SEPTIC SHOCK
993 PROTECTIVE EFFECTS OF HEMIN ON THE SEPSIS-INDUCED SKELETAL MUSCLE
WASTING VIA UP-REGULATION OF HO-1
994 THE CLINICAL VALUE OF NEUTROPHIL EXTRACELLULAR TRAPS IN PNEUMONIA SEPSIS
995 A MULTIDISCIPLINARY EDUCATIONAL APPROACH TO DECREASING TIME TO ANTIBIOTIC
ADMINISTRATION IN SEPSIS
996 A COMPARISON OF APACHE II AND APACHE III SCORES IN PREDICTING MORTALITY OF
PATIENTS WITH SEPSIS
997 PROCALCITONIN LEVEL AND SOFA SCORE AT ICU DISCHARGE PREDICTS POST-ICU
MORTALITY
998 RHS-TM COULD HAVE A SYNERGISTIC EFFECT BOTH IN INFLAMMATION AND DIC IN
SEPSIS
999 WEIGHT-BASED DOSING OF VASOPRESSIN IN PATIENTS WITH SEPTIC SHOCK
1000 LONG-TERM ORGAN DYSFUNCTION AFTER SEVERE SEPSIS
Poster Session: Sepsis 8
PUBLISHING NUMBER
1001 IMPACT OF BODY MASS INDEX ON NOREPINEPHRINE REQUIREMENTS AND
HEMODYNAMICS IN SEPTIC SHOCK
1002 A COMPREHENSIVE TIME-BASED META-ANALYSIS OF SIRS AND SEPSIS REVEALS A
ROBUST DISCRIMINATORY GENE SET
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
1003 RISK FACTORS FOR MORTALITY IN SEPTIC PATIENTS WHO RECEIVED MULTIPLE
VASOPRESSORS
1004 EVALUATION OF ADHERENCE TO THE
2012 SURVIVING SEPSIS CAMPAIGN GUIDELINES AND ASSOCIATED OUTCOMES
1005 IMPACT OF GRM+ VS. GRM- ANTIBIOTIC INITIATION SEQUENCING ON VASOPRESSOR
REQUIREMENTS IN SEPTIC SHOCK
1006 LEVOSIMENDAN VS DOBUTAMINE IN SEPTIC SHOCK. SYSTEMATIC REVIEW AND
META-ANALYSIS
1007 DEVELOPMENT OF TELE-ICU MULTIDIMENSIONAL SEVERITY ADJUSTED PIRO SEPSIS
MODEL
1008 EFFECT OF ZINC SUPPLEMENTATION IN A MURINE MODEL OF STAPH AUREUS
SUPERINFECTION AFTER H1N1 INFLUENZA
1009 DETECTION OF SEVERE SEPSIS IN THE PRE-HOSPITAL SETTING: HOW ARE WE DOING?
Poster Session: Sepsis 9
PUBLISHING NUMBER
1010 THE EFFECTS OF CONTINUOUS BLOOD PURIFICATION ON PATIENTS WITH SEVERE
SEPSIS
1011 SEPSIS SEVERITY SCORE: A SYSTEMATIC REVIEW OF LITERATURE
1012 IMPLEMENTATION OF AN INTENSIVIST ALBUMIN STEWARDSHIP PROGRAM FOR SICU
PATIENTS WITH SEPTIC SHOCK
1013 ROLE OF ARTERIAL LINE IN SEPTIC SHOCK (R.A.S.S.)
1014 EFFECT OF EARLY INTRAVENOUS GLUCOSE ON OUTCOME OF SEPTIC SHOCK PATIENTS
BASED ON SEPSIS GUIDELINE
1015 PREVALENCE AND IMPACT OF SEPTICEMIA ON OUTCOMES IN HOSPITALIZED END STAGE
RENAL DISEASE PATIENTS.
1016 A "THREE DELAYS" MODEL FOR SEVERE SEPSIS IN RESOURCE-LIMITED SETTINGS
1017 FLECAINIDE ACETATE ATTENUATES ENDOTOXIN-INDUCED ACUTE LUNG INJURY IN A
RAT MODEL
1018 SIRT1 ACTIVATORS ALTER TRANSCRIPTIONAL PROFILES OF INFLAMMATORY RESPONSE
& IMPROVE OUTCOME IN SEPSIS
Poster Session: Sepsis 10
PUBLISHING NUMBER
1019 THE ROLE OF IP-10 IN LOCAL INFLAMMATORY ENVIRONMENT WITH SYSTEMIC
INFLAMMATORY RESPONSE SYNDROME
1020 EFFECT OF SEPTICEMIA ON OUTCOMES IN PATIENTS HAVING RENAL
TRANSPLANTATIONS IN USA
1021 THE ROLE OF CENTHAQUIN IN RESUSCITATION OF ENDOTOXIC SHOCK IN RATS
1022 MYOCARDIAL STRAIN CORRELATES WITH SHOCK SEVERITY IN PEDIATRIC SEPSIS
PATIENTS
1023 INCREASED RISK OF ONE-YEAR ALL-CAUSE MORTALITY AFTER PEDIATRIC SEVERE
SEPSIS
1024 OXIDATIVE STRESS IS ELEVATED IN THE PLASMA OF CRITICALLY ILL CHILDREN
1025 NEONATAL SEVERE SEPSIS: CURRENT TRENDS FROM THE PEDIATRIC HEALTH
INFORMATION SYSTEMS DATABASE
1026 ASSOCIATION BETWEEN CRP TREND AND MORTALITY IN PEDIATRIC SEPSIS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Surgery/Trauma/Burns 1
PUBLISHING NUMBER
1027 USEFULNESS OF BONE SCANNING IN THE DIAGNOSIS OF HIDDEN FRACTURE IN MAJOR
TRAUMA PATIENTS
1028 DISPARITY IN TRAUMA AND CRITICAL CARE FOR TRAUMATIC BRAIN INJURY IN ARIZONA
1029 TRANEXAMIC ACID FOR PEDIATRIC TRAUMA
1030 EMERGENT WARFARIN REVERSAL (EWR) COMPARING 3 COAGULATION FACTOR
PRODUCTS: PCC3, PCC4, LDRFVIIA
1031 SURVIVAL IMPROVEMENT BY ANTI-RAGE ANTIBODY ADMINISTRATION IN A RAT MODEL
OF CRUSH INJURY
1032 THE LUNG NEUTROPHIL TRANSCRIPTOME AFTER TRAUMA INFLUENCES THE WORSE
OUTCOMES OF THE OLD TO PNEUMONIA
1033 PREDICTION OF THE ROLE OF OPTIC NERVE SHEATH DIAMETER IN BRAIN EDEMA IN
PATIENTS WITH SEVERE TBI
1034 SURGICAL OUTCOMES OF COLONIC VOLVULUS
1035 HOMELESS AND IN SHOCK: MORBIDITY AND MORTALITY IN THE HOMELESS AFTER
TRAUMATIC HEMORRHAGIC SHOCK
Poster Session: Surgery/Trauma/Burns 2
PUBLISHING NUMBER
1036 A NEW STRATEGY FOR DIFFICULT AIRWAY MANAGEMENT WITH VISUAL NEEDLE
CRICOTHYROIDOTOMY: A MANIKIN STUDY
1037 EFFECT OF SCHEDULED ACETAMINOPHEN ON INTRAVENOUS OPIOID USE IN TRAUMA
PATIENTS
1038 IMPACT OF LATE FLUID BALANCE ON CLINICAL OUTCOMES IN CRITICALLY ILL
SURGICAL AND TRAUMA PATIENTS
1039 KETAMINE MAY INCREASE THE RISK OF PE IN SELECTED TRAUMA PATIENTS
1040 NIACIN ATTENUATES ACUTE LUNG INJURY INDUCED BY HEMORRHAGIC SHOCK IN RATS
1041 EXTRACORPOREAL MEMBRANE OXYGENATION USE IN PEDIATRIC HEMOPHAGOCYTIC
LYMPHOHISTIOCYTOSIS PATIENTS
1042 A NOVEL APPROACH TO DEVELOPMENT OF FREESTANDING TRAUMA CENTERS IN LATIN
AMERICA: RIO DE JANEIRO, BRA
1043 A RISK PREDICTION MODEL FOR POST-TRAUMATIC VENOUS THROMBOEMBOLISM
1044 INFECTION RELATED VENTILATOR ASSOCIATED CONDITIONS CAPTURE THE MINORITY
OF VAP IN TRAUMA PATIENTS
Poster Session: Surgery/Trauma/Burns 3
PUBLISHING NUMBER
1045 IMPACT OF EJECTION FRACTION ON THE RISK FOR POSTOPERATIVE INFECTIOUS AND
RENAL COMPLICATIONS
1046 HEALTHCARE SERVICES UTILIZATION IS ASSOCIATED WITH HOSPITAL READMISSION
FOR SURGICAL PATIENTS
1047 RESPIRATORY COMPLICATIONS IN TRAUMA PATIENTS STRONGLY ASSOCIATED WITH
CONTACT ISOLATION PRECAUTIONS
1048 ANALGESIA AND SEDATION IN MECHANICALLY-VENTILATED TRAUMA PATIENTS WITH A
HISTORY OF STIMULANT USE
1049 COMPLICATIONS ASSOCIATED WITH USE OF RHBMP IN CHILDREN HAVING SPINAL
FUSION PROCEDURES IN USA
1050 VENOUS THROMBOEMBOLISM PROPHYLAXIS IN CRITICALLY ILL SURGICAL PATIENTS
1051 ICP MONITORING IN CHILDREN: WHY ARE WE NOT ADHERING TO GUIDELINES?
1052 EARLY RESUSCITATIVE THORACOTOMY FOR CARDIAC ARREST: DOES AGE HAVE AN
IMPACT ON SURVIVABILITY?
1053 FACTORS AFFECTING INFECTIOUS COMPLICATIONS IN PATIENTS WITH GUNSHOT
WOUNDS TO THE PELVIS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Surgery/Trauma/Burns 4
PUBLISHING NUMBER
1054 ACIDOSIS DEVELOPMENT DURING FIRST BURN EXCISION INCREASES MORTALITY
1055 IMPACT OF PRIMARY BLAST LUNG INJURY DURING COMBAT OPERATIONS IN
AFGHANISTAN
1056 EFFICACY OF INTRAPLEURAL TPA FOR RETAINED HEMOTHORAX IN TRAUMA PATIENTS
1057 ANTI-FACTOR XA ACTIVITY IN NON-WEIGHT BASED ENOXAPARIN DOSING FOR VTE
PROPHYLAXIS IN TRAUMA PATIENTS
1058 THC IS MORE PREDICTIVE OF A GREATER INJURY SEVERITY SCORE THAN ALCOHOL FOR
TRAUMA PATIENTS OVER 30
1059 THE RESULT OF PREOPERATIVE ELECTROCARDIOGRAM ADDS NO VALUE IN
HYPERTENSIVE PATIENTS OVER 50 YEARS
1060 IMPACT OF BMI ON OUTCOMES AFTER TRAUMATIC BRAIN INJURY
1061 HEMODYNAMIC CHANGES AFTER DECOMPRESSIVE CRANIECTOMY FOR INTRACRANIAL
HYPERTENSION
1062 EVALUATION OF ANTI-XA LEVEL MONITORING FOR ENOXAPARIN IN TRAUMA PATIENTS
Poster Session: Surgery/Trauma/Burns 5
PUBLISHING NUMBER
1063 COMPARISON OF WEIGHT-BASED DOSING OF 23.4% HTS VERSUS FIXED DOSING FOR ICP
REDUCTION IN TBI PATIENTS
1064 WELL’S CRITERIA FOR DVT: A RELIABLE PREDICTOR OF DVT IN THE TRAUMA
POPULATION?
1065 THE NEED FOR ICU MANAGEMENT FOR POST-CRANIOPLASTY PROCEDURES IN TRAUMA
PATIENTS
1066 THE INCIDENCE OF HYPOCALCEMIA IN TRAUMA PATIENTS RECEIVING MASSIVE
TRANSFUSION PROTOCOL
1067 ACUTE KIDNEY INJURY AFTER SERIOUS MOTOR VEHICLE CRASHES: ASSOCIATED
PATIENT IMAGING FACTORS
1068 TRANSFUSION PRACTICES IN PEDIATRIC TRAUMA PATIENTS ADMITTED TO THE
INTENSIVE CARE UNIT
1069 A 20-YEAR REVIEW OF FIREARM-RELATED VIOLENCE IN PREGNANT PATIENTS AT A
LEVEL I TRAUMA CENTER
1070 DOES OBESITY AFFECT OUTCOMES IN CHILDREN ADMITTED FROM TRAUMA CENTERS?
1071 LACTATE AFTER CARDIAC SURGERY IS ASSOCIATED WITH MORBIDITY INDEPENDENT OF
SURGICAL COMPLICATIONS
1072 EFFECTIVENESS AND SAFETY OF ENOXAPARIN PROPHYLAXIS DOSED BY A PREDICTIVE
EQUATION IN BURN PATIENTS
Poster Session: Surgery/Trauma/Burns 6
PUBLISHING NUMBER
1073 RISK FACTORS OF MORTALITY IN PATIENTS WHO UNDERWENT EMERGENCY OPERATION
DUE TO SECONDARY PERITONITIS
1074 TRAUMA TO REQUEST FOR TRANSFER AS A MEASURE OF A REGIONAL TRAUMA SYSTEM
MATURITY
1075 THE PROXIMAL HUMERUS MAY BE A VIABLE SITE FOR CONTRAST INJECTION USING A
POWER INFUSER FOR CT EXAM
1076 SURGICAL ATTENDING PRACTICE PATTERNS REGARDING THE TIMING OF
TRACHEOSTOMY
1077 IMPACT OF KETAMINE ON THE ABILITY TO WEAN OFF FENTANYL INFUSIONS IN
CRITICALLY ILL TRAUMA PATIENTS
1078 NET CUMULATIVE ICU FLUID BALANCE IS ASSOCIATED WITH INCREASED MORTALITY IN
THE BLUNT TRAUMA PATIENT
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
1079 ARE HEMOGLOBIN OXIMETRY, VITAL SIGNS AND LABORATORY VALUES ABLE TO
PREDICT EMERGENCY TRANSFUSION?
1080 POSTOPERATIVE METABOLIC ACIDOSIS ASSESSMENT IN HIGH RISK SURGICAL
PATIENTS: PROGNOSTIC IMPORTANCE
1081 SCHEDULED 23.4% SODIUM CHLORIDE FOR INTRACRANIAL PRESSURE CONTROL IN
TRAUMATIC BRAIN INJURY
1082 PREVALENCE OF KIDNEY INJURY IN BURN PATIENTS REQUIRING FLUID
RESUSCITATION
Poster Session: Surgery/Trauma/Burns 7
PUBLISHING NUMBER
1083 PREHOSPITAL MANAGMENT AS A PREDICTOR OF MORTALITY IN TRAUMATIC BRAIN
INJURY
1084 SURGERY DOES NOT MEAN STARVATION: THE SAFETY OF EARLY AND FULL TUBE
FEEDINGS FOLLOWING PEG PLACEMENT
1085 ACUTE RESPIRATORY DISTRESS SYNDROME AFTER TRAUMATIC HEMORRHAGIC SHOCK:
MORE THAN JUST VENT SETTINGS!
1086 INTENSIVE CARE UTILIZATION OF PEDIATRIC PATIENTS UNDERGOING LAPAROTOMY
AFTER ABDOMINAL TRAUMA
1087 PEDIATRIC SOLID ORGAN INJURY OPERATIVE INTERVENTIONS AT HARBORVIEW
MEDICAL CENTER, 2001 TO 2012
1088 FEASIBILITY OF EARLY JEJUNAL ENTERAL NUTRITION FOR PATIENTS WITH SEVERE
DUODENAL INJURIES
1089 ARTERIAL CATHETER FAILURE: A PICTORIAL CASE SERIES
1090 HIGH-DOSE MIDAZOLAM VERSUS PENTOBARBITAL FOR INTRACRANIAL HYPERTENSION
IN TRAUMATIC BRAIN INJURY
1091 IS BIGGER REALLY BETTER? LABORATORY TESTING OF CHEST TUBES WITH VARIABLE
RIB SPACE DISTANCE
1092 VITAMIN D AND GLUTAMINE REDUCE MORTALITY RATE AT A LEVEL I TRAUMA CENTER
IN CRITICALLY ILL PATIENTS
Poster Session: Surgery/Trauma/Burns 8
PUBLISHING NUMBER
1093 MINI SURGICAL VERSUS STANDARD METHOD IN PERCUTANEOUS DILATION
TRACHEOSTOMY
1094 VTE RISK ASSESSMENT HAS SUBOPTIMAL INTEROBSERVER RELIABILITY AMONGST
INEXPERIENCED CLINICIANS
1095 DEVELOPMENT OF MULTI-DRUG RESISTANT ORGANISMS IN NECROTIZING FASCIITIS: A
SIX-YEAR REVIEW
1096 EVALUATION OF HEMODYNAMIC AND ADVERSE EFFECTS OF KETAMINE VERSUS
ETOMIDATE FOR RSI IN TRAUMA
1097 MORTALITY IN PATIENTS UNDERGOING DOUBLE PROSTHETIC VALVE REPLACEMENT
AND CORONARY BYPASS SURGERY
1098 THE EFFICACY OF A NOVEL PAIN MANAGEMENT STRATEGY IN POSTOPERATIVE
CARDIOTHORACIC SURGERY PATIENTS
1099 THE ROLE OF SURGICAL INTENSIVISTS IN THE EICU
1100 IMPACT OF COAGULOPATHY ON TRAUMATIC SPLENIC INJURIES
1101 SUBARACHNOID HEMORRHAGE AND REBLEEDING AND MORTALITY
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Surgery/Trauma/Burns 9
PUBLISHING NUMBER
1102 THE GHAJAR GUIDE: AN ASSESSMENT OF SUITABILITY
1103 ICU READMISSION AFTER BLUNT TRAUMATIC HEMORRHAGIC SHOCK: RISK FACTORS
AND PREDICTORS OF MORTALITY
1104 MOTOR VEHICLE ACCIDENTS IN CHILDREN AND ADOLESCENTS IN USA: IS THERE A
SEASONAL VARIATION?
1105 UTILIZATION OF SEIZURE PROPHYLAXIS IN TRAUMATIC BRAIN INJURY (TBI) PATIENTS
1106 SURGICAL MANAGEMENT INVOLVING CATASTROPHIC INJURIES: WHEN IS ENOUGH,
ENOUGH?
1107 IMPACT OF THREE ANTIFIBRINOLYTIC REGIMENS IN CARDIAC SURGERY
1108 SUPERIOR MESENTERIC ARTERY SYNDROME AFTER SPINAL FUSION REPAIR IN
ADOLESCENTS: AN ANALYSIS USING KID
1109 ELEVATED SERUM NEUTROPHIL GELATINASE-ASSOCIATED LIPOCALIN (NGAL) IS AN
EARLY MARKER OF ACUTE KIDNEY
1110 POSTOPERATIVE TRANSFUSION MANAGEMENT AFTER CRANIOFACIAL
RECONSTRUCTION: AN INSTITUTIONAL EXPERIENCE
Poster Session: Case Reports
PUBLISHING NUMBER
1141 SODIUM OF 94
1142 MASSIVE INTENTIONAL INGESTION OF VISCOUS LIDOCAINE AND ASSOCIATED
NEUROTOXICITY
1143 FOLLICULAR CARCINOMA OF THE THYROID PRESENTING WITH ANTERIOR MEDIASTINAL
MASS AND CARDIOGENIC SHOCK
1144 CHARACTERIZATION OF 4-FACTOR PROTHROMBIN COMPLEX CONCENTRATE IN
ORTHOTOPIC HEART TRANSPLANTATION
1145 THE TOXIC EFFECTS OF SYNTHETIC CANNABINOIDS
1146 INTRAVENOUS INJECTION OF ORAL NARCOTICS CAUSING ACUTE RIGHT HEART FAILURE
IN CYSTIC FIBROSIS PATIENT
1147 HEPARIN-INDUCED THROMBOCYTOPENIA IN A CHILD WITH POST-INFECTIOUS
GLOMERULONEPHRITIS
1148 DIGOXIN TOXICITY ASSOCIATED WITH NEGATIVE INTERFERENCE FROM DIGOXIN-LIKE
IMMUNOREACTIVE SUBSTANCES
1149 IRON PILL ASPIRATION SYNDROME
1150 MEDIASTINAL ABSCESS AS A RARE PRESENTATION OF HISTOPLASMOSIS
1151 CUPRIAVIDUS GILARDII: A RARE CAUSE OF PNEUMONIA
1152 AIR EMBOLISM: A RARE COMPLICATION AFTER ENDOSCOPIC RETROGRADE
CHOLANGIOPANCREATOGRAM
1153 MYCOPLASMA HOMINIS INFECTION POST HEART-LUNG TRANSPLANT PATIENTS–A CASE
SERIES
1154 A CASE OF ACUTE DISSEMINATED ENCEPHALOMYELITIS IN A MIDDLE-AGED ADULT
1155 PHARMACOKINETICS OF CONTINUOUS INFUSION MEROPENEM WITH EXTRACORPOREAL LIFE SUPPORT AND CRRT
1156 USE OF ANTI-D IN PATIENTS WITH SEVERE DENGUE
1157 CHYLOPTYSIS WITH MEDIASTINAL LYMPHANGIOMA IN 46-YEAR-OLD FEMALE
1158 PLASMAPHERESIS SIGNIFICANTLY REDUCES SERUM AMLODIPINE LEVELS FOLLOWING
INTENTIONAL OVERDOSE
1159 A CASE OF JIMSONWEED TOXICITY
1160 RECURRENT EPISODES OF METHEMOGLOBINEMIA IN AN INFANT
1161 DELAYED MULTI-SYSTEM REACTION WITH FENTANYL INFUSION IN A CRITICAL ILL
PATIENT
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
1162 PALLIATIVE INOTROPIC SUPPORT AT HOME FOR CHILDREN WITH END-STAGE HEART
FAILURE
1163 DKA PRESENTING AS STEMI-PSEUDOINFARCTION DIAGNOSED EN ROUTE TO CARDIAC
CATH, ABG SAVED A LIFE...
1164 ACUTE HEART FAILURE WITH GEMELLA MORBILLORUM NATIVE VALVE ENDOCARDITIS
1165 SEVERE NEAR FATAL SALICYLATE INTOXICATION TREATED WITH EXTRACORPOREAL
SUPPORT
1166 A RARE CASE OF EBV INDUCED HEMOPHAGOCYTIC LYMPHOHISTOCYTOSIS.
1167 METASTATIC NEUROBLASTOMA PRESENTING AS DILATED CARDIOMYOPATHY AND
HYPERTENSIVE EMERGENCY
1168 TRANSFUSION-ASSOCIATED NECROTIZING ENTEROCOLITIS (TANEC) IN INFANTS WITH
CONGENITAL HEART DISEASE
1169 DIAGNOSTIC DILEMMA: HYPOVENTILATION IN YOUNG ADULT WITH GRAFT VERSUS
HOST DISEASE
1170 GUT TO BRAIN TRANSLOCATION?LISTERIA RHOMBENCEPHALITIS IN AN
IMMUNOCOMPETENT HIGH RISK PATIENT
1171 COINFECTION OF H1N1 INFLUENZA WITH PNEUMOCYSTIS JIROVECI PNEUMONIA IN
IMMUNOCOMPETENT PATIENT
1172 2 VENTS, 1 AIR LEAK: USE OF INDEPENDENT LUNG VENTILATION IN THE MANAGEMENT
OF PNEUMOTHORAX
1173 QTC PROLONGATION PROGRESSING TO TORSADE DE POINTES SECONDARY TO IBOGAINE
INGESTION
1174 ADMINISTRATION OF SEVOFLURANE TO TREAT SEVERE BRONCHOSPASM
1175 ASYSTOLIC CARDIAC ARREST IN NEWLY DIAGNOSED JUVENILE DERMATOMYOSITIS
1176 PROFOUND HYPOXEMIA AFTER MULTI-SYSTEM TRAUMA: ECMO AND HEPARIN IN THE
SETTING OF ACUTE HEMORRHAGE
1177 EXTREME HYPERTONIC DEHYDRATION IN 2-WEEK OLD NEWBORN
1178 A RARE COMPLICATION OF COMMON SURGERY: PLATYPNEA-ORTHODEOXIA SYNDROME
AFTER PNEUMONECTOMY
1179 SPONTANEOUS RUPTURE OF AN ACCESSORY SPLEEN 15 YEARS AFTER TRAUMATIC
SPLENECTOMY: A CASE REPORT
1180 AN UNUSUAL CAUSE FOR PERSISTENT SHOCK
1181 MUTATION IN SONIC HEDGEHOG GENE ASSOCIATED WITH ADRENAL INSUFFICIENCY
1182 HYDRALAZINE-INDUCED VASCULITIS MANIFESTING IN ALVEOLAR HEMORRHAGE
1183 HYPERTRIGLYCERIDEMIA UPTO THIRTY THOUSAND DUE TO ESTROGEN: CONSERVATIVE
MANAGEMENT
1184 EMERGENT THYROIDECTOMY FOR THYROID STORM: A RARE CASE
1185 EXTRACORPOREAL MEMBRANE OXYGENATION AS PROLONGED SUPPORT FOR AIRWAY
OBSTRUCTION FROM A VASCULAR RING
1186 NECROTIZING EOSINOPHLIC MYOCARDITIS AND RAPID CARDIAC FAILURE
1187 DRUG REACTION WITH EOSINOPHILIA AND SYSTEMIC SYMPTOMS (DRESS) SECONDARY
TO ORAL VANCOMYCIN
1188 RECURRENT MASSIVE HEMOPTYSIS FOLLOWING MITRAL VALVULOPLASTY FOR MITRAL
STENOSIS
1189 A RARE CASE OF CARDIAC TAMPONADE SECONDARY TO EMPYEMA
1190 DISSEMINATED FUNGAL INFECTIONS IN A POST CARDIAC TRANSPLANT PATIENT
1191 POINT OF CARE ULTRASOUND: DIAGNOSIS OF SEPSIS INDUCED CARDIAC
CALCIFICATION (SICC)
1192 AORTIC MYCETOMA FROM DISSEMINATED CUNNINGHAMELLA INFECTION
1193 SEVERE PULMONARY HYPERTENSION AND RHF TREATED WITH ECMO PRIOR TO
DOUBLE LUNG TRANSPLANT
1194 SECONDARY PULMONARY HYPERTENSION IN A YOUNG FEMALE
1195 A RARE MANIFESTATION OF POSTPARTUM INFECTION WITH MRSA ASSOCIATED SEPSIS
AND SEPTIC PULMONARY EMBOLI
1196 FATAL SYSTEMIC BLASTOMYCOSIS IN AN IMMUNE COMPETENT OTHERWISE HEALTHY
MALE - A CASE REPORT
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
1197 DELAYED PRESENTATION OF AN IATROGENIC BURN IN THE ICU
1198 REFRACTORY TORSADES DE POINTES SECONDARY TO TARGETED THERAPY INDUCED
PROFOUND HYPOMAGNESEMIA
1199 PULMONARY EMBOLISM FOLLOWING RECEIPT OF 4-FACTOR PROTHROMBIN COMPLEX
CONCENTRATE IN A TRAUMA PATIENT
1200 SEVERE HEMOPTYSIS FOLLOWING EPTIFIBATIDE FOR ACUTE MI AND STENT PATENCY
DURING ECMO
1201 THE ROLE OF HELIOX IN EXTRINSIC AIRWAY OBSTRUCTION
1202 PERSISTENT HYPOXEMIA AFTER NORWOOD STAGE 1 SURGERY: ALVEOLAR CAPILLARY
DYSPLASIA
1203 ISCHEMIC OPTIC NEUROPATHY AFTER PRONE VENTILATION FOR ARDS
1204 COMMON DRUG CAUSING UNCOMMON REACTION
1205 CONSERVATIVE MANAGEMENT OF MASSIVE RIVAROXABAN AND ENOXAPARIN
OVERDOSE
1206 CATACLYSMIC CYTOKINE RELEASE SYNDROME WITH RABBIT ATG THERAPY AFTER
COMBINED LIVER/KIDNEY TRANSPLANT
1207 HEMOPTYSIS – AN UNCOMMON CULPRIT TO A VERY COMMON PROBLEM.
1208 AN INFAMOUS CAUSE OF ENCEPHALITIS- ANTI NMDA RECEPTOR ENCEPHALITIS
1209 FIXED AND DILATED, WHAT PERCHERON HAD IN MIND?
1210 DIFFUSE ALVEOLAR HEMORRHAGE IN THE SETTING OF NOVEL ANTICOAGULANT USE
AND POSITIVE AUTOIMMUNE SCREEN
1211 REVERSAL OF OSMOTIC MYELINOLYSIS SYNDROME BY RE-LOWERING SERUM SODIUM
1212 DAPTOMYCIN RESISTANT ENDOCARDITIS TREATED WITH CEFTAROLINE
1213 DIAGNOSIS OF PARTIAL ANOMALOUS PULMONARY VENOUS RETURN FOLLOWING
CENTRAL LINE PLACEMENT
1214 SUPRATHERAPEUTIC RESPONSE TO ARGATROBAN THERAPY IN A PATIENT WITHOUT
LIVER OR HEART FAILURE
1215 SEPTIC PULMONARY EMBOLISM ASSOCIATED WITH DUODENOVENOUS FISTULA OF THE
PORTAL VEIN–A CASE REPORT
1216 ESOPHAGEAL DIEULAFOY LESION,AN UNCOMMON CAUSE OF GI BLEEDING
1217 RARE CASE OF LEFT ATRIAL SPINDLE CELL SARCOMA
1218 EXTRACORPOREAL MEMBRANE OXYGENATION IN AN ADULT PATIENT WITH SEPTIC
SHOCK AFTER FECULENT ASPIRATION
1219 ACUTE HYPOXEMIC RESPIRATORY FAILURE IN PATIENT WITH HYPEREOSINOPHILIC
SYNDROME
1220 URETER TRANSECTION AND ASSOCIATED ILIAC VEIN LACERATION IN PEDIATRIC BLUNT
TRAUMA
1221 ROLE OF DOFETILIDE IN MANAGEMENT OF ATRIAL FIBRILLATION POST-LUNG
TRANSPLANTATION
1222 BILATERAL THALAMIC INFARCTION IN A MULTIPLE TRAUMA PATIENT AFTER INITIAL
NEGATIVE HEAD CT
1223 A CASE OF HEPARIN-INDUCED HYPERKALEMIA
1224 WHEN IT'S NOT HLH: PARECHOVIRUS IN A NEONATE
1225 THE 4G ALLELE OF PLASMINOGEN ACTIVASE INHIBITOR TYPE 1 AND SUDDEN CARDIAC
DEATH IN A TEEN ATHLETE
1226 CEREBRAL AIR EMBOLISM, STROKE AND STATUS EPILEPTICUS FOLLOWING PICC
INSERTION
1227 SUBACUTE RIGHT VENTRICULAR PERFORATION BY PACEMAKER LEAD PRESENTING
WITH LEFT HEMOTHORAX AND SHOCK
1228 ACUTE RESPIRATORY FAILURE: COULD IT BE GILCHRIST’S DISEASE?
1229 SPURIOUS BICARBONATE FROM HYPERTRIGLYCERIDEMIA IN DIABETIC KETOACIDOSIS
(DKA): IMPLICATIONS FOR ICU
1230 RARE CARE OF COMA: CEREBRAL FAT EMBOLISM FOLLOWING ARTHROPLASTY
1231 REFEEDING SYNDROME AND CARDIAC ARREST IN A MALNOURISHED PATIENT
RECEIVING TOTAL PARENTERAL NUTRITION
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
1232 THE THROMBOELASTOMETRY VS STANDARD COAGULATION TESTS IN AN ANHEPATIC
PATIENT AFTER BLUNT TRAUMA
1233 HEAT STROKE COMPLICATED BY SEPSIS: A CASE REPORT OF BACTEREMIA FOLLOWING
INTENSE PHYSICAL EXERTION
1234 DYNAMIC LEFT VENTRICULAR OUTFLOW TRACT OBSTRUCTION AFTER ACUTE ANTERIOR
MYOCARDIAL INFARCTION
1235 RIGHT VENTRICLE LACERATION AND PSEUDOANEURYSM FORMATION DUE TO A
FRACTURED STERNAL WIRE POST CABG
1236 A NEW MASQUERADER(OR AN OLD FOE)
1237 INTRAVENOUS LIDOCAINE INFUSION FOR SUNCT SYNDROME
1238 GRADE IV BLUNT CARDIAC INJURY WITH AORTIC VALVE RUPTURE MANAGED WITH
VALVULOPLASTY
1239 ATYPICAL HEMOLYTIC UREMIC SYNDROME PRESENTING WITH DIFFUSE ALVEOLAR
HEMORRHAGE
1240 ELEVATED PROCALCITONIN AFTER ANTI-THYMOCYTE GLOBULIN FOR FAMILIAL
HEMOPHAGOCYTIC LYMPHOHISTIOCYTOSIS
1241 RECTAL PROPRANOLOL TO CONTROL PAROXYSMAL SYMPATHETIC HYPERACTIVITY
1242 THE GOOD, THE BAD, AND, THE UNKNOWN: INTRAPULMONARY FACTOR VII IN DIFFUSE
ALVEOLAR HEMORRHAGE
1243 A CASE OF REFRACTORY STATUS EPILEPTICUS AND MULTI ORGAN FAILURE FROM
ROCKY MOUNTAIN SPOTTED FEVER
1244 PROLONGED REFRACTORY STATUS EPILEPTICS SUCCESSFULLY TREATED WITH PLASMA
EXCHANGE AND RITUXIMAB
1245 HYPERTRIGLYCERIDEMIA-INDUCED ACUTE SYMPTOMATIC PANCREATITIS TREATED BY
EXTENDED PERIOD OF INSULIN
1246 INTENTIONAL OVERDOSE IN A TEENAGER WITH LATE SALICYLATE TOXICITY
SECONDARY TO BEZOAR FORMATION
1247 RETROPERITONEAL HEMORRHAGE AS A CONSEQUENCE OF “TAZING”- AN UNSUAL
CAUSE
1248 A RARE CASE OF A BAROTRAUMA INDUCED UPPER THORACIC ESOPHAGEAL
PERFORATION MANNAGED NON-OPERATIVELY
1249 STAPHYLOCOCCUS LUGDUNENSIS ENDOCARDITIS IN AORTICO-LEFT VENTRICULAR
TUNNEL
1250 TREATMENT OF SUPER-REFRACTORY STATUS EPILEPTICUS WITH PERAMPANEL IN AN
INTENSIVE CARE UNIT
1251 BETA LACTAMASE PRODUCING CLOSTRIDIUM PERFRINGENS BACTEREMIA IN A MAN
WITH ACUTE PANCREATITIS
1252 POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME SECONDARY TO BLOOD
TRANSFUSION
1253 A CASE OF KAWASAKI DISEASE AND SMALL BOWEL OBSTRUCTION?AN UNUSUAL
PRESENTATION
1254 MYCOPLASMA PNEUMONIAE ENCEPHALITIS
1255 EXTREME PHYSICAL THERAPY–PROGRESSION OF FUNCTIONAL MOBILITY OF 25-YEAR
OLD ON ECMO 72 DAYS
1256 RECURRENT LIFE-THREATENING BRONCHOSPASM SECONDARY TO PARAINFLUENZA IN
A CHILD WITH CONTROLLED ASTHMA
1257 CEREBRAL VENOUS SINUS THROMBOSIS AS A POSTOPERATIVE COMPLICATION OF
TETROLOGY OF FALLOT IN A CHILD
1258 “THE FLIP SIDE”–22 DAYS OF PRONE VENTILATION IN A LUNG TRANSPLANT RECIPIENT
1259 COCAINE INDUCED CARDIOTOXICITY
1260 A CASE IN WHICH EFFECTIVE DRAINAGE WAS POSSIBLE FOR AN ABSCESS BY THE ISOP
METHOD
1261 THOUGHT TO BE A LUNG CANCER, ASPERGILLOSIS IN A HEALTHY LUNG
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
1262 INTRAVENTRICULAR NICARDIPINE EVERY SIX HOURS IS A SAFE ALTERNATIVE FOR
REFRACTORY CEREBRAL VASOSPASM
1263 SYSTEMIC CAPILLARY LEAK SYNDROME SUCCESSFULLY MANAGED USING
HEMODYNAMIC PARAMETERS
1264 PULMONARY-RENAL SYNDROME IN GRANULOMATOSIS WITH POLYANGIITIS
1265 RARE MANIFESTATION OF GASTRIC VOLVULUS –CASE REPORT OF GASTRIC VOLVULUS
WITH UGIB
1266 ANAPHYLACTIC REACTION AND QT PROLONGATION CAUSED BY CHINESE HERBAL
MEDICINE
1267 USE OF HEMODIALYSIS FOR ACETAMINOPHEN OVERDOSE
1268 DIFFUSE ALVEOLAR DAMAGE IN A PATIENT WITH GRAFT-VERSUS-HOST DISEASE
1269 NOVEL APPROACH TO PAIN MANAGEMENT IN CRITICALLY ILL PATIENTS WITH RIB
FRACTURES SECONDARY TO TRAUMA
1270 AN UNUSUAL CAUSE OF RESPIRATORY FAILURE
1271 A CASE OF DEADLY VARICELLA PNEUMONIA IN AN IMMUNOSUPPRESSED PATIENT
1272 HYPERINSULINEMIA EUGLYCEMIA THERAPY TO REVERSE CIRCULATORY COLLAPSE IN
DILTIAZEM OVERDOSE
1273 SEVERE SEPSIS AND MENINGITIS DUE TO PARAMENINGEAL SPREAD OF OTITIS MEDIA
IN A GERIATRIC PATIET
1274 DISTAL ESOPHAGEAL STENT COMPLICATED WITH BRONCHO-ESOPHAGEAL FISTULA
1275 DELAYED HEMOTHORAX SECONDARY TO PENETRATING THORACIC TRAUMA
1276 A RARE CASE OF RHEUMATOLOGICAL FRUIT SALAD
1277 DROWNING IN PUS: REPORT OF AN EMPYEMA PROGRESSING TO NECROTIZING FASCIITIS
OF CHEST
1278 POST VIRAL INFLUENZA INVASIVE PULMONARY ASPERGILLOSIS: A CHALLENGE TO
EARLY DIAGNOSIS
1279 UNUSUAL PRESENTATION OF PNEUMOCEPHALUS AS A COMPLICATION OF LUMBAR
EPIDURAL INJECTION
1280 AEP PRESENTING AS SEVERE ARDS DUE TO RECENT HEAVY SMOKING IN YOUNG
FEMALE ALLERGIC TO SULFUR
1281 MALTOMA - RARE CAUSE OF BILATERAL PULMONARY NODULES
1282 NOT JUST CHILD'S PLAY: A CONFIRMED CASE OF ADULT ADEM
1283 TAKOTSUBO’S CARDIOMYOPATHY IN AN ECLAMPTIC PATIENT
1284 STAPHYLOCOCCAL TOXIC SHOCK SYNDROME WITHOUT RASH: UTILITY OF SKIN BIOPSY
AS DIAGNOSTIC TOOL
1285 DIPHENHYDRAMINE INGESTION LEADS TO CEREBRAL EDEMA AND BRAIN DEATH
1286 DECREASE OF VASOPRESSIN CONCENTRATION WITH SEPTIC SHOCK INDUCE DIABETES
INSIPIDUS
1287 CONSERVATIVE MANAGEMENT OF SPONTANEOUS ESOPHAGEAL PERFORATION IN A
PATIENT WITH ACHALASIA
1288 IDIOPATHIC FIBROSING MEDIASTINITIS IN YOUNG PREGNANT FEMALE–A RARE
CONDITION
1289 MULTIPLE CARBOXYLASE DEFICIENCY PRESENTING AS SEVERE SEPSIS
1290 ACUTE AMITRAZ INGESTION MANAGED WITH YOHIMBINE AS A RESCUE THERAPY
1291 RECURRENT LANGERHANS CELL HISTIOCYTOSIS WITH NEAR TOTAL SKIN LOSS, SEPSIS,
AND ARDS
1292 NATIVE VALVE INFECTIVE ENDOCARDITIS WITH CITROBACTER KOSERI IN AN
IMMUNOCOMPETENT ADULT
1293 TRANEXAMIC ACID RESTORES CLOTTING IN THROMBUS ASSOCIATED
HYPERFIBRINOLYSIS WITH OVERT BLEEDINGS
1294 MAN’S BEST FRIEND? A CASE OF DISSEMINATED PASTEURELLA MULTOCIDA INFECTION
1295 FATAL DIFFUSE ALVEOLAR HEMORRHAGE AND HYPOXEMIC RESPIRATORY FAILURE
ASSOCIATED WITH RIVAROXABAN
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
1296 RARE PRESENTATION OF CARDIAC TAMPONADE IN A PATIENT WITH HYPOTHYROIDISM
1297 HEARTWARE IMPLANTABLE CONTINUOUS FLOW PUMP AS BIVAD SUPPORT IN
ADOLESCENT WITH ACUTE MYOCARDITIS
1298 POSTOPERATIVE BRONCHOPLEURAL FISTULA: SUCCESSFUL TREATMENT WITH
ENDOBRONCHIAL VALVE PLACEMENT
1299 HEMOPTYSIS GALORE DIAGNOSIS IS A CHORE!
1300 HIGH ATTENUATION MUCUS AS A SIGN OF ABPA
1301 ACQUIRED HEMOPHILIA A (AHA) PRESENTING AS PROGRESSIVE INTRACRANIAL
HEMORRHAGE
1302 FUNCTIONAL RECOVERY IN A PATIENT WITH POSTANOXIC MYOCLONUS SECONDARY TO
ANAPHYLACTIC SHOCK
1303 GROUP B STREPTOCOCCUS INFECTIVE ENDOCARDITIS IN A NEONATE
1304 CIRCULATORY SHOCK IN THE SETTING OF AN UNUSUAL MALIGNANCY
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Oral Abstract Session: Acute Care Surgery
1
3
CORRELATION OF CHADS2 WITH NEW ONSET ATRIAL
FIBRILLATION IN THORACIC AND VASCULAR SURGICAL
PATIENTS
MORTALITY RISK FACTORS WITH CARBAPENEM-RESISTANT BACTEREMIA: IMPACT OF COMBINATION THERAPY
Kirstin Kooda1, Benjamin Dreesman2, Ross Dierkhising3, James Onigkeit4, Arun
Subramanian5; 1Mayo Clinic Rochester, Rochester, MN, 2Mayo Clinic-Saint Marys
Hospital, Rochester, MN, 3Mayo Clinic, Rochester, MN, 4Mayo Clinic Department of Anesthesiology, Rochester, MN, 5The Mayo Clinic, Rochester, MN
Learning Objectives: Incidence of new onset postoperative atrial fibrillation
(POAF) ranges from 9–20% of non-cardiac major thoracic and vascular surgeries and is associated with worse postoperative outcomes. A CHADS2 score
of ≥ 2 has previously been associated with new onset POAF in cardiac surgery
patients. The objective of the present study was to determine whether CHADS2
score alone and in the context of other clinical risk factors would be predictive
of new onset POAF in non-cardiac major thoracic and vascular surgical patients.
Methods: After IRB approval, 1,566 patients undergoing major non-cardiac thoracic and vascular surgery without known atrial fibrillation from 2006 through
2013 who were admitted to a surgical intensive care unit postoperatively were
retrospectively identified. Baseline CHADS2 and clinical variables including
daily fluid balance, electrolyte values, intra- and postoperative vasopressor and
inotrope requirements, operation length, blood transfusion, and resumption of
home cardiac medications were collected. The primary endpoint was correlation
of CHADS2 with incidence of POAF. A multivariable Cox proportional hazards
model was used to assess association between risk factors and POAF. Results:
Two hundred twenty-one (14.1%) patients developed POAF at a median of 55
hours (IQR 30–93.7) after surgery. On univariate analysis, CHADS2 was significantly associated with POAF (HR 1.22 [95% CI 1.08–1.37] for every unit
increase in score). This association persisted after multivariate adjustment (HR
1.17 [95% CI 1.04–1.31]). Intraoperative fluid administration (HR 1.03 [95%
CI 1.01–1.06] per 1000 ml), preoperative beta blocker use (HR 2.04 [95% CI
1.44–2.90]), calcium channel blocker use (HR 0.67 [95% CI 0.49–0.93])
and postoperative day 1 SOFA score (HR 1.08 [95% CI 1.03–1.12] for every
unit increase in score) were also significantly associated. Model R2 was 0.76.
Conclusions: CHADS2, when used in combination with baseline and clinical
variables, is predictive of new POAF after major thoracic or vascular surgery and
maybe useful in identifying at risk patients.
Stephanie Bass1, Elizabeth Neuner2, Seth Bauer3, Simon Lam2; 1Cleveland Clinic
Foundation, Cleveland, OH, 2Cleveland Clinic, Cleveland, OH, 3N/A, Cleveland, OH
Learning Objectives: There are limited treatment options for carbapenemresistant gram-negative (CR-GN) infections. Currently, there are suggestions
in the literature that combination therapy should be used which frequently
includes antibiotics with in vitro resistance to the causative pathogen. Methods: This case-control study evaluated risk factors for mortality in critically ill
patients with CR-GN bacteremia. Adult patients admitted to an ICU with sepsis
due to CR-GN bacteremia were included. Patients with polymicrobial, recurrent, or breakthrough infections were excluded. Patients were divided into those
alive (controls) or deceased (cases) at 30 days after positive blood culture. Data
describing baseline characteristics, antibiotic susceptibility and administration,
and mortality were collected. Results: Of 302 patients screened, 168 patients
were included, of which 90 patients died (53.6% cases) and 78 survived (46.4%
controls) at 30 days. More survivors received appropriate antibiotics (antibiotics
with in vitro activity) compared with non-survivors (93.6% vs. 53.3%, p<0.001).
There was no difference in time to appropriate antibiotics (59h [27.5–102.2]
vs. 66.7h [21.6–88.7], p=0.85) or first appropriate antibiotic used (p=0.42 for
all comparisons) between survivors and non-survivors. Combination therapy,
defined as two or more agents with in vitro activity given for 48 hours or more,
was more common in survivors than non-survivors (32.1% vs. 7.8%, p<0.001),
however there was no difference in multiple agent use when in vitro activity was
not considered (87.2% vs. 80%, p=0.21). On logistic regression analysis, 30-day
mortality was positively associated with increased age (OR 1.04, 95% CI: 1.02–
1.07, p=0.002) and SOFA score (OR 1.22, 95% CI: 1.1–1.35, p<0.001), while
negatively correlated with combination therapy (OR 0.12, 95% CI: 0.04–0.35,
p<0.001). Conclusions: These data suggest combination therapy with two or
more agents with in vitro activity is associated with improved survival in critically
ill patients with CR-GN bacteremia. However, that association is lost if in vitro
activity is not considered.
4
2
FLUID OVERLOAD COSTS IN CARDIOVASCULAR PATIENTS:
ARE SMALL VOLUME INFUSIONS A PROACTIVE SOLUTION?
RCT OF CHLORHEXIDINE VS. SOAP & WATER BATHING
FOR PREVENTION OF HOSPITAL-ACQUIRED INFECTIONS
IN SICU
Debra Child1, Zhun Cao2, Laura Seiberlich3, Scott Robinson2, Harold Brown2,
Anne Swanson3, Martha Sewall3; 1Smith’s Medical ASD, Inc., St. Paul, MN,
2
Premier Inc, Charlotte, NC, 3Smiths Medical ASD, Inc., St. Paul, MN
Joshua Swan1,2,3, Lan Bui1,2, Vy Pham4, Beverly Shirkey2, Edward Graviss3, Shaikh
Hai2, Carol Ashton3,2, Nelda Wray3; 1Texas Southern University, Houston, TX,
2
Houston Methodist Hospital, Houston, TX, 3Houston Methodist Research
Institute, Houston, TX, 4Memorial Hermann Northwest Hospital, Houston, TX
Learning Objectives: Fluid overload (FO) in critically ill patients remains a challenging clinical dilemma. Many continuous medications in the US are delivered
as dilute solutions, adding significantly to a patient’s daily intake. This study tested
the hypothesis that cardiovascular patients with FO receiving continuous infusions are associated with increased hospital costs, longer hospital stays, and higher
clinical resource utilization. Methods: A retrospective cohort study (FO vs nonFO) was conducted using the Premier research database (>500 US hospitals). The
FO cohort included adult intensive care unit (ICU) patients with a primary or
secondary diagnosis of cardiovascular disease, a central line receiving intravenous
(IV) loop diuretics, and 2+ continuous infusions on 50%+ of ICU days. NonFO cohort included patients matched to the FO patients on demographics and
severity without IV diuretic use. The primary outcome of the study was total hospitalization cost. Additional outcomes were ICU costs, mortality, total and ICU
length of stay (LOS), 30-day readmission rates, and ventilator use. Unadjusted
descriptive analysis used Chi-squared or paired-t tests to compare the cohorts.
Results: 60,221 cardiovascular patients were identified in each cohort. The FO
cohort had an unadjusted mean cost of $15,317/visit, 56.6% higher than the
non-FO cohort (p<0.001). The unadjusted ICU cost for FO cohort was $5,241/
visit, 93.2% higher than the non-FO cohort (p<0.001). FO patients had higher
mortality (3%), prolonged LOS (3.5 days) and ICU LOS (2.6 days), higher risk of
30-day readmission (0.8%) and ventilator usage (19.5%) than their matched controls (p-values<0.001). Conclusions: In cardiovascular patients receiving multiple
continuous infusions, FO is associated with increased healthcare resources and
costs. Proactively providing maximally concentrated medications as small-volume
infusions (SVI) could be a potential solution to prevent iatrogenic FO in critically
ill patients. Further prospective research is warranted to assess the impact of the
SVI dispensing model on patient outcomes and healthcare costs.
Learning Objectives: Preventing four of the five most common hospital-acquired
infections (HAIs) (surgical site [SSI], bloodstream [BSI], catheter-associated urinary tract [CAUTI], and ventilator-associated pneumonia [VAP]) is a national
priority. Compared to soap and water (S&W) daily bathing, 2% chlorhexidine
gluconate (CHG) bathing every 48 hours for up to 28 days was hypothesized
to decrease the hazard ratio (HR) of acquiring these four HAIs (primary BSI,
CAUTI, VAP, or incisional SSI) in surgical intensive care unit (SICU) patients.
Methods: This single-center, pragmatic, randomized, controlled trial compared
the HR for acquiring four HAIs between two bathing strategies: CHG vs. S&W.
Patients and clinicians were aware of treatment group assignment; investigators
who enrolled patients or determined outcomes were blinded. Adults admitted
to the SICU from 07/2012 through 05/2013 with an anticipated SICU stay
≥48 hours were included. Patients with Braden scores <9, pregnancy, CHG
allergy, or skin irritation were excluded. A multiple endpoint survival model
with stratified Cox regression (two-sided alpha of 0.05) was used for primary
analysis. This study was IRB approved with a waiver of informed consent, registered (#NCT01640925), and internally funded. Results: Although 350 were
randomized, only 325 subjects were analyzed (164 S&W vs. 161 CHG) as 24
were excluded due to prior enrollment and 1 subject withdrew consent. Subjects
were 57% male, 59% white, aged 60 ± 16 years, and had significant comorbidities
(APACHE II scores 26 ± 9, 38% with liver failure, and 50% with kidney failure).
Subjects acquired 53 HAIs: 2 BSIs (2 vs. 0), 21 CAUTIs (14 vs. 7), 9 SSIs (6 vs.
3), and 21 VAPs (13 vs. 8) for S&W vs. CHG, respectively. Compared to S&W
bathing, CHG bathing decreased the hazard of acquiring four HAIs (HR=0.555,
95% CI 0.309–0.998, P=0.049). For S&W vs. CHG, incidence rates per 1000
days at risk were 2 vs. 0 for BSI, 22 vs. 12 for CAUTI, 40 vs. 26 for VAP, and 12
vs. 6 for SSI, respectively.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Conclusions: Compared with S&W, CHG bathing every other day decreased
the hazard of acquiring these four HAIs by 44% in the SICU.
hyperpermeability, clinical fluid derangements, and causes alterations in endothelial cell structure: melatonin attenuates these changes.
5
7
IMMUNOMODULTAING DIET CONTANING WHEY PROTEIN AND EPA SUPPRESSED REACTIVE OXYGEN SPECIES
PRODUCTION
PHYSICAL THERAPY CONSULTATION AND ITS EFFECT ON
SURGICAL TRAUMA ICU LENGTH OF STAY
Norio Sato1, Naoki Hatanaka2, Takayuki Irahara2, Satoru Murata1, Junpei
Ogura1, Kosuke Ohtake2, Takuya Okuno1, Kaoru Koike3; 1Kyoto University,
Kyoto, Japan, 2Nippon Medical School, Tokyo, Japan, 3Kyoto University Graduate School of Medicine, Shogoin, Sakyo-Ku, Kyoto
Learning Objectives: Reactive oxygen species (ROS) is known to contribute
to the development of organ dysfunction during sepsis. Enteral feeding in the
critically ill patients is crucial and immune-modulating diet (IMD) might have
potential to prevent oxidative stress and inflammation. However we are not
sure whether IMD containing whey protein as a complete peptide and EPA
is suppressed excessive ROS production during sepsis. The present study was
conducted to investigate the ROS production by the effect of IMD containing
whey protein and EPA in a rodent sepsis model. Methods: Sprague-Dawley
rats were fed with IMD containing whey protein and EPA or control diet (CD)
for 7 days. Rats were injected with lipopolysaccharide (LPS) 10mg/kg or normal saline (NS) via intraperitoneally. Blood plasma samples were collected at 5
hours after injection for measurement of derivatives of reactive oxygen metabolites (d-ROMs) as an oxidative stress marker. Biological anti-oxidant potential (BAP) and oxy adsorbent test (OXY) as total anti-oxidant. BAP/dROMs
and OXY/dROMs were used for compare between groups. Results: In normal
S-D rat BAP/d-ROMs levels were (10.5 ± 0.3) and OXY/d-ROMs levels were
(1.3 ± 0.03). In septic rat treated by LPS 10mg/kg BAP/d-ROMs and OXY/dROMs levels were (11.4 ± 0.9) and (1.1 ± 0.06) respectively. OXY/d-ROMs levels were significantly decreased between normal and septic rats. BAP/d-ROMs
levels were lower in IMD-LPS (15.01 ± 1.0) group than CD-LPS (12.6 ± 0.4),
IMD-NS (12.4 ± 0.8), CD-NS (12.5 ± 1.2) groups. OXY/d-ROMs levels were
significantly higher in IMD-LPS (1.74 ± 0.1) than CD-LPS (1.32 ± 0.1), IMDNS (1.5 ± 0.1), CD- NS (1.5 ± 0.1). Conclusions: These results indicate IMD
suppressed excessive ROS production and enhanced total antioxidant in a
rodent sepsis model. IMD with whey protein and EPA has potential to prevent
oxidant injury.
6
MELATONIN INHIBITS HEMORRHAGIC SHOCK INDUCED
FLUID LEAK AND MICROVASCULAR ENDOTHELIAL
DERANGEMENTS
Katie Wiggins-Dohlvik1, Himakarnika Alluir2, Chinchusha Anasooya Shaji3,
Vivayak Govande3, Madhava Beeram3, Amin Mohammad3, Matthew Davis3,
Binu Tharakan3; 1N/A, Temple, TX, 2Texas A&M Health Science Center College
of Medicine, Temple, TX, 3Scott and White Health, Temple, TX
Learning Objectives: Hemorrhagic shock (HS) induces global ischemia and
reperfusion injuries, resulting in vascular hyperpermeability. The mechanisms
that regulate this process are unclear. We hypothesized that matrix metalloproteinase-9 (MMP-9) is pivotal therein and that such damage can be
attenuated with melatonin. Methods: Rats were divided into sham, HS, and
HS plus melatonin groups (shock for one hour, n=5). Laparotomy was performed and mesenteric post capillary venules were examined with intravital
microscopy. Fluorescent intensities were measured intravascularly and extravascularly to assess vessel permeability, vital signs and fluid requirements were
recorded, and serum and tissue were collected. MMP activity was assayed in
lung tissue homogenates (n=8). In parallel, rat lung microvascular endothelial cells (RLMEC) were grown and divided into the following groups: sham
serum, HS serum, sham serum plus melatonin, and HS serum plus melatonin
were applied. Albumin flux across the monolayers was obtained as a marker
of permeability (n=6). RLMEC grown on chamber slides (n=4) were stained
for adherens junction protein β-catenin and the cytoskelatal protein F-actin,
and protein degradation was examined with confocal microscopy. Statistical
analysis was conducted using Student’s t-test and ANOVA. Results: Intravital microscopy revealed an increase in vascular hyperpermeabiltiy following
HS, which was attenuated with melatonin (p<0.05). HS animals required
more fluid to maintain normotension and this was mitigated with melatonin
(p<0.05). MMP-9 activity was elevated in lung homogenates from HS animals
and levels were lower with melatonin treatment (p<0.05). Monolayer permeability was increased with exposure to HS serum and melatonin attenuated this
(p< 0.05). Chamber slides showed HS serum induced disruption of adherens
junction proteins and incited formation of F-actin stress fibers: melatonin preserved baseline configuration of both. Conclusions: HS induces microvascular
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Ai-Yui Tan1, Alexandra Coritsidis2, Aleef Rahman1, Kristina Kordesch1, Saad
Bhatti1, Jeffrey Fine1; 1Elmhurst Hospital Center, Icahn School of Medicine at
Mount Sinai, Queens, NY, 2Fordham University, Bronx, NY
Learning Objectives: Our institution is one of the busiest trauma centers in
the metropolitan New York City area with over 300 trauma-related ICU admissions each year. Our goal was to expedite initiation of rehabilitation services for
ICU patients by identifying clinical and work flow factors that impede initiation
of rehabilitation based therapeutic interventions at our institution. Methods:All
trauma admissions to the Surgical Trauma ICU (STICU) between 2011 and
2013 were reviewed. Exclusion criteria for our review included: patient expiration, traumatic brain injury, no request or cancelled rehabilitation consultations.
Demographics, timing of consults, surgery, and ICU length of stay (LOS) were
analyzed. Univariate and multivariate regression models were utilized to determine significance between LOS and our co-variates. Results: 329 STICU admissions were identified, of which 142 met the inclusion criteria. Average length
of stay (LOS) was 24.2+/-21.5 days, Average Injury Severity Score (ISS) was
18.04+/-9.2. The type of trauma includes motor vehicle accidents (39.7%), falls
(31.9%), and assault (12.7%). Orthopedic trauma accounts for 30.3% of our
patients. After correcting for age and sex, LOS is significantly associated with
ISS (P<0.05), increased number of days between surgery and rehabilitation consultation (P<0.005) and Friday rehabilitation consultation (P<0.035). Age and
sex were not significant. Conclusions: In trauma patients, after correcting for
age, sex, ISS, the presence of rehabilitation therapy interventions over the weekend and earlier post-op rehabilitation consultations may decrease ICU length
of stay, improve function, reduce complications of bedrest and improve patient
well being. Considering the costs and expense of an ICU length of stay, the
greater availability of physical therapy in STICU setting will likely be financially
beneficial.
8
SIMPLE, RELIABLE SEPSIS SCREENING TOOL IMPROVES
MORTALITY IN TRAUMA PATIENTS
Laura Moore1,2, Rosemary Kozar3, Jeff Brekke4, Joseph Love5, Michelle McNutt5,
Bryan Cotton4, Rondel Albarado6, John Holcomb4; 1Univeristy of Texas Health
Science Center, Houston, Houston, TX, 2University of Texas Health Science
Center at Houston, Houston, TX, 3University of Texas-Houston Medical School,
Houston, TX, 4The University of Texas Health Science Center, Houston, TX,
5
University of Texas Health Science Center At Houston, Houston, TX, 6University of Texas-Anderson Cancer Center, Houston, TX
Learning Objectives: The recent update to the Surviving Sepsis Campaign
Guidelines advocates for the use of routine sepsis screening. We have previously
shown that sepsis screening improves outcomes in surgical patients but data
are lacking in the trauma population. The purpose of this prospective, observational study was to determine the utility of a novel screening tool for the early
identification of sepsis in trauma patients. Methods: Patients admitted to the
trauma service were screened for sepsis twice daily using our sepsis screening tool
which assesses a patient’s white blood cell count, respiratory rate, temperature,
and heart rate and assigns a numeric score (0 to 4) for each. Patients with a
score of ≥4 screened positive. ACCP/SCCM Consensus definitions were used
to diagnose sepsis. Sensitivity and specificity were calculated using a standard
two by two table. Chi square analysis was used for categorical data. Values are
expressed as mean ± standard deviation. Results: 10,201 screens were completed
on 1,637 trauma patients admitted to a Level 1 Trauma Center. The incidence
of sepsis was 7.3%. The sepsis screening tool had a sensitivity of 92.5%, specificity of 97.4%, positive predictive value of 73.5% and negative predictive value
of 99.4%. There was no difference in the age (43.3 ± 18.15 vs. 42.7 ± 19.1, p=
0.74) or gender (74.1% male vs. 68.7% male, p=0.22) of patients with sepsis
and without sepsis. Patients that developed sepsis had higher injury severity
scores (23.3 ± 12.3 vs.12.7 ± 9.3, p<0.0001), increased hospital length of stay
(31.1 ± 26.7 vs. 8.5 ± 8.4, p <0.0001), increased intensive care unit (ICU) length
of stay (16.4 ± 16.3 vs. 1.7 ± 3.9, p<0.0001), and fewer ICU free days (14.7 ± 19.4
vs. 6.9 ± 7.1, p <0.0001). Thirty-day ICU mortality decreased from 13% to 8%
(p=0.08) after implementing the sepsis screening tool. Conclusions: Sepsis in
trauma patients has a significant impact on patient outcomes. Our sepsis screening tool accurately identifies sepsis in trauma patients with a high sensitivity
and specificity. The implementation of routine screening was associated with
improved ICU mortality rates.
Oral Abstract Session: CPR/Resuscitation
9
ADAMTS13 IS ASSOCIATED WITH NEUROLOGICAL OUTCOME IN PATIENTS WITH OUT-OF-HOSPITAL CARDIAC
ARREST
Daisuke Kudo1,2, Hiroyuki Obe2, Taku Omura3, Satoshi Yamanouchi1,4,
Tomoyuki Endo1,2, Takeaki Sato5, Ryosuke Nomura2, Shigeki Kushimoto1,2;
1
Tohoku University Graduate School of Medicine, Sendai, Japan, 2Tohoku
University Hospital, Sendai, Japan, 3Chiba University Hospital, Chiba, Japan,
4
Tohoku Uniersity Hospital, Sendai, Japan, 5Tohoku University Hospital, Sendaishi, Japan
Learning Objectives: A disintegrin-like and metalloprotease with thrombospondin type 1 motifs 13 (ADAMTS13) regulates primary hemostasis by cleaving von
Willebrand factor. ADAMTS13 levels have been associated with disease severity and mortality in patients with systemic inflammation such as severe sepsis.
Although post-cardiac arrest syndrome (PCAS) has been recognized as a systemic
inflammatory condition secondary to generalized ischemia/reperfusion, the role
of ADAMTS13 in cases of successful resuscitation after out-of-hospital cardiac
arrest (R-OHCA) is not clear. We investigated whether ADAMTS13 was associated with mortality and neurological outcome in cases of R-OHCA and evaluated
the role of ADAMTS13 in the disease pathophysiology. Methods: Prospective
observational study of adult patients after R-OHCA was conducted in an academic hospital. ADAMTS13 activity in the plasma and levels of inflammatory,
immunological, and coagulation markers were evaluated at admission (day 1)
and the next day (day 2). Cerebral performance category (CPC) was evaluated
on day 90. Results: On day 2, ADAMTS13 plasma activity was lower in 28-day
non-survivors (n = 12) than in 28-day survivors (n = 21) (54.0 ± 23.2% vs.
82.3 ± 26.2%, p < 0.05), and lower in patients with poor neurological outcome
(CPC 3–5; n = 17) than in patients with good neurological outcome (CPC 1–2;
n = 16) (59.6 ± 26.6% vs. 87.6 ± 23.0%, p < 0.01). Soluble thrombomodulin,
an endothelial damage marker, levels on day 1 showed strong correlation with
ADAMTS13 activity on day 2 (p < 0.05). Further, on day 2, ADAMTS13 activity showed negative correlations with SOFA score and levels of plasminogen activator inhibitor-1, high-mobility group box 1 protein, and IL-6 (p < 0.05), but
showed positive correlation with the expression of HLA-DR on monocytes (p
< 0.05). Conclusions: Decreased ADAMTS13 activity is associated with high
mortality, poor neurological outcome, and worsened immunoinflammatory
status in R-OHCA patients. These results suggest that ADAMTS13 may have
pathophysiological relevance in PCAS.
10
CPR IN ADULT PATIENTS UNDERGOING MAJOR SURGICAL
PROCEDURES IN USA: PROFILE AND PREDICTORS.
Veerajalandhar Allareddy1, Sankeerth Rampa2, Ashima Das3, Romesh Nalliah4,
David Speicher1, Alexandre Rotta1, Veerasathpurush Allareddy5; 1Rainbow Babies
& Children’s Hospital, Cleveland, OH, 2University of Nebraska Medical University, College of Public Health, Omaha, NE, 3Rainbow Babies & Children’s Hospital, CASE University, Cleveland, OH, 4Dental Medicine, Harvard University,
Boston, MA, 5College of Dentistry, University of Iowa, Iowa City, IA
Learning Objectives: National estimates of cardio pulmonary resuscitation(CPR)
following major surgical procedures(MSP) and associated outcomes are unknown.
We sought to examine the prevalence of CPR in adult patients undergoing MSP
and to elucidate the role of patient related factors on odds of having a CPR
during hospitalization. We hypothesize that a heterogeneous mix of co-morbid
conditions(CMC), infectious complications(IC), age, sex, and race could be
associated with need for CPR. Methods: We analyzed the Nationwide Inpatient
Sample for years 2009–2010 selecting all adult patients who had a MSP. CPR
during hospitalization was used as the primary outcome variable. The association between age, sex, race, insurance status, co-morbid burden, IC, insurance
status, hospital teaching status, and hospital region and the odds of having a CPR
was examined by multivariable logistic regression. Results: Of the 12,631,502
patients who had a MSP, 0.2% had CPR. Odds of having CPR increased: with
increasing age(OR=1.02, p<0.0001), blacks(OR=1.51, 95%CI=1.35–1.68,
p<0.0001, ref:whites), septicemia (OR=2.60, 2.34–2.86, p<0.0001), mycoses
(OR=1.18, 1.04–1.34, p=0.01), or post-operative pneumonia(OR=3.05, 2.75–
3.39,p<0.0001). Patients with CMC such as rheumatoid arthritis/collagen vascular disease(OR=1.23, 1.02–1.48, p=0.03), congestive heart failure(OR=1.59,
1.42–1.77, p<0.0001), coagulopathy (OR=2.54, 2.30–2.81, p<0.0001), diabetes
(OR=1.19, 1.09–1.29, p<0.0001), drug abuse(OR=1.19, 1.03–1.37, p=0.02),
fluid/electrolyte disorders(OR=3.50, 3.18–3.85, p<0.0001), neurological disorders (OR=1.64, 1.45–1.84, p<0.0001), obesity (OR=1.13, 1.03–1.23, p=0.006),
peripheral vascular dis(OR=1.57, 1.41–1.74, p<0.0001), pulmonary circulation dis(OR=2.24,1.94-2.59, p<0.0001), or renal failure(OR=1.71, 1.55–1.88,
p<0.0001) were associated with higher odds for CPR, as were the uninsured,
compared to their counterparts(p<0.0001). Conclusions: In this large surgical
cohort nearly 1 in 500 patients had a CPR. Profile and risk predictors of CPR are
identified. Risk modification may enable optimization of outcomes.
11
LOWER OXYGEN CONCENTRATION REDUCED SYSTEMIC
INFLAMMATORY RESPONSE AND IMPROVED THE OUTCOME OF CPR
Shen Zhao1, JIE QIAN1, Jiangang Wang1, PING GONG2, Zhengfei Yang3, Jena
Cahoon4, Xiaobo Wu5, Wanchun Tang1; 1Weil Institute of Critical Care Medicine, Rancho Mirage, CA, 2Weil institute of critical care medicine, rancho mirage,
CA, 3Weil Institute of Critical Care Medicine, Guangzhou, Guangdong,4the Weil
Institute of Critical Care Medicine, Rancho Mirage, CA, 5Weil Institue of Critical Care Medicine, Rancho Mirage, CA
Learning Objectives: Oxidative injury triggered by CPR is associated with
a systemic inflammatory response. This study was to investigate the effects of
lower inspired oxygen concentration on systemic inflammatory response and
the outcomes of CPR. We hypothesized that lower inspired oxygen concentration inhibits systemic inflammatory response and improves the cardiac and
neurologic outcomes of CPR. Methods: Ventricular fibrillation was induced
and untreated for 8 mins in 23 male Sprague-Dawley rats. Defibrillation was
attempted after 8 mins of CPR. The animals were randomized into three groups:
mechanical ventilation with 100%, 50% and 21% O2 during CPR and one
hr following the return of spontaneous circulation. Normoxic ventilation was
maintained thereafter. Serum inflammatory biomarker was evaluated using the
enzyme-linked immunosorbent assay (ELISA). Post-resuscitation myocardial and
neurological function were monitored in all animals. Results: Compared with
the 21% and 100% groups, the 50% group demonstrated a lower interleukin-6
[21%: (2040 ± 215)pg/ml, 100%: (1665 ± 185) pg/ml vs. 50%: (1008 ± 105)
pg/ml, p<0.05] and tumor necrosis factor-α [(12 ± 1.3)pg/ml, (9.5 ± 2.0) pg/ml
vs.(6.8 ± 0.9) pg/ml, p<0.05] levels at 4 hrs post-resuscitation. Significantly better
cardiac output [(65.2 ± 7.0)ml/min, (74.3 ± 6.7) ml/min vs.(85.5 ± 8.4) ml/min,
p<0.05] and reduced neurologic deficit scores [at 24 hr: 400 ± 175, 326 ± 105
vs.206 ± 84, p<0.05] were observed in the 50% group. A significantly longer
duration of survival was observed in the 50% group when compared with the
two other groups [5 hrs (95% CI: 2.4–7.6 hrs), 18 hrs (95% CI: 6.9–29.1 hrs)
vs.24 hrs (95% CI: 7.2–29.5 hrs)]. Conclusions: In a rat cardiac arrest model,
ventilation with 50% inspired oxygen during early post-ischemic reperfusion
contributed to a decreased systemic inflammatory response and better cardiac
and neurological function.
12
PRO-INFLAMMATORY CYTOKINES ARE ELEVATED IN
THE RAT HIPPOCAMPUS DURING CARDIOPULMONARY
RESUSCITATION
Jihong Xing1, Xiaoliang Liu1, Jian Lu2; 1First Hospital of Jilin University, Changchun, China, 2Jilin Province Carcinoma Hospital, Changchun, China
Learning Objectives: Pro-inflammatory cytokines (PICs) are small cell-signaling
protein molecules released by both leukocytes and myocytes and lead to nucleus
gene transcription. There is considerable evidence demonstrating that PICs are
present in central nervous system and are involved in regulating pathophysiological functions in numerous acute and chronic ischemic diseases. In this study, we
examined the protein levels of several important PICs in the rat hippocampus after
transient global ischemia induced by cardiac arrest (CA) and cardiopulmonary
resuscitation (CPR). Those PICs measured in this study include tumor necrosis
factor-α (TNF-α), interleukin-6 (IL-6), interleukin-1α (IL-1α), interleukin-1β
(IL-1β), monocyte chemotatic protein-1 (MCP-1), chemokine ligand-5 (CCL-5),
microphage inflammatory protein (MIP), and interferon (IFN). Methods: The
rat model of CA induced by asphyxia was used in the current study. The rats who
survived from CPR were sacrificed 0 hrs as control (n=15), 3 hrs (n=15) and 6
hrs (n=15) after CPR and the hippocampus was obtained for ELISA to determine
the protein levels of those PICs. Note that all data are presented as mean ± SE
and analyzed by ANOVA. Results: Among all PICs, TNF-α, IL-6 and IL-1β (ng/
mg protein) were significant elevated in the hippocampus 3–6 hrs after CPR as
compared with control group. For control, 3 hours and 6 hours groups, TNFα: 0.71 ± 0.06; 0.83 ± 0.02* and1.02 ± 0.05*; IL-6: 1.76 ± 0.09; 2.19 ± 0.10*and
2.28 ± 0.24*; IL-1β:1.66 ± 0.11; 1.91 ± 0.07* and 2.42 ± 0.19*. *indicate: P<0.05
vs. control. Conclusions: Transient global ischemia induced by CA selectively
increases the levels of TNF-α, IL-6 and IL-1β in the rat hippocampus. These
PICs appear to be greater at least 3 hrs after CA and persists. Results of our
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
study suggest that PICs play a role in regulating cerebral ischemia reperfusion
during CPR. PICs-mediated nucleus transcription pathways are likely a target in
improvement of tissues against ischemia.
13
TEACHING SITUATION AWARENESS DURING CARDIAC
ARRESTS AND RAPID RESPONSES - A SIMULATION STUDY
Akiva Andrew Dym1, Carla Venegas-Borsellino2, Maneesha Bangar2, Dmitry
Lisenenkov2, Adam Keene2, Lewis Eisen2; 1Albert Einstein College Of Medicine,
Bronx, NY, 2Montefiore Medical Center, Bronx, NY
Learning Objectives: During rapid responses (RR) and cardiac arrests (CA),
team leaders must be aware of multiple factors simultaneously in order to successfully manage them. Situation awareness (SA) is a necessary skill for leaders to
optimize patient outcomes. SA can be divided into 3 components: facts, comprehension, and projection. SA involves understanding the current situation, having
the ability to look at all the data, synthesizing the information and determining
its relevance. We hypothesized that residents’ SA and ability to manage RR/CA
scenarios can be improved with simulation training. Methods: Internal Medicine
residents (n=48) participated in 8 RR/CA scenarios using High Fidelity Simulation (HFS). They were scored in 2 pre-training cases, then received feedback and
education about SA and RR/CA management, participated in 4 more cases for
education penetrance, and scored again in 2 cases as post-training evaluation. A
modified SABAR (Situation Awareness Behaviorally Anchored Rating) scale was
used, ranging from 1 (very poor) to 5 (very good). Scoring was performed by a
trained observer. Results: After training the residents’ SA during RR/CA scenarios improved from 2.4+0.6 to 4.4+0.4 (p< 0.01). All 20 evaluated items showed
statistically significant improvement (p<0.01) The greatest improvements were
in: employ team members appropriately to perform needed tasks (2.1 to 5.0); use
team members to effectively assess the situation (1.8 to 4.4) and ask for pertinent
information (2.4 to 4.7). After training the lowest scores were in: gather follow
up information when needed (3.4); perform a team leader’s overview (3.5); project future possibilities and create contingency plans (3.5). Conclusions: Novice
code leaders often struggle with maintaining awareness of the dozens of inputs
they may receive during a RR/CA situation. HFS training improves SA of medical residents markedly and rapidly. Although improved, residents still had some
difficulty with items related to taking a general overview and projection of the
future patient course.
15
ZONIPORIDE COMBINED WITH Α-MNE OPTIMIZES THE
HEMODYNAMIC EFFICACY OF CHEST COMPRESSION
Lorissa Lamoureux1, Herbert Whitehouse1, Jeejabai Radhakrishnan2, Alvin Baetiong1, Raul Gazmuri3; 1Rosalind Franklin University of Medicine and Science,
North Chicago, IL, 2Rosalind Franklin University, North Chicago, IL, 3Captain
James A. Lovell Federal Health Care Center, North Chicago, IL
Learning Objectives: We have reported that Na+-H+ exchanger isoform-1
(NHE-1) inhibition preserves left ventricular distensibility during resuscitation from VF enabling generation of higher blood flows for a given compression depth. Others have shown that α-methylnorepinephrine (α-MNE) - a
peripheral selective α2-adrenoreceptor agonist - is superior to epinephrine
given its lack of β-agonist effects shown to intensify myocardial ischemia. We
assessed in a rat model of VF and closed-chest resuscitation the effects of combining the NHE-1 inhibitor zoniporide (ZNP) with α-MNE by measuring
aortic pressure and end tidal CO2 tension (PETCO2) – a surrogate of blood
flow during CPR when ventilation is controlled. Methods: VF was induced
in 32 male rats and resuscitation attempted 8 minutes later by 8 minutes of
chest compression (200 compressions/min) and ventilation with 100% oxygen
(25 unsynchronized breaths/min with a tidal volume of 6 ml/kg) followed by
delivery of electrical shocks. Rats were randomized 1:1:1:1 to receive a 3 mg/kg
bolus of ZNP or 0.9% NaCl before chest compression and a 100 μg/kg bolus
of α-MNE or its vehicle at minute 2 of chest compression. Results: Administration of α-MNE, as expected, increased the aortic pressure; yet the PETCO2
varied contingent on ZNP. In its absence, PETCO2 decreased by approximately 50% of the value before α-MNE administration (p < 0.001); whereas,
in its presence PETCO2 remained at pre-α-MNE levels and comparable to
ZNP alone and to vehicle controls. More rats treated with the α-MNE/ZNP
combination were resuscitated and survived an observation interval of 240
minutes. Conclusions: We interpret reductions in PETCO2 by α-MNE as
secondary to reductions in blood flow generated by chest compression, possibly resulting from accelerated reductions in left ventricular distensibility.
Maintenance of PETCO2 by ZNP would suggest preservation of left ventricular distensibility and therefore left ventricular filling before compression;
thus, supporting further work on the α-MNE/ZNP combination for cardiac
resuscitation.
16
14
CENTRAL VENOUS PRESSURE: IS IT AN ACCURATE REFLECTION OF INTRAVASCULAR VOLUME STATUS?
VIDEO LARYNGOSCOPY IMPROVES ODDS OF FIRST
ATTEMPT SUCCESS AT INTUBATION IN THE INTENSIVE
CARE UNIT
Catherine Lindsay McKnight1, Chayanin Musikasinthorn1, Scott Harvey1, David
Inouye1, Michael Hayashi1, Nicole Morikawa1, Christie Nakamura1, Mihae Yu1;
1
University of Hawaii School of Medicine, Honolulu, HI
Learning Objectives: Tracheal intubation in the Intensive Care Unit (ICU) is
associated with a high risk of procedural complications relative to the Operating Room or Emergency Department. ICU patients have poor physiologic
reserve and are less tolerant of prolonged attempts at intubation. Complication
rates increase with the number of attempts at intubation and because of this,
optimizing First Attempt Success (FAS) has become the goal in airway management research. It has been demonstrated outside of the ICU that the use of
video laryngoscopy (VL) improves the rate of FAS, however fewer data exist
comparing VL against traditional Direct Laryngoscopy (DL) in the ICU. The
purpose of this study was to test the hypothesis that use of VL improves the
odds of FAS in the ICU. Methods: Prospective observational study of 664 consecutive patients intubated in the ICU of a university medical center from January 1, 2012-June 30, 2014. Data were collected through a continuous quality
improvement program on all patients intubated in the ICU over the study
period. Data relating to patient demographics, intubation, and complications
were analyzed. A propensity adjustment was performed to account for factors
influencing the decision to use VL. An adjusted multivariate regression analysis
was performed to evaluate the odds of FAS when VL was used compared to DL.
Results: Over the study period there were 120 patients intubated with DL, and
544 patients intubated with VL. There were no significant differences in patient
demographics. The median total difficult airway predictors (DAPs) for patients
intubated with DL was 1.5 (IQR 1–3) and for VL was 2 (IQR 1–3, p=ns). FAS
for DL was 68% (95%CI 58%-76%) and 80% for VL (95%CI 77%-84%).
The unadjusted odds of FAS for VL was 1.96 (95%CI 1.27–3.04, p=0.003).
The propensity adjusted odds of FAS when VL was used, controlling for total
DAPs and operator level of training was 2.38 (95%CI 1.44–3.95, p<0.001).
Conclusions:After controlling for potential confounders, this propensityadjusted analysis demonstrates improved odds of FAS at intubation in the ICU
with the use of a video laryngoscope.
Learning Objectives: Guidelines for fluid resuscitation frequently use a central venous pressure (CVP) of 8–12 as an endpoint. Blood volume analysis (BVA) measures circulating blood volume and may be a better guide for
fluid management. (1) CVP may not reflect intravascular volume status.
Methods: Patients with Septic Shock, Severe Sepsis, Cardiovascular collapse,
Respiratory failure with PaO2/FiO2 < 150 while on PEEP ≥12 cm H20, had
simultaneous measurement of CVP and BVA (BVA-100, Daxor, NY, NY) at
approximately 24 and 48 hours after resuscitation (Day 1 and Day 2 respectively). Albumin tagged with I-131 was injected and allowed to mix completely throughout the circulation for 12 minutes. To correct for albumin
transudation, serial blood measurements of 5 mL were collected at 12, 18, 24,
30, and 36 minutes post albumin I-131 injection and extrapolated to time
zero to calculate the plasma volume (PV). The red cell volume (RBCV) was
derived from Hematocrit = (RBCV)/(RBCV+PV). Whole blood volume =
PV+RBCV. BV values were compared to patient’s normal volumes to account
for size differences. BV of 0 to 10% from normal was categorized as normal,<0% as low, and >10% as high. CVP measurements were grouped into 3
categories:>12 mm Hg (high), 8–12 mm Hg (normal), and <8 mm Hg (low).
Results: 50 patients were studied: mean age was 63 ± 16 years, 32 male: 18
female, APACHE II score was 27 ± 2 with a mortality rate of 26%. 41 patients
contributed 2 data points at Day 1 and Day 2, while 9 patients contributed 1
data point at Day 1. Of the 52 data points for CVP >12 mmHg group (high
CVP group), BV results demonstrated 34 high, 12 normal, and 6 low BV
values. Of the 36 data points for the CVP 8–12 mmHg (normal CVP group),
BV results demonstrated 19 high, 8 normal, and 9 low BV values. Of the 3
data points for the CVP<8 mm Hg (low CVP group), BV was low in all 3
instances. Hypovolemia was seen in 15/88 times when the CVP values were
normal or high. Conclusions: Patients who demonstrate a normal or high
CVP value after fluid resuscitation, can be hypovolemic 17% of the time. (1)
Yu, M et al, Shock 2011;35:220–228.
Cameron Hypes1, John Sakles1, Josh Malo1, John Bloom1, Jarrod Mosier1; 1University of Arizona, Tucson, AZ
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Oral Abstract Session: Epidemiology
17
19
EPIDEMIOLOGY AND OUTCOMES OF IN-HOSPITAL CARDIAC ARREST ACROSS HOSPITALS OF VARIED CENTER
VOLUME
EPIDEMIOLOGY OF ACUTE KIDNEY INJURY AND FLUID
OVERLOAD IN CRITICALLY ILL CHILDREN
Punkaj Gupta1, Casey Lauer2, Xinyu Tang3, Christine Gall4, Thomas Rice5,
Randall Wetzel6; 1Arkansas Children’s Hospital, Little Rock, AR, 2VPS, LLS,
Milwaukee, WI, 3Arkansas Childrens Hospital, Little Rock, AR, 4Virtual PICU
Systems, LLC, Los Angeles, CA, 5Children’s Hospital of Wisconsin, Milwaukee,
WI, 6Children’s Hospital of Los Angeles, Los Angeles, CA
Learning Objectives: Relationship between center volume and cardiac arrest rate
(or survival after an arrest) in children with critical illness has not been investigated to date. It is hypothesized that a high center volume may help maintain
a team approach and adherence to protocol, and thereby decrease incidence of
cardiac arrest and improve outcomes for patients with cardiac arrest. To address
these knowledge gaps, we undertook this study of epidemiology and outcomes
of in-hospital cardiac arrest among critically ill children across centers of varying
center volume using the Virtual PICU Systems (VPS, LLC) Database. Methods:
Patients <18 years of age in the VPS, LLC Database (2009–2013) were included.
Patients with both cardiac and non-cardiac diagnoses were included. Data on
demographics, patient diagnosis, cardiac arrest, severity of illness and outcomes
were collected. Hierarchical cluster analysis was performed to categorize all the
participating centers into low, low-medium, high-medium, and high volume
groups using the center volume characteristics. Multivariable models were used
to evaluate association of center volume with incidence of cardiac arrest, and
mortality after cardiac arrest, adjusting for patient and center characteristics.
Results: Of 329,982 patients (108 centers), 2.2% (n= 7,390) patients had cardiac
arrest with an associated mortality of 35% (n=2,586). In multivariable models
controlling for patient and center characteristics, center volume was not associated with either the incidence of cardiac arrest (OR: 1.00; 95% CI: 0.95–1.06;
p=0.98), or mortality in those with cardiac arrest (OR: 0.93; 95% CI: 0.82–1.06;
p=0.27). These associations were similar across cardiac and non-cardiac disease
categories. Conclusions: Both incidence of cardiac arrest, and mortality in those
with cardiac arrest vary substantially across hospitals. However, center volume
is not associated with either of these outcomes, after adjusting for patient and
center characteristics.
18
ADR SURVEILLANCE USING A MULTICENTER CLINICAL
DATABASE: PROPOFOL RELATED INFUSION SYNDROME
INCIDENCE
Priyank Yagnik1, Vinai Modem1; 1University of Texas Southwestern Medical Center, Dallas, TX
Learning Objectives: Acute kidney injury (AKI) and fluid overload (FO) are
common problems in the intensive care unit (ICU). In this study, our objective
was to describe the epidemiology of AKI and FO and to identify their association with ICU mortality. Methods: In this retrospective cohort study, all children (≤ 18 years) admitted to our ICU between Jan 2010 and Dec 2012 were
eligible. Exclusion criteria were children with < 3 days of ICU stay and children
admitted to trauma and cardiac ICU. We measured creatinine clearance (CrCl)
with Schwartz formula and daily cumulative fluid balance. Cumulative fluid
balance was assessed as net fluid balance since ICU admission and expressed
as a % of body weight. Survivors were compared with non-survivors for renal
function and fluid balance during the first 3 days of ICU stay. We adjusted
confounders by multivariate logistic regression analysis. Results: 1043 children
met the study criteria. ICU mortality was 4.3% (N=45). Infection-related diagnoses were seen in 40% (N=424) of whom 24% had sepsis (N=103). Infants (1
month to 2 years) were the predominant age group (40%, N=413). Neonates
(<1 month) had the highest mortality (10%) and school-age children (6–12
years) had the lowest mortality (1%). Median fluid balance on ICU day 3 was
7% (IQR 3–12%). Fluid balance >12% on day 3 was associated with increased
mortality (OR 2.24, p 0.02). Median CrCl was higher for survivors compared
to non-survivors on admission (95 vs. 69 ml/min/1.73m2, p<0.001) and on day
3 (110 vs. 69 ml/min/1.73 m2, p<0.001). CrCl <60 ml/min/1.73m2 was associated with higher mortality both on admission (OR 2.25, p 0.03) and day 3 (OR
2.6, p 0.01). Multivariable logistic regression analysis showed CrCl at the time
of admission (categorized into five stages) as a significant predictor of mortality
after adjusting for other covariates including age group and diagnosis categories
(OR 1.43, p 0.009). Conclusions: In our large, retrospective cohort study of
critically ill children, lower CrCl at the time of ICU admission and cumulative fluid balance > 12% on day 3 of ICU stay were independent predictors of
mortality
20
HETEROGENEOUS TREATMENT EFFECT OF RED BLOOD
CELL TRANSFUSION (RBCT) IN THE CRITICALLY ILL
PATIENTS
Omar Badawi1, Ashleigh Lowery2, Erkan Hassan1, Reza Sedeh3, Usha Raghavan3,
Daniel Elgort3; 1Philips Healthcare, Baltimore, MD, 2University of Maryland
Medical Center R Adams Cowley Shock Trauma Center, Baltimore, MD, 3Philips Research North America, Briarcliff Manor, NY
Xinggang Liu1, Omar Badawi1, Christine Franey2, Ilene Zuckerman2, Craig
Lilly3; 1Philips Healthcare, Baltimore, MD, 2University of Maryland, Baltimore,
MD, 3University of Massachusetts Memorial Medical Center / EICU Support
Center, Worcester, MA
Learning Objectives: Propofol (PF) related infusion syndrome (PRIS) has been
reported in ICU patients (pts) receiving prolonged, high doses of PF and carries a
mortality rate > 50%. Most PRIS literature is based on case reports and although
estimated to occur in 1.1% of pts on PF for >24 hrs, the actual incidence is
unclear. The goal was to estimate the incidence of PRIS through evaluation of
a large, multicenter ICU clinical database. Methods: ICU pts with continuous
infusion sedatives (CI-S) between 2007–2012 in the Philips eICU Research Institute database were evaluated for PRIS. Exclusions: rhabdomyolysis; pancreatitis;
cardiac arrest; renal failure (RF) on ICU admission. PRIS defined as all of the
following after PF exposure: metabolic acidosis, acute RF, cardiovascular failure
and either TG>400mg/dL or CPK>10,000mcg/L. The total dose and duration
of PF was calculated from nurse charting. A falsification hypothesis estimated the
incidence of a PRIS-like syndrome (PLS) in pts receiving CI-S other than PF. The
primary outcome was PF attributable risk (AR) of PRIS defined by the incidence
difference in PF vs non-PF pts. P-values were calculated using Fisher’s exact test
for AR, Chi-square for mortality and t-test for all others. Results: 80,939 pts
receiving CI-S (52,847 PF and 27,992 non-PF). 43% of pts administered CI-S
were in a mixed ICU; 22% surgical; 22% cardiac; 8% medical; 5% other. 133
(0.25%) of pts on PF met PRIS criteria compared to 44 (0.16%) of non-PF pts
(p=0.006). The estimated AR from PF was 0.09%. The median cumulative dose
and duration of PF at the time of PRIS was 90mg/kg and 51 hrs respectively.
No significant difference between PRIS and PLS pts in any of the following: avg
APACHE IV scores= 94 vs 107 (p=0.05); hospital mortality=50.4% vs 65.9%
(p=0.06); avg age=51 vs 53 years (p=0.42). Conclusions: By leveraging a large
multicenter clinical database for ADR surveillance, the incidence of PRIS attributable to PF is estimated at 0.09%. A previously undescribed PLS syndrome can
occur in the absence of PF. It is unclear if PLS represents natural disease progression or is secondary to use of CI-S.
Learning Objectives: Despite substantial evidence suggesting restrictive RBCT
strategies for critically ill, very little is known about the heterogeneity of benefit
in the general ICU population. We hypothesize the benefit of RBCT varies by
patient (pt) subtypes and physiology immediately prior to RBCT. Methods:
All adult ICU pt admissions between 1/1/2008 and 6/30/2012 with complete
input/output data and calculated APACHE IV score were included from the
Philips eICU Research Institute database. In a discrete time survival model, ICU
length of stay (LOS) was restructured into 6 hr intervals. Pt exposure to RBCT
and the corresponding Hgb within current interval and 3 intervals before were
examined in a logistic regression which modelled the log odds of dying within
current interval as outcome, while adjusting for age, gender, race, APACHE IV
score, time since admission, and time-varying hemodynamic status. Results:
376,049 ICU pt stays were included. 50,549 pts were diagnosed with acute
bleeding, 78,863 with shock or hypovolemia, and 112,138 did not have a diagnosis possibly associated with higher risk of receiving RBCT. Among pts without
a high risk diagnosis, the odds ratio (OR) for death within the current 6 hr
interval for RBCT was 0.13(0.04 to 0.44), 0.36(0.16 to 0.79) and 0.30(0.09
to 0.95) for Hgb<7g/dL, 7-<8g/dL and 8-<9g/dL, respectively. RBCT given at
Hgb>=9g/dL did not yield a difference in ICU mortality. Pts with acute bleeding
(OR: 0.40; 0.20–0.93) and shock or hypovolemia (OR: 0.37; 0.20–0.70) benefited from transfusion at an Hgb between 9-<10g/dL. In contrast, no benefit
is observed with RBCT among patients surviving the 6 hr transfusion interval, in all three groups regardless of the Hgb level. Conclusions: Patients with
active bleeding, shock, or hypovolemia receive immediate mortality benefit from
RBCT given at a higher Hgb than those without any high risk diseases or conditions. The greatest benefit of RBCT was observed when given to ICU patients
with immediate risk of dying while limited benefit or even harm is observed
when given to stable patients.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
21
23
HOSPITALIZATIONS & OUTCOMES ATTRIBUTED TO EPIDERMAL NECROLYSIS IN USA: PREDICTORS OF MORTALITY.
THE OBESITY PARADOX IS NOT OBSERVED IN CRITICALLY
ILL PATIENTS ON EARLY ENTERAL NUTRITION
Sankeerth Rampa1, Romesh Nalliah2, Veerasathpurush Allareddy3, David
Speicher4, Veerajalandhar Allareddy4, Alexandre Rotta4; 1University of Nebraska
Medical University, College of Public Health, Omaha, NE, 2Dental Medicine,
Harvard University, Boston, MA, 3College of Dentistry, University of Iowa, Iowa
City, IA, 4Rainbow Babies & Children’s Hospital, Cleveland, OH
Learning Objectives: Severe mucocutaneous reactions marked by extensive
necrosis and detachment of the epidermis (epidermal necrolysis [EN]) include
the spectrum of Stevens-Johnson syndrome (SJS,<10% body surface area), toxic
epidermal necrolysis (TEN,>20% BSA) and the SJS-TEN overlap(10–20%BSA).
Large population-based hospitalization outcomes attributed to EN are lacking. We
sought to describe the outcomes associated with EN hospitalizations and examine the association between mortality and various patient/hospital-level factors.
Methods: We performed an analysis of the Nationwide Inpatient Sample, for the
years 2009–2010.for all hospitalizations with a primary diagnosis of SJS(ICD9-CM-965.13), SJS-TEN overlap(965.14) or TEN syndrome(965.15). Primary
outcome variables of interest included in-hospital mortality(IHM), length of
stay(LOS) and hospital charges(HC). Multivariable logistic regression analysis was
used to examine the association between IHM and patient/hospital characteristics. Results: There were,5978 hospitalizations attributed to EN (SJS:4215, SJSTEN:1048, TEN:715). Characteristics of SJS, SJS-TEN, TEN included: mean
age(46.2y; 51.1y; 55.5y), males(48.4%, 38.6%, 44.8%), whites(56.3%, 45.5%,
39.4%), presence of at least 1 co-morbid condition(78.5%, 92.1%,88.9%), and
hospitalization teaching status(53.9%, 75.9%, 66.9%), respectively. Outcomes of
SJS, SJS-TEN, TEN included LOS(6.4d;13.4d;12.8d), HC ($44638; $172,625;
$142,948), and IHM(2.5%; 10.4%; 14.5%) respectively. The majority of deaths
in EN occurred in patients aged greater than 40years. Predictors of IHM included
SJS-TEN (2.63[1.24–5.57],p=0.01)TEN (4.9[2.43–9.88],p<0.001),ref(SJS);
each 1unit increase in comorbid burden (1.31[1.1–1.57],p<0.0001);and in teaching hospitals(TH) (2.98[1.43–6.20],p<0.0001), ref(non TH) Conclusions:
In this large retrospective study of EN necessitating hospitalization, age(> 40y),
BSA(>10%), and presence of co-morbidity were predictors of higher IHM. Teaching hospitals had higher odds of mortality, however, SJS-TEN group and those with
co-morbid conditions were more likely to receive care in teaching hospitals.
Kimberley Harris1, Jiachen Zhou2, Erkan Hassan2, Xinggang Liu2, Omar
Badawi2; 1University of Maryland Medical Center, Baltimore, MD, 2Philips
Healthcare, Baltimore, MD
Learning Objectives: The obesity paradox in the ICU has been described as
improved survival for obese critically ill patients compared to those with normal body mass index (BMI). The role of nutrition in the relationship between
BMI and survival is unclear. We hypothesize that early enteral nutrition modifies the relationship between BMI and mortality such that the protective benefit of high BMI will not be observed in patients receiving enteral nutrition.
Methods: The Philips eICU Research Institute database composed of patients
in tele-ICU programs between 2004 and 2014 within the US was used in this
study. Adults with an APACHE IV score and BMI were included. Early enteral
nutrition was defined by an order for enteral nutrition within the first 48 hours
of ICU admission. The relation between BMI categories and hospital mortality
was estimated by multivariable modified Poisson regression models. The relative
risk (RR) of hospital mortality was described for each BMI category relative to
18.5–24.9 for all and repeated within the stratum of patients with early enteral
nutrition. Results: 1,163,234 ICU stays from 292 units were included with an
average age of 63.3 years, APACHE IV score of 54.2, and hospital mortality of
8.6%. Compared to patients within a normal range of BMI (18.5–24.9), hospital mortality was elevated among the underweight (BMI <18.5) (RR 1.22, 95%
CI 1.19–1.25) and reduced among BMI groups 25–29.9 (RR 0.89, 95% CI
0.88–0.91), 30–34.9 (RR 0.88, 95% CI 0.86–0.89), 35–39.9 (RR 0.88, 95%
CI 0.85–0.90), and 40–49.9 (RR 0.91, 95% CI 0.88–0.93). However, among
the 85,177 patients on early enteral nutrition, no reduction in mortality was
observed among BMI groups 25–29.9 (RR 0.99, 95% CI 0.95–1.02), 30–34.9
(RR 0.96, 95% CI 0.92–1.00), 35–39.9 (RR 0.96, 95% CI 0.91–1.02), and
40–49.9 (RR 1.01, 95% CI 0.95–1.07) compared to the normal BMI group.
Conclusions:The obesity paradox was observed in this large cohort of critically
ill patients but not among those on early enteral nutrition. These data suggest
that early enteral nutrition modifies the relationship between BMI and mortality
among the critically ill.
24
22
PREDICTORS OF HOME DISCHARGE AMONG SURVIVORS
OF NECROTIZING FASCIITIS: A POPULATION-BASED STUDY
Lavi Oud1, Phillip Watkins2; 1Texas Tech University Health Sciences Center,
Odessa, TX, 2Texas Tech University HSC, Lubbock, TX
Learning Objectives: Necrotizing fasciitis (NF) is associated with high resource utilization and increased mortality; there are no population-level data on the residual
morbidity among hospital survivors of NF and the factors affecting their disposition.
Methods: We used the Texas Inpatient Public Use Data File to identify hospitalizations with NF for patients aged ≥15 years for the years 2001–2010, using ICD-9-CM
code 728.86. Multivariate logistic regression models were used to examine candidate
predictors of H. We examined patients’ demographics, health insurance, chronic comorbidities, hospital type, and development and type of organ failures. Results: There
were 12,172 NF hospitalizations during study period, with 54% males, aged <65 years
in 76%, with ICU care in 50.3%, and hospital mortality 9.3%. Among hospital survivors, 60.7% were discharged home. The following key predictors were independently
associated with reduced H (odds ratio [OR] and interquartile range [IQR]): Age ≥75
yrs 0.3 (0.2–0.4), Medicare insurance 0.6 (0.5–0.7), congestive heart failure 0.8 (0.7–
0.9), chronic liver disease 0.7 (0.5–0.9), respiratory failure 0.5 (0.4–0.6), septic shock
0.7 (0.6–0.8), and renal failure 0.7 (0.6–0.8). The following covariates were associated
with increased odds of H: male 1.2 (1.1–1.3), Hispanic 1.2 (1.1–1.3), lack of health
insurance 2.2 (1.9–2.5), and teaching hospital 1.3 (1.1–1.4). Conclusions: The present cohort of NF is the largest reported to date. Older age, Medicare insurance, selected
chronic co-morbidities, and type of failing organs adversely affected H. Unexpectedly,
male gender, Hispanic ethnicity, lack of health insurance, and being managed at a
teaching hospital appeared to be associated with lower residual morbidity and thus H.
Our findings require further corroboration in other populations.
EPIDEMIOLOGIC FEATURES AND OUTCOME OF SEPSIS IN
NEUROLOGIC INTENSIVE CARE UNIT PATIENTS
Farid Sadaka1, Margaret Cytron1, Kimberly Fowler1, Victoria Javaux1, Jacklyn
O’Brien1; 1Mercy Hospital St Louis/St Louis University, Saint Louis, MO
Learning Objectives: Sepsis is a major contributor to mortality in patients admitted
to a general intensive care unit (ICU). Early recognition and treatment of sepsis is
key in improving outcomes. The epidemiology and outcome of sepsis in neurologic
ICU (NeuroICU) has not been evaluated. Methods: We retrospectively identified
all patients admitted to our 16 bed NeuroICU between 6/2009 and 12/2013 using
the APACHE Outcomes database. We excluded patients admitted with an infection,
such as meningitis, encephalitis, brain or spinal abscess, or with any other infection. We compared NeuroICU patients who did to NeuroICU patients who did not
develop sepsis after ICU admission. The diagnosis of sepsis was based on the Surviving Sepsis Campaign definition. Results: There were a total of 2025 patients, out
of which 29 patients (1.4 %) developed sepsis. Patients who developed sepsis were
older (67 ± 13 vs 61 ± 11 years, p = 0.07), had more male gender (69% vs 51.5%, p =
0.07), higher acute physiologic and chronic health evaluation (APACHE) III scores
(58 ± 17 vs 43 ± 21, p = 0.0001), and higher acute physiologic scores (APS) (43 ± 16
vs 32 ± 18, p = 0.001) than patients who did not develop sepsis. Patients who developed sepsis had higher ICU mortality (41.4 % vs 5.1 %, odds ratio [OR] = 13.1;
95% confidence interval [CI], 6.1 – 28.2, p < 0.0001), and higher hospital mortality (44.8% vs 8.2 %, OR = 9.0; 95% CI, 4.3 – 19.0, p < 0.0001). Conclusions:
Sepsis developed in 1.4% of patients admitted to a NeuroICU. Predictors of sepsis
development were comorbidities and worsening acute physiologic variables. Patients
who developed sepsis had significantly higher mortality. Vigilance to development of
sepsis in neuroICU is paramount, especially in this era when early recognition and
intervention of sepsis significantly improves outcomes.
Oral Abstract Session: Neuroscience
25
DIFFERENCES IN END OF LIFE CARE FOR INTENSIVE CARE
UNIT (ICU) PATIENTS WITH VS. WITHOUT CANCER
Geoffrey Koff1, Edward Len1, David Oxman, MD1, Urvashi Vaid1; 1Thomas Jefferson University Hospital, Philadelphia, PA
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Learning Objectives: Cancer is a common comorbidity of critically-ill patients,
and the utilization of ICU care by patients with cancer is increasing. We explored
whether having cancer at the time of ICU admission influenced end of life care
and the intensity of ICU treatments amongst patients who ultimately died in the
ICU. Methods: We conducted a retrospective analysis of consecutive medical
ICU patient deaths over an 18 month period in an urban tertiary care hospital
using electronic records. Active malignancy was defined as a recognized ongoing
malignancy with or without concurrent treatment. Patient demographics, comorbidities, diagnosis, intensity of care provided, code status changes, palliative care
consultation, time to first family meeting, and cause of death, were collected.
Results: There were a total of 403 patient deaths; 182 patients had a diagnosis
of active malignancy at time of ICU admission (45%). The ICU length of stay
for patients with malignancy compared to no malignancy was 4 days and 5 days,
respectively (p=0.048). The time to a DNR code status change was 1 day shorter
in patients with malignancy (p=0.47). There was both a decreased incidence of
mechanical ventilator usage as well as a decrease in ventilator days in patients with
malignancy (70.7% vs. 83.7%, p<0.01; 3 vs. 4 days, p<0.01). Time to first family
meeting was 1 day shorter in the malignancy group (p<0.01), and consultation
of palliative care services were more common in the malignancy group (32.4%
vs. 17.6%, p<0.01). There were no significant differences in patient demographics, admission code status, ICU admission diagnosis, or withdrawal of life support between the two groups. Conclusions: We concluded that the diagnosis of
malignancy influences the aggressiveness of care and utilization of palliative care
in the medical ICU. Compared to patients without active malignancy, patients
with cancer stop life support earlier and use palliative care services more often.
It is unclear if this difference is due to patient/surrogate preferences and earlier
readiness for end of life or clinician biases toward the use of life support.
26
EFFECT OF STEROIDS ADMINISTRATION ON BRAIN DEAD
ORGAN DONORS AND RECIPIENTS: A SYSTEMATIC REVIEW
Frederick D’Aragon1, Arnav Agarwal2, Maureen Meade3, Emilie Belley-Cote1,
Anne Julie Frenette4, Francois Lamontagne5, Sonny Dhanani6; 1McMaster University, N/A, 2McMaster University, Hamilton, Ontario, 3Hamilton Health Science Corp., Hamilton, ON, 4Montreal General Hospital, Montreal, QC, 5Centre
Hospitalier Universitaire De Sherbrooke, Sherbrooke, QC, 6Childrens Hospital
Eastern Ontario, Ottawa, ON
Learning Objectives: Administration of Methylprednisolone is recommended by
North American guidelines on brain dead organ donors. These recommendations
are based on observational studies. RCTs have been published since guidelines
publication. The aim of this systematic review was to evaluate the clinical efficacy
of steroids on brain dead donors and to assess the quality of these RCTs. Methods:
A search through EMBASE, MEDLINE and CENTRAL was conducted from
inception to February 2014. An extensive search of grey literature was also realized. RCT involving administration of steroid to brain dead donors was included
for full review. Studies were assessed in duplicate. In case of disagreement, a third
party took the decision. Sought outcomes were vasopressor requirement, physiologic parameters, organ recovery and graft outcomes. If needed, trial authors
were contacted for additional information. The GRADE approach was used to
summarize the quality of evidence for each outcome. Results: Our search identified 2949 citations. Ninety one full text articles were assessed for eligibility. Seven
met eligibility criteria and 4 articles were identified through the grey literature.
There was a good agreement for relevance (minimum k=0.64) and an excellent
agreement for eligibility(minimum k =1.0). Most studies administered boluses of
Methylprednisolone 5–8 hours before organs recovery. There was no difference
between groups on vasopressor requirement, number of organ recovered and graft
outcomes in each study. When pooled, there was no difference on vasopressor
requirement (3 studies;N=452,RR 0.95 [95%CI 0.83to1.08]), number of multiorgan donors (2 studies;N=309,RR 0.89 [95%CI 0.64to1.24]) or kidney graft
survival at 3 months (4 studies;N=251,RR 1.00 [95%CI 0.81to1.22]). There was
significant clinical and statistical heterogeneity for each of these outcomes. The
quality of evidence for each outcome was very low. Conclusions: The findings
suggest no evidence to support administration of steroids in brain dead donors.
Several methodological challenges in donor management research need to be
address for future well designed RCTs
27
BENEFITS OF LEVETIRACETAM AFTER CONTROLLED
CORTICAL IMPACT IN RATS: STUDIES FROM THE OBTT
CONSORTIUM
Megan Browning1, Samuel Poloyac2, Edward Dixon3, Philip Empey3, Travis Jackson4, Erik Brockman1, Jeremy Henchir3, Patrick Kochanek5; 1Children’s Hospital of Pittsburgh of UPMC, Pittsburgh, PA, 2University of Pittsburgh School
of Pharmacy, Pittsburgh, PA, 3University of Pittsburgh, Pittsburgh, PA, 4Safar
Center for Resuscitation Research, University of Pittsburgh School of Med, Pittsburgh, PA, 5Safar Center for Resuscitation Research, Pittsburgh, PA
Learning Objectives: Operation Brain Trauma Therapy (OBTT), a multi-center
pre-clinical drug and biomarker screening consortium that tests new TBI therapies, selected levetiracetam as its 5th medication. Despite limited preclinical
TBI studies, levetiracetam emerged as a candidate given its sporadic clinical use
treating posttraumatic seizures and favorable safety profile. Its proposed actions
in TBI (potentiation of GABAergic and calcium channel inhibition) may confer
anticonvulsant, anti-excitotoxic and other benefits. Levetiracetam administration
early after TBI in rats will result in improved functional and histologic outcome
vs. vehicle. Methods: We assessed the efficacy of a single 15min post-injury IV
dose (54 or 170mg/kg) on neurobehavioral and neuropathological outcomes in
the controlled cortical impact (CCI) model. After randomization into 4 groups
(Sham, TBI vehicle, TBI low dose, TBI high dose), 40 male Sprague-Dawley
rats underwent CCI (4m/s, 2.5-mm deformation) or sham surgery followed by
IV levetiracetam/vehicle (normal saline). Motor function (beam-balance/beamwalk) was assessed on d1-5 and Morris water maze (MWM) (acquisition/probe
trial) on d14-20. Rats were sacrificed on d21 to assess lesion volume and hemispheric tissue loss. ANOVA, and post-hoc testing corrected for multiple comparisons, was used for data analysis. Results: After TBI, beam-balance testing
improved in high but not low dose groups (p<0.05 vs vehicle) while on beamwalk, all groups performed worse than sham (p<0.05). Latency to find the hidden
platform on MWM was higher in vehicle and high dose groups vs. sham, but not
in low dose. Probe trial performance did not differ between groups. Levetiracetam markedly reduced hemispheric tissue loss (p<0.05, high dose vs. vehicle).
Conclusions: Early single IV dosing of levetiracetam produced multiple benefits
across outcome categories after CCI and represents the most promising agent
tested thus far by the OBTT consortium. Our data suggest the need for dose
optimization and therapeutic window, and consideration of clinical evaluation.
Support: US ArmyW81XWH-10-1-0623
28
PLATELET DYSFUNCTION ON THROMBOELASTOGRAM
IS ASSOCIATED WITH INCREASED MORTALITY IN HEAD
TRAUMA
Mitchell Daley1, Evan Peterson2, Zachary Enright3, Joseph Nguyen3, Jayson
Aydelotte4, Thomas Coopwood4, Carlos Brown5; 1N/A, N/A, 2Seton Medical
Center Austin, Austin, TX, 3University Medical Center Brackenridge, Austin,
TX, 4University of Texas Southwestern - Austin, Austin, TX, 5University of Texas
Southwestern - Austin, N/A
Learning Objectives: Adenosine diphosphate (ADP) dysfunction observed on
thromboelastogram (TEG) is an early feature of coagulopathy in traumatic brain
injury. Although ADP inhibition greater than 60% has been shown to predict
severe coagulopathy requiring multiple transfusions in cardiothoracic surgery
patients, the effect of ADP inhibition on outcomes in patients with head trauma
is unknown. The purpose of this study is to determine if ADP platelet dysfunction on TEG is associated with increased in-hospital mortality in patients with
head trauma. The hypothesis is that ADP dysfunction is associated with increased
mortality. Methods: This retrospective chart review evaluated all trauma patients
admitted to an urban, level 1 trauma center from February 2011 to October
2013 who received a TEG. Patients were included if the TEG was drawn within
the first 24 hours of admission and the head abbreviated injury score (AIS) was
greater than or equal to 3. Patients were categorized as ADP dysfunction if the
degree of ADP inhibition on TEG exceeded 60%. Results: A total of 98 patients
were included (ADP dysfunction, n=53; no ADP dysfunction, n=37). The time
from admission to first TEG (ADP dysfunction 222 minutes ± 302 vs. no ADP
dysfunction 240 minutes ± 284 minutes; p=0.78), initial Glasgow Coma Scale
[GCS (11 ± 5 vs. 12 ± 4; p=0.26)], and use of pre-injury antiplatelet agents (28%
vs. 30%; p=0.88) was similar between groups. Patients with ADP dysfunction
on TEG had a higher in-hospital mortality rate (32% vs. 8%; p<0.01). ADP
dysfunction was independently associated with in-hospital mortality upon fixed
logistic regression (OR 6.5, 95% CI 1.3–32.9; p=0.02) while controlling for age,
gender, hypotension, GCS and injury severity score. Conclusions: ADP dysfunction on TEG is associated with increased mortality in head trauma patients. Prospective studies should seek to determine if early platelet transfusion in patients
with ADP dysfunction and head trauma improves mortality.
29
SEIZURES AND STATUS EPILEPTICUS EXACERBATE VENTRICULAR INSTABILITY IN CHILDREN WITH EPILEPSY
Wail Ali1, Bubolz Beth2, Danny Castro3, Curtis Kennedy4, Yi-Chen Lai5; 1Baylor
College of Medicine/Texas Childrens Hospital, Houston, TX, 2Baylor College of
Medcine, Texas Children’s Hospital, Houston, TX, 3Texas Children’s HospitalBaylor College of Medicine, Houston, TX, 4Baylor College Of Medicine, Houston, TX, 5Texas Childrens Hospital, Houston, TX
Learning Objectives: Adults with epilepsy exhibit potentially arrhythmogenic cardiac changes. Seizures can acutely exert added arrhythmogenic effects on the heart,
manifested as peri-ictal alterations in the ventricular repolarization. Whether altered
ventricular repolarization occurs following seizures and status epilepticus (SE) in
children; and whether children with epilepsy exhibit more pronounced derangement
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
remain to be fully explored. We hypothesize that altered ventricular repolarization
occurs following seizures/SE in children and is more pronounced in children with
epilepsy. Methods: We retrospectively reviewed pediatric intensive care unit (PICU)
admissions with primary diagnosis of seizures/SE from 2/1/2011 to 2/28/2013.
Patients were classified as control, new onset seizure, or epilepsy. 12-lead EKG were
included if: 1) obtained within 24h of PICU admission; 2) not on cardiac medications; 3) no history of heart disease or ion channel defects. A blinded cardiologist
independently reviewed all EKGs. The stability of ventricular repolarization was
assessed by the short-term variability (STV) of the QTc intervals. STV =(Σ|QTcn+1
- QTcn|)/(N x √2), where |QTcn+1 - QTcn| is the difference between 2 successive
QTc, N is the number of QTc. Data were analyzed using ANOVA or χ2. Results:
Of the 4681 PICU admissions, 442 patients were admitted with the primary diagnosis of seizures/SE. 59 EKG (28 new onset, 31 epileptic) were compared with 28
control EKG. The seizure groups exhibited more ST segment changes (control: 14%,
new onset: 32%, epileptic: 58%, p<0.01) and QRS axis deviation (control: 0%, new
onset: 18%, epileptic: 23%, p<0.05). The epileptic group had higher risk for abnormal EKG with relative risk of 2.5 and odds ratio of 7.3 (p<0.001). The epileptic
group exhibited higher STV (control: 6.5 ± 0.8 ms, new onset: 9.4 ± 0.7 ms, epileptic: 10.1 ± 1.2 ms, p<0.05). Conclusions: Our data suggest that seizures can acutely
affect ventricular repolarization. More pronounced abnormalities in the epileptic
children suggest that they may be at higher risk for seizure-induced arrhythmias.
30
THE EFFECT OF ANEURYSMAL SUBARACHNOID HEMORRHAGE ON WORK PRODUCTIVITY
Elizabeth Crago1, Thomas Price2, Catherine Bender2, Dianxu Ren3, Samuel
Poloyac4, Paula Sherwood3; 1University Of Pittsburgh School of Nursing, Pittsburgh, PA, 2University of Pittsburgh, Pittsburgh, PA, 3University of Pittsburgh
School of Nursing, Pittsburgh, PA, 4University of Pittsburgh School of Pharmacy,
Pittsburgh, PA
Learning Objectives: Aneurysmal subarachnoid hemorrhage (aSAH) is a sudden
debilitating condition affecting many individuals during the most productive times
of their lives. Advanced treatment options have reduced mortality rates but increased
the number of survivors facing deficits in physical and neuropsychological (NP) function. This study examined associations between NP function and work productivity
following aSAH. Methods: Fifty two aSAH subjects, employed prior to hemorrhage,
were recruited from an ongoing NIH study (NIHR01NR004339). Work Limitations
Questionnaire (WLQ), NP tests (executive function, psychomotor speed, attention
and mental flexibility, memory) and Patient Assessment of Own Function (PAOF)
were completed at 3 & 12 months after aSAH. Correlation analyses were completed
using SPSS 19 to examine the relationship between NP and PAOF domains and
with work limitations in each WLQ subscale as well as the total sum score. Results:
Over 20% of subjects reported difficulty in areas of the WLQ at 3 & 12 months.
Lower scores on the WLQ in time management and mental/interpersonal subscales
were associated with poorer performance in psychomotor function (r=.5, p=.04 &
r=42, p=.09). Poorer mental flexibility and working memory correlated with time
management difficulty at 3 months (r=-.4, p=.09 & r=.54, p=.02). Patients performing poorly on story recall tests were more likely to report difficulty with job physical
performance (r= -.42, p=.09) and completing work effectively (r=.61, p=.009). Poorer
working memory performance was associated with lower scores on mental/ interpersonal WLQ subscales (r=.45, p=.05) and overall health related work productivity loss
(r=.47, p=.04). WLQ areas also correlated with participants’ perception of their NP
function at 3 & 12 months after aSAH. Conclusions: These results suggest that NP
deficits have an impact on work quality after hemorrhage and provide strong impetus for future studies so that domain specific interventions can be implemented to
improve outcomes that affect quality of life including work productivity.
31
TRAUMATIC BRAIN INJURY LEADS TO ALTERED BRAIN
DRUG TRANSPORTER EXPRESSION
Frederick Willyerd1, Ryan Hart2; 1N/A, Phoenix, AZ, 2Phoenix Children’s Hospital, Phoenix, AZ
Learning Objectives: ATP-binding cassette (ABC) transporters function to selectively regulate the brain biochemical milieu through active transport of substrates.
Little is known about how traumatic brain injury (TBI) alters the expression of
these transporters. Changes in the expression of ABC transporters after TBI could
influence therapeutic drug penetrance and outcome. The purpose of this study
is to determine if ABC transporter expression changes after TBI. We hypothesize that quantifiable changes occur in ABC transporter expression after TBI.
Methods:Adult Sprague-Dawley rats (n=3/group) underwent moderate midline
fluid percussion injury (mFPI) then were killed at eight time points post-injury.
Tissue from parietal cortex, hippocampus, and thalamus was collected, processed,
and analyzed via western blot. Sham injured animals (n=4) were used for comparison. Results: Bcrp showed at least a 2-fold decrease (P< 0.05) at days 1, 5, 7, 14,
and 56 post-injury in parietal cortex. Bcrp hippocampal and thalamic expression
decreased up to 4-fold (P< 0.05) at all points except day 3 post-injury. Mrp1
increased at least 2-fold (P< 0.05) at days 1, 2, 7, and 14 post-injury in parietal
cortex and thalamus and days 7 and 14 post-injury in the hippocampus. P-gp
increased 2-fold (P< 0.05) at days 1, 2, 3, and 5 post-injury in parietal cortex with
the same level of increase (P< 0.05) on days 1 and 2 post-injury in hippocampus.
P-gp in thalamic tissue increased 2-fold (P< 0.05) on day 1 post-injury. Conclusions: We found Bcrp decreased significantly at both early and late time point’s
post-TBI. This could cause decreased export of substrates like glutathione and
estradiol. We found an increase in Mrp1 and P-gp expression acutely. Increased
ABC transporters could cause elevated export of substrates like opioids, anti-seizure medication, and prostaglandins. With this data we must suppose therapeutic
drugs used in TBI may not reach beneficial levels if administered during a period
of transporter overexpression. This could affect our clinical treatments requiring
personalized tailoring of therapies to treat patients who suffer TBI.
32
GIVING YOUR PATIENTS M.O.R.E: IMPLEMENTING OF A
NON-PHARMACOLOGIC PROTOCOL TO PREVENT ICU
DELIRIUM
Ryan Rivosecchi1, Sandra Kane-Gill2, Shauna Campbell3, Sue Svec3, Pamela
Smithburger4; 1UPMC-Presbyterian Hospital, N/A, 2University of Pittsburgh,
Pittsburgh, PA, 3University of Pittsburgh Medical Center - Presbyterian Hospital, Pittsburgh, PA, 4University of Pittsburgh School of Pharmacy, Pittsburgh, PA
Learning Objectives: Previous studies, incorporating early mobilization, have
demonstrated the positive impact of non-pharmacologic prevention protocols
on delirium which makes the influence of “other” non-pharmacologic interventions difficult to isolate. The purpose of this evaluation was to determine if an
evidence- based, non-pharmacologic protocol reduced on the percentage of time
spent delirious in a medical-intensive care unit (MICU) that already uses a sedation and mobility protocol. Methods: This was a prospective, pre-post quality
improvement project of MICU patients conducted from September 2013 to
April 2014 in a large, academic medical center. Data elements collected in both
the pre and post protocol groups were demographics, Intensive Care Delirium
Screening Checklist scores every 4 hours and predisposing risk factors for ICU
delirium. Effective, single non-pharmacologic interventions were selected after
a literature review and bundled for incorporation into our protocol. The protocol consisted of Music, Opening /closing of blinds, Reorientation /cognitive
stimulation, and Eye/ear care (M.O.R.E). Nursing education about the protocol was completed. Results: 729 patients were evaluated with 230 and 253
included in the pre and post phases, respectively. There was a 40.4% reduction
(16.1% v. 9.6%, p < 0.001) in the percentage of time in the ICU that was spent
delirious. Mechanical ventilation (MV), APACHEII, and dementia were statistically significant independent predictors of delirium development. The protocol
reduced the odds of developing delirium by 57% (OR 0.43, 95% CI 0.24–0.77)
after controlling for age, APACHE II, MV, and dementia. Conclusions: After
bundling effective, single non-pharmacologic interventions into a protocol, we
observed an additional benefit in reducing the time patients’ spend delirious after
sedation and mobility protocols were already in use. Institutions should consider
implementing evidence-based non-pharmacologic delirium prevention interventions, in addition to appropriate sedation and mobility protocols as part of their
standard of care.
Oral Abstract Session: Pediatrics
33
ACCURATELY IDENTIFYING DEGREE OF LUNG INJURY IN
PEDIATRIC ACUTE RESPIRATORY DISTRESS SYNDROME
Nadir Yehya1, Neal Thomas2; 1Children’s Hospital of Philadelphia, Philadelphia,
PA, 2Penn State Children’s Hospital, Hershey, PA
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Learning Objectives: While all definitions of acute respiratory distress syndrome
(ARDS) rely on some measure of hypoxemia as a marker for severity of lung
injury, neither the 2012 Berlin definition of ARDS, nor the proposed definitions by the Pediatric Acute Lung Injury Consensus Conference (PALICC) utilizing oxygenation index (OI) categories, specifies timing of PaO2/FiO2 (PF) or
OI measurements. Methods: In this prospective, observational study on children with ARDS over 3 years (7/2011 to 6/2014) in the Children’s Hospital of
Philadelphia intensive care unit, data were collected to study risk factors associated with mortality and ventilator-free days (VFD) at 28 days. We hypothesized
PF or OI would be more useful for risk stratification and prognostication when
collected 24 hours after meeting ARDS criteria, rather than initial values. Results:
There were 283 children with ARDS (Berlin definition) with 37 deaths (13%).
Neither initial PF (area under receiver operating characteristic curve [AUROC]
0.58 [95% CI 0.48–0.68], p>0.1) nor OI (AUROC 0.58 [0.47–0.69], p>0.1)
at time of meeting ARDS criteria predicted mortality. However, 24 hours after
ARDS onset, both PF and OI discriminated mortality (AUROC 0.68 [0.59–
0.77] and 0.66 [0.57–0.75], p<0.001). PF 24 hours after meeting ARDS criteria
also categorized severity of lung injury, with increasing mortality rates of 5%
(PF > 300), 8% (PF 201–300), 18% (PF 101–200), and 37% (PF ≤ 100) across
worsening Berlin ARDS categories. This trend with 24-hour PF was seen for
VFD (22, 19, 14, and 0 VFD with worsening Berlin categories, Kruskal-Wallis
p<0.001) and length of mechanical ventilation in survivors (6, 9, 13, and 24 days
with worsening Berlin categories, p<0.001). Similar results were obtained when
24-hour OI (PALICC categories) was used instead of 24-hour PF. Conclusions:
PF and OI 24 hours after meeting ARDS criteria discriminate mortality in pediatric ARDS, and can stratify degree of lung injury. Initial PF and OI were not
helpful for prognostication. Definitions of ARDS may benefit from addressing
timing of oxygenation metrics to stratify disease severity.
34
ALVEOLAR DEAD SPACE FRACTION DISCRIMINATES SURVIVAL IN PEDIATRIC ACUTE RESPIRATORY DISTRESS
SYNDROME
Nadir Yehya1, Anoopindar Ghuman2, Robinder Khemani2; 1Children’s Hospital of
Philadelphia, Philadelphia, PA, 2Childrens Hospital Los Angeles, Los Angeles, CA
Learning Objectives: Physiologic dead space fraction is associated with mortality in acute respiratory distress syndrome (ARDS), but its measurement
is cumbersome. Alveolar dead space fraction (AVDSf ) relies on the difference
between partial pressures of arterial and (more readily-obtained) end-tidal carbon dioxide (AVDSf = (PaCO2 – ETCO2)/ PaCO2). In children with acute
respiratory failure, a single study demonstrated AVDSf was associated with
mortality. Methods:Using a prospectively constructed database of children with
ARDS (Berlin definition) over a 3 year period (7/2011 to 6/2014) in the Children’s Hospital of Philadelphia intensive care unit, we retrospectively abstracted
AVDSf and tested association with mortality. Results: Of the 283 children with
ARDS (37 deaths, 13%), 266 had available ETCO2. AVDSf was lower in survivors (median 0.13 [IQR 0.06, 0.23]) than non-survivors (0.31 [0.19, 0.42],
p<0.001) at ARDS onset, but not 24 hours after establishing ARDS (survivors
0.12 [0.06, 0.18], non-survivors 0.14 [0.06, 0.25], p=0.430). AVDSf at ARDS
onset discriminated mortality with an area under receiver operating characteristic curve of 0.76 (95% CI 0.64–0.87, p<0.001). When analyzing quartiles of
AVDSf, mortality was 6–7% in the 3 lowest quartiles (AVDSf < 0.25) but was
35% in the highest quartile (AVDSf > 0.25). AVDSf at ARDS onset correlated
with extrapulmonary organ failure (Spearman’s rho = 0.19, p=0.001), vasopressor
score (rho = 0.19, p=0.001), and worst oxygenation index (OI) in the initial 24
hours of ARDS (rho = 0.34, p<0.001). In multivariate analysis after adjusting for
the above variables, AVDSf at ARDS onset was independently associated with
mortality. Conclusions: AVDSf at ARDS onset was independently associated
with mortality in pediatric ARDS. AVDSf may reflect both parenchymal disease
and lung perfusion, as it correlated with both markers of alveolar injury (worst
OI) and cardiac output (extrapulmonary organ failure and vasopressor score).
AVDSf lost prognostic ability as ARDS progressed, possibly related to improved
pulmonary perfusion after resuscitation.
35
methylprednisolone (n=17) vs. placebo (n=18) infusions. We analyzed 56 serum
samples using a multiplex assay for 38 different cytokines, chemokines, or growth
factors (IL-1α, IL-1β, IL-1RA, IL-2, IL-3, IL-4, IL-5, IL-6, IL-7, IL-8, IL-9,
IL-10, IL-12p40, IL-12p70, IL-13, IL-15, IL-17A, EGF, FGF-2, VEGF, eotaxin,
TGF-α, G-CSF, GM-CSF, Flt-3L, fractalkine, IFN-α, IFN-γ, GRO, MCP-3,
MDC, sCD40L, IP-10, MCP-1, MIP-1α, MIP-1β, TNF-α, TNF-β). Results:
At Day 0, we found no differences between the placebo and steroid groups in
any inflammatory mediators except for IL-15, which was increased in the placebo group. Concentrations of IL-6 (p=0.0025), MCP-1(p=0.0037), IFN-α
(p=0.026), G-CSF (p=0.004) and GM-CSF (p=0.026) decreased significantly
from Day 0 to 7 in the methylprednisolone group, but not in the placebo group.
Methylprednisolone also prevented decreases in IL-1α (p=0.037) and IFN-γ
(p=0.041), which occurred in the placebo group by Day 7. IL-17A increased significantly from Day 0 to 7 (p=0.045) in the methylprednisolone group, but not
in the placebo group. IL-10 decreased significantly in both groups from Day 0
to 7 (p<0.035). No significant changes occurred in TNF-α in both groups. Conclusions: Low-dose methylprednisolone therapy in early pediatric ARDS significantly alters inflammatory mediator profiles. Relating these changes to clinical
outcomes in a larger trial will determine the physiological basis for glucocorticoid
therapy in pediatric ARDS. (Clinical Trials.gov number, NCT01274260)
36
IMPACT OF KETAMINE COADMINISTRATION DURING
DEXMEDETOMIDINE SEDATION FOR PEDIATRIC MRI.
John Berkenbosch1, Jodie Hignite2, Frances Gilliland2, Debbie Farrell2, Ramakanth Yakkanti2, Janice Sullivan2; 1Univ. of Louisville/Kosair Children’s Hospital,
Louisville, KY, 2University of Louisville, Louisville, KY
Learning Objectives: Dexmedetomidine (DEX) continues to gain popularity
for pediatric MRI sedation. Its disadvantages include slower onset, longer recovery, and relatively frequent hypotension and bradycardia. The sympathomimetic
effects of ketamine seem to ameliorate CV effects but reports only describe this
during painful procedures. We reviewed our experience with ketamine addition
to DEX during MRI sedation, hypothesizing that it would maintain efficiency
and efficacy while decreasing adverse CV events during non-painful procedures.
Methods:Patients (pts) sedated primarily with DEX for MRI between 1/1/092/28/14 were retrospectively identified. Demographic and sedation-related information including adjunct ketamine and/or midazolam use, were recorded. The
impact of co-administrations on induction time and adverse event rates were
calculated and compared between ketamine (K) and no ketamine (NK) groups.
Results: 1345 pts aged 49 ± 47 mo were identified. 174 pts (12.9%) received ketamine. Groups were similar regarding age and ASA status. Fewer pts having brain
MRI received ketamine (10.3% of CNS vs 24.1% of non CNS scans, p<0.0001).
Induction times were similar between groups (13.7 ± 7.5 vs 12.7 ± 5.8 min,
p=0.12). Pts receiving ketamine had less hypotension (20.5 vs 13.8%, p=0.04)
and bradycardia (21.1 vs 12.6%, p=0.008). Hypotension duration was similar
between groups (18 ± 16 vs 17 ± 11 min, p=0.72). Bradycardia duration trended
towards shorter in the K group (22 ± 20 vs 14 ± 15 min, p=0.06), but did not
reach significance. 3 pts had significant airway events including obstruction
(1=K, 1=NK) and apnea requiring intubation (1=K). There were 5 sedation failures (0.37%; 2=K, 3=NK, p=0.12) and no emergence reactions. Conclusions:
Adjunct use of ketamine during DEX sedation did not adversely impact sedation
efficiency or efficacy, was associated with fewer adverse CV effects, and does not
appear to induce recovery-related delirium. While more formal prospective evaluation is still required, consideration may be given to adding ketamine to DEX for
MRI or other non-invasive procedural sedation to minimize CV events.
37
PERFORMANCE OF INTERLEUKIN 27 AS A SEPSIS DIAGNOSTIC BIOMARKER IN CRITICALLY ILL CHILDREN
DIFFERENTIAL REGULATION OF INFLAMMATORY BIOMARKERS BY METHYLPREDNISOLONE IN EARLY PEDIATRIC ARDS
William Hanna1, Hector Wong2; 1Cincinnati Children’s Hospital Med Center,
Cincinnati, OH, 2Cincinnati Children’s Hospital Medical Center, Cincinnati, OH
Learning Objectives: Low-dose methylprednisolone reduces systemic inflammation, shortens duration of mechanical ventilation and ICU length of stay in adult
Acute Respiratory Distress Syndrome (ARDS). A pilot randomized trial in early
pediatric ARDS showed that low-dose glucocorticoid therapy does not alter duration of ventilation or mortality, but may improve oxygenation and ventilation.
We sought to determine if methylprednisolone therapy alters the inflammatory
mediator profiles in children with early ARDS. Methods: Serum samples were
collected before study drug (Day 0), on Days 7 and 14 in patients receiving
Learning Objectives: Use of biomarkers to distinguish bacterial infections from
non-infectious conditions remains a diagnostic challenge in the critically ill.
Despite increasing clinical use, biomarkers such as procalcitonin (PCT) continue
to exhibit inconsistent results. Interleukin 27 (IL27) has shown early promise in
critically ill children, with high specificity and positive predictive values in a preliminary study. This ongoing prospective study tested the performance of IL27 as
a bacterial diagnostic biomarker in critically ill children. Methods: Patients with a
clinical suspicion of infection were eligible, defined by a decision to acquire blood
cultures by the primary team. Blood collected within 6 hours of cultures was then
tested for IL27 and PCT. Bacteremic cases (N=43), defined as patients with positive blood cultures, were then compared to those with no microbiologic or clinical
evidence of infection (N=299), judged by an intensivist chart review blinded to
biomarker results. Performance comparisons included calculations of ROC curves
Dai Kimura1,2, Cynthia Rovnaghi3, Bin Teng2, Bonny Drago4, Gianfranco
Meduri2, Kanwaljeet Anand1,2, Andreas Schwingshackl1,2; 1Le Bonheur Children’s
Hospital, Memphis, TN, 2University of Tennessee Health Science Center, Memphis, TN, 3University of Tennessee Health Sciences Center, Memphis, TN, 4State
University of New York at Stony Brook, Stony Brook, NY
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
for both IL27 and PCT in addition to a combination strategy using a CART analysis generated decision tree. Further analysis was performed on a subset of patients
(N=133) classified as immune compromised. Results: Ages ranged from 2 months
to 34 years, with median 9.0 and IQR 3–13. ROC curves for IL27 and PCT
yielded AUCs of 0.76 (0.67,0.84) and 0.72 (0.64,0.81). Using the prior cut-point
of ≥ 5.0 ng/ml for IL-27 yielded a specificity of 95% (92, 97). In the immune
compromised, IL27 and PCT AUCs were 0.82 (0.72–0.93) and 0.73 (0.60–0.86).
A CART derived decision tree incorporating IL27 and PCT yielded an AUC of
0.89 (0.83–0.95), significantly greater than the AUC for PCT alone (p=0.02), and
with a sensitivity of 100% (77,100) and specificity of 63% (53,75). Conclusions:
Consistent with the prior study results, IL27 may serve as an effective “rule in” test
for bacteremia in critically ill children. Among immune compromised patients, its
sensitivity appears promising, with a combination IL27 and PCT strategy yielding
an improved performance compared to PCT alone.
38
PHYSIOLOGICAL VARIABLES OF BURN INJURY IN INFANTS:
AN OVERVIEW
Arham Ali1, Celeste Finnerty2, Ronald Mlcak3, Felicia Williams4, David Herndon5, Jong Lee5; 1University of Texas Medical Branch Hospitals, Galveston, TX,
2
Shriners Hospital for Children, Galveston, TX, 3Shrines Hospital for Children,
Galveston, TX, 4Shriners Hospitals For Children, Galveston, TX, 5University of
Texas Medical Branch, Galveston, TX
Learning Objectives: According to the 2014 National Burn Repository (NBR),
infants with severe burn injury exhibited over twice the mortality than children in
childhood and adolescence age groups combined (25% vs. 12%). The aim of this
study is to outline physiological perturbations in infants with burn injury admitted
or referred to a single specialized burn care center. Methods: A total of 73 children under the age of 1 year with burns covering ≥30% of the total body surface
area (TBSA) admitted to Shriners Hospitals for Children- Galveston were included
in this study. Burn injury demographic data was collected in addition to clinical
outcomes pertaining to metabolic, cardiopulmonary, renal, hepatic, and gastrointestinal systems. Where applicable, outcomes were compared to those reported in
the 2014 NBR. Statistical analysis was performed using Fisher’s exact test, KruskalWallis one way ANOVA on ranks, and mixed linear models to test for differences
among time points where appropriate. Results: Age at the time of burn injury
was 8 ± 3 months (mean±SD). Partial thickness and full thickness burns covered
49 ± 15 and 29 ± 24 percent of the TBSA respectively. Infants remained hypermetabolic throughout hospital admission as assessed by indirect calorimetry (p<0.05).
Stroke volume and heart rate were elevated for up to 6 months and 1 year post
burn, respectively. Liver size remained constant at 1, 6, and 12 months post burn
(8.5 ± 1.8, 8.1 ± 2.2, and 8.1 ± 0.9 cm respectively; p>0.05). Cytokines IL-6, IL-8,
GM-CSF, and MCP-1 remained persistently elevated for up to 1 year post burn
(p<0.05). Conversely, α2-macroglobulin, apolipoprotein A1, and serum transferrin
levels were decreased for the first month following burn injury (p<0.05). Pneumonia afflicted 14% of children. Mortality in this cohort was significantly lower than
that reported by the 2014 NBR for children of the same age group (4/73 [5%] vs.
93/374 [25%]; p<0.0001). Conclusions: Burn injury in children less than 1 year
of age results in altered physiology and homeostasis. Meticulous care and referral to
a specialized burn care center is warranted to confine mortality.
39
RED BLOOD CELL DISTRIBUTION WIDTH IS ASSOCIATED WITH INCREASED MORTALITY IN CRITICALLY ILL
CHILDREN
Ahmed Said1, Mary Hartman2, Allan Doctor1, Philip Spinella3; 1Washington
University School of Medicine, Saint Louis, MO, 2N/A, St. Louis, MO, 3Washington University In Saint Louis, Saint Louis, MO
Learning Objectives: Red blood cell (RBC) distribution width (RDW) is
associated with poor outcome in adults and is suggested to mark abnormal
RBC energetics or systemic iron metabolism. Our objective was to determine
if increased RDW is associated with ICU mortality in children. Methods: We
screened, pediatric ICU admissions from Jan 2005 to Dec 2012. We included
patients with a CBC drawn on admission and excluded patients with diagnoses
of maligncy, bone marrow or solid organ transplant, hemoglobinopathy, epilepsy
and history of RBC transfusion within 14 days prior to or 7 days after PICU
admission. RDW was collected on admission (A-RDW) and for the following
7 days if available. Relative Change in RDW (RC-RDW) was defined as (Highest RDW – A-RDW)/A-RDW. We performed multivariate logistic regression to
determine if A-RDW and RC-RDW were independently associated with ICU
mortality including covariates with a p<0.2 on univariate analysis (Pediatric Index
of Mortality II score, initial white blood cell count, hematocrit, mean corpuscular volume, peak and lowest heart rates in the first 12 hours of admission, and
need for ECMO during their ICU stay). Results: Of 17,351 patients screened,
3,913 patients were analyzed. Mean age was 7.5 ± 6.7 years., ICU mortality was
2.9%, mean hemoglobin at admission was 11.9 g/dl±2.9 with a mean A-RDW of
14.1 ± 1.9. Mean 7 day RC-RDW was 1.02% ± 6.7 of admission RDW. On univariate analysis, A-RDW and RC-RDW were associated with increased mortality,
Odds Ratio (OR) = 1.2 (95% CI 1.1–1.2, p<0.001), and 1 (95% CI 1–1.01,
p 0.0016), respectively. On multivariate analysis, both A-RDW and RC-RDW
were significantly associated with increased mortality, OR = 1.1 (95% CI 1.0–
1.3, p<0.001), and 1.03 (95% CI 1.0–1.05, p<0.001), respectively. The strength
of our model was determined by a receiver operator curve analysis, with an area
under the curve of 0.93. Conclusions: Increased A-RDW and RC-RDW is
independently associated with ICU mortality in critically ill children. Additional
study is needed to determine the mechanisms involved, such as impaired systemic
iron metabolism or RBC energetics.
40
RICHMOND AGITATION SEDATION SCALE INTER-RATER
RELIABILITY IN CRITICALLY ILL PEDIATRIC PATIENTS
Meg Kihlstrom1, Ashley Purdy2, Jenny Boyd2; 1University of North Carolina at
Chapel Hill, Pittsboro, NC, 2University of North Carolina at Chapel Hill, Chapel Hill, NC
Learning Objectives: The Richmond Agitation Sedation Scale (RASS) is a valid
and reliable scale for the assessment of sedation status in adult intensive care
unit (ICU) patients and is deemed as one of the most reliable sedation tools
by the 2013 adult clinical practice guidelines for sedation in ICU patients. A
similar valid and reliable sedation tool has not been established for mechanically
ventilated critically ill pediatric patients. Our goal was to demonstrate the interrater reliability of the RASS in sedated, intubated PICU patients before and
after an educational intervention. Methods: This prospective, interventional
study was completed in a 20-bed PICU from July 2013 to July 2014. Children
≤18 years of age requiring mechanical ventilation and receiving sedative medications were eligible. Simultaneous blinded, paired provider RASS assessments
between nurses and physicians were completed in three phases: baseline before
an educational intervention, post-intervention, and over subsequent months
to document sustained reliability. Inter-rater agreement was evaluated using
weighted κ statistics. Results: A total of 347 assessments were completed on
47 PICU patients: 49 paired provider RASS assessments at baseline, 228 postintervention, and 70 maintenance. The pre-intervention weighted κ increase
from 0.56 (95% CI 0.39–0.72) to 0.86 (95% CI 0.77–0.95) post-intervention
was significant (p<0.001). The improvement was maintained in subsequent
months with weighted κ 0.78 (95% CI 0.61–0.94). Conclusions: In this first
study investigating RASS inter-rater reliability in a pediatric population, the
high weighted κ proves the RASS to be an excellent tool for assessment of sedation status in mechanically ventilated, sedated PICU patients. With a simple
educational intervention, the inter-rater reliability improved significantly, and
this was maintained over subsequent months. The use of a reliable and objective
tool, such as the RASS, is the first step to provide consistent sedation care, which
may limit exposure to neurotropic medications, avoid over/under sedation and
mitigate delirium.
Oral Abstract Session: Pulmonary and Monitoring
41
FORECASTING CARDIO-RESPIRATORY INSTABILITY IN
MONITORED PATIENTS: A MACHINE LEARNING APPROACH
Lujie Chen1, Artur Dubrawski1, Marilyn Hravnak2, Gilles Clermont2, Michael
Pinsky2; 1Carnegie Mellon University Auton Lab, Pittsburgh, PA, 2University of
Pittsburgh, Pittsburgh, PA
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Learning Objectives: Patients with continuously monitored vital sign (VS) often
show subtle changes prior to cardio-respiratory instability (CRI). We hypothesize
that these changes follow patterns that can be learned by machine learning (ML)
models from reference data, and that the resulting models can predict future CRI.
Methods: A training set of 229 step-down unit patient stays provided continuous
VS monitoring data which was evaluated for CRI events (VS excursion beyond
stability thresholds) and adjudication of events as real alerts or artifact. Of these
stays 135 contained at least one real (non-artifact) alert while 94 never had such
events. The positive data set was constructed from 640 real alerts (BP 9%, HR
23%, RR 30%, SpO2 37%). For each, statistical features (mean, variance, slope,
min and max) were extracted from VS data for 5, 10, and 15 min time windows
that ended at various leading times before CRI threshold was crossed. The negative
data reflected the first 6 hrs of each stay without any CRI using analogical features.
We built 30 ML models for lead times from 1 to 30 min prior to onset of CRI using
Random Forest as the specific ML method, and computed the leave-one-patientout cross-validation scores. Results:AUC (area under Receiver Operating Characteristic) scores for predicting all alerts were 80%, 80%, 87% and 90% at lead times
of 30, 15, 5 and 1 min respectively. Models built for predicting only the first alert
in a possible sequence yielded AUC of 71%, 78%, 82% and 90% for those lead
times. At 15 min lead time, the model was able to recall 62% of real HR alerts, 59%
RR alerts, and 39% SpO2 alerts, and 67% HR, 66% RR and 64% SpO2 at 5 min.
Shortage of BP alerts training data limited the utility of BP models. Conclusions:
ML has a potential to identify informative VS abnormalities in advance of overt
CRI. Lead time of prediction varies by VS type. SpO2 alerts become more predictable when getting closer to onset. Predictability of HR and RR is relatively constant
over the lead times investigated. These findings have promise for future utilization.
FUNDING: NIH R01NR013912; NSF 0911032, 1320347
Hypothesis: Minute CO2 Elimination (VCO2) obtained by volumetric capnography will correlate with Cardiac Output (CO) and Effective Pulmonary Blood Flow
(QEP) in patients with single ventricle physiology or 2 ventricles with intracardiac
shunting. Methods: This prospective cohort study included children younger
than 18 years with congenital heart disease who underwent cardiac catheterization as part of clinical care. Hemodynamic data, including CO (QS), Pulmonary
Blood Flow (QP), and calculated QEP were collected. VCO2, Minute Ventilation
and End-Tidal CO2 were simultaneously obtained via a volumetric capnography
monitor. Spearman’s rank correlation coefficients were used to assess correlation
between measurements after controlling for minute ventilation. Results: Seventeen patients were included; eight single ventricle patients, and nine patients with
2-ventricle physiology with intracardiac shunting. Median age was 4 (interquartile
range: 3.0 - 9.5) months. The median VCO2, CO and QEP were 27.4 (18.7–
38.6) ml/min, 1.05 (0.95–1.48) L/min and 0.885 (0.54–1.46) L/min respectively.
The correlation coefficient between VCO2 and QEP was 0.95 (p <0.001) and
that for VCO2 and CO was 0.94 (p <0.001). Conclusions: VCO2 may be a surrogate marker for cardiac output and effective pulmonary blood flow in patients
with single ventricle physiology or 2-ventricles with intracardiac shunting. It may
serve as a non-invasive tool in the assessment of hemodynamic status in the ICU.
Further studies are needed to establish its utility in critically ill cardiac patients.
42
44
RANDOM FOREST MODELS SEPARATE VITAL SIGN EVENTS
AS REAL OR ARTIFACT IN CONTINUOUS MONITORING
DATA
NUTRITION STATUS AND OUTCOMES IN NONCARDIOGENIC ACUTE RESPIRATORY FAILURE: A COHORT STUDY
Marilyn Hravnak1, Lujie Chen2, Artur Dubrawski2, Donghan Wang2, Eliezer
Bose1, Gilles Clermont3, Michael Pinsky3; 1University of Pittsburgh School of
Nursing, Pittsburgh, PA, 2Carnegie Mellon University Robotics Institute, Pittsburgh, PA, 3University of Pittsburgh School of Medicine, Pittsburgh, PA
Learning Objectives: False alarms from monitoring artifact causes alarm fatigue.
We used Random Forest (RF) machine learning algorithms, trained on expertlabeled data, to automatically classify events as real alerts or artifact in continuous
vital sign (VS) data from bedside monitors. Our purpose was to determine if RF
differentiated real alerts from artifact in previously unseen monitoring data to a
clinically helpful degree. Methods: Noninvasive monitoring data from 8 weeks
of admissions in a 24-bed step-down unit (heart rate [HR], respiratory rate [RR;
bioimpedance], oscillometric blood pressure [BP], peripheral oximetry [SpO2])
were recorded at 1/20Hz. VS deviation beyond stability thresholds (HR 40–140,
RR 8–36, systolic BP 80–200, diastolic BP<110, SpO2>85%) and persisting for
80% of a 5 min moving window comprised events. Of 1,582 events, 631 were
labeled by consensus of four expert clinicians as real alerts, artifact, or unable to
classify (UTC), and the remaining 795 held as unseen. Using the 631 labeled
events, RF was trained to tell apart real alerts from artifact, then cross-validated
to mitigate overfitting. Next the resulting model was applied to the 795 unseen
events, which were then reviewed by the experts for external validation of RF
predictions. Results: 418 alerts were labeled by experts as real alerts (SpO2 44%,
RR 32%, BP 11%, HR 14%), 158 as artifact (SpO2 59%, RR16%, BP25%,
HR0%), and 55 UTC. For the 795 unseen events, of 510 RR events, experts
agreed with 100% of the RF artifact predictions, and 99% of real alert predictions
(UTC=1%). Of 55 BP events, the agreement was 80% and 76% (UTC=0%). Of
230 SpO2 events, there was 55% artifact agreement (UTC=10%) and 92% real
alert agreement (UTC=3%). Conclusions: A RF model trained on a small set of
expert-labeled data was able to discriminate real alerts from artifact in monitored
RR and BP data to a clinically helpful degree. SpO2 artifact was the most difficult
to discriminate. Such algorithms, when further refined, may improve event adjudication in VS monitoring devices and reduce alarm fatigue. FUNDING:NIH
NINR R01NR013912; NSF 0911032, 1320347
Kenneth Christopher1, James Rawn2, Kris Mogensen3; 1Renal Division, Brigham
and Women’s Hospital, Boston, MA, 2Department of Surgery, Brigham and
Women’s Hospital, Boston, MA, 3Department of Nutrition, Brigham and Women’s Hospital, Boston, MA
Learning Objectives: Malnutrition is present in a substantial minority of the critically ill. Whether malnutrition at critical care initiation has prognostic implications for patients with acute respiratory failure has not been studied. Methods: We
studied 1,788 patients, age ≥ 18 years, who received critical care between 2004 and
2011 who were formally evaluated by a Registered Dietitian. All patients had noncardiogenic acute respiratory failure identified by ICD9 codes for respiratory failure or pulmonary edema and mechanical ventilation, excluding congestive heart
failure. The exposure of interest, nutritional status was defined as no malnutrition,
nonspecific malnutrition or protein-energy malnutrition (mild, moderate or severe
protein-energy malnutrition, or marasmus). The primary end point was 30-day allcause mortality following ICU admission. Adjusted odds ratios were estimated by
multivariable logistic regression models with inclusion of covariate terms thought
to plausibly associate with both nutrition status and mortality. Mortality was also
analyzed with a risk-adjusted Cox proportional hazards regression model. Results:
The cohort had 58% men, 76% whites, 50% medical patients, 24% with sepsis
and a mean age of 60 yrs. Nonspecific malnutrition was recorded in 57%, proteinenergy malnutrition in 11% and 32% had no malnutrition. The 30-day mortality
rate was 19%. Validation of ICD9 acute respiratory failure assignment against
the Berlin Definition showed a Positive Predictive Value of 84.4% and a Negative
Predictive Value of 57.4%. The adjusted hazard ratio of mortality in patients with
nonspecific or protein-energy malnutrition were 1.31 (95%CI, 1.12–1.54), and
2.40 (95%CI, 1.94–2.97) relative to no malnutrition. The adjusted OR for 30
day mortality with nonspecific or protein-energy malnutrition were 1.21 (95%CI,
0.94–1.56), and 2.57 (95%CI, 1.79–3.71) relative to no malnutrition. Conclusions: Patients with malnutrition who suffer acute respiratory failure are a highrisk group for adverse outcomes. Further study is needed to determine if nutrition
status is a modifiable risk factor for mortality.
45
43
VOLUMETRIC CAPNOGRAPHY IN THE ASSESSMENT OF
HEMODYNAMIC STATUS IN INFANTS WITH CARDIAC
DISEASE
Awni Al-Subu1, Gregory Fleming2, Christoph Honrik3, Edmund Jooste2, Ira
Cheifetz1, Jennifer Turi4, Kevin Hill1, George Ofori-Amanfo5; 1Duke University
Medical Center, Durham, NC, 2Duke Children’s Hospital, Durham, NC, 3Duke
Children’s Hospital, Durham, NC, 4N/A, Durham, NC, 5Duke University Children’s Hospital, Durham, NC
Learning Objectives: Assessment of Pulmonary Blood Flow (QP) and systemic
output (QS) is critical in the postoperative management of patients with single
ventricle physiology or two-ventricle physiology with intracardiac shunting. Currently, such hemodynamic data are only obtainable by invasive procedures such as
cardiac catheterization or the use pulmonary artery catheters. Ready availability
of such information in the critically ill cardiac patient, especially if obtainable
non-invasively, could be an important addition to postoperative monitoring.
ACUTE RESPIRATORY DISTRESS SYNDROME FOLLOWING
HEMATOPOIETIC STEM CELL TRANSPLANTATION
Hermang Yadav1, Matthew Nolan1, John Bohman2, Steve Peters1, Rodrigo Cartin-Ceba1, Ognjen Gajic3, Daryl Kor4; 1Mayo Clinic, Rochester, MN, 2Mayo
Clinic Department of Anesthesiology, Rochester, MN, 3Mayo Graduate School
of Medicine(Rochester), Rochester, MN, 4Mayo Clinic (CCM), Rochester, MN
Learning Objectives: Pulmonary complications are common following hematopoietic stem cell transplantation (HSCT). While a multitude of pulmonary
syndromes have been described following HSCT, diagnosis can be challenging since these syndromes are incompletely characterized, often with overlapping presentations. Patients at the severe end of this spectrum may present with
hypoxemic respiratory failure and acute lung edema, ultimately fulfilling criteria
for the Acute Respiratory Distress Syndrome (ARDS). However, limited data
exists regarding the incidence of ARDS following HSCT. We aimed to characterize the epidemiology of ARDS in patients undergoing HSCT. Methods:
We performed a retrospective cohort evaluation of patients undergoing HSCT at
Mayo Clinic Rochester between 1/1/2005 to 12/31/2012. Patients were screened
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
for ARDS development within one year of HSCT. ARDS adjudication was performed in accordance with the 2011 Berlin Criteria by three trained adjudicators (HY, MEN and JKB). Disagreements were addressed by a third consulting
expert (DJK). Results: 130 cases of ARDS developed in 2635 patients undergoing HSCT (4.9%). ARDS developed in 72/481 patients undergoing allogenic
HSCT (15.0%) and 58/2154 patients undergoing autologous HSCT (2.7%).
Median time to ARDS development was 50.0 days (IQR: 15.0 to 138 days)
after allogenic HSCT and 14.2 days (IQR: 10.5 to 124 days) after autologous
HSCT. The 28-day mortality following development of ARDS was 46.9%. At 12
months following HSCT, 87/130 ARDS patients had died (66.9%) compared to
297/2505 patients who did not develop ARDS (11.9%). 7/130 (5.4%) ARDS
cases met criteria for engraftment syndrome and 15/130 (11.5%) for diffuse alveolar hemorrhage. The majority of the ARDS cases (n = 108; 83.1%) did not meet
diagnostic criteria for a specific post-HSCT pulmonary complication. Conclusions: The incidence of ARDS in the year following HSCT is 4.9%. Incidence
of ARDS is higher, and ARDS develops later, in patients undergoing allogenic
HSCT compared to those undergoing autologous HSCT. Mortality following
development of ARDS is substantial, with a 28-day mortality of 46.9%.
46
CHYLOTHORAX IS ASSOCIATED WITH AN INCREASED
RISK OF THROMBOSIS IN ADULTS
Sumedh Hoskote1, Hemang Yadav1, Prashant Jagtap1, Craig Daniels2; 1Mayo
Clinic, Rochester, MN, 2Mayo Clinic College Of Medicine, Rochester, MN
Learning Objectives: Chylothorax is characterized by the presence of chyle in
the pleural space due to disruption of thoracic lymphatics. Loss of antithrombin
through chyle has been thought to contribute to a procoagulant state, and chylothorax has been shown to increase the risk of vascular thrombosis in children. We
hypothesized that a similar risk may exist in adults. Limited data exist about the
epidemiology of thrombosis in adults with chylothorax. Methods: We performed
a single-center retrospective cohort review of all adult patients developing chylothorax between 1/1/2000 and 6/30/2014. Chylothorax was defined as pleural fluid
triglycerides ≥110 mg/dL, or pleural fluid triglylcerides between 50 and 110 mg/dL
with chylomicrons seen on microscopy. Those patients who had pleural lipid analysis
but did not have chylothorax were defined as the control group. Thrombotic events
were identified by thrombosis-related ICD-9 diagnosis codes (codes containing 415,
434, 444, 452 and 453) occurring within 14 days (before/after) of pleural fluid
analysis. Results: 1527 patients underwent pleural fluid analysis that included lipid
testing. 811/1527 patients met diagnostic criteria for chylothorax. 451/811 were
male (56%), and median age was 62 years (IQR 51–71). In those with chylothorax,
114/811 (14.1%) had an associated thrombotic event. 716/1527 underwent pleural
fluid lipid testing but did not meet diagnostic criteria for chylothorax. 399/716 were
male (56%), median age was 62 years (IQR 51–72). In those without chylothorax,
64/716 (8.9%) had an associated thrombotic event. The relative risk of thrombosis
in those who had chylothorax compared to those who did not was 1.57 (95% CI
1.18–2.10, p=0.002). Conclusions: Chylothorax is associated with a 14.1% risk
of thrombotic events and this risk is significantly higher compared to the risk of
associated thrombosis in patients who had pleural lipid analysis but did not have
chylothorax. Further investigation is needed to define the epidemiology and risk
factors for developing thrombosis in the setting of chylothorax.
47
LIPOPOLYSACCHARIDE PRIMES THE INFLAMMASOME BY
INCREASING LEVELS OF IMMUNOREACTIVE NALP3
SeungHye Han1, Courtney Snavely2, Jake Jerome2, Rama Mallampalli2,3; 1University of Pittsburgh Medical Center, Pittsburgh, PA, 2University of Pittsburgh,
Pittsburgh, PA, 3Veterans Affairs Pittsburgh Healthcare System, Pittsburgh, PA
Learning Objectives: The inflammasome is an intracellular multi-protein complex
that, when activated, releases potent pro-inflammatory cytokines such as IL-1β and
IL-18, known to be associated with the high mortality of acute respiratory distress
syndrome. Specifically, the NALP3 (NACHT, LRR and PYD domains-containing
protein 3) inflammasome requires two-step signaling, priming and activation, to
be functional. The priming process increases the levels of NALP3 protein and proIL-1β in a dose- and time-dependent fashion in mice. However, the mechanisms
underlying NALP3 protein abundance in cells remain unknown. We investigated
how lipopolysaccharide (LPS) primes NALP3 levels in cells. We hypothesized that
LPS priming up-regulates steady-state levels of NALP3 protein by prolonging its
half-life. Methods: We treated human monocyte U937 cells (total 3x10ˆ6 cells) with
LPS (100–1,000ng/mL) for different durations (0–20 hours). The protein levels of
NALP3 were measured by immunoblotting, and mRNA levels were measured by
real time PCR after RNA isolation followed by reverse transcription. We measured
the half-life of NALP3 protein in U937 cells by inhibiting new protein synthesis
with cyclohexamide at 40ng/mL, both at baseline and after LPS exposure. Results:
We verified a dose- and time-dependent increase in NALP3 protein levels after LPS
exposure in human monocyte cells. The steady-state mRNA expression of NALP3,
however, was not changed after LPS exposure, suggesting post-translational regulation. The half-life of NALP3 is approximately 4 hours in an unchallenged condition,
and prolonged to >6 hours after LPS exposure. NALP3 degradation was reduced
with MG132, but not with a lysosomal inhibitor, leupeptin, indicating the degradation of NALP3 occurs via the ubiquitin proteasome system rather than the lysosome.
NALP3-ubiquitin binding, measured by co-immunoprecipitation, was decreased
after LPS exposure. Conclusions: LPS increases NALP3 protein levels by decreasing
its degradation, not by increasing new protein synthesis. LPS prolongs the lifespan of
NALP3 protein, most likely, via ubiquitin-mediated proteasomal processing.
48
OSTEOPONTIN INDUCES NEUTROPHIL MIGRATION
IN SEPSIS-INDUCED ACUTE LUNG INJURY VIA ERK
ACTIVATION
Yohei Hirano1, Monowar Aziz1, Weng-Lang Yang1, Zhimin Wang1, Mian Zhou1,
Mahendar Ochani1, Adam Khader1, Ping Wang1; 1The Feinstein Institute For
Medical Research, Manhasset, NY
Learning Objectives: Acute lung injury (ALI) is a common complication of
sepsis. Osteopontin (OPN) secreted from immune cells causes inflammation in
various diseases. However, its role in ALI remains unexplored. We hypothesize
that the treatment of OPN neutralizing antibody (anti-OPN Ab) could protect
mice against sepsis-induced ALI. Methods: Sepsis was induced in C57BL/6 mice
by cecal ligation and puncture (CLP). Anti-OPN Ab (50 µg/mouse) was injected
(i.v) at the time of CLP. After 20h, the expression of OPN and inflammatory
cytokines in tissues and blood were assessed by real-time PCR, Western blot
and ELISA. Neutrophil infiltration was determined by Gr-1 immunostaining.
The effect of recombinant mouse OPN (rmOPN) on human neutrophil cells,
HL-60 migration was performed by Boyden chamber assays. Results: After 20h
of sepsis, mRNA and protein levels of OPN were significantly induced in the
lungs, spleen and blood than shams. Compared to the vehicle group, treatment
of anti-OPN Ab in septic mice significantly reduced serum levels of injury markers (ALT: 69 ± 5.5 vs. 49 ± 4.2; AST: 138 ± 9.4 vs. 104 ± 6.4; LDH: 445 ± 62 vs.
256 ± 36 U/L, p<0.05). Inflammatory cytokines in lungs were greatly reduced at
the mRNA (IL-6: 30 ± 12 vs. 5 ± 2; MIP-2: 31 ± 11 vs. 13 ± 5 folds) and protein
levels (IL-6: 480 ± 346 vs. 177 ± 34; MIP-2: 1546 ± 743 vs. 929 ± 66 pg/g protein)
in anti-OPN Ab treated animals than vehicles. The lung histology, MPO (31 ± 4
vs. 19 ± 3 U/g tissue, p<0.05) and neutrophil infiltration (10 ± 1 vs. 3 ± 0.4 cells/
field, p<0.05) were significantly improved in anti-OPN Ab treated mice compared to the vehicle mice. Treatment with rmOPN in HL-60 cells significantly
increased their adhesion and migration. The neutrophils treated with rmOPN
increased the phosphorylation of focal adhesion kinase (FAK) and ERK. Pretreatment of the ERK inhibitor in HL-60 cells showed significant decrease in
OPN-mediated migration (275 ± 56 vs. 117 ± 4 cells/field, p<0.05). Conclusions: The treatment of anti-OPN Ab in mice attenuates neutrophil migration
in lungs, implicating it as a novel therapeutic potential in sepsis-induced ALI.
Oral Abstract Session: Quality, Safety, and Outcomes
49
ICU OUTCOMES OF PHYSICIAN ASSISTANTS AND ACUTE
CARE NURSE PRACTITIONERS COMPARED TO RESIDENT
TEAMS
Joseph Keller1, Harrison Reed1, Xiaofeng Wang1, Jorge Guzman1; 1Cleveland
Clinic, Cleveland, OH
Learning Objectives: Physician assistants and acute care nurse practitioners (PA/
ACNP) assume ever-expanding roles in high-acuity settings and, in many cases,
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
have replaced traditional resident physician models. Previous studies sought to
validate this growing trend but few have directly compared PA/ACNP and resident intensive care unit teams by the most crucial outcome: mortality. We compared ICU and hospital outcomes of PA/ACNP and resident teams in the same
medical intensive care unit of a quaternary academic medical center. We hypothesized no significant difference in mortality outcomes between the two models of care. Methods: This retrospective cohort study examined similar patient
populations admitted to either an 11-bed PA/ACNP team or a 10-bed resident
team during a 9 month period. The same pool of pulmonary/critical care attending physicians, fellows and proceduralists supported both teams. We performed
propensity score matching (PSM) analysis to match samples of the two groups
based on APACHE III, Acute Physiology Score (APS), and source of ICU admission. We compared categorical outcomes with the Pearson’s Chi-square test and
continuous outcomes with the nonparametric Kruskal-Wallis test. Results: The
two ICU teams admitted a total of 1138 patients and 1054 (527 per team) were
matched for analysis. APACHE III score, APS, and source of ICU admission
were statistically similar for both teams before and after PSM. After PSM, ICU
and hospital length of stay were comparable, however patients on the PA/ACNP
team had significantly lower ICU mortality (7.8% vs. 11.4%, p= 0.0468) and
hospital mortality (14.4% vs. 19.2%, p= 0.0394). Conclusions: A PA/ACNP
medical ICU team can reduce ICU and hospital mortality when compared to a
traditional resident physician model. These findings suggest the partnership of
PAs and ACNPs with pulmonary/critical care physicians and fellows can improve
outcomes in a Medical ICU and help alleviate the projected shortage of bedside
intensivists.
opinions. A cluster of RR artifacts on features RR mean [0,4] and RR sd [2,5]
likely suggests a loose ECG lead, while a pattern RR mean [33,40] and RR sd
[0,10] is likely due to insufficient bioimpedance. For SpO2 artifacts, features
SPO2 min and SPO2 slope expose patterns suggesting motion, sensor reattachment and loose lead or low perfusion. The patterns identified for RR artifacts
(HR-DD~=0, SPO2-DD bimodal with peaks at 0.1 and 0.01) suggest the lack
of ECG electrode integrity. For SPO2, decreases in both HR-DD and RR-DD
appear associated with artifact and suggest an overall problem with signal pickup
in both SPO2 and the ECG/RR sensors. Conclusions: Informative clustering
techniques support automated interpretation of artifacts identified in VS monitor data streams. Identified artifact archetypes agree with clinical intuition and
can potentially be used to guide corrective actions in practice. FUNDING: NIH
NINR R01NR013912; NSF 0911032, 1320347
50
ASSOCIATIONS BETWEEN SEDATIVES, VENTILATOR-ASSOCIATED EVENTS, LENGTH OF STAY, AND MORTALITY
52
A PICU SEDATION PROTOCOL FOR MECHANICALLY
VENTILATED PATIENTS NEEDS SUSTENANCE BEYOND
IMPLEMENTATION
Beryl Yaghmai1, Jane Di Gennaro1, Jerry Zimmerman1; 1Seattle Children’s Hospital, Seattle, WA
Learning Objectives: Providing appropriate sedation and analgesia for mechanically ventilated pediatric patients remains a significant challenge in the PICU.
While adequate sedation and analgesia is essential for patient safety and comfort,
excessive sedation can be detrimental. Following implementation of a PICU sedation protocol in 2008 we demonstrated a decrease in total days of sedation exposure, days on mechanical ventilation (MV), and PICU length of stay (LOS). Since
that time we have not re-evaluated these outcomes or the amount of sedation our
patients receive on the protocol. Methods: Using retrospective chart review we
identified patients admitted to the PICU from September 2012–August 2013
who required greater than 2 MV days, excluding any who had neurologic dysfunction/seizure, ECLS, tracheostomy, PCA, epidural, or neuromuscular blockade use, transfer from another ICU, or who had expired. Our comparison group
was all May 2008–April 2009 admissions meeting the same criteria. Data were
summarized using median and interquartile range for continuous variables and
proportions for categorical variables. We used the Wilcoxon rank-sum test to
compare continuous variables and the chi-square test to compare binary variables.
Results: 94 patients were identified in the current group (2012–2013), and 118
were included in the original group (2008–2009). Median PRISM scores, 6, were
identical in both groups. Median total days of sedation exposure was significantly
higher in the current group (9 vs. 5, p=0.0001) as was exposure to dexmedetomidine (64% vs. 23%, p<0.0001) and MV days (6 vs. 5, p=0.0058). Although
not statistically significant median opiate infusion days was also higher in the
current group (6 vs. 5, p=0.1643) as was PICU LOS (10 vs. 9 days, p=0.3259).
Conclusions: Our data suggests that we have not sustained our sedation quality
improvement (QI) realized in 2008–2009. Previous gains in use of opiate infusions, total days of sedation exposure, PICU LOS, and MV days have all deteriorated. Sustained QI requires routine monitoring of key variables, and ongoing
staff education to ensure continued effectiveness.
Michael Klompas1, Paul Szumita2, Lingling Li3, Michael Murphy3; 1Dept of Population Medicine, Boston, MA, 2Brigham and Women’s Hospital, Boston, MA,
3
Harvard Pilgrim Health Care Institute, Boston, MA
Learning Objectives: Sedatives vary in their pharmacology and adverse event
profiles. We evaluated the impact of different sedating agents on ventilatorassociated events (VAEs), duration of mechanical ventilation, hospital lengthof-stay, and mortality. Methods: We assessed daily benzodiazepine, propofol,
dexmedetomidine, opioid, paralytic, and antipsychotic exposures for all patients
ventilated for >2 days in Brigham and Women’s Hospital from June 2006 to
December 2013. We used Cox proportional hazard models to calculate VAE risk
for each sedative and proportional subdistribution hazard models with competing
risks to calculate hazards for ventilator and hospital length-of-stay and mortality.
All models were adjusted for daily sedative exposures, age, sex, ICU type, severity
of illness, and comorbidities. Results: We evaluated 9,603 consecutive episodes
of mechanical ventilation. Benzodiazepines and propofol were associated with
increased risk for VAEs (HR 1.2, 95% CI 1.0–1.4 for benzodiazepines and HR
1.3, 95% CI 1.1–1.5 for propofol). Dexmedetomidine, opioids, and antipsychotics did not affect VAE risk. Benzodiazepines, propofol, and opioids were associated with prolonged mechanical ventilation (HRs for extubation 0.67, 95% CI
0.62–0.72 for benzodiazepines, 0.83, 95% CI 0.78–0.89 for propofol, and 0.84,
95% CI 0.79–0.90 for opioids) and longer hospital lengths-of-stay (HRs for discharge 0.99, 95% CI 0.98–1.00 for benzodiazepines, 0.98, 95% CI 0.98–0.99
for propofol, and 0.98, 95% CI 0.97–0.99 for opioids). Conversely, dexmedetomidine and antipsychotics were associated with fewer ventilator days (HR for
extubation 1.7, 95% CI 1.5–2.0 for dexmedetomidine and 1.2, 95% CI 1.1–1.3
for antipsychotics) and lower mortality risk (HR 0.95, 95% CI 0.91–1.00 for
dexmedetomidine and 0.97, 95% CI 0.96–0.98 for antipsychotics). Paralytics
were associated with increased risk for VAEs, prolonged mechanical ventilation,
prolonged length-of-stay, and mortality. Conclusions: Sedatives differ in their
associated risks for VAEs and other outcomes. These findings have important
implications for clinical care and quality improvement.
53
51
ARCHETYPING ARTIFACTS IN MONITORED NONINVASIVE
VITAL SIGNS DATA
Madalina Fiterau1, Artur Dubrawski1, Marilyn Hravnak2, Lujie Chen1, Michael
Pinsky3, Gilles Clermont4, Eliezer Bose5; 1Carnegie Mellon University Auton Lab,
Pittsburgh, PA, 2University of Pittsburgh, Pittsburgh, PA, 3Univ. of Pittsburgh
School of Medicine, Pittsburgh, PA, 4University of Pittsburgh Medical Center,
Pittsburgh, PA, 5University of Pittsburgh School of Nursing, Pittsburgh, PA
Learning Objectives: False alerts in monitored patients cause alarm fatigue in
clinical staff and can adversely impact medical outcomes. We used an informative
clustering approach (Fiterau, Dubrawski: A Unified View of Informative Projection Retrieval, ICMLA 2013) to identify human interpretable archetypes of false
alerts as a preliminary step to corrective action plans. Methods:Noninvasive vital
signs (VS) data including ECG-derived heart rate (HR), respiratory rate (RR),
systolic and diastolic blood pressure (BP), and peripheral oximetry (SpO2) collected at 1/20Hz frequency contained 1582 physiological abnormality episodes
(HR140, RR36, systolic BP 200, diastolic BP>110, SpO2<85%). A committee
of 4 expert clinicians adjudicated them as 1115 real alerts, 318 artifacts, 149
unclear. Statistical features extracted from periods of 4 min before each event:
mean, std dev (sd), min, max, data duty cycle (DD), min and max of 1st order
differences, gradient, etc. were used to cluster artifacts triggered by exceedences
in specific vitals: RR (111), SPO2 (137), BP (70) in low-d projections for easy
interpretation. Results: Clinician review of the patterns elicited the following
BIG DATA, OPEN SOURCE TOOLS, AND CLINICAL DECISION SUPPORT IN A PEDIATRIC ICU
Curtis Kennedy1, Ayse Arikan2, Eric Williams3; 1Baylor College Of Medicine,
Houston, TX, 2Baylor College of Medicine, Houston, TX, 3Baylor College of
Medicine/Texas Childrens Hospital, Houston, TX
Learning Objectives: The purpose of clinical decision support (CDS) is to
reduce the cognitive demands of bedside caregivers by providing them with useful information when and where they need it. Our overarching hypothesis is that
automated screening of data from a pediatric intensive care unit (PICU) can help
caregivers identify potential problems, providing an opportunity to reduce morbidity and mortality. Here we describe an infrastructure we engineered using freely
available, open source software to automate the process of data screening and its
delivery as CDS to our PICU clinicians. Methods: This project is IRB approved.
Using freely available, open source software, we developed a system that automates
data extraction from our electronic medical record, synthesizes raw data elements
into clinically useful measures, and alerts caregivers of potentially important signals. The system’s output can be directed to one or more of: email, pager, and
SMS messages, web pages, and mobile tablet / smartphone interfaces. Results: The
system has collected over 39 million data elements on over 6700 PICU admissions
for over 5700 patients. Median data latency is approximately 10 minutes from
time of entry. 12 modules generate an average of 7 pager messages, 25 email alerts,
and 600 web pages per day. With the implementation of the smartphone / tablet
interface, clinicians can easily provide feedback about the utility of specific alerts.
Additional benefits of the system include rapid data extraction for retrospective
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
studies and quality improvement projects (under separate IRB protocols), and
automated data entry into web portals for national registries. Conclusions: Free,
open source software can be used to implement a Clinical Decision Support system that can help caregivers find important signals in a timely fashion, helping
them achieve the mission of delivering the right care at the right time.
54
COST SAVINGS FROM REAL TIME PRESSURE MAPPING ON
HOSPITAL ACQUIRED PRESSURE ULCERS IN A MEDICAL ICU
Ogochukwu Azuh1, Harriet Gammon1, Amir Ghaznavi1, Aamir Siddiqui1, Bruno
DiGiovine1; 1Henry Ford Hospital, Detroit, MI
Learning Objectives: Annually $9.6-$11.6 billion is spent on management of
pressure ulcers. Our institution has combined policy and the use of continuous real time pressure mapping (RTPM) to combat Hospital acquired pressure
ulcers (HAPU). RTPM technology allows the bedside care team to identify areas
of increased pressure and provide effective patient repositioning. We hypothesize that using RTPM will translate into a significant cost savings. Methods:
A 3-month prospective controlled study was conducted in a Medical intensive
care unit (MICU) of a 900-bed teaching hospital. All MICU admissions were
assigned to 2 different groups. Group A assigned to a bed equipped with a RTPM
device and Group B assigned to a bed without. The patients’ skin was assessed
daily and weekly to recognize and treat HAPUs. Control group patients were
turned every 2 hours per MICU policy. RTPM patients were also turned every 2
hours, however turned in a way to offload high-pressure points that corresponded
to the RTPM graphical display. Outcomes measured included development of
ulcers between groups and cost savings. Cost savings was calculated using a methodology similar to a prior ICU financial modeling of cost savings after implementation of an ICU early physical rehabilitation program. Results: Two patients in
Group A (n=217) developed HAPUs (0.9%) compared to ten patients in Group
B (n=213; 4.7%; P=0.02). RTPM vs Control group comparison showed no differences in age, length of stay, acuity, patient weight, co-morbidities and Braden
score. Incurred cost of development of HAPUs in the RTPM vs control group
was $15,684 vs $78,420. Calculated cost savings percentage between both groups
over the 3-month study duration was 80.5%. Conclusions: By comparing two
equivalent populations we have shown a statistically significant reduction in ICU
pressure ulcer development. A significant cost savings percentage is also achieved
when analyzed with a cost savings model. RTPM not only improves patient outcomes but improves cost savings. Future studies will be conducted to determine
cost of implementation of RTPM in scalable health care environments.
55
EFFICACY OF SIMPLE SCAVENGING SYSTEM APPLIED FOR
VOLATILE-BASED, LONG-TERM ICU SEDATION
Marcin Wasowicz1, Kelvin Wong2, Deep Grewal2, Margaret Doherty3, Niall
­ erguson4, Andrew Steel5, Angela Jerath6; 1Toronto General Hospital, Toronto,
F
ON, 2Department of Anesthesia and Pain Management, Toronto General Hospital, Toronto, Ontario, 3Toronto General Hospital, Toronto, Ontario, 4Medico-Surgical Intensive Care Unit, Toronto General Hospital, Toronto, Ontario,
5
Medico-Surgical Intensive Care Unit and Department of Anesthesia and Pain
Toronto General Hospital,, Toronto, ON, 6Department of Anesthesia, Toronto
General Hospital, Toronto, ON
Learning Objectives: Volatile anesthetics (VA) are potentially an ideal ICU sedative agents, however administration of volatile-based sedation within ICU has
been somewhat limited by concerns regarding staff exposure and pollution. Previously, our group developed a simple scavenging system used with the Anesthetic
Conserving Device (AnaConDa®, Sedana, Sweden) and applied it for short term
sedation. System minimazed ICU polution below 2 ppm. We postulate that the
same system can used for long-term, volatile-based sedation to reduce contamination of ICU environment. This is safety sub-study of RCT studying long term
volatile-based sedation (VALTS trial). Methods: VALTS is a prospective, multicenter RCT recruiting ICU patients requiring mechanical ventilation over 48
hours. With REB approval, patients were randomized (2:1 ratio) to receive either
isoflurane via AnaConDa® or intravenous sedation. Sedation was titrated to SAS
score of 3–4 using an explicit protocol. First 12 patients receiving isoflurane sedation were included in this analysis. Atmospheric pollution was minimized using
an active scavenging system developed by our group. This system consists of 2
Deltasorb® canisters (Bluezone, Canada) arranged in-series from the expiratory
port of the ICU ventilator to wall outlet suction. Isoflurane concentrations were
measured daily using the InfraRan Vapor Analyzer (Wilkins Ent. Inc. USA) at
4 points along the system: (1) expiratory port, (2) post 1st Deltasorb, (3) post
2nd Deltasorb, (4) at patient’s head. Results: 12 analyzed patients received isoflurane for a mean ±st. dev. of 4.5 ± 3.2 days. There were no technical difficulties
pertaining to the scavenging system or AnaConDa®. The mean (SD) isoflurane
levels at measurements point 1, 2, 3 and 4 were 5.4 (±3.3) ppm, 3.3 (±1.6) ppm,
1.9 (±1.4) ppm, and 0.5 (±0.6) ppm (ambient air), respectively. Conclusions:
Results of this study showed that isoflurane can be safely administered for longterm sedation with use of AnaConDa combined with simple scavenging system.
System maintained atmospheric levels of VA well below current North American
occupational exposure limits.
56
PREDICTING PICU ADMISSION AND TEAM COMPOSITION
FROM TRANSPORT RISK ASSESSMENT IN PEDIATRICS
SCORE
Maria Esperanza1, Jennifer Darcy1, Chantal Keizer2, James Schneider3; 1Cohen
Children’s Medical Center, New Hyde Park, NY, 2N/A, N/A, 3Cohen’s Children’s
Medical Center, New Hyde Park, NY
Learning Objectives: Emergency room providers are uncomfortable with the triage and care of pediatric patients. The accurate and timely disposition of pediatric
transports rely on the accuracy of their assessments. The use of a scoring system
may facilitate timely and appropriate decision making by medical control. We
hypothesize that the Transport Risk Assessment in Pediatrics Score (TRAP) at the
time of transport intake may be utilized to predict the admission location, transport team composition, and required urgency of response. Methods: A retrospective chart review was performed on patients transported into a tertiary children’s
hospital from May to July 2013. Patient demographics, clinical information, and
transport data were collected. Using the data provided at the time of referral, the
TRAP scores were calculated by the investigators. Results were analyzed using
Mood’s Median Test and logistic regression analysis. Results: A total of 388 transports were analyzed. Median age is 8 years (interquartile range [IQR] 3, 13).
61% (n=235) were males. The referring diagnoses are as follows: gastrointestinal
(26%), neurologic (18%), trauma-related (17%) and respiratory (11%). Overall
median TRAP score is 1 (IQR 0,2). The TRAP scores by receiving location were
statistically significant, with those requiring critical care higher than those less
severely ill; (PICU-3 [IQR 1,5]; Medical Floor-1 [IQR 0,2]; ED-1[IQR 0,2] (p
value < 0.001). The TRAP scores by team composition were also statistically significantly higher for those with a full team including an ICU physician and nurse;
EMS-0[IQR 0,2]; EMS/RN-1.5[IQR 1,3]; EMS/RN/MD/RT 6 [IQR 3,7] (p
value < 0.001). The TRAP scores by transport category (emergent -3 [IQR 1,7];
urgent -2 [IQR 0.2]; non-emergent -2 [IQR 0,2]) were not statistically significant
(p value = 0.087). Regression analysis of TRAP scores and likelihood of PICU
admission had a p value of 0.000 and an R-squared adjusted value of 17.1%.
Conclusions: The TRAP score at the time of the intake can predict the likelihood
to require ICU admission and the use of an advanced practice transport team.
Oral Abstract Session: Sepsis
57
IMPACT OF ORAL HEALTH ON INFECTIOUS COMPLICATIONS IN ADULTS HOSPITALIZED DUE TO LEUKEMIAS IN
THE USA
Sankeerth Rampa1, Kyungsup Shin2, Romesh Nalliah3, Veerajalandhar Allareddy4,
Veerasathpurush Allareddy2; 1University of Nebraska Medical University, College of Public Health, Omaha, NE, 2Department of Orthodontics - College of
Dentistry, The University of Iowa, Iowa City, IA, 3Dental Medicine, Harvard
University, Boston, MA, 4Rainbow Babies & Children’s Hospital, Cleveland, OH
Learning Objectives: Infections are a major cause of morbidity and mortality in
hospitalized leukemic patients. In general, it is well known that poor oral hygiene
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
is associated with increased risk of infections. The impact of presence of certain
dental conditions(gingivitis, periodontitis-GP) and risk of infections in hospitalized leukemic adults is unknown. We sought to estimate the prevalence of
gingivitis and periodontitis (GP) in adult patients hospitalized due to leukemias.
Further, we examined the impact of GP on development of infectious complications. Methods: The Nationwide Inpatient Sample for the years 2004 to 2010
was used. All patients (aged 18 years and above) who were hospitalized primarily
due to any of the leukemias were analyzed retrospectively. Prevalence of GP in
this cohort was examined. Association between occurrence of GP and infectious
complications(IC) were examined by multivariable logistic regression analyses.
Effects of confounders such as age, sex, race, insurance status, co-morbid burden, type of admission, and hospital characteristics were adjusted. The present
study was considered IRB exempt. Results:During the study period, a total of
252,382 adults were hospitalized primarily due to leukemias. GP was present in
0.4% of patients. The mean age of patients was 61 years and 55% were males.
Outcomes(with GP vs without GP) include: Septicemia(24.3% vs 16.7%), Bacterial infections(17.9% vs 8.5%), Mycoses(19.6% vs 8.7%), pneumonia(16.2%
vs 15.4%). Following adjustment for patient and hospital level confounders,
patients who had GP were associated with significantly higher odds for septicemia (OR=1.36, 95% CI=1.00–1.86, p<0.05), bacterial infections (OR=2.04,
95% CI=1.45–2.87, p<0.0001), and mycoses (OR=2.14, 95% CI=1.43–3.20,
p<0.0001) when compared to those who did not have GP. Conclusions: Poor
oral health is an independent predictor of increased risk of infections, including septicemia, in hospitalized leukemic adults. Optimal oral care may play an
important role in preventing infections in such high risk patients.
(58 to 136)%, (P<0.01); and LL-37: -17 (-9 to -23)%, 4 (-10 to 14)%, and 30
(23 to 48)%, (P=0.04). % change in hsCRP levels did not differ between groups.
A positive correlation was observed between LL-37 and bioavailable 25(OH)D
(rho=0.4, P=0.03), but not total 25(OH)D. Conclusions: High-dose cholecalciferol supplementation rapidly enhances total and bioavailable 25(OH)D levels
in patients with severe sepsis or septic shock. Changes in bioavailable 25(OH)D
are associated with concomitant increases in circulating LL-37. Larger RCTs are
needed to verify our findings and to assess whether optimizing vitamin D status
and LL-37 may improve clinical outcomes.
58
Scott Harvey1, Catherine Lindsay McKnight2, Chayanin Musikasinthorn3,
David Inouye3, Michael Hayashi4, Kazuma Nakagawa1, Danny Takanishi3,
Mihae Yu5; 1University of Hawaii, Honolulu, HI, 2Queens Medical Center,
Honolulu, HI, 3N/A, Honolulu, HI, 4University of Hawaii At Manoa John
A Burns School of Medicine, Honolulu, HI, 5University of Hawaii School of
Medicine, Honolulu, HI
EBI3 GENETIC DEFICIENCY INCREASES LUNG AND SYSTEMIC INFLAMMATION IN MICE SUBJECTED TO SEPSIS
Travis Langner1, Michael O’Connor2, Paul Hake2, Giovana Piraino3, Hector
Wong4, Basilia Zingarelli1; 1Cincinnati Children’s Hospital, Cincinnati, OH,
2
CCHMC, Cincinnati, OH, 3CCMC, Cincinnati, OH, 4Cincinnati Children’s
Hospital Medical Center, Cincinnati, OH
Learning Objectives: Epstein-Barr virus-induced gene 3 (EBI3) codes for a
subunit of the cytokines interleukin-27 (IL-27) and IL-35. IL-27 is produced
by antigen presenting cells after heterodimerization of EBI3 with the IL-27p28
subunit. IL-35 is produced by regulatory T cells after heterodimerization of EBI3
with the IL12α subunit. Both cytokines have important modulatory functions
in the innate and adaptive immune responses. Previous studies in a model of
sepsis combined with necrosis of the cecum by cecal ligation and puncture have
suggested that EBI3 may have a pro-inflammatory role. However, there are no
studies investigating the role of EBI3 in bacterial infections alone. Objective of
our study was to investigate the regulatory role of EBI3 in the innate immune
response in a model of polymicrobial infection induced by fecal slurry injection
without cecum necrosis. Methods: Male and female C57BL/6 (n=6) and genetically deficient EBI3 knockout mice (n=6) (8–9 weeks old) were subjected to
intraperitoneal injection of fecal slurry (0.8 mg/g body weight). Plasma cytokines
were detected by multiplex array and myeloperoxidase activity (MPO) assay was
performed on lung tissue at 6 hours after challenge. Results: At 6 hours after fecal
slurry injection, lung neutrophil infiltration, as evaluated by MPO assay, was significantly higher in the EBI3 knockout mice (102.5 ± 9.1 U/100 mg tissue) when
compared to wild-type mice (39.3 ± 5.9 U/100 mg tissue, P<0.05). EBI3 knockout mice also exhibited higher plasma levels of IL-1 β (512.9 ± 303.0 pg/ml), IL-6
(42.2 ± 9.2 ng/ml) and IL-10 (15.7 ± 6.1 ng/ml) at 6 hours when compared with
levels of wild-type mice (12.6 ± 5.4 pg/ml, 26.1 ± 7.9 ng/ml and 1.5 ± 0.8 ng/ml,
respectively; P<0.05). Conclusions: Our data suggest that EBI3 subunit plays an
integral role in the innate immune response and may be important in modulating
lung and systemic inflammation after bacterial sepsis. (Supported by NIH R01
GM067202; R01 AG027990; R01 GM099773; R01 GM096994).
60
PERSISTENTLY HIGH ALBUMIN LEAK IS ASSOCIATED
WITH MORTALITY.
Learning Objectives: Degree of capillary permeability is associated with endothelial dysfunction and severity of inflammation. An albumin transudation rate
can be measured by injecting radioactive albumin into the circulation, and measuring the concentrations over time. The results are presented as part of the blood
volume analysis (BVA) which measures circulating plasma volume and red cell
volume. Hypothesis: A high albumin transudation rate in the critically ill patients
is associated with mortality. Methods: Surgical patients requiring resuscitation
had BVA’s performed on Day 1, Day 2, Day 3, and Day 5 after the initial resuscitation. Injection of I-131 labeled albumin (1ml) was followed by 5 timed-drawn
aliquots, which was analyzed by BVA-100 (Daxor Corp. NY, NY) to calculate the
albumin leak rate. The results were classified as “high” if the leak rate was >0.25%/
minute and “low” if ≤0.25%/minute. Results: 50 patients completed the study
and comparison between survivors (S) (n=37), and non-survivors (NS) (n=13)
were done. Age in years was 62 ± 16 (S), 67 ± 13 (NS), p=0.31.Sex (Male:Female)
was 24:13 (S), 8:5 (NS), p=0.90. No. of patients with Severe sepsis, septic shock
was 26/37 (S), 8/13 (NS), p=0.81; with Cardiovascular collapse was 3/37 (S) and
4/13 (NS), p=0.12; with ARDS was 8/37 (S), and 1/13 (NS), p=0.49. APACHE
II score was 26 ± 2 (S), 28 ± 2 (NS), p=0.003. Number of patients with high leak
rate on Day 1 was 13/37 (S), 1/13 (NS), p=0.22. Number of patients with high
leak rate on Day 3 was 11/37 (S), 8/13 (NS), p=0.089. Of the 11 survivors who
had high leak rates on Day 3, 6 converted to normal leak rates by day 5. Of the 8
non-survivors who had normal leak rates on Day 3, 3 converted to high leak rates
by Day 5. Therefore, 32/37 survivors demonstrated a normal leak rate during
Day 3–5 and 11/13 non-survivors demonstrated a high leak rate during Day 3–5
(p=0.0001). Conclusions: Persistently high albumin leak rates at and more than
3 days after resuscitation was associated with higher mortality.
61
59
EFFECT OF CHOLECALCIFEROL SUPPLEMENTATION ON
VITAMIN D STATUS AND CATHELICIDIN IN SEPSIS
Sadeq Quraishi1, Gennaro DePascale, MD2, Joseph Needleman2, Carlos
Camargo, Jr., MD, DrPH2, Ednan Bajwa2, Ishir Bhan, MD, MPH2; 1Massachusetts General Hospital, Boston, MA, 2Massachusetts General Hospital, Boston,
United States
Learning Objectives: Vitamin D status is associated with morbidity and mortality in ICU patients. While critically ill patients tend to have low 25-hydroxyvitamin D [25(OH)D] levels, little is known about supplementation strategies
during acute stress. We performed a randomized, controlled trial (RCT) to rapidly optimize vitamin D status and cathelicidin (LL-37), a vitamin D-regulated
antimicrobial peptide, in patients with severe sepsis or septic shock. Methods:
We randomized 30 patients to receive: placebo (n=10); 200,000 IU cholecalciferol (n=10); or 400,000 IU cholecalciferol (n=10), within 24 hours of new onset
severe sepsis or septic shock. Blood samples were obtained at baseline and on days
3, 5, and 7, to assess total 25(OH)D, as well as vitamin D binding protein and
albumin to calculate bioavailable 25(OH)D. Plasma LL-37 and high sensitivity
C-reactive protein (hsCRP) levels were also measured. Groups were compared
using Kruskal-Wallis tests. Spearman correlation was used to assess change in
LL-37 relative to changes in vitamin D status. Results: At baseline, median (IQR)
plasma 25(OH)D was 17 (13 to 22) ng/mL. 25(OH)D levels peaked by day 5 in
all three groups. Relative to baseline, on day 5, median changes in biomarkers for
the placebo, 200,000 IU cholecalciferol, and 400,000 IU cholecalciferol groups,
respectively, were: total 25(OH)D: 3 (-3 to 8)%, 49 (30 to 82)%, and 69 (55 to
106)%, (P<0.001); bioavailable 25(OH)D: 4 (-8 to 7)%, 45 (40 to 70)%, and 96
PRE-ADMISSION ORAL STEROIDS ARE ASSOCIATED WITH
A DECREASED RISK OF ARDS IN ICU PATIENTS WITH SEPSIS
Erin McGuinn1, Matthew Semler1, David Janz2, Lorraine Ware1, Todd Rice1;
1
Vanderbilt University Medical Center, Nashville, TN, 2Louisiana State University School of Medicine, New Orleans, LA
Learning Objectives: Inflammation’s central role in Acute Respiratory Distress
Syndrome (ARDS) development has prompted trials of corticosteroids for inpatients at risk for and with ARDS with inconsistent results. It is unknown if oral
steroid exposure prior to onset of inflammatory injury protects against ARDS
development. Methods: We conducted a retrospective analysis of the Validating Acute Lung Injury biomarkers for Diagnosis cohort to test the hypothesis
that in patients septic on ICU admission oral corticosteroid use lowers ARDS
incidence. Patients receiving any dose of oral corticosteroids prior to hospital
admission were compared to those not receiving steroids in univariate and multivariate analyses with regard to the primary endpoint of ARDS incidence in
the first 96 hours of ICU admission. Secondary outcomes included in-hospital
mortality, ventilator-free days to day 28 (VFDs), and ICU length of stay. Results:
Of 1120 septic patients, the 178 (15.9%) receiving oral corticosteroids prior to
admission had similar baseline characteristics except lower rate of tobacco (14.6%
vs. 35.1%, p<0.001) and alcohol use (5.1% vs 15.9%, p<0.001), higher medical
ICU admission rate (90.4% vs. 75.8%, p<0.001), and higher rate of hematologic
malignancy or stem cell transplant (24.7% vs. 10.4%, p<0.001) than those not
on steroids. ARDS incidence in the first 96 hours was 33.1% for those with preadmission corticosteroids compared to 40.7% for those without (p=0.060). In
multivariable regression analysis, pre-admission corticosteroids were associated
with lower incidence of ARDS (OR 0.52, 95% CI 0.34–0.81, p=0.004). The
corticosteroid group experienced higher mortality (30.4% vs. 22.7%, p = 0.036)
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
with similar VFDs (18 ± 12 vs 18 ± 11 days, p=0.8) and ICU length of stay (8 ± 8
vs. 9 ± 9 days), p=0.17). Conclusions: Oral corticosteroids prior to admission are
independently associated with lower incidence of ARDS but higher mortality in
ICU patients with sepsis. Whether administration of steroids to at risk patients
prior to inflammatory insult prevents ARDS requires prospective study.
62
RECOMBINANT HUMAN THROMBOMODULIN INHIBITS
NEUTROPHIL EXTRACELLULAR TRAPS FORAMATION IN
VITRO
Mika Suga1, Yasuyo Shimomura1, Osamu Nishida1, Naohide Kuriyama1,
Tomoyuki Nakamura1, Toshikazu Sakai1, Yu Kato1, Yoshitaka Hara1; 1Anesthesiology and Critical Care Medicine, Fujita Health University School of Medicine,
Toyoake, Aichi
Learning Objectives: Neutrophil extracellular traps (NETs) are important for the
innate immune system as the first line of local defense against pathogens by preventing their spread. However, excessive NET formation might induce multiple
organ failure (MOF) by accelerating microvascular thrombosis and/or endothelial
dysfunction. NET formation is increased by activated platelets. Thrombin is an
activator of platelets. Thus thrombin might be associated with NET formation.
Thrombomodulin (TM), an endothelial anticoagulant protein, neutralizes thrombin. Therefore, TM might inhibit NET formation and reduce the deterioration of
MOF. Recombinant human TM (rh-TM) has been approved for the treatment
of DIC in Japan. Therefore, we investigated whether TM could decrease NET
formation using its recombinant form, and NET formation could be inhibited by
a specific thrombin inhibitor, Hirudin. Methods: Peripheral blood was obtained
from healthy volunteers. Neutrophils were isolated using Polymorphprep. For
platelet isolation, whole blood was centrifuged to obtain platelet-rich plasma. By
in vitro study of NET formation, neutrophils (5 × 104) and platelets (5 × 105) were
incubated in the presence of 0.2 μg/ml lipopolysaccharide (LPS). Anticoagulant
reagents used included 2 μg/ml rh-TM, 10 U/ml unfractionated heparin, 10 U/
ml antithrombin (AT), and 40 nM Hirudin. NET formation was confirmed by
immunostaining and confocal microscopy. Cells were stained using antibodies
against myeloperoxidase and histone H2A.X, followed by species-specific secondary antibodies. DNA was stained with DAPI. Results: NET formation in human
neutrophils was induced by LPS. NET formation was reduced by rh-TM. Heparin
could not reduce it, despite adding AT to heparin treatment. A specific thrombin
inhibitor, Hirudin, reduced NET formation. Conclusions: These findings suggested that NET formation is associated with thrombin and that inhibition of
NET formation is also possible for TM on endothelium as host defense. The data
support the effectiveness of rh-TM against sepsis or DIC.
63
REWS: REAL-TIME EARLY WARNING SCORE FOR SEPTIC
SHOCK
Katharine Henry1, Chris Paxton1, Kwang Sik Kim1, Julius Pham2, Suchi Saria1;
1
Johns Hopkins University, Baltimore, MD, 2Johns Hopkins Hospital, Baltimore, MD
Learning Objectives: Sepsis is the 11th leading cause of patient mortality. Mortality rates have been reported to be nearly 57.3% in those who experience shock
due to sepsis. Currently, there exist no dedicated clinical early warning scores
geared towards early recognition of impending shock. We present REWS, a
real-time early warning score that identifies patients at high risk of developing
septic shock based on routinely collected measurements. Methods: 7424 adult
patients (age ≥ 15 years) admitted to the the Beth Israel Deaconess Medical ICUs
between 2001 and 2007 were included in this study (776 with septic shock).
Their data were obtained from the MIMIC II Database. From the set of routinely collected clinical, physiological and laboratory results in the ICU, we developed REWS using a machine learning algorithm. REWS combined static (e.g.,
age) and time-varying (e.g., time since first presentation of Systemic Inflammatory Response Syndrome(SIRS)) factors, including temporal trends (e.g., slope
of heart rate (HR) over the past 12 hours) from the past 12 hours of data to
compute a predictive risk score. For comparison, a SIRS+BP score was used that
quantified risk based on the presence of SIRS and the systolic blood pressure
measurement. The main outcome measure was the odds ratio (OR) of impending
septic shock at 80% sensitivity. 10-fold cross-validation was used for splitting
patients into training and validation sets and reporting test-performance. The
Cochran-Mantel-Haenszel test was used for computing the mean odds ratio for
shock at a given sensitivity, and the associated 95% confidence interval. We also
report specificity (spec) at 80% sensitivity. Results: Increased REWS (OR 14.5,
95% CI 11.9–17.7, p 2.78e-227, spec 0.781) and SIRS+BP (OR 8.63, 95%
CI 8.63–12.8, p=3.13e-166, spec=0.717) scores were significantly associated
with impending septic shock. However, REWS had significantly higher odds (p
<0.001) of impending shock compared to SIRS+BP. Conclusions: An increased
REWS was significantly associated with impending shock. REWS implemented
within electronic medical records can enable early intervention.
64
SHOCK INDEX TO ASSESS OUTCOMES ON PEDIATRIC
INTERFACILITY TRANSPORT
Ryan Jennings1, Kathryn Felmet2, Joseph Carcillo2, Richard Orr2, Bradley Kuch2,
Ericka Fink2; 1University of Pittsburgh School of Medicine, Pittsburgh, PA,
2
Children’s Hospital of Pittsburgh, Pittsburgh, PA
Learning Objectives: Shock Index (SI), the ratio of heart rate to systolic blood
pressure, is useful in assessing prehospital mortality risk and guiding interventions in adults. Increased SI was associated with mortality among children with
sepsis in intensive care units (ICU). In children, adherence to treatment guidelines decreased SI and improved outcomes prior to interfacility transport, but
the effect of transport interventions is unknown. Methods: We reviewed the
Children’s Hospital of Pittsburgh (CHP) transport database of children aged 1
mo – 21 y transported to CHP from another facility with at least 2 sets of vital
signs recorded. Subjects were divided into 4 age groups: group 1 (< 1 y), group
2 (1–3 y), group 3 (4–11 y), and group 4 (≥ 12 y). Suspected sepsis was defined
based on referring facility classification and diagnosed sepsis was defined based
on discharge diagnosis. The primary outcomes, ICU admission and survival, were
evaluated with multivariate logistic regression analysis to determine associated
variables. Results:We studied 3,519 children (56% male, age 75 ± 65 mos). Overall, 1,819 (52%) were admitted to an ICU, 1,572 (45%) had suspected sepsis,
and 493 (14%) had diagnosed sepsis. Initial transport SI decreased with age:
group 1: 1.45 ± 0.42 (mean ± standard deviation), group 2: 1.36 ± 0.32, group 3:
1.20 ± 0.34, group 4: 1.00 ± 0.32 (p<0.001). Change in initial and final transport
SI was not associated with survival (p=0.647). Increased initial SI, age > 1 y,
suspected and confirmed sepsis, and longer transport times were independently
associated with ICU admission while increased initial SI and longer transport
times were associated with mortality (p<0.05). Conclusions:Increased initial SI
may be a good indicator for need for ICU resources and in identifying children at
increased risk of mortality requiring interfacility transport.
Poster Session: Research Citation Finalists
101
PHARMACOKINETICS OF MICAFUNGIN IN PLASMA AND
BURN ESCHARES IN CRITICALLY ILL BURNED PATIENTS
Maria Jose Asensio1, Manuel Sanchez1, BEATRIZ GALVÁN2, Eva Herrero1,
Lucia Cachafeiro1, Alexander Agrifolio1, Sonia Luque3, Abelardo García-deLorenzo1; 1Burn Unit/Intensive Care Unit/UniversityHospital la Paz/IdiPAZ,
Madrid, Spain, 2Burn Unit/Intensive Care Unit/UniversityHospital la Paz/­IdiPAZ,
MADRID, Spain, 3Hospital del Mar. Parc de Salut Mar, Barcelona, Spain
Learning Objectives: Introduction: Micafungin (MCF) is an echinocandin
agent with broad activity against Candida spp., which are frequently isolated in
blood and eschar cultures of critically ill patients with severe burn injuries, who
present different pharmacokinetic (PK) characteristics. Hypothesis: To study the
concentrations of micafungin after the first and repeated doses in plasma and
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
burn eschar tissues and to correlate them with patients’ clinical characteristics.
Methods: Methods: Pharmacokinetic study of MCF during a 6 months period
in 10 critically ill burn patients treated with 100 mg/day by 1h intravenous infusion for at least 5 days. MCF blood concentrations were obtained at end of the
infusion (Cmax) on day1, before next dosing (Cmin) on day2 and at steady state
(Cmax and Cmin on day 4 and 5 of therapy); and after 1-3h of MCF infusion
on day5 in burn tissues and were measured by HPLC. Spearman’s rho test or the
Pearson test were used for bivariate correlations between MCF levels and burned
total body surface area (TBSA), hypoalbuminemia or vasopressors. Results:
Results: Ten patients (8 male; age 18–77 years; median SOFA 5(3–5.6), TBSA
42.0% (34.0–70.0), full thickness 34.5% (12–70)). Mean Cmax of MCF were
5.5, 6.7 and 6.7 μg/ml and Cmin were 0.8, 1.2 and 1.2 μg/ml on days 1, 4 and 5
of therapy, respectively, while 0.8 μg/g in burn eschars. Peak levels of MCF after
the initial and repeated administration were inversely correlated with % burned
TBSA (Spearman’s rho = -0.695 and -0.750 (p<0.05)), respectively. No other
significant correlations were found. One patient (10%) presented candidemia
and the crude mortality was 40%. No adverse events to MCF were reported.
Conclusions: Conclusions: This is the largest pharmacokinetic study of 100mg/
daily of MCF in severely burned critically ill patients. Peak level of MCF was
inversely correlated with burned TBSA but not with other clinical variables. After
the first and multiple doses, MCF levels in plasma and burn eschar tissue higher
than the reported MIC90 against most clinically important Candida species.
102
ADHERENCE TO GUIDELINES BASED ANTIBIOTIC THERAPY IN THE TREATMENT OF COMMUNITY ACQUIRED
PNEUMONIA
Mahmoud Nour1, ayman gaber2, mohamed momtaz2; 1kasr aini, Giza, 2kasr aini,
giza, Egypt
Learning Objectives: In community acquired pneumonia, rapid selection and
initiation of appropriate antibiotic therapy is vital, shortening the illness course
and significantly reducing the risk of complications or mortality. Methods: The
current study was conducted as a prospective observational study involving 100
patients admitted to Critical care Department and diagnosed as having community acquired pneumonia. We recorded demographic data, comobidities,
antibiotic treatment data, data on severity of critical illness using Acute Physiology and Chronic Health Evaluation (APACHE II) scoring system & pneumonia severity index (PSI). Outcome parameters were also recorded & included
mortality, length of stay, need for mechanical ventilation (its duration, ventilator
free days), time to clinical stability, time to radiological resolution & 30 days
readmission rate. All data were statistically analyzed. Results: Fifty nine patients
received IDSA guidelines adherent antibiotic therapy while 41 patients received
initial therapy discordant with the guidelines.There was no significant difference
in the mean APACHE II score (17.6 vs 17.9, P: 0.319) & pneumonia severity
index (P: 0.321).The guidelines adherent group showed a statistically significant
lower mortality rate (13.6 vs 56.1%, P< 0.001), lower mean duration of ICU stay
(10.3 days vs 15.5 days, P< 0.001) & higher ventilator free days (6.3 days vs 3.5
days, P< 0.001)yet was not associated with reductions in time to clinical stability
or time to radiological resolution.In a multivariate analysis, age & adherence to
guidelines based antibiotic therapy were predictors for 30 days readmission. Conclusions: Local compliance to IDSA guidelines is moderate.Adherence to guidelines based empirical antibiotic therapy in patients with community acquired
pneumonia was associated with reduction in the inpatient mortality, length of
ICU stay, and 30 days readmission rate with higher ventilator free days but not
associated with any beneficial effect regarding need for ventilatory assistance, time
to clinical stability or time to radiological resolution.
103
EVALUATION OF SEPSIS TREATMENT OUTCOMES IN PORTAU-PRINCE, HAITI
Alfred Papali1, Marc Augustin2, Lovely Colas2, Carl Jean-Francois2, Avelino
Verceles1, Nevins Todd1; 1University of Maryland School of Medicine, Baltimore,
MD, 2St. Luke Family Hospital, Port-au-Prince, Haiti
Learning Objectives: Severe sepsis is a global phenomenon affecting high- and
low-income countries alike; however, the developing world carries the greatest
burden of sepsis-related mortality. Developing sustainable models for the diagnosis and management of severe sepsis in resource-limited environments should
therefore be an urgent priority. Methods: An 80-bed urban community hospital in Port-au-Prince, Haiti was chosen for implementation of a severe sepsis
clinical pathway adapted from the World Health Organization’s IMAI District
Clinician Manual. Prior to protocol implementation, a needs assessment was
performed by retrospectively reviewing charts of all Emergency Department
patient evaluations from January through March, 2012 to determine the number of patients meeting criteria for sepsis syndrome. Statistical analysis was then
performed on qualifying charts. Results: Out of 1094 eligible charts screened,
139 patients (12.7%) and 116 (10.6%) met clinical criteria for sepsis and severe
sepsis, respectively. In-hospital mortality between septic and severely septic
patients showed a statistically significant difference (9/139 [6.5%] vs 44/116
[37.9%], p<0.001). Intravenous fluids were given to 93 septic and 95 severely
septic patients, respectively (66.9% vs. 81.9%, p=0.01). Only 69 septic and 65
severely septic patients received any antimicrobial agent within 24 hours of triage (49.6% vs. 56%, p=0.37). A second complete set of vital signs after triage
was documented in 94 septic and 93 severely septic patients (67.6% vs. 80.2%,
p=0.03). Conclusions: Significant limitations exist in the treatment of septic
and severely septic patients in Port-au-Prince, Haiti, consistent with findings
from studies in similar resource-limited settings. These limitations highlight the
need for targeted efforts to improve patient outcomes and suggest the potential for successful implementation of a culturally sensitive, resource-appropriate
protocol-based intervention.
104
A POTENTIAL NOVEL ROLE FOR OLFACTOMEDIN 4 IN
SEPSIS
Matthew Alder1, Patrick Lahni2, Hector Wong2, David Hildeman1; 1Cincinnati
Children’s Hospital, Cincinnati, OH, 2Cincinnati Children’s Hospital Medical
Center, Cincinnati, OH
Learning Objectives: Sepsis is a major cause of morbidity and mortality in adult
and pediatric intensive care units. While much of the mechanism of sepsis pathology is understood, novel research may help understand heterogeneity within the
syndrome. Through whole genome expression profiling of peripheral blood leukocytes from patients with sepsis we found olfactomedin 4 (OLFM4) as highly upregulated in septic patients. OLFM4 is a member of the conserved olfactomedin
protein family that functions both intracellularly and extracellularly to facilitate
protein-protein interactions. While functions for other olfactomedin family proteins have been identified, the role of OLFM4 is unknown. OLFM4 is expressed
in a subset of human neutrophils and is one of the few proteins to differentiate
neutrophil subsets. Mice deficient in OLFM4 are viable and are protected from
death induced by intraperitoneal injection of E. coli and S. aureus. Methods: We
performed whole genome expression profiling on peripheral blood leukocytes
from 180 patients with sepsis. We also measured levels of OLFM4 protein levels
in the plasma of 450 septic patients. Finally we utilized the mouse model of cecal
ligation and puncture to investigate the expression of OLFM4 in murine sepsis. We performed quantitative PCR to characterize mouse OLFM4 expression
in sepsis. Results: Transcripts for OLFM4 were significantly up-regulated in non
survivors compared to survivors (131 vs 60 expression relative to microarray controls, p=0.006) and increased expression correlated with complicated course from
sepsis and increasing numbers of organ failures. Increased protein levels in the
serum of septic patients also correlated with complicated course from sepsis (46 vs
61 ng/ml, p=0.005). Mice also show increased expression of OLFM4 during sepsis
and like humans expression is primarily in neutrophils. Conclusions: OLFM4 is
up-regulated in patients with sepsis and expression correlates with disease severity.
Mice with sepsis demonstrate expression of OLFM4 similar to humans suggesting
it may be a potential model to determine the role of OLFM4 in sepsis.
105
COMPARING ACCURACY OF 2 PHASES OF A PEDIATRIC
ELECTRONIC SEVERE SEPSIS SCREENING ALGORITHM
Peter Michael Mangubat1, Samir Shah2; 1LeBonheur Children’s Hospital, Memphis, TN, 2Le Bonheur Children’s Hospital, Memphis, TN
Learning Objectives: Earlier recognition of pediatric severe sepsis is critical for
timely implementation of goal-directed therapy and improving patient outcomes.
The potential impact of prospectively implementing an electronically integrated
Pediatric Severe Sepsis Screening Algorithm (eASSIST) within the Electronic
Medical Record (EMR) to facilitate earlier detection of severe sepsis remains
unclear. Based on phase 1 data analysis of the eASSIST algorithm, phase 2
modifications were made to determine if predictive value would further improve.
Methods: Pre-defined physiological and laboratory data variables were used to
develop an electronic algorithm for severe sepsis which was tested prospectively
during two separate offline periods prior to real time implementation. We prospectively investigated the accuracy of the eASSIST algorithm on all adolescents
(age 12–18 years) admitted to a tertiary-care children’s hospital over two time
periods. Phase 1 was conducted over a 2-week period, while Phase 2 was over a
6-week period. Physiological threshold modifications, eliminating known severe
sepsis mimics and withholding alerts for specific post-operative patients for 48
hours were few of the changes implemented in Phase 2. A comparison between
the 2 phases was performed. Institutional Review Board approval was obtained
prior to study initiation. Results: Phase 1 and Phase 2 had 101 and 348 inpatients respectively that were electronically screened for severe sepsis. Phase 1 had
24 alerts with 10 true positive (TP) alerts, 14 false positive (FP) alerts, and no
false negatives. Specificity was 90.5%. Positive Predictive value (PPV) was 40%.
Phase 2 application had 29 alerts, 17 TP alerts, 12 FP alerts, and no false negatives. Specificity was 97%. PPV improved to 44%. Sensitivity for both phases was
100%. Conclusions: Changes effected within the eASSIST algorithm demonstrated improved tool specificity and PPV. False positive rates decreased thereby
improving algorithm accuracy.
106
DOES PICC INSERTION
INCREASE CLABSI RATE?
IN
BACTEREMIC
PATIENTS
F. Maguire1, Russell Acevedo1, David Landsberg1, Daniel Polacek1, Todd Olrich1,
David Martin1, Lynette Johnson1; 1Crouse Hospital, Syracuse, NY
Learning Objectives: PICC (peripherally inserted central catheters) utilization
is increasing despite concerns for CLABSI (central line associated blood stream
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
infection). There is little evidence or consensus regarding the safety of PICC
placement with concurrent bactermia or sepsis. Methods: For the study period
January 1, 2010 to May 1, 2014, information on all PICC lines inserted on
hospitalized adult patients was analyzed and matched to microbiological data
collected from our infection control database. The bacteremic group was defined
as those having any positive blood cultures within the 4 days prior to PICC
insertion. The non-bactermic group included patients without cultures or with
negative cultures prior to PICC insertion. Charts of those PICCs associated with
CLABSI were reviewed. Results: A total of 5,742 PICCs were placed over the 52
month period. Blood cultures were drawn within the 4 days prior to PICC line
insertion in 1,744 patients. Blood cultures were positive in 474 patients and 159
of those patients had known bactermia at the time of PICC insertion. Fifteen
PICCs had blood cultures attributed to CLABSI, however, chart review revealed
the CLABSI were due to pre-existing lines and none of the 15 PICCs developed CLABSI. There were 61 CLABSIs identified during the study period. The
CLABSI rate for the non-bacteremic group was 61/5268 (1.2%), which was significantly greater than the 0/474 rate (p=0.009) for the bacteremic group. Conclusions: Withholding PICC placement in the setting of bactermia over concerns
for CLABSI is not supported in this study. Several limitations may exist given
the retrospective nature of this study and it is not known whether failing to meet
CLABSI criteria equivocated to improved clinical outcomes. This point carries
increasing significance to healthcare organizations while the National Healthcare
Safety Network definitions are implemented curtailing reimbursement and is an
area for further study.
of BCAA therapy. Methods: Young adult male mice underwent lateral fluid percussion injury (FPI), a model of mild-moderate TBI, and after 2 days of recovery,
were treated with either 100mM of BCAAs (equimolar concentration of each
BCAA) or placebo daily for 2, 3, 4, 5, 10 days, or BCAAs for 5 days followed
by 5 days of placebo (total N=122). Cognitive functioning was assessed using
percent freezing in conditioned fear response (CFR), a hippocampal-dependent
contextual memory task, after BCAA treatment completed. Higher percent freezing indicates better cognitive performance. Data were analyzed using a two-way
ANOVA and one-way ANOVA, respectively. Results: Injured mice receiving
BCAA therapy for 5 or 10 days showed greater behavioral recovery (33 and
41% freezing), compared to equal duration placebo-treated injured mice (23%),
and injured mice receiving BCAAs for 2, 3, or 4 days (23, 28, 26%; p<0.0001).
Injured mice receiving BCAAs for 10 days had significantly greater percent freezing (41%) in CFR than injured mice treated with BCAAs for 5 days followed by
placebo for 5 days (26%). These partially treated mice did not perform differently from injured mice receiving 10 days of placebo (25%; p<0.05). Conclusions: BCAA therapy is required for at least 5 consecutive days to be effective
in improving hippocampal-dependent cognitive performance after FPI. Cessation of enteral BCAA therapy after only 5 days resulted in a functional relapse,
such that cognitive performance at 10 days was equivalent to untreated animals.
Ongoing BCAA therapy may be necessary to sustain cognitive recovery after TBI,
possibly via restoration of regional network excitability.
107
PLASMA HIGH-MOBILITY GROUP BOX-1 (HMGB1) CONCENTRATION IN PEDIATRIC SEPSIS AND MULTI-ORGAN
FAILURE
109
COMBINING EEG AND SERUM BRAIN BIOMARKERS TO
CLASSIFY MORTALITY AFTER PEDIATRIC CARDIAC ARREST
Katherine Anetakis1, Satyanarayana Gedela1, Patrick Kochanek2, Yoshimi
Sogawa1, Ericka Fink3; 1Children’s Hospital of Pittsburgh of UPMC, Pittsburgh,
PA, 2University of Pittsburgh Medical Center, Pittsburgh, PA, 3Children’s Hospital of Pittsburgh, Pittsburgh, PA
Learning Objectives: Certain serum biomarkers and electroencephalography
(EEG) features are associated with neurologic outcome. Our objective was to
evaluate the accuracy of EEG and serum biomarkers alone and in combination
to classify neurologic outcome after CA, hypothesizing that the combination of
serum biomarkers and EEG would have better classification accuracy of outcome
versus either alone. Methods: Serum neuron specific enolase (NSE) and S100b,
from neurons and astrocytes, respectively, were measured approximately 24 h after
CA in 58 subjects in a single center. Patient and CA characteristics and outcome
at 6 months were abstracted. An EEG was obtained 15.4 ± 18.0 (mean±standard
deviation)h post-CA. Two board-certified clinical neurophysiologists independently evaluated the first 60 min of each EEG and graded as follows: 1, continuous, not low voltage, not slow; 2, continuous, low voltage or slow; 3, continuous
low voltage, and slow; 4, discontinuous (including burst suppression); 5, isoelectric. A favorable EEG included grades 1–3; an unfavorable EEG included grades
4–5. We correlated biomarkers and EEG scores and built a multivariate model
using biomarkers for prediction of mortality. Results:Children were 5.8 ± 6.2 y
of age and 25 (43%) died. Serum NSE (56 ± 40 vs. 26 ± 25 ng/ml) and S100b
(0.24 ± 0.35 vs. 0.04 ± 0.08 ng/ml) concentrations were increased and unfavorable
EEG (68% vs. 17%) occurred more frequently in children who died vs. survived
(all p< 0.05). Serum NSE (ρ=0.27, p<0.05), and S100b (ρ=0.35, p<0.05), were
moderately correlated with unfavorable EEG. Serum NSE in combination with
EEG had a positive predictive value to classify mortality=73% (p<0.05) with an
area under the curve (AUC)=0.82 compared to serum NSE alone (AUC=0.79)or
EEG alone (AUC=0.71). Serum S100b in combination with EEG had a positive
predictive value to classify mortality=82% (p<0.05) with an AUC=0.85, comparable to serum S100b alone (AUC=0.86). Conclusions: Isolated Serum S100b
at 24 h alone or S100b or NSE at 24 h in combination with EEG may aid in
outcome classification of children with CA.
108
THE ROLE OF BRANCHED CHAIN AMINO ACIDS IN THE
FUNCTIONAL RECOVERY FROM TRAUMATIC BRAIN INJURY
Matthew Kirschen1, Jaclynn Elkind1, Miranda Lim2, Brendan Putnam3, Akiva
Cohen3; 1Children’s Hospital of Philadelphia, Philadelphia, PA, 2Portland Veterans Affairs Medical Center, Portland, OR, 3Children’s Hospital of Philadelphia,
Philadelphia, PA
Learning Objectives: Cerebral concentrations of the branched chain amino acids
(BCAA) - valine, isoleucine, and leucine - are reduced following traumatic brain
injury (TBI) in both animal models and humans, and enteral BCAA therapy
ameliorates hippocampal-dependent behavioral deficits. The minimum duration
of BCAA therapy necessary to restore cognitive performance after TBI remains
unknown, and it is unclear whether these behavioral deficits recur after cessation
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Diana Pang1, Ronald Aaron Bola2, Alicia Au3, Joseph Carcillo4, Eric Halstead5,
Robert Clark4, Rajesh Aneja1; 1Children’s Hospital of Pittsburgh of UPMC,
Pittsburgh, PA, 21University at Buffalo, State University of New York, Buffalo,
NY, 3Childrens Hospital of Pittsburgh, Pittsburgh, PA, 4Children’s Hospital of
Pittsburgh, Pittsburgh, PA, 5Penn State College of Medicine Hershey Children’s
Hospital, Hershey, PA
Learning Objectives: HMGB1 is a prototypic member of the “alarmin” family
and is considered to be a late mediator of sepsis. Elevated plasma HMGB1 levels
in adult septic patients were associated with mortality and multi-organ failure
(MOF). A single pediatric study has reported on HMGB1 as a potential diagnostic and prognostic marker of serious bacterial infection and bacteremia, but
data on plasma HMGB1 in pediatric sepsis and MOF is lacking. Our hypothesis
is that plasma HMGB1 is elevated in pediatric patients with severe sepsis and
MOF. Methods: This IRB-approved study included 48 children admitted to the
pediatric intensive care unit (PICU) who presented with clinical signs and symptoms of severe sepsis. Critically ill non-septic patients were enrolled as controls
(n=10). Blood samples were collected within the first 24 hours of enrollment.
Demographic and clinical data were reviewed, including Organ Failure Index
(OFI) and mortality. Serum HMGB1 was measured by enzyme-linked immunosorbent assay. Mann-Whitney rank sum test and receiver-operating characteristic
(ROC) analysis were used. Results: The mean age of this group was 6.1 ± 0.9
years, and 48% were males. Thirty one patients (65%) had septic shock and 38
patients (78%) had MOF. Mortality was 6% (n=3). Mean PRISM score was 9.
Septic patients had significantly higher HMGB1 levels than critically ill nonseptic patients (16.8 ± 3.7 ng/mL vs 3.2 ± 1.0 ng/mL, P=0.0004). Furthermore,
plasma HMGB1 levels were significantly higher in septic patients with MOF as
compared to patients without (19.6 ± 4.7 ng/mL vs 6.3 ± 1.1 ng/mL, P=0.027).
ROC analysis demonstrated an area under the curve (AUC) (95% confidence
interval (CI)): 0.729 (0.58–0.84). A plasma HMGB1 concentration of 9.54 ng/
mL had a sensitivity of 55% and specificity of 90% (P = 0.0041) for detecting
MOF. Conclusions: Our data suggest that elevated plasma HMGB1 levels may
be a reliable biomarker that correlates with MOF. Further inquiry into the regulation of HMGB1 expression and its role in immune responses will be helpful in
designing therapeutic strategies for the treatment of sepsis.
110
HIGH-DOSE ERYTHROPOIETIN IMPROVES SURVIVAL IN A
SWINE MODEL OF VENTRICULAR FIBRILLATION
Raul Gazmuri1, Herbert Whitehouse2, Vesna Borovnik-Lesjak2, Kruti Shah2,
Alvin Baetiong2, Jeejabai Radhakrishnan3; 1Captain James A. Lovell Federal
Health Care Center, North Chicago, IL, 2Rosalind Franklin University of Medicine and Science, North Chicago, IL, 3Rosalind Franklin University, North
­Chicago, IL
Learning Objectives: We and others have reported beneficial effects associated
with administration of erythropoietin (EPO) during cardiac resuscitation in
animal models of cardiac arrest and in one clinical study. EPO was associated
with improved hemodynamic efficacy of chest compression, reduced duration
of the resuscitation effort, lesser post-resuscitation myocardial dysfunction, and
improved survival. We investigated the effects of EPO on hemodynamic and
myocardial function along with subsequent survival in a swine model of ventricular fibrillation (VF) and closed-chest resuscitation. Methods: VF was electrically
induced in 16 male immature domestic pigs (35 to 41 kg) and left untreated for
8 minutes. Chest compression was delivered using a LUCAS device and defibrillation attempted 10 minutes later. Resuscitated pigs were observed for 120
minutes. Pigs were then recovered from anesthesia and observed for a maximum
of 72 hours. Pigs were randomized 1:1 to receive 1,200 U/kg of EPO or vehicle
control into the right atrium before starting chest compression. Results: LUCAS
delivered CPR was highly effective hemodynamically yielding an aortic diastolic
pressure of approximately 45 mmHg in both groups and a comparable resuscitation rate. Post-resuscitation there was comparable early hemodynamic and
myocardial function as well as comparable organ blood flow but more control
pigs died after resuscitation with only 2 of 8 control pigs and 6 of 8 EPO pigs
surviving 72 hours (p = 0.048 by log-rank test). Demise – documented during
the monitored period – was characterized by progressive hemodynamic deterioration. Conclusions: The present study is consistent with an emerging body of
preclinical work and a single non-randomized, open-label, clinical study supporting a potential role of EPO for resuscitation for cardiac arrest. The present study
failed to demonstrate effects during CPR or the early post-resuscitation phase but
indicated an effect mitigating post-resuscitation myocardial and hemodynamic
dysfunction that resulted in improved survival from cardiac arrest.
111
VARIATION OF CENTRAL VENOUS CATHETER USAGE IN
THREE ICUS MANAGED BY THE SAME INTENSIVIST GROUP
Richard Woerndle1, Alex Hoyt2, John Hoyt3; 1N/A, N/A, 2MGH Institute of
Health Professions, Boston, MA, 3Allegheny General Hospital, Pittsburgh, PA
Learning Objectives: The complications and costs associated with central venous
catheters (CVC) have led to much interest in their incidence and epidemiology.
A wide variability of use in ICUs has been identified with subsequent speculation
that provider practice patterns as opposed to patient factors, including acuity,
influence their use. A further understanding of CVC utilization by fellowshiptrained intensivists in a group practice would assist in risk-benefit analysis and
facilitate consensus opinion on appropriate usage. Hypothesis: There would not
be a significant difference in CVC use in ICUs managed by Pittsburgh Critical
Care Associates (PCCA). Methods: A retrospective observational study utilizing
data derived from an APACHE II B database that included three community
hospital ICUs managed by PCCA, from January 1, 2013 to December 31 2013.
Multivariate regression models were used to estimate the association between the
presence and duration of a CVC at anytime during the ICU stay and APACHE
II score on admission to the ICU, ICU length of stay, presence of an endotracheal
tube (ET), presence of an arterial catheter (AC), and hyperalimentation (HAL).
Results: 2,736 patients were admitted to the three ICU’s in 2013, of which 423
received a CVC. The incidence was similar at ICU1 (9.6%) and ICU2 (12.7%),
but higher at ICU3 (32.3%). ICU3 had higher acuity (mean APACHE II score
23.4 ICU3 vs. 18.8 ICU1 vs. 19.3 ICU2), longer ICU stays, and higher incidence
of ET, AC, and HAL compared with ICU1 or ICU2. In a logistic regression
model adjusting for APACHE II, ET, AC, HAL, and ICU days, the odds of CVC
were 46.4% lower at ICU1 compared with ICU3 (OR 0.54; 95%CI 0.40–0.71)
and 26.7% lower at ICU2 compared with ICU3 (OR 0.73; 95%CI 0.54–1.0). In
contrast, a linear regression employing the same variables among those with CVC
found that CVC duration was 0.52 days longer at ICU1 (95%CI -0.06 – 1.1)
and 0.64 days longer at ICU2 (95%CI 0.09–1.19). Conclusions: Significant
variations in incidence and duration of CVCs in ICUs managed by the same
intensivist group exist and are not fully explained by patient acuity.
112
VCO2, measured REE (MREE), predicted REE (PREE), use of sedatives/analgesics and dose classified as high or low, hospital day, and ventilator day. Results:
269 IC reports with sedative/analgesic data were available for review. Sample
demographics are: mean age 60.5 (17.5) yrs, 62% male, 80% Caucasian, BMI
30.2, 71% receiving sedation/analgesia, mean hospital and ventilator days were
11.5 and 6.3, respectively. Mean (m) MREE 1792 + 585 kcals/d, mPREE 1585
+ 329 kcals/d, mVO2 .260 (.08) L, mVCO2 .204 (.07) L, and mRQ .79 (.09).
Hypermetabolic patients (V02 > .250 L; n=119) were younger (60.5 y) with a
significantly greater MREE 2291 + 510 kcals/d than other ICU patients (n=147)
who were older (70 y) with MREE 1389 + 215 kcals/d; p < .001. Amount of
sedation/analgesia was correlated with MREE; high dose agents compared with
no agents had higher MREE; mean difference of +355.9, SE 104.2; p=.002; this
contradicts the assumption that higher levels of sedation/analgesia lower the
REE. Conclusions: Both SCCM and ASPEN guidelines recommend the use of
IC for critically ill patients. Energy needs are often unpredictable and hypermetabolism may not be reduced by sedative agents, even at higher doses. Further
research into choice of sedative/analgesic agents and impact on REE is needed.
113
EPIDEMIOLOGY AND OUTCOMES OF NEW-ONSET ATRIAL
FIBRILLATION IN THE ICU: A 6-YEAR RETROSPECTIVE
STUDY
Perliveh Carrera1, Charat Thongprayoon2, Wisit Cheungpasitporn2, Vivek Iyer2,
Teng Moua3; 1Mayo Clinic, Department of Critical Care Medicine, Rochester,
MN, 2Mayo Clinic, Rochester, MN, 3Mayo Clinic (CCM), Rochester, MN
Learning Objectives: Atrial fibrillation (AF) is the most common arrhythmia in
the critically ill. However, data in the medical intensive care unit (MICU) is scare.
This study was conducted to determine epidemiology and outcomes of newonset atrial fibrillation (NOAF) in non-cardiac and non-surgical ICU patients.
Methods: Single center, retrospective cohort study of patients admitted to the
MICU at Mayo Clinic, Rochester from 2008 to 2013. Patients were grouped
into AF and no AF identified using ICD-9 diagnosis code 427.3x. AF cohort
was further divided into NOAF and pre-existing AF. Demographics, comorbidities, CHADS2, and APACHE III scores were abstracted from the medical record
along with outcomes such as vasopressor use, renal replacement therapy (RRT),
mechanical ventilation (MV), length of stay (LOS) and mortality. Logistic regression analysis was used to compare outcomes of patients with NOAF, pre-existing
AF, and no AF. Effects of age, CHADS2, and APACHE were adjusted for in
regression models. Results: A total of 10,836 MICU patients were included in
the study, of which 582 (5%) had NOAF, 2368 (22%) pre-existing AF, and 7886
(73%) no AF. Baseline characteristics were significantly different between groups
(p<0.001) with AF patients being older (73.5 vs 78.6 vs 59.8). Hypertension was
the most common comorbidity (68% vs 81% vs 53%). APACHE scores higher
in the NOAF group (57 vs 54 vs 42). Outcomes significantly different (p<0.001)
between cohorts with higher vasopressor use (33% vs 18% vs 12%); RRT (11%
vs 9% vs 5%); MV (39% vs 22% vs 24%); MICU mortality (11% vs 8% vs 5%);
and hospital mortality (20% vs 16% vs 8%) in the NOAF group. Logistic regression models comparing NOAF with no AF showed increased need for vasopressors (OR 2.45); RRT (OR 2.15); MV (OR 1.69); MICU and hospital mortality
(OR 1.40; 1.63). Conclusions: NOAF was noted in 5% of MICU admissions.
Our study suggests that even after adjusting for age, CHADS2 and APACHE III,
NOAF patients exhibited poorer outcomes and higher resource utilization with
increased need for vasopressors, RRT and MV along with higher MICU and
hospital LOS and mortality.
114
VALIDATION OF THE SWIFT SCORE FOR INTENSIVE CARE
UNIT (ICU) READMISSIONS IN AN ASIAN POPULATION
USING INDIRECT CALORIMETRY DATA TO ASSESS THE
IMPACT OF SEDATIVES ON REE IN THE ICU
Eric Heymann1,2, Liv Maier1,2, Amartya Mukhopadhyay2; 1University Hospital
Centre of Vaud, Lausanne, Switzerland, 2National University Hospital, Singapore, Singapore
Learning Objectives: Continuous intravenous sedation is used frequently in
the ICU to promote comfort and reduce anxiety associated with therapeutic
modalities, such as mechanical ventilation. Nutrition support is also important
to minimize metabolic demands. The contribution of sedation/analgesia, often
with multiple pharmacologic agents, to resting energy expenditure (REE) is not
well-described in the literature. The aim of this project was to examine the impact
of these agents on REE by comparing predicted with measured REE obtained by
indirect calorimetry (IC). Methods: This retrospective, correlational design used
a convenience sample of adult ICU patients. Data from ICU patients during
the period from October 2009 to present are summarized. Variables of interest
include actual body weight, BMI, age, gender, respiratory quotient (RQ), VO2,
Learning Objectives: Readmissions occur in nearly 10% ICU discharges. Since
readmissions are costly and often associated with high mortality, many tools have
been devised and validated to prevent this from occurring. One such clinical
tool is the Stability and Workload Index for Transfer (SWIFT) score which has
been validated in several ICU centers worldwide. No study has of yet validated
this tool in Asian population. Methods: We reviewed the records of all patients
admitted/discharged from the medical ICU of a large university Hospital in Asia
from January to June of 2008. The SWIFT score for each patient was calculated
from their electronic medical records. The SWIFT score was then compared with
the readmission rates to determine if it can be a valuable predictor for readmission
in an Asian population. Results: 409 patients were admitted over the set time
period. 59 patients were excluded from the study due to incomplete data [necessary for SWIFT score calculation]. 80 patients died before initial ICU discharge.
Mary McCarthy1, Janet Fabling1, Christopher Poprawski1, Cristin Mount1;
1
Madigan Army Medical Center, Tacoma, WA
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Therefore 270 patients [age 18 - 97 ± 19.3 years; 173 males] were included in
the study. 17 patients were readmitted of which 5 died and 12 survived the second ICU admission. With a hypothetical SWIFT score over 15 being predictive
of readmission, our group of patients demonstrated a similar trend (t=1.7933,
p=0.0918). Patients readmitted had higher mean SWIFT scores than those not
readmitted (respectively, mean=21.82 and mean=10.68, p<0.0001,). Patients
who were readmitted and survived had a lower SWIFT score mean compared to
those who were readmitted and died (respectively, mean=15.75 adn mean=36.4,
p=0.0081). Conclusions: Our ICU presents a low readmission rate (4.4%)
compared to other ICUs studied to validate the SWIFT score (9% in the South
American study and 8,8% in the North American study). Patients readmitted
to the ICU had a significantly higher SWIFT score compared to patients who
were not readmitted. In light of the increased cost and mortality associated with
readmission to the ICU, our study has shown that the SWIFT score can be useful
predictor to reduce readmission in an Asian population.
CAZ, piperacillin/tazobactam (P/T) and meropenem (MER) were 86.1/91.8%,
88.0/94.3% and 97.8/99.2%, respectively. MER was active against 75.1/85.4%
of MDR-ENT and 8.1/27.1% of XDR-ENT from ICU/non-ICU. CAZ-AVI
inhibited 96.4/100.0% of MER-non-S KPN (KPC-producers) from ICU/nonICU at ≤4 μg/ml (MIC90, 2/2 μg/ml), and all ENT species had ≥99.4% of
strains inhibited at ≤4 μg/ml of CAZ-AVI. S rates for PSA from ICU/non-ICU
(842/2,240 strains) were 77.7/86.9% for CAZ, 71.2/82.2% for P/T, 76.6/84.7%
for MER PSA and 95.6/97.5% for CAZ-AVI at ≤8 μg/ml (CLSI S breakpoint
for CAZ). S rates for CAZ, P/T and MER ranged from 7.5–20.8/9.0–24.5%
among MDR-PSA from ICU/non-ICU. CAZ-AVI inhibited 78.6/81.9% of
MDR- and 71.6/76.3% of XDR-PSA from ICU/non-ICU at ≤8 μg/ml. Conclusions: Lower S rates were observed among ICU compared to non-ICU isolates.
CAZ-AVI exhibited potent activity against a large collection of GN isolated from
ICU and non-ICU patients, and provided greater coverage than β-lactams currently available.
115
117
CEREBRAL PERFUSION PRESSURE IN PATIENTS UNDERGOING HYPOTHERMIA AFTER CARDIAC ARREST
IMPACT OF MACROLIDE ANTIBIOTICS ON OUTCOMES IN
ICU PATIENTS WITH ACUTE EXACERBATIONS OF COPD
Fabio Silvio Taccone1, Katia Donadello2, Antonio Dell’Anna1, Sabino Scolletta3,
Jean-Louis Vincent4; 1Erasme Hospital, Brussels, Belgium, 2N/A, Brussels, Belgium, 3Erasme Hospital, Dept. of Intensive Care, Brussels, Belgium, 4Erasme
University Hospital, Brussels, Belgium
Learning Objectives: Brain perfusion is a major determinant of the severity
of brain damage in experimental cardiac arrest (CA). Although cerebral perfusion pressure (CPP) can be non-invasively estimated using trans-cranial Doppler (TCD), few data are available in the clinical setting. Methods: Prospective
study including patients admitted to the ICU after CA between January 2012
and December 2013 who survived for at least 48 hours. We collected demographic data, CA characteristics and neurological outcome at three months
(good=Cerebral Performance Category [CPC] 1–2; poor=CPC 3–5). TCD
assessment included systolic velocities of the middle cerebral artery (sFV), diastolic velocities (dFV), mean velocities (mFV) and pulsatility index (PI). Regional
cerebral oxygen saturation (rSO2) was evaluated using the near-infrared spectroscopy technique. TCD values, rSO2, mean arterial pressure (MAP) and PaCO2
were collected within 4 hours (T1), 12 hours (T2), 24 hours (T3) and 48 hours
(T4) after CA. CPP was calculated using the following formula: (mFV*[MAPdiastolic arterial pressure])/(mFV-dFV). Results: We studied 24 patients (60
[50–70] years; 19/24 male), with a median time to return of spontaneous circulation of 16 [9.5–22.5] minutes; 17 patients had out-of-hospital CA and 11
had an initial shockable rhythm. Ten patients (41%) had a good neurological
outcome. At T1, CPP values were low (49 [38–63] mmHg) but increased during
the study period (68 [62–73] mmHg at T4, p<0.001). Similarly, rSO2 increased
over time whereas MAP and PaCO2 remained unchanged. Regression analysis
showed no correlation between CPP and MAP, PaCO2 or rSO2 at different timepoints. Patients who had CPP >60 mmHg at all time-points (n=7) had higher
rSO2 than the other patients (p=0.001), in particular at T1 (69 vs. 60 mmHg);
however, MAP and PaCO2 were similar in the two groups. There were no significant differences in CPP, MAP or PaCO2 between patients with good and
those with poor neurological outcomes. Conclusions: Neurological outcome was
not clearly related to the CPP, although higher CPP was associated with better
cerebral oxygenation.
Tyree Kiser1, Richard Allen2, Kavita Nair1, R Vandivier1; 1University of Colorado
Anschutz Medical Campus, Aurora, CO, 2Peak Statistical Services, Inc, Evergreen, CO
Learning Objectives: Macrolide antibiotics have an anti-inflammatory effect in
addition to their antimicrobial properties and studies of azithromycin have demonstrated a reduction of COPD exacerbations in outpatients treated chronically
with the medication. The purpose of this study was to examine the effectiveness
of macrolide antibiotics compared to other antimicrobials in patients admitted to
the ICU with an acute exacerbation of COPD (AECOPD). Methods: This pharmacoepidemiological cohort study evaluated ICU patients with a primary diagnosis of AECOPD admitted to one of 470 hospitals and treated with antibiotics
on the first 2 days between January 1, 2003 and December 31, 2008. Patients
were grouped into macrolide or non-macrolide groups based on antibiotic utilization on hospital day 1 and 2. Patients with pneumonia, shock, pneumothorax,
pulmonary embolism, transferred from an outside hospital, and those staying
less than 2 days were excluded. The primary outcome was hospital mortality.
Results: A total of 14,558 patients were included, 4,766 (33%) were in the macrolide group and 9,792 (67%) in the non-macrolide group. Fluoroquinolones
were the most common prescribed antibiotic in the non-macrolide group (78%
of patients). Fifteen percent of patients received invasive ventilation and 32%
of patients received non-invasive ventilation on hospital days 1 or 2. Mortality occurred in 5.7% of macrolide patients compared to 5.9% of non-macrolide
patients (p=0.48). After propensity score matching (n=3570 per study group),
treatment with macrolides was not associated with a reduction in mortality (5.4%
vs. 6.0%; p=0.28), median hospital length of stay (7 vs. 7 days; p=0.88), ICU
length-of-stay (2 vs. 2 days; p=0.17), length of ventilation (2 vs. 2 days; p=0.75),
or hospital costs ($24,333 vs. $23,493; p=0.19). Macrolide therapy was associated with reduced 30 day hospital readmissions (19.2% vs. 22.4%, p<0.01).
Conclusions: Macrolide therapy did not significantly impact mortality, length of
stay, time on ventilation, or hospital costs, but was associated with a reduced 30
day hospital readmission rate.
118
116
CEFTAZIDIME-AVIBACTAM TESTED AGAINST GRAMNEGATIVE BACTERIA FROM INTENSIVE CARE UNIT (ICU)
PATIENTS
Helio Sader1, Mariana Castanheira1, David Farrell1, Robert Flamm1, Rodrigo
Mendes1; 1JMI Laboratories, North Liberty, IA
Learning Objectives: Ceftazidime-avibactam (CAZ-AVI) consists of CAZ combined with the novel non-β-lactam β-lactamase (BL) inhibitor AVI, that inhibits
Ambler classes A (eg, ESBL and KPC), C, and some D enzymes. Methods: Clinical isolates were consecutively collected from 71 USA medical centers in 2012–
2013 and tested for susceptibility (S) at a central laboratory by reference broth
microdilution methods. Results for 4,381 bacterial isolates from ICU patients
were analyzed and compared to those of 14,483 organisms from non-ICU
patients. BL encoding genes were evaluated for 966 Enterobacteriaceae (ENT)
by microarray-based assay. Results: The most frequent organisms isolated from
ICU/non-ICU patients were P. aeruginosa (PSA)/E. coli (EC), followed by EC/
PSA, K. pneumoniae (KPN)/KPN and Enterobacter spp. (ESP)/ESP. CAZ-AVI
was active against 99.7/99.9% of ENT (MIC90, 0.25/0.25 μg/ml) from ICU/
non-ICU patients (2,948/10,872 strains), including multidrug-resistant (MDR;
96.9/99.1%) and extensively drug-resistant (XDR; 91.9/95.3%) strains, at MIC
of ≤4 μg/ml (S breakpoint for CAZ). Against ENT, S rates (ICU/non-ICU) for
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
PREHOSPITAL HYPOTENSION CORRELATES WITH INJURY
SEVERITY AND OUTCOMES
Clayton Damme1, Jiangtao Luo2, Keely Buesing3; 1University of Nebraska Medical Center, Omaha, NE, 2University of Nebraska Medical Center, College of Public Health, Omaha, NE, 3The Nebraska Medical Center, Dept of General Surgery,
Division of Trauma/Surgical Critical Care, Omaha, NE
Learning Objectives: Significantly injured patients who are prehospital hypotensive but arrive normotensive may be under-triaged; thus, the purpose of this
study was to determine whether prehospital hypotension portends poor outcomes despite achieving normal blood pressures in the trauma bay. We hypothesize that prehospital hypotension will correlate with increased morbidity and
mortality regardless of normotension upon hospital arrival. Methods: This prospective study of patients 10 years and older was conducted at an urban, Level 1
trauma center. Hypotension was defined as a systolic blood pressure (SBP) ≤ 110
mmHg. The lowest recorded prehospital SBP and the first recorded SBP upon
arrival to the hospital were analyzed. Patients who failed to achieve normotension
upon hospital arrival or who presented by a non-EMS service were excluded from
this study. Data were analyzed using the Student’s t-test, setting significance at
p<0.05. Results:150 patients met inclusion criteria (male, n=86; female, n=64,
p=NS). Compared to normotensive patients (NP) (n=117 patients), hypotensive
patients (HP) (n=40 patients) had lower Glasgow Coma Scores both prehospital (12.6 ± 4.18 vs. 14.4 ± 1.8, p<0.05) and at hospital admission (13.1 ± 4.1
vs. 14.4 ± 2.19, p<0.05). Prehospital hypotension positively correlated with ICU
admission (HP 48.5% vs. NP 21.4%, p<0.05), ICU length of stay (LOS) (HP
1.24 ± 1.94 vs. NP 0.46 ± 1.24, p<0.05), ventilator days (HP 0.46 ± 1.24 vs. NP
0.19 ± 0.96 days, p<0.05), and repeat hypotensive episodes during their hospital stay (HP 87.9% vs. NP 60.7%, p<0.05). Injury Severity Score (ISS) correlated with prehospital hypotension (HP 12.4 ± 10.4 vs. 8.68 ± 7.25, p<0.05).
Conclusions:Prehospital hypotension in trauma patients is a significant indicator
of injury severity and is associated with increased admissions to the ICU, ICU
LOS, days on the ventilator, and marks the risk of repeat hypotension during hospitalization, an important consideration in trauma patients. Regardless of admission normotension, prehospital hypotension should be given heavy consideration
when making triage and treatment decisions.
119
THE EVALUATION OF CEREBRAL FUNCTION AFTER HYPOTHERMIA IN A PIG MODEL OF CPR
Ziren Tang1, Peng Peng2, Jiang Tao2, PING GONG3, Wanchun Tang4; 1Weil
Institute of Critical Care Medicine, rancho mirage, CA, 2Beijing Chao-Yang
Hospital, Capital Medical University, Beijing, China, 3Weil institute of critical
care medicine, rancho mirage, CA, 4Weil Institute of Critical Care Medicine,
Rancho Mirage, CA
Learning Objectives: Studies have demonstrated that hypothermia (32–34°C)
improves survival and long-term neurological outcomes in cardiac arrest (CA)
patients. In the present study, we investigated the effects of hypothermia on the
changes in cerebral blood flow and perfusion within 72 hrs after the return of
spontaneous circulation (ROSC) using the perfusion weighted imaging (PWI) of
MRI. We hypothesized that hypothermia (33°C) increases the cerebral blood flow
and improves the perfusion of the brain during the first 72 hrs after ROSC in a
porcine model. Methods: Ventricular fibrillation (VF) was induced in 30 inbred
Wuzhishan miniature pigs. After 8 mins of untreated VF, standard CPR was performed and 28 animals were resuscitated. The resuscitated animals were then
randomly assigned to either the normothermia group (NT, n=14) or the hypothermia group (HT, n=14). In the HT group, the blood temperature was reduced
to 33°C with endovascular cooling and was maintained for 12 hrs, followed by
passive rewarming at 0.5°C/hr to 37°C. The PWI was scanned at baseline, 6,
12, 24 and 72 hrs after ROSC. Results: The PWI index includes time-to-peak
(TTP), mean transition time (MTT) and cerebral blood flow (CBF). The TTP/
baseline in the HT group was significantly lower than the NT group (1.0 ± 0.32
vs. 1.3 ± 0.27 p<0.01) at 24 hrs after ROSC. The MTT/baseline in the HT group
was significantly lower than the NT group (1.4 ± 0.30 vs. 1.7 ± 0.29 p<0.01) at
6 hrs after ROSC. The CBF/ baseline in the HT group was greater than the NT
group (0.57 ± 0.10 vs. 0.22 ± 0.09 p<0.01) at 6 hrs after ROSC. Compared with
the NT group, the HT group exhibited a greater 72 hr survival rate and (78.6%
vs. 42.9%, p<0.05 p<0.05) superior neurological deficit scores (45.27 vs. 119.50;
p=0.001). Conclusions: Hypothermia increases the cerebral blood flow and
improves the perfusion of the brain in pigs within the first 72 hrs after ROSC.
120
PATTERNS OF DETERIORATION IN HOSPITALIZED PEDIATRIC ONCOLOGY PATIENTS REQUIRING ICU ADMISSION.
Asya Agulnik1, Peter Forbes1, Nicole Stenquist1, Carlos Rodriguez-Galindo1,
Monica Kleinman1; 1Boston Children’s Hospital, Boston, MA
Learning Objectives: Pediatric oncology and stem cell transplant (SCT) patients
are a high risk population with frequent intensive care unit (ICU) admission
and high mortality. The purpose of this study is to describe the timing, vital sign
changes, and clinical characteristics of unplanned ICU transfers in these patients.
Methods: This study is a retrospective cohort of all oncology and SCT patients
admitted to Boston Children’s Hospital from September 2011 to December 2013
who required unplanned ICU transfer. Results: During the study period, there
were 110 unplanned ICU transfers (43 oncology and 67 SCT) involving a total
of 83 patients, with a range of 1 to 3 ICU admissions per patient. Of these, 14%
of oncology and 21% of SCT ICU transfers died during their ICU admission.
SCT patients had longer inpatient stays prior to transfer to the ICU than oncology patients (mean 28 vs 12 days, p=.006; median 18 vs 4; p<.001) and longer
ICU lengths of stay (mean 11 vs 5 days, p=.01; median 5 vs 3, p=.001). Distinct patterns of deterioration could be identified in these patients. SCT patients
were more likely to have respiratory distress prior to ICU transfer (78% vs 42%,
p<.001) and oncology patients were more likely to have tachycardia (35% vs
10%, p=.002) and electrolyte imbalance (16% vs 1%, p=.004). Hypotension was
present in 37% of oncology and 24% of SCT transfers in the 24 hours prior to
ICU admission. The ICU was initially consulted, on average, 3.1 hours (SD 4.0;
median 2.0) prior to ICU transfer. Patients transferred to the ICU for hemodynamic changes reached the 90th percentile of age-adjusted heart rate ten hours
prior to ICU transfer. Mortality was higher in patients with respiratory distress
(24% vs 8%, p=.04) and those with high serum lactate on admission to the ICU
(39% vs 14%, p=.02). Conclusions:Oncology and SCT patients admitted to
the ICU have high mortality rates. There are distinct patterns of deterioration
that can be identified using clinical parameters hours prior to ICU transfer. Early
recognition of deterioration in these patients may allow for timely interventions
and improved overall outcomes.
121
FEASIBILITY OF A NON-INVASIVE SENSOR FOR MEASURING ICU PATIENT MOBILITY
Andy J Ma1, Andong Zhan1, Gunnar Sigurdsson1, Nishi Rawat2, Dale Needham1,
Suchi Saria1; 1Johns Hopkins University, Baltimore, MD, 2Johns Hopkins University, Columbia, DC
Learning Objectives: Early Mobilization reduces complications caused by prolonged bed rest in the ICU. Despite its importance, patients’ mobility is not
routinely measured, due, in part, to the burden of manual measurement. Methods: To create a Non-Invasive Mobility Sensor (NIMS) to measure patients’
mobility, 3 Microsoft Kinect cameras were deployed in a single adult ICU room
at Johns Hopkins Hospital. 362 hours of color and depth (RGBD) image data
were collected. The NIMS was developed using the following two steps. First, a
state-of-the-art Computer Vision (CV) algorithm was implemented to automatically track the location and pose (e.g. lying, sitting or standing) of the patient.
Second, using these tracking results over fixed 10-minute time periods, a decision
tree combined the location and pose information to automatically classify the
highest level of mobility achieved over that period into a simplified 6-category
ICU mobility scale: lying in bed, passively moved to chair, sitting over edge of
bed, standing, transferring bed to chair with standing, and walking. To validate
NIMS, we manually reviewed and coded 33 randomly sampled 10-minute video
segments using the simplified ICU mobility scale. The weighted Kappa (κ) with
95% confidence intervals (CI) was used to measure agreement between NIMS
and the manually coded categories. Results: NIMS achieved a κ score of 0.90
(CI: 0.81, 0.98) which is significantly higher (p < 0.0001) than a classifier which
randomly assigned each segment into 1 of the 6 mobility categories. NIMS
achieved a κ score of 1.00 for the mobility categories of lying, sitting and walking. The κ score was lowered in video segments where the patients’ pose changed
greatly (e.g., from sitting to standing) with κ = 0.63 (CI: 0.43, 0.83) due, primarily, to errors in the tracking algorithm that is not robust to large variations in the
pose. Conclusions: A highly accurate NIMS for automating measurement of
patient mobility is feasible using RGBD sensors and CV technologies. A refined
tracking algorithm robust to large variations in patient pose will further improve
accuracy for mobility classification.
122
CULTURE ALGORITHM TO REDUCE URINE CULTURE AND
CATHETER-ASSOCIATED URINARY TRACT INFECTION
RATES
Ashok Cattamanchi1, Lindsay Stevenson1, Priscilla Jang1, Laith Altaweel1, Svetolik Djurkovic1, Nitin Puri1, Sujata Ambardar1, Jason Vourlekis1; 1Inova Fairfax
Hospital, Falls Church, VA
Learning Objectives: Unnecessary urine cultures (UC) may result in false positive
results, antibiotic over-utilization and an increase in reported hospital acquired
infections. As part of a multi-faceted catheter-associated urinary tract infection
(CAUTI) reduction strategy, we introduced a culture algorithm in the ICU. We
hypothesized that this would reduce urine culture rates and also result in reduced
CAUTIs. Methods: An algorithm was developed focusing on fever, with evaluation of clinical data, including U/A for pyuria, over the last 72 hours before sending cultures. This algorithm was implemented in four adult ICUs at Inova Fairfax
Hospital in February, 2014: medical surgical (MSICU), neuroscience (NSICU),
coronary care (CCU), and cardiovascular surgery (CVICU). UC rates were compared for four months before and five months after implementation. CAUTI
and urinary catheter utilization (UCU) rates were compared from 2013 to five
months after implementation. Pearson chi-squared test was used to determine
statistical significance. Results: Comparing before and after implementation, 577
and 442 UC were obtained during 7645 and 9324 patient days, respectively. UC
rates (per 100 patient-days) decreased for all ICUs from 7.55 to 4.74, P<0.0001;
for CVICU 6.89 to 2.58, P<0.0001; for NSICU 7.53 to 4.47 P<0.0001; for
MSICU 8 to 6.18, P<0.001; for CCU 7.8 to 6.25, P=0.06. CAUTI rates (per
1000 urinary catheter days) decreased from 3.15 to 1.65, P=0.09. UCU (catheter
days/patient days) showed a slight increase from 0.50 to 0.52, P<0.001. Conclusions: A culture algorithm reduced UC rates with a commensurate reduction in
CAUTIs. Improved culture practices and catheter maintenance were likely the
major reasons for CAUTI reduction, since device utilization was not impacted.
The culture algorithm most likely screened out patients with colonizing microorganisms. However, It is conceivable that symptomatic CAUTIs were not being
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
identified and treated. Subsequent analysis will compare ICU length of stay, antibiotic use and mortality between the two study periods.
123
PEDIATRIC PROCEDURAL SEDATION USING DEXMEDETOMIDINE: PROVIDER SPECIALTY AND COMPLICATION
RATES
Carmen Sulton1, Courtney McCracken1, Kiran Hebbar2, Harold Simon1, Jason
Reynolds3, Joseph Cravero4, Pradip Kamat1; 1Emory University, Atlanta, GA,
2
Egleston Children’s Hospital, Atlanta, GA, 3Texas Children’s Hospital, Fort
Worth, TX, 4Children’s Hospital Boston, Boston, MA
Learning Objectives: Dexmedetomidine (DEX) is widely used in Pediatric Procedural Sedation (PPS) by a variety of pediatric subspecialists (PS). The objective
of our study was to determine if type of PS affects complication rates when using
DEX to provide PPS. Methods: We performed a retrospective review of patients
from the Pediatric Sedation Research Consortium (PSRC) database to identify
children that received DEX as their primary sedation agent for elective PPS.
Demographic and clinical data, provider subspecialty and sedation-related complications were abstracted. Serious adverse events (SAE) were defined as cardiac
arrest, airway obstruction, death, laryngospasm, emergent airway intervention,
unplanned hospital admission/increased level of care, aspiration or emergency
anesthesia consult. Event rates, 95% confidence intervals (CI), and adjusted odds
ratios (AOR) were calculated. Results: 13,072 children were sedated using DEX.
Seventy-three percent of sedates were ASA class I or II. The providers responsible
for DEX sedates were anesthesiologists (35%), intensivists (34%), emergency
medicine physicians (12.7%), hospitalists (1.1%) and others (17%). The overall
AE rate was 466/13,072 (3.6%; 95% CI: 3.3%-3.9%). AE rate per 10,000 was
highest for emergency medicine (EM) (782) followed by intensivist (583), other
providers (414), hospitalist (355) and anesthesiologist (131). After adjusting for
weight, prematurity, URI, location, and ASA class, compared to anesthesia, the
AOR for having an AE were 8.5 times higher for EM (p<0.001); 5.3 times higher
for intensivists (p<0.001); 4.6 times higher for other providers (p<0.001); and 3.7
times higher for hospitalists (p=0.007). Overall SAE rates were low (38/10,000)
but did not significantly differ by PS. Airway obstruction was the most common
SAE, 35/13,072 cases (0.27%, 95% CI: 0.19%-0.37%). Conclusions: In the
PSRC, PPS performed using DEX is unlikely to yield serious adverse events. No
differences were noted in rates of SAE among different pediatric subspecialists;
however, rates of minor complications may vary.
124
PREDICTORS OF PTSD AND DEPRESSION AMONG FAMILY
AND FRIENDS OF PATIENTS ADMITTED TO THE ICU
Ann Marie Warren1, Megan Reynolds1, Monica Bennett2, Michael Foreman3,
Evan Rainey1, Rebecca Weddle4; 1Baylor University Medical Center, Dallas, TX,
2
Baylor Scott & White Health Care System, Dallas, TX, 3Urgent Surgery Associates, PA, Dallas, TX, 4Department of Surgery, Dallas, TX
Learning Objectives: In the US, almost 5 million people are admitted yearly to
an intensive care unit (ICU). Recent research has examined the impact of ICU
admission on the loved ones of those patients. Though research has identified
adverse psychological outcomes in individuals who have a patient admitted to
an ICU, few studies have examined predictors of these outcomes. Therefore, we
sought to identify predictors of negative psychological outcomes among family
and friends of patients admitted to the ICU. Further, we hypothesized that the
subjects’ relationship of the to the patient would have an impact on psychological outcome. Methods: 100 subjects were enrolled at an urban hospital with a
Level I trauma center as a prospective convenience sample of family and friends
(≥18 years of age) of patients(≥ 18 years of age) admitted to the the trauma/
critical care ICU for ≥48 hours, expected to survive ≥ 96 hours. Depression was
measured using the Patient Health Questionnaire 8 (PHQ-8) and posttraumatic
stress disorder (PTSD) symptoms were evaluated using the Primary Care Posttraumatic Stress Disorder Screen (PC-PTSD). Results:Within the cohort, mean
age was 48.7 years; 77% were female. Over half of subjects were employed (57%),
with 53% having an income > $50,000 a year. Thirty-eight family/friends (38%)
screened positive for depression, and 24 (24%) screened positive for PTSD. Low
income was the only significant demographic factor in screening positive for
PTSD. In predicting who is most at risk for PTSD, being a parent of an ICU
patient was the only significant finding (OR=12.8). When examining depression symptoms in the same group, male gender was protective. Family/friends
with a pre-morbid psychological disorder had a significant risk for developing
depression. Conclusions: Based on these results, there are serious psychological
consequences, including PTSD and depression, among family and friends after
the ICU stay of a loved one. We believe that these mental health issues should be
addressed as part of best global patient care, given that these individuals are often
caregivers of patients post-discharge.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
125
USE OF A PEDIATRIC TRAUMATIC BRAIN INJURY PATHWAY
IS ASSOCIATED WITH IMPROVED OUTCOMES
Natalie Tillman1, Wei Dong2, Andrew Reisner1, Tracie Walton2, Karen Walson1,
Toni Petrillo-Albarano3, Joshua Chern2, Atul Vats4; 1Children’S Healthcare of
Atlanta, Atlanta, GA, 2Children’s Healthcare of Atlanta, Atlanta, GA, 3Children’s
Healthcare Of Atlanta, Atlanta, GA, 4Emory University School of Medicine,
Atlanta, GA
Learning Objectives: Traumatic brain injury (TBI) is a major cause of morbidity and mortality in children. Unlike adult populations, the efficacy of evidence based guidelines used to manage children who have sustained a TBI is
poorly substantiated. Methods: A multidisciplinary committee at Children’s
Healthcare of Atlanta (Children’s) was formed with the primary goal of improving the management of TBI patients. National guidelines for acute management of pediatric severe TBI were used. Treatment algorithms were digitized in
computerized order sets. The guidelines were modified at quarterly meetings,
based on evidence when available, and consensus when not. Compliance was
continually monitored, and frequent education seminars were held. Outcome
measures of patients < 18 years that suffered a TBI with Glasgow Coma Score
(GCS) <9 were reviewed over a 4 year period, 2 prior and 2 after introduction
of the program. Parameters measured pre and post guideline implementation
were mortality rates, ICU length of stay (LOS), ventilator LOS, functionality of survivors as measured by WeeFIM scores on admission and discharge
from rehabilitation service. In addition, compliance was measured by usage
of ICP monitors. Results: Outcome measures pre-guideline-implementation
(May 2009 – Mar 2011) were compared to post-implementation (April 2011 –
Mar 2014). 71 patients were identified pre-implementation compared with 121
post-implementation. Mortality rate decreased from 32% to 19% (p<0.001).
ICP monitor usage increased by 20.5% (71/209=34% pre vs 121/222=54.5%
post). The WeeFIM discharge scores were improved post-implementation,
though not statistically significant (68.5 vs 56.5, p=0.76). Acute length of stay
(LOS) (median 11 vs 12, p=0.27), ICU LOS (Median 10 vs 10, p=0.31) and
ventilator LOS (median 8 vs 8, p =0.44) were unchanged. Conclusions: A
multidisciplinary effort to develop, educate, monitor and implement a comprehensive severe pediatric TBI guideline program at Children’s was associated
with improved outcomes.
126
GLYCEMIC VARIABILITY WITH TEMPERATURE CHANGES
DURING THERAPEUTIC HYPOTHERMIA AFTER CARDIAC
ARREST
Krystal Haase1, Jennifer Grelle2, Faisal Khasawneh3, Chiamaka Ike4; 1Texas Tech
University Health Sciences Center School of Pharmacy, Amarillo, TX, 2Texas
Tech University Health Sciences Center School of Pharmacy, Abilene, TX, 3Texas
Tech University Health Sciences Center School of Medicine, Amarillo, TX,
4
St. Luke’s Hospital, Houston, TX
Learning Objectives: Therapeutic hypothermia (TH) is recognized as standard
of care for cardiac arrest patients. Despite recognized benefits, TH may cause
physiologic changes including glucose dysregulation and insulin resistance. Variations in glucose control and insulin requirements have been described. However, the magnitude and clinical impact of these differences, particularly during
temperature transitions, is unknown. We hypothesize that meaningful changes
in glycemic control occur during temperature transitions in TH, particularly
during rewarming. Methods: We reviewed all adult patients with sudden cardiac
arrest who completed 24-hr TH and received insulin infusion protocol between
1/1/2010 and 6/30/2013. Hourly glucose and insulin were compared for each
treatment phase (induction, maintenance, rewarm, and post-TH). The primary
endpoint was frequency of glycemic excursions (>180 or <70 mg/dL). Average glucose, insulin dose, and glucose variability (max-min) were also assessed.
Results: Glycemic excursions occurred in 92% of the 26 patients who met
inclusion criteria. Hyperglycemia was most prevalent during induction (88.9%)
and maintenance (73.1%) with significant declines during rewarm (13.6%).
Hypoglycemia was most likely to occur during rewarm (27.3%) compared
with induction (0%), maintenance (7.7%), and post-TH (3.9%). Patients with
hypoglycemia received higher insulin doses prior to rewarm than those without
hypoglycemia (16.2 vs 2.1 units/hr, p=0.032). Mean blood glucose varied significantly across phases (280, 187, 124, 128 mg/dL, p<0.0001) as did mean glucose variability (40, 128, 50, 37, mg/dL, p=0.001). Mean insulin requirements
trended higher during induction and maintenance (8.2, 8.3, 3.9, 1.1 units/hr,
p=0.067). Conclusions: Glycemic excursions are common during TH and are
phase-specific. Higher glucose values and insulin requirements during cooling/
maintenance suggest the presence of temperature-associated insulin resistance
and/or reduced insulin secretion. Hypoglycemia can occur during rewarming
and is most problematic in patients who require higher insulin doses during
maintenance phase.
127
IN-HOSPITAL ARRESTS, ANOXIC/HYPOXIC ISCHEMIC
ENCEPHALOPATHY, AND G TUBE/TRACHEOSTOMY
ESTIMATES.
Veerajalandhar Allareddy1, Sankeerth Rampa2, Romesh Nalliah3, Karen Lidsky4,
Veerasathpurush Allareddy5, Alexandre Rotta1; 1Rainbow Babies & Children’s
Hospital, Cleveland, OH, 2University of Nebraska Medical University, College
of Public Health, Omaha, NE, 3Dental Medicine, Harvard University, Boston,
MA, 4Rainbow Babies & Children’s Hosp., Cleveland, OH, 5College of Dentistry, University of Iowa, Iowa City, IA
Learning Objectives: Current prevalence estimates of placement of gastrostomy
tube(GT) /tracheostomy in patients with anoxic/hypoxic ischemic encephalopathy injury(AHIE) post cardiopulmonary resuscitation(CPR) are unknown. Our
objective is to estimate the prevalence of AHIE in hospitalized patients who had
CPR and to identify patient level factors that predict the performance of GT
+/- tracheostomy in those with AHIE Methods: We performed a retrospective
analysis of the Nationwide Inpatient Sample(years 2004–2010). All patients who
developed AHIE following CPR were included. In this cohort the odds of having
GT and tracheostomy was computed by multivariable logistic regression analysis.
Patient and hospital level factors were the independent variables Results: During
the study period, a total of 686,578 hospitalizations had a CPR event. Of these,
13.7%(N=94,336) had AHIE. In the cohort of patients with AHIE, 6.8% had
GT and 8.3% had tracheostomy. Patients 70yrs old or older comprised 40% of
this cohort. When compared to the 40-49yrs age group, those aged >/=70yrs were
associated with lower odds for GT(OR=0.65, p<0.0001). Those aged <18 yrs &
those>/=60 yrs were associated with lower odds for having tracheostomy when
compared to the 40-49 yrs group(p<0.0001). Each one unit increase in co-morbid burden was associated with higher odds for having GT(OR=1.19,p<0.0001)
or tracheostomy(OR=1.17, p<0.0001). Blacks, Hispanics, Asians/Pacific
Islanders, and Other Races were associated with higher odds for having GT or
tracheostomy when compared to whites(p<0.05). Hospitals located in northeastern regions were associated with higher odds for performing GT(OR=1.48,
p<0.0001) or tracheostomy (OR=1.63, p<0.0001) when compared to those in
Western regions. Teaching hospitals(TH) were associated with higher odds for
performing tracheostomy when compared to non-TH (OR=1.36, p<0.0001)
Conclusions: AHIE injury occurs in a significant number of in-hospital arrests
requiring CPR. Certain predictors of GT/ Tracheostomy placement are identified. Patients in teaching hospitals were more likely to receive tracheostomy than
their counterparts
with worse outcomes in adults. Further study is necessary to delineate pediatric
delirium associated risk factors and outcomes.
129
FAMILY PRESENCE DURING TRACHEAL INTUBATIONS IN
PEDIATRIC ICUS
Ronald Sanders1, G. Bysani2, Margaret Parker3, Sholeen Nett4, Vinay Nadkarni5,
Akira Nishisaki6; 1N/A, Little Rock, AR, 2Pediatric Acute Care Associates of
North Texas, Dallas, TX, 3Stony Brook University, Stony Brook, NY, 4N/A, Lebanon, NH, 5Children’s Hospital of Philadelphia, Philadelphia, PA, 6The Children’s
Hospital Philadelphia, N/A
Learning Objectives: Family presence (FP) during procedures in pediatric ICUs
has been advocated. However, the current practice has not been described in a
large scale. We hypothesized practice of FP during tracheal intubations (TI) vary
across pediatric ICUs, and is associated with severity of patient condition upon
TI and resident participation as an airway provider. Methods:We analyzed data
from a prospective multicenter TI database (National Emergency Airway Registry for Children:NEAR4KIDS) from 7/2010-3/2013. FP was defined as family
member present at the bedside or in a patient room. Patient factors included:
age, PIM2 on admission, shock, acute respiratory failure, elective TI, history of
difficult airway. Provider factors include resident participation as a primary airway provider. We also evaluated the association between FP and occurrence of
adverse TI associated events (TIAEs) while adjusting for patient and provider
factors. Univariate (Fisher’s exact) and multivariate (logistic regression); significance as p< 0.05. Results: 3986 TIs from 21 PICUs were reported. Median age
was 1y (IQR:0-6). Indications were: 58% respiratory failure, 11% hemodynamic
instability, 18% elective procedure. 86% of TIs had data in FP. Overall family
member was present in 19% with wide variability across the sites (0.4-46%).
PIM2 on admission (p<0.001) but no other patient factors were associated with
family presence at TI (all p>0.05). Resident participation was associated with
higher FP (23% in resident participated TI vs. 18% in non-resident participated
TI, p<0.001). FP was not associated with incidence of adverse TIAEs in univariate (p=0.63) and multivariate analysis adjusting for patient and provider factors
(Odds ratio 1.0, 95% CI:0.8-1.3, p=0.89). Conclusions: Wide variability exists
in FP in TIs across PICUs. Surprisingly resident participation was associated with
more FP. FP was not associated with adverse TIAEs.
130
128
PEDIATRIC DELIRIUM PREVALENCE AND MOTORIC SUBTYPES IN CRITICALLY ILL INFANTS AND YOUNG CHILDREN
Christina Goben1, Maalobeeka Gangopadhyay2, Mary Hamilton Chestnut3, Natalie Jacobowski4, Catherine Fuchs5, E. Wesley Ely6, Pratik Pandharipande7, Heidi
Smith1; 1Vanderbilt Children’s Hospital, Nashville, TN, 2Vanderbilt Childrens
Hospital, Nashville, TN, 3Vanderbilt Medical Center, Nashville, TN, 4Vanderbilt
Medical Center, Nashville, TN, 5Vanderbilt University, Nashville, TN, 6Vanderbilt University School of Medicine, Nashville, TN, 7Vanderbilt University Medical Center, Nashville, TN
Learning Objectives: Advances in delirium research among infants and young
children lag behind that in adults due to the lack of valid and developmentally
appropriate delirium monitoring tools. The PreSchool Confusion Assessment
Method for the ICU (psCAM-ICU) is a bedside delirium tool recently validated
against formal neuropsychiatric evaluation, with a sensitivity of 84% and specificity of 91%. The objective of this study was to determine the prevalence and
motoric subtypes of delirium in critically ill infants and children. Methods: We
prospectively enrolled critically ill infants and children aged 6 months to 5 years,
admitted to the pediatric ICU (PICU). This cohort was part of the psCAM-ICU
validation study where enrolled patients were independently assessed for delirium
daily by the research team using the psCAM-ICU and the reference standard,
consisting of formal neuropsychiatric assessment. The motoric subtype was determined by the concurrent sedation score accompanying a positive delirium assessment. Results: A total of 631 psCAM-ICU assessments were performed on 242
critically ill patients with a mean age of 22.6 months, 62% male, 77% Caucasian, and 36% admitted for acute respiratory syndrome. Within the cohort 53%
required mechanical ventilation. The mean PICU length of stay was 12.9 days.
The mortality rate was 4%. Delirium occurred at least once in 100 of 242 (41%)
patients. Rates of delirium were 49% in patients ≤2 years and 31% when >2
years. Of the 187 (30%) positive psCAM-ICU delirium assessments, the hypoactive subtype (81%) was more common than the hyperactive subtype (19%). The
reference standard rated 31% of their assessments as delirium positive, with only
8% of delirium diagnoses related to drug withdrawal. Conclusions: Delirium
is extremely prevalent among critically ill children. The most common presentation is hypoactive delirium, which is concerning as this subtype is associated
POST-RESUSCITATION REDUCTION OF HEPATIC MICROCIRCULATION REFLECTS CARDIAC BUT NOT LIVER
DYSFUNCTION
JIE QIAN1, Shen Zhao1, Jiangang Wang1, PING GONG2, Zhengfei Yang2,
Xiaobo Wu3, Jena Cahoon4, Wanchun Tang1; 1Weil Institute of Critical Care
Medicine, Rancho Mirage, CA, 2Weil institute of critical care medicine, rancho
mirage, CA, 3Weil Institue of Critical Care Medicine, Rancho Mirage, CA, 4the
Weil Institute of Critical Care Medicine, Rancho Mirage, CA
Learning Objectives: Multiple organ dysfunction following successful resuscitation from cardiac arrest is associated with a low survival. Little is known about
the impact of cardiac arrest and resuscitation on the liver. We investigated postresuscitation hepatic microcirculatory changes in a rat model of cardiac arrest and
resuscitation and related those changes to cardiac function and liver function.
We hypothesize that the changes in post-resuscitation hepatic microcirculation
are closely related with cardiac and liver function. Methods: Fifteen SpragueDawley rats (450-550g) were randomized into two groups: 1) CPR group: 8
mins of untreated ventricular fibrillation (VF) followed by 8 mins of CPR and
defibrillation (n=10); 2) sham control: animals underwent the same surgical procedure except that VF and CPR were not performed (n=5). An upper midline
laparotomy was performed to visualize the right lobe of the liver. Hepatic microcirculation was recorded with the sidestream dark field video microscope at three
locations at baseline, 1, 2, 4 and 8 hrs after the return of spontaneous circulation. Myocardial function was measured by echocardiography and serum liver
function Alanine (ALT) and aspartate aminotransferases (AST) was measured by
enzyme-linked immunosorbent assay. Results: Following resuscitation, hepatic
microcirculatory indicators including sinusoidal diameter (BL: 10.9 ± 0.7μm;
PR 8 hrs: 7.7 ± 0.9μm), sinusoidal blood flow velocity (BL: 341 ± 58 μm/s; PR
8 hrs: 88 ± 19 μm/s) and postsinusoidal venular diameter (BL: 37.4 ± 11.7; PR
8 hrs: 25.9 ± 3.2 μm) decreased significantly (all p<0.05 vs. baseline and sham
control). The decreased hepatic microcirculatory blood flow was closely correlated with reduced cardiac output (r=0.891, p<0.01). There were no significant
differences in the values of ALT (BL: 14.5 ± 2.1 U/L, PR 8hrs: 18.2 ± 1.6 U/L;
p>0.05) and AST (BL: 65.6 ± 2.6 U/L, PR 8hrs: 61.4 ± 5.3 U/L; p>0.05) after
resuscitation. Conclusions: The significant reduction of hepatic microcirculation
was correlated with myocardial dysfunction. However, it did not cause severe
liver dysfunction.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Poster Session: Administration 1
131
133
EFFECT OF ENVIRONMENT OF CARE WITHIN PIRO SEPSIS MODEL: IS TELE-HEALTH THE ANSWER FOR HEALTH
POLICY?
CLINICAL PREDICTORS OF RESOURCE UTILIZATION IN
SEVERE PEDIATRIC TRAUMATIC BRAIN INJURY
Donna Armaignac1, Carlos Valle2, Julie Lamoureux2, Louis Gidel2, Xiaorong
Mei2, Emir Veledar2; 1Baptist Health South Florida, Coral Gables, FL, 2Baptist
Health South Florida, Miami, FL
Learning Objectives: To determine the effect Hospital and ICU admission
source on risk of sepsis severity, mortality, and acutely acquired organ dysfunction (AAOD). Methods: Using Tele-health data we created a physiological and
severity adjusted observational cohort obtained at 6 hospitals from 2008 to
2013 (n = 10,232; 5,643 sepsis, 2,321 severe sepsis, 2,268 septic shock. Environmental characteristics were examined as part of PIRO multivariate regression models that included socio-demographic and acute physiologic factors.
Examination of environmental characteristics revealed: on admission, 1,896
were septic (18.5%) (POA) while the rest of the sample acquired this condition
while hospitalized (81.46%) (non-POA). There was a significantly larger proportion of sepsis POA cases (89.2%) compared non-POA (47.4%); severe sepsis POA (1%), non-POA (27.6%); septic shock POA (8%); non POA (25%).
Results: In all prediction models environmental characteristics were highly
significant independent predictors of worse outcomes. 91.11% patient’s point
of origin was the ER; 59.4% went directly to ICU with the lowest mortality
(18%), of the remaining 31.7%, 26% went to ICU by way of the floor with
highest mortality (25%). ICU admissions from floor higher risk sepsis severity (OR 1.19 p<.000); mortality (OR 1.48 p<.000), and AAOD (OR 3.19
p<.000); transfer from other hospital higher risk mortality (OR 1.71 p,.006)
and AAOD (OR 1.70 p=.006); operating room higher risk sepsis severity (OR
1.52 p<.000), lower mortality (OR 0.71 p=.013), but highest risk of AAOD
(OR 4.65 p=.000); and recovery room aligned with OR for lower mortality
(OR 0.51 p=0.001), but higher risk AAOD (OR 2.26 p<.000). Conclusions:
Direct admits to ICU from Surgical and Recovery environments have highest
sepsis severity, lower mortality, but a four-fold increase in AAOD, are least
likely to go home and most likely to go to a skilled nursing facility. Sepsis
acquired during hospitalization is of higher severity with the worst outcomes.
Tele-health, through surveillance, can and may support efforts to prevent floor
patients from descending into ICU.
132
A SURVEY ASSESSING PICU PROVIDERS’ KNOWLEDGE OF
THE COST OF CARE
Venessa Pinto1, Ashly Westrick1, Truc Le1, Amber Greeno1, Chevis Shannon1,
James Leathers2; 1Vanderbilt Univeristy, Nashville, TN, 2Vanderbilt University,
Nashville, TN
Learning Objectives: The purpose of our study was to identify clinical characteristics of pediatric patients with severe traumatic brain injury (TBI) that
were predictive of increased resource utilization. We hypothesized that clinical factors were associated with a utilization surrogate of ICU length of stay
(LOS) and disposition to a rehabilitation facility. Methods: This retrospective
study collected data from the trauma registry at Vanderbilt Children’s Hospital. 1816 patients, aged less than 18 years, underwent management for TBI
between January 2006 and April 2013; 346 had a Glasgow Coma Scale of
8 or less on initial presentation. Descriptive statistics, multivariate and logistic regression were conducted using SAS 9.4. Results: Of the 346 patients in
our cohort, 56% were male and 74% were Caucasian. The mean age was 7.7
years ± 5.58 and mean ICU LOS was 4.73 days (SD 5.68, range 1-46 days).
The main mechanism of injury was motor vehicle collision (MVC) (51%). The
majority of our cohort was transported by helicopter (74%) from the scene
(55%). Factors predictive of longer LOS included seizure medication at discharge (p<0.0001) and mechanism of injury (p=0.0051) with injuries due to
MVC (p=0.0049) and abusive head trauma (AHT) (p=0.0003) significantly
increasing the LOS compared to other mechanisms. Stratifying by those discharged to rehab and those who died, 75 patients (12.6%) were discharged
to rehab and 79 (22%) expired prior to discharge. The mean age for those
discharged to rehab was significantly older than those who died (9.7 ± 5.3 years
vs 5.8 ± 5.5 years, (p<0.0001)). Younger age (P=0.0001), seizure medication at
discharge (p=0.0002) and injury mechanism (p=0.013) were found to be associated with a disposition of death. Injury mechanism (p<0.0001), increasing
age (p<0.0001) and seizure medication at discharge (p<0.0001) were associated with the disposition to rehab. Conclusions: Injury mechanism and the
need for seizure medication at discharge can be predictive of increased resource
utilization. Type of intracranial hemorrhage was not found to be significant for
increased LOS or disposition to rehab.
134
PHYSICIAN ASSISTANT BILLING AND PROCEDURES IN THE
INTENSIVE CARE UNIT
Christopher Horvat1, Ann Thompson2; 1Children’s Hospital of Pittsburgh of
UPMC, Pittsburgh, PA, 2Children’s Hospital of Pittsburgh, Pittsburgh, PA
David Carpenter1, Beth Bush2, Hannah Watson2, Craig Coopersmith3; 1Emory
Critical Care Center, Atlanta, GA, 2AAPA, Washington, DC, 3Emory University
School of Medicine, Atlanta, GA
Learning Objectives: There are increasingly frequent calls for healthcare
cost containment in the United States. In order to optimize rational resource
utilization, it is necessary to first clarify providers’ current knowledge of the
costs and charges of hospital care. By exposing knowledge gaps, educational
interventions and quality improvement initiatives can be implemented to
improve the cost-effectiveness of care delivery. Methods: A 14 question
survey assessing respondents’ knowledge of the charges and costs associated
with common components of care was distributed to physician and nurse
practitioner providers in the PICU and CICU at a major children’s hospital. Accuracy was defined as estimates within +/- 25% of the actual cost or
charge. The use of ethacrynic acid was measured before and after a simple
educational initiative to determine whether ordering habits were influenced
by cost data. Results: Eighty-one percent of eligible subjects participated. In
general, accuracy was low, with only 12.8% of providers accurately estimating
charges and costs associated with diagnostic imaging and laboratory studies.
Charges for the most expensive medications and tests were underestimated
by an average of 81% and 52%, respectively. Twenty-six of 30 respondents
(87%) reported that readily available cost and charge information would
make them more mindful in selecting less-expensive but clinically comparable therapies. Following a simple educational initiative, the number of
ordered doses of ethacrynic acid per patient per day declined by 19% in the
CICU. Conclusions: There is both an opportunity and a willingness among
pediatric intensive care providers’ to improve their knowledge of the costs
and charges associated with routine care in the PICU. Preliminary evidence
indicates that educating providers on the values of clinically comparable but
dramatically cost-discrepant tests and treatments will lead to more rational
resource utilization. Quality improvement initiatives, such as the creation
of a diuretic selection algorithm, will help guide providers in making more
cost-effective decisions.
Learning Objectives: Physicians assistants are employed by both hospital based
and specialty critical care practices. However, there is little data on their billing
and procedural practices in the ICU. Methods: Utilizing the American Academy
of Physician Assistant census, an 11 question survey was added for all PAs that
identified their primary workplace as the ICU. Additional data was collected by
sending the AAPA survey to all members of the SCCM PA section. SCCM data
was combined with AAPA data using national certification numbers to avoid
duplication. Results:302 surveys were returned. 69% of PAs surveyed bill for
their services, 51% bill for critical care (CCM), 51% bill for evaluation and
management (E/M), and 59% bill for procedures. The majority of ICU PAs are
employed in four areas, single specialty physician group (SS, N=29), multispecialty physician group (MS, N=28), community hospitals (CO, N=125), and
university hospitals (UN, N=90). MS PAs are most likely to bill with 61% billing
CCM, 71% E/M and 75% Proc. Compared to MS PAs, CO and UN PAs are less
likely to bill for CCM 50% (p=0.0008), 43% (p=0.004), E/M 49% (p=0.003)
42% (p=0.013), and procedures 59% (p=0.08), 53% (p=0.035). SS PAs are also
more likely to bill for CCM (62%), E/M (66%), Proc (59%) than CO and UN
CCM (p=0.0009, 0.005), E/M (p=0.003, 0.14) and Proc (p=0.008, 0.04). There
is no statistical difference between MS and UN PAs. CO PAs are more likely to
bill for CCM than UN PAs (p=0.03) but are otherwise similar. For CCM PAs
performing procedures, arterial line is the most common (76%) then CVL (74%)
and Intubation (54%). CO or UN PAs are more likely to perform Intubation
(58% and 66%) than SS or MS (39% and 38%) with the difference between
CO and MS or SS rising to statistical significance (p=0.017, 0.018). Conclusions: 1/3 of CCM PAs do not bill for their services. There is further discordance
between billing and procedures done, hospital PAs doing more procedures but
billing less than specialty PAs. There also exist significant differences between
procedures done by employer type reflecting the patient population and how
PAs are utilized.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
135
DEMAND FORECAST AND OPTIMAL PLANNING OF ICU
BEDS: A CASE STUDY IN RIO DE JANEIRO (RJ)
Rosane Goldwasser1, Edilson Arruda2, Maria Lobo3, Simone Angelo2; 1Hospital
Univerrsitário Clementino Fraga Filho. Federal University of Rio De Janeiro, Rio
de Janeiro, RJ, 2Industrial Engineering Program, Alberto Luiz Coimbra Institute
- Graduate School, Rio de Janeiro, Brazil, 3Hospital Universitario Clementino
Fraga Filho. Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
Learning Objectives: ICU beds (ICUb) overcrowding results in delay for healthcare,
long waits and higher mortality. There is an entry flow obstruction when the number
of patients requiring ICU is greater than beds available. Determining the optimal
number of ICUb is essential due to both the expensive cost and the increasing demand
for them. We strive to find the optimal number of ICUb for RJ. In order to tackle
the problem, we make use of time series of a Queuing model. Methods:The authors
collected a series of daily requests for ICU admissions and outcomes, from 2010 to
2011. According to the information extracted from the Rio’s Regulation database,
they employed time series theory to forecast future demand rates. The novelty is that
the model predicts the input rate of a queuing model which takes into account the
stochastic variations during the actual operation of the system.The output rate was
obtained from the DATASUS 2013. For carrying out all predictions they used the
statistical software R Development Core Team, 2012. To estimate number of beds
they compared total requests X longer and shorter lengths of stay (LOS). For each scenario the optimal number of ICUb was predicted for a prescribed maximum waiting
time in such a way that only a prescribed percentage 0<p Results: There were 33.101
requests. For 1 year prediction the number of daily requests was 52.7 and the average interval between requests was 0.45 hours and λ = 2.19 patients/ hour. When the
average LOS was 11.2 days then μ = 0.004 patients/ hour. We calculated 594 ICUb
for the system to be stable.When the average LOS 6.4 days then μ= 0.006 patients/
hour. The number of ICUb for system to be stable was 342. Conclusions:Queuing
theory provides an accurate means of determining the appropriate supply of ICU
beds. Shorting LOS, one can reduce the number of necessary ICUb, keeping the
waiting time small. As expected, a lower violation requires a higher number of ICU
beds, and the decision is taken at the managerial level.</p
136
LESSONS LEARNED IN THE EVOLUTION OF PEDIATRIC CRITICAL CARE: APPLICABILITY IN DEVELOPING COUNTRIES
Toah Nkromah1, Robert Tamburro2, NJ Thomas3; 1Penn State Hershey Medical
Center, Hershey, PA, 2Penn State Childrens Hospital, Hershey, PA, 3Penn State
Children’s Hospital, Hershey, PA
Learning Objectives: Over the years, Pediatric Critical Care Medicine(PCCM)
has grown significantly in the role it plays treating and saving lives of critically ill or
injured children. In many developing countries(DCs), PCCM is either non-existent or in a nascent state. The experiences of US practitioners can potentially benefit
the development of PCCM in DCs. To date, there are few published manuscripts
to guide PCCM development worldwide. This study sought to explore insights and
perspectives of experienced PCCM providers in the US and consider the applicability of lessons learned, in the design and implementation of PCCM in DCs. We
hypothesized that we could identify common themes based on those perspectives
that may be used to formulate recommendations for DCs. Methods: An exploratory qualitative approach was used. Semi-structured face-to-face interviews were
performed lasting 39-58 minutes to highlight perspectives and insights of PCCM
providers with over 20 years experience. Purposive sampling was used to recruit participants in the Mid/South-Atlantic regions, though cumulatively they had experience throughout the US and 22 other countries. Of 24 recruited participants, 12
consented and were enrolled: 7 males, 5 females; 9 physicians, 3 nurses. All participants were actively practicing at the time of the interview, with duration of practice
24-37 years. Results: Three prominent themes emerged from qualitative analysis:
1) development of PCCM in the US is influenced by society, notably economic and
human resources; 2) advancements of biomedicine and technology drive change
but lead to ethical quandaries; and 3) changes have generated significant impacts
on patients, families and practitioners. Conclusions: PCCM development in the
US has spawned challenges and dilemmas. Based on themes that emerged, the following recommendations can support and inform the advancement of PCCM in
DCs: 1) document and establish resources and cost/benefit of PCCM; 2) anticipate
potential ethical issues in applying technology and PCCM practices; 3) contemplate utility of lessons learned and how they may be distinct and/or adapted.
137
HOSPITAL COSTS ASSOCIATED WITH SIGNIFICANT PEDIATRIC BRAIN INJURIES
Alexandra Schaller1, Saquib Lakhani1, Benson Hsu1; 1Sanford School of Medicine, University of South Dakota, Sioux Falls, SD
Learning Objectives: Previous studies have shown that pediatric patients with
traumatic brain injury incur more than $1 billion annually in total hospital
charges. However, no studies have examined either the cost of care, in contrast
to charges, or the impact of severity of illness to cost. This study aims to fill
this gap by examining costs associated with significant head trauma within the
pediatric population. Methods: We conducted a retrospective study of hospitalized children with a diagnosis of significant head trauma using the Agency for
Healthcare Research and Quality 2009 Kids’ Inpatient Database. Diagnosis of
significant head trauma was based on an All Patient Refined Diagnosis-Related
Groups (APR-DRG) of 055: “Head trauma with coma greater than 1 hour or
hemorrhage.” APR-DRG validated severity classes segmented severity of illness
into four levels. Cost to charge ratios were applied for analysis. Weighted statistical analysis utilized STATA 11.2. Results: Our weighted sample of 11,156 pediatric patients with significant head trauma had a mean age of 9.4 and was 32.3%
female. Mean total hospital costs per discharge were $8,758.10 with mean daily
costs of $3,314.66. Total hospital costs increased from lower to higher severity
levels ($5,015.81, $8,255.43, $15,840.52, $33,572.91) with similar trends seen
in daily costs ($2,891.55, $3,232.37, $4,325.58, $5,827.86). Within the highest
severity level, total hospital costs were $43,790.90 for survivors versus $19,842.93
for non-survivors. Comparatively, daily costs were $3,301.84 for survivors versus
$10,197.53 for non-survivors. Conclusions: Significant head trauma incurred
hospital costs of almost $100 million in 2009. Our study found that severity of
illness had a positive relationship to overall and daily hospital costs. Interestingly,
non-survivors within the highest severity level had higher daily costs but lower
total costs, suggesting a short term, high resource utilization need of those who
died. While this study examined only a subpopulation of traumatic brain injury,
it begins to characterize the relationship of severity of illness to costs.
138
FREQUENT FLYERS TO AN ONCOLOGIC ICU: CHARACTERISTICS AND OUTCOMES
Anil Singh1, Sanjay Chawla2, Stephen Pastores1, Natalie Kostelecky3, Gleb Kirnicinii3, Neil Halpern1; 1Memorial Sloan-Kettering Cancer Center, New York, NY,
2
Memorial Sloan Kettering Cancer Center - Anesthesia & CCM, New York, NY,
3
Memorial Sloan Kettering Cancer Center, new york, NY
Learning Objectives: The association between ICU readmissions in a single hospitalization and poor outcomes is well described. Cancer patients commonly require
several hospital admissions either for defined oncologic therapies or to manage
complications of treatment. The characteristics and outcomes of cancer patients
who are repeatedly admitted to the ICU during repeat hospitalizations have not
been previously reported. Methods: Using hospital and ICU databases, we identified patients who had ≥3 ICU admissions during unique hospitalizations from
January 2008 to December 2013 to an oncologic med/surg ICU at a tertiary cancer
center. We excluded patients who had an ICU readmission during any single hospitalization. Demographic, clinical and outcome variables were analyzed. Data are
presented as numbers (%) and mean (±SD). Results:Over the study period, there
were 5,673 ICU admissions; 4,617 were unique admissions. 173 patients had multiple ICU admissions; of these, 62 had ≥3 ICU admissions during unique hospitalizations and comprised the study group. The mean age on first ICU admission was
54 (±14.9) years and half were males. On average, ICU admissions occurred over
12 (±8.9) months. Three ICU admissions occurred in 81% of cases, 4 admissions
in 14% and 5 or more admissions in 5% of cases. 43% of patients had hematologic
malignancies and/or underwent hematopoietic stem cell transplantation (HSCT),
and constituted the predominant group. Pneumonia (22%) and septic shock from
an abdominal source (10%) were the main ICU diagnoses. The majority (83%) had
different diagnoses on each ICU admission. The mean ICU length of stay (LOS)
was 6 days (±6) and hospital LOS was 17.0 days (±15.9). ICU mortality was 37%
and hospital mortality was 55%. Overall ICU mortality for all admissions during
the study period was 17% and total hospital mortality of 35%. Conclusions: Cancer patients who require repeated ICU admissions during multiple hospitalizations
predominantly have hematologic malignancy or are HSCT recipients and have
high ICU and hospital mortality rates.
139
PHYSICIAN ASSISTANT DEMOGRAPHICS IN THE INTENSIVE CARE UNIT
David Carpenter1, Beth Bush2, Hannah Watson2, Craig Coopersmith3; 1Emory
Critical Care Center, Atlanta, GA, 2AAPA, Washington, DC, 3Emory University
School of Medicine, Atlanta, GA
Learning Objectives: With the shortage of intensivists and the decrease in resident hours many ICUs are turning to physician assistants (PA) to staff ICUs,
however; there is little demographic data on PAs who work in the ICU. Methods: Utilizing the American Academy of Physician Assistant (AAPA) census, an
11 question survey was added for all PAs that identified their primary workplace
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
as the ICU. Additional data was collected by sending the AAPA survey to all
members of the SCCM PA section. SCCM data was combined with AAPA data
with national certification numbers used to avoid duplication. CCM PA data was
compared with the AAPA non-CCM PA population. Results: 302 surveys were
returned. The CCM PA population was younger (36.4 vs 40.8 years p<0.0001),
less experienced (8.5 vs 10.7 years p<0.0001) and had less years in specialty (6.4
vs 7.7 years p=0.0005). 90% of work in one of four environments (University
Hospital, Community Hospital, Single Specialty Physician Group, and MultiSpecialty Physician Group) in contrast to 65% of the general PA population
(p<0.0001). Medical ICUs (21%), Surgical ICUs (20%) and CV Surgery ICUs
(14%) are the most common environment. Neonatal ICUs (11%), Neuro ICUs
(10%), Pediatric ICUs (9%), and Cardiac ICUs (9%) employ most of the rest.
Multi-specialty ICUs (7%) and Trauma (1%) employ the least PAs. Cardiac and
Cardiovascular PAs have the most general (10.9 and 9.4 years) and specialty experience (10.5 and 9.0) years. Multi-specialty, Surgical, and Medical ICU PAs have
8.7, 7.8, and 7.1 years of general experience with 5.8, 5.1, and 4.6 years of specialty experience. Neuro and Trauma ICU PAs have the least experience with 6.7
and 4.7 years of general experience with 4.6 and 4.7 years of specialty experience.
Conclusions:Overall, the average CCM PA is younger; less experienced, has less
specialty experience and is more likely to work for a hospital or physician specialty group than the general PA population. Most PAs work in Surgical, Medical
or CV Surgery ICUs. Given the increasing use of CCM PAs understanding the
ICU PA demographics will help organizations plan for additional PAs.
140
THE IMPACT OF A HOME HEALTH, NURSE-DRIVEN
TELEMONITORING PROGRAM ON HEART FAILURE
READMISSIONS
Daleen Penoyer1, Steven Talbert2, Brenda Randall1, Laura Wright-Winterstine1;
1
Orlando Health, Orlando, FL, 2University of Central Florida, Orlando, FL
Learning Objectives: Hospital readmissions for patients with heart failure (HF) are
common and costly, with reduced reimbursement for those within 30 days of D/C.
Telemonitoring (TM) for HF patients after discharge has been met with mixed success, with national readmission rates of about 25%. The organization has a dedicated
TM program in the Home Health (HH) division to facilitate HF self-care and early
recognition of complications. The purpose of this study was to evaluate the impact
of the TM HH program on 30-day readmissions of HF patients. The hypothesis for
the study was that patients with HH augmented with TM would have fewer readmissions than those who have HH alone. Methods: The study used a retrospective,
descriptive cohort analysis design using data from the hospital databases. Discharged
HF patients referred to HH and TM from 1/1/08-12/31/11 were included. Patients
referred who had HH, but opted out of TM served as a cohort control group for
comparison. The TM program was run by specific HH nurses, with daily electronic
transmission of vital signs & weight, calls to patients and primary care physician if
values were outside established parameters. Results: Over the 4 year period, 491
patients met inclusion; 357 in the TM (73%), 134 in the control group. The TM
group was significantly older (74 vs 71 yrs; p=0.05) and more females (p=0.025). No
difference was found between the number of HH visits between the groups (p=0.49)
In total, 94 (19.1%) patients were readmitted for all causes within 30 days; 8 of
those (1.6%) readmitted twice. In the TM group, 63 (17.6%) were readmitted vs 31
(23.1%) in the control group. Chi-Square analysis did not show a significant statistical difference in readmissions between the groups (p=0.169). Conclusions: Findings
showed that patients with HF who participated in HH coupled with TM had fewer
30-day readmissions than those with HH alone. While no statistical difference was
found in readmissions between groups, 5.5% lower readmissions in the TM group
is clinically significant. Patients in this study may be sicker than general HF patients,
so TM may be useful for HH HF care.
141
EFFECT OF DELIRIUM MOTORIC SUBTYPES ON ICD-9
DOCUMENTATION OF DELIRIUM IN THE INTENSIVE CARE
UNIT
Lan Bui1,2, Vy Pham3, Joshua Swan2,4,5; 1Texas Southern University College of Pharmacy and Health Sciences, Houston, TX, 2Houston Methodist Hospital, Houston,
TX, 3Memorial Hermann Northwest Hospital, Houston, TX, 4Texas Southern
University, Houston, TX, 5Houston Methodist Research Institute, Houston, TX
Learning Objectives: Studies have attempted to quantify delirium prevalence
using International Classification of Diseases-Ninth Revision (ICD-9) administrative codes. We hypothesized that surgical intensive care unit (SICU) patients
with hyperactive/mixed delirium (HYPER/MIX) vs. hypoactive delirium
(HYPO) would be more likely to receive ICD-9 documentation for delirium.
This study’s purpose was to report the proportions of patients with HYPER/
MIX vs. HYPO that received delirium ICD-9 documentation. Methods: This
retrospective cohort study was conducted at a 24-bed SICU from 06/01/2012 to
05/31/2013. Adult patients with less than 24 hours SICU care, were at another
ICU, or not screened with the Confusion Assessment Method for the ICU
(CAM-ICU) were excluded. Delirium was assessed twice daily and was defined
as one or more positive CAM-ICU ratings during SICU stay. Delirious patients
were categorized into three motoric subtypes using corresponding Richmond
Agitation Sedation Scores (RASS), where all RASS of 1 to 4 was HYPER, all
RASS -3 to 0 was HYPO, and the presence of RASS that were both 1 to 4 and
-3 to 0 was MIX. We identified 26 unique ICD-9 codes used in previous studies; documentation of delirium was defined as having ≥1 of these 26 codes not
present on admission. Proportions were compared with the Chi-squared test.
Results: Of included patients, 40% (423/1055) were diagnosed with delirium
and 17% (182/1055) had an ICD-9 code for delirium. The sensitivity, specificity,
positive and negative predictive values, and diagnostic accuracy of ICD-9 codes
for delirium were 36%, 95%, 83%, 69% and 71%, respectively. Patients with
HYPER/MIX were 50% more likely to receive ICD-9 documentation compared
with HYPO (42% [95% CI 35-48; 105/253] HYPER/MIX vs. 27% [95% CI
21-34; 46/170] HYPO, relative risk = 1.5 [1.1- 2.2], P=0.002). Conclusions:
Administrative codes had a poor sensitivity for documenting delirium in SICU
patients. Patients with HYPER/MIX were 50% more likely to receive an ICD-9
code for delirium compared with HYPO. Oversampling HYPER/MIX may bias
studies that use ICD-9 codes to quantify delirium prevalence.
Poster Session: Administration 2
142
CRITICAL CARE CAPACITY IN LOW-INCOME COUNTRIES: A
SYSTEMATIC REVIEW
Aleksandra Leligdowicz1, Srinivas Murthy2, Neill Adhikari3; 1University of
Toronto, Toronto, ON, 2University of British Columbia, Vancouver, BC, 3Sunnybrook Health Sciences Center, Toronto, ON
Learning Objectives: In low-income countries, the burden of critical illness is substantial, but the capacity to provide care for critically ill patients in intensive care units
(ICUs) is unknown. We systematically reviewed the published literature to estimate
the current ICU capacity of hospitals in low-income countries. Methods: Eleven
databases were searched and included studies of any design, published 2004-2013,
with data on ICU capacity for pediatric and adult patients in 36 low-income countries (defined by World Bank criteria; population 850 million). Neonatal, temporary,
and military ICUs were excluded. We extracted data on ICU bed numbers, capacity
for mechanical ventilation, and information about the hospital (referral population
size, public accessibility, source of funding). Two reviewers independently searched
for relevant articles and extracted data from included studies; a third reviewer resolved
disagreements. Analyses were descriptive, with continuous data summarized as mean
(standard deviation, SD) or median (interquartile range, IQR) and categorical data
as number (percent). Results: Of 1,759 citations, 43 studies from 15 low-income
countries met inclusion criteria. They described 36 individual ICUs in 31 cities, of
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
which 16 had population greater than 500,000 and 14 were capital cities. The median
annual ICU admission rate was 401 (IQR 234-711, 24 ICUs with data) and median
ICU size was 8 beds (IQR 5-10, 32 ICUs with data). The mean ratio of adult and
pediatric ICU beds to hospital beds was 1.5% (SD 0.9%; 15 hospitals with data).
Nepal and Uganda, the only countries with national ICU bed data, had 16.7 and 1.0
ICU beds per million population respectively. Despite exhaustive search strategies,
capturing national data in other countries was not possible due to the lack of relevant
publications. Conclusions: Low-income countries lack ICU beds, most ICUs are
located in large referral hospitals in major cities, and more than 50% of these countries lack published data on ICU capacity. A central database of ICU resources may
help evaluate health system access and develop related health policy.
143
CURRENT PRACTICE OF MECHANICALLY VENTILATED
PATIENTS TREATED OUTSIDE THE ICU IN JAPAN
Yoshiaki Iwashita1, Kazuto Yamashita2, Masamitsu Sanui3, Hiroshi Imai1, Yuichi
Imanaka2; 1Mie University Hospital, Tsu, Japan, 2Kyoto University, Kyoto, Japan,
3
Saitama Medical Center, Jichi Medical University, Saitama, Japan
Learning Objectives: Mechanically ventilated patients are generally treated
in the ICU in USA. In Japan, because of the shortage of the ICU beds, not
all the mechanically ventilated patients are treated in the ICU. However, the
epidemiological data of the patients who were treated outside the ICU has not
been reported. The aim of this study was to clarify the epidemiological data of
mechanically ventilated patients who were treated outside the ICU. Methods:
The data source was derived from the Quality Indicator/Improvement Project,
which is a voluntary data administration project from more than 300 acute care
hospitals in Japan. Data of mechanically ventilated patients treated in or outside
the ICU from Apr 2010 to Mar 2012 were analyzed. Data of adult patients who
were ventilated for more than 3 days was analyzed. Patients whose diagnosis was
related to cancer were excluded. Patients’ demographic data and the rate of standard critical care provided were compared. Results: In the study period, 17,775
mechanically ventilated patients were treated only outside the ICU (non-ICU
group) while 20,516 patients were treated once in the ICU (ICU group) (46.4%
vs 53.6%). The average age was higher in non-ICU group patients than ICU
group patients (72.8 vs 70.2, p<0.001). The mean ventilation days were longer
in non-ICU group patients than in ICU group patients (11.7 vs 9.5, p<0.001).
Hospital mortality was higher in non-ICU group patients than in ICU group
patients (41.4% vs 38.8%, p<0.001). Standard critical care, such as arterial line
placement, enteral nutrition and stress ulcer prevention, were provided significantly less often in non-ICU group. Conclusions: We have described the current
practices of the mechanically ventilated patients in Japan. Patients treated in the
ICU have a better survival with a higher rate of critical care compared to those
treated outside the ICU.
144
LESSONS LEARNED FROM A PICU SURGE CAPACITY EXERCISE IN A NEW YORK CITY CHILDREN’S HOSPITAL
Erika Mark1, Nora Caplan2, Donell Harvin2, Michael Moculski3, Lewis Singer4,
Henry Ushay1; 1Children’s Hospital At Montefiore, Bronx, NY, 2New York City
Pediatric Disaster Coalition, New York, NY, 3Montefiore Medical Center, Bronx,
NY, 4The Children’s Hospital At Montefiore, Bronx, NY
Learning Objectives: A full scale exercise (FSE) sponsored by the NYC Pediatric
Disaster Coalition (PDC) and incorporating scenario-driven, operations-based
activities was held to assess our Pediatric ICU’s surge plan. Methods: An introductory seminar, a table top exercise (TTX), a TTX after action (AA) meeting,
the FSE, a hot wash and a FSE AA meeting were organized by a planning team
over a span of 7 months. The PICU surge plan was revised and integrated into
the hospital comprehensive emergency management plan (CEMP). Results: 48
staff members signed in but many more participated in the FSE. The census of
the 26 bed PICU was set at 22 (85%). Upon notification of the imminent arrival
of 10 patients, a triage area was established. Surge space was operationalized
in the PACU and on an inpatient unit with monitoring and utilities adequate
to support mechanical ventilation. Mannequins with written scenarios arrived
by EMS. Realistic complications (extubation, vasoactive drips stopping, chest
tube mishaps and EVD malfunction) were incorporated. Additional stress was
imposed by increasing the number of arriving patients from 10 to 15. Two real
emergency PICU admissions occurred during the FSE. In less than 2 hours, 15
critically ill children were triaged and admitted to the PICU or surge spaces.
Conclusions:Identified strengths included knowledge of the surge plan, rapid
establishment of triage and surge spaces, teamwork, engagement, identification
and transfer of patients and mobilization of staff. Almost all aspects of communication needed improvement. FSE notification through electronic and overhead
paging systems did not work. The HCC couldn’t receive faxed status reports. The
triage area had poor cell phone coverage and the nearest landline was 15 feet away.
Frustrations arose when the HCC dictated bed decisions to the PICU. A tie line
system was difficult to use. Planning the FSE allowed us to refine a surge plan and
build interdisciplinary teams. The FSE tested our plan under realistic conditions.
Communication was the area in need of most improvement.
145
A COMMUNITY HOSPITAL TELEMEDICINE PROGRAMINCREASING UTILIZATION OVER A 4 YEAR PERIOD
Phillip Ludwig1, J Marcus2, B Ludwig2, M Marquez2, K Ramos3, R Lewis2;
1
NuVIEW Health, Boca Raton, FL, 2NuVIEW Health, Boca Raton, FL,
3
NuVIEW Health, B, FL
Learning Objectives: ICU telemedicine has proven to be a useful modality to
improve access to Intensivist directed care. Previous experience has shown that
implementation is not uniform. This study details increasing telemedicine utilization during a 4 year period and outlines program structural changes that
improved utilization. Methods: The study hospital has a 16 bed medical surgical
ICU. It is staffed by a 12 hour day Intensivist program with telemedicine coverage at night. There is a mandatory intensivist consult for all admissions. The
telemedicine system utilizes a portable cart that allows visualization of the patient
and connectivity to the EMR and PACS systems. Patients seen by telemedicine
are managed by direct communication and by order entry into the CPOE system.
Data was collected for a four year period. At the beginning of year 4 program
structural changes were put in place. Results: During the intial 3 year period
studied there were a total of 297 new patient seen by the teleintensivist. This
increased to 265 in year 4, a 265% increase (p<.01). At the beginning of year
4 several structural changes were made to increase utilization and compliance
with a mandatory consultation on admission to the ICU of new patients. The
following initiative was put in place: 1. A mandatory evening MDR rounds with
the ICU charge nurse with “walk rounds” on all critical patients. 2. Immediate
activation of the teleintensivist once the decision for ICU admission was made. 3.
Case review daily by program medical director and review with physicians, nursing and administration. The common diagnoses were respiratory 31% of cases in
the first 3 years, 39% in year 4. In years 1-3 sepsis 13%, cardiac 12%, neuro 11%.
In year 4 neuro 26%, GI 11%, sepsis 8%. ICU LOS during the study was 4.6
days not significantly different from all ICU admissions (4.4). ICU mortality was
8.8% for the study period vs. 8.4% for all ICU admissions. Conclusions: The
use of telemedicine in critically ill patients improves outcomes. An improvement
in utilization can occur if a strong structural process is put in place to manage
ICU admissions.
146
COMPARISON OF PROVIDER TYPES WHO PERFORMED
PREHOSPITAL LIFESAVING INTERVENTIONS: A PROSPECTIVE STUDY
Vikhyat Bebarta1; 1San Antonio Military Medical Center/ US Army ISR, San
Antonio, TX
Learning Objectives: Life Saving interventions (LSIs) are important procedures
that reduce morbidity. In the combat theater, providers with different levels of
training now operate in the prehospital setting. Our objective was to describe
prehospital LSIs performed, performed incorrectly, and missed (procedures not
performed, but were indicated) by provider type to facilitate future practice
guidelines. Methods: We prospectively recorded LSIs performed on patients
transported to 6 combat hospitals. Trained site investigators evaluated patients
on arrival and recorded demographics, vital signs, LSIs performed, if the LSI
was performed correctly, and if the LSI was missed. LSIs included airway, thoracic, extremity, vascular access procedures, and resuscitation techniques. From
a larger dataset, we analyzed which provider type was recorded. Provider types
were Medic (emergency medical technician); Advanced Medic (Pararescueman/
Special Ops/IDMT); Doctor/Nurse; or Other. Incidence and proportions were
compared with chi-square or fisher’s exact tests. A p<0.05 was considered significant. Results: 529 LSIs were performed on 170 patients. 49% of LSIs were performed by Medics, 19% Advanced Medics, 11% Doctor/Nurses, and 21% Other
(p=0.008). Of complex LSIs, Medics performed 43% of intubations, 33% of
cricothyrotomies, 33% of blood infusions, and 60% of chest needles. Advanced
medics performed 14% of intubations, 33% of cricothyrotomies, 11% of blood
infusions, and 20% of chest needles. Doctor/Nurses performed 14% of intubations, 28% of blood administrations, and no cricothyrotomies or chest needles.
Doctors/nurses performed 50% (5/10) of chest seals, p<0.0001. Fluid infusion
was performed more by medics (70%, p<0.0001) as was hypothermia prevention
(58%, p=0.04). 3.4% of LSIs were incorrectly performed. 3% of the LSIs were
missed. LSIs performed incorrectly or missed was not different among provider
types. Conclusions: In a combat prehospital setting, 50% of LSIs are not performed by medics. Combat medics did perform complex LSIs. Missed LSIs and
incorrectly performed LSIs were rare and similar among provider types.
147
OPTIMAL THRESHOLDS FOR A PICU VENTILATOR ALLOCATION ALGORITHM IN A PANDEMIC
Philip Toltzis1, Christine Gall2, Robert Kanter3, Alexander Kolker4, Randall Wetzel5; 1Rainbow Babies & Children’s Hosp., Cleveland, OH, 2VPS, LLC, Milwaukee, WI, 3Virginia Tech Carilion School of Medicine, Roanoke, VA, 4API
Healthcare / GE Healthcare, Hartford, WI, 5Children’s Hospital of Los Angeles,
Los Angeles, CA
Learning Objectives: A global pandemic may overwhelm ICU capacity, activating crisis standards of care (CSC) in which scarce resources will be diverted from
selected patients to ensure maximum population survival. CSC ICU resourceallocation algorithms (ALGs) exist for adults. Our goal was to evaluate a CSC
pandemic ALG for children. Methods: 150,000 records were obtained from the
Virtual PICU Systems database, from which prediction equations for probability
of death (POD) and duration of ventilation (DOV) were derived (SCCM Congress 2014, Abst 602). We estimated pandemic ICU activity by proportionally
assigning peak weekly deaths caused by the 1918 influenza pandemic, using projected numbers in Ohio as an example. PICU capacity was taken as the number
of surge beds in Ohio PICUs. Discrete Event Simulation (DES) was used to
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
determine ALG thresholds of POD and DOV that would maximize PICU occupancy and patient survival. DES was employed further to estimate total population survival, which then was compared to survival using a random-allocation
first-come, first-served (FCFS) strategy. Results: We assumed that in CSC (i)
only children requiring ventilation would be considered for ICU entry; (ii) optimal PICU use would require assessment of both POD and predicted DOV at
presentation; (iii) all children denied ICU entry would die. For a 6 week period of
CSC with an Ohio pediatric volume 7000, DES determined optimal PICU entry
thresholds of POD < 39% and DOV < 4.1 days. ALG performance compared
with FCFS was as follows: proportion gaining PICU entry 69.1% ALG vs 63.9%
FCFC; survival among children gaining PICU entry 95.1% ALG vs 91.1%
FCFS; total survival in the population 4788 ALG vs 4240 FCFS. Simulation
using optimal POD/DOV thresholds for patient volumes ranging 5000-10000
all demonstrated superior survival compared with FCFS: 10-24% improvement
(all P < .01), with survival advantage increasing with patient volume. Conclusions: The pediatric CSC ALG, the first based on actual clinical data, consistently
improved population survival compared with FCFS by favoring children with
low POD and limited ventilator use.
148
INTERHOSPITAL TRANSFER OF CHILDREN IN RESPIRATORY FAILURE: A CLINICIAN INTERVIEW QUALITATIVE
STUDY
Fola Odetola1, Renee Anspach2; 1University of Michigan, Ann Arbor, MI,
2
­University of Michigan, Ann Arbor, United States
Learning Objectives: Of all sources of admission to Level I PICU care, interhospital transfer admissions from Level II PICUs carry the highest mortality burden. The decision-making underlying transfer from Level II to Level I PICUs is
poorly understood. Objective: To determine factors that influence the decision to
transfer by Level II PICU physicians when managing pediatric respiratory failure. Methods: In-person semi-structured interviews with attending physicians
at Level II PICUs in Michigan and Northwest Ohio. A hypothetical scenario
of a 2 year old girl with influenza, in respiratory failure, at 3 time points, was
presented: -Baseline: Mechanical ventilation with Rate of 25, Peak inspiratory
pressure 28, Positive end-expiratory pressure 8, fraction of inspired oxygen concentration 100%, PaO2 140. Central venous and peripheral arterial catheters are
inserted. - Escalation point #1: After 8 hours, now on higher ventilator settings
with mean airway pressure 19, and oxygenation index 32, PaO2 59. -Escalation point #2: Mean airway pressure 26, oxygenation index 40. Results: 19 of
20 eligible physicians completed interviews. Indices that raised concern for poor
response to therapy included elevated oxygenation index(11), high inflation pressure(6), high FIO2(5), and low P/F(4). At escalation point #1, 70% (12/17)
of the respondents felt the patient had <50% probability of clinical turnaround
without escalating treatment, and would initiate high frequency oscillatory ventilation–HFOV (17) or inhaled nitric oxide therapy (2). Four respondents will call
for transfer, though 2 of them would initiate HFOV first. At escalation point #2,
12 (63%) respondents would continue HFOV, 4 of whom would then transfer,
while 5 others would transfer immediately. All respondents would call for transfer for extracorporeal membrane oxygenation if the escalated therapies failed to
reverse the patient’s clinical deterioration. Conclusions: Transfer of critically ill
children with respiratory failure is triggered by failure of response to escalation of
locally available intensive care modalities.
149
INTERHOSPITAL TRANSFER OF CHILDREN IN SEPTIC
SHOCK: A CLINICIAN INTERVIEW QUALITATIVE STUDY
Fola Odetola1, Renee Anspach2, clark Sarah3, Yong Han4; 1University of Michigan, Ann Arbor, MI, 2University of Michigan, Ann Arbor, United States, 3University of Michigan, Ann arbor, United States, 4N/A, Kansas City, MO
Learning Objectives: Inter-hospital transfer admissions of children with septic
shock from Level II to Level I PICUs have high mortality burden. However, the
decision-making underlying these transfers is poorly understood. Objective: To
determine factors influencing the decision to transfer by Level II PICU physicians when managing pediatric septic shock. Methods: Methods: In-person
semi-structured interviews were conducted with attending physicians at Level II
PICUs in Michigan and NW Ohio. A hypothetical scenario involving a 14 year
old boy in septic shock, at two time points, was presented: - Baseline: 40 mL/kg
fluid resuscitation, central venous and peripheral arterial access, and high-dose
vasopressor infusions have been provided; - Escalation point: Patient is oliguric, in catecholamine-resistant shock, and on invasive mechanical ventilation.
Results: 19 of 20 eligible physicians completed interviews. Indices that raised
concern for poor response to therapy included low blood pressure (11), elevated
lactate (9), low urine output (8), and low central venous saturation (6). At the
escalation point, 7 (37%) respondents would have given more fluid, while 8
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
(42%) would have used central venous pressure to guide additional fluid resuscitation. While 13 of 18 respondents felt there was < 50% probability of clinical
turnaround without escalating treatment, only 4 (21%) would call for transfer.
Rather, transfer decision-making was conditioned on poor response to additional
varying adjunctive therapies, including vasopressin infusion [yes (11), maybe
(3), no (3)]; and steroids [yes (12), maybe (1), no (1)]. Ultimately, 15 (79%) of
the respondents would have requested transfer for either extracorporeal membrane oxygenation or continuous renal replacement therapy only if there was no
response to escalated therapies over time. Four respondents would not transfer
the patient for various reasons. Conclusions: Decision-making regarding transfer
of critically ill children with septic shock from Level II to Level I PICUs is conditioned on poor response to escalated, locally-available intensive care therapies.
150
STRESS ULCER PROPHYLAXIS PROTOCOL COMPLIANCE IN
A MICU MANAGED BY ACNPS VERSUS MEDICAL RESIDENTS
Karin Clifton1, Komal Patel1, Justin Muir2, Natalie Yip1, Jennifer Cunningham3,
Daniel Brodie3, Amy Dzierba4; 1New York Presbyterian Hospital, New York, NY,
2
New York Presbyterian Hospital-Columbia, New York, NY, 3New York Presbyterian Hospital-Columbia Campus, New York, NY, 4New York Presbyterian,
New York, NY
Learning Objectives: Stress ulcer prophylaxis (SUP) is widely used in critically
ill patients. Protocols help providers determine high-risk patients who need acid
suppression therapy (AST) to prevent clinically significant GI bleeding. An
AST protocol in the medical intensive care unit (MICU) promoting histamine
2-receptor antagonists (H2RAs) in two identical ICUs differing only in the presence of acute care nurse practitioners (ACNPs) or medical residents. The objective of this study was to assess the compliance of a SUP protocol in medical ICU
patients cared for by ACNPs (ICU-NP) versus a medical resident-managed ICU
(ICU-R). Methods: An IRB-approved, retrospective chart review was conducted
between January and June 2013 for all adult patients admitted to the MICU.
Patients were included if they received at least one dose of either an H2RA or
once daily proton pump inhibitor (PPI) within the first 72 hours of MICU
admission. The indication for AST initiation, initial choice of AST, and duration of AST therapy were recorded. Wilcoxon rank sum test for two-independent
samples was used to compare continuous data and Fisher’s exact test was used for
categorical data. A p<0.05 was considered significant. Results:There were 114
patients included in the ICU-NP group and 132 in the ICU-R group. There
was no difference in age or ICU length of stay between the two groups. There
was a significant difference in the proportion of patients receiving H2RAs in the
ICU-NP group compared to the ICU-R group; 73.5% vs 60.5%, respectively,
p=0.04. Length of AST therapy while in the ICU was not different between the
two groups; 7 days (4, 11) in the ICU-NP group vs. 6 (4, 10) in the ICU-R
group, p=0.16. There was a significant difference in the proportion of patients
in the ICU-R group that had a major indication for AST (respiratory failure and
coagulopathy) as compared with the ICU-NP group; 77% vs. 61%, respectively,
p=0.009. Less than 1% of patients had no indication for AST in both groups;
p=1.0. Conclusions: Unit based ACNPs demonstrated improved compliance
with the AST protocol promoting the use of H2RAs as compared to residents.
151
IMPACT OF COMPUTERIZED PHYSICIAN ORDER ENTRY
ON SEDATION DEPTH AND RELATED OUTCOMES IN THE
ICU
Joel Feih1, William Peppard2, Seth Thomas3, David Herrmann1, Thomas Carver4;
1
Froedtert Hospital, Milwaukee, WI, 2Froedtert Hospital, Germantown, WI,
3
Ministry Door County Medical Center, Sturgeon Bay, WI, 4Medical College of
Wisconsin, Milwaukee, WI
Learning Objectives: Agitation is common in patients who are mechanically
ventilated (MV) and often requires pharmacologic sedation. Multiple studies
have demonstrated that deep sedation can lead to worse outcomes. In 2012, computerized physician order entry (CPOE) was implemented, and since, pharmacists have perceived the sedation order has been less frequently utilized, which has
led to more deeply sedated patients. Therefore based on the potential for worse
outcomes, we decided to investigate the influence of CPOE on sedation practices.
We hypothesized that CPOE created opportunities to bypass ICU protocols,
which resulted in worse outcomes. Methods: This retrospective study evaluated
40 patients before and 41 patients after CPOE who were MV for greater than
48 hours. Patients were included if they received lorazepam, midazolam, propofol, or dexmedetomidine during MV. The primary outcome measure was the
proportion of time patients spent at their Richmond Agitation Sedation Scale
(RASS) goal. Pertinent secondary outcomes were the number of patients with a
prescribed RASS goal, use of the order set, MV days, survival to ICU and hospital
discharge, and ICU and hospital length of stay (LOS). Results: There was no
difference in time spent at the RASS goal between the two groups (50% vs 40%,
p = 0.178). The Post-CPOE group was less likely to have the order set used (76.9
vs 29.3%, p <0.001) and a prescribed RASS goal (92.3 vs 58.5%, p <0.001).
There were no differences in duration of MV, ICU LOS, hospital LOS, or ICU or
hospital mortality. Prescription of a RASS goal was associated with a longer duration of MV and ICU LOS, but was also associated with a reduced risk of both
ICU (OR 0.207, 0.039 – 1.091, p = 0.0633) and hospital mortality (OR 0.176,
0.032 – 0.970, p = 0.046), respectively. Conclusions: This study highlights the
importance of prescribing RASS goals and titrating sedation based on protocols.
Implementation of CPOE however, can create opportunities to bypass protocols;
thus complex electronic protocols should undergo quality improvement prior to
implementation to prevent worse outcomes.
152
EVALUATION OF SAS-BASED SYMPTOM-TRIGGERED
TREATMENT OF ALCOHOL WITHDRAWAL IN CRITICALLY
ILL PATIENTS
Phil Grgurich1, Amanda Tulolo1, James Dargin1, Soumitra Sen1, Anthony Gray1;
1
Lahey Hospital & Medical Center, Burlington, MA
Learning Objectives: This study compared outcomes for critically ill patients
with alcohol withdrawal syndrome (AWS) before and after implementation of
a Sedation Analgesia Scale (SAS)-based, symptom-triggered order set. It was
hypothesized that a symptom-triggered protocol using SAS results in shorter
AWS treatment versus the combination of fixed and symptom-triggered dosing with CIWA. Methods: In this observational, single center study, data were
gathered before and after implementation of a symptom-triggered AWS order
set in 2 adult medical ICUs at a tertiary care center. Pre-intervention data from
7/2011-8/2013 were retrospectively collected. Data for patients managed using
the SAS-based symptom-triggered order set were prospectively gathered from
April-June 2014. Data include: demographics, laboratories, APACHE II score,
comorbidities, duration of AWS treatment, lorazepam dosing, ICU and hospital length of stay (LOS), duration of mechanical ventilation, ICU and hospital
mortality, complications, and adjunctive medication use. Groups were compared
using Wilcoxon Rank Sum and Fisher’s exact tests. Results: 135 patients were
included in the pre-intervention group and 5 have been enrolled in the postintervention group thus far. Baseline characteristics were similar. Median AWS
treatment lasted 8 (IQR, 5-12) and 4 days (IQR, 2-4) in the pre- and postintervention groups, respectively (p=0.02). 59% of the pre-intervention patients
received benzodiazepine infusions with a median cumulative lorazepam dose of
137mg (IQR 32-554). No patients in the post-intervention group received benzodiazepine infusions (p=0.01) and the median lorazepam dose was 8mg (IQR,
5.5-10) (p=0.002). The median ICU LOS was 7 (IQR, 4-11) and 2 days (IQR,
2-5) for patients in the pre- and post-intervention groups, respectively (p=0.05).
Pre-intervention ICU and hospital mortality rates were 2.2% and 4.5%, respectively. No patients in the post-intervention group died (NS). Conclusions: Preliminary data suggest symptom-triggered therapy for AWS in critically ill patients
may reduce duration of AWS treatment, benzodiazepine use, and ICU LOS.
Poster Session: Cardiovascular 1
153
CORRELATION BETWEEN INVASIVE AND NON-INVASIVE
CARDIAC OUTPUT ASSESSMENT IN HEART TRANSPLANT
PATIENTS
Awni Al-Subu1, Ira Cheifetz1, Andrew Lodge1, Christoph Hornik1, George OforiAmanfo2; 1Duke University Medical Center, Durham, NC, 2Duke University
Children’s Hospital, Durham, NC
Learning Objectives: Mixed venous oxygen saturation (SvO2) is a marker of
oxygen delivery and extraction at the tissue level in critically ill patients and represents an indirect assessment of cardiac output. Cerebral Near Infra-Red Spectroscopy (NIRS) is used to estimate regional oxygen saturation (rSO2) in the brain
and has been suggested to correlate with SvO2. An objective relationship between
measured cardiac output and cerebral NIRS has not been established. Hypothesis: Cerebral NIRS correlates with cardiac output measured by pulmonary artery
catheter. Methods: This retrospective cohort study included children younger
than 18 years who underwent heart transplantation and had a pulmonary artery
catheter upon admission to Pediatric Cardiac Intensive Care Unit. SvO2, cerebral
rSO2 and cardiac index (CI) were recorded hourly for 8-92 hours post-transplantation. A spearman’s rank correlation coefficients analysis was used to assess
the agreement between these measurements. Results: A total of 10 patients were
included with median age of 14 years (range, 7–17). Indications for transplantation were: dilated cardiomyopathy (n=8), restrictive CM (n=1), failed CHD
palliation (n=1). A total of 410 data points were collected. Median and interquartile ranges of cerebral rSO2, CI and SvO2 were 65% (54-69), 2.9 l/min/m2
(2.2-4.0), and 75% (69-79) respectively. Spearman’s rank correlation coefficients
were computed to assess the relationship among the different variables. The correlation coefficient between cerebral rSO2 and CI was 0.104 (p = 0.034) and that
for cerebral rSO2 and SvO2 was 0.11 (p = 0.029). When graphically presented,
cerebral NIRS followed the same trend as CI trends most of the times. Conclusions: The correlation between cerebral rSO2 and CI and that between cerebral
rSO2 and SvO2 were weak. However, NIRS trends correlated with changes in
measured cardiac index. Further studies are warranted to assess NIRS as a tool for
early detection of low cardiac output state in critically ill children.
154
ASSOCIATION OF PARP-1 ACTIVITY WITH MYOCARDIAL
DYSFUNCTION IN PATIENT WITH SEPTIC SHOCK
Li Li1, Bangchuan Hu2, ShiJin Gong3, Yihua Yu1, Haiwen Dai1, Jing Yan1; 1Zhejiang Hospital, Hangzhou, China, 2Zhejiang Provincial People’S Hospital, Hangzhou, China, 3ZheJiang Hospital, HangZhou, China
Learning Objectives: Severe sepsis and septic shock are the leading causes of
morbidity and mortality in hospitalized patients. This study aimed to investigate
the association of poly(ADP-ribose) polymerase-1 (PARP-1) activity in circulating mononuclear cells with myocardial dysfunction in patients with septic shock.
Methods: A total of 64 patients with septic shock were divided into the survival
group (n=41) and the nonsurvival group (n=23) according to mortality at 28
days after enrollments. PARP-1 activity in circulating mononuclear cells, brain
natriuretic peptide (BNP), Acute Physiology and Chronic Health Evaluation II
score (APACHEII), the cardiac index (CI), the cardiac function index (CFI),
global ejection fraction (GEF), and the left ventricular contractility index (dp/dt
max) were measured after admission to the intensive care unit. Results:PARP-1
activity in circulating mononuclear cells and BNP levels in the nonsurvival group
were significantly higher than those in the survival group. The CI, the CFI, GEF,
and dP/dt max in the nonsurvival group were significantly lower than those in the
survival group. PARP-1 activity in circulating mononuclear cells was significantly,
positively correlated with APACHE II scores and BNP levels (r=0.608, P<0.05;
r=0.685, P<0.05, respectively). However, PARP-1 activity in circulating mononuclear cells was strongly, negatively correlated with the CI, the CFI, GEF, and
dp/dt max (r=–0.702, P<0.05; r=–0.678, P<0.05; r=–0.702, P<0.05; r=–0.736,
P< 0.05, respectively). Multiple logistic regression analysis showed that PARP-1
activity (OR=2.01, 95% CI: 1.24–3.18, P=0.01) in circulating mononuclear cells
was an independent risk factor of myocardial dysfunction. The area under the
ROC curve was 0.74. The cutoff point was 942 nmol/L, and the sensibility and
specificity for prediction of 28-day mortality for the patients with septic shock
were 78.2% and 65.1%, respectively. Conclusions: PARP-1 activity in circulating mononuclear cells is significantly associated with myocardial dysfunction and
may have prognostic value in patients with septic shock.
155
CARDIAC FUNCTION INDEX PREDICTS OUTCOME OF
TAKOTSUBO CARDIOMYOPATHY AFTER SUBARACHNOID
HEMORRHAGE
Tatsushi Mutoh1, Ken Kazumata2, Yasuyuki Taki1, Kentaro Inoue1, Akifumi
Suzuki3, Tatsuya Ishikawa3; 1Institute of Development, Aging, and Cancer,
Tohoku University, Sendai, Japan, 2Hokkaido University, Sapporo, Japan,
3
Research Institute for Brain and Blood Vessels-AKITA, Akita, Japan
Learning Objectives: Takotsubo cardiomyopathy (TCM) is a life-threatening
systemic consequence early after subarachnoid hemorrhage (SAH), but precise
hemodynamics and related outcome are not well-understood. We aimed to
investigate the TCM-induced cardiac function by transpulmonary thermodilution and its impact on clinical outcome of SAH. Methods: Forty-six consecutive
SAH patients who developed TCM and treated surgically or endovascularly were
analyzed retrospectively. Patients were divided into two groups of LVEF <40%
(TCM with LV dysfunction) and LVEF ≥40% (TCM without LV dysfunction).
Cardiac function index (CFI) and extravascular lung water index (ELWI) were
monitored by transpulmonary thermodilution. Results: Transpulmonary thermodilution-derived CFI was correlated significantly with echocardiographic left
ventricular ejection fraction (LVEF) (r = 0.82, P <0.0001). The CFI between day
0 to day 7 was significantly lower in patients with LV dysfunction (LVEF <40%)
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
than in patients with LVEF ≥40% (P <0.05). CFI had a better ability than cardiac output to detect cardiac dysfunction (LVEF <40%) (Area under the curve:
0.85 ± 0.02; P <0.001). A CFI value of <4.2 min-1 had a sensitivity of 82% and
specificity of 84% for detecting LVEF <40%. The CFI <4.2 min-1 was associated
with delayed cerebral ischemia (DCI) (odds ratio [OR], 2.14; 95% confidence
interval [CI], 1.33-2.86; P = 0.004) and poor 3-month functional outcome on
modified Rankin Scale of 4-6 (OR, 1.87; 95% CI, 1.06-3.29; P = 0.02). An
ELWI >14 mL/kg after day 4 increased the risk of poor functional outcome at
3-month follow-up (OR, 2.10; 95% CI, 1.11-3.97; P = 0.04). Conclusions: Prolonged cardiac dysfunction and pulmonary edema increased the risk of DCI and
poor 3-month functional outcome in patients with SAH suffering from TCM.
Serial measurements of CFI and ELWI by transpulmonary thermodilution may
provide an easy bedside method of detecting early changes of the cardiopulmonary function in directing proper post-SAH treatment.
(3.4%). T-I elevation carried a mortality of 18% and was diagnosed in 303 of 803
(37.7%) of patients who expired within 30 days of surgery. The frequency of T-I
testing, incidence of T-I elevation, and mortality within 30 days of surgery were
each increasingly more common in patients with a higher SLUScore™, progressing at rates of 2% (1.6-2.3%), 2.5% (2-3%), and 3.3% (2.7-4%) per SLUScore™
increment, respectively (p<0.0001). Conclusions: The present data suggest that
intraoperative hypotensive exposures are common and associated with increased
postoperative cardiac morbidity (a more frequent clinical decision to test for T-I
elevation and to diagnose an MI) as well as mortality within 30 days of surgery.
156
Sankeerth Rampa1, Satheesh Elangovan2, Kyungsup Shin3, Romesh Nalliah4,
Veerajalandhar Allareddy5, Veerasathpurush Allareddy3; 1University of Nebraska
Medical University, College of Public Health, Omaha, NE, 2Department of Periodontics, College of Dentistry, The University of Iowa, Iowa City, IA, 3Department of Orthodontics - College of Dentistry, The University of Iowa, Iowa City,
IA, 4Dental Medicine, Harvard University, Boston, MA, 5Rainbow Babies &
Children’s Hospital, Cleveland, OH
WHAT IS ASSOCIATED WITH THE DISCREPANCY BETWEEN
NIBP AND IBP?
Junji Kumasawa1, Hisakazu Kohata1, Kenichi Aoyagi1, Akitosh Ohara1; 1Department of Critical Care Medicine, Sakai City Hospital, Sakai City, Japan
Learning Objectives: Noninvasive (NIBP) and invasive (IBP) blood pressure
monitoring are used in ICU and there are discrepancy between NIBP and IBP.
Some studies have reported that NIBP was higher than IBP during the periods
of hypotension. However, the details of factors associated with this discrepancy
remain unknown. Methods: To describe the difference between the patients
whose systolic NIBP is higher than systolic IBP at ICU admission (NIBP higher
group) and the patients whose systolic IBP is higher than systolic NIBP at ICU
admission (IBP higher group), we conducted cross sectional study. We retrospectively reviewed the medical records from January to July 2014. Patients (≥20 years
old) who were admitted to our medical and surgical ICU and whose IBP was
simultaneously recorded with NIBP were included. We compared the baseline
characteristics and proportion of patients with shock at ICU admission (systolic
IBP≤90mmHg) between the two groups. As a subgroup analysis, we analyzed
patients with shock. Results: 159 patients were included in this study (31
patients in NIBP higher group and 128 patients in IBP higher group). The mean
of systolic blood pressure (SBP) of IBP was higher in IBP higher group than in
NIBP higher group (144.7 ± 29.5 vs 78.5 ± 13.5, p<0.0001; IBP higher group and
NIBP higher group respectively). The proportion of patients with shock is larger
in NIBP higher group than in IBP higher group (8/128 vs 31/31, p<0.0001).
In subgroup analysis of these 39 patients with shock, all 31 patients were septic shock in NIBP higher group and 4 patients were cardiogenic shock and 4
patients were hypovolemic shock in IBP higher group. The mean of SBP was not
significantly different between both groups (82.4 ± 8.0 and 78.5 ± 13.5, p=0.44).
The mean of ScVO2 at ICU admission was significantly lower in IBP higher
group compared with NIBP higher group (53.1 ± 8.2 vs 74.8 ± 6.7, p<0.0001).
Conclusions: In analysis of patients with shock, SBP was not significantly different between both groups. ScVO2 was significantly lower in IBP higher group.
Cardiac output could be associated with the discrepancy between NIBP and IBP.
157
THE SLUSCORETM: A NOVEL METRIC QUANTIFYING THE
ADVERSE IMPACT OF INTRAOPERATIVE HYPOTENSIVE
EXPOSURE
Christopher Paul1, Hui Yuan1, Jefferson Dryden2, Audrey Vizzi2, Peter Vuong2,
Wolf Stapelfeldt2; 1Saint Louis University, Saint Louis, MO, 2Saint Louis University, St. Louis, MO
Learning Objectives: Recent findings at three US institutions introduced a
novel scoring methodology for intraoperative hypotension based on the number
of exposure limits that were exceeded for cumulative time spent at a mean arterial
pressure (MAP) below thresholds between 75 and 45 mm Hg (SLUScore™). In
116,541 patients studied, every third patient was found to exceed some or all of
these limits and experience approximately twice the 30-day all-cause mortality in
association with a SLUScore™ of > 0 versus a SLUScore™ of 0, independent of
these patients’ co-morbidity. The present study examined testing for myocardial
injury in the postoperative period as well as the role of Troponin (T-I) elevation
>0.04 as a possible mediator of the adverse impact of the SLUScore™. Methods: With IRB approval the intraoperative hemodynamic and medical records
of patients undergoing non-cardiac surgery were reviewed. Minute to minute
MAPs were analyzed and the SLUScore™ was calculated as the number of exposure limits exceeded (0 - 31). The associations of the SLUScore™ with T-I testing,
MI diagnosis (peak T-I elevation > 0.04) and death within 30 days of surgery
were examined using logistic regression, with results being expressed as mean and
95% CI. Results: Of 49,800 non-cardiac surgical patients anesthetized, 3,905
(7.8%) had T-I tests within 30 days of surgery. 1,673 had peak elevations > 0.04
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
158
IMPACT OF ORAL HEALTH ON OUTCOMES IN PATIENTS
HAVING HEART VALVE REPLACEMENT PROCEDURES IN
USA.
Learning Objectives: Heart valve replacement procedures(HVRP) are commonly performed complex surgical procedures. The impact of oral health on such
surgical procedures and related outcomes is poorly described. The objective is to
examine the prevalence of gingivitis and/or periodontitis(GP) in patients having
heart valve replacement procedures and to quantify the impact of these dental
conditions on hospital charges(HC), length of stay(LOS), and infectious complications (IC). Methods: We performed a retrospective analysis of the Nationwide Inpatient Sample for the years 2004-2010. All patients who had HVRP
were selected. Prevalence of acute/chronic gingivitis and/or periodontitis (GP)
was examined in these patients. The impact of GP on HC, LOS and IC was
examined by multivariable linear and logistic regression models. The effects of
potential confounders such as age, sex, race, insurance status, co-morbid burden,
teaching status of hospital, and hospital region were adjusted in the regression
models. The effects of clustering of outcomes within hospitals were adjusted in all
regression models. The study was IRB exempt. Results: During the study period
a total of 596,190 patients had HVRP. Amongst these, GP was present in close
to 0.2%(1 in 500) of patients. Outcomes included: median HC($175,418 wGP
vs $149,353 woGP) and median LOS(14d wGP vs 8d woGP). After adjusting
for the effects of patient and hospital level confounding factors in the regression
models, HC were 13.1% higher(p=0.001) and LOS was 40.7% longer(p<0.0001)
in those with GP compared to their counterparts. Further, patients with GP had
significantly higher odds for having bacterial infections(OR=3.40, 95%CI=2.334.98,p<0.0001) when compared to those without GP. Conclusions: In this large
retrospective study, although, the overall prevalence of gingivitis and periodontitis in patients undergoing heart valve replacement procedures appears to be low,
it is associated with higher risk of infections and significant hospital resource
utilization, suggesting opportunities for better dental-medical collaboration in
the care of such high risk surgical patients.
159
POOR ORAL HEALTH IN CABG SURGERY RECIPIENTS
INCREASES THE RISK OF INFECTIOUS COMPLICATIONS
Sankeerth Rampa1, Kyungsup Shin2, Romesh Nalliah3, Veerajalandhar Allareddy4,
Veerasathpurush Allareddy2; 1University of Nebraska Medical University, College of Public Health, Omaha, NE, 2Department of Orthodontics - College of
Dentistry, The University of Iowa, Iowa City, IA, 3Dental Medicine, Harvard
University, Boston, MA, 4Rainbow Babies & Children’s Hospital, Cleveland, OH
Learning Objectives: Coronary artery disease necessitating bypass
grafting(CABG) is a frequently performed surgical procedure in United States.
Infection complicating CABG is associated with increased morbidity & mortality. Poor oral health is associated with increased risk of bacterial infections.
The impact of oral health on CABG outcomes is unknown. The objective is to
identify the prevalence of certain dental conditions(a marker of poor oral health)
in patients who underwent CABG. Further, we sought to examine the association between the presence of dental conditions & the risk of developing bacterial infections. Methods: A retrospective analysis of the Nationwide Inpatient
Sample(2004-2010)was performed. All patients who underwent CABG were
selected. Presence of dental conditions(acute apical periodontitis of pulpal origin,
periapical abscess with/without sinus, chronic apical periodontitis, mouth cellulitis, acute/chronic gingivitis, and acute/chronic periodontitis) were identified
using ICD-9-CM codes. Occurrence of bacterial infections was the primary outcome variable. Association between presence of dental conditions & occurrence
of bacterial infections was examined by multivariable logistic regression analysis.
The present study was IRB exempt. Results: During the study period, a total
of 1,889,257 CABG surgeries were performed. Of these, 2,780(0.15%) had a
dental condition. The mean age of those who had CABG was 66 years. 71.5% of
patients were males. Bacterial infections were present in 5% of those who had a
dental condition (compared to 1.8% in those who did not have a dental condition). Following adjustment for all confounding variables including age, sex, race,
co-morbidity, insurance status, hospital teaching status & region, those who had
dental conditions were associated with a significantly higher odds for developing
bacterial infections (OR=2.90, 95% CI=2.06-4.08, p<0.0001) compared to their
counterparts. Conclusions: In this large surgical cohort nearly 1 in 750 had a
dental condition. Poor oral health was associated with a higher risk of developing
bacterial infections in CABG recipients.
160
ANTICOAGULATION INDICES IN EXTRACORPOREAL MEMBRANE OXYGENATION PATIENTS
Pamela Ader1, Scott Benken1, Ishaq Lat2, Sajni Patel3, Avery Tung4; 1N/A, Chicago, IL, 2University of Chicago Hospitals Critical Care, Chicago, IL, 3University
of Chicago Medicine, Chicago, IL, 4University of Chicago, Chicago, IL
Learning Objectives: Patients receiving extracorporeal membrane oxygenation
(ECMO) are at risk for both bleeding and thrombosis. The goal of anticoagulation is to prevent thrombosis while avoiding excessive bleeding. The purpose of
this evaluation was to identify patients who were difficult to anticoagulate and
factors related to bleeding and thromboembolic events in adult cardiac ECMO
patients. Methods: This is a single-centered, retrospective, observational, cohort
analysis assessing institution-specific anticoagulation indices in adult ECMO
patients between March 1, 2008 and August 1, 2013. Patients were considered
difficult to anticoagulate if activated partial thromboplastin time (aPTT) or activated clotting time (ACT) values were out of goal range greater than 30% of the
time. Incidences of major bleeding, minor bleeding, and thromboembolic events
were assessed, as well as average heparin doses, change in heparin dose related to
time on ECMO, and in-hospital mortality. Results: In the 32 patients included
in the analysis, wide variability was observed between heparin doses, monitoring,
and titration strategies. One hundred percent of the cohort met the definition for
difficult to anticoagulate, with a subtherapeutic majority (65.8%) of ACT and
aPTT values. Heparin doses were increased in patients with larger body surface
areas (p = 0.028), and were not impacted by age or presence of renal replacement therapy. Change in heparin dose over time increased as the duration of
ECMO increased (p = 0.005). There were 19 major bleeding events in 17 (53%)
patients and an additional 14 (44%) minor bleeding events; higher initial heparin
doses were associated with minor bleeding events (p = 0.037). Conclusions: The
data demonstrates that the optimal target anticoagulation goal for adult cardiac
ECMO patients has not yet been identified in this cohort. Despite not meeting
target goals, with most aPTT or ACT values below target goal, there were still
many more bleeding events than thromboembolic events. With the greater incidence of bleeding, perhaps more conservative anticoagulation management of
ECMO patients is warranted.
Poster Session: Cardiovascular 2
161
PREDICTION OF MAJOR ADVERSE CARDIOVASCULAR
EVENTS BY PLASMA NGAL AT CCU DISCHARGE
Kent Doi1, Masamichi Ito2, Masao Takahashi2, Eisei Noiri2, Naoki Yahagi3;
1
Tokyo University Hospital, Tokyo, Japan, 2The University of Tokyo, Tokyo,
Japan, 3The University of Tokyo Hospital, Tokyo, Japan
Learning Objectives: Acute exacerbation of renal dysfunction has a great
impact on the outcomes of cardiovascular patients in critical conditions.
Emerging acute kidney injury (AKI) biomarkers, including neutrophil gelatinase-associated lipocalin (NGAL), have a high potential for detecting renal tissue injury, better than serum creatinine. This study aimed to evaluate whether
plasma NGAL can predict the mortality and major adverse cardiovascular
events after discharge from the cardiac care unit (CCU). Methods: Patients
who were admitted in the CCU of the Tokyo University Hospital were prospectively enrolled. Blood and urinary markers, including the blood NGAL, brain
natriuretic peptide, creatinine, cystatin C, urinary albumin, N-acetyl-β-Dglucosaminidase, and L-type fatty acid-binding protein, were measured at CCU
discharge. The primary outcome was major adverse cardiac events (MACEs)
until at least 6 months after CCU discharge. Results: Of 101 enrolled patients,
35 patients experienced MACEs (35%). Among the clinical parameters and
biomarkers, the plasma NGAL and serum cystatin C at CCU discharge were
significantly higher in patients with MACEs than those without MACEs. Multivariate logistic analysis revealed that the plasma NGAL, length of CCU stay,
and complications of diabetes and heart failure were independent predicting
factors for MACEs. Patients with the highest NGAL at discharge (>75th percentile) showed a significantly higher risk of MACEs than those with the lowest
NGAL (<25th percentile) (log-rank test; Hazard ratio, 5.15; 95% confidential
interval 1.84–18.20; p<0.01). Conclusions: Plasma NGAL at CCU discharge
is a significant prognostic indicator of outcomes at 6 months in critically ill
cardiac patients treated in a CCU.
162
ALTERATIONS IN PROTEINASE-ACTIVATED RECEPTOR-1
EXPRESSION WITH INCREASED PULMONARY BLOOD
FLOW
Jun Maki1, Rebecca Johnson2, Sanjeev Datar3, Wenhui Gong2, Michael Johengen2, Christine Sun2, Peter Oishi4, Jeffrey Fineman3; 1Kyushu University Hospital, Fukuoka, Japan, 2Univeristy of California, San Francisco, San Francisco,
CA, 3University of California San Francisco Medical Center, San Francisco, CA,
4
University Of California San Francisco, San Francisco, CA
Learning Objectives: Proteinase activated receptor-1 (PAR1), the primary
thrombin receptor involved in thrombin-mediated platelet thrombosis, has
been implicated in a variety of cardiovascular disorders. Platelet aberrations and
thrombosis contribute to the pathobiology of pulmonary hypertension (PH),
but data on PAR1 in PH are lacking. The aim of this study was to determine
potential changes in PAR1 expression in lambs with PH secondary to increased
pulmonary blood flow (PBF). Methods: Fetal lambs (n=9) underwent placement of an 8mm aortopulmonary vascular graft (shunt). Four weeks following
delivery, hemodynamics were obtained, and pulmonary arteries (PA) and veins
(PV), and peripheral lung tissue were harvested from shunt and twin control
lambs. PAR1 protein and mRNA levels were evaluated in PA and PV by western
blot and real time RT-PCR, respectively. Localization of PAR1 was determined
by immunohistochemistry (IHC) on peripheral lung tissues. Results: Shunt
lambs had a pulmonary to systemic blood flow ratio of 3.4:1. Mean pulmonary
arterial pressure was higher in shunt than control lambs (19.0+4.9 vs. 14.0+2.7
mmHg, p<0.01). In PA, protein expression of PAR1 was higher in shunt than
control lambs (0.48 ± 0.04 vs. 0.30 ± 0.03 arbitrary unit normalized by β-actin
(AU), p<0.01). However, in PV PAR1 protein was lower in shunt than control
lambs (0.77 ± 0.09 vs. 1.09 ± 0.10 AU, p=0.03). Similarly, mRNA expression of
PAR1 in PA was higher in shunt than control lambs (4.36 ± 0.88 fold increase,
p<0.01), while lower in shunt than control lambs (1.91 ± 0.32 vs 4.49 ± 1.06
fold increase, p=0.01) in PV. IHC demonstrated PAR1 expression in endothelial
and smooth muscle layers in PA from shunt and control, and PV from control;
expression appeared to be higher in the endothelial layer in these vessels. In
PV from shunt lambs, endothelial staining was not appreciated. Conclusions:
In an ovine model of PH 2° to increased PBF, there are early changes in PAR1
expression, with differential changes between PA and PV. The physiological consequences of these changes, and its potential role in the pathobiology of PH
warrant further investigation.
163
PERIOPERATIVE ANTICOAGULATION SPECIFIC TO CARDIAC INTERVENTIONAL PROCEDURES
Joel Regalado1, Mayola Rowser2; 1Valley Health System, Ridgewood, NJ, USA,
2
University of Southern Indiana, Evansville, IN
Learning Objectives: The challenge of continuing anticoagulation therapy in
patients preparing for elective cardiac interventional procedures is increased
risk of post-operative bleeding. Conversely, interruption of such therapy may
increase the risk of thromboembolism. An opportunity exists to form an anticoagulant/antiplatelet management plan to achieve a low incidence of bleeding and thrombosis. Methods: Retrospective electronic chart review of 2,617
adults post cardiac interventional procedures from January 2010 to December
2012. The associations between the patients demographics, medications used
and procedural complications were examined using correlational statistics with
significant values set at p<0.05 as predictor for complication development.
Results: Female sex is significantly correlated (p<0.001) to the need for post
procedural transfusion as well as lower BMI (p=0.028). Age ≥70 were a significant factor for bleeding episodes (p=0.020) and need for post procedural
transfusion (p=0.001). Comorbidities that have significant correlation (p<0.05)
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
to post procedural transfusion were heart failure, diabetes and peripheral arterial
disease. Increase INR level and activated partial thromboplastin time (aPTT)
are both significantly correlated to complication development (p<0.05). The
types of medications that are significantly correlated to post procedural transfusion included Unfractionated Heparin (p=0.009), Clopidogrel (p=0.041) and
GP2B3A inhibitor (p=0.039). Prasugrel (p=0.001) and Bivalirudin were the
only medications that significantly did not show an increase in the need for
transfusion. The antiplatelet Aspirin (p>0.05) and low molecular weight (LMW)
Heparin (p>0.05) were the only medications that did not show significant correlation to bleeding and transfusion. Conclusions: Practitioners should take into
consideration the patient’s age ≥70, female sex, low BMI, coagulation status
(elevated INR and aPTT level) and concomitant use of anticoagulant as a basis
when prescribing anticoagulant therapy among patients undergoing cardiac
interventional procedures
164
THE PROGNOSTIC VALUE OF SERUM 25- HYDROXY VITAMIN D LEVEL IN PATIENTS WITH ST-SEGMENT ELEVATION
MI
Samir Hegazy1, Mostafa Alkomi2, Mohamed Alsawy2, Hesham Elashmawy2;
1
N/A, alexandria, Egypt, 2Faculty of Medicine, Alexandria university, alexandria,
Egypt
Learning Objectives: Vitamin D deficiency traditionally recognized as the
cause of musculoskeletal pathology, but links to cardiovascular disease has only
recently been suggested. (1) Vitamin D suppresses the renin–angiotensin system,(2) affects endothelial function and has anticoagulant effects by upregulating thrombomodulin and downregulating tissue factor. (3) These effects may
have direct relevance to cardiovascular disease. (4) Methods: In a prospective
cohort study, 53 patients with acute ST segment elevation myocardial infarction were included. According to the patients’ 25 (OH) D levels (ng/ml) level
patients were categorized into two groups one with low 25 (OH) D levels and
the other with normal level. Clinical characteristics, laboratory data, in-hospital
outcomes and 6 months mortality were recorded. Results: Almost 70% of the
STEMI group were vitamin D deficient (<30 ng/ml). Patients with history of
hypertension had significantly lower vitamin D levels (p value <0.001). Moreover, a significant positive relationship between hospital length of stay and
levels of vitamin D (p value <0.003). In addition, hospital length of stay was
significantly higher in patients who undergone primary percutanous intervension (p value <0.008). Conclusions: Vitamin D deficiency is highly prevalent
in patients with acute STEMI and in patients with history of hypertension.
Vitamin D deficiency is associated with longer length of hospital stay in STEMI
patients
with AKI AKIN 1 was unable to prevent the need for dialysis, but decreased the
in hospital mortality rate.
166
THE IMPACT OF VASOPRESSIN ADMINISTRATION ON ACUTE
KIDNEY INJURY FOLLOWING OPEN HEART SURGERY
Jahan Porhomayon1, Pradeep Arora2, SINA DAVARI FARID3, Nader Nader1;
1
N/A, Buffalo, NY, 2University at Buffalo, Buffalo, NY, 3University at Buffalo,
BUFFALO, NY
Learning Objectives: Severe hypotension in the perioperative period in cardiac surgery patients is a common problem that is most commonly treated by
administrating vasopressor drugs. As one of the avidly used Vasopressor drugs,
Arginine vasopressin, despite its efficiency, has been shown to have serious
clinical side effects such as kidney and liver dysfunction and also thrombocytopenia. The purpose of the present study was to compare the incidence of
Acute Kidney Injury in patients who received vasopressin in comparison to
the patients who did not receive any vasopressor drug or received other pressor
drugs. We hypothesized that vasopressin use is associated with increased risk
of acute kidney injury (AKI) in the postoperative period. Methods: In a retrospective study, 483 patients (>99% Male) who underwent open-heart surgery
since April 2004 till April 2010 were studied. Baseline demographics, perioperative hemodynamic parameters and the incidence of postoperative complications were extracted. The exclusion criteria were: 1) Valve surgery, combined
valve/CABG and Aortic surgery, 2) preexisting chronic kidney disease stage 3
or higher, 3) Off-pump procedure. Patients were divided in two groups; vasopressin (cases) and no vasopressin (controls). To calculate AKI severity, Acute
Kidney Injury Network (AKIN) classification was used. Results: 280/483
patients received vasopressin in the perioperative period. The AKI incidence
was 70 out of 483 patients (14.5%); the incidence was 56/280 (20%) in vasopressin group and 14/203 (6.1%) in non-vasopressin group. In the univariate analysis, vasopressin use showed significant increase in postoperative AKI
incidence (p<0.005); baseline hypertension and perioperative blood loss were
also associated with increased AKI. In the multivariate analysis, only vasopressin demonstrated a statistically significant increase in AKI incidence; OR=3.60
[1.22-10.62], (p=0.02). Conclusions: AKI is a common complication after
cardiac surgery and vasopressin use increases its incidence.
167
ARTERIAL CATHETER FAILURE IN CRITICALLY ILL
PATIENTS
GOAL-DIRECTED THERAPY DOES NOT REVERSE AKI IN
CRITICALLY ILL PATIENTS BUT DECREASES MORTALITY.
Nicholas Watson1, Ryan Bylsma2, Ashwin Gupta3, Shawn Reidy3, Robert Robinson4, Mina Todorov5, Marc Hoeksema5, Gaby Iskander5; 1Anesthesia Practice
Consultants, PC, Grand Rapids, MI, 2Grand Rapids Medical Education Partners, Grand Rapids, MI, 3Michigan State University College of Human Medicine, Grand Rapids, MI, 4St. Joseph Mercy Oakland, Pontiac, MI, 5N/A, Grand
Rapids, MI
Learning Objectives: Evaluate if the use of a strategy for hemodynamic optimization in patients with acute kidney injury (AKI) is able to prevent the need
for dialysis Methods: A controlled, randomized, multicenter study. Patients
with acute kidney injury (AKI) classified as AKIN 1 (increase in serum creatinine > 0.3 mg/ dL and urine output less than 0.5ml/kg/h over 6 hours) for
less than 12 hours were enrolled. The Intervention group was monitored with
FloTrac/Vigileo and optimized with fluid challenges, dobutamine and blood
transfusion, if necessary, to maintain a IDO2>600ml/min/m2 during 8 h. The
control group was treated according the discretion of the attending physician.
The outcome measures where the need for hemodialysis, mortality and length
of stay. Results: A total of 102 patients were included, 52 in the control group
and 50 in the intervention group. The mean age was 66 years and 63% were
male. Hemodialysis rates were similar in both groups (26.5 vs. 26.0%, p=0.95).
Mortality rate in hospital was 51.9% in the control group and 30% in the
intervention group (p =0.025). Number needed to treat=4. SOFA 24 h (OR
1.24, CI 95%1,07-1,44; p=0.004) and control group (OR 3.5, CI 95% 1,007,12; p=0.05) were associated with increased risk of death in the multivariate
analysis. SOFA 24h (OR: 1.4, CI 95%1,17-1,79; p=0.01) and lactate at 8 h
(OR: 4.8, CI 95% 2,05-11,32; p=<0.001) were independent predictors of need
for hemodialysis. Conclusions: The optimization of oxygen delivery of patients
Learning Objectives: The purpose of this study was to evaluate arterial catheter (AC) failure rate and factors associated with AC failure in a mixed surgical
and neurological intensive care unit (ICU) at a tertiary medical center. The null
hypothesis was that no difference would exist in comparing the characteristics
of AC with and without failure. Methods: We retrospectively studied 382
consecutive AC placements in patients admitted to the ICU over a 6 month
period in 2013. Arterial waveform and patency during flushing were routinely
electronically documented. AC failure was rigidly defined in accordance with
the electronic documentation options. Primary variables studied: conditions at
time of placement (location performed, time, emergent nature, lidocaine use,
percutaneous vs wire exchange, attempts, securing method, sedation, operator
type), gender, ICU length of stay (LOS), sidedness, anatomical location, size
of AC, and duration to failure or elective removal of AC. Quantitative variables compared by t-test and nominative variables by Chi-square. Significance
defined as p < 0.05. Results: Of 382 AC placed during the study period, 363
(95%) had complete records and were included in analysis. AC failure rate was
41.6% (95%CI 36.6%-46.7%). Average duration (+/- SD) to AC failure was
31.3 (+/- 39.3) hours. ICU LOS was significantly greater for failed AC 14.8
(+/-13.1) days versus AC without failure 10.1 (+/- 9.5) days, p < 0.001. AC
failure was significantly greater for AC placed in the ICU (48.9%) versus AC
placed in the OR (37.3%), p = 0.030. No additional significant differences
were found. Conclusions: This study suggests that AC placement in the ICU
(vs OR) and increased LOS are associated with greater AC failure rates. A
number of potentially modifiable variables were not significantly associated
with AC failure in an ICU patient population. This study establishes a baseline AC failure rate that can be used for comparison in future studies aimed at
decreasing AC failure.
165
Cristina Amendola1, Joao Silva2, Taisa Carvalho3, Emerson Lima4, Emmanuel
Burdmann5, Luiz Malbouisson6, Suzana Lobo7; 1Hospital de Câncer de Barretos-Fundação PIOXII, Barretos,SP, Brazil, 2University Sao Paulo, Sao Paulo, SP,
3
Hospital de Câncer de Barretos- Fundação PIO XII, Barretos, Brazil, 4Hospital
de Base de são José do Rio Preto-Famerp, Sao Jose do Rio Preto, Brazil, 5Sao Jose
Do Rio Preto Medical School, Sao Jose do Rio Preto, SP, 6N/A, Sao Paulo, Brazil,
7
Associacion De Medicina Intensiva Brasileira, Sao Paulo, SP
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
168
169
LOW CARDIAC OUTPUT SYNDROME SCORE – THE NEW
COMPANION TO THE VASOACTIVE-INOTROPIC SCORE?
NON-INVASIVE MEASURE OF MUSCLE PH CORRELATES
WITH SPLANCHNIC PERFUSION DURING SHOCK
Kalia Ulate1, Ofer Yanay1, Jane Di Gennaro1, Howard Jeffries1, Harris Baden1,
Cohen Gordon2, Jerry Zimmerman1; 1University of Washington, Seattle, WA,
2
University of California, San Francisco, San Francisco, CA
Learning Objectives: The study objective was to evaluate an empirically derived
low cardiac output syndrome (LCOS) score (LCOSS) as a clinical assessment
tool for the presence and severity of LCOS and its association with clinical outcomes.We hypothesized that higher peak and cumulative LCOSS (pLCOSS and
cLCOSS) would be associated with worse outcomes in infants undergoing surgical repair or palliation of congenital heart defects (CHD). Methods: Prospective
observational cohort study of infants undergoing surgery for CHD at Seattle
Children’s Hospital from January 1st 2011-January 1st 2012. Clinical and laboratory data were recorded hourly for the first 24 hours after surgery. A LCOSS
was obtained by assigning 1 point for each of the following: tachycardia, oliguria, toe temperature <30°C, need for volume administration in excess of 30 ml/
kg/day, decreased near infrared spectrometry (NIRS) measurements, lactate
>2mmol/L, and need for inotropes in excess of milrinone at 0.5mcg/kg/min. A
cLCOSS was obtained by adding LCOSS on arrival to CICU, and postoperative
hours 8, 12 and 24 as a combined measure of duration and severity of LCOS.
Scores were analyzed for association with combined morbidity(CM)(prolonged
duration of mechanical ventilation [MV], infection, renal dysfunction, acute
central nervous system events, cardiorespiratory arrest, need for extracorporeal
life support, death) and CICU and hospital length of stay (LOS). Results: 54
patients were included. Overall CM was 38.8%. Patients with CM had higher
pLCOSS and cLCOSS (median [IQR]: 2 [1-3] vs 3 [2-5] p=0.008 and 2[1-4.3]
vs 8 [4.8-10.8]*). After adjusting for other relevant continuous variables (age,
inotropic score,CPB, Aox and CA times) by multivariate logistic regression,
cLCOSS was independently associated with CM (OR:1.45; 95% CI:1.2-1.8*).
An ROC curve analysis of cLCOSS vs CM revealed an optimal cutoff of >7
(AUC: 0.84*). Patients with cLCOSS >7 had higher morbidity*, longer duration of MV*, CICU LOS* and hospital LOS (p=0.002).*p<0.001 Conclusions:
Higher pLCOSS and cLCOSS are associated with increased morbidity in infants
following surgery for CHD.
Erin Bohula May1, Babs Soller2, Molly O’Brien1, Stephen Kidd1, David Berg1,
Ryan O’Malley3, Stephen Wiviott1, David Morrow1; 1Brigham and Women’s
Hospital, Boston, MA, 2University of Massachusetts, Westboro, MA, 3Stanford
University, Palo Alto, CA
Learning Objectives: Early identification of hypoperfusion is essential in the
treatment of critically ill patients. It has been shown that blood flow to skeletal
muscle parallels splanchnic organ perfusion during shock. Local muscle pH has
previously been shown to be an indicator of acute liver injury (ALI) in a swine
hemorrhagic shock model (Soller et al. J of Surg Res 2003). We hypothesized that
non-invasive measures obtained with the CareGuide monitor, a surface device
using near-infrared spectroscopy to evaluate local muscle pH would predict ALI
in humans with shock. Methods: Thirty-six subjects were enrolled in the BWH
Cardiac Care Unit with established shock (n=32; hypotension or pressor use and
evidence of organ hypoperfusion) or emerging shock (n=4; new hypotension
and evidence of new organ hypoperfusion). The CareGuide monitor was applied
to the deltoid and muscle pH (pHm) was measured continuously in a blinded
fashion. Two subjects failed to capture any pHm measurements. Clinical parameters were recorded according to usual care during monitoring, including new
or ongoing ALI (ALT, AST or total bilirubin >2x ULN). The minimum pHm
value within a 4 hour block was assessed for the ability to predict ALI on the
subsequent calendar day. Results: Of the 34 subjects analyzed, 76.5% were male
with a mean age of 59.3 (13.8) years. Most cases were classified as cardiogenic
shock by the treating physician (76.5%), with the remaining classified as mixed,
distributive or other. Subjects were monitored for a mean of 5(2.6) calendar days.
Univariate analysis demonstrated that minimum pHm was significantly associated with subsequent ALI where a 0.1 unit decrease in pHm predicted a 37%
increased odds of ALI (OR=1.37, 1.17-1.60, p=0.0001). After adjustment for
several univariate confounders (subject ID, gender, race, BMI, cardiogenic shock,
renal failure, hypotension, pressor use and mechanical circulatory support),
the relationship between minimum pHm and future ALI remained consistent
(OR=1.52, 1.19-1.93, p=0.0006). Conclusions: pHm provides early and noninvasive detection of splanchnic hypoperfusion manifest as ALI.
Poster Session: Cardiovascular 3
170
NASAL ALAR BLOOD FLOW IS MAINTAINED WITH OCCLUSION OF THE FACIAL AND/OR OPHTHALMIC ARTERIES
decreased aPPGA by up to 88% (simulating poor perfusion) but never prevented
calculation of OS on either NA. The NA appear to be a preferred site for PO.
Richard Melker1, Mark Rice2, Lori Deitte3, Timothy Morey2, Sean Cohen4,
Matthew Rush4, Donn Dennis1; 1Department of Anesthesiology, University of
Florida College of Medicine; Xhale, Inc., Gainesville, FL, 2Department of Anesthesiology, University of Florida College of Medicine, Gainesville, FL, 3Department of Radiology, University of Florida College of Medicine, Gainesville, FL,
4
Xhale, Inc., Gainesville, FL
Steven Trottier1, Cheikh OuldEthmane2, Zerihun Bunaye1; 1Saint John’s Mercy
Medical Center, Saint Louis, MO, 2Mecry Hospital, Saint Louis, MO
Learning Objectives: Digit pulse oximetry (PO) is an ICU standard. When it
fails, forehead sensors are used, but can cause necrosis. The nasal alae (NA) receive
bidirectional blood flow (BF) from the ophthalmic (OA) and facial (FA) arteries with intercarotid and transfacial anastomoses. We hypothesize the NA are
a superior site for PO. Doppler ultrasound (DUS) measured BF in the nasal
angular artery (AA) and photoplethysmography (PPG) measured oxygen saturation (OS) and magnitude of BF at the NA during occlusion (OC) of the FA
and/or OA. Methods: With IRB approval 23 subjects (16F) 20-77 years of age
(mean 43.8) were studied. Bilateral NA sensors were placed. The FA, AA and OA
were identified by DUS on one side randomly. The DUS transducer was placed
over the AA and the FA, then the OA, and then both were occluded for <15
seconds. A Mindray M7 recorded DUS and matched oximeters OS and PPG.
NA PPG amplitude (aPPGA) change with OC was calculated as the percentage
drop from baseline aPPGA prior to OC. Results:One way RM ANOVA showed
an overall significant (P<0.001) mean (±SD) decrease in aPPGA of 38.5 ± 28.9%
after FA OC, 9.2 ± 13.8% after OA OC, and 21.4 ± 24.4% after OC of both;
pairwise comparisons using SNK testing showed an effect rank order of OC FA
> OC Both > OC OA. 17 subjects had flow reversal with FA OC and 1 with OA
OC. Contralateral aPPGA did not change, nor was there hysteresis after OC. OS
was measurable at all times from both NA. Conclusions: NA BF is adequate to
measure OS even with OC of both the FA and OA. The FA is dominant for NA
perfusion in a majority of subjects (more had a decrease in aPPGA and of greater
magnitude during FA than OA OC). Flow reversal in 17 subjects during FA
OC indicates BF to the NA from the ipsilateral OA, while its absence indicates
transfacial flow. While aPPGA decreased in 14 subjects with OC of both vessels,
BF was always present indicating transfacial flow. OC of a single or both vessels
Learning Objectives: With the appropriate level of training and experience, an
intensivist can perform and interpret bedside focused critical care echocardiograms
(echos). Intensive care unit telemedicine offers an additional possible dimension
to the focused echocardiogram: real time remote assessment. The purpose of this
study is to assess the feasibility of performing and interpreting real time remote
focused critical care echos via telemedicine. Methods: A prospective cohort study in
a medical surgical intensive care unit was performed. Patients that had undergone
formal echo within twenty-four hours of the study tele-echo were eligible. The telemedicine intensivist used the real time video camera to view the bedside tele-echo.
The bedside echo was performed by a first year critical care fellow with limited
echocardiographic experience. The goal of the assessment was to obtain 3 views
(parasternal long and short axis and apical four chamber) to determine a visual
estimate of the left ventricular ejection fraction (LVEF) and the presence or absence
of a pericardial effusion. If these three views were inadequate, a subcostal view was
obtained. The results were compared to the formal echo report performed by board
certified cardiologists. Results: Thirty five patients were evaluated and thirty four
(97%) had interpretable tele-echo views. The average age was 69 +/- 19 years and 14
(40%) patients were female. The average BMI was 29 and 16 (46%) patients were
mechanically ventilated. The estimated tele-echo LVEF was within 10 percentage
points of the formal echo study in 32 (94%) of 34 patients. The correlation coefficient was 0.876 by the Pearson’s R test. The tele-echo documented 6 patients with
a pericardial effusion and the formal echo study confirmed 5 of the 6. Conclusions:
This study confirms the feasiblity and accuracy of real time focused critical care teleecho assessing for LVEF and pericardial effusion compared is formal echo results.
Tele-echo may have a role in the evaluation critically ill patients admitted to areas
with limited resources. Further evaluation is required to confirm these findings.
171
ADVANCING ICU TELEMEDICINE: REAL TIME FOCUSED
CRITICAL CARE MEDICINE TELE-ECHOCARDIOGRAM
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
172
174
COMPARISON OF UNCALIBRATED, CALIBRATED AND
THERMODILUTION-DERIVED CARDIAC INDEX: A PROSPECTIVE STUDY
PROPHYLACTIC AMIODARONE AND MAGNESIUM FOR
POSTOPERATIVE ATRIAL FIBRILLATION IN CARDIAC
SURGERY
Wolfgang Huber1, Bastian Brandt1, Analena Beitz1, Mair Sebastian1, Benedikt
Henschel1, Roland Schmid2; 12nd Medical Department; Technical University of
Munich, Munich, Germany, 22nd Medical Department; Technical University of
Munich, München, Germany
Learning Objectives: After calibration by thermodilution (TD), the PiCCO
device is able to assess cardiac index (CI) using pulse contour (PC) analysis.
Furthermore, there are several devices providing an un-calibrated estimate of
CI (CI-uncal) including the ProAqt (Pulsion Medical Systems, Germany). CIuncal is assumed to be based on analysis of the arterial pressure curve, empirical and biometric data. It was the aim of our prospective study to evaluate the
predictive capabilities of un-calibrated (CI-uncal) and calibrated CI-PC regarding CI-TD. Methods: In 29 patients (21m; 8f; APACHE-II 16 ± 5) with TDmonitoring a total of 232 datasets were recorded (8 datasets per patient within
24h). Immediately before TD calibrated CI-PC (PiCCO; Pulsion Medical
Systems, Germany) and un-calibrated CI-uncal - provided by a ProAqt-device
connected to the arterial TPTD catheter - were recorded and compared to the
subsequent thermodilution-derived CI-TD (PiCCO). Results: Results: CI-PC
was not significantly different from CI-TD (3.96 ± 1.24 vs. 3.94 ± 1.13L/min*m2;
p=0.746). Bias (0.017 ± 0.58L/min*m2) and percentage-error (PE; 28.7%) were
acceptable. CI-uncal (4.06 ± 0.94) was not different from CI-TD (p=0.104) and
provided acceptable bias of 0.12 ± 1.03L/min*m2. However, PE (50.5%) was
markedly above the acceptable threshold of 30%. CI-uncal significantly predicted
“CI-TD≤2.5L/min*m2” (AUC 0.684; p=0.001) and “CI-TD≥5L/min*m2”
(AUC 0.724; p<0.001). However, AUCs were markedly larger for CI-PC (0.957
and 0.927; p<0.001). Changes in CI-TD were moderately associated to changes
in CI-PC (r=0.326; p<0.001) and to changes in CI-uncal (r=0.230; p<0.001).
Comparison of changes in CI-PC and changes in CI-uncal provided the highest
coefficient of correlation (r=0.567; p<0.001) suggesting a similar pulse contour
algorithm for CI-pc and CI-uncal. Conclusions:Calibrated CI-PC estimares
CI-TD with appropriate accuracy and precision. Although accuracy, prediction
of trends and critical thresholds are acceptable, precision of CI-uncalib is not
appropriate with a PE of 50.5%. Precision of CI-uncal might be improved by
external calibration (PAC; ECG).
Sara Varnado1, Pamela Burcham1, Danielle Blais1, Kyle Porter1, Erik Abel1; 1The
Ohio State University Wexner Medical Center, Columbus, OH
Learning Objectives: Postoperative atrial fibrillation (POAF) is the most
common complication of cardiac surgery. Many therapies have been investigated for POAF prophylaxis with beta blockers and amiodarone showing the
most efficacy. Despite positive results, there is still a high incidence of POAF
and the benefits of combination therapy have not been well elucidated. The
purpose of our study was to compare the rate of POAF within a control
group receiving standard care compared to standard care plus a POAF prophylaxis protocol. Methods: This was a single-center, retrospective, cohort
study of CABG and/or valvular surgery patients identified using the Society of Thoracic Surgeons database. A historical control group who received
standard care of beta blockers was compared to patients who received this
standard care plus our prophylaxis protocol including pre- and postoperative oral amiodarone and postoperative intravenous magnesium. Patients
were excluded if they were <18 years old or ≥ 89 years old, incarcerated,
had a diagnosis of atrial fibrillation preoperatively, underwent rhythm correction surgery, were on any chronic antiarrhythmic medication or had a
transcatheter aortic valve replacement (TAVR) procedure. Results: There
was no difference in the incidence of POAF between our control group and
our protocol group (24.6% vs. 25%, p=0.91). The median length of hospital
stay was reduced by 1 day in the protocol group [10 (7-15) days vs. 9 (5-13)
days, p=0.02], while no other secondary outcomes were significant including in-hospital mortality, stroke and 30-day hospital readmission for atrial
fibrillation. The compliance with preoperative beta blockers was significantly higher in our protocol group compared to the control group, 74.8%
vs. 95.5%, p<0.001. Conclusions:Beyond standard care, the addition of a
prophylaxis protocol including amiodarone plus postoperative intravenous
magnesium did not reduce the incidence of POAF. High compliance with
perioperative beta blockers may provide similar reductions in POAF when
not contraindicated.
175
173
NON-INVASIVE MEASURE OF TISSUE PERFUSION, SMO2,
COMPARED WITH STANDARD INVASIVE ASSESSMENTS OF
SHOCK
CARDIAC DYSFUNCTION IN ADULT HEART DONORS &
TEMPORAL CHANGES OF LV SYSTOLIC FUNCTION OVER
TIME
Erin Bohula May , Babs Soller , Molly O’Brien , Stephen Kidd , David Berg ,
Ryan O’Malley4, David Morrow1, Stephen Wiviott1; 1Brigham and Women’s
Hospital, Boston, MA, 2University of Massachusetts, Westboro, MA, 3Brigham
and Women’S Hospital, Boston, MA, 4Stanford University, Palo Alto, CA
Shan Modi1,2, Xenia Pachmann1,3, Vijay Krishnamoorthy1,3, Ali Rowhani-Rahbar1,4,
Michael Souter5, Monica Vavilala6; 1Harborview Injury and Prevention Center, Seattle,
WA, 2University of Texas Medical Branch, Galveston, TX, 3University of Washington, Seattle, WA, 4University of Washington, Seattle, TX, 5University Of Washington,
Seattle, WA, 6Harborview Medical Center, Seattle, WA
Learning Objectives: Early identification of shock and ongoing assessment of
tissue perfusion is essential in the treatment of critically ill patients. Complications associated with invasive monitoring are important contributors to ICU
morbidity. We hypothesized that non-invasive measures obtained with the CareGuide monitor, a surface device using near-infrared spectroscopy to evaluate
local tissue perfusion, would correlate with standard invasive measures of tissue
perfusion. Methods: Thirty-six subjects were enrolled in the Brigham & Women’s Hospital Cardiac Care Unit with established shock (n=32; systolic blood
pressure < 90mmHg or pressor use and evidence of organ hypoperfusion) or
emerging shock (n=4; new hypotension and evidence of new organ hypoperfusion). The CareGuide monitor was applied to the deltoid and muscle oxygen
saturation (SmO2) was measured continuously in a blinded fashion. Clinical
parameters, including venous oxygen saturation (SvO2) and cardiac index (CI),
were recorded according to usual care throughout the monitoring period. Every
24 hour period was divided into 4 hours blocks and minimum values for SvO2
and CI were compared to SmO2 in the same window. Two subjects failed to
capture any SmO2 data. Results: Of the 34 subjects analyzed, 76.5% were male
with an average age of 59.3 (13.8) years. Most cases were classified as cardiogenic
shock by the treating physician (76.5%), with the remaining classified as mixed,
distributive or other. Subjects were monitored for an average of 5 (2.6) calendar
days. Univariate analysis demonstrated that lower minimum SmO2 was significantly associated with lower CI (β=0.015, p=0.0007), lower SvO2 (β=0.295,
p=<0.0001), and in-hospital death (β=-0.016, p=0.0028). After adjustment
for several potential confounders, including subject ID, etiology and timing
of shock, race, age, BMI, new pressor use, end organ dysfunction, mechanical
circulatory support and death, the relationship with CI (β=0.018, p=0.0016)
and SvO2 (β=0.208, p=0.0001) remained consistent. Conclusions: SmO2, a
non-invasive measure of tissue perfusion, correlates with invasively-measured
SvO2 and CI.
Learning Objectives: Exclusion of hearts with left ventricular systolic dysfunction directly contributes to the lack of donor availability. While prior
studies have suggested that appropriate donor management and evaluation
with serial echocardiography have improved organ harvest, no widespread
studies have been performed to fully evaluate this premise. Thus, the aim of
this study is to illustrate the significance of serial echocardiography in cardiac harvest of patients with prior cardiac dysfunction for a large sample size.
Methods: A cross-sectional retrospective study was performed using an organ
database (Life Center Northwest) to identify adult organ donors diagnosed
with brain death between Jan 2011 and Nov 2013. 246 potential adult donors
were identified with at least one transthoracic echocardiogram (TTE) following brain death, with 55 donors receiving at least 2 TTEs following brain
death. TTEs were reviewed for cardiac dysfunction, with the defining criteria being an ejection fraction (EF) <50% and/or presence of regional wall
motion abnormalities (RWMA). Descriptive statistics were used to analyze
clinical characteristics and describe longitudinal echocardiogram findings in
all patients receiving serial echocardiograms (n=55). Results: Cardiac dysfunction (CD) was present in 74 (30%) of patients. Of the patients receiving serial
echocardiograms, 29 patients (53%) presented with cardiac dysfunction. 15
(52%) patients of this subset had their CD resolve over time leading to organ
harvest; the remaining 14 subjects were not harvested for transplantation. Statistical analysis revealed that younger patients were more prone to CD following brain death. In the patient subset with CD not receiving serial echoes,
only 6 (13.3%) of the group were transplanted. Conclusions:In 29 patients
initially ruled out for transplant due to CD, 15 (52%) had their CD resolve
over time leading to organ harvest for transplantation. Well-designed prospective studies are still needed to determine the indications of cardiac dysfunction
during brain injury, and the survival rates in those receiving previously CD
affected hearts.
1
2
3
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
1
1
176
SPECKLE TRACKING IMAGING FOR EVALUATION OF EFFECTS
OF PEEP LEVEL ON RIGHT VENTRICULAR FUNCTION
Melis Türker1, Aynur Camkiran Firat1, Bahar Pirat1, Atilla Sezgin1, Gulnaz
Arslan2, Arash Pirat2; 1Baskent University Faculty of Medicine, Ankara, Turkey,
2
Baskent University, Faculty of Medicine, Bahcelievler, Ankara
Learning Objectives: Positive end expiratory pressure (PEEP) is commonly
used to correct hypoxemia in intensive care unit. However, PEEP may impair
right ventricular functions by increasing its afterload. Speckle tracking imaging
(STI) is a new echocardiography strain analysis technique that provides direct
assessment of myocardial contractility during systole and diastole. The aim of
this study was to evaluate the effects of different PEEP levels on right ventricular
functions by using STI in patients undergoing coronary artery bypass grafting
surgery. Methods:After ethics committee approval and patients’ written consent, we prospectively analyzed 20 CABG surgery patients. After initiation of
mechanical ventilation and before sternotomy 5,10, and 20 cmH2O of PEEP
were applied in 5 minutes intervals consequently. After stabilization at each
PEEP level four and two chamber images of right ventricle were recorded using
TEE.The right ventricle diameter,velocity,longitudinal strain,SR, and fractional
area change (RVFAC) were calculated and evaluated from the recorded images.
Results: The mean age of study patient (85% male) was 59,7 ± 10,5 years. Intraoperative mean, systolic, and diastolic arterial blood pressures and heart rate were
similar at the three PEEP levels.Compared with 5 and 10cmH2O PEEP, mean
RVFAC significantly decreased at 20cmH2O PEEP (p=0.001). Right ventricle
velocity reduced with incremental PEEP increases (p<0.05). Mean SR values
decreased at 20cmH2O PEEP when compared with 5cmH2O PEEP(p=0.03).
Mean right ventricle diameter measurements decreased with incremental PEEP
increases, however this decrease was significantly different between 20cmH2O
PEEP and other two PEEP levels (p = 0.01).Mean right ventricle strain value
significantly decreased at 20cmH2O PEEP when compared with other two PEEP
levels (p<0.001 for both) Conclusions: Compared with 5 and 10cmH2O PEEP
levels,right ventricle functions in terms of strain, SR, right ventricle diameter, and
RVFAC were significantly impaired at 20cmH2O PEEP level.
177
A NONPHARMACOLOGICAL APPROACH TO DECREASE
RESTRAINT USE IN A TRAUMA INTENSIVE CARE UNIT
Roberta Johnson1, Valerie Curry2, Kari Johnson2; 1John C Lincoln Hospital-nm,
Phoenix, AZ, 2John C Lincoln North Mountain Hospital, Phoenix, AZ
Learning Objectives: Once delirium is diagnosed, pharmacologic (sedation,
antipsychotics) and non- pharmacologic (physical restraints) measures are implemented. Restraints increase risk of dehydration, immobility, decrease skin integrity
and anxiety. Alternative interventions can promote cognition, function, diversion,
and reduce falls. The purpose is to evaluate an alternative intervention to decrease
restraints in patients in a Trauma Intensive Care Unit (TICU) and evaluate nurse’s
perceptions regarding restraints. Patients who are admitted to a TICU at a Level
One Trauma Hospital and score CAM-ICU+ with the confusion assessment
method will receive an alternative intervention to decrease restraint use. Methods: Descriptive Correlational Design. Nurses assessed patients for delirium on
admission and every 12 hours using the CAM-ICU. Restraint use was measured
per each occurrence applied in a 24 hour period from 0000–2359. Perceptions
of Restraint Use Questionnaire (PRUQ) was completed by nursing to determine
the importance that nurse’s attribute to reasons for restraint use pre intervention.
Nurses were educated on alternative interventions. Patients who were CAM-ICU
positive were provided an alternative device. Results: Nurses completed 58 completed questionnaires. Mean PRUQ overall was 3.57 (possible range 1-5), indicating nurses had positive attitude toward restraints in certain circumstances. Highest
ranked reason for restraints was “protecting patients from falling out of bed”, 37 or
72.5%, and “protecting patients from falling out of chair”, 34 or 66.7%. Baseline
interventions of PRUQ used by nurses to protect patients included psychosocial
interventions (sitters, family member at bedside, reorientation). During the same
time period, mean and Standard Deviation for restraints per 1000 patient days
pre intervention was 314.1 (35.4). Post alternative interventions included activity
blankets and distraction devices, with restraint use decreased (mean 237.8 and SD
56.4; (p = 0.008). Conclusions: Alternative interventions are low cost, low risk,
noninvasive, and can be implemented at the bedside.
178
CONTINUATION OF AMIODARONE AT DISCHARGE FOR
NEW-ONSET ATRIAL FIBRILLATION IN CRITICALLY ILL
PATIENTS
Robert Nietupski1, Cassandra Bellamy1, Todd Miano1, Mark Mikkelsen1, Christina Candeloro2; 1Hospital of The University of Pennsylvania, Philadelphia, PA,
2
Hospital of the University of Pennsylvania, Philadelphia, PA
Learning Objectives: New onset atrial fibrillation (AF) in the intensive care unit
(ICU) is common and often transient. Amiodarone use is widespread in hemodynamically unstable patients given its short-term side effect profile, but continued
use is associated with multiple long-term severe toxicities. Considering the risks of
chronic therapy, examination of the amiodarone continuation rate at hospital discharge is imperative. Hypothesis: Patients with new onset AF in the ICU are continued on amiodarone at hospital discharge. Factors such as severity of illness and
surgical versus medical care are associated with continuation. Methods: This was
a retrospective cohort study of adult patients who received amiodarone for new
onset AF in medical or noncardiac surgical ICUs between Jan 1 2009 and June 30
2013 at a single academic medical center. Exclusions were previous history of AF,
amiodarone as a home medication, in-hospital mortality, or age less than 18 years.
A multivariable logistic regression was used to identify independent risk factors for
amiodarone continuation at discharge. Results: The study included 177 of 1,016
patients admitted to the ICU with an intravenous amiodarone order. Patients had
a median age of 67 years, 57.0% were male, 68.4% were in the surgical ICU, and
the median APACHE II score was 21. One-hundred and one (57.0%) patients
were continued on amiodarone at discharge. Older age (p = 0.031) and not converting to sinus rhythm (p < 0.001) were associated with amiodarone continuation at discharge. The median (IQR) duration of therapy prior to discharge in
all patients was 8.1 (14.4) days. Of those discharged on amiodarone, 61% had a
cardiology follow-up appointment scheduled. Conclusions: Our institution had
a 57% rate of amiodarone continuation at hospital discharge when initiated for
new onset AF in the ICU. Lack of sinus rhythm and older age were predictive of
continuation. The high incidence of continuation at discharge and 61% rate of
cardiology follow-up warrant future studies that examine amiodarone treatment
duration and management during ICU transitions of care are warranted.
Poster Session: Cardiovascular 4
179
EFFICACY OF CHEMICAL PLEURODESIS WITH DOXYCYCLINE FOR CHYLOUS PLEURAL EFFUSION AFTER CARDIAC
SURGERY
Jason Parker1, Cesar Mesia1, Achintya Moulick2, Randy Stevens1, Jeffrey Cies1,
Viean Tan3, Ramin Nazari1; 1St. Christopher’s Hospital for Children/ Drexel university college of Medicine, Philadelphia, PA, 2St. Christopher’s hospital for Children/ Drexel College of Medicine, Philadelphia, PA, 3Drexel University College
of Medicine/ St. Christopher`s Hospital for Children, Philadelphia, PA
Learning Objectives: Chylothorax in children occurs most frequently as a
complication after surgery for congenital heart disease. Chylothorax is associated with major morbidity, increased length of stay and mortality, particularly in patients with single ventricle physiology Objective: Determine the
efficacy of chemical pleurodesis with doxycycline as a therapeutic modality
for its management after surgery for congenital heart disease. Methods: Medical and surgical databases in our institution were used to identify all patients
who had surgery for congenital heart disease and subsequently experienced
postoperative chylous pleural effusion. Among them, those patients with chylous effusion who received chemical pleurodesis were identified. Data were
collected regarding patients’ demographics, procedures, any underline genetic
disorders, chylous drainage and its management and outcomes. Procedure
complexity was assessed by Risk Adjustment for Congenital Heart Surgery
Medical records were reviewed and daily chest drainage before and during
pleurodesis were recorded. Results: From January 2011 to December 2013,
445 cardiac operations were followed by 11 cases of chylous pleural effusion,
for an incidence of 2.5%. All patients firstly were managed by fat-free diet or
total parentral nutrition. Somatostatin analogue (Octreotide) was used adjunctively in 3 patients and no decrease in daily output was observed. The mean
duration of pleurodesis was 5.7 days with range of 2-8 days. Nine patients (81
%) responded favorably to the first course of pleurodesis, and two patients
(19 %) required more than one course of pleurodesis. There were no allergic
reaction or any other side effect related to chemical pleurodesis. Conclusions:
Chemical pleurodesis with doxycycline is a safe and effective method for treating chylous effusion after surgical treatment of congenital heart disease, especially after failed conservative treatment. However, some patients may need
more than one pleurodesis.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
180
SEVERE PULMONARY HYPERTENSION AND RHF TREATED
WITH ECMO PRIOR TO DOUBLE LUNG TRANSPLANT
Michael Kim1, Benjamin Scott2, Breandan Sullivan3, Martin Zamora4; 1University
of Colorado Health Science Center, Denver, CO, 2University of Colorado, Aurora,
CO, 3University of Colorado, Denver, Aurora, CO, 4University of Colorado, N/A
Learning Objectives: Veno-veno ECMO,as a bridge to lung transplantation, can
allow patients with end stage disease to be liberated from mechanical ventilation.
With increased use of double lumen right IJ ECMO cannulas, patients may have
an opportunity for a safer bridge to lung transplantation Methods: We present the
case of a woman with familial pulmonary hypertension who was transferred to our
institution with an admitting diagnosis of line sepsis, acute on chronic hypoxic
respiratory failure due to pulmonary hypertension and right heart failure. Her diagnostic cath procedure 2 months prior to admission revealed an elevated RA pressure of 15mmHg and mean PA pressure of 60mmHg. During this admission, we
were able to control her pulmonary hypertension with high dose IV Treprostonil,
Bosentan, and Tadalafil. Initially, she was recovering well, but on hospital day 23
acutely decompensated. This prompted the cannulation for veno-venous ECMO as
a bridge to lung transplant. On VV ECMO, she was able to ambulate while requiring only 5L via NC. After 3 weeks of VV ECMO, her course was complicated by
sepsis from her right IJ catheter, which progressed to pressor dependent cardiogenic
shock. She was continued on VV ECMO via femoral vessels. This post-operative
course was complicated by GI bleeding, leading to refractory hypotension and
worsening heart failure, leading to veno-arterial ECMO. Four days after initiation
of VA ECMO, she successfully underwent orthotopic double lung transplantation.
She is currently recovering from her transplant and her heart failure. Results: None.
Conclusions: In conclusion, to the best of our knowledge, the present case represents one of the first successful uses of both VV and VA ECMO as a bridge to lung
transplantation in these chronic pulmonary hypertension patients with refractory
right heart failure. Despite the complications associated with mechanical circulatory support, its use may be the only viable option for patients who are refractory
on advanced medical therapy and awaiting lung transplantation.
181
TRANSFUSION RELATED PULMONARY COMPLICATIONS
IN CARDIOVASCULAR SURGICAL PATIENTS
Aravindh Ganapathy1, Faisal Masud1, Asma Zainab1; 1Houston Methodist Hospital, Houston, TX
Learning Objectives: Transfusion Related Acute Lung Injury (TRALI) is a complication of blood transfusion and is clinically defined. It can be differentiated
into classic TRALI (antibody-mediated) and non-antibody mediated TRALI.
Non-antibody mediated TRALI has been recently defined and its incidence
is variably reported, warranting further analysis. As transfusions are associated
with increased morbidity and mortality in cardiac surgical patients, we investigated non-antibody mediated TRALI’s incidence and risk factors in CVICU
patients. Methods: Over one year, 94 patients were enrolled in this prospective
study, who underwent cardiovascular surgeries leading to CVICU admittance
and received blood transfusions 6-24 hours prior to enrollment. Patients with
pre-existing ALI, ARDS, respiratory insufficiency, and pulmonary edema were
excluded. Data collection included number of transfusions, PaO2/FiO2 ratio,
bilateral infiltrates on chest X-ray, pulmonary pressures, number of ventilator
days, and renal insufficiency (creatinine > 1.4 mg/dl). Analysis was performed
using Chi-square and two-sample t-test, both with α=0.05. Correlation between
TRALI and cardiopulmonary bypass pump (CPB) was also studied. Results:In
CVICU patients, our calculated TRALI incidence was 0.309 with a binomial
probability of 0.088. CPB use was not correlated with an increased incidence of
non-antibody mediated TRALI. The Chi-square value was 3.0777 with a p-value
of 0.0793. Furthermore, renal insufficiency did not correlate (p = 0.638) with
TRALI status. When comparing number of ventilation days between patients
with and without TRALI, two-sample t-test showed no significant difference (t =
1.626 and t-crit = 2.160) between the groups. Conclusions: This study compared
pump use within a group of cardiac surgical patients who required transfusions.
Our results demonstrate that blood transfusion is not associated with increased
incidence of non-antibody mediated TRALI in CVICU patients compared to
other critically ill patients. Furthermore, CPB use, when compared to non-CPB
use, does not increase incidence of non-antibody mediated TRALI.
182
CORRELATION BETWEEN P WAVE DURATION ON ADMISSION AND NURSING AND SEVERITY INDEXES IN ICU
PATIENTS.
Aristeidis Vakalos1, Eleni Drampala2; 1Xanthi General Hospital, Xanthi, Greece,
2
ICU, Xanthi General Hospital, Xanthi, Greece
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Learning Objectives: P wave duration longer than 120 ms may indicate left
atrial enlargement, classically due to mitral stenosis. In association with ventricular hypertrophy may indicate systemic hypertension, aortic stenosis, and hypertrophic cardiomyopathy. All these clinical situations may impair physiological
status and may have an impact on ICU hospitalization indexes. The aim of our
observation retrospective study was to test the hypothesis that a correlation exists
between p wave duration in ICU patients on admission ECG, and nursing and
severity indexes in our both medical and surgical ICU served in community hospital. Methods: From October to December 2013 we looked for p wave duration (ms) in ECG automatically analyzed on admission in 48 ICU patients who
survived ICU. Mean age (years) 60.06, mean APACHE II score on admission:
23.28, mean length of ICU stay (LOS, days): 8.43, mean duration of mechanical
ventilation (VD, days): 5.41, Predicted Mortality (%).Using linear correlation
method, we looked for linear slope, correlation coefficient (r), and coefficient
of determination (r2), and by linear regression method using ANOVA test we
looked for p value, according p wave duration and nursing (LOS, VD) and severity (age, APACHE, Predicted mortality) indexes. Results: Index / Slope / St.
Error / r / r2 / L. CI / U CI / P value Age / 0.575 / 0.115 / 0.633 / 0.401 / 0.341
/ 0.810 / 0.0001 APACHE / -0.091 / 0.061 / -0.238 / 0.056 / -0.216 / 0.032 /
0.1438 Pr. Mort / -0.256 / 0.207 / -0.199 / 0.039 / -0.678 / 0.164 / 0.2246 LOS
/ -0.076 / 0.088 / -0.141 / 0.019 / -0.254 / 0.102 / 0.3919 V.D / -0.035 / 0.079
/ -0.073 / 0.005 / -0.197 / 0.125 / 0.6572 Conclusions: According to our data,
there was no statistically significant correlation detected between p wave duration
and APACHE, Pr Mort, LOS nor VD. On the other hand, there was statistical
extremely significant, moderate positive linear correlation between p wave duration and age. Our data suggest that p wave duration in mixed ICU patients (not
specially coronary) on admission ECG may not be used as an accurate severity
index or as a prognostic nursing index.
183
THE RELATION BETWEEN INTERLEUKIN-18 AND ACUTE
CORONARY SYNDROME
Samir Hegazy1, Tarek Elbadawy2, Mona Ayad2, Amr Mohamed3; 1Faculty of
Medicine, Alexandria University, alexandria, Egypt, 2Faculty of Medicine, Alexandria university, alexandria, Egypt, 3Faculty of Medicine, Alexandria university,
a, Egypt
Learning Objectives: Atherosclerosis is a complex multifactorial process resulting from an excessive inflammatory response to various forms of injurious stimuli
to the arterial wall (1-4). Interlukin-18 (IL-18), through activation of myocytes
macrophages, lymphocytes and endothelial cells, may has the potential to promote both atherosclerotic plaque instability and systemic inflammatory responses
(5) Methods: a prospective cohort study was carried out on sixty patients presenting with chest pain to the critical care medicine department of the Alexandria main university hospital. Patients divided into three groups (patients with
unstable angina, patients with ST segment elevation myocardial infarction and
successful thrombolytic therapy and patients with ST segment elevation myocardial infarction and failed thrombolytic therapy). all patients subjected to to full
history taking including the demographic data, historical data for the present
condition, cardiovascular risk factors as smoking, DM, HTN & IHD, other comorbidities and drug history. Thorough clinical examination carried out on every
subject including 12 lead ECG. Laboratory investigations also done and included:
Troponin I, CK-MB and IL-18 Results: In all patient groups, IL-18 was lower
in presence of complications but without statistical significance. Conclusions:
IL-18 is a protective cytokine released as an anti-inflammatory response counteracts the inflammation associated with atherosclerotic plaque disruption, which
causes ACS, so its high level indicates good protection against complications
184
EVOLUTION OF LIVER FUNCTION AFTER INITIATION
OF VENO-ARTERIAL EXTRACORPOREAL MEMBRANE
OXYGENATION
Irene Lamanna1, Elio Antonucci2, Antonio Dell’Anna1, Jean-Louis Vincent3,
Daniel De Backer3, Fabio Silvio Taccone1; 1Erasme Hospital, Brussels, Belgium,
2
Erasme Hospital, Bruxelles, Belgium, 3Erasme University Hospital, Brussels,
Belgium
Learning Objectives: Veno-arterial (VA) Extra Corporeal Membrane Oxygenation (ECMO) has become a lifesaving procedure for the management of lifethreatening cardiopulmonary failure. Liver function has not been well studied
during VA-ECMO. Methods: In a retrospective analysis of our institutional
ECMO database (n=162) from November 2008 to December 2013, for patients
with survival of 48 hours or more, we collected aspartate (AST) and alanine transaminases, lactate dehydrogenase (LDH), prothrombin time (PT), total bilirubin
and fibrinogen at time of ECMO initiation (baseline) and then once a day for
the following 3 days. Elevated liver enzymes (ELE) were defined if AST and/or
ALT were > 200 UI/L. Repeated measures were analysed using two-way ANOVA.
Results: A total of 69 patients were included; 2 patients received VA ECMO for
severe ARDS associated with cardiac failure, 15 for refractory cardiac arrest and
52 for cardiogenic shock. Of them, 28 (41%) had ELE at the moment or immediately after ECMO initiation (median AST 482[345-1802] UI/L and median
ALT 401 [177-1215] UI/L. There was a significant increase in PT and bilirubin
and a decrease in AST over the study period, while other tests did not change significantly. PT and fibrinogen values were significantly higher in survivors (n=32)
than non-survivors (n=37. Among the 28 patients with ELE, 9 had a further
elevation in AST/ALT and 6 eventually died with multiple organ failure. Of the
19 patients with reduction of AST/ALT, only 7 normalized their levels within 3
days since ECMO initiation. The reduction in AST/ALT after ECMO initiation
was more frequent in survivors (12/15) than in non-survivors (7/13). Conclusions: A substantial proportion of patients needing VA-ECMO have early ELE,
which usually improves over time, especially in the survivors. PT and fibrinogen
values are also higher in survivors than non-survivors. Recovery of normal liver
function needed more than 3 days in most of patients.
185
GOAL DIRECTED ECHOCARDIOGRAPHY BY NON-CARDIOLOGIST IN CRITICALLY ILL PATIENTS; EGYPTIAN
EXPERIENCE
Ahmed Hasanin1, Ahmed Mukhtar1, Ahmed Gado1, Reham Mahros1; 1Cairo
University, Cairo, Egypt
Learning Objectives: Goal directed echocardiography (GDE) done by non-cardiologist intensive care physician is a useful tool for hemodynamic monitoring in
critically ill patients (1). Although many studies in literature reported the benefit of
GDE in intensive care unit (ICU), its impact on patient’s outcome was not reported.
In this study we evaluated our experience in a surgical ICU in Cairo University
with the impact of GDE on diagnosis of the cause of shock as well as the patient
outcome Methods: All critically ill non-bleeding hypotensive patients admitted to
our ICU for six months were enrolled in the study. Goal directed echocardiography
(GDE) was done by 3 trained intensivists. Four views were examined in each patient;
Parasternal long axis view (PLAV), Parasternal short axis view (PSAV), Apical four
chamber view (A4CV), and subcostal view (SV). Two dimensional eyeballing technique was used to determine pump failure, hypovolemia, right side enlargement,
and cardiac tamponade. Neither M-mode nor Doppler was used in GDE. Estimated
cause of shock was reported before and after GDE as well as seven day outcome
of the patients Results: Fifty four consecutive patients were included in the study.
The estimated causes of shock before GDE were; distributive shock (53.6%), pump
failure (32.1%), hypovolemia (5.4%), and obstructive shock (5.4%). After GDE;
causes of shock were; hypovolemia (37.5%), pump failure (19.6%), obstructive
shock (16.1%), and distributive shock (10.7%). The most clearly visualized view
in this cohort was A4CV [52 cases (92%)], followed by PSAV [45 cases (80.4%)],
PLAV [44 cases (78.6%)], and subcostal view [38 cases (67.9%)] GDE changed
the diagnosis in 35 cases (62.5%), confirmed the diagnosis in 12 cases (21.4%) and
didn’t reach a diagnosis in nine cases (16.1%). Seven days mortality was lower in
patients whom GDE determined the cause of shock compared to in those whom the
cause of shock was not diagnosed (66.7% Vs 100%, P=0.05) Conclusions: GDE
performed by non-cardiologists was beneficial in improving the diagnosis as well as
the seven day outcome of shocked patients in the ICU
186
ASSESSING HEMORRHAGE SEVERITY WITH CONTINUOUS
AUTOMATIC HEART-RATE-COMPLEXITY MONITORING IN
SWINE
Slava Belenkiy1, Timothy Park2, William Baker3, Bryan Jordan3, Michael
Dubick4, Jose Salinas4, Leopoldo Cancio4, Andriy Batchinsky5; 1Untied States
Army Institute of Surgical Research, Fort Sam Houston, TX, 2San Antonio Military Medical Center, Fort Sam Houston, TX, 3Untied States Army Institute of
Surgical Research, Fort Sam Houston, TX, 4United States Army Institute of Surgical Research, Fort Sam Houston, TX, 5United States Army Institute of Surgical
Research, Fort San Houston, TX
Learning Objectives: Heart-rate-complexity (HRC) calculated off-line was associated with injury severity, mortality, and the performance of life-saving interventions
in animal and human studies. We hypothesized that real-time automatic HRC measurements by the Aesculon monitor (Cardiotronic-Osypka Medical, USA) are associated with hemodynamic status and mortality. Methods: Spontaneously breathing
consciously sedated swine were shed 65% of blood volume over 1 hour, then were
randomized to 3 groups: control (C, n=7); transfusion of shed blood (TSB, n=7);
or endovascular balloon occlusion of the aorta (REBOA) (Pryor Medical, Arvada,
CO) for up to 60 minutes followed by TSB (n=21). Epinephrine boluses were
given if mean arterial pressure (MAP) < 40 mmHg in the TSB and REBOA groups.
After resuscitative interventions, animals were followed for 240 min or death. Aesculon monitor performed continuous, real-time measurements of HRC, i.e. sample
entropy (SampEn) and multiscale entropy (MSE). At 30 minutes after all interventions, heart rate (HR), MAP, Lactate (Lac), and HRC metrics were assessed for their
association with death using logistic regression and receiver-operating-characteristic
(ROC) curve analysis. Results: All animals died in group C, 2/7 in group TSB,
and 1/21 in group REBOA. SampEn and MSE decreased with hemorrhage and
increased after interventions (TSB or REBOA+TSB). After resuscitative interventions, HRC metrics individually were associated with death: SampEn p=0.0002,
area under the curve (AUC) =.88; MSE p=0.002, AUC=.83; both SampEn and
MSE together p=0.0005, AUC=.90. Traditional vital signs were also associated with
death: HR, p=0.02, AUC .72; MAP, p=0.01, AUC .85; Lac p=0.05, AUC=.69;
and for all three metrics together p<0.03, AUC=0.85. When traditional and HRC
variables were combined into a single model the overall AUC was .93, p=0.003.
Conclusions: Real-time unsupervised calculation of HRC by the Aesculon monitor improves diagnosis of hemorrhage severity and is significantly associated with
mortality in a model of non-compressible hemorrhage treated with REBOA.
187
ECG STUDY IN ICU PATIENTS: QTC INTERVAL.
Aristeidis Vakalos1, Eleni Drampala2; 1Xanthi General Hospital, Xanthi, Greece,
2
ICU, Xanthi General Hospital, Xanthi, Greece
Learning Objectives: Causes of prolonged QT interval corrected (QTc) which
is calculated by Bazett’s Formula, include cardiomyopathy, severe bradycardia,
high-grade AV block, anti-arrhythmics, hypothyroid and hypothermia. Normal
QTc ≤ 440 msec.The aim of our observation retrospective study was to test the
hypothesis that a correlation and a shift exists in QTc interval in ICU patients
on admission and discharge ECG, in our both medical and surgical ICU served
in community hospital. Methods: From October to December 2013 we looked
for QTc (ms) in ECG automatically analyzed on admission and discharge in 48
ICU patients who survived ICU. We looked for statistical significant difference (p
value two tailed) between the mean values of admission and discharge, using the
unpaired Mann - Whithney test (nonparametric) or the unpaired t test Welch corrected (parametric), according to the normality test, which was obtained using Kolmogorow – Smirnov method. Using linear correlation method, we looked for linear
slope, correlation coefficient (r), and coefficient of determination (r2), and by linear
regression method using ANOVA test we looked for p value according QTc interval
on admission and discharge. Results: Comparison between QTc values on admission and discharge (/) Mean: 443.21 / 426.84, St Dev: 32.09 / 28.34, St Error: 4.73
/ 4.17, Min: 383 / 372, Max: 529 / 510, Lower C.I: 433.68 / 418.42, Upper CI:
452.76 / 435.27, p value: 0.0023 Correlation between QTc values on admission
and discharge: Slope: 0.315, St Error: 0.124, r: 0.35, r2: 0.127, Lower CI: 0.064,
Upper CI: 0.566, p value:0.0149 Conclusions: According to our data, there was
statistically very significant difference detected in QTc interval between admission
and discharge, by means that QTc interval on discharge was lower. On the other
hand there was statistical significant, moderate positive linear correlation between
QTc interval on admission and discharge. Our data suggest that QTc interval in
our ICU patients shifted to lower values on discharge, assuming that causes of QTc
interval variation on admission were solved during ICU hospitalization.
Poster Session: Cardiovascular 5
188
THE PREVALENCE OF CHRONIC ATRIAL FIBRILLATION:
PRE-OPERATIVE FACTORS ASSOCIATED
I Macias-Guarasa1, De Miguel-Aparicio F.J.1, R. Gutierrez-Rodriguez, M.D.1
Arias-Verdu, R. Rivera-Fernandez1; 1Hospital Regional Carlos Haya, Malaga,
Spain
Learning Objectives: The objetive or our study is to identify risk factors associated with the increase in the prevalence of pre-operative chronic atrial fibrillation
in patients subjected to cardiovascular surgery. Methods: A retrospective study
of patients admitted to our intensive care unit between 2009 - 2012. Exclusion
factors: none. Variables analysed: sex, age, ICU and hospital mortality. Type of
surgery: bypass, coronary artery, valve replacement (isolated, double or combined
with a bypass, or aortic tube). Scores gravity (APACHE II, Charlson Index and
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Euroscore). Presence of cardiovascular risk factors,chronic or paroxysmal atrial
fibrillation, ischemic cardiopathology, depressed ejection fraction, previous renal
insufficiency. Statistics used: mean, typical deviation. Analysis of qualitative
variables by chi square, quantitative variables analysed according to the Student
T test. Multivariable analysis by logistical regression Results:243 patients were
studied. Mean age 67.5 ± 12 years. Mean Charlson Index 4.5 ± 2, APACHE II
15.3 ± 6.5, Euroscore 9.05. Hospital Mortality 14.4%. The sample studied is
divided into two groups according to the presence of previous atrial fibrillation,
30.5%. In the single variable analysis the following factors were linked significantly, P< 0,05, to the presence of pre-operative atrial fibrillation: advanced age
> 65 years old, 36%, female, 42%, and those having had double prosthetic valve
surgery, 64%. In multi-variable analysis the following factors were linked independently to the higher prevalence of atrial fibrillation, female gender, OR 10.7
(CI 95%, 2.29-48), and the need for a double valve replacement OR 7.3 (CI
95%, 1-12,7). There was no link found between mortality and previous atrial
fibrillation, but greater postoperative morbidity with an increase in the rate of
postoperative atrial fibrillation, 66.2%, which was linked significantly, P < 0.005,
pleural effusion, 52%, and prolonged stay 51% (significant difference P< 0,05).
Conclusions: previous atrial fibrillation does not seem to reduce survival rates,
but it does cause as greater postoperative morbidity
189
CORRELATION OF INTRACELLULAR HISTAMINE AND
CLINICAL SYMPTOMS IN ANAPHYLACTIC PATIENTS
Satoshi Yamaga1, Satoshi Morioke2, Shinichiro Ohshimo1, Kei Suzuki1, YASUMASA IWASAKI1, Nobuyuki Hirohashi1, Michihiro Hide2, Koichi Tanigawa1;
1
Department of Emergency and Critical Medicine,Hiroshima University, Hiroshima, Japan, 2Department of Dermatology,Hiroshima University, Hiroshima,
Japan
outcomes included other adverse events, intensive care unit length of stay following cardiac surgery, 30-day readmission for a cardiac cause and 30-day mortality
rom a cardiac cause. A p-value <0.05 was considered significant. Results: POAF
occurred more frequently in the non-ranolazine group (41.9%) compared with
the ranolazine group (10.1%) in unmatched analysis (p<0.0001) After adjusting
for potential sources of bias through propensity score matched pairs and conditional logistic regression, ranolazine was an independent predictor of preventing
POAF (p<0.0001). No significant difference was found in the length of stay in
the intensive care unit following cardiac surgery. The ranolazine-treated patients
had a significant reduction in readmission for a cardiac cause within 30 days
(p=0.046) in the unmatched analysis that was not retained in matched analysis.
No difference was found in 30-day cardiovascular mortality. Early, symptomatic
hypotension occurred more frequently in the ranolazine group although this difference did not persist after 72 hours. Conclusions: Ranolazine was independently associated with a significant decrease in POAF development after CABG
and valve surgeries.
191
EFFECT OF DEXMEDETOMIDINE ON POSTOPERATIVE
TACHYARRHYTHMIAS AFTER VALVULAR SURGERY
Daryl Glick1, Mona Patel2, Hannah Wunsch3, Gregg Rosner4, Jorie Frasiolas2;
1
Kingsbrook Jewish Medical Center, Brooklyn, NY, 2NewYork-Presbyterian Hospital, Columbia University Medical Center, New York, NY, 3Sunnybrook Health
Sciences Centre, Univ of Toronto, Toronto, ON, 4Columbia University, New
York, NY
Learning Objectives: Histamine plays an important role in the development of
anaphylaxis. However, elevated plasma levels of histamine have not been observed
in the majority of anaphylaxis.The aim of our study was to investigate the correlation between the levels of intracellular histamine and clinical symptoms in anaphylaxis. Methods: We collected blood samples of patients with anaphylaxis who
were admitted to our ICU. In addition to clinical characteristics, routine blood
analysis including C-reactive protein (CRP), treatments, outcomes, and levels of
intracellular histamine were evaluated. The levels of intracellular histamine were
defined as the difference between the levels of histamine in whole blood and in
plasma. We used high-performance liquid chromatography (HPLC) to analyze
histamine levels. Results:Consecutive 16 patients (12 males and 4 females) with
anaphylaxis admitted to our ICU were enrolled. Mean age was 54.7 ± 18.3 years.
Clinical characteristics included hypoxemia (n=8), shock (n=15), decrease levels
of CNS (n=10) and severe abdominal impairment (n=5). No patient has died.
The levels of intracellular histamine were inversely correlated with the severity of
shock (p=0.044), decrease levels of CNS (p=0.0056) and abdominal impairment
(p=0.0038), whereas histamine levels in plasma varied widely. Higher CRP levels
were also correlated significantly with abdominal impairment (p=0.046). Conclusions: The decrease of intracellular histamine is correlated with poor organ
perfusion in anaphylaxis, i.e. severe shock, decrease levels of CNS and abdominal
impairment. Elevated levels of CRP, which characterize a late-phase response in
immediate hypersensitivity reactions, may support these findings. The results of
our study indicate that the magnitudes of degranulation of mast cells and/or
basophils may be associated with the severity of shock in anaphylaxis.
Learning Objectives: Postoperative tachyarrhythmias occur in up to 50% of
patients after valvular surgery and are associated with increased intensive care
unit (ICU) and hospital lengths of stay, healthcare costs, and mortality. Dexmedetomidine, a central alpha2-agonist commonly used for sedation after cardiac surgery, may exhibit inhibitory effects on supraventricular and ventricular
tachyarrhythmias due to its sympatholytic properties. The objective of this
retrospective review was to evaluate the effect of dexmedetomidine on tachyarrhythmias following valvular surgery. Methods: An IRB-approved retrospective
chart review was conducted in adult patients who underwent isolated open aortic or mitral valve repair or replacement from June 2012 to June 2013. Exclusion criteria were reoperation, heart failure requiring inotropes, left ventricular
ejection fraction < 20%, liver disease, diabetes requiring insulin, end-stage renal
failure, chronic obstructive pulmonary disease on home oxygen, severe systemic
disease, and use of mechanical circulatory support between postoperative days
zero and seven. Total postoperative dexmedetomidine, occurrence of tachyarrhythmias, hypotension, and bradycardia were recorded for each patient. Data are
presented as median (interquartile range). A p<0.05 was considered significant.
Results: There were 114 patients randomly selected for inclusion. Postoperative
tachyarrhythmias occurred in 33 patients (58%) who received dexmedetomidine,
compared to 36 patients (63%) who did not; p=0.57. Patients in the dexmedetomidine group received a total dose of 1 mcg/kg (0.6, 2) for a duration of 3
hours (2, 5). Postoperative hypotension occurred more frequently in patients who
received dexmedetomidine compared to those who did not (53% versus 36%);
p<0.01. There was no difference in length of ICU or hospital stay, duration of
mechanical ventilation, or postoperative complications. Conclusions: The use
of dexmedetomidine did not influence the development of tachyarrhythmias,
though patients in this cohort had a low severity of illness and received dexmedetomidine for a short duration.
190
192
SHORT-COURSE OF RANOLAZINE PREVENTS POST-OPERATIVE ATRIAL FIBRILLATION FOLLOWING CARDIAC
SURGERIES
EFFECT OF V-V ECMO FLOW RATES ON IVC DIAMETER
VARIATION ON TRANS-THORACIC ECHOCARDIOGRAPHY.
Drayton Hammond1, Carmen Smotherman2, Christopher Jankowski3, Stephen
Tan3, Omeni Osian3, Dale Kraemer2, Marci DeLosSantos3; 1University of Arkansas for Medical Sciences, Little Rock, AR, 2Center for Health Equity and Quality
Research, Jacksonville, FL, 3UF Health Jacksonville, Jacksonville, FL
Learning Objectives: Postoperative atrial fibrillation (POAF) is a common complication arising after coronary artery bypass grafting (CABG) and valve replacement or repair surgeries that is associated with increased mortality, morbidity
and cost. The purpose of this study was to evaluate the effect of ranolazine for
POAF prevention following CABG and valve replacement and repair surgeries.
Methods: This IRB-approved, retrospective, cohort study evaluated 205 patients
who received either ranolazine (1,000 mg preoperatively, followed by 1,000 mg
twice daily for 7 days) or no ranolazine in combination with standard perioperative care surrounding CABG, valve or combination surgeries. The primary
outcome, POAF development within 7 days of cardiac surgery, was analyzed with
the Fisher exact test before and after propensity-score matched pairs analysis.
Conditional logistic regression and log-rank tests were performed. Secondary
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Killol Patel1, David Baran2, Habib Nazir2, Thiruvengadam Anandarangam2;
1
Newrak Beth Israel Medical Center, Newark, NJ, 2Newark Beth Israel Medical
Center, Newark, NJ
Learning Objectives: Inferior Vena Caval (IVC) diameter variation has never
been evaluated in patients on Veno-Venous Extracorporeal Membrane Oxygenation (V-V ECMO). We wanted to see if there is any correlation between
flow rates and its effect on IVC variation / distensibility. Methods: 5 data points
were recorded on three patients requiring V-V ECMO therapy. IVC diameter
(D) at end-expiration (Dmin) and at end-inspiration (Dmax) was measured by
M-mode during echocardiography using a subcostal approach. The distensibility
index of the IVC (dIVC) was calculated as the ratio of Dmax - Dmin / Dmin,
and expressed as a percentage. Results: Flow rate had an inverse correlation
with dIVC as seen on our data-points. All our patients had a normal fluid status prior to placement on V-V ECMO as noted on right heart catheterization.
Two data points were obtained on conventional mode of ventilation (Pressure
Regulated Volume Control) whereas the other three were obtained on airway
pressure release ventilation (APRV). dIVC changed from 50% to 20% in patient
1 with increase in his flow rates from 3300 ml/min to 4200 ml/min inspite of the
decrease in Dmax from 2.00 cm to 1.48 cm. Similarly for patient 2 when flow
rates were kept constant the dIVC only changed from 80% to 90% with decrease
in Dmax from 1.40 cm to 0.95 cm. The third patient had a dIVC of 20% with
flow rates of 4500 ml/min with a Dmax of 1.33 cm. Conclusions: It has been
found that dIVC can be used an accurate predictor of volume responsiveness in
septic patients on conventional ventilation. Flow rates have an inverse correlation
with dIVC in patients on V-V ECMO. With the increase in flow rates, there
might be an increase in inflow of blood from the IVC preventing it from developing the variation which would normally be seen. Also the presence of the catheter
in the vessel might alter the distensibility index. There have been no previously
reported studies looking at IVC variation/distensibility in V-V ECMO patients;
our study may give preliminary data in assessing the correlation between the flow
rates and dIVC.
193
DATA DRIVEN PERSONALIZED RISK PREDICTION IN PEDIATRIC INTENSIVE CARE UNITS
Chih-Wen Cheng1, Kevin Maher2, May Wang1, Nikhil Chanani3; 1Georgia
Institute of Technology, Atlanta, GA, 2Children’s Healthcare of Atlanta Emory
University, Atlanta, GA, 3Emory University, Children’s Healthcare of Atlanta At
Egleston, Atlanta, GA
Learning Objectives: Clinicians in ICUs rely on standardized scores as risk prediction models to predict a patient’s vulnerability to life-threatening events. Current scales calculate scores from a fixed set of conditions collected within a specific
time window. However, modern monitoring technologies generate complex, temporal, and multimodal patient data that conventional prediction scales cannot
fully integrate into clinical practice. Thus, a more sophisticated model is needed
to tailor individual characteristics and incorporate multiple temporal modalities
for a personalized risk prediction. Methods: We have developed a novel ICU
risk prediction system, called “icuARM-II”, using a pediatric ICU database from
Children’s Healthcare of Atlanta (CHOA). This novel database contains clinical
data collected in 5,739 ICU visits from 4,975 patients over one year. We propose
a temporal rule-mining framework to predict clinical risks based on all available observed conditions without being restricted by a fixed observation window.
We introduce a scanning strategy to count temporal association rules. We then
applied classification-based rule generation to produce a decision list. Given a
decision list, we proposed a classification approach, using the principle of leaveone-out cross validation, to calculate a new reliability metric. icuARM-II also
features an interactive user interface to enable the real-world clinical decision
support. Results: The proposed framework was tested using the clinical lab dataset for the prediction of short-term (i.e., 2-hr) ICU mortality. Using icuARM-II,
our results not only outperform conventional Classification Based on Association
in all 12 selected lab tests, but also suggest important usability, including quality
assessment of individual tests, evaluation of interactions among tests, suggestion
of additional tests, and investigating the change of observation length. Conclusions: Manifesting a real-time interactive user interface, we has demonstrated a
new solution for real-time and reliable risk prediction using personalized clinical
data that can have a direct impact on critical care.
194
RISK FACTORS FOR DEXMEDETOMIDINE-ASSOCIATED
HEMODYNAMIC INSTABILITY IN NON-CARDIAC ICU
PATIENTS
Calvin Ice1, Heather Personett2, Erin Frazee2, Ross Dierkhising1, Rahul Kashyap1,
Richard Oeckler3; 1Mayo Clinic, Rochester, MN, 2Mayo Clinic-Saint Mary’s
Hospital, N/A, 3Mayo Graduate School of Medicine, Rochester, MN
Learning Objectives: The reported incidence of hypotension and bradycardia occurring in patients receiving dexmedetomidine (Dex) for sedation varies
but commonly exceeds 50%. The purpose of this study is to describe the incidence and significance of Dex-associated hemodynamic instability (HDI) and
to identify patient- and treatment-specific risk factors with which it is related.
Methods:We conducted a retrospective cohort study of non-cardiac ICU adults
receiving Dex for sedation from 11/1/12 to 10/31/13. The primary endpoint was
HDI, a composite of hypotension and/or bradycardia, defined as systolic blood
pressure (BP) <80 mmHg, diastolic BP <50 mmHg, or heart rate <50 beats per
minute during Dex therapy. Cox proportional hazards models were constructed
to determine hazards ratios (HR) and 95% confidence intervals (CI) for risk factors of HDI. Secondary endpoints were the total number of HDI events and
number of clinical interventions required. Results: HDI occurred in 197 of the
analyzed 300 patients receiving Dex, which resulted in cumulative incidence of
71% at 24 hours via Kaplan-Meier estimate and median time-to-event of 4.25
hours. Univariate analysis identified age (HR 1.15 per 10 years, 95% CI 1.061.25, p=0.001) and low baseline BP (HR 2.40 at Dex start, 95% CI 1.70-3.37,
p<0.0001) to be associated with increased risk of HDI. Multivariable analysis
demonstrated independent associations between age (HR 1.23 per 10 years, 95%
CI 1.10-1.38, p<0.001) and low baseline BP (HR 2.42 at Dex start, 95% CI
1.68-3.49, p<0.0001) and risk of HDI. A total of 435 HDI events were evaluated, and 210 events (48%) required ≥1 clinical intervention, the most common
of which was Dex dose decrease (28%). Conclusions: HDI occurs commonly in
critically ill adults receiving Dex, with over two-thirds of this cohort experiencing
hypotension and/or bradycardia within 24 hours of initiation. Increasing age and
low baseline BP were associated with the development of HDI. These findings
suggest clinicians should carefully weigh the potential risks and benefits of using
Dex in patients with advanced age or low baseline BP.
195
RESULTS OF A RESTRICTIVE V. LIBERAL TRANSFUSION
STRATEGY IN NEONATAL AND INFANT CARDIAC SURGERY.
Jill Cholette1, Jeffrey Rubenstein1, Kelly Henrichs1, Karen Powers1, Louis Daugherty1, Michael Swartz1, George Alfieris1, Neil Blumberg1; 1University of Rochester, Rochester, NY
Learning Objectives: The purpose of this study is to determine if a restrictive
transfusion strategy is tolerated in neonates and infants requiring surgical palliation or repair for congenital heart disease. We hypothesized that a restrictive
red cell transfusion strategy would decrease red cell transfusions without affecting arterial lactate or clinical outcomes. Methods: A prospective, randomized,
non-inferiority controlled clinical trial of infants’ ≤ 10kg with congenital heart
disease following surgery randomized to a restrictive v. liberal transfusion strategy.
Restrictive group: red cells were transfused for any hemoglobin (Hb) < 7.0 g/dL
for biventricular repair, or <9.0 g/dl for palliative procedure. Liberal group: red
cells were transfused for any Hb < 9.5 g/dL for repair; or <12 g/dl for palliation.
Primary endpoint was LacTime (% time arterial lactate > 4.0 mmol/L). Secondary endpoints were Hb, transfusion and clinical outcome data. Results: Of 162
infants studied; 72 (44%) were neonates. Mean age was 100 ± 127 days; mean
weight was 4.7 ± 1.8 kg. Pre and intra-op characteristics were similar between
groups. The restrictive group received fewer RBC transfusions and exposures than
the liberal group (p < 0.001). 56 infants underwent palliative procedures (29
restrictive; 27 liberal) and 106 (52 restrictive; 54 liberal) underwent biventricular
repair. For palliated subjects the restricted group had lower Hb levels [10.9 ± 0.4
v. 13.7 ± 0.3 g/dl (p < 0.001)] without a significant difference in LacTime [4.0%
v. 2.6% (p = 0.59)]. Similarly, biventricular subjects in the restrictive group had
lower Hb levels [9.4 ± 0.9 v. 11.8 ± 0.9 g/dl (p < 0.001)] with no significant difference in LacTime [0.05% v. 0.8% (p=0.29)]. There were no clinical outcome
differences between groups. 5 subjects required ECMO (2 restrictive, 3 liberal).
30 day survival was 96%; 5 of 6 deaths (83%) (p = 0.21) occurred in the liberal group. Conclusions: Despite their medical complexity, neonates and infants
undergoing cardiac surgical palliations and repairs can be managed safely with a
restrictive transfusion strategy.
196
USING ABDOMINAL NIRS TO PREDICT GASTROINTESTINAL MORBIDITY IN NEONATES AFTER CARDIAC SURGERY
Rhiannon Hickok1, Darren Klugman1, John Berger1, Michael Spaeder1, Jennifer
Schuette1; 1Children’s National Medical Center, Washington, DC
Learning Objectives: Despite recent advances in the care of newborns following surgery for congenital heart disease (CHD), post-operative gastrointestinal (GI) morbidities such as necrotizing enterocolitis (NEC) are prevalent.
The development of NEC in newborns is associated with a longer length of
stay and neonates with single ventricle physiology who develop NEC have
increased mortality. Changes in regional oxygenation saturation as measured
by near infrared spectroscopy (NIRS), have been shown to precede the clinical
manifestations of NEC in premature infants; however, there are limited data on
the use of NIRS to predict development of NEC in neonates following repair
of CHD. We hypothesize that regional NIRS values, measured on the lower
abdomen are associated with gastrointestinal morbidity in neonates following
surgery for CHD. Methods: We conducted a prospective observational study
of neonates admitted to the cardiac intensive care unit following cardiac surgery. Anterior abdominal NIRS values were continuously recorded in a blinded
fashion. Data collection began in the post-operative period and continued
until discharge from the intensive care unit. Mean hourly NIRS values were
correlated with the development of NEC. Data were analyzed using student’s
T-test, analysis of variance and receiver operating characteristic curve (ROC),
as appropriate. Results: Twenty-six patients were enrolled in the study including 5 (19%) diagnosed with NEC. The mean hourly NIRS values for both the
24-hour period prior to initiation of feeds (31% vs. 49%) and following initiation of feeds (29% vs. 46%) were lower in the NEC group (both p<0.001). By
ROC analysis, a pre-feed NIRS value of less than 38% (sensitivity=73% and
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
specificity=55%) and post-feed NIRS value of less than 30% (sensitivity=83%
and specificity=65%) best predicted the development of NEC. Conclusions:
Our results suggest abdominal NIRS values prior to initiation of feeds may
identify neonates at increased risk of post-operative NEC. Following the initiation of post-operative feeds, abdominal NIRS may be a useful tool to identify
those at risk for NEC.
Poster Session: Cardiovascular 6
197
IMAGE ACQUISITION AND INTERPRETATION OF BEDSIDE
ULTRASOUND BY PEDIATRIC CRITICAL CARE PROVIDERS
Maki Ishizuka1, Thomas Conlon1, Meryl Cohen1, Robert Berg1, Akira Nishisaki1;
1
The Children’s Hospital of Philadelphia, Philadelphia, PA
Learning Objectives: Bedside ultrasound (BUS) for hemodynamic evaluation
in critically ill children is being recognized as an important skill for intensivists. Limited data exist regarding the training required to achieve sufficient skills
in image acquisition and interpretation. Our institution implemented a training
process for pediatric critical care providers in BUS. We hypothesized that studies
performed by certified providers (C) have better image quality and accurate interpretation compared to studies performed by non-certified providers (non-C).
Methods: A cardiologist blinded to performer judged BUS hemodynamic study
image quality for each of 5 core cardiac views (Excellent=3, Good=2, Fair=1,
Unacceptable=0) and interpretation of 6 hemodynamic domains (Agreement=3,
Minor Disagreement=2, Disagreement=1). Image quality score (IQS) was an
average of the cardiac views, and interpretation score (IS) was an average of the
interpretation points. Fisher’s exact and Wilcoxon rank-sum test with p=0.05 as
cutoff. Results: 48 studies were performed over 8 months including 9 by C, 18
supervised by C, and 21 by non-C without supervision. Mean patient age was
6.7y(IQR 1-12), 85%(37/44) were intubated and 45%(19/42) were on vasopressor support. Overall image quality was judged Good to Fair (IQS: median
1.2, IQR 1.7-1.2); study interpretation was judged Agreement to Minor Disagreement (IS: median 2.8, IQR 3-2.4). Studies performed or supervised by C
had higher IQS (median 1.5, IQR 1.8-1) than those by non-C (median 1, IQR
0.6-1.25), p=0.022; and higher IS (median: 3, IQR 3-2.75) than those by non-C
(median: 2.7, IQR 3-2), p=0.01. Disagreement was found in 20%(10/48) of
studies (C or C supervised:11%, non-C:33%, p=0.08). Disagreement was due
to inadequate image quality for interpretation (n=4), LV contractility assessment
(n=4), RV size estimation (n=2) and preload assessment (n=1) with 1 study having 2 areas of disagreement. Conclusions: BUS performed by certified pediatric
critical care providers have significantly better image quality and accurate interpretation compared to studies performed by non-certified providers.
patients who utilized PW. These predictive factors should be considered when
placing PW in postoperative cardiac patients in our institution. Temporary PW
placement and removal was found to be safe in this study with no significant
complications.
199
EARLY DETECTION OF CRITICAL CONGENITAL HEART
DISEASE IN THE NEWBORNS BY PULSE OXIMETRY
Amar Taksande1; 1N/A, Wardha, India
Learning Objectives: Congenital cardiovascular malformations are the most
common category of birth defects and responsible for mortality in the first twelve
months of life. Critical congenital heart disease (CCHD) will be present in
approximately one quarter of these children, which requires catheter or surgery
intervention in the first year of life. Methods: Pulse oximetry was performed on
clinically normal newborns within first 24 hours of life. If screening oxygen saturation (SpO2) was below 95%, echocardiography was then performed. Inclusion
criteria: All newborns who were admitted in postnatal ward & NICU. Exclusion
criteria: Out born babies and babies with a prenatal diagnosis of duct dependent
circulation. Results: Pulse-oximetric screening was performed on 5767 clinically
normal newborns. Low SpO2 (<90%) was found in 18 babies sixteen of them
had CCHD, including six neonates with TGA, four with tricuspid atresia, three
with tetralogy of fallot, two with truncus arteriosus and one with total anomalous
of pulmonary venous connection. A pulse oximetry cut-off value of below 95%
for detecting CCHD showed 100% sensitivity, 99.97% specificity, 88.89% positive predictive value, 100% negative predictive value. Conclusions: Pulse oximetry is safe, feasible and noninvasive, can be used as screening tool for detecting
CCHD in clinically normal newborn. If SpO2 is below 95% in clinically normal
newborns within 24 hours of birth, urgent echocardiography is suggested to rule
out CCHD.
200
198
PREDICTORS OF THE UTILIZATION OF TEMPORARY PACING WIRES IN PEDIATRIC PATIENTS AFTER CARDIAC
SURGERY
Madalsa Patel1, Andrew Blaufox2, Dorota Gruber2, Meredith Akerman3, David
Meyer2, Vincent Parnell2, Adnan Bakar2; 1Cohen Children’s Medical Center of
New York, New Hyde Park, NY, 2Cohen Children’s Medical Center, New Hyde
Park, NY, 3North Shore LIJ Health System Feinstein Instittue, Manhasset, NY
Learning Objectives: There is a significant incidence (14-48%) of arrhythmias
after cardiac surgery in pediatric patients. Arrhythmias such as junctional ectopic
tachycardia and high grade atrioventricular block can be mitigated by pacing.
Temporary pacing wires (PW) are often placed during pediatric cardiac surgery,
however there are no established criteria by which to determine the pts most
likely to utilize PW. Previous studies have not focused on pt age or type of repair
as associated with PW use. Hypothesis: Pts less than 6 months old (mo) and pts
who have ventricular septal defect (VSD) closure as part of their surgery are more
likely to have arrhythmias and therefore utilize PW, either for diagnosis (dx) or
therapy (tx). Methods: A retrospective chart review of 159 pts ≤ to 18 years of
age who underwent cardiac surgery from September 2010 to September 2013
with cardiopulmonary bypass was performed. Pts with pre-existing arrhythmias
requiring pacemakers and permanent pacemaker placement as part of their surgery were excluded. Pt variables including age, weight, cardiac repair, bypass time,
cross clamp time, intraoperative and postoperative arrhythmias, PW placed, and
the use of PW for dx and/or tx were collected. Objectives were to identify which
cardiac lesions and age groups were associated with the utilization of temporary
PW, complications of PW placement, and other predictive variables associated
with PW use. Results: Upon multivariate logistical regression analysis of variables
associated with tx and dx use of PW, 3 variables were significant: age ≤ 6 mo (OR
4.0), intraoperative arrhythmias (OR 25.2) and the Fontan procedure (OR 11.7).
There were no complications from PW. Conclusions: Age ≤ 6 mo, intraoperative
arrhythmias and Fontan procedures as predictors of PW use identified 89% of
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
EVALUATION OF PULMONARY VASODILATORS IN PEDIATRIC CONGENITAL CARDIOVASCULAR CARE
Caitlin Aberle1, Sonya Desai1, Sujata Chakravarti2; 1NYU Langone Medical Center, New York, NY, 2New York University Medical Center, NY, NY
Learning Objectives: Pulmonary hypertension (PH) is a serious complication that occurs in some patients following congenital heart surgery (CHS)
and increases mortality risk. Inhaled (INH) iloprost is a prostacyclin analog
that has been successfully used in pediatric patients but data are limited. We
hypothesize that INH iloprost is safe and effective for prevention or treatment
of post-operative PH and can be weaned by protocol in pediatric patients following CHS. Methods: This was a retrospective review of pediatric patients who
underwent CHS at our institution from January 2013 to May 2014. All patients
who received INH iloprost for prevention or treatment of PH were included.
There were no exclusion criteria. The primary outcome measures were the efficacy
and safety of INH iloprost defined by the effect on the pulmonary to systemic
pressure ratio (P/S) and systolic blood pressure (SBP) respectively. Secondary
outcomes included evaluation of INH iloprost dosing and weaning strategy.
The Wilcoxon signed rank test was used to compare measures. P values less than
0.05 were considered significant. Results: Sixteen patients were included with a
median age at surgery of 2 months (0.07 to 136 months) and a median weight of
3.9 kg (2.2 to 25.4 kg). The median starting dose of INH iloprost was 0.5 mcg/
kg (0.2- 1.25 mcg/kg). Two patients had the dose increased during the treatment
period. Fifteen patients received the drug every two hours at initiation. Following
initiation of INH iloprost median P/S decreased in all patients (0.69 to 0.39;
p<0.005) and there was no change in median SBP (71.5 versus 72.9 mmHg;
p=0.08). Eight patients were weaned to an every four hour and then every eight
hour regimen prior to discontinuation. Median overall wean duration was 48
hours. No patients suffered a pulmonary hypertensive crisis during or after the
treatment period. Conclusions: INH iloprost is safe and effective for prevention or treatment of post-operative PH following pediatric CHS. A dose of 0.5
mcg/kg administered every 2 hours is effective, well tolerated and may be safely
weaned off over 48 hours.
201
THE INCIDENCE OF LEFT VENTRICULAR DIASTOLIC DYSFUNCTION IN PEDIATRIC PATIENTS WITH SEPSIS.
Renee Willett1, James Strainic2, Katherine Mason3; 1Johns Hopkins University
School of Medicine, Baltimore, MD, 2Rainbow Babies and Children’s Hospital
Case Western Reserve School of Medicine, Cleveland, OH, 3Rainbow Babies and
Children’s Hospital Case Western Reserve Schoolof Medicine, Cleveland, OH
Learning Objectives: Numerous studies have used echocardiographic measures to
demonstrate systolic and diastolic dysfunction in adult patients with sepsis. While
systolic dysfunction has been well documented in pediatric patients with sepsis, the
occurrence of diastolic dysfunction has not been well studied in this population.
Bedside noninvasive echocardiographic methods for the determination of diastolic
dysfunction have been developed and validated and provide the opportunity to
assess whether diastolic dysfunction occurs in pediatric patients with sepsis. The
purpose of this study was to evaluate the incidence of left ventricular diastolic dysfunction in pediatric patients with sepsis being treated in the Pediatric Intensive
Care Unit (PICU) using the ratio of mitral valve inflow velocities in early and late
diastole (E/A) as well as early mitral valve inflow velocity to early diastolic annular
velocity (E/e’). The identification of diastolic dysfunction in this patient population
would allow for more physiologically targeted medical management. Methods: A
retrospective chart review was done to identify all patients aged 28 days to 18 years
who met the 2005 International Consensus Conference on Pediatric Sepsis criteria
for sepsis and had an echocardiogram performed between 2010 and 2014. Children
with a history of trauma in the preceding 24 hours or congenital heart disease were
excluded. The E/A and E/e’ values were obtained as part of routine echocardiography
and reviewed and analyzed by a board certified Pediatric Cardiologist using standard
published specifications and reference values. Results: 50 patients were identified
that met inclusion criteria and had complete echocardiographic studies permitting
the determination of the E/A and E/E’ ratios. Of these, 42% had diastolic dysfunction using E/A ratio and 26% had diastolic dysfunction as determined using E/e’
criteria. Conclusions:Diastolic dysfunction occurs frequently in pediatric patients
with sepsis. Clinicians managing this population should consider diastolic dysfunction as a potential complicating factor in the clinical care of these patients.
202
EXTUBATION FAILURE IN POSTOPERATIVE SINGLE-VENTRICLE INFANTS WITH PARALLEL CIRCULATION
Shinya Miura1, Masaki Osaki2; 1Shizouka Children’s Hospital, Shizuoka, Japan,
2
Shizuoka Children’s Hospital, Shizuoka, Japan
Learning Objectives: Extubation failure was commonly seen in single-ventricle
children with parallel circulation after palliative cardiac surgery. However, the literature on extubation failure of those children is currently limited. We sought to
identify prevalence, etiology, and predictive factors of extubation failure in this population. Methods: A retrospective observational study was performed for scheduled
extubation after cardiac surgery for infants with parallel circulation from May 2011
to March 2014 at a tertiary pediatric cardiac center. The main outcome is prevalence and etiology of extubation failure. Extubation failure was defined as a need for
reintubation within 72 hours. We collected diagnosis, surgical procedure, characteristics, and perioperative data to identify the predictive factor of extubation failure.
Accumulated data were analyzed with the chi-square test or Mann-Whitney U test.
Results: Of the 61 eligible cases undergoing extubation during the study period,
extubation failure occurred in 13 cases (21%). Among them, two cases required
reintubation within the first 6 hours after extubation, ten cases within 6–24-hour
period, and one case 72 hours after extubation. The etiology of extubation failure
was hemodynamic instability in six, respiratory impairment in six, bleeding in one.
For the patients with extubation failure, the age at the operation was significantly
younger (8 days vs 27 days, p<0.05), and the duration of mechanical ventilation
prior to the first extubation was longer (8 days vs 5 days, p=0.05) than the patients
with successful extubation. Diagnosis, operative procedure, body weight and commodities were not associated with extubation failure. Conclusions: Extubation
failure occurred in 21% of the postoperative single-ventricle infants with parallel
circulation and the etiology was diverse. Reintubation was mostly required within
the first 24 hours. The younger age was identified as the predictive factor for extubation failure. Our data suggested that the young single-ventricle infants after cardiac
surgery required deliberate observation in the first 24 hours after extubation.
203
BOUND AND FREE CORTISOL RESPONSE AND THE RELATION TO OUTCOMES AFTER INFANT CARDIOPULMONARY
BYPASS
Eric Wald1, Carl Backer1, Zhuo Li2, William Oliver2, Joseph Dearani2, Sheri
Crow2; 1Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL,
2
Mayo Clinic, Rochester, MN
Learning Objectives: Hypothalamic-pituitary-adrenal (HPA) axis dysfunction
may be partially responsible for the hemodynamic instability experienced by infants
after cardiopulmonary bypass (CPB). This dysfunction may be exacerbated by the
use of pre or perioperative corticosteroids, a common strategy to attenuate the postoperative inflammatory state. Our objective was to describe perioperative changes
in the infant HPA axis after CPB. We provide the first characterization of the bound
(BC) and free cortisol (FC) response surrounding infant CPB and the relationship
of that response with clinical outcomes. Methods: We conducted a prospective
trial of 71 infants (age ≤365 days) from two institutions who received 1 mg/kg of
dexamethasone before CPB initiation. BC, FC, ACTH and corticosteroid-binding
globulin (CBG) were measured directly before CPB (TP1), after intensive care unit
arrival (TP2), and 24 hours after surgery (TP3). A 1 mcg ACTH stimulation test
was performed at each time point to test adrenal responsiveness. Results: Sixty-nine
infants completed all study procedures. The levels of BC, FC, CBG, and ACTH
decreased significantly between pre-op and 24 hour post-op measurements. Median
BC levels decreased from 14.2 mcg/dL at TP1, to 7.3 mcg/dL at TP2, to 2.9 mcg/
dL at TP3. Median CBG levels decreased from 36 ug/mL at TP1 to 20 ug/mL
at TP2. Median FC declined from 1725 ng/dL at TP1 to 584 ng/dL at TP2 and
124 ng/dL at TP3. ACTH stimulation produced an increase in cortisol level > 9ug/
dL for 59% of infants at TP2 and 71% at TP3. Infants with inadequate stimulation tests (≤ 9 ug/dL) at TP2 had greater median fluid requirements (276 mL/
kg vs 120 mL/kg, p<.001), greater median chest tube output (113 mL vs 56 mL,
p<.001) in the first 24 hours, and greater median length of stay (LOS) (12 vs 8
days, p=.007). Conclusions: Infants treated with steroids before CPB demonstrate
suppression of the HPA axis that persists throughout the first 24 hours post-op and
may pose risk for adverse outcomes. Low dose ACTH stimulation tests may identify infants with clinical adrenal insufficiency during the post-op period.
204
RELATIONSHIP OF COPEPTIN AND ARGININE VASOPRESSIN MEASUREMENTS AFTER PEDIATRIC CARDIAC SURGERY
Kevin Valentine1, Noreen Rossi2, Haiping Chen2, Ralph Delius3, Henry Walters III4,
Christopher Mastropietro5; 1Wayne State University / Children’s Hospital of Michigan, Detroit, MI, 2Wayne State University / John D. Dingell VAMC, Detroit, MI,
3
Childrens Hospital of Michigan, Detroit, MI, 4Children’S Hospital of Michigan,
Detroit, MI, 5Indiana University / Riley Hospital for Children, Indianapolis, IN
Learning Objectives: Hemodynamic response to arginine vasopressin (AVP) therapy after pediatric cardiac surgery is, in part, related to pre-infusion endogenous
plasma AVP concentration. Measurement of plasma AVP concentration however
is challenging. Copeptin, a more stable and easily measured product of pro-AVP
processing, has demonstrated potential as a surrogate marker for AVP. We aimed to
determine if measurements of plasma Copeptin concentration using a rapid automated assay would correlate with measurements of plasma AVP concentration in
children undergoing cardiac surgery with cardiopulmonary bypass (CPB). Methods:
Patients < 18 years of age undergoing surgery with CPB were prospectively enrolled
between 8/2013 and 2/2014. Plasma AVP and Copeptin concentrations were measured before CPB and 4 and 24 hours after CPB. Copeptin measurements were performed using the CT-proAVP Kryptor automated assay (Thermo Fisher Scientific,
Germany), which can be completed in ~ 30 minutes. Data are represented as median
(intraquartile range) unless otherwise noted. Measurements at 4 and 24 hours were
compared to baseline values using Mann-Whitney U tests. Statistical significance
was set at P<0.025 (Bonferroni correction for multiple comparisons). Results:
Twenty-three patients with varying degrees of surgical complexity were enrolled
(STS-EACTS categories 1-5). Median age was 3 years (range: 9 days - 17.8 years).
AVP and Copeptin concentrations at baseline were 1.6 pg/mL (0.5-5.5) and 16.4
pmol/L (9.9-48.2), respectively. AVP and Copeptin were increased significantly at 4
hours after CPB [11.6 pg/mL (2.8-33.8) (P=0.003) and 175.5 pmol/L (40.4-468)
(P<0.001)], then were decreased toward baseline at 24 hours. AVP and Copeptin
concentrations were significantly correlated (Spearman rho = 0.6664, p<0.0001).
Conclusions: Changes in Copeptin measured using a rapid automated assay mimicked changes in AVP concentration in children in children undergoing surgery with
CPB. Copeptin may represent a practical means of estimating endogenous plasma
AVP concentrations and thus guide use of exogenous AVP therapy in these patients.
205
HEMODYNAMIC SAFETY OF PROLONGED DEXMEDETOMIDINE USE IN PEDIATRIC CARDIAC CRITICAL CARE
PATIENTS
Marco Pinder1, Miriam Abadie2, Teihl Ratchinsky1, Teresa Moll3, Lindsey Lepard4, Natalie Montgomery4, Jarrod Knudson5; 1University of Mississippi Medical Center Dept. of Pediatrics, Jackson, MS, 2Georgetown University Hospital,
Depts. of Internal Medicine and Pediatrics, Washington, DC, 3University of Mississippi Medical Center, Jackson, MS, 4University of Mississippi Medical Center Dept. of Pharmacy, Jackson, MS, 5University of Mississippi Medical Center
Dept. of Pediatrics, Div. of Critical Care, Jackson, MS
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Learning Objectives: Dexmedetomidine is an alpha 2- adrenoceptor agonist
used for sedation in pediatric cardiac critical care patients in the peri-extubation
window due to its favorable hemodynamic profile and sparing of respiratory
drive. Recent studies indicate that dexmedetomidine can be administered safely
for a period up to 48-72 hours without untoward side effects (arrhythmias,
rebound tachycardia or hypertension). With recent literature (samples < 100
patients) suggesting extending the duration of use, we hypothesize that dexmedetomidine is safe and effective for yet longer durations of use, i.e. 72-96
hours. Additionally, we are analyzing a relatively large cohort (~500 patients).
Methods: Retrospective chart review of children in the pediatric cardiac intensive care unit at a tertiary children’s medical center that received a dexmedetomidine infusion over a three year period (n = 138, with continuing chart review).
Patient demographics, hemodynamic data, time on mechanical ventilation,
ICU and hospital length of stay, RACHS scores, other sedative/analgesics and
inotrope/vasopressor use have been recorded. Continuous variables have been
analyzed with paired t-test and repeated measures ANOVA. Results: Median
age is 17.1 months (range 0 - 423). Median length of therapy is 9.7 hours (range
1-72). With initiation of dexmedetomidine infusion, no patients experienced
significant bradycardia or hypotension. With discontinuation of therapy, heart
rate and systolic/diastolic blood pressures all increase (p < 0.001 for all); however, increases are clinically insignificant (no benzodiazepines/clonidine used
to treat rebound effects). No patients experienced symptomatic bradycardia.
Additionally, there were no arrhythmias associated with dexmedetomidine
use.Conclusions: Dexmedetomidine has been used safely and effectively for up
to 72 hours in our pediatric cardiac critical care patients. Continued analysis
of our patient population is required to substantiate or refute this conclusion,
either of which will provide new and important information for pediatric cardiac
intensivists.
Poster Session: Cardiovascular 7
206
FRACTURES RELATED TO METABOLIC BONE DISEASE IN
WITH CONGENITAL HEART DISEASE
Henry Cheng1, Fabio Carmona2, Catherine Gordon3, Jeannette Perez-Rossello4,
Frank Pigula4, Peter Laussen5, Satish Rajagopal1; 1Boston Children’s Hospital,
Boston, MA, 2University of Sao Paulo, Sao Paulo, Brazil, 3Hasbro Children’s
Hospital, Providence, United States, 4Boston Children’s Hospital, Boston, United
States, 5Hospital For Sick Children, Toronto, ON
Learning Objectives: Critically ill children with congenital heart disease (CHD)
are at risk for metabolic bone disease (MBD) which may result in iatrogenic bone
fractures. We characterize a cohort of children with CHD and iatrogenic fractures and evaluate the effectiveness of a Fragile Bone Protocol (FBP) targeting the
reduction of fracture rates. Methods: Patients who developed fractures while in
the Cardiac Intensive Care Unit (CICU) of Children’s Hospital Boston between
March 2008 and June 2014 were identified by querying quality improvement
and radiology databases, and their medical records were reviewed. The FBP (initiated in July 2011) systematically identifies and flags patients at risk for MBD
who are then handled with specific precautions. Results: Twenty-three iatrogenic
fractures were identified in 15 children. Six patients (40%) had single ventricle
heart disease, and 6 patients (40%) required extracorporeal membrane oxygenation during their hospital stay. Nine patients (60%) survived to hospital discharge, compared to an overall CICU mortality rate of 2.6% (p<0.01). Median
age at fracture identification was 6.2 months (range: 1.5 - 23.3 months) with a
pre-fracture median duration of hospitalization of 2.7 months (0.1 - 6.5 months).
The fractures were incidentally discovered in 11 patients (73%). Two patient
required interventions for their fractures (closed reduction/casting and casting
alone). Hyperparathyroidism and low 25-OH vitamin D levels were common,
present in 77% and 40% of those tested, respectively. The fracture case rate fell
after implementation of the FBP (2.6 cases/1,000 admissions versus 0.7/1,000,
p=0.04). At a median follow-up of 34.8 months (1.9-51.9 months), no survivors
had clinically evident sequelae from their fractures. Conclusions: Critically ill
children with CHD are at risk for fragility-related fractures. They represent a
young, medically complex group of patients who frequently have hyperparathyroidism and hypovitaminosis D. A FBP consisting of identification and careful
handling of patients at risk for MBD may decrease fracture rates.
207
OUTCOMES ASSOCIATED WITH USE OF DIALYSIS IN CHILDREN RECEIVING ECMO AFTER HEART SURGERY
Punkaj Gupta1, Brandon Beam1, Michael Schmitz1; 1Arkansas Children’s Hospital, Little Rock, AR
Learning Objectives: There are very sparse data on the impact of dialysis on the
outcomes in children receiving extracorporeal membrane oxygenation (ECMO).
This study was designed to evaluate this association using the Pediatric Health
Information System (PHIS) database. Methods:Patients aged ≤ 18 years receiving ECMO before or after pediatric heart operation (with or without cardiopulmonary bypass) at a PHIS-participating hospital (2004-2013) were included. The
association between dialysis and each study outcome was computed using logistic
regression first as a bivariate analysis and then as multivariable analysis. Results:
3,502 patients from 43 hospitals qualified for inclusion. Of these, 484 (14%)
patients received dialysis during their hospital stay. After adjusting for patient
and center characteristics, the odds of mortality were significantly higher in
dialysis group (OR: 1.86, 95% CI: 1.46- 2.37, p<0.0001). However, there were
significantly improving trends in odds of mortality after adjusting for patient
and center characteristics, compared to unadjusted odds of mortality. In adjusted
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
models, length of ECMO was longer by 0.81 days (95% CI: 0.13- 1.49, p=0.02)
in patients receiving dialysis. This was significantly lower in adjusted models
compared to unadjusted models. However, there was no difference in adjusted
length of mechanical ventilation, and adjusted hospital length of stay in dialysis
group compared to no dialysis group. We further demonstrated that the odds of
mortality increased by approximately 2% for each day increase in the timing of
dialysis initiation after ECMO. Conclusions: In this large observational study,
we demonstrated worsening outcomes, including mortality, in children receiving
ECMO with dialysis compared to children receiving ECMO without dialysis.
However, there were significantly improving trends in the outcomes after adjusting for patient and center characteristics, compared to unadjusted analysis. These
data provide no evidence for a survival benefit afforded by dialysis, however, it is
possible that these results reflect residual confounding by severity of illness.
208
INFERIOR VENA CAVA COLLAPSIBILITY AND VASCULAR
REACTIVITY IN PEDIATRIC PATIENTS.
Grace Chong1, Heather Fagan1, Paula Williams1, Nadia Khan1, Sudhir Sriram1;
1
University of Chicago, Chicago, IL
Learning Objectives: Determining intravascular volume is a critical component in the care of patients. Dynamic measurements to evaluate intravascular
status show promise. The goals of this study were to define age-based normative values of ultrasound-derived Inferior Vena Cava Collapsibility Index (IVCCI) in a healthy pediatric population and to determine the effect of fluid and
dexmedetomidine on these indices. We hypothesized that collapsibility of the
IVC correlated to vascular capacity and vascular filling. Methods: Children from
0-18 years of age who utilized sedation services for planned procedures were
enrolled. Each patient received intravenous fluid (IVF) and dexmedetomidine.
Subxiphoid views by bedside ultrasonography (BUS) were captured to establish
IVC diameters during inspiration and expiration at two time points – before
and after intravenous fluids and dexmedetomidine were administered. These
values were used to calculate IVC collapsibility indices. Hemodynamic parameters were recorded concurrently. Results: Of 46 patients enrolled, there was a
15.2% reduction in maximum IVC diameters (p<0.002) and a 23.5% reduction
in minimum IVC diameters (p<0.002) after fluid and sedation interventions.
There was a 30% increase in IVC-CI between time points (30.4% ± 13% to
39.5% ± 15%; p<0.0001). An increase in IVC-CI with dexmedetomidine dose
(slope 0.52, r2=0.046. p=0.17) was noted with less correlation between IVF and
the change in IVC-CI (slope -0.51, r2=0.078, p=0.06). Heart rate decreased by
17% (p<0.001) and mean arterial pressure decreased by 14% (p<0.001) after
interventions. Mean values of IVC diameters and IVC-CI at baseline increased
with each age group. Conclusions: We propose that increased IVC collapsibility
after interventions is a result of dexmedetomidine on vascular tone via an inhibition of neurohumoral effects. By demonstrating that dexmetomidate decreases
vascular capacity, the reliability of IVC-CI measurements to predict vascular tone
and filling emerge. Using IVC-CI by BUS provides a swift noninvasive approach
to predict intravascular volume assessments and reactivity in pediatric patients.
209
ASSOCIATION BETWEEN SERUM CORTISOL LEVELS AND
HYDROCORTISONE THERAPY AFTER PEDIATRIC CARDIAC
SURGERY
Alicia Teagarden1, Christopher Mastropietro1; 1Riley Hospital for Children /
Indiana University School of Medicine, Indianapolis, IN
Learning Objectives: Use of hydrocortisone (HC) to treat refractory hemodynamic instability in children recovering from cardiac surgery is common practice.
We aimed to determine if there is a relationship between serum cortisol, which
is often measured prior to initiation of HC at our center, and the hemodynamic
response to this therapy. Based on prior studies, we hypothesized that the hemodynamic response to HC would not be significantly related to pre-HC serum
cortisol. Methods: We performed a retrospective study of patients < 18 years
who underwent cardiac surgery between 1/1/2012-12/31/2013 and had pre-HC
serum cortisol measurements within the first 72 postoperative hours. Favorable
responders were defined as patients in whom, at 24 hours after the first dose of
HC, systolic blood pressure (SBP) was increased or maintained and vasoactiveinotrope score (VIS) was decreased, or SBP was increased by ≥ 10% of baseline
and VIS was unchanged. Patients who received < 24 hours of HC and patients
who were receiving extracorporeal life support during HC therapy were excluded.
Variables were compared in those who responded favorably to those who did
not using t-tests or Mann Whitney tests as appropriate. Results: Of 20 patients
identified, 11 (55%) responded favorably to HC. At 24 hours, mean SBP was
increased by 22% and VIS was decreased by 21% in patients who responded
favorably, while mean SBP was increased by 1% and VIS was increased by
29% in those who did not respond favorably. Mean pre-HC cortisol in patients
who responded favorably was 16.1 ± 10 mg/dL (range:1.6-29.9), as compared
to 49.5 ± 46 mg/dL (range: 2.6-125) in those who did not respond favorably,
P=0.03. Age, timing of first HC dose, total number of HC doses, duration of
mechanical ventilation, ICU stay, and mortality were not statistically different
between groups. Conclusions:Children recovering from cardiac surgery who had
a favorable hemodynamic response to HC, contrary to our initial hypothesis,
were more likely to have lower pre-HC serum cortisol. Favorable hemodynamic
response to HC however was not associated with better postoperative outcomes.
210
DEXAMETHASONE LEVELS AND THE ASSOCIATION WITH
CLINICAL OUTCOMES AFTER INFANT CARDIOPULMONARY BYPASS
Sheri Crow1, Joseph Dearani1, William Oliver1, Zhuo Li1, Carl Backer2, Eric
Wald2; 1Mayo Clinic, Rochester, MN, 2Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL
Learning Objectives: Corticosteroids are often used to mediate the inflammatory response after cardiopulmonary bypass (CPB) in children. The potential for
corticosteroid-induced suppression of the innate stress response is well known but
poorly characterized following infant cardiac surgery. We hypothesize that infants
with high Dex levels in the first 24 hours after surgery have a decreased cortisol/
stress response and higher rate of adverse outcomes. Methods: We conducted a
prospective trial of 90 infants (age ≤365 days) from two institutions who received
1 mg/kg of Dex pre-CPB initiation. Blood was analyzed for cortisol, free cortisol, adrenocorticotropin hormone (ACTH), and Dex levels immediately before
CPB, after intensive care unit (ICU) arrival, and 24 hours after surgery. Eighteen
patients were excluded from analysis at 24 hours due to steroid supplementation
for extubation. Patients were grouped as high Dex (≥15 μg/dL) or low Dex (<15
μg/dL) based on their levels at ICU arrival. Results: Dex levels varied significantly
between the high (n =52) and low (n = 38) Dex groups throughout the postoperative course and correlated highly with cortisol and ACTH response. Infants with
high Dex levels had lower median fluid requirements in the first 24 post-op hours
(p= 0.002) and lower median chest tube output (p=0.001) but increased median
ventilator hours (p=0.015). Patients whose Dex level persisted > median at 24
hours had higher inotrope scores (p=0.005), and lactates (p=0.01) and decreased
median free cortisol levels at 24 hours (p=0.002). There were no significant differences between groups for CPB and cross-clamp times, or length of stay. Conclusions: Postoperative Dex levels are highly correlated with the magnitude of the
postoperative stress response for infants after CPB. High postoperative Dex levels
are associated with lower cortisol levels, reduced fluid requirements, and longer
duration of mechanical ventilation. The current dosing strategy of corticosteroids
pre-CPB generates variable suppression of the innate stress response that may
have implications for clinical outcomes.
211
Pediatric Health Information System (PHIS) database. Methods:Patients aged ≤
18 years receiving ECMO after pediatric cardiac surgery (with or without cardiopulmonary bypass) at a PHIS-participating hospital (2004-2013) were included.
De-identified data obtained from retrospective, observational dataset included
demographic information, baseline characteristics, operation details, patient diagnoses, and center data. Outcomes evaluated included in-hospital mortality, length
of mechanical ventilation, length of ICU stay, length of hospital stay, and hospital
charges. Multivariable logistic regression and Cox proportional hazards models were
fitted to study the probability of study outcomes as a function of ECMO duration.
Results: 998 patients from 37 hospitals qualified for inclusion. The median duration of ECMO run was 4 days (IQR: 1,7). After adjusting for patient and center
characteristics, there was 12% increase in the odds of mortality for every 24 hours
increase in ECMO duration (Odds Ratio: 1.12, 95% CI: 1.07-1.18, p<0.001).
Patients receiving longer duration of ECMO were associated with longer length of
mechanical ventilation (Hazard Ratio: 0.90, 95% CI: 0.87- 0.94, p<0.001), longer length of ICU stay (Hazard Ratio: 0.91, 95% CI: 0.89-0.93, p<0.001), longer
length of hospital stay (Hazard Ratio: 0.92, 95% CI: 0.89- 0.94, p<0.001), and
higher hospital charges (Hazard Ratio: 0.90, 95% CI: 0.86- 0.94, p<0.001). Conclusions: Data from this large multicenter database suggest that longer duration of
ECMO support after pediatric cardiac surgery is associated with worsening outcomes. Careful selection of patient population, multi-disciplinary team approach,
and candid discussions with families are crucial in the successful outcomes of children receiving prolonged ECMO after congenital heart surgery.
212
IMPACT OF TIMING OF ECMO INITIATION ON OUTCOMES
AFTER PEDIATRIC HEART SURGERY
Punkaj Gupta1, Michael Robertson2, Paul Seib2, Janet Simsic3, Joseph Tobias4,
Brandon Beam1; 1Arkansas Children’s Hospital, Little Rock, AR, 2University of
Arkansas for Medical Sciences, Little Rock, AR, 3Emory University, Children’s
Healthcare of Atlanta At Egleston, Atlanta, GA, 4Nationwide Children’s Hospital, Columbus, OH
Learning Objectives: There are very sparse data on patient outcomes related
to timing of ECMO initiation in children after pediatric cardiac surgery. This
study was designed to evaluate this association using the Pediatric Health Information System (PHIS) database. Methods: Patients aged ≤ 18 years receiving
ECMO after pediatric cardiac surgery (with or without cardiopulmonary bypass)
at a PHIS-participating hospital (2004-2013) were included. Data collection
included demographic information, baseline characteristics, pre-ECMO risk factors, operation details, patient diagnoses, and center data. Outcomes evaluated
included in-hospital mortality, duration of ECMO, duration of mechanical ventilation, duration of ICU stay, duration of hospital stay, need for reoperation, and
hospital charges. Multivariable and Cox proportional hazards models were fitted
to study the probability of study outcomes as a function of timing from cardiac
surgery to ECMO initiation. Results: 953 patients from 38 hospitals qualified
for inclusion. The median timing of ECMO initiation after cardiac surgery was 2
days (IQR: 1 day-10 days). After adjusting for patient and center characteristics,
increasing duration of time from surgery to ECMO initiation was not associated
with worsening outcomes, including mortality (OR: 1.00, 95% CI: 0.98- 1.01,
p=0.54), duration of mechanical ventilation (MV) (HR: 1.00, 95% CI: 0.991.01, p=0.56), duration of ICU stay (HR: 0.99, 95% CI: 0.98-1.00, p=0.15),
or hospital charges (HR: 0.99, 95% CI: 0.98-1.01, p=0.34). However, a longer
period of time from surgery to initiation of ECMO was associated with a significantly shorter duration of ECMO (HR: 1.01, 95% CI: 1.00- 1.02, p=0.01).
Need for reoperation on ECMO increased with increasing duration of ECMO
initiation after cardiac surgery (OR: 1.01, 95% CI: 1.00-1.03, p= 0.02). Conclusions: Increasing duration of ECMO initiation after cardiac surgery is not
associated with worsening outcomes. However, increasing duration of time from
cardiac surgery to ECMO cannulation is associated with a higher incidence of
reoperation, and a shorter duration of ECMO.
213
INTERMEDIATE TERM RESULTS AFTER EXTRA CARDIAC
CONDUIT FONTAN SURGERY IN CHILDREN AND YOUNG
ADULTS
RELATIONSHIP OF ECMO DURATION WITH OUTCOMES
AFTER PEDIATRIC CARDIAC SURGERY
Shashi Raj1, Ruchi Gupta1, Eliot Rosenkranz1, Barbara Sears1, Sethuraman
Swaminathan1; 1Holtz Children’s Hospital, University of Miami, Miami, FL
Learning Objectives: There are very sparse data on the outcomes of children receiving prolonged extracorporeal membrane oxygenation (ECMO) after cardiac surgery. This study was aimed to evaluate the association of ECMO duration with
outcomes in children undergoing surgery for congenital heart disease using the
Learning Objectives: The Fontan surgery and its modifications are currently the
standard palliation to separate venous and arterial circulation in patients with
single ventricle physiology. We evaluated the outcome of patients who underwent
an extracardiac Fontan surgery at our center since 2000 to assess morbidity, mortality and New York Heart Association (NYHA) functional class in the current
era. Methods: Medical records of 97 patients who underwent an extracardiac
Fontan surgery between November 7, 2000 and October 30, 2013 were reviewed
Punkaj Gupta1, Michael Robertson2, Brandon Beam1, Michael Schmitz1; 1Arkansas Children’s Hospital, Little Rock, AR, 2University of Arkansas for Medical Sciences, Little Rock, AR
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
to determine diagnosis, age at surgery, surgical technique, post-operative complications, NYHA class at last follow-up, echocardiographic parameters, and most
recent Holter results. Results: Median age at surgery was 3.4 years [interquartile
range (IQR) 2.8-4.5 years]. There were 4 deaths with one in the immediate postoperative period. Nine patients underwent conversion from classical Fontan to
extracardiac conduit. There were 48 patients with anatomic dominant single right
ventricle, 43 patients with dominant single left ventricle, 3 patients with balanced
ventricles and 3 patients with indeterminate ventricular morphology. Seventy eight
of the 97 patients (80%) underwent fenestrated Fontan surgery. Median follow up
was 3.9 years available in 88 patients (IQR 0.2-12.2 years). At the latest follow up,
55 patients were determined to be in NYHA class I, 27 patients in NYHA class
II, and 6 patients in NYHA class III and the median oxygen saturation was 92%
(IQR 86-96). There were 15 patients with history of pre-operative arrhythmias
and six of them required pacemaker placement at the time of surgery. One patient
developed ectopic atrial tachycardia and 1 patient had clinical thromboembolism
on follow up. Systolic function of the single ventricle by transthoracic echocardiogram at the latest follow up was described as normal in 70 patients (78%), fair in
19 patients (21%) and poor in 1 patient (1%). Conclusions: Our study shows
that patients who undergo extracardiac Fontan surgery in the modern era may
have significantly less morbidity and mortality when compared to earlier years.
214
ARE COMPLICATIONS OF SURGICAL VENTRICULAR SEPTAL DEFECT CLOSURE, AGE OR WEIGHT DEPENDENT?
Ravi Samraj1, Dilachew Adebo2, Mehrdad Salamat2; 1Shands Children’s Hospital, University of Florida Health, Gainesville, FL, 2Driscoll Children’s Hospital,
Corpus Christi, TX
Learning Objectives: Surgical closure of a VSD is the most common openheart procedure performed in pediatric cardiac surgery. There are very limited
studies to determine whether surgical closure of VSD at an early age or in
infants with low weight is associated with increased morbidity or mortality.
Our study was undertaken to determine if the short term complications of surgical VSD closure were age or weight related. Methods: We undertook a large
(10 year) retrospective study of all children who underwent surgical closure of
VSD (with or without concomitant closure of ASD and/or PDA) at Driscoll
Children’s Hospital between July 1999 and July 2009. Continuous variables
were compared using the Wilcoxon rank sum test and Categorical variables
were compared by chi-square test. Results: 118 children were included of
which 44 children (37.2%) were less than 3 months of age and 10 children
(9%) weighed less than 3 kg. Most frequent complications were post operative
arrhythmias (10.2%), sepsis (8.4%), re-intubation (5.9%), readmission within
30 days (3.4%), pleural effusions requiring drainage (2.5%), pneumothorax
(2.5%), hemodynamically significant residual VSD (2.5%) and AV block
requiring permanent pacemaker (1.7%). 52.3% of children who were less than
3 months of age had complications while only 18.9% of those above 3 months
had complications (Odds ratio: 4.7; 95% CI = 2.0 – 10.7; p value = 0.0002).
70% of children who weighed less than 3kg had complications compared to
27.3% of children who weighed more than 3 kg (Odds ratio 7.17; 95% CI
= 1.7-28.9; p = 0.003). 2 children died postoperatively, both of them were
less than 3 months (2 months, 1.7 months) and less than 3 kg (2.4 kg, 2.5kg).
Conclusions: Our study shows that there is an increased risk of complications
in children with surgical closure of isolated VSD when they were less than 3
months of age or when their body weight was less than 3 kg. We recommend
considering postponement of surgical closure of isolated VSD, if medically
feasible or to consider placement of a pulmonary artery band while awaiting
definitive repair at a later date to improve outcomes.
Poster Session: Cardiovascular 8
215
OUTCOMES ASSOCIATED WITH PREOPERATIVE USE OF
ECMO IN CHILDREN UNDERGOING HEART OPERATION
Punkaj Gupta1, Brandon Beam2, Mallikarjuna Rao Rettiganti3; 1Arkansas Children’s Hospital, Little Rock, Arkansas, 2Arkansas Children’s Hospital, Little Rock,
AR, 3Arkansas Childrens Hospital, Little Rock, AR
Learning Objectives: There are very sparse data on patient outcomes related to
the use of extracorporeal membrane oxygenation (ECMO) prior to heart operation in children with congenital heart disease. This study was designed to evaluate
this association using the Pediatric Health Information System (PHIS) database.
Methods: Patients aged ≤ 18 years receiving ECMO before or after pediatric
heart operation (with or without cardiopulmonary bypass) at a PHIS-participating hospital (2004-2013) were included. Data collection included demographic
information, baseline characteristics, operation details, patient diagnoses and
complications, and center data. Multivariable logistic regression or cox proportional hazards models were fitted to study the effect of timing of ECMO initiation
in relation to cardiac surgery on study outcomes. Results: 3,498 patients from
42 hospitals qualified for inclusion. 494 (14%) patients received ECMO prior
to heart operation (pre-surgery ECMO), while 3,004 (86%) patients received
ECMO after heart operation (post-surgery ECMO). Unadjusted mortality was
significantly lower in pre-surgery ECMO group compared to post-surgery ECMO
group (30% versus 45%, p<0.0001). After adjusting for patient and center characteristics, odds of mortality were significantly lower in pre-surgery ECMO group
(OR: 0.46, 95% CI: 0.36, 0.59, p<0.0001). There were no significant differences
in ECMO duration, length of hospital stay and hospital charges between the two
groups in adjusted models. Conclusions: This study suggests that ECMO can be
used with satisfactory outcomes prior to heart operation in children with congenital heart disease. Further study is warranted to determine the exact pathophysiological reasons for the need of ECMO in pre-operative period.
216
KETOROLAC USE FOR PAIN CONTROL IN PEDIATRIC
PATIENTS AFTER CARDIAC SURGERY
Tracie Lin1, Jyoti Bhatia2, Deepa Patel2, Sandeep Gangadharan3; 1N/A, N/A,
2
Cohen Children’s Medical Center, New Hyde Park, NY, 3Cohen Children’S
Medical Center, New Hyde Park, NY
Learning Objectives: Pain control is an essential aspect of care after cardiac
surgery, both in itself and with the potential consequences of analgesics used,
such as opioid-related respiratory depression impeding extubation or NSAID
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
nephrotoxicity in the context of impaired cardiac function and cardiopulmonary
bypass-related renal insult. In this study, we examined the effects of ketorolac in
the early post-op period following pediatric cardiac surgery. Methods: Retrospective cohort study of patients between 0 to 18 years old who had cardiac surgery
at a tertiary children’s hospital from January to August 2012. All RACHS-1 categories included. Pain scores were recorded, as were most recent pre-op and maximum post-op creatinine levels. Results: Of the 19 patients studied, 8 received
ketorolac starting within 12 hours post-op and 11 did not. There was no statistically significant difference in mean age, sex, chest incision type, presence of
chest tube, recent pre-op opioid use, nor post-op benzodiazepine or non-opioid
analgesic use. Opioid use was lower in the ketorolac group than non-ketorolac
group: 0.65 vs. 3.05 mg/kg IV morphine equivalents during the first 24 hours
post-op (p=0.007), 0.11 vs. 3.51 mg/kg from 24-48 hours post-op (p=0.001),
and 0.03 vs. 3.07 mg/kg from 48-72 hrs post-op (p=0.002). Patients were painfree at equal percentages of assessments and there was no difference in maximum
pain scores, p>0.05. In the ketorolac group, there was a shorter intubation duration (0.38 vs. 6.2 days, p=0.01), ICU length of stay (LOS) (113 vs. 707 hours,
p=0.08), and hospital LOS (5 days vs. 35 days, p=0.02). The median percent
change in serum creatinine was not statistically significant. Conclusions: Patients
given ketorolac in the immediate post-op period had equal pain control as their
non-ketorolac-using counterparts, had dramatically lower opioid use, as well
as shorter intubation duration and length of stay. Our finding of no additional
nephrotoxicity associated with ketorolac use suggests that it is safe for children
after cardiac surgery, including patients undergoing procedures of all RACHS
risk categories.
217
A RETROSPECTIVE EVALUATION OF RECRUITMENT
MANEUVERS IN A CARDIAC PEDIATRIC INTENSIVE CARE
UNIT
Rhonda Schum1, Cynthia White2, David Nelson2; 1Cincinnati Childrens Hospital Med Center, Cincinnati, OH, 2Cincinnati Children’s Hospital Medical Center, Cincinnati, OH
Learning Objectives: Managing patients with atelectasis can be challenging.
Despite a lack of evidence supporting specific interventions to reverse atelectasis,
there is increasing interest in utilization of Recruitment Maneuvers (RM’s) in
the clinical setting. Although atelectasis is common in children after congenital
heart surgery, there has been apprehension for using recruitment strategies in this
population secondary to the impact on cardiopulmonary interactions and limiting venous return. We hypothesized that RMs are a safe and effective modality for
children with heart disease who develop atelectasis. Methods: An evidence based
protocol for performing 2 different types of RM strategies was implemented in
our Cardiac Intensive Care Unit (CICU). We conducted a retrospective chart
review of all patients who received RMs while on mechanical ventilation in the
CICU from November 2013- March 2014. Approval was obtained from the IRB.
Hemodynamics and pulmonary mechanics were recorded from the GE Solar and
Philips NM3 monitors. These values were collected pre and post RM. Wilcoxin
Ranked Sign test was utilized to evaluate differences in pre and post RM outcome
variables (SPSS version 20). Results: There were a total of 33 patients in this
retrospective review with 348 individual RMs. 55% of the patients were less than
1y/o, with a median age of 9 months. Hemodynamic variables did not change
after RMs, but pulmonary mechanics improved VCO2 (p=.01), Vte (p=.07),
alveolar VT (p=.02), and dynamic compliance (p=.01) all increased post RM.
A small pneumothorax was detected on routine CXR in one patient, but it is
unknown if the pneumothorax was related to RM. Conclusions: RMs were performed safely in a group of pediatric patients with congenital heart disease. In this
cohort of patients, RM’s increased dynamic compliance, alveolar tidal volume,
and VCO2, without altering hemodynamic status. More rigorous studies are warranted in this unique population to evaluate the impact of RM’s on outcome
218
PULSE PRESSURE VARIATION SHOWS CONSISTENT AND
ROBUST CHANGE IN RESPONSE TO FLUID BOLUS IN
CHILDREN
Kavita Morparia1, Laura Olivieri2, Michael Spaeder1, Jennifer Schuette1; 1Children’s National Medical Center, Washington, DC, 2Children’s National Medical
Center, Washington, DC, DC
was used in 134 patients (65%); median CS transfused was 82% of the available volume. Patients who received CS did not differ significantly from those
who did not in age, weight, total CS processed, percentage of CS used before
CICU admission, and 12 hour hemoglobin level. CICU admission hemoglobin
level was lower (mean 12.7 g/dL vs 13.2 g/dL) in patients who received CS (p=
0.02). Accounting for patients who received >75% of available CS volume, only
6 patients received PRBC transfusion >4 hours after CICU admission; in those
who did not receive CS only 8 patients received PRBC transfusions >4 hours after
CICU admission. In both groups, PRBC given within 4 hours of CICU admission was allogeneic blood to which the patient had already been exposed to in the
operating room. Conclusions: CS availability within 4 hours of CICU admission decreases the need for PRBC transfusion in patients of all ages undergoing
pediatric cardiac surgery. Only 14/207 (6.7%) of patients would have potentially
benefited from longer availability of CS. A 4 hour shelf life for CS is sufficient in
light of the limited PRBC needs after that time.
220
PRESERVED FETAL RIGHT VENTRICULAR NO SIGNALING
IN AN OVINE MODEL OF CONGENITAL HEART DISEASE
Rebecca Kameny1, Catherine Morris1, Youping He2, Christine Sun2, Jun Maki3,
Sanjeev Datar4, Peter Oishi5, Jeffrey Fineman4; 1University of California, San
Francisco, San Francisco, CA, 2Univeristy of California, San Francisco, San
Francisco, CA, 3N/A, Kurume-Shi, Fukuoka-Ken, 4University of California San
Francisco Medical Center, San Francisco, CA, 5University Of California San
Francisco, San Francisco, CA
Learning Objectives: Pulse pressure variation (PPV) represents the alteration in
left ventricular stroke volume with each mechanical tidal breath. It has been validated in adults as a marker of fluid responsiveness, and is available as a real-time
continuous measurement in patients with arterial access. We hypothesize that
PPV will predictably fall in response to fluid resuscitation in children, and we
aim to quantify this change in relation to that in other variables. Methods: We
conducted a prospective study in mechanically ventilated children in the pediatric
intensive care unit. Hemodynamic data immediately before and after a fluid bolus
were collected in real time by an investigator at the bedside. All fluid resuscitation
decisions (timing, type and amount of fluid to be given) were at the discretion
of the ICU medical team. Paired t-test or Wilcoxon matched pairs sign rank test
were used as appropriate for each hemodynamic variable. Results: We assessed
13 sets of hemodynamic measures from 11 unique patients. In 12/13 instances,
there was a drop in PPV in response to a fluid bolus. The average PPV before and
after a fluid bolus was 16 ± 7.9 and 10 ± 4.7 respectively, which represents a 38%
decrease (p<0.001). There was no significant change in either systolic or diastolic
blood pressure (BP), with heart rate (HR) being the only other hemodynamic
variable which showed a significant change (6% decrease, p=0.01). Conclusions:
Reliable predictors of fluid responsiveness are needed in children, with HR and
BP being confounded by medications and physiologic factors such as temperature and intracranial pressure, and CVP proven to be of no benefit. Our study
demonstrates that while decisions regarding fluid resuscitation are often based
on HR and BP, HR shows a weaker response than PPV, while BP does not show
a statistically significant change in response to fluid administration. PPV is a
promising marker, showing a consistent and robust change in response to fluid
resuscitation and continuous bedside monitoring may reveal predictable trends
reflecting overall fluid status in sick children.
Learning Objectives: We recently reported that the right ventricle (RV) of lambs
in a model of congenital heart disease (CHD) with increased pulmonary blood
flow (shunt) has a robust response to afterload due to the Anrep Effect-the slow
increase in contractility due to myocyte stretch beyond the Frank-Starling Effect.
This finding in shunt lambs may account for the preserved RV function seen in
patients with pulmonary hypertension and CHD and may reflect preservation of
a fetal phenotype since the RV of shunt lambs remains exposed to increased pressure postnatally. Nitric oxide (NO) production by NO synthase (NOS) is activated by myocyte stretch and is a necessary intermediary of the Anrep response.
We hypothesized that NOS signaling would be increased in fetal and shunt
lambs compared to controls. Methods: Late gestation fetal lambs (n=5) underwent placement of an aortopulmonary vascular graft (shunt). Four weeks after
delivery, RV tissue was harvested from shunt and twin controls. Fetal RV tissue
was obtained from late-gestation lambs. RNA expression levels were determined
by quantitative PCR; eNOS protein levels were determined by Western blot.
Results: In shunt and fetal lambs, endothelial NOS (eNOS) RNA (3.0 ± 1.0- and
4.9 ± 0.7-fold control, respectively) and protein expression (1.3-fold and 1.6-fold
control) were increased (p<0.05). Similarly, RNA expression of both inducible (iNOS) and neuronal (nNOS) was increased in shunt and fetal RV (iNOS
2.0 ± 0.7- and 3.2 ± 0.8-fold control; nNOS 10.2 ± 4.9- and 25.3 ± 7.2-fold control, respectively; p<0.05). In addition, RNA expression of Akt 1 (2.9 ± 1.0- and
4.1 ± 0.7-fold control, respectively), a serine/threonine kinase that activates NOS,
and calmodulin (88.8 ± 6.9- and 16.8 ± 2.2-fold control), a calcium-binding protein that promotes NOS activity, was increased in shunt and fetal RV (p<0.05).
Conclusions: In ventricular hypertrophy, recapitulation of the fetal phenotype
is traditionally implicated as a harbinger of ventricular failure. However, we have
shown persistence of fetal NOS expression in the RV associated with an adaptive
physiologic response to afterload challenge.
219
221
EARLY CELL SAVER TRANSFUSION DECREASES THE NEED
FOR ALLOGENEIC BLOOD AFTER PEDIATRIC CARDIAC
SURGERY
HYPOALBUMINEMIA PREDICTS THE CLINICAL COURSE IN
PEDIATRIC PATIENTS AFTER OPEN HEART SURGERY
Michael Wolf1, Nina Guzzetta1, Bruce Miller1, Ann Marie McGoldrick2, Kathy
Spitzer2; 1Emory University School of Medicine, Atlanta, GA, 2Children’s Healthcare of Atlanta, Atlanta, GA
Learning Objectives: Infants and children often require blood products immediately following cardiac surgery. Intraoperative salvage of autologous blood with
a cell saver device (CS) can decrease the need for transfusion of allogeneic packed
red blood cells (PRBC) in the postoperative period. Current American Association of Blood Bank regulations limit CS room air shelf life to 4 hours. We examined whether availability of CS for pediatric patients within the limited shelf life
will decrease the need for PRBC transfusion within the first 24 postoperative
hours. Methods: A prospective analysis of all patients who underwent cardiopulmonary bypass (CPB) and returned to the CICU with CS was performed.
Patients’ records were reviewed for total CS delivered after CICU admission,
PRBC received within 24 hours, initial and 12 hour hemoglobin, and characteristics of patients who did not receive available CS. Results: Of 368 total CPB cases,
207 (56%) had CS available (median volume 17 ml/kg) at CICU admission. CS
Jose Lugo-Bernier1, Manuel Iglesias2, Anabel Puig-Ramos2, Janice GómezGaray2, Yelitza Rodríguez2, Alberto Pueyo3, Erskin Bezares-Casiano2, Ricardo
Garcia De Jesus2; 1University Of Puerto Rico School Of Medicine, San Juan,
PR, 2UPR-MSC Critical Care Section, San Juan, PR, 3University of Villanova,
Philadelphia, PA
Learning Objectives: Despite the ability to correct complex congenital heart
defects in neonates and infants, there are limitations in clinical outcomes that
are related to the use of a cardiopulmonary bypass (CPB) during an open heart
surgery. CPB disturbs the balance between the regulatory forces of plasma and
interstitial fluid exchanged, such as hypoalbuminemia which is one of the main
factors contributing to tissue edema directly after CPB. In this study we evaluate
hypoalbuminemia as a predictor of patient’s outcome after open heart surgery.
Methods:Prospective, observational cohort study of patients with congenital
heart disease from 0 to 21 years of age admitted to the PCICU who underwent
open heart surgery. Demographics and clinical data were collected from baseline
through 4 days after surgery. Hypoalbuminemia was defined as normal >3.3g/dl,
mild 3.2-3.0g/dl, moderate 2.9-2.5g/dl and severe <2.5g/dl. Demographic data
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
were presented as mean and percentages. Logistic regression was used to evaluate
mortality rate. Kruskal-Wallis test was used to evaluate the type of hypoalbuminemia on length of stay and MV days. Two-way ANOVA was used to evaluate
levels of albumin over time between patients with or without CPB. Results: Most
patients had a RACHS score of 3 (38%). Overall mortality rate was 11.4%, where
67% patients had severe hypoalbuminemia. There is no association between mortality and CPB. Logistic regression showed that mortality was associated with
younger age. Severe hypoalbuminemia was associated with increased LOS, prolonged CPB time and higher RACHS score. Of overall mortality In the group of
patients without CPB, albumin levels dropped initially but gradually increased to
baseline levels. Patients in CPB albumin levels decreased but remained lower in
the ranges of mild to moderate hypoalbuminemia. Conclusions: Although there
was no direct association between CPB and patient survival, there was an association between CPB and development of hypolabuminemia. These findings suggest
that prospective management of severe hypoalbuminemia should be considered
to improve patients clinical course.
222
VARIATION OF VENTILATION PRACTICES WITH CENTER
VOLUME AFTER PEDIATRIC HEART SURGERY
Punkaj Gupta1, Xinyu Tang2, Jeffrey Gossett3, Christine Gall4, Casey Lauer5,
Thomas Rice6; 1Arkansas Children’s Hospital, Little Rock, AR, 2Arkansas Childrens Hospital, Little Rock, AR, 3Arkansas Children’s Hospital Researcher Institute, Little Rock, AR, 4Virtual PICU Systems, LLC, Los Angeles, CA, 5VPS, LLS,
Milwaukee, WI, 6Children’s Hospital of Wisconsin, Milwaukee, WI
Learning Objectives: Several studies have documented a relationship between
center volume and mortality after pediatric cardiac surgery. None of the existing literature to-date has truly compared the volume-outcome relationship with
mechanical ventilation after pediatric cardiac surgery as an outcome. To address
these knowledge gaps, we undertook this project to evaluate the odds of mechanical ventilation, and duration of mechanical ventilation after pediatric cardiac
surgery across centers of varying center volume using the Virtual PICU Systems
(VPS, LLC) Database. Methods:Patients <18 years of age undergoing operations
(with or without cardiopulmonary bypass) for congenital heart disease at one of
the participating ICUs in the VPS database were included (2009-2013). Center
volume was defined as average number of cardiac surgery cases per year for each
center during the study period. Logistic regression models and Cox proportional
hazards models were fitted for the probability of conventional mechanical ventilation, and duration of mechanical ventilation respectively to investigate the
difference in the outcomes between different center volume groups with/without
adjustment for other risk factors. Results: 10,378 patients from 43 centers qualified for inclusion. Of these, 7,648 (74%) patients received conventional mechanical ventilation after cardiac surgery. Higher center volume was significantly
associated with lower odds of mechanical ventilation after cardiac surgery (odds
ratio in centers with 275 cases per year = 2.68 [95% CI: 2.15- 3.35], p<0.001).
However, patients receiving mechanical ventilation in these centers were associated with longer duration of mechanical ventilation, compared to lower volume
centers (hazard ratio in centers with 275 cases per year = 1.26 [95% CI: 1.161.37], p<0.001). This association was most prominent in the lower surgical risk
categories. Conclusions: Large clinical practice variations were demonstrated for
mechanical ventilation following pediatric cardiac among ICUs of varied center
volumes.
223
CEREBRAL OXYGENATION AND HEMODYNAMICS IN NEONATES AFTER CARDIAC SURGERY
Eric Peters1, Fernando Beltramo2, Alicia DeMarco1, Sylvia Del Castillo1; 1Children’s Hospital Los Angeles, Los Angeles, USA, 2Miami Children’s Hospital,
Miami, USA
Learning Objectives: Near-Infrared Spectroscopy (NIRS) monitoring is a
method of evaluating regional cerebral (cSaO2) and other regional oxygen saturations that has become increasingly common in the perioperative management of
patients with complex congenital heart disease. Although data regarding its use
in the operating room during cardiopulmonary bypass has been published, there
are few articles that describe both cerebral and renal oximetry behavior postoperatively in neonates and its correlation with other hemodynamic parameters such
as heart rate, blood pressure, central venous pressure, and pulse oximetry. Methods: Data was collected 24 hours post-operatively for neonates (<28 days of life)
with either cyanotic or acyanotic congenital heart disease who had undergone a
surgical intervention. Data recorded included cSaO2, renal regional saturation
(rSaO2), heart rate, mean arterial blood pressure (MAP), central venous pressure (CVP), and systemic oxygen saturation (SpO2). The data for all variables
was plotted in a graph for each two hour time period. These graphs were visually
inspected to identify the trends, and their temporal relationships, for each of the
variables. Results: Data was collected for 17 neonates. 10 (59%) were male, 7
(41%) were female. The median age of the patients at the time of surgery was
7 days of life. The median weight was 3kg. 10 (59%) patients pre-operatively
had cyanotic lesions, 7 (41%) had acyanotic lesions. 8 (47%) of the patients
underwent single ventricle palliation. The timing of significant changes in cSaO2
and rSaO2 tended to reflect changes in other hemodynamic variables such as
MAP and SpO2, but the NIRS monitoring did not consistently change prior
to the other hemodynamic parameters for patients with either cyanotic or acyanotic heart lesions. Conclusions: For neonates with congenital heart disease in
the immediate post-operative time period changes in cerebral and renal oxygen
saturation were associated with, but did not precede, changes in other commonly
monitored hemodynamic parameters.
224
DATA DRIVEN MATHEMATICAL MODELING OF THE SINGLE VENTRICLE ANATOMY AND PHYSIOLOGY
Michael McCulloch1, Lei Chen2, Gilberto Schleiniger2, Tobin Driscoll2; 1Alfred
I DuPont Hospital for Children, Wilmington, DE, 2University of Delaware,
Newark, DE
Learning Objectives: The greatest challenge in treating newborns with hypoplastic left heart syndrome (HLHS) is a dependence on non-specific, slowly developing surrogate measures of systemic oxygen delivery(DO2) such as urine output,
serum lactate and systemic blood pressure. Herein we describe our preliminary
experience analyzing continuous waveform data from HLHS patients in an effort
to provide an instantaneous predictor of impending cardiovascular compromise.
Methods: Arterial waveforms were collected from HLHS neonates and infants
≤4 months of age with indwelling arterial catheters following stage I Norwood
procedure with 3.5 mm B-T shunt. The computer software ixTrend converted
these waveforms to numerical data at 8 ms intervals, which was then processed to
produce heart rate, stroke volume (SV, area under the arterial waveform curve)
and cardiac output (CO, product of heart rate and stroke volume) measurements.
Using both mean values and measures of sample entropy (iRAD, a measure of
distributional asymmetry), statistical and clustering analyses were performed to
assess the model’s ability to predict periods of inadequate DO2. Results: Three
patients had lactates greater than 2. The first 15 minutes of data after initial lactate elevation (T1) were compared to the two preceding 30-minute intervals(T2
and T3). Mean calculated CO {T1 960, T2 930 (change 3.1%), T3 620 (change
54.8%)} and HR {T1 166, T2 160.3 (change 3.6%), T3 139 (change 19.4%)} both
progressively increased while SV {T1 5.9, T2 6.1 (change -3.9%), T3 6.4 (change
-9%)} progressively decreased before documentation of lactate elevation. Further,
iRAD calculations comparing T1 with T2 and T1 with T3 demonstrated marked
decreases in data variation with closer proximity to lactate elevation {(HR 0.3 vs
0.68), (SV 0.19 vs 0.22), (CO 0.18 vs 0.41)} suggesting decreasing hemodynamic
variability with impending hemodynamic compromise. Conclusions:Our early
work suggests this strategy can inform clinicians of impending arterial lactate
elevations in HLHS patients. This individualized approach may allow for preventative interventions and improved outcomes.
Poster Session: CPR/Resuscitation 1
225
PHYSIOLOGICAL MONITORING OF CPR QUALITY IS ASSOCIATED WITH IMPROVED SURVIVAL FROM CARDIAC
ARREST
Peter Meaney1, Benjamin French2, Christopher Parshuram3, Stephen Schexnayder4, Dana Edelson5, Benjamin Abella6, Raina Merchant6, Robert Sutton7;
1
Children’s Hospital Of Philadelphia, Philadelphia, PA, 2The University of
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Pennsylvania School of Medicine, Philadelphia, PA, 3The Hospital for Sick Children, Toronto, ON, 4University of Arkansas For Medical Sciences, Little Rock,
AR, 5The University of Chicago, Chicago, IL, 6University of Pennsylvania Health
System, Philadelphia, PA, 7Children’s Hospital of Philadelphia, Philadelphia, PA
Learning Objectives: The American Heart Association (AHA) recommends
monitoring CPR quality using diastolic blood pressure (DBP) and end tidal carbon dioxide (ETCO2). The objective of this study is to assess whether the use of
DBP or ETCO2 to monitor in-hospital CPR quality is associated with return of
spontaneous circulation (ROSC). Methods: This was a Get with the Guidelines
– Resuscitation (GWTG-R) Registry prospective, multisite, observational study
of all in-hospital CPR events reported from 2000 – 2012. Events without an arterial catheter or invasive airway in place at the time of arrest were excluded from
the DBP and ETCO2 cohorts, respectively. The primary predictor variables –
reported use of DBP or ETCO2 – were obtained from the GWTG-R CPR quality section. Logistic regression models accounting for clustering of patients within
hospitals were used to estimate the associations between quality monitoring and
ROSC. Other candidate variables were included a priori or if their adjustment
resulted in >10% absolute change in the effect estimate for monitoring. Results:
Among 245,300 events, 16,301 (6.6%) were included in the DBP cohort, of
these 11,259 (69%) had ROSC and 4212 (26%) had DBP used to monitor CPR
quality; 47,135 (19%) were included in the ETCO2 cohort, of these 30,980
(66%) had ROSC and 1648 (3.5%) had ETCO2 used to monitor CPR quality.
After adjustment for age, sex, race, year of arrest, first pulseless rhythm, duration
of arrest, and other confounders, the use of DBP (OR 1.23, CI95 1.12 – 1.36;
p<0.001) and ETCO2 (OR 1.25, CI95 1.10 – 1.43; p<0.001) were both associated with improved ROSC. In the subset of events in which ETCO2 was used,
achieving an ETCO2 > 10mmHg was also associated with improved ROSC (OR
2.11, CI95 1.63 – 2.72; p<0.001) compared to events were ETCO2 > 10mmHg
was never achieved. Conclusions: The use of DBP and ETCO2 to guide inhospital CPR quality is not common, even if available at the onset of arrest.
However, monitoring CPR quality with either was associated with significantly
improved event survival outcome even after controlling for important patient and
event confounders.
228
DELIRIUM IN SURVIVORS OF CARDIAC ARREST TREATED
WITH MILD THERAPEUTIC HYPOTHERMIA
226
DEFINING HEAD-TILT POSITION OF RESUSCITATION
Divya Gutala1, Malvi Hemani1, Steven Chen1, Grant Kitchen1, Robert Allen1,
Soumyadipta Acharya1, Thangamadhan Bosemani1, Utpal Bhalala1; 1Johns Hopkins University, Baltimore, MD
Learning Objectives: Head-tilt maneuver assists with achieving and maintaining airway patency during resuscitation. The relationship between degree/angle
of head-tilt and airway patency has not been defined. We hypothesized that a
specific degree or angle of head-tilt is associated with airway patency in children. Methods: We performed a retrospective study of MRI of head of children
(0-5 years) from January 1984-December 2013, to define the angle of head-tilt
for airway patency. We excluded MRIs with an artificial or malformed airway.
On sagittal and axial MRI images, we measured AP and lateral airway diameters at the level of palate and tongue. We defined head-tilt angle as the angle
between occipito-ophisthion and ophisthion-C7 spine line in sagittal MRI view.
We evaluated medical records for underlying medical condition and exposure
to sedation during MRI. We compared mean ± SD of the measurements using
student t-test with p<0.05 as significant. Results: Out of 1956 children that
underwent MRI of head, 1714 were excluded due to an artificial or malformed
airway. Of the remaining 242 children, 29 infants and 99 toddlers had airway
occlusion. In those with open airway, 82 had exposure to sedative or underlying brain disease. The airway diameters (mean ± SD) in spontaneously breathing, sedated or obtunded infants and toddlers with open airway were 5.9 ± 2.0,
7.9 ± 3.0 mm (AP at palate); 7.4 ± 2.9, 6.7 ± 3.0 mm (AP at tongue); 6.3 ± 1.6,
13.0 ± 0.4 mm (lateral), respectively. The mean head-tilt angle (121.90 ± 11.18 in
infants, 118.34 ± 6.56 in toddlers) associated with open airway in spontaneously
breathing, sedated or obtunded children was significantly different from mean
angle of a blocked airway in flexion (136.88 ± 7.32 in infants, 136.54 ± 2.29 in
toddlers) and hyper-extension (101.73 ± 8.31 in infants, 101.56 ± 7.29 in toddlers) (p ≤ 0.05). Conclusions: The mean head-tilt angle with a patent airway in
spontaneously breathing, sedated children (0-5 years) is 121.90 ± 11.18 in infants
and 118.34 ± 6.56 in toddlers. This information would help to create a built-in
shoulder roll within a resuscitation mat.
Jeremy Pollock1,2, Ryan Hollenbeck3, Benjamin Homes3, Michael Young3, Li
Wang4, E. Wesley Ely5, John McPherson3, Eduard Vasilevskis6; 1N/A, N/A,
2
University of Maryland Medical Center, Baltimore, MD, 3Vanderbilt University, Nashville, TN, 4Vanderbilt University, Nasvhille, TN, 5Vanderbilt University School of Medicine, Nashville, TN, 6Vanderbilt University Medical Center,
Nashville, TN
Learning Objectives: Mild therapeutic hypothermia (TH) is a recommended
treatment for comatose patients resuscitated from cardiac arrest. To our knowledge, the incidence of delirium and its associated risk factors has not been assessed
in survivors of cardiac arrest treated with TH. Methods: Retrospective analysis
was performed on 251 consecutive comatose survivors of cardiac arrest treated
with TH from 2007 to 2013 at Vanderbilt University Medical Center following
sudden cardiac arrest. The incidence and duration of delirium were measured
in patients who awoke from coma after cardiac arrest and survived to ICU discharge. Delirium evaluations began after TH (temp >36 degrees Celsius), and
were performed at least daily using the Richmond Agitation-Sedation Scale and
the Confusion Assessment Method for the ICU. A multivariable logistic regression analysis was performed to examine the effect of cardiac arrest and post-arrest
management characteristics (prior to warming) on delirium duration. This model
adjusted for age, APACHE II score, time to cardiopulmonary resuscitation
(CPR), time from CPR to return of spontaneous circulation (ROSC), bystander
CPR, initial rhythm (ventricular fibrillation/tachycardia, pulseless electrical activity/asystole), total dose of midazolam, and total dose of propofol. Results: Of the
251 patients analyzed, 107 (43%) survived and awoke from coma; 107 (100%)
of the survivors had at least one day of delirium in the ICU. The median number
of delirium days was 4.0 (2.0 - 7.5 IQR). The majority of delirium was hypoactive (90%). The majority of delirium was hypoactive (90%). Multivariable analysis showed that severity of illness (OR 1.77, 95% CI 1.00 - 3.15 p= 0.05) and
longer times from CPR to ROSC (OR 1.53, 95% CI 1.12 - 2.09, p=0.01) were
significantly associated with increased number of delirium days. Conclusions:
Delirium occurred in all survivors of cardiac arrest who awoke from coma. Efforts
are needed to identify potential reversible risk-factors for delirium in hopes of
reducing incidence and improving outcomes.
229
227
CARDIOPULMONARY RESUSCITATION IN
ONBOARD COMMERCIAL AIRLINE FLIGHTS
in-flight pediatric cardiac arrests from 2009 to 2013 reported to a ground-based
medical support (GBMS) center covering ~35% of all commercial airline traffic
worldwide were reviewed. Cases were assisted in real time by GBMS emergency
physicians with expertise in aviation medicine and airline protocols. Operational
details, basic subject demographic information, comorbidities, nature of the
emergency, and outcomes were obtained and treated with descriptive statistics.
Results:Fifteen cases (0.12%) of cardiac arrest were identified among 12,226
pediatric in-flight medical emergencies (1 in 815) in 77 airlines from 6 continents. All cases received CPR and assistance was mostly provided by physician
passenger volunteers (66.7%). An AED was used in 40% of cases and none had
an indication for shock. Aircraft diversion occurred in 9 cases (60%). Sustained
return of spontaneous circulation (ROSC) occurred in only 1 subject (6.7%)
who was then transported to a hospital following aircraft diversion. Most cases
of cardiorespiratory arrest (11 of 15 [73.3%]) involved subjects younger than 2
years of age, the age until which children are allowed to share a seat with an adult
(lap infants). Five of those 11 patients (45.5%) did not have a known pre-existing
condition and were found pulseless and apneic, akin to what is seen in sudden
unexpected infant death (SUID). Conclusions: Despite high rates of bystander
CPR led by a medical volunteer, and rapid access to emergency medications and
AEDs, the rate of sustained ROSC in children experiencing cardiorespiratory
arrest onboard commercial airline flights is low and in-line with other out-ofhospital arrest situations.
CHILDREN
Alexandre Rotta1, Paulo Alves2, Richard Speicher1, Karen Lidsky1, Steven Shein1,
Veerasathpurush Allareddy3, Neil Nerwich2, Veerajalandhar Allareddy4; 1Rainbow Babies & Children’s Hospital, Cleveland, OH, 2MedAire Inc., Tempe, AZ,
3
University of Iowa, Iowa City, IA, 4Rainbow Babies and Children’s Hospital,
Cleveland, OH
Learning Objectives: Pediatric cardiac arrests onboard commercial airline
flights are unique due to close proximity of subjects and rescuers, widespread
presence of volunteers proficient in CPR, and availability of emergency medications and AEDs. However, access to definitive care can be significantly delayed,
even when aircraft diversion is possible. We attempt to characterize outcomes
of in-flight CPR involving children using a worldwide sample. Methods: All
METHOD OF COOLING IS NOT ASSOCIATED WITH
CHANGES IN SURVIVAL FOR THERAPEUTIC HYPOTHERMIA PATIENTS
Ian Butler1, Michelle Root1, James Curtis1; 1The Chester County Hospital, West
Chester, PA
Learning Objectives: There are multiple methods used to induce hypothermia
in post-cardiac arrest (PCA) patients undergoing therapeutic hypothermia (TH),
but there is uncertainty surrounding whether the method used impacts survival.
We hypothesized that an intravascular cooling device would not be associated
with a difference in mortality when compared to surface cooling. Methods: We
conducted a retrospective analysis of data collected on all PCA patients admitted
between 2/2011 and 3/2014 and treated with 24 hours of hypothermia (goal
32-34C). We identified 26 patients with complete data including cooling method
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
used, demographics, comorbidities, type of arrest, and survival at discharge. Time
to target temperature (TTT) was defined as minutes from initiation of TH to
temperature <34C. A change in our hospital protocol allowed for two distinct
groups based on the type of cooling device used in their care: patients undergoing
intravascular vs surface cooling. Results: The following did not differ between
the intravascular-cooling group (ICG, n = 15) and surface-cooling group (SCG
n = 11): shockable rhythm (n = 9 (60%) vs n = 9 (81.8%), p = 0.23), or presence
of 2 or more comorbidities (n = 6 (40%) vs n = 7 (63.6%), p = 0.23). Average
TTT in minutes for the ICG was 164 versus 202 in the SCG (p = 0.66). Of
note, there was a difference in average age between the two populations (50 vs
63.5, p = 0.02). Eleven patients (73.3%) in the ICG survived to discharge versus
eight (72.7%) in the SCG (Odds ratio 0.97; 95% confidence interval, 0.17 to
5.6, p = 0.97). Conclusions: Among a small number of comatose PCA patients
treated with hypothermia, use of a intravascular cooling device was not associated
with changes in survival rates when compared to a surface cooling device. Of
note, there was a trend towards shorter times to target temperature in the ICG
though this did not reach statistical significance.
230
DEVELOPMENT OF AN INNOVATIVE IN-SITU CARDIAC
ARREST SIMULATION TRAINING PROGRAM
David Carlbom1, Margaret Chapman2, Chris Laux1; 1Harborview Medical Center, Seattle, WA, 2Northwestern Memorial Hospital, Chicago, IL
Learning Objectives: Code Blue teams consist of multiple healthcare providers
who rapidly assemble to deal with in-hospital, life-threatening emergencies,
predominantly cardiac arrest. Code team members may have limited knowledge of each others expertise and role delineation can be confusing. Immediate
feedback regarding chest compression quality, a comprehensive resuscitation
training program, and strong leadership are metrics that have been shown
to impact outcomes after a Code Blue response. Methods: We developed an
innovative, realistic Cardiac Arrest Simulation Training Program with in-situ
training sessions for the members of a Code Blue response team. The training
program used unannounced mock codes, structured debriefing, and physician
leadership training. Specific roles and tasks were pre-assigned based on each
member’s clinical title. Team assembly time was compared before and after the
simulation training. Chest compression quality information was collected during mock codes using a portable full-scale mannequin simulator. We used a
survey after each simulation to evaluate the effectiveness of the team. Outcome
data for actual resuscitations were obtained from hospital documentation and
compared before and after the education. Results: Mean team assembly time
decreased from 4 min (SD 1.9 min) to 3 min (SD 1.4 min). Average compression depth increased from 41.3mm to 43.2mm with simulation and live feedback. Compression rate remained stable between 110 and 112 compressions
per minute. Return of spontaneous circulation occurred in 68% of cases before
the training and 78% after the intervention. Cardiac arrest survival to hospital
discharge improved from 26% to 30%. Team members rated positive leadership
qualities as “always happening” 69% of simulations. Conclusions: An innovative training program using high-fidelity simulation and structured instruction
was associated with improved multidisciplinary teamwork, patient-care processes, and survival rates.
231
EFFECT OF HYPOTHERMIA ON POST-RESUSCITATION
CEREBRAL MICROCIRCULATION IN A RAT MODEL OF CPR
Haifang Yu1,2, Lu Yin1, Jiangang Wang1, Shen Zhao1, JIE QIAN1, Xiaobo Wu3,
Jena Cahoon4, Wanchun Tang1; 1Weil Institute of Critical Care Medicine, Rancho Mirage, CA, 2West China Hospital of Sichuan University, Chengdu, Sichuan, China, 3Weil Institue of Critical Care Medicine, Rancho Mirage, CA, 4the
Weil Institute of Critical Care Medicine, Rancho Mirage, CA
Learning Objectives: Therapeutic hypothermia improves the outcomes of
cerebral function after resuscitation from cardiac arrest (CA). However, the
neuroprotective mechanism of therapeutic hypothermia following CPR is
less defined. In the present study, we investigated the effect of therapeutic
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
hypothermia on the cerebral cortex microcirculation in a rat model. We hypothesized that mild hypothermia is associated with an improved cerebral cortex
microcirculation. Methods:Thirty male Sprague-Dawley rats (450-550g)
were randomized into three groups: 1) normothermia group (NT, n=10) : the
temperature of the rats was maintained at 37 ± 0.5°C for 6 hrs; 2) intra-arrest
hypothermia group (IAH, n=10): hypothermia of 33 ± 0.5°C was started at the
same time with the initiation of CPR and maintained for 6 hrs; 3) post-resuscitation hypothermia (PRH, n=10): hypothermia of 33 ± 0.5°C was started 5
mins after the return of spontaneous circulation (ROSC) and maintained for
6 hrs. In all groups, ventricular fibrillation (VF) was electrically induced and
CPR was initiated after 8 mins of untreated VF and continued for 8 mins.
Defibrillation was then attempted. Hemodynamics, electrocardiogram and
body temperature were continuously recorded. Cerebral cortex microcirculation were measured at baseline, 1, 3 and 6 hrs after ROSC. Results:All animals were successfully resuscitated. The duration of CPR of the NT, IAH and
PRH groups were 563.1 ± 76.3, 486.8 ± 47.6 and 567 ± 54. The numbers of
defibrillation were 5.5 ± 3.1, 3 ± 2.4 and 5.1 ± 2.12, respectively. Compared to
the NT and PRH groups, the duration of CPR and numbers of defibrillation of the IAH group were significantly reduced (p<0.05). Microvascular flow
indexes (MFI) of all groups were reduced at 1, 3 and 6 hrs after ROSC. However, more significant reduction was observed in the NT group (p<0.05). The
MFI of NT were 2.22 ± 21, 2.19 ± 0.15 and 1.87 ± 0.31 at 1, 3 and 6 hrs. The
IAH were 2.47 ± 0.13, 2.48 ± 0.19 and 2.22 ± 0.07. The PRH were 2.38 ± 0.11,
2.41 ± 0.24 and 2.17 ± 0.16. Conclusions: Hypothermia during CPR reduces
the duration of CPR, number of defibrillations and improves the cerebral cortex microcirculation.
232
EVALUATION OF POST-INTUBATION HYPOTENSION USING
PRE-INTUBATION SHOCK INDEX AND MODIFIED SHOCK
INDEX
Sangita Trivedi1, Onur Demirci1, Grace Arteaga1, Rahul Kashyap1, Nathan Smischney1; 1Mayo Clinic, Rochester, MN
Learning Objectives: Pre-intubation Shock Index (SI) and Modified Shock
Index (MSI) have demonstrated predictive capability for post-intubation
hypotension (PIH) in emergency department. Primary aim of our study was
to explore the relationship between SI and MSI with the development of postintubation hemodynamic instability in critical care unit. The secondary aims
were to evaluate the relationship of these indices with intensive care unit (ICU)
mortality, ICU length of stay (LOS), and 30-day mortality. Methods: This
was a non-concurrent cohort study, conducted from Jan 2010 to Dec 2011
in medical and surgical ICUs at a tertiary care medical center. A total of 333
patients were emergently intubated in the ICU. Of these, 140 patients met
inclusion criteria=>18 years old, and hemodynamically stable 60-minutes prior
to emergent intubation. SI=heart rate (HR)/systolic blood pressure (SBP)
and MSI=HR/mean arterial pressure (MAP) were evaluated to predict postintubation hemodynamic instability defined by SBP <90 mmHg (PIH), MAP
<65 mmHg, and use of vasopressors within 1 hour of intubation. Results:
Pre-intubation SI >0.9 had a significant association with SBP <90 mm Hg in
the Univariate model [OR=2.1; 95%CI (1.07-4.35)]. However, the association
was not significant in the Multivariate model after adjusting for confounders
(age, sepsis, fluid administration within 24-hours) [OR=1.3; 95%CI (0.533.57)]. Pre-intubation SI >0.9 was also associated with higher ICU mortality
in both Univariate [OR=4.5; 95%CI (1.26-12.67)] and Multivariate analyses
[OR=4.5; 95%CI (1.42-17.75)] after adjusting for confounders. There was no
association of MSI with post-intubation hemodynamic instability and ICU
mortality; and of pre-intubation SI and MSI with ICU LOS and 30-day mortality. Conclusions: Our findings indicate Shock Index >0.9 is a predictor of
ICU mortality in emergently intubated adult patients. However, we did not
find its association with SBP <90 mm Hg after adjusting for confounders; and
with 30-day mortality or ICU LOS. Modified Shock Index was not associated
with any of the outcomes of interest.
Poster Session: CPR/Resuscitation 2
233
235
OUTCOMES OF DELAYED RRT ACTIVATION IN PATIENTS
TRANSFERRING TO THE ICU
HOW WELL DO WE DOCUMENT NEONATAL RESUSCITATION? AMEND (ASSESSMENT OF NEONATAL DOCUMENTATION) STUDY
Amelia Barwise1, Charat Thongprayoon1, Vitaly Herasevich1, Brian Pickering2,
Ognjen Gajic3, Jeff Jensen1; 1Mayo Clinic, Rochester, MN, 2Mayo Clinic - College
of Medicine, Rochester, MN, 3Mayo Graduate School of Medicine(Rochester),
Rochester, MN
Learning Objectives: The Rapid Response Team (RRT) was designed to reduce
serious adverse events such as cardiac arrest on the floor by activating a “critical
care team” to the bedside of the deteriorating patient. To date there has been
mixed evidence about the effectiveness of rapid response teams in decreasing patient mortality and in reducing adverse outcomes. To be most effective,
the RRT should be activated early in the course of physiological deterioration.
This study examines the effect of delay on RRT activation on hospital mortality
and morbidity. It was hypothesized that delay in RRT activation would result
in worse patient outcomes. Methods: A retrospective cohort study of all the
Rapid Response Team (RRT) activations taking place between January 2012
and December 2012 was performed in a tertiary academic center. The subjects
were patients admitted to the ICU following a RRT activation. Data was compared between those patients who had a timely RRT activation (60 minutes),
after adjustment for patient characteristics using multivariate Cox proportional
regression analysis. The primary outcome was 30-Day mortality after RRT activation. The secondary outcomes were hospital and ICU length of stay, mechanical
ventilator and vasopressor use in ICU. Results: Of 1120 patients who required
ICU admission after RRT call, 698 (62%) had >60 minute delay in RRT activation. Patients who experienced delay in RRT activation after meeting physiologic
RRT criteria had increased mortality (adjusted hazard ratio 1.5 (95% 1.05-2.2):
p=0.02. Mortality was positively correlated with increased time in hours from
first abnormal vital sign to RRT activation (adjusted Hazards Ratio 1.03) (95%
1.01-1.04): p=0.001. Patients with delayed activation had increased ICU length
of stay, p=0.004, increased ventilator use, p= 0.04 and vasopressor use, p < 0.001.
Conclusions:Delayed RRT activation occurred frequently and was independently associated with increased mortality and ICU resource utilization.
234
EXPRESSION OF SUPEROXIDE DISMUTASE AND NF-ΚB IS
AUGMENTED IN THE HIPPOCAMPUS OF RATS DURING
CPR
Jihong Xing1, Jian Lu2, Xiaoliang Liu3; 1First Hospital of Jilin University, Changchun, China, 2Jilin Province Carcinoma Hospital, Changchun, China, 3First Hospital of Jilin University, Changchun, Jilin
Learning Objectives: Superoxide dismutases (SOD) is considered as an important antioxidant. NF-kB is a crucial transcription factor in involvement of cellular responses to stressors and cellular survival. The purpose of this study was to
determine the role played by antioxidant in regulating the augmented NF-kB
responses in the rat hippocampus after transient global ischemia induced by
cardiac arrest (CA) and cardiopulmonary resuscitation (CPR). We hypothesized
that protein expression of SOD and NF-kB are upregulated in the rat hippocampus during CPR and that maintained SOD decreases expression of NF-kB
in the processing of oxidative stress. Methods:The rat model of CA induced by
asphyxia was used in the current study. The rats who survived were sacrificed 0
hrs as control (n=20), 3 hrs (n=20) and 6 hrs (n=20) after CPR and the hippocampus was obtained for western blot analysis to examine the levels of SOD.
Also, NF-kB in the hippocampus was assessed in control rats (n=12), and rats
(n=12) who survived for 6 hrs after CPR and received administration of tempol (a
mimetic of SOD) (i.v.30mg/kg) and rats who survived for 6 hrs without tempol
(n=12). Note that all data are presented as mean ± SE and analyzed by ANOVA.
Results: SOD was significantly increased in the hippocampus 3-6 hrs after CA.
Namely, optical density of SOD was 1.01 ± 0.01 (control); 1.17 ± 0.01 (3 hrs);
and 1.43 ± 0.03 (6 hrs). Note that P<0.05 was seen in control and 3 hrs group vs.
6 hrs group. There was no significant difference between control and 3 hrs interventions. In addition, a significant increase in expression of NF-κB was observed
in rats’ hippocampus 6 hrs after CA compared with control (P<0.05); however,
increased NF-κB was significantly inhibited in rats with tempol administration
(P<0.05). Conclusions: The protein levels of SOD and NF-κB are increased in
the hippocampus during CPR. Supplement of SOD mimetic for anti-oxidation
suppresses the expression of NF-κB in the hippocampus of rats with CA, suggesting that antioxidant is likely to play a beneficial role in regulating cerebral
ischemia reperfusion via NF-κB nucleus transcription pathways.
Matthew Braga1, Gautham Suresh1; 1Children’s Hospital at Dartmouth, Lebanon, NH
Learning Objectives: Adequate documentation of neonatal resuscitation is essential to
measure and improve the quality of resuscitation, but there are no universally accepted
criteria or evaluation methods for such documentation. We aimed to determine the
adequacy of neonatal documentation (which has never been studied in the US), and
to determine patient, provider and institutional factors associated with completeness of
such documentation. Methods: This was a multi-center (six institution) retrospective
study of a sample of sequentially born Very Low Birth Weight infants in 2013. The
description of resuscitation in each infant’s record was evaluated for the presence or
absence of 29 Ideal Data Items that together would constitute comprehensive documentation. Each record was then assigned a Documentation Score and covariates associated with this Score identified using multiple linear regression. Results: Charts of 263
infants were reviewed. The median gestational age was 28.4 weeks, and the median birth
weight 1050 grams. Of the infants, 66% were singletons, and 74% were delivered by
Cesarean section. The median (interquartile) Documentation Score was 14 (11, 16) out
of a total possible score of 29. Items most frequently present were; review of obstetric history (98%), apgar scores (96%), oxygen use (77%), suctioning (71%), and stimulation
(62%). Items consistently absent were; room and infant temperature (0%), pre delivery
briefing (2%), personnel present (2%), equipment check (20%), and family presence
(40%). In our completely adjusted model only the institution and documentation by
a resident were significantly associated with the Documentation Score. Conclusions:
Neonatal resuscitation documentation was frequently missing Ideal Data Items. Variation in documentation was mostly dependent on the institution, and not on characteristics of the infants or individual providers. Standardization of neonatal documentation
can ensure more comprehensive documentation of neonatal resuscitation.
236
BLOOD LACTATE LEVELS AFTER CARDIAC ARREST
Antonio Dell’Anna1, Irene Lamanna1, Ilaria Belloni1, Katia Donadello2, JeanLouis Vincent3, Fabio Silvio Taccone1; 1Erasme Hospital, Brussels, Belgium,
2
N/A, Brussels, Belgium, 3Erasme University Hospital, Brussels, Belgium
Learning Objectives: We lack reliable biomarkers to guide the management of patients
after cardiac arrest (CA). Blood lactate levels (Lac) and their time course have been
related to mortality in various groups of acutely ill patients. We explored the relationship
between Lac during the first 48 hours after CA and neurological outcome. Methods: In
a retrospective analysis of a single-center database of adult patients (> 18 years) admitted
to our Dept. of Intensive Care after CA who survived for at least 24 hours, we retrieved
all data concerning CA characteristics, hemodynamic variables (heart rate [HR], mean
arterial pressure [MAP]), cardiovascular SOFA (cSOFA) score, and Lac on admission
and after 6, 12, 24 and 48 hours. We also studied the decline in Lac concentration
(DLC) over time as absolute changes per hour (mEq/L.h) or as the percentage variation
from the baseline (DLC%). Results: We enrolled 214 patients (66% male, 59% outof-hospital CA, 62 ± 15.5 yrs of age), of whom 74 (35%) had a favorable neurological
outcome (FO) at 3 months (CPC1-2). Patients with poor neurological outcome (PO)
at 3 months were less likely to receive bystander CPR and to be found in VF/VT as
presenting rhythm (57% vs. 73%, p=0.025; 28% vs. 76%, p<0.001, respectively). pH,
pO2 and pCO2 did not differ between FO and PO, while lactate at admission was significantly lower in patients with FO (2.5 [1.4÷5.6] vs. 4.7[2.4÷8.7] mEq/L, p<0.001),
as well as cardiovascular SOFA (0 [0÷3] vs. 2[0 ÷4], p=0.046). Differences in lactate
concentrations were also found also at each subsequent time point between the two
groups. On the opposite DLC did not differ between groups. Similarly, HR and MAP
did not show any differences between FO and PO neither on admission nor at any
time point. In a multivariable model adjusted for known confounders (age, VF/VT,
bystander CPR, cSOFA on admission), lactate on admission emerged as a significant
predictor of PO (OR 0.87, 95%CI 0.78-0.96). Conclusions: Lac levels on admission
are an independent predictor of PO after CA, while changes in lactate levels and other
hemodynamic variables were not correlated with outcome.
237
EFFECTS OF PROGESTERONE ON NEUROLOGICAL OUTCOMES IN A RAT MODEL OF CARDIAC ARREST AND
RESUSCITATION
Jiangang Wang1,2, Xiaobo Wu3, Shen Zhao1, JIE QIAN1, Zhengfei Yang4, Haifang
Yu1, Jena Cahoon5, Wanchun Tang1; 1Weil Institute of Critical Care Medicine,
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Rancho Mirage, CA, 2Hangzhou Emergency Center, Hangzhou, China, 3Weil
Institue of Critical Care Medicine, Rancho Mirage, CA, 4N/A, Guangzhou,
Guangdong, 5the Weil Institute of Critical Care Medicine, Rancho Mirage, CA
Learning Objectives: A large number of survivors from cardiac arrest and resuscitation
suffer permanent brain damage. Previous animal studies have demonstrated the neuroprotective effects of progesterone in regional brain injury. In the present study, we investigated the neuroprotective effects of progesterone in global cerebral injuries as a result
from cardiac arrest and resuscitation. We hypothesized that progesterone administrated
during CPR resulted in better neurological outcomes. Methods: Fourteen male SpragueDawley rats weighing between 450-550g were randomized into two groups: 1) saline
(n=7); 2) progesterone (n=7). After 8 mins of untreated ventricular fibrillation, progesterone (25 mg/ml, 8 mg/kg) or saline was injected. Precordial compression and mechanical
ventilations were simultaneously initiated for 8 mins. Defibrillation was then attempted.
The neurological deficit score (NDS) was measured at 24-hr intervals for a total of 72 hrs.
The duration of survival was recorded. Results: All animals except for one in the saline
group were resuscitated. The NDS was significantly better in the progesterone group as
compared to the saline group at 48 and 72 hrs after resuscitation (223 ± 259 vs. 485 ± 40,
p< 0.05 at 48 hours; 285 ± 267 vs. 500 ± 0 at 72 hours, p< 0.05). Mean survival time was
50.4 hrs (95% CI: 31.77 – 68.89 hrs) in the progesterone group and 21.17 hrs (95% CI:
4.75 – 37.58 hrs) in the saline group (p< 0.05). Conclusions: The administration of progesterone during CPR improves the neurological outcomes and prolongs the duration of
survival after resuscitation in a rat model of ventricular fibrillation.
238
RETROSPECTIVE USE OF AN ELECTRONIC CHECKLIST AT
RAPID RESPONSE TEAM ACTIVATIONS: A CERTAIN STUDY
John O’Horo1, Ronaldo Sevilla Berrios1, Alice Gallo De Moraes1, Mazen O. AlQadi1, Pramod Guru1, Rahul Kashyap1, Oguz Kilickaya1, Ognjen Gajic2; 1Mayo
Clinic, Rochester, MN, 2Mayo Graduate School of Medicine(Rochester), Rochester, MN
Learning Objectives: Acute decompensation is a high stress situation which puts
strain on providers to make rapid decisions. Recall and memory have been the corner
stone of every approach used to standardized resuscitation algorithms, like on ATLS
and ACLS training, which is not necessarily reliable for stressed providers facing uncertain scenarios. We have created an electronic interactive checklist, the Checklist for
Early Recognition and Treatment of Acute Illness (CERTAIN), which allows providers to select a clinical syndrome, and use this framework to simultaneously assess and
treat a patient in an emergent situation. Although this software has shown promising
results in simulation testing, it is unclear how it would perform in a real uncontrolled
clinical situation. Methods: From the rapid response team (RRT) database maintained
in our tertiary academic medical center, we choose a random cluster of rapid response
team activations to retrospectively analyze. Four clinicians who serve as RRT leaders
independently reviewed a cluster of patients to evaluate if the syndromic approach in
CERTAIN adequately cover the spectrum of clinical decompensations seen in actual
hospital practice. Ratings were given on a 5 point Likert scale for whether CERTAIN
was perceived as useful, and if the practitioner would want to use it clinically for this
scenario. Results: A total of 76 patients were reviewed by 4 independent reviewers.
Average patient age was 65 ± 17, with 57% of them been male and 65.3% of them
were admitted to a non-surgical team. Overall, 65% of scenarios were rated as 3 or
higher for utility in guiding through the clinical scenario, and 58% as 4 or higher. The
most commonly used algorithms were all highly rated, medians of 5 [1-5] for cardiac
emergencies; 4 [2.5-5] for sepsis and hypotension, and; 4 [2-5] for dyspnea. The fourth
most common, altered mental status, demonstrated some room for improvement with
a median of 2 [1-4]. Conclusions: CERTAIN adequately covers the majority of commonly encountered clinical scenarios and was perceived useful by RRT leaders.
239
PROGNOSTIC VALUE OF MR DIFFUSION IMAGING IN CARDIAC ARREST PATIENTS TREATED WITH HYPOTHERMIA
THERAPY
Seung Mok Ryoo1, Won Young Kim1, Chang Hwan Sohn1, Shin Ahn1, Dong
Woo Seo1, Michael Donnino2, Kyoung Soo Lim1; 1Asan Medical Center, Seoul,
South Korea, 2Beth Israel Deaconess Medical Center, Boston, MA, USA
Learning Objectives: Diffusion-weighted magnetic resolution imaging (MRI) is
highly sensitive and specific in the detection of acute brain ischemia. Many of comatose post cardiac arrest patients have ischemic brain injury. The aim of this study was
to assess regional brain injury on MRI and to associate regional injury with neurologic outcome in patients treated with therapeutic hypothermia (TH) afterout-ofhospital cardiac arrest (OHCA) Methods: Multicenter, registry-based, retrospective
cohort study conducted in 24 hospitals across South Korea between January 2007
and December 2012. Of the 930 adult (≥18 years) non-traumatic OHCA patients
treated with TH, we included the patients who had a brain MRI in the first 1 week
after cardiac arrest. We compared the MRI findings of good neurologic outcome
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
(cerebral performance category score of 1 or 2) with bad neurologic outcome (cerebral
performance category score ≥3). Results: Of all 172 patients, 118 patients (68.6%)
had bad neurologic outcome. Total 106 patients had positive MRI findings and 102
patients of them were bad neurologic outcome. Positive MRI findings, defined as any
of regional brain injury lesion in MRI, had 86% of sensitivity, 93% of specificity, 96%
of positive predictive value, and 76% of negative predictive value for bad neurologic
outcome and if there are more than two regional brain injury lesion, positive predictive values increased up to 99%. In multivariate analysis, positive MRI finding (OR
72.51 [95% CI 18.25-288.15]) was associated with bad neurologic outcome. And
shockable initial rhythm (OR 0.19 [95% CI 0.05-0.78]) and pupil light reflex (OR
0.21 [95% CI 0.05-0.84]) had negative correlation with bad neurologic outcome.
Conclusions: Diffusion MRI was potentially helpful tools for predicting bad neurologic outcome in resuscitated comatose patients treated with TH after OHCA.
240
UNDERSTANDING HOW BASIC LIFE SUPPORT TRAINING
IS UTILIZED BY OUR MEDICAL STUDENTS ON CLINICAL
ROTATI
Nancy Stewart1, Audrey Tanksley2, Dana Edelson1, Vineet Arora1; 1The University of Chicago, Chicago, IL, 2University of Chicago, Chicago, IL
Learning Objectives: Although cardiopulmonary resuscitation (CPR) is the
mainstay of therapy for cardiac arrest patients, it is a complex psychomotor skill
that is difficult to perform well. We sought to understand how medical students
incorporate their Basic Life Support (BLS) training into their clinical clerkships.
Methods: All medical students at a single academic medical center received BLS
training and certification within 2 weeks of starting their first year, and recertification at the end of their second year. During the last 2 quarters of the year, an
anonymous, optional paper survey was distributed to all third year students during
the Internal Medicine Clerkship. During orientation week, all incoming interns
prior to ACLS training received the same anonymous optional survey. De-identified data were collected from paper survey responses. Results: Of the 61 M3 and
57 incoming interns surveyed, 72% M3 students and 81% of incoming interns
responded. Although 50% of M3s surveyed felt confident with compression skills,
only 16% knew the appropriate compression rate. In contrast to the M3s, 85%
of incoming interns felt confident with compression skills, and 60% correctly
answered the question on the appropriate rate of compressions. Of the 70% of
M3s who had witnessed a resuscitation attempt, only 39% of those students felt
prepared for their role. Of the incoming interns, 96% had witnessed a resuscitation attempt, only 50% felt prepared for their role. In fact, 45% of the M3s
who witnessed a code felt awkward, with 29% feeling marginalized, while 61% of
incoming interns who witnessed a code felt awkward, and 30% felt marginalized.
Out of all respondents, only 16% of M3s and 35% of incoming interns consider
themselves essential members of the code team. Conclusions: As students progressed through their medical training, they felt more comfortable with compression/ventilation skills. Many students reported not feeling prepared, or as though
they were a member of the code team. Educating medical students and residents
on the role of the student and how to involve them may improve their experience.
241
TIME TO TARGET TEMPERATURE DURING THERAPEUTIC HYPOTHERMIA AFTER CARDIAC ARREST: EFFECT ON
OUTCOME
Hangyul Chung-esaki1, Michael Mlynash1, Irina Eyngorn1, Karen Hirsch1; 1Stanford University, Stanford, CA
Learning Objectives: Therapeutic hypothermia (TH) improves neurologic
outcome after cardiac arrest, but the clinical significance of time to target
(TTT) remains unknown. Prior data suggest shorter TTT is associated with
improved neurologic outcome and survival, while other studies suggest shorter
TTT or early cooling within 180 minutes post-arrest are associated with
increased mortality. TTT may be a measure of TH efficacy or marker of disease
severity. In this study, we studied the association between TTT, initial temperature, and rate of cooling with neurologic outcome. Methods: This prospective,
observational study enrolled patients who remained comatose after successful
resuscitation after cardiac arrest. Patient characteristics, details of TH, including TTT and rate of cooling, and clinical and laboratory data were recorded.
Target temperature was set by the clinician (usually 33 ± 0.5 °C). Clinical outcomes data were collected at 1, 3, 6 and 12 months. Comparative statistics,
chi-square, Mann Whitney U, and t-tests were performed. A good outcome
was defined as a modified Rankin Scale ≤3 at 12 months. Results: 62 subjects
were included in the analysis. 39 patients (63%) were male, with mean age of
56.9 ± 2.3 (SEM) years. TH was continued for a mean duration of 23 hours ±
0.49. While 21 (34%) had a good outcome, TTT was not significantly different
between good and poor outcome groups (160 min (IQR 13-423) vs. 375 min
(103-542), p=0.24). Initial temperature and rate of cooling also did not differ
between outcome groups (35.9 ± 0.27 °C vs. 35.8 ± 0.21 °C, p=0.83; 0.020 °C/
min (IQR 0.004-0.199) vs. 0.006 °C /min (0.004-0.014), p=0.48). Among
other variables assessed, older age and higher neuron-specific enolase levels were
associated with poor outcome. Conclusions: TTT, initial temperature, and rate
of cooling were not significantly correlated with 12-month functional outcome,
though this study was limited by the sample size. Additional studies are needed
to better account for disease severity in this heterogeneous population and to
develop a more customized approach to TH in cardiac arrest patients.
Poster Session: CPR/Resuscitation 3
242
EXPRESSION OF HIF-1Α AND NF-ΚB IN THE HIPPOCAMPUS OF RATS INDUCED BY CARDIOPULMONARY
RESUSCITATION
Jihong Xing1, Jian Lu2, Xiaoliang Liu3; 1First Hospital of Jilin University, Changchun, China, 2Jilin Province Carcinoma Hospital, Changchun, China, 3First Hospital of Jilin University, Changchun, Jilin
Learning Objectives: Hypoxia inducible factor-1 (HIF-1) has an important contribution to pathophysiological changes of homeostasis under conditions of oxygen deprivation and ischemia. Accumulated subunit HIF-1α modulates the expression of several
target genes in protecting tissues against ischemia and infarction. In this study, we first
examined protein expression of HIF-1α in the rat hippocampus after transient global
ischemia induced by cardiac arrest (CA) and cardiopulmonary resuscitation (CPR).
In addition, we examined the effects of stabilization of HIF-1α by administration of
dimethyloxalylglycine (DMOG) on expression of the hippocampus’s NF-kB, a crucial
transcription factor involved in cellular responses to stressors as well as cellular survival.
Methods: The rat model of CA induced by asphyxia was used in the current study. The
rats who survived were sacrificed 0 hrs as control (n=12), 3 hrs (n=12) and 6 hrs (n=12)
after CPR and the hippocampus was obtained for western blot analysis to determine
the protein levels of HIF-1α. Also, NF-kB in the hippocampus was assessed in control
rats (n=12), and rats (n=12) who survived for 6 hrs after CPR without DMOG and
rats (n=12) who survived for 6 hrs and received DMOG administration (i.p.20 mg/
kg). All data are presented as mean ± SE and analyzed by ANOVA. Results: HIF1α was significantly increased in the hippocampus 3-6 hrs after CA. Namely, optical density of HIF-1α was 0.98 ± 0.02 (control); 1.27 ± 0.01 (3 hrs); and 1.41 ± 0.02
(6 hrs). P<0.05 was seen in all the time groups vs. control. There was no significant
difference between groups of 3 hrs and 6 hrs groups. Also, a significant increase in
expression of NF-κB was observed in rats’ hippocampus 6 hrs after CA compared with
control (P<0.05); however, increased NF-κB was significantly inhibited in rats with
DMOG administration (P <0.05). Conclusions:Transient global ischemia induced
by CA increases HIF-1α and NF-κB in the hippocampus of rats. Stabilization of HIF1α suppresses NF-κB during CPR, suggesting that the role for HIF-1α in alleviating
cerebral ischemia injury via NF-κB nucleus transcription mechanism.
243
COMBINATION THERAPY OF NIACIN AND SELENIUM
ATTENUATES BRAIN INJURY AND IMPROVES NEUROLOGICAL OUTCOME
Jae Seong Kim1, Woon Yong Kwon1, Gil Joon Suh2, Kyung Su Kim2, Kyoung
Min You2, Jihwan Bu2, Se Jong Lee2; 1Dept. of Emergency Medicine, Seoul
National University Hosp., Seoul, South Korea, 2Seoul National University Hospital, Seoul, South Korea
Learning Objectives: We performed this study to examine whether the combination therapy of clinically relevant doses of niacin and selenium attenuates
brain injury and improves neurological outcome after cardiac arrest in rats, and
to determine if its beneficial effects are associated with synergistic activation of
the glutathione redox cycle and down-regulation of the mitogen-activated protein kinase (MAPK) pathway. Methods: Ventricular fibrillation was induced in
male Sprague-Dawley rats. After 6 minutes of no flow time, cardiopulmonary
resuscitation was provided and return of spontaneous circulation (ROSC) was
achieved. Animals were then administered vehicle (CPR group), 360 mg/kg of
niacin (CPR + NA group), 60 μg/kg of selenium (CPR + Se group), or niacin
plus selenium (CPR + NA + Se group), respectively. Neurologic deficit scales
were scored at 24, 72 hours, and 7 days post-ROSC. Then, a separated set of
animals were sacrificed at 72 hours post-ROSC and brain tissues were harvested.
Results: The combination therapy of clinically relevant doses of niacin and selenium attenuated cellular apoptosis and neuronal damage in hippocampal cornu
ammonis 1 region and reduced neurologic deficits. The combination therapy of
niacin and selenium decreased malondialdehyde level, the phosphorylations of
p38 and c-Jun N-terminal kinase/stress activated protein kinase (JNK), and the
cleavage of caspase 3 in brain tissues. However, individual therapy of niacin or
selenium failed to do so. Although no statistical significances were observed, brain
reduced nicotinamide adenine dinucleotide phosphate (NADPH) and reduced
glutathione (GSH) levels were increased in the CPR + NA and CPR + NA + Se
groups. Brain glutathione peroxidase activity was increased in the CPR + Se and
CPR + NA + Se groups. Conclusions: The combination therapy of clinically relevant doses of niacin and selenium activated the glutathione redox cycle, reduced
lipid peroxidation, suppressed the MAPK pathway, attenuated brain injury, and
improved neurological outcome after cardiac arrest in rats.
244
THE NEUROPROTECTIVE EFFECT OF VALPROATE COMBINED WITH HYPOTHERMIA ON ASPHYXIAL CARDIAC
ARREST MODEL
Ji Eun Hwang1, Kyuseok Kim2, You Hwan Jo1, Jae Hyuk Lee3, Joonghee Kim4,
Heajin Chung5, Jungyoup Lee6; 1Seoul National University Bundang Hospital,
Seongnam-si, Gyeonggi-do, South Korea, 2Seoul National University Bun Dang
Hospital, Seong Nam, South Korea, 3Seoul National University Bundang Hospital, Seongnam-Si, Gyeonggi-Do, 4Seoul National University Bundang Hospital,
N/A, 5Seoul National Univ. Bundang Hospital, Seongna-si, Gyeonggi-do, 6N/A,
Sungnam, South Korea
Learning Objectives: Therapeutic hypothermia has been used to protect brain
injury after cardiac arrest. Recently, valproate as a histone deacetylase inhibitor
has been reported to have survival benefit and neuroprotective effect in cardiac
arrest model. This study was designed to investigate the effect of valproate combined with hypothermia on neurological outcome in asphyxial cardiac arrest
model of rats. Methods: 28 Male Sprague-Dawley rats underwent asphyxial cardiac arrest for 6 minutes with subsequent cardiopulmonary resuscitation (CPR).
After ROSC, therapeutic hypothermia (target temperature = 32.5 ± 0.5°C, 4
hours of hypothermia and 2 hours of rewarming) or normothermia (target temperature = 37 ± 0.5°C for 6 hours) was applied and valproate (VPA) 300mg/kg
or normal saline (NS) was administered intraperitoneally. Rats were randomly
allocated into four groups; VPA/HT, NS/HT, VPA/NT, NS/NT. After 6 hours of
temperature management, mechanical ventilation was weaned. Neurological deficit score (NDS) and latency and success rate of tape removal test were measured
every 24 hours after ROSC for 3 days. For histological evaluation, hematoxylin
and eosin staining sections of hippocampal CA1 sector were evaluated blindly
by a pathologist using semiquantitative scale. Kruskal-Wallis test followed by the
Mann-Whitney U-test with Bonferroni correction was performed. Results: All
rats were successfully resuscitated and survived. In the NT-treated group, NDS
was significantly higher in the VPA/NT group than in the NS/NT group (p <
0.05). In the HT-treated group, NDS was also higher in the VPA/HT group than
in the NS/HT group (p <0.05). The latency and success rate was significantly
different only between the VPA/HT and the NS/HT group. Histological injury
score in hippocampal CA1 sector was significantly lower in the VPA/NT group
than in the NS/NT group (p < 0.05) and showed a similar tendency between the
VPA/HT and the NS/HT group (p = 0.06). Conclusions: In asphyxial cardiac
arrest model of rats, administration of valproate improved neurological outcomes
and it added the neuroprotective effect of therapeutic hypothermia.
245
COMPARISON OF SURVIVAL HOSPITAL DISCHARGE
FOR PATIENTS RECEIVING ECPR IN WEEKEND VERSUS
WEEKDAYS
Dae Sang Lee1, Jeong-Am Ryu1, Tae Sun Ha1, chi ryang Chung2, Kyeongman
Jeon1, Chi-Min Park3, Gee Young Suh4, Jeong Hoon yang1; 1Samsung Medical
Center, Seoul, South Korea, 2samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, South Korea, 3N/A, Seoul, South Korea, 4Samsung Medical Center/Sungkyunkwan Univ, Seoul, South Korea
Learning Objectives: Extracorporeal CPR (ECPR) requires urgent decision and high
quality skills, which may not be uniformly available throughout the week. There are
little data on outcomes of patients with cardiac arrest received in-hospital ECPR on
the weekday versus weekend. Methods:Between January 2004 and December 2013,
696 patients were supported by extracorporeal membrane oxygenation (ECMO).
Among them, 200 patients deployed ECMO following in-hospital cardiac arrest was
analyzed retrospectively in this study. We divided patients into the weekdays as 08:00
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
on Monday to 17:59 on Friday and weekdays as 18:00 on Friday through 07:59.
The primary outcome was survival to hospital discharge rate. Results: A total of 135
ECPR cases of in-hospital cardiac arrest occurred during weekdays (including 64 on
day/evening hours and 71 on night hours), and 65 cases occurred during weekends
(including 39 on day/evening hours and 26 on night hours). Rates of survival to
discharge was higher in weekdays compared to weekends (35.8% vs 21.5%, p =
0.041). Cannulation failure was more frequent in weekends group (1.5% vs 7.7%,
p = 0.038). There was more complication rate in weekend comparing weekday; cannulation site bleeding (3.0% vs 10.8%, p=0.041), limb ischemia (5.9% vs 15.6%,
p=0.026) and procedure related infection (0.7% vs 9.2%, p= 0.005). Conclusions:
ECPR on weekends had not only low survival rate but also low resuscitation quality
such as higher cannulation failure and higher complication rate.
246
PATIENT AND PROVIDER CHARACTERISTICS IN TRACHEAL
INTUBATION ASSOCIATED CARDIAC ARREST EVENTS
Yuko Shiima1, Hillary Bogner2, Knashawn Morales3, Vinay Nadkarni4, Robert
Berg4, Akira Nishisaki5; 1The Children’s Hospital of Philadelphia, Philadelphia,
PA, 2Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA,
3
Hospital of the University of Pennsylvania, Philadelphia, PA, 4Children’s Hospital of Philadelphia, Philadelphia, PA, 5The Children’s Hospital Philadelphia,
Philadelphia, PA
Learning Objectives: To determine the occurrence of cardiac arrest (CA), and patient
and intubating provider characteristics associated with CA among patients who require
tracheal intubation (TI) in pediatric ICUs (PICUs). CA during TI will be associated
with the indication for TI of “shock”. TIs with residents (vs. senior providers) as the
initial intubation provider will be associated with CA during TI, after accounting for
patient selection confounders. Methods:Retrospective cohort study with the data
reported to the National Emergency Airway Registry for Children (NEAR4KIDS)
from 7/2010 to 3/2014. CA was defined as CPR >1min. Patient characteristics
include age, gender, indications, and history of difficult airway. Provider characteristics include training level, and discipline. Fisher’s exact test for univariate analysis with
categorical variables, logistic regression for multivariate analysis. P<0.05 as significant.
Results:5,232 TIs were reported from 26 PICUs. Patient age was median 1yr (IQR:
0-6), 57% were males. Median Risk of Mortality (PIM2) was 2.4% (IQR: 0.9-6.7,
n=4,357). The occurrence of CA was 85 (1.6%): CA with ROSC 70(1.3%), CA without ROSC 16(0.3%). A shock state was reported in 586 (11%), and oxygenation
failure in 2,000 (38%) as indications for TI. In univariate analysis, shock status (OR
6.1 95%CI: 3.8-9.7, p<0.0001) and oxygenation failure (OR 4.2 95%CI: 2.6-7.1,
p<0.0001) were associated with CA during TI. Resident provider was associated with
lower CA occurrence (0.2% vs. 1.4%, p=0.005). In multivariate analysis accounting
for patient characteristics likely to confound selection of patient for resident intubation attempt, shock status remained associated with CAs (OR 6.2, 95%CI: 3.9-9.7,
p<0.0001) while oxygenation failure and resident providers were not (p=0.54, p=0.62
respectively). Conclusions: CAs during TIs in PICUs are not rare events. Shock was
independently associated with occurrence of CAs during TI. Residents as intubating
providers were not associated with CAs. Registry data can be used to identify risk factors for CAs upon TIs for the future quality improvement interventions.
247
SEIZURE INCIDENCE IN THERAPEUTIC HYPOTHERMIA
PATIENTS POST CARDIAC ARREST
Ruchi Patel1, Michael Silverstein1, Brian Faley1; 1Hackensack University Medical
Center, Hackensack, NJ
Learning Objectives: Despite the benefit of therapeutic hypothermia (TH) seen in
two landmarks trials, it is not without risks. Recent studies suggest the incidence of
seizures to be as high as 44% in post cardiac arrest patients, and may be associated
with poor functional outcomes. Our study aims to measure the incidence of seizures in
patients undergoing TH and determine its effect on functional outcomes. Methods:
This is a single-center, retrospective analysis of patients treated with TH after ventricular fibrillation or ventricular tachycardia arrest monitored with continuous video EEG
(cvEEG). This study was conducted at a suburban level 2 trauma center from May
2010 to April 2014. Demographics, incidence of electrographic seizures, survival, and
functional neurologic outcome as measured by the Cerebral Performance Categories
(CPC) were recorded. CPC were dichotomized to either 1-3 (recovery of awareness
at discharge) versus 4-5 (vegetative state, brain death, or dead). cvEEG tracings were
independently reviewed by an epileptologist for the presence or absence of seizures.
Each cvEEG file was analyzed to evaluate for nonconvulsvie status epilepticus (NCSE)
as defined in previous studies. Results: Out of the thirty patients that underwent therapeutic hypothermia, twelve patients had cvEEG reports available for review. Mean
age was 59 years, the majority of patients were male (92%), and none of the patients
had a prior history of seizure disorders. NCSE occurred in 25% (3/12) of patients.
Out of the nine patients who did not show cvEEG evidence of NCSE, five received
antiepileptics. Fifty percent of patients survived until hospital discharge with a CPC
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
between 1 and 3. No patients experiencing NCSE survived until hospital discharge.
Conclusions: NCSE is common among TH patients at our institution. Outcomes are
poor in patients experiencing NCSE demonstrated by the 100% mortality rate in our
study. Based on our results, cvEEG monitoring is necessary to assist the clinicians in
prediction of functional outcomes post TH.
248
RESUSCITATIVE ENDOVASCULAR BALLOON OCCLUSION OF
THE AORTA IMPROVES SURVIVAL IN LETHAL HEMORRHAGE
Timothy Park1, Andriy Batchinsky2, William Baker3, Slava Belenkiy4, Bryan Jordan3, Michael Dubick4, Jose Salinas4, Leopoldo Cancio4; 1San Antonio Military
Medical Center, Fort Sam Houston, TX, 2United States Army Institute of Surgical Research, Fort San Houston, TX, 3United States Army Institute of Surgical
Research, Fort Sam Houston,, 4United States Army Institute of Surgical Research,
Fort Sam Houston, TX
Learning Objectives: Resuscitative Endovascular Balloon Occlusion of the Aorta
(REBOA) using generic balloon catheters placed into the descending aorta under
fluoroscopy has been used to treat hemorrhagic shock in animal models. We tested
a new non-image guided 7F ER-REBOA catheter (Pryor Medical Arvada, CO) for
its potential to improve survival in a 100% lethal model of hemorrhagic shock. We
hypothesized that ER-REBOA, placed without fluoroscopic guidance, improves
survival. Methods: Spontaneously breathing, consciously sedated, sexually mature
male Sinclair pigs undergone computerized exponential hemorrhage of 65% of their
blood volume over 1 hour via an arterial line. Animals were then randomized into
groups of 7 animals each including: negative control (NC), no resuscitation; positive
control (PC), immediate transfusion of shed blood (TSB); ER30; 30 min of ERREBOA then TSB; ER60, 60 min of ER-REBOA then TSB; ER, 60 min of ERREBOA with TSB after 30 min of REBOA. After balloon deflation, epinephrine was
given if mean arterial pressure was under 40 mm Hg. Up to 20 min of mechanical
ventilation (FiO2 .21, RR 12, TV 10 ml/kg, ZEEP) was provided if animal suffered
respiratory arrest. Animals were monitored for 240 min post-hemorrhage or until
death. Survival was assessed via Kaplan-Meier analysis. Balloon placement was verified via post-mortem CT scan and at necropsy. Results: ER-REBOA was placed successfully in 100% of cases without fluoroscopy. Survival in the NC and PC groups
was 0 and 71% respectively. Analysis showed significantly higher survival in the
ER-REBOA groups: 100% in ER30 and ER60 groups and 86% in ER (p<0.001).
Epinephrine was given to 4/7 PC animals and to 6/7, 7/7, and 2/7 animals in ER30,
ER60, and ER groups respectively. Ventilation support was given to 1/7, 2/7, and
3/7 in the ER30, ER60, and ER groups and to 2/7 in the PC group respectively.
Conclusions: ER-REBOA is an effective, percutaneous, endovascular life-saving
intervention for the management of cardiovascular collapse in hemorrhagic shock.
249
CODE TEAM TRAINING: IMPROVING TEAM DYNAMICS
AND ADHERENCE TO AHA GUIDELINES
Claire Stewart1, Ken Tegtmeyer1, Jamie Shoemaker2; 1Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, 2Cincinnati Children’s Hospital, Cincinnati, OH
Learning Objectives: In our previous work, we documented the implementation of designated roles for all responding members of the code team. In hopes of
improving this team dynamic as well as further educating each code team member
on their designated role, code team training was instituted in January of 2014.
Using a dedicated team training setting and recording events using a two camera,
integrated set up, we hypothesize that we will enhance our ability to review code
team performance and identify areas for improvement in all code related tasks.
Methods: The sixteen members of the code team meet monthly, both during day
and night shift, at a designated time and bed space. Two scenarios are run with
debriefing after each scenario; this includes not only the details of the resuscitation
but also positioning in the room, communication issues, etc. Each session is videotaped. Videos are then reviewed for adherence to AHA resuscitation guidelines,
specifically, the presence of a team leader and backboard for chest compressions,
ventilation rate of <12 breaths per minute, compression rate between 100-120 per
minute, and a chest compression fraction (CCF) of >80%. Results: Eight sessions
have been completed with attendance for code team members nearing 100%. 145
members of the code team across all disciplines participated. Of the four videos
reviewed, 100% demonstrated a team leader, use of backboard, and CCF >80%.
66% demonstrated a compression rate of 100-120. No teams demonstrated a
ventilation rate of <12 breaths per minute. In all reviewed sessions, site lines were
adequate to monitor these markers of performance. Reviews of historical in situ
mock codes showed poor ability for scoring performance due to obstructed views.
Conclusions: Through video review of regular, monthly code team training, we
will enhance adherence to AHA guidelines and will be able to provide ongoing
targets and measures for improvement processes. Use of video in actual events may
benefit from similar analysis, but multiple challenges exist.
250
EVALUATION OF A THERAPEUTIC HYPOTHERMIA PROTOCOL AT A COMMUNITY HOSPITAL IN ALABAMA
Christen Freeman1, Rebecca Lee1, Fabian Salinas2; 1DCH Regional Medical Center, Tuscaloosa, AL, 2N/A, Tuscaloosa, AL
Learning Objectives: Alabama’s rate of survival to discharge for EMS-treated out
of hospital cardiac arrest (OHCA) has been reported as 3% for all cases and 7.7%
for ventricular fibrillation (VF) cases, well below that of other regions of the US.
Therapeutic hypothermia (TH) has been recommended by the AHA since 2005
for comatose adult patients with return of spontaneous circulation (ROSC) after
cardiac arrest based on improved rates of survival and neurological outcomes. The
purpose of this study was to evaluate the impact of a TH protocol and determine
whether benefits can be obtained in a community hospital that serves several rural
counties in Alabama. Methods: A retrospective, single-center chart review was
conducted to evaluate comatose survivors of cardiac arrest who received TH per
institutional protocol from 2008-2013. TH was accomplished using chilled saline,
ice packs and a surface cooling device. Patients were included regardless of location of arrest (in- vs. out-of-hospital) or initial rhythm. Patients were excluded
if TH was stopped prior to rewarming or if functional status was unable to be
assessed at discharge. The primary endpoint was survival to hospital discharge.
Secondary endpoints were survival and Cerebral Performance Category (CPC) at
6 month post-arrest. Results: Eighty-two patients met inclusion criteria. Median
age was 58 years. Ninety-five percent of all arrests were OHCA, 89% were witnessed arrests and 39% were VF arrests. Average EMS response time was 10.7
minutes. Mean time to ROSC was 23 minutes; TH was initiated in 4 hours or less
in 55% of patients. The rate of survival to hospital discharge was 54%; 43% of
survivors demonstrated a favorable neurological outcome (CPC 1 or 2) at hospital
discharge. Of survivors who were not lost to follow-up (n=37), 67.5% survived 6
months post-arrest and 46% had a favorable neurologic outcome (CPC 1 or 2) at
6 months. Conclusions: Benefits of TH were realized in the community hospital
setting. Implementation of a TH may be one particularly beneficial strategy for
improving outcomes in geographic regions with low rates of survival to discharge.
Poster Session: CPR/Resuscitation 4
251
WHOLE BLOOD TRANSFUSION VIA IO ACCESS DOES NOT
RESULT IN GROSS HEMOLYSIS IN A PRE-CLINICAL STUDY
Tatiana Puga1, Diana Montez1, Chris Davlantes1, Mireya Garcia1, Russell Higgins2, Larry Miller1, Thomas Philbeck3,1; 1Vidacare Corporation, Shavano Park,
TX, 2University of Texas Health Science Center at San Antonio, San Antonio,
TX, 3N/A, Shavano Park, TX
Learning Objectives: Blood product transfusion through the intraosseous (IO)
route provides a promising alternative for patients without IV access; however, the
possibility of hemolysis at clinically beneficial flow rates has not been evaluated. The
purpose of this prospective, pre-clinical pilot study was to evaluate the procedure of
IO blood transfusion for attainable flow rates and changes in laboratory values that
may suggest hemolysis. The hypothesis is that there will be no gross hemolysis resulting from blood transfusion through IO access. Methods: Using standard blood collection bags, 1-2 units of blood were collected from the pre-vena cava of 10 mature
anesthetized swine. The blood was then auto-transfused via the IO route using a
standard blood transfusion set and a pressure bag set to 300 mmHg. Venous blood
samples for the measurement of free hemoglobin were collected pre- and post- transfusion and from the blood transfusion bags. Results: A total of 18 units of blood
were transfused in one unit quantities into 10 swine; 8 received bilateral transfusions. Seventeen transfusions were given through the proximal humerus IO site and
one through the proximal tibia. Mean blood unit volume delivered through each
limb was 266 ± 74 mL (n=18); mean transfusion time was 5.7 ± 3.5 minutes (n=18);
and the mean flow rate was 61.6 ± 37.3 mL/min (n=18). Free hemoglobin results
were obtained from 6 swine. The mean free hemoglobin values were: pre-transfusion
7.05 ± 5.2 mg/dL (n=6); post-transfusion 7.16 ± 3.62 mg/dL (n=6); blood collection
bags 3.81 ± 5.12 mg/dL (n=12); all within the swine reference interval (0–10 mg/dL).
Individually, one swine demonstrated free hemoglobin levels above the upper limit
of the reference interval in all samples (i.e. blood bag, pre-, and post-transfusion)
suggesting hemolysis unrelated to IO transfusion. Conclusions: In conclusion, pressurized blood transfusion through IO vascular access resulted in high flow rates and
did not result in appreciable hemolysis as indicated by free hemoglobin values. Limitations of this study include sample size and use of swine and not humans.
252
NEUROMUSCULAR BLOCKING AGENTS DO NOT IMPACT
TIME TO TARGET TEMPERATURE WITH THERAPEUTIC
HYPOTHERMIA
James Curtis1, Gretchen Zettlemoyer1, Ian Butler1; 1Chester County Hospital,
West Chester, PA
Learning Objectives: When post-cardiac arrest (PCA) patients are treated with
therapeutic hypothermia (TH), shivering is a common occurrence that may lead to
lengthened times to a target temperature (TTT) and increased oxygen consumption. To avoid these potentially detrimental effects, neuromuscular blocking agents
(NMBA) may be utilized. NMBA adverse effects include loss of neurological exam
and increased incidence of myopathy of critical illness. We hypothesized that the
use of NMBA’s does not impact TTT in PCA patients who are treated with TH.
Methods:We conducted a retrospective cohort analysis of all PCA patients admitted
between 2/2011 and 3/2014 and treated with 24 hours of hypothermia (32-34C).
Inclusion criteria was complete data including demographics, comorbidities, type
of arrest, time to target temperature (TTT), and survival at discharge. Patients were
divided into two groups based on the presence or absence of any NMBA use during
the first 24 hours of TH. Results: Twenty six patients met the criteria for our study.
The following did not differ between the neuromuscular blockade group (NMBA, n
=19) and non-neuromuscular blockage group (non-NMBA n = 7): shockable initial
rhythm (NMBA: n = 15 (78.9%) vs non-NMBA: n = 3 (42.8%) p = 0.27, and average age (NMBA, n = 56.5, range 24 to 82 vs non NMBA, n = 56.28, range 29-77,
p = 0.909). The average TTT with NMBA was 198 minutes vs non-NMBA of 120
minutes, p =0.13. The survival at discharge with NMBA was n = 16 (84.2%) versus
non-NMBA n = 3 (42.8%) (Odds ratio 5.33; 95% confidence interval, 0.834 to 34.1,
p = 0.064). Conclusions: Use of a neuromuscular blocking agents in PCA patients
being treated with TH did not appear to effect TTT. There was a trend towards increased
survival in the NMBA group, however this did not reach statistical significance. Our
patient population was similar to prior studies in areas of patient age and comorbidities,
however, our findings were limited due to our small sample size. Further research should
be performed before routine administration of NMBAs can be recommended in TH.
253
THE EFFECTS OF TEMPERATURE VARIABILITY ON THE
OUTCOME OF COMATOSE SURVIVORS AFTER CARDIAC
ARREST
Leda Nobile1, Vito Fontana1, Irene Lamanna2, Katia Donadello3, Antonio
Dell’Anna2, Jean-Louis Vincent4, Federico Pappalardo5, Fabio Silvio Taccone2;
1
Erasme Hospital, Bruxelles, Belgium, 2Erasme Hospital, Brussels, Belgium,
3
N/A, Brussels, Belgium, 4Erasme University Hospital, Brussels, Belgium, 5Instituto San Raffaele, Milano, Italy
Learning Objectives: Clinical studies have shown that spontaneous alterations of
temperature homeostasis after cardiac arrest (CA) were associated with worse outcome. However, none of them considered whether high temperature variability
(TV) during cooling procedures would also influence outcome. Thus, the aim of
this study was to evaluate the determinants of TV after CA and its effects on neurologic recovery. Methods: We reviewed the data of all comatose patients admitted to our Dept of Intensive Care after CA between December 2006 and January
2014 who underwent target temperature management and survived at least 24 h.
We collected demographic data, CA characteristics, ICU survival and neurological outcome at three months (favourable neurological outcome (FNO) = Cerebral
Performance Category 1-2). TV was expressed using the standard deviation (SD)
of all measurements during hypothermia. High TV was arbitrarily defined as a
SD > 1°C. Results: We studied 229 patients, of whom 88 had FNO. Median
temperature on arrival was 35.8 [34.9-36.9]°C, while the median time to hypothermia, defined as body temperature below 34°C, was 3 [4-7] hours. Median
TV was 0.9 [0.6-1.0] °C. In a multivariate logistic regression model, witnessed
CA, VF/VT and previous neurological disease were independent risk factors of
large TV (n=57, 25%). FNO was higher, although not statistically significant,
was more common in patients with high TV than others (27/57 vs. 61/172,
p=0.12). Younger age, bystander CPR, time to ROSC, cardiac origin of arrest,
shockable rhythm, time to target temperature were found to independently predict FNO, while TV was not. Conclusions: Among comatose survivors after
CA, 25% of patients had large TV during the induced hypothermic phase. The
main predictors of high TV were unwitnessed CA, shockable rhythm and previous neurological diseases. The impact of TV on patients’ outcome needs to be
further determined.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
254
INCORPORATION OF POINT OF CARE ULTRASONOGRAPHY INTO ACLS PROTOCOLS
Stephanie Cha1, Aliaksei Pustavoitau2, Erik Su1, Adam Schiavi1, Adam Dodson1,
Allan Gottschalk3; 1Johns Hopkins Hospital, Baltimore, MD, 2Johns Hopkins
University School of Medicine, Baltimore, MD, 3Johns Hopkins, Baltimore, MD
Learning Objectives: The ALCS algorithm revolves around optimization of resuscitative efforts to provide adequate blood flow to the brain and other vital organs
and identifying reversible causes of the arrest. Cardiac-specific causes of Pulseless
Electrical Activity (PEA) arrest include cardiac tamponade, left ventricular failure,
right ventricular failure and hypovolemia. Cadiac ultrasound can identify all these
causes, however, safe incorporation of ultrasound in an ALCS protocol requires
additional training. Methods: Critical care medicine fellows and CME course
participants received 2 hours of instructions and 2.5 hours of hands-on training in critical care cardiac ultrasonography prior to participation in cardiac arrest
simulation. During simulation, groups of 3-5 providers were exposed to 5 adult
PEA arrest scenarios in predefined sequence: hypovolemia, tamponade, myocardial infarction, pulmonary embolism and tension pneumothorax. Each scenario
addressed proper team leadership and coordination during resuscitative efforts
and appropriate use of ultrasound during no-flow intervals (NFI). Duration of
NFI was recorded. Results: 4 groups of fellows and 4 groups of CME participants successfully completed simulated cardiac arrest scenarios. The duration of
NFI was 25.9 seconds (95% CI 22.5-29.4) during the 1st scenario, and significantly lower during scenarios 2-5, the shortest NFI being during scenario 5 - 12.3
seconds (95% CI 4.4-20.2). There were no significant differences in duration of
NFI between scenarios 2-5. There were no differences in duration of NFI between
fellows and CME course participants. Conclusions: Use of ultrasound during
adult PEA cardiac arrest may result in identification of reversible cardiac causes,
however, additional training is required to maintain compliance with minimizing
duration of NFI, thus, maintaining the integrity of life-saving CPR
255
SERUM CYTOCHROME C IS ASSOCIATED WITH OUTCOME
AND CARDIAC DYSFUNCTION AFTER PEDIATRIC CARDIAC
ARREST
Jenny Mendelson1, Hulya Bayir2, Patrick Kochanek3, Ericka Fink2; 1Children’s
Hospital of Pittsburgh of UPMC, Pittsburgh, PA, 2Children’s Hospital of Pittsburgh, Pittsburgh, PA, 3University of Pittsburgh Medical Center, Pittsburgh, PA
Learning Objectives: Pathways leading to cellular and organ dysfunction are
activated after pediatric cardiac arrest (CA). We investigated the role of serum
cytochrome c (cyt c), a mitochondrial protein found in high concentration in
cardiac and brain tissue that is involved in apoptosis, in organ dysfunction after
CA and association with outcome. Methods: Serum cyt c was measured in children post-CA at 2 time points (TP) after CA (TP1 median (interquartile range
[IQR]) 8 [4-12] and TP2 68 [65-72] h. Pediatric Logistic Organ Dysfunction
(PELOD) scores were tabulated on d 1 and 2 after CA and outcome (favorable
= Pediatric Cerebral Performance Category (PCPC) 1-3, unfavorable = PCPC
4-6) and mortality were assessed at 6 mos. First echocardiography (n=16), serum
troponin I (n=24), and serum S100b, an astrocyte biomarker (n=40) results were
recorded if obtained in the first 48 h. Results: Of 40 subjects, 16 (40%) died and
23 (64%) had unfavorable outcome. Serum cyt c was increased in subjects with
unfavorable versus favorable outcome at TP1 (0.99 [0.84-1.29] vs. 0.77 [0.720.90] ng/ml, p=0.01 and TP2 0.86 [0.75-0.94] vs. 0.72 [0.67-0.77], p= 0.006).
Cyt c correlated with PELOD at TP1 and TP2 (ρ=0.35, p=0.27 and ρ=0.39,
p=0.01), and was independently associated only with the cardiac component of
PELOD at TP2 (ρ=0.04, p=0.048). Cyt c was increased in subjects with cardiac
vs. asphyxial etiology (1.21 [0.80-3.29] vs.0.84 [0.72-0.92], p=0.008). Cyt c was
correlated with troponin I and shortening fraction (SF) at TP1 (ρ=0.41, p=0.04
and ρ=-0.60, p=0.01) but not at TP2 (ρ=0.18, p=0.40 and ρ=-0.12, p=0.56);
troponin I and SF were not correlated. Troponin I was also increased in subjects
with cardiac vs. asphyxial etiology (p<0.05) and was associated with mortality
but not outcome whereas SF was not associated with either. Although not associated with the neurological component of PELOD, cyt c was strongly correlated
with S100b (ρ=0.63, p<0.001). Conclusions:Preliminary data suggest increased
serum cyt c parallels evidence of cardiac and neurologic dysfunction and may be
a useful serum marker of outcome after pediatric CA.
256
TARGETED TEMPERATURE MANAGEMENT POST CARDIAC
ARREST:33°C VS 36°C, SHIVERING AND HYPERTHERMIA
CONTROL
David Carlbom1, Melissa Irwin1, Chris Laux1, Natalie Alotis1; 1Harborview Medical Center, Seattle, WA
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Learning Objectives: Cardiac arrest survivors are at high risk for death and neurologic
deficits. A recent randomized trial showed no difference in neurological outcomes
when comatose survivors of cardiac-etiology arrest were cooled to 33°C compared to
36°C. The purpose of this project is to describe initial experience with implementing
targeted temperature management (TTM) and fever control in a busy resuscitation
center. Methods: Adult patients who remained comatose after resuscitation from
cardiac arrest of any etiology were cooled to 36°C for 24 hours using an external
cooling device. If they remained comatose, the temperature was kept <37.5°C for an
additional 48 hours. For shivering control during the first phase we used sedation and
neuromuscular blockade. In the second phase we used a stepwise approach comprised
of counter-warming, acetaminophen, buspirone, clonidine, magnesium and sedation.
Results: Thirty-two patients received TTM therapy over three months. The average
age was 58.9 years old; 84% of the patients were male. 87.5% of the cardiac arrests
occurred out-of-hospital; the presenting rhythm was ventricular fibrillation in 32.3%,
pulseless electrical activity 41.9%, and asystole in 29% of cases. The mean temperature on ED arrival was 35.4°C and on ICU arrival 35.6°C. We observed hyperthermia
and shivering in 68.8% of patients; 62.5% during the 36°C phase and 34.4% in the
<37.5°C phase. Shivering for VF, PEA, and asystole rhythms was 80%, 53.8%, and
77.8% respectively. Overall survival was 31.3%. Survival for VF, PEA, and asystole
rhythms was 50%, 30.8%, and 11.1%. Of the ten survivors, nine had motor GCS
score of six and were following commands. Conclusions: This is the first case series
of 36°C TTM use in comatose survivors of cardiac arrest from any etiology, not just
cardiac-etiology arrests. We observed frequent occurrence of shivering in all presenting rhythms. Despite the frequent rate of shivering, survival was good. Additional
research needs to be performed to assess timing, dose, duration, and method of temperature management survivors of cardiac arrest.
257
THE IMPACT OF VASOPRESSOR SUPPORT ON SURVIVAL IN
PATIENTS UNDERGOING THERAPEUTIC HYPOTHERMIA
James Curtis1, Ian Butler1, Megan Doble1; 1Chester County Hospital, West Chester, PA
Learning Objectives: While the use of vasopressors in the management of shock is
well understood in the critical care setting, there is wide physiologic and pharmacokinetic variability in patients undergoing therapeutic hypothermia (TH). We compared
survival in patients who required vasopressor support during TH to those patients that
did not require vasopressor support. We hypothesized that those who did not require
vasopressor support would have an improved survival rate at discharge. Methods: We
conducted a retrospective cohort analysis of patients who received TH following cardiac arrest between February 2011 and March 2014. Patients were divided into two
groups based on vasopressor use within 24 hours of TH. Vasopressors used included
phenylephrine, norepinephrine, vasopressin, dobutamine, and dopamine. Twenty six
patients were identified with complete data including demographics, comorbidities,
type of arrest, time to target temperature (TTT), and survival at discharge. Results:
Twenty-six patients met the inclusion criteria. Of these subjects, 15 (57.7%) received
at least one vasopressor agent during TH. The following did not differ between the
pressor group (PG, n = 15) and non-pressor group (NPG, n = 11): TTT in minutes
(PG= 172 vs. NPG= 191, p = 0.47),average age (PG= 55.9 years vs. NPG= 55.5
years, p = 0.82, and presence of 2 or more comorbidities (PG, n= 8 (53.3%) vs. NPG,
n= 5 (45.4%), p= 0.69). The presence of a shockable initial rhythm was higher in the
pressor group (PG, n= 13 (86.6%) vs. NPG, n= 5 (45.4%), p= 0.02). Twelve patients
(80%) in the PG survived to discharge versus seven patients (63.6%) in the NPG
(Odds ratio 2.3, 95% confidence interval 0.39 - 13.3; p= 0.35). Conclusions: Survival at discharge in the vasopressor group was 80% compared to 64% in the group
that did not receive vasopressor support. Our sample size was too small to detect a
statistical difference between these two populations, however our data suggests that
vasopressors may not negatively impact survival in PCA patients undergoing TH.
258
SUBLINGUAL MICROCIRCULATION IS RELATED WITH
BULBAR CONJUNCTIVA MICROCIRCULATION IN A RAT
MODEL
Lu Yin1,2, Haifang Yu1, JIE QIAN1, Shen Zhao1, Jiangang Wang1, Xiaobo Wu3,
Jena Cahoon4, Wanchun Tang1; 1Weil Institute of Critical Care Medicine, Rancho Mirage, CA, 2Intensive Care Unit, the Second Hospital of Anhui Medical University, Hefei, China, 3Weil Institue of Critical Care Medicine, Rancho
Mirage, CA, 4the Weil Institute of Critical Care Medicine, Rancho Mirage, CA
Learning Objectives: In previous studies, we demonstrated that the changes
in sublingual microcirculation are closely related to the outcomes of CPR. In
the present study, we investigated the relationship between the sublingual and
bulbar conjunctiva microcirculation in a rat model of cardiac arrest. Methods: A total of five Sprague-Dawley rats (450-550g) were utilized. Ventricular
fibrillation was induced and untreated for 8 mins followed by 8 mins of CPR.
Sublingual and bulbar conjunctiva microcirculatory blood flow was visualized
by the sidestream dark-field imaging device at baseline and 30 mins, 1, 2, 4 and
8 hrs post-resuscitation. Both perfused vessel density (PVD) and microcirculatory flow index (MFI) were recorded. Results: All animals were successfully
resuscitated. The post-resuscitation PVD and MFI decreased significantly in
both sublingual and bulbar conjunctiva sites. Sublingual PVD decreased from
baseline of 5.9 ± 0.3 to 3.3 ± 0.3n/mm at 30 mins post-resuscitation and MFI
from 3.0 ± 0.0 to 1.5 ± 0.3 (both p < 0.05 vs. baseline). Bulbar conjunctiva PVD
was significantly reduced from baseline of 6.7 ± 0.3 to 4.1 ± 0.4 n/mm at 30
mins post-resuscitation and MFI from 3.0 ± 0.0 to 1.3 ± 0.2 (both p < 0.05 vs.
baseline). The decreases in sublingual microcirculatory blood flow were closely
correlated with the reductions of bulbar conjunctiva microcirculatory blood
flow (perfused small vessels density: r = 0.80, p < 0.01; microcirculatory flow
index: r = 0.83, p < 0.01). Conclusions: Sublingual microcirculatory flow is
closely correlated with bulbar conjunctiva microcirculatory flow in a rat model
of cardiac arrest.
Poster Session: CPR/Resuscitation 5
259
COMPARISON OF PERFORMANCE OF AED BETWEEN
TRAINED AND UNTRAINED RESCUERS IN A MANIKIN
STUDY
Zhengfei Yang1, Jiangang Wang1, Xiaobo Wu2, Ziren Tang1, Wanchun Tang1,3;
1
Weil Institute of Critical Care Medicine, Rancho Mirage, CA, 2Weil Institue of
Critical Care Medicine, Rancho Mirage, CA, 3Keck School of Medicine of the
University of Southern California, Los Angeles, CA
Learning Objectives: More widespread use of automated external defibrillators
(AEDs) ensures early defibrillation for ventricular fibrillation (VF) victims. A userfriendly, safe and effective AED is important for untrained bystanders. In this manikin
study, we investigated the performance of the AED between trained professionals and
untrained bystanders. Methods: Thirty-six volunteers from three basic life support
(BLS) training centers authorized by the American Heart Association were recruited.
Half of the volunteers were BLS providers and assigned to the trained group; the other
half were untrained bystanders and assigned to the untrained group. Their performance of the AED in a cardiac arrest simulated scene was recorded by two observers.
After the completion of the test, they were asked to rate the difficulty of usability of
the device from 0 - 10 (0 represents very easy and 10 represents very difficult). Results:
There were no differences in demographics between the trained and untrained groups.
Subjects in both groups successfully and safely completed the defibrillation process.
Mean time to defibrillation was 83 ± 12 secs (95% CI, 78-89 secs) for the untrained
bystanders and 62 ± 9 seconds (95% CI, 59-65 secs) for the trained health providers
(P<.001). The difference in the mean values between the trained and untrained was
21 secs, with a 95% CI of the difference from 14 - 27 secs. Subjective scores in the
difficulty of usability of the device were significantly greater in the untrained group
when compared with those in the trained group (4.3 ± 2.1 vs 2.5 ± 1.1, P=.003). The
correlation coefficient was 0.78 between subjective scores in the difficulty of usability
of the device and the duration of defibrillation (P<.001). Conclusions:Better performance of the AED is achieved by the trained health providers. However, both trained
and untrained groups effectively and safely used the AED by the instructions and the
voice prompt in this manikin study. The absolute differences between the two groups,
however, were small and may be of little clinical relevance.
260
SURVIVAL FOLLOWING AKI IN ADULTS WHO RECEIVED
EXTRACORPOREAL CARDIOPULMONARY RESUSCITATION.
Pramod Guru1, Rahul Kashyap2, Dawit Haile2, Roxann Pike2, Michael Nemergut2,
Devon Aganga2, Kianoush Kashani3, Gregory Schears2; 1Mayo Clinic Department
of Pulmonary & Critical Care, Rochester, MN, 2Mayo Clinic, Rochester, MN,
3
Division of Nephrology and Hypertension, Mayo Clinic, Rochester, MN
Learning Objectives: Extracorporeal Cardiopulmonary Resuscitation (ECPR)
has recently been utilized more frequently in patients with both in and out-ofhospital cardiac arrest, with some reports of favorable outcome. Acute kidney
injury (AKI) is very common (up-to 75%) and associated with poor outcomes
(mortality and resource utilization) in patients receiving extracorporeal therapy.
However the incidence, time of onset, renal replacement therapy requirement
and outcomes with ECPR remains unknown. Here we report the effect of acute
kidney injury on hospital survival for patients who undergo ECPR. Methods:
Retrospective analysis of an IRB approved data registry for adult extracorporeal
membrane oxygenation (ECMO) patients (n=448) from 1/1/2001 to 6/30/2014
is performed. Adult patients >17 years old with cardiac arrest on ECMO were
included. Excluded patients were those who received ECMO for reasons other
than cardiorespiratory arrest. We recorded the patient demographics, types of
ECMO support and survival. AKI is defined by AKIN criteria in the first 72
hours after initiation of ECMO. Results:Out of 65 patients, 34 were included
in the analysis. All received Veno-Arterial ECMO. 19 (56%) were male and the
median (IQR) age was 55 (36-64) years, duration of CPR was done for 28 (1562) minutes, and serum creatinine prior to start of ECMO was 1.1 (0.9-1.4).
Preexisting renal dysfunction found in 7(21%). AKI was diagnosed in 24 (71%)
and 18 (53%) received continuos renal replacement therapy within 24 hour initiation of ECMO. A total of 12 (36%) patients had cardiac arrest following cardiac surgery, 8 (23%) post myocardial infarction, 1 (3%) ARDS, and 13 (38%)
had other. The median (IQR) ECMO time was 76 hours (24-162). 10 (29%)
patients survived 30 days, 14 (41%) withdrew care, 9 (27%) expired in hospital,
and 1 (3%) died after hospital discharge. Patient with AKI vs. without AKI has
no difference in mortality, 7 (70%) vs. 17 (71%); p=1.0. Conclusions: Incidence
of dialysis requiring AKI in ECPR patients is very high. Short term survival is not
associated with renal failure.
261
UTILITY OF LEFT VENTRICULAR EJECTION FRACTION AS
A PREDICTOR OF SURVIVAL AFTER CARDIAC ARREST
Barry Burstein1, Regina Husa1, Dev Jayaraman2; 1Jewish General Hospital, Montreal, Canada, 2N/A, Montreal, QC
Learning Objectives: Cardiopulmonary resuscitation and early defibrillation have
been shown to improve outcomes of cardiac arrest. Despite these interventions,
survival from both in-hospital (IHCA) and out-of-hospital cardiac arrest (OHCA)
remains poor. The significance of the post-arrest echocardiogram, specifically the left
ventricular ejection fraction (LVEF) is unknown. This study aims to determine the
significance of the LVEF on post-cardiac arrest survival. Methods: We performed a
retrospective cohort study of patients who suffered from OHCA or IHCA between
January 1, 2009 and December 31, 2013. We included all patients who achieved
return of spontaneous circulation (ROSC), and were admitted to the Intensive Care
Unit (ICU) or Coronary Care Unit (CCU) of a tertiary care hospital in Montreal,
Canada. Medical charts were reviewed and all patients who underwent echocardiography within 24 hours of cardiac arrest were included for analysis. LVEF was stratified as a dichotomous variable (greater or less than 40%) and the primary outcome
was survival to 30 days post-arrest or hospital discharge. Results: We identified 151
patients who achieved ROSC; 97 underwent post-arrest echocardiogram within 24
hours. 76.2 % were males and the mean age was 63.9 years (SD 15.9). The mean
LVEF at 24 hours was 35.6 (SD: 17.8) and 40.2% had LVEF ≤ 40%. LVEF > 40%
was not predictive of survival to hospital discharge upon univariate analysis (OR:
1.09 (CI95: 0.48-2.44) p=0.84). Multivariate analyses including other significant (α
= 0.05) predictors in the model did not alter this conclusion. Conclusions: Although
echocardiograms are frequently ordered, left ventricular ejection fraction greater than
40% in patients who are resuscitated after a cardiac arrest is not a predictor of survival.
262
MAGNETIC RESONANCE AND ELECTROENCEPHALOGRAPHIC CORRELATES OF MYOCLONUS IN CARDIAC
ARREST SURVIVORS
David Seder1, Kyle Deerwester1, Michael DiGianvittorio1, Brian Livingston1,
Barbara McCrum1, Richard Riker1; 1Maine Medical Center, Portland, ME
Learning Objectives: The classification of myoclonus after cardiac arrest (CA) is
rudimentary; one pragmatic approach defines myoclonus with electroencephalographic (EEG) discharges as “cortical” (C) versus “subcortical” (SC) when EEG
discharges are absent. We sought to compare MRI findings and outcomes in
patients with SC and C subtypes of myoclonus. Methods: A convenience sample
of CA survivors from 2006-2014 with the physical examination finding of myoclonus, treated with targeted temperature management, monitored by continuous
EEG, and with MRI were studied. EEG was interpreted blind to MRI by a certified electroencephalography specialist. MRI was interpreted in terms of “regions
of interest” using DWI, ADC imaging, and FLAIR by a neuroradiologist blind
to EEG findings. Patients were categorized into C or SC based on EEG data.
Data are presented as median (Interquartile Range). Results: 18 patients were
enrolled, with median age of 62 (41-71) years, 72% male, initial rhythm VT or
VF in 28%, time to recovery of spontaneous circulation of 14 (9-26) minutes,
peak neuron specific enolase value of 46 (36-73). Myoclonus was classified C
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
in 15 (83%) and SC in 3 (17%). MRI findings showed cortical injury alone in
50% of C vs 33% of SC (NS), cortical and subcortical in 50% C vs 67% SC,
and subcortical alone or no injury in none. Good outcome was obtained in 0%
C vs 33% SC. Of note, the single patient with SC myoclonus by EEG and good
outcome had multifocal cortical injury on MRI. Conclusions: This pilot study
found that patients after cardiac arrest classified into “cortical” or “subcortical”
types of myoclonus based on EEG data were similar regarding distribution of
MRI abnormalities. Additional research is warranted to explain the variable presentations and outcomes associated with myoclonus after cardiac arrest.
to participate in both baseline and post education sessions for analysis. There
were reduced omissions of critical tasks with CERTAIN (46% to 32%, p <0.01).
The post-test survey indicated that 72% subjects felt better prepared during an
emergency scenario using the CERTAIN model. However, subjects also found
the software somewhat challenging to learn, with only 30% agreeing that the
software was easy to use. Conclusions: The CERTAIN model of care improves
clinicians’ performance when dealing with medical emergencies in high fidelity simulation environment. Improved training and usability enhancements will
facilitate clinical testing and implementation.
263
265
IMPACT OF INDUCED HYPOTHERMIA ON CARDIAC
ARREST SURVIVAL AND ASSOCIATED INITIAL RHYTHM
“TEAM CODE”: COUNTING ON DEBRIEFS: IMPROVING TEAM PERFORMANCE AT AN UNIVERSITY MEDICAL
CENTER
Keri Morgan1, Lisa Hall Zimmerman2, Abby Roetger2, Lesly Jurado2, Claire
Corbett2, Mary Beth Bobek2; 1Charleston Area medical Center, Charleston, WV,
2
New Hanover Regional Medical Center, Wilmington, NC
Renee Hebbeler-Clark1, Ann Schlinkert2, Kimberely Williams2, Barbara Smith2;
1
N/A, N/A, 2University of Cincinnati Medical Center, Cincinnati, OH
Learning Objectives: Neurologic outcomes and morbidity are significantly
impacted in patients who survive out of hospital cardiac arrest (OHCA). Induced
hypothermia (IH) to 32-34C results in decreased neurologic injury secondary
to hypoxia after cardiac arrest with return of spontaneous circulation (ROSC).
However, a recent trial implicates equivocal impact on mortality with IH versus maintaining normothermia after OHCA with ROSC. This study evaluated
survival characteristics after OHCA with ROSC comparing IH versus no IH.
Methods: A retrospective analysis was performed of consecutive OHCA adults
with ROSC from any initial rhythm from 8/2012-5/2014. Neurologic outcomes
were defined using the cerebral performance category (CPC) with a score of 1-2
(good) and 3-5 (poor) neurological function at hospital discharge. Results: Of
175 OHCA patients, mean age was 64 ± 16yrs with initial rhythms of asystole
(34%), PEA (30%), and ventricular tachycardia/v fibrillation (28%). Patients
with left heart catheterization (LHC) <6hrs from event onset survived more
(61% alive v 10% dead, p<0.001) or if IH was initiated for any rhythm (69%alive
v 32%dead, p<0.001). Survival was more likely with shorter time of event to
ROSC (16 ± 9alive v 23 ± 14dead min, p=0.002) and shorter CPR to ROSC time
(13 ± 8alive v 21 ± 12dead min,p<0.001). Death was less likely if CPR to ROSC
< 20 minutes (75%alive v 47%dead, p< 0.001). In-hospital mortality for OHCA
with ROSC was 79%. CPC score of 1-2 occurred in 89% of surviving patients.
IH was more readily performed with STEMI/NSTEMI (40% IH v 16% no
IH, p<0.001). Survival tended to occur with IH when the initial rhythm was
vtach/vfib (39%alive v 26%dead, p=0.14) but tended not to be with asystole/
PEA (52%alive v 67% dead, p=0.14). Conclusions: IH has shown neurologic
outcome benefits in patients who experience OHCA with ROSC. Overall, our
population was more likely to survive with shorter CPR to ROSC times, early
LHC and IH performed. Survival benefit tended to be seen if the initial rhythm
was vtach/vfib. Hence these data prompted a change in initiation of IH for future
OHCA patients at our institution.
Learning Objectives: Breakdowns in team performance and communication are
one of the leading causes of patient harm and medical errors. The use of human
factors training including team training in debriefing with a focus on situational
awareness and critical language have been shown to improve team culture and
awareness in a collaborative effort, thereby improving patient safety. Methods:
The objective was to develop and implement a standardized team debrief tool to
use after a Code Blue occurred at an academic medical center inpatient medicine
service. A quality improvement project that included a multidisciplinary team
using a rapid cycle improvement method including a PDSA (Plan Do Study Act)
approach was conducted August 2013-Feburary 2014. After development, education and pilot testing, the multidisciplinary team debrief was adapted by all
team members. Simulation training was utilized to teach the debrief process to
the code team. Performance was tracked in both simulated cases and real code
blue calls. The performance data collected and reviewed included: team dynamics, communication, collaboration and situational awareness, equipment and
systems issues. Run charts and key driver diagrams were utilized to develop and
follow progress during the development and institution period. Monthly run
charts were utilized to follow the rate of return of team debriefs and the tracking
of safety elements identified. Results: The initial rate of debriefs completed was
35%. At month 3 of the project the rates were at 75% consistently. At the end
of the project rates exceeded 95%. Rates of debriefs were calculated on a weekly
basis. This has sustained during the 6 month follow up period. Conclusions: The
multidisciplinary approach to team debrief following code blue events improved
team perception, attitude and awareness. Spread is key to any quality improvement project and the team has been successful at 2 academic clinical sites. Further
process improvement cycles need to continue to develop in order to show correlation in patient outcomes and improved patient safety.
264
THE VALUE OF AEEG AND RSO2 ASSESSMENT OF POSTCARDIAC ARREST SYNDROME WITH THERAPEUTIC
HYPOTHERMIA
266
PROMPTING WITH ELECTRONIC CHECKLIST IMPROVES
CLINICIAN PERFORMANCE IN MEDICAL EMERGENCIES:
HIGH FIDE
Ronaldo Sevilla Berrios1, John O’Horo2, Christopher Schmickl2, Aysen Erdogan3, XIAOMEI CHEN4, Lisbeth Garcia Arguello2, Yue Dong2, Ognjen Gajic5;
1
Mayo Foundation, Rochester, MN, 2Mayo Clinic, Rochester, MN, 3Department
of Anesthesiology, Mayo Clinic, Rochester, MN, 4N/A, ROCHESTER, MN,
5
Mayo Graduate School of Medicine(Rochester), Rochester, MN
Learning Objectives: The Golden Hour, the time when quick interventions can
determine the course of resuscitation, can be impeded by inefficient processes
of care delivery. Checklists have shown to be an effective tool for standardizing
care models. We developed an electronic tool, Checklist for Early Recognition
and Treatment of Acute Illness (CERTAIN) to prescribe a standard evaluation
and treatment approach for acutely decompensating patients. The checklist was
enforced by use of a “prompter,” a team member separate from the leader who
reviews pertinent CERTAIN algorithms, and verbalizes these to the team. The
CERTAIN model, with use of the tool and prompter, can improve health care
provider performance and satisfaction in the evaluation of acute decompensating
patients in a simulated environment. Methods: Volunteer clinicians with valid
ACLS certification were invited to test the CERTAIN model in a high fidelity
simulation center. The first session was used to establish a baseline in a standard clinical resuscitation scenario. Each subject then underwent online training
before returning for a live didactic lecture, software knowledge assessment, and
practice scenarios. Each subject was then evaluated on a scenario with similar
content to the baseline. All subjects took a satisfaction survey. Video recordings
of the pre-and post-test sessions were evaluated by two blinded reviewers. Disagreements were resolved by discussion. Results: A total of 18 subjects were able
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Shingo Ihara1, Tomohide Komatsu1, Atsushi Sakurai1, Atsunori Sugita1, Junko
Yamaguchi2, Takashi Moriya1, Kosaku Kinoshita3; 1Nihon University School of
Medicine, Tokyo, Japan, 2Nikon University School of Medicine, Tokyo, Japan,
3
Nihon University, School of Medicine, Tokyo, Japan, Japan
Learning Objectives: The pathophysiology of cerebral blood flow and metabolism in post cardiac arrest syndrome (PCAS) treated with therapeutic hypothermia (TH) is still unclear and outcomes cannot be predicted. Assessment of
regional saturation of oxygen (rSO2) and amplitude integrated electroencephalography (aEEG) of PCAS patients may be useful in predicting neurological
outcomes. Methods: We prospectively studied PCAS patients treated with TH
who were monitored by aEEG and rSO2 in the intensive care unit at admission.
Patients were divided into two groups according to EEG; a continuous EEG
(C) group and a non-continuous EEG (NC) group. Neurological outcome was
assessed using the Cerebral Performance Category (CPC) scale at discharge from
the intensive care unit. Good neurologic outcome was defined as a CPC score of
1 or 2. Results: A total of 27 patients treated with therapeutic hypothermia were
included in the study. Measurements were taken at 5 ± 3.0 h (mean ± standard
deviation) after return of spontaneous circulation. The C group (6/8: favorable/
unfavorable: 75%) had a significantly (p = 0.002) more favorable neurological
outcome than the NC group (2/19: 10.5%). There were no significant differences
in rSO2 values between the C and NC groups (55.2 ± 7.0% vs 57.2 ± 18.3%, p =
0.691). Most of the rSO2 values of the C group were lower than normal. Conclusions: In PCAS patients treated with TH, initial continuous EEG may be useful
in predicting a favorable neurological outcome. In such patients, initial rSO2
tended to be lower than normal indicating that cerebral oxygen metabolism may
have recovered more than cerebral blood flow.
267
I-FABP IS AN INTESTINAL INJURY MARKER IN SIRS FOLLOWING CARDIAC ARRESTS
Kentaro Shimizu1, Hiroshi Ogura2, Hiroyuki Funaoka3, Jotaro Tachino4, Takeshi
Shimazu5; 1Osaka University Graduate School of Medicine, Suita, Osaka, Japan,
2
Osaka University Graduate School of Medicine, SUITA, OSAKA, Japan, 3DS
Pharma Biomedical Co., Ltd., Osaka, Japan, 4Osaka University Graduate School
of Medicine, Suita,Osaka, Japan, 5Osaka university graduate school of medicine,
suita,Osaka, Japan
Learning Objectives: Reperfusion after cardiac arrest has been reported to cause
systemic inflammatory responses such as proinflammatory cytokine production and endothelial injury. However, there is few specific marker for intestinal injury in the clinical setting. Intestinal fatty acid-binding protein (I-FABP)
is a cytosolic protein, abundant in the mucosa of the small bowel. It has been
used as an intestinal specific marker such as necrotizing enterocolitis, ulcerative
colitis and small bowel diseases. In this study, we evaluated I-FABP in patients
following cardiac arrest. Methods: We retrospectively included systemic inflammatory response syndrome (SIRS) patients who were measured I-FABP during
their stay in the ICU. We compared out-of hospital cardiac arrests patients who
were resuscitated at the hospital (Group A) and other SIRS patients (Group B).
We compared the value of serum I-FABP after admission. Results: Twenty-one
SIRS patients were included in this study. APACHE II scores on admission were
33.6 ± 15.3 in Group A and 12.0 ± 15.3 in Group B. In Group A, the initial
rhythm of cardiac arrest was VF/VT in 4 patients. The time from collapse to
return of spontaneous circulation was 56.3 ± 11.1min. pH on arrival was 7.0 ± 0.1
and blood lactate was 129 ± 29.3mg/dL (mean±SD). Serum I-FABP in Group
A was significantly increased higher than that in Group B (214.9 ± 246.8 vs.
3.0 ± 3.7; normal 1.1 ± 0.9 (ng/ml)). Conclusions: I-FABP showed higher values
after intestinal reperfusion injury following cardiac arrest. It could be a direct
marker of intestinal injuries in these patients.
Poster Session: CPR/Resuscitation 6
268
ASSOCIATION OF BODY MASS INDEX WITH TIME TO TARGET TEMPERATURE IN THERAPEUTIC HYPOTHERMIA
PATIENTS
James Curtis1, Rick Terkowski1, Ian Butler1; 1Chester County Hospital, West
Chester, PA
Learning Objectives: Body Mass Index (BMI) may influence the time to
target temperature (TTT) in post-cardiac arrest (PCA) patients undergoing
therapeutic hypothermia (TH) possibly impacting the neurological outcomes
of patients. We hypothesize that a BMI >30 is associated with an increase
in TTT. Methods: We conducted a retrospective analysis of collected data
on all PCA patients admitted between February 2011 and March 2014 and
treated with 24 hours of hypothermia (32-34°C). Patients with complete data
including demographics, comorbidities, type of arrest, time to target temperature (TTT) in minutes, and survival at discharge were included. Patients were
divided into two groups defined a priori based on their BMI score >30 and
BMI <30. TTT was defined as the time in minutes from initiation of The to
reaching target temperature of 34°C. Results: Twenty-four patients met the
inclusion criteria for study. Of these subjects, 7 (29.2%) were obese. The following did not differ between the obese group (n = 7) and non-obese group
(n = 17): average age in the obese (62.3 years, range 43 to 77) vs. non-obese
(54.9 years, range 24 to 82, p = 0.12); presence of 2 or more comorbidities in
the obese (n = 4, 57.1%) vs. non-obese (n = 5, 45.4%, p = 0.69), and presence
of a shockable initial rhythm in the obese (n = 5, 71.4%) vs. the non-obese
group (n =12, 70.6%), p = 0.97). Average TTT in the obese group was 197
minutes vs. 168 minutes in the non-obese group (p = 0.47). Four patients
(57.1%) in the obese group survived to discharge compared to 15 patients
(88.2%) in the non-obese group (Odds ratio 5.6, 95% confidence interval:
0.69 to 46, p = 0.09). Conclusions: Among a small number of comatose
PCA patients treated with TH, obese patients with a BMI of >30 had a tendency to have a prolonged time to target temperature when compared to nonobese patients, though this did not meet statistical significance. Obese patients
trended towards decreased survival at discharge when compared to non-obese
patients. Further research is needed to draw more significant conclusions as
our study is limited due to small sample size.
269
THE USE OF ULTRASOUND GUIDANCE FOR EMERGENCY
INTUBATIONS IN THE ICU.
Rohan Arya1, David Gerber1; 1Cooper Medical School of Rowan University,
Cooper University Hospital, Camden, NJ
Learning Objectives: In intensive care units patients are frequently emergently
intubated for various reasons. Many critically ill patients are often unstable
and, although confirmatory procedures are employed to ensure that endotracheal tubes are placed in the trachea (auscultation of bilateral breath sounds
and end-tidal capnography), chest roenterograms are often necessary to confirm
placement. Having another modality that can confirm correct endotracheal
placement in real time would enhance patient safety. The use of ultrasound as
a diagnostic tool has quickly become a mainstay in rapid evaluation of patients
and arguably is pushing to replace older and more invasive interventions.
Methods: Our study is a prospective study that included any patient admitted
to the Cooper University Hospital ICU, requiring emergent intubation at any
point during their ICU stay. It was approved by the Cooper University Hospital
IRB. Our ICU is a multidisciplinary ICU where fellows from various backgrounds (Internal Medicine, Emergency Medicine and combined Internal and
Emergency Medicine) are completing their critical care training. Results: To
date, the ultrasound (US) procedure has been used on 23 patients who required
emergent intubation. In all 23 procedures, US accurately (100%) determined
placement of the ETT in either the trachea or the esophagus. After tracheal
intubation, the findings were confirmed using standard post-intubation protocol. In 12 cases, the intubating fellow was able to visualize the vocal cords.
The remaining 11 cases had partial views of the glottic opening. Conclusions:
Ultrasound is able to correctly determine whether the ETT has been placed in
either the esophagus or the trachea. The US maneuver did not interfere with
the intubation process. Placement of the endotracheal tube is confirmed if the
intubating physician (in this case, the critical care fellow) visualizes the tube
passing through the vocal cords. The use of US in emergent intubations would
be most valuable in situations where the vocal cords are not visualized during
the intubation process.
270
ROLE-BASED RESUSCITATION AND INTERDISCIPLINARY
CODE BLUE TEAM TRAINING
Sheryl Greco1, Kimberly Jackson1, Patricia Kritek2, Keri Nasenbeny3, Stephanie
Shushan1, Brian Ross1; 1University of Washington Medical Center, Seattle, WA,
2
N/A, Seattle, WA, 3Univesity of Washington Medical Center, Seattle, WA
Learning Objectives: Code Blue (CB) team efficiency and effectiveness can be
improved through a role-based resuscitation response supported by multidisciplinary team training. Such large scale system changes require interdisciplinary
champions and senior administrative support. Methods: A multidisciplinary
group from two affiliated academic medical centers reviewed best practices
for resuscitation teams and developed a CB team response with an integrated
training curriculum. Team communication and role-based resuscitation were
emphasized. Responsibilities of CB responders were established with set
positions for each team member at the resuscitation. Two roles were added
to optimize team performance through greater situational awareness (Operations RN) and additional support of the code team leader (Supervising MD).
Interdisciplinary work was crucial in effecting system changes. Senior physicians, nurse leaders and department managers worked together to design and
implement the restructure. Direct care clinical staff and ancillary support staff
were involved in designing and providing the educational curriculum. Members of the restructured CB team participated in videotaped multidisciplinary
mock code exercises in a high-fidelity simulation lab. Computer based learning
modules highlighted the new CB team response structure and in-situ mock
codes allowed periodic practice of learned roles. Results: Electronic surveys
were distributed to members of the restructured CB team to obtain feedback
on the new model. Out of 103 respondents, 78% felt that communication
was clear during the code. The majority (85%) of code team leaders felt supported in their role and 95% felt they worked well with the nurse team leader.
Team members expressed increased comfort with established roles and defined
responsibilities and felt their voices were heard. Conclusions: Designated Code
Blue team roles and responsibilities, supported by multidisciplinary team training exercises, can create an organized and less stressful approach to resuscitation
efforts. Large scale system changes are best accomplished by interdisciplinary
collaboration.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
271
273
IMPACT OF CARDIO PULMONARY RESUSCITATION(CPR)
ON OUTCOMES IN ADULT STEM CELL TRANSPLANT
RECIPIENTS
BALANCED RESUSCITATION IN POST-OPERATIONAL
PATIENTS AFTER DIGESTIVE SURGERY IN ICU
Veerajalandhar Allareddy1, Sankeerth Rampa2, Ashima Das3, Romesh Nalliah4,
Veerasathpurush Allareddy5, David Speicher1, Alexandre Rotta1; 1Rainbow
Babies & Children’s Hospital, Cleveland, OH, 2University of Nebraska Medical University, College of Public Health, Omaha, NE, 3Rainbow Babies &
Children’s Hospital, CASE University, Cleveland, OH, 4Dental Medicine,
Harvard University, Boston, MA, 5College of Dentistry, University of Iowa,
Iowa City, IA
Learning Objectives: National estimates of CPR and associated outcomes in
hospitalized stem cell transplant(SCT) recipients are unclear. We conducted
this study to evaluate the impact of CPR on hospital charges (HC), length of
stay (LOS), and in-hospital mortality(IHM) in adults undergoing SCT and to
examine patient-level factors associated with having CPR. We hypothesized
that use of CPR is associated with poor outcomes and that a mix of patient
level factors is associated with risk of having a CPR. Methods: The Nationwide
Inpatient Sample for the years 2004 to 2010 was used to select all patients >18
years who had SCT procedures. Performance of CPR in this cohort was identified and its impact on HC and LOS examined by multivariable linear regression analyses. For IHM, multivariable logistic regression was used. The effects
of confounding factors such as age, sex, race, insurance status, type of SCT,
type of admission, co-morbid burden, hospital teaching status, and hospital
region were adjusted. A heterogeneous mix of patient related factors on the
odds of having CPR was computed by using multivariable logistic regression
analysis. Results: 85,772 patients had SCT. The mean age was 50.7 yrs and
59% were males. CPR was performed in 0.3% of patients. Outcomes(wCPR
vs woCPR)include: median charges ($264,104 vs $191,471), median LOS
days(21.1 vs 20.3), respectively. CPR was associated with significantly higher
HC(23.5% higher, p=0.01). LOS was not significantly associated with CPR
following adjustment of confounders. IHM(wCPR vs woCPR) was 78.2%
vs 4.3%.(wCPR: OR=112, 95% CI=35-361, p<0.0001, ref woCPR). Blacks
(OR=2.39, 95% CI=1.06-5.40, p=0.04, reference whites), increase in comorbid burden(OR=1.42, 95% CI=1.24-1.62, p<0.0001), and those who
developed septicemia (OR=2.95, 95% CI=1.51-5.78, p<0.0001) or pneumonia (OR=3.27, 95% CI=1.69-6.33, p<0.0001) were associated with significantly higher odds for having CPR. Conclusions: In this large cohort of SCT
recipients nearly 1 in 330 had CPR. The associated mortality and hospital
resource utilization is significant. Certain predictors of risk of having CPR
are identified.
272
INCREASED SURVIVAL IN SMOKERS TREATED WITH
THERAPEUTIC HYPOTHERMIA FOLLOWING CARDIAC
ARREST.
Amanda Radisic1, James Curtis1, Ian Butler1; 1The Chester County Hospital,
West Chester, PA
Learning Objectives: Recent research links a history of smoking to an increase
in survival for post-cardiac arrest (PCA) patient populations treated with therapeutic hypothermia (TH). This has been hypothesized to be due to periods of
hypoxia induced in the body through the act of smoking: the “smoker’s paradox”. We hypothesized that a history of smoking would be associated with
increased rates of survival at discharge in PCA patients treated with TH in our
hospital. Methods:We conducted a retrospective analysis of data collected on all
PCA patients admitted between 2/2011 and 3/2014 and treated with 24 hours
of induced hypothermia (33C). We identified 26 patients with complete data
including demographics, comorbidities, type of arrest, time to target temperature (TTT), survival at discharge and at 3 and 6 months. Patients were divided
into two groups defined a priori based on a history or absence of history of
smoking. Results: The following did not differ between the smoking group (SG,
n = 10) and non-smoking group (NSG n = 16): initial rhythm (shockable SG:
n = 6 (60%) vs shockable NSG: n = 12 (75%), p = 0.57), and TTT in minutes
(162 vs 184, p = 0.65). Average age in the SG was lower (50.3 years, (range 24
to 82) than the NSG (61.8 years (41 to 78) (p = 0.1)). Both the SG and the
NSG had approximately the same presence of 2 or more comorbidities (n = 5
(50%) vs n = 9 (56%), p = 0.1). Eight patients (80%) in the SG survived to discharge versus ten patients (62.5%) in the NSG (Odds ratio 2.4, 95% confidence
interval 0.38-15.3; p = 0.25). These numbers were not significantly changed
at 3 or 6 month follow-up. Conclusions: Among a small number of comatose
PCA patients treated with TH, a presence of smoking history was associated
with trends to higher rates of survival, though this did not meet statistical significance. Our patient population was similar to prior studies in areas of patient
age and comorbidities, however, our findings were statistically limited due to
our small sample size.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
R. Gutierrez-Rodriguez1, P. Martinez-Lopez2, I Macias-Guarasa1, R. Rivera-Fernandez1; 1Hospital Regional Carlos Haya, Malaga, Spain, 2Hospital Virgen De La
Victoria, Malaga, Spain
Learning Objectives: study the changes in resuscitation and initial handling of fluids after emergency digestive surgery and its link to observed mortality. Methods:
Retrospective, descriptive comparative study of ICU patients after emergency digestive surgery between 2009 and 2010, and 2010 and 2011. variables: demographics,
associated co-morbidity according to Charlson Index, gravity according to scores,
APACHEII and SOFA. Evaluation of fluid therapy administered during the first 24
hours of the post-operative period, both to cover base needs and as part of a balanced
resuscitation (alternation between saline solution, isosmolar substances, plasmalyte,
ringers is permited) and non-balanced (where an exclusive resuscitation is performed
with a single type of serum such as saline at 0.9%, colloids or simply blood products).
Significance rated at P < 0.05. X2 for qualitative variables and T-student for quantitative variables. Results: we studied 150 patients after emergency digestive surgery,
Mean age was 59 ± 16, scores, SOFA 2.4 ± 3.1, APACHE II 20.4 ± 7.3 y Charlson
index 1.2 ± 2.5. Mean ml serum in the first 24 hours. In the univariable analysis, not
receiving a balanced resuscitation, 27% showed no significant link to a greater production of metabolic acidity, coagulopathy or a greater positive balance of fluids. Significant differences were observed P < 0.05 in patients who presented a non-balanced
resuscitation, and the p[ercentage of multiple transfusions in the first 48 hours, 69%,
vs 39%. There was a greater incidence of renal dysfunction according to RIFLE, 57%
vs 52.2%. Equally those patients who were resuscitated with colloids 15%, presented
a greater incidence of nosocomial infections, 54.5% vs 30%, P< 0001, and multiple
transfusions during surgery 36.4% vs 30%. Resuscitation with blood products, 9%,
presented 97.7% highly positive balance, P < 0.05, and multiple transfusions in the
first 48 hours, 50% vs 12%. Conclusions: this study suggests that complications
caused by a poor management of fluids following emergency digestive surgery were
linked more with the type of fluids than with the ml received.
274
COMPARISON BETWEEN TWO METHODS OF TARGETED
TEMPERATURE MANAGEMENT IN PATIENTS WITH CARDIAC ARREST
Brett Lindgren1, Uyen Hoang1, Mohamed Abou El Fadl2; 1Mercy Catholic Medical Center, N/A, 2N/A, N/A
Learning Objectives: Targeted temperature management (TTM) has been used
more frequently in treatment of patients with cardiac arrest over the last decade.
The purpose of this study is to investigate the effects of two methods of inducing mild hypothermia on patients with out-of-hospital cardiac arrest to evaluate if
intravascular cooling is superior to external cooling. Methods:Retrospective chart
review of patients with cardiac arrest admitted to two inner city community teaching hospitals between May 2012 and December 2013. Patients who underwent
TTM were included and divided into 2 groups. Those who underwent external
cooling were included in Group I and Intravascular cooling in Group II. Both ICUs
were managed by the same group of intensivists and followed the same protocols.
Results: 41 patients were included in this study: 18 in Group I (External method)
and 23 in group II (Intravascular method). Mean±SD age was similar (65 ± 12 vs
62 ± 12 years, groups I and II respectively, P=0.52). Group I had significantly higher
severity of illness (APACHE II 35 ± 4.8 vs 31.2 ± 5.9, SOFA 13.5 ± 2.4 vs 11.4 ± 2.2,
for groups I and II respectively, P<0.05 for both). There was no difference on incidence of Vfib, PEA and asystole (22% vs 30%, 56% vs 57%, 11% vs 13%, groups
I and II respectively, P=NS). Both groups had comparable requirements of paralytics and sedatives (44% vs 39%, 89% vs 96 %, group I and group II respectively,
P=0.7 for both). Vasopressor use and incidence of seizures was higher in group I,
however did not reach statistical significance due to sample size (67% vs 35%, 44%
vs 21% P=0.06). ICU LOS and Hospital LOS (significant) was shorter for group
I (5.28 ± 5.3 vs 9.05 ± 10.7 and 5.28 ± 5.3 vs 11.8 ± 12, respectively P=0.18 and
P=0.04). Survival to hospital discharge was significantly lower in group I (22% vs
60%, P=0.01). Conclusions: The intravascular group had a trend of more favorable
outcomes. The shorter LOS and lower survival rate in the external group could be
possibly explained by the higher severity of illness. More studies with larger sample
sizes are needed to detect a significant difference in clinical outcomes.
275
PREDICTION FOR NEED OF VASOPRESSORS BY VITALS
AND PHYSICAL EXAMINATION FINDINGS IN EARLY SHOCK
Lucie Kukralova1,2, Lisbeth Garcia Arguello1, Ognjen Gajic1, Rahul Kashyap1;
1
Mayo Clinic, Rochester, MN, 2Charles University in Prague, Faculty of Medicine in Hradec Kralove, Hradec Kralove, Czech Republic
Learning Objectives: A need of vasopressors in shock patients is an indication of
worsening condition. Evaluation of basic vitals and physical examination findings
may predict vasopressor use in next 24 hours. Methods: In a subset analysis of a
prospective observational study all adult patients admitted to emergency department
of a tertiary care hospital were screened. The inclusion criteria were systolic blood
pressure (SBP) <90 or a drop ≥40 mm Hg from baseline, shock index >1 or lactate
>3 mmol/L without evidence of underlying liver disease. Selected patients underwent
physical examination which included evaluation of skin temperature, presence of skin
mottling, strength of peripheral pulses, capillary refill time, presence of rales, cardiac
gallop (S3 sound), and jugular venous distension (JVD). Heart rate (HR), respiratory rate (RR) and oral temperature were recorded. We excluded patients who were
already intubated, received vasopressor or inotropic medications, or had congenital
heart disease. Vasopressors administration requirement in next 24 hours was assessed
by electronic medical record review. Results: Total 120 patients were observed prospectively. The median (IQR) age was 69 (58-80) years. Sixty five (54%) of them were
men. Thirty three (27%) patients required vasopressors within 24 hours of physical
examination. The median (IQR) mean arterial pressure (MAP) was found to be lower
in patients requiring vasopressors vs. those who did not.; 58 (53-71) vs. 66 (58-74),
p=0.04. The HR, RR and temperature were no different. There was no difference in
pulse quality between patients requiring vasopressors vs. not, weak pulse in 9 (27%)
vs. 38 (44%), p=0.14; neither in skin temperature, 9 (27%) vs. 33 (38%), p=0.3;
nor capillary refill time, delayed in 19 (58%) vs. 49 (56%), p=1.0. Presence of rales,
skin mottling, S3 sound and JVD had very few incidences, found unfit for meaningful analysis. Conclusions: In a sample of prospectively enrolled early shock patients,
lower MAP predicted the need for vasopressors use in next 24 hours. No other early
physical examination findings were found to be predictive.
276
DEVELOPMENT OF A CARDIOPULMONARY RESUSCITATION NON-TECHNICAL SKILLS SCORING TOOL (CPR-NTS)
Kareen Jones1, Michael Rosen2, Jordan Duval-Arnould2, Elizabeth Hunt3;
1
Johns Hopkins Hospital, Baltimore, MD, 2Johns Hopkins University School
of Medicine, Baltimore, MD, 3John Hopkins University School of Medicine,
Baltimore, MD
Learning Objectives: In-hospital CPR is a team exercise with many factors
influencing quality, performance, and outcome. Limited data exist characterizing whether associations may exist between non-technical skill (NTS)
use and team performance during CPR. We hypothesized:1)team performance during simulated in-hospital cardiac arrests (IHCA) could be stratified into categories of high and low performance based on American Heart
Association (AHA) quality measures and 2)well executed NTS would be
associated with CPR performance category. Our goal is to build and validate
a CPR-NTS scoring tool that can be used to evaluate teams during both
simulated and actual IHCA. Methods: 120 medical students, grouped in
2-person teams, took part in a video-recorded simulated ventricular fibrillation IHCA. Non-student participants played other team-member roles,
assisting with the resuscitation as directed by the students. 60 sessions were
reviewed to measure: chest compression (CC) start and stop times, chest
compression fraction (CCF), time to defibrillation, and use of NTS. Performance was stratified according to AHA CPR quality standards and associations between NTS and CPR performance was explored. Results: No
team met the AHA criteria of a CCF>80%, thus “High Performers” were
identified as those starting CC≤10 sec, defibrillating≤180 sec, and a CCF
of >70%. 20% of teams met “High Performers” criteria. “Low Performers”
were defined as the teams who did not start CC≤10 sec, and/or defibrillate≤180 sec, and had a low CCF. Examples of NTS that were more frequently seen in the High vs Low Performers include:action-linked phrases
use and coaching quality of CC. NTS were divided into existing teamwork
categories. A preliminary CPR-NTS scoring tool was built from this data.
Conclusions: Next steps are to evaluate performance of the CPR-NTS scoring tool on a new cohort to assess whether higher scores on the tool are
consistently associated with improved CPR performance. Ultimately, our
goal is for the CPR-NTS scoring tool to be incorporated into CPR educational programs to help improve CPR performance in simulated and
actual IHCAs.
Poster Session: CPR/Resuscitation 7
277
INTRAVASCULAR GAS OF POST CPR MAY ASSOCIATE WITH
HYPERCAPNIA DURING CHEST COMPRESSION.
Tsunehiro Matsubara1, Mitsuo Ohnishi2, Hiroshi Ogura3, Takeshi Shimazu4, Jotaro
Tachino5; 1Osaka University Graduate School of Medicine, Suita, Japan, 2Osaka
University, Suita, Osaka, Japan, 3Osaka University Graduate School of Medicine,
SUITA, OSAKA, Japan, 4Osaka university graduate school of medicine, suita,Osaka,
Japan, 5Osaka University Graduate School of Medicine, Suita,Osaka, Japan
Learning Objectives: It is important to understand changes caused by cardiopulmonary resuscitation. Findings of post cardiac arrest CT (PCACT) images are not
known very well. Particulary, PCACT findings which may associated with resuscitation were intracardiac gas (ICG) and intrahepatic gas (IHG). These gases may have
harmful effects for resuscitation. The aim of this study was to determine the factor
that affects ICG and/or IHG detected by PCACT images. Methods: The data were
collected from medical records of the patients more than 17 years old with nontraumatic cardiopulmonary arrest who were admitted to our hospital between April 2012
and July 2014. The incidences of the gas detected by PCACT were analyzed with
the factors of age, gender, presence of witnesses, presence of bystanders, use of automatic cardiopulmonary resuscitation device, number of peripheral and central venous
catheters, duration of CPR and blood gas on admission. Results: One hundred sixty
one patients were included in this study (mean age 73.3, 64.5% men). Return of
spontaneous circulation occurs in 102 patients. In the rest of 59 patients, 17 (28.8%)
patients had ICG and 15 (25.4%) had IHG. PaCO2 in patients with ICG and IHG
were 101.9 mmHg and 104.7 mmHg respectively. These were significantly higher
than patients without ICG (70.5 mmHg) or IHG (71.0 mmHg). There were no difference between the patients with and without ICG or IHG in age, gender and duration of CPR. Conclusions:Intravascular gas detected by PCACT might be associated
with hypercapnia during chest compression. Intravascular gas might deteriorate the
possibility of return of spontaneous circulation since the gas would become embolus.
278
THE STATE OF CARDIOPULMONARY ARREST WITH SEVERE
HYPOTHERMIA
Hidenori Mitani1, Sachiko Ohde1, Shinichi Ishimatsu1, Toshiaki Mochizuki1,
Hiroyuki Tanaka1; 1St.Luke’s International Hospital, Tokyo, Japan
Learning Objectives: It is difficult to judge whether hypothermia is the cause
of cardiopulmonary arrest(CPA) or the result. We researched the factors concerned with return of spontaneous circulation(ROSC) of CPA with severe
hypothermia. Methods: We conducted a retrospective case-control study of
patients treated in our hospital from April 2007 to March 2014, who received
advanced life support(ALS) and tried to rewarm following out-of-hospital cardiac
arrest(OHCA) with severe hypothermia under 30°C. We compared patients who
achieved ROSC with those who did not. The clinical values measured included
witness, bystander cardiopulmonary resuscitation(CPR), first arrest rhythm, deep
body temperature, and blood gas analysis(PaO2,PaCO2,potassium and lactate).
The analysis was conducted with χ2 tests and Mann-Whitney U tests. Results:
In total, 15 patients were evaluated in this study; 7 patients achieved ROSC, and
8 patients did not. The deep body temperature of patients achieved ROSC was
higher than those who did not.(27.9°C vs 23.8°C, p<0.05). The other factors
did not have significant differences. Conclusions: We confirmed that lower deep
body temperature made vital prognosis worse. We could not find that blood gas
analysis was useful to estimate prognosis. More patients and further studies are
needed to determine the prognostic factors.
279
SHIVERING IN CARDIAC ARREST PATIENTS UNDERGOING THERAPEUTIC HYPOTHERMIA IS ASSOCIATED WITH
SURVIVAL
Dena Rocchio1, Ian Butler1, James Curtis1; 1Chester County Hospital, West
Chester, PA
Learning Objectives: Shivering has been associated with improved neurologic
outcomes in post-cardiac arrest (PCA) patients undergoing therapeutic hypothermia (TH). We hypothesized that increased episodes of shivering in PCA
patients undergoing TH at our hospital would be associated with increased rates
of survival at discharge. Methods: We conducted a retrospective analysis of all
PCA patients admitted between 2/2011 and 3/2014 and treated with 24 hours of
hypothermia (32-34C). We identified 27 patients with complete data including
demographics, comorbidities, type of arrest, time to target temperature (TTT),
and survival at discharge. Patients were given a score (0-24) based on a presence
of shivering as assessed on an hourly basis. Patients were divided into two groups
defined as those who were above or below the median score. Results: The median
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
shivering score was 5.5 and patients were placed grouped into two groups: shivering group (above 5.5) or non-shivering group (below 5.5). The following did not
differ between the shivering group (SG, n =14) and non-shivering group (NSG
n=13): shockable versus non-shockable (n =10 (71.4%) vs n =8 (61.5%), p =
0.89); age (57.2 vs 55.7, p = 0.99), or presence of 2 or more comorbidities (n =
7 (50%) vs n = 7 (53.8%), p = 0.84). Notably, there was a difference in TTT in
minutes (248 vs 100, p = 0.0006), with the shivering group taking on average
over 2 hours longer to reach goal temperature. Twelve patients (85.7%) in the SG
survived to discharge versus 7 patients (53.8%) in the NSG (Odds ratio 5.14;
95% confidence interval, 0.81 to 32.77, p =0.07). Conclusions: Among a small
number of comatose PCA patients treated with TH, increased rates of shivering
were associated with trends to higher rates of survival, though this did not meet
statistical significance. Our patient population was similar to prior studies in areas
of patient age and comorbidities, however, our findings were limited due to our
small sample size.
280
EXTERNAL VERSUS INTERNAL COOLING FOR THERAPEUTIC HYPOTHERMIA: DOES THE METHOD MATTER?
Harminder Sikand1, Jordan Lee2; 1N/A, San Diego, CA, 2USC, Los Angeles, CA
Learning Objectives: In the US approximately 300,00 out of hospital cardiac
arrests occur each year with a survival rate of 6-12%. Neurologic injury is the
most common cause of death in patients with out of hospital cardiac arrests.
Neurologic recovery is < than 50% of admitted patients. Published literature at
the time of the study showed good neurologic recovery if the brain temperature
is 32-34 °C during the first few hours after cardiac arrest. Advanced cardiac life
support protocols recommend the use of therapeutic hypothermia (TH). The
method of cooling, external vs internal thus far in the literature does not show
superiority. This study aims to investigate in a Level 1 and Level 2 Trauma center if two separate methods of cooling make a difference in patient outcomes.
Methods: Concurrent and retrospective observational analysis across three hospitals in a 4-health system was conducted. Patients were included if the were >
18 years, had non-traumatic cardiac arrest, persistent coma after ROSC, ability
to maintain SBP > 90 or MAP > irrespective of fluid or vasopressor support.
Time to initiation of TH has to be < 6 hours from ROSC and core temperate
at presentation > 34 °C. Patients were excluded if intravenous fluids, vasopressors, transfusion therapy, inotropic therapy and antibiotics were given prior to
initiation of TH. Patients were also excluded if on paralytics or sedatives prior to
start of TH. Results: Analysis included 70 patients across 3 hospitals using either
invasive or non-invasive techniques or both at one hospital. The patient population was largerly male (70%). Out of hospital cardiac arrest occurred in 90% of
the patients, with 37% asystole, 21% PEA and 35% VF arrest. Interventional
procedure was done 30% of the time with 60% use of vasopressors. Overall 76%
achieved goal temperature and ROSC irrespective to TH method used. There was
no difference in length of stay, ICU, ventilator days and mortality between hospitals. Conclusions: Internal versus external cooling methodology in our analysis
in 70 patient across the system did not significantly change patient outcome.
281
MONITORING OF CIRCULATING WATER TEMPERATURE CAN DETECT FEVER DURING THERAPEUTIC
HYPOTHERMIA
Jin-Heon Jeong1, Jun Young Chang2, Jeong-Ho Hong3, Moon-Ku Han1; 1Department of Neurology, Seoul National University Bundang Hospital, Seongnam,
South Korea, 2Department of Neurology, Seoul National University Bundang
Hospital, Seong Nam, South Korea, 3Department of Neurology, Dongsan Medical Center, Daegu, South Korea
Learning Objectives: Therapeutic hypothermia (TH) is increasingly used as a
treatment of cerebral edema in neurocritical care unit. Infection is frequent complication during hypothermia, and the prevention and management of infection
is challenging. The masking of fever prevent detecting infection, and physician
don’t know about optimized timing of blood cultures. We retrospectively assessed
infective complications and evaluated the effect of monitoring of circulating
water temperature. Methods: We identified all patients treated with TH from
March 2011 to May 2014. We collected demographic data, evidence of infection, and the results of blood cultures. During TH, we daily measured complete
blood cell counts and C-reactive protein, and obtained blood culture samples
according to laboratory tests. Since March 2013, we monitored the temperature
of circulating water in the cooling device, and blood culture samples were collected at or around time of circulating water temperature decline. Results: A total
39 patients were included, and 22 patients monitored circulating water temperature. 27 patients (69.2%) presented infectious complications, and pneumonia
was the most frequent infectious complications (23 episodes, 59%). Urinary tract
infection, phlebitis, central line-associated bloodstream infection, clostridium
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
difficile associated disease, and acute cholecystitis occurred to one patient of each.
After monitoring of circulating water temperature, the blood culture positive rate
was increased (0% vs 13.6%), but there was no statistically significant difference
(p=0.243). Conclusions: Patient treated with TH is commonly complicated by
infections, and accurate diagnosis of infection is difficult during hypothermia.
We show that the monitoring of circulating water temperature in the cooling
device can detect fever during hypothermia and increase positive rates for blood
cultures.
282
ANTI-SHIVERING MEDICATION REQUIREMENTS IN THERAPEUTIC NORMOTHERMIA: SURFACE VS. ENDOVASCULAR
COOLING
Andrew Kirk1, Cara McDaniel2, Dorota Szarlej3, Fred Rincon2; 1N/A, Philadelphia, PA, 2Thomas Jefferson University Hospital, Philadelphia, PA, 3Jefferson
Hospital for Neuroscience, Philadelphia, PA
Learning Objectives: Shivering during targeted temperature management
(TTM) should be minimized because it can cause cerebral and metabolic stress.
It has been proposed that patients treated with surface cooling (SC) may experience more shivering compared to those treated with endovascular cooling (EC)
methods. The purpose of this study was to compare the anti-shivering medication
requirements and degree of shivering between these two groups. Methods: This
was a retrospective cohort study of patients treated with TTM to therapeutic
normothermia (TN) via SC or EC methods. The number of interventions and
daily dose of anti-shivering medications required per patient-day was compared
between the two groups. The degree and intensity of shivering was assessed with
the Bedside Shivering Assessment Scale (BSAS). Results: A total of 66 patients
were included in the study. Patients in the EC group (n=23) required more antishivering interventions per patient-day than those in the SC group (n=43) (3.28
vs. 2.66, p=0.0018). The EC group was treated with acetaminophen (81% vs.
59%, p=0.0002), buspirone (75% vs. 53%, p=0.0005), and magnesium infusions (52% vs. 36%, p=0.0122) on more patient-days than those in the SC group.
Patients treated with SC required more patient-days of propofol (35% vs. 19%,
p=0.0062) and higher average dexmedetomidine dosing per patient-day (0.70 vs.
0.56 mcg/kg/hour, p=0.0302). Dosing of other medications was similar between
the two groups. There were no observed differences in the degree or intensity of
shivering. Conclusions: In our cohort, patients treated with EC required more
anti-shivering interventions but less sedation during TN than patients in the SC
group. An anti-shivering protocol using non-sedating medications, such as acetaminophen, buspirone, and magnesium infusions, may decrease the requirement
for sedatives to control shivering. Our findings require further study.
283
VECTOR AUTO-REGRESSIVE (VAR) MODEL FOR EXPLORING
CAUSAL DYNAMICS OF CARDIORESPIRATORY INSTABILITY
Eliezer Bose1, Marilyn Hravnak2, Gilles Clermont3; 1University of Pittsburgh
School of Nursing, Pittsburgh, PA, 2University of Pittsburgh, Pittsburgh, PA,
3
University of Pittsburgh Medical Center, Pittsburgh, PA
Learning Objectives: Patients undergo continuous physiologic monitoring of
vital signs (heart rate [HR], respiratory rate [RR], pulse oximetry [SpO2]). Vital
signs undergo inter-related changes in situations of stress, and upon recovery
from stress. Patterns of this cross-talk could portend impending cardiorespiratory
instability (CRI). We proposed using VAR modeling and Granger causality to
explore causal dynamics across the vital signs time-series (VSTS) in patients prior
to overt CRI. We hypothesize that patient-specific VAR modeling of VSTS will
expose Granger causal dynamics in evolving CRI. Such information could help
target surveillance monitoring. Methods: CRI was defined as vital signs beyond
normality thresholds (HR=40-140/min, RR=8-36/min, SpO2>85%) and persisting for 4-mins of a 5-min moving window. A 6-hr window prior to first CRI
onset was chosen in 25 CRI patients. The uniform time series (freq=1/20 Hz)
for each vital was assessed for stationarity, followed by: VAR model construction
and diagnostics such as significant lags, LM test for residual autocorrelation, AR
roots and Wald test. With the final stable model, Granger causality/block exogeneity Wald chi-square test assessed for significance of the lagged variable on the
dependent variable. Results: The primary cause of CRI was SpO2 (48% cases),
followed by RR (28%) and HR (24%). Within CRI cases, Granger causality
revealed that HR Granger-caused (GC) RR (28%) (i.e. HR changed before RR
changed) more often than RR GC HR (13%). Similarly, HR GC SpO2 (20%)
was more common than SpO2 GC HR (15%). For RR and SPO2, RR GC SPO2
(17%) was more common than SpO2 GC RR (6%). Conclusions: VAR modeling indicates that, within this sample, HR changes seem to occur before those in
RR. It is unclear if this means that HR is causative, or if HR is a more nimble
vital sign and able to attempt compensation in response to subtle abnormalities
in RR or SpO2 before overt CRI. Nevertheless, our data suggests that contextual
assessment of HR changes as the earliest sign of CRI is warranted. More rigorous
testing of causal dynamics in a larger sample is needed.
284
DONOR TISSUE OXYGEN SATURATION CORRELATES WITH
THE NUMBER OF ORGANS TRANSPLANTED PER DONOR
Silvia Perez-Protto1, J. Hata1, Jing You1, Samir Latifi2,3, James Reynolds4, Daniel Lebovitz2,3; 1Cleveland Clinic, Cleveland, OH, 2Akron Children’s Hospital,
Akron, OH, 3Lifebanc, Cleveland, OH, 4University Hospitals, Cleveland, OH
Learning Objectives: The goal of targeted donor management is to increase the
number of organs transplanted per donor (OTPD). Current donor management
is based on macro-hemodynamic changes, which have limited effects on organ
perfusion. Near-infrared spectroscopy (NIRS) allows monitoring of tissue oxygen
saturation (StO2) as a surrogate of organ perfusion. This study sought to determine
baseline StO2 in deceased by neurological criteria (DNC) organ donors and to
determine if there is an association between StO2 during the donor management
phase and the OTPD. Hypothesis: StO2 in the DNC donor during donor management is predictive of the number of OTPD. Methods: Lifebanc Medical Advisory
Board approval. Enrollment criteria: DNC, ≥ 15 years of age, and ≥ 45 Kg body
weight. StO2 was measured using an InSpectra NIRS monitor (Hutchinson, MN).
The association between the StO2 time-weighted average (TWA), with the number
of OTPD and the difference between actual and predicted number of OTPD was
evaluated using multivariable linear regression. Fourteen pre-specified potential confounders were included in the model via backward selection procedure. Pearson correlations between StO2 TWA and macro-hemodynamic parameters were estimated.
Results: Between April 2013 and March 2014, 60 DNC donors were enrolled. During management phase, the median initial and terminal StO2 were 84.5% [Q1, Q3:
78%, 89.5%] and 92% [87%, 93.5%]. Average StO2 TWA was 87.5% ± 5.2%
and average OTPD was 3.5 ± 2. Higher StO2 TWA during the donor management
phase was associated with an increase in OTPD: a 5% rise in the StO2 TWA yielded
an estimated increase of 0.47 OTPD (P=0.004; 95% CI, 0.16, 0.78). Higher StO2
TWA was associated with 0.33 more OTPD than predicted (0.01, 0.65) for a 5%
increase in StO2 TWA (P=0.046). None of the macro-hemodynamic measurements
was significantly correlated with StO2. Conclusions: Higher StO2 during donor
management was associated with an increased number of OTPD. Agents that target
the microvasculature to improve tissue perfusion may have clinic impact on OTPD.
StO2 goal directed donor management merits further investigation.
285
OUTCOMES ASSOCIATED WITH CPR IN STEM CELL TRANSPLANT RECIPIENT CHILDREN IN USA
Ashima Das1, Sankeerth Rampa2, Romesh Nalliah3, Veerasathpurush Allareddy4,
David Speicher5, Alexandre Rotta5, Veerajalandhar Allareddy5; 1Rainbow Babies
& Children’s Hospital, CASE University, Cleveland, OH, 2University of Nebraska
Medical University, College of Public Health, Omaha, NE, 3Dental Medicine,
Harvard University, Boston, MA, 4College of Dentistry, University of Iowa, Iowa
City, IA, 5Rainbow Babies & Children’s Hospital, Cleveland, OH
Learning Objectives: Single center studies have shown that the need for cardiopulmonary resuscitation (CPR) in hospitalized stem cell transplant (SCT)
recipient children is associated with extremely high mortality rates. Advances
in medical care, technology and CPR programs are thought to have improved
outcomes. Current national estimates and outcomes of CPR in hospitalized
SCT recipient children are unknown. We conducted this study to describe the
prevalence of CPR in hospitalized SCT recipient children, and examine the
impact of CPR on hospital outcomes. Methods: In this retrospective study,
all children aged < 17 years who had SCT procedures were selected from the
Nationwide Inpatient Sample for the years 2004-2010. Performance of CPR in
this cohort was identified and its impact on hospital charges(HC) and length
of stay (LOS) was examined by multivariable linear regression analyses. In hospital mortality rates were calculated. The effects of confounding factors such
as age, sex, race, insurance status, type of SCT, type of admission, co-morbid burden, hospital teaching status, and hospital region were adjusted. The
effects of clustering of outcomes within hospitals was adjusted in the regression models. Results: A total of 15,661 children had SCT, including infants
(13.6%), toddlers (17.9%), pre-school (12.9%), school age (25.3%), early
adolescents (16.7%), and middle adolescents (13.5%). About 58% were males.
CPR was performed in 0.4% of patients. Outcomes (with CPR vs without
CPR) included: median charges($604,977 vs $302,016), median LOS(55.5d
vs 30.6d). After adjustment for confounders in the regression models, those
who had CPR were associated with significantly higher HC(81.3% higher,
p=0.003) and LOS(43.5% higher, p=0.03). In hospital mortality rate(wCPR vs
woCPR) was 84.6% vs 5%. Conclusions: In this large cohort of hospitalized
SCT recipients the overall prevalence of CPR was low. There appears to be an
acceptable survival rate among those who received CPR. Future research should
focus on morbidity and quality of life in the survival group especially given the
high hospital resource utilization.
Poster Session: Education 1
286
IMPACT OF INTERPROFESSIONAL COLLABORATION ON
DELIRIUM SCREENING AND TREATMENT IN A PICU
Shari Simone1, Allison Lardieri2, Sarah Edwards3, L. Kyle Walker1, Sean Pustilnik3, Susan dosReis2; 1University of Maryland Pediatric Intensive Care Unit,
Baltimore, MD, 2University of Maryland School of Pharmacy, Baltimore, MD,
3
University of Maryland School of Medicine, Baltimore, MD
Learning Objectives: Delirium is a neuropsychiatric syndrome associated with
cognitive impairment and psychiatric symptoms, and if left untreated can result
in significant morbidity and mortality. Despite increasing evidence that delirium
presents in children, it often goes undetected, in large part, because staff is not
knowledgeable of the signs, symptoms, or screening tools. To address this important clinical issue, we examined the impact of an interprofessional collaboration
(IPC) to improve detection of pediatric delirium. We hypothesized that implementation of an IPC clinical practice protocol would enhance systematic screening, detection and increase delirium treatment. Methods: Pediatric, pharmacy,
nursing, and child psychiatry professionals developed a clinical practice protocol
for assessment, prevention, diagnosis and treatment of delirium in December
2013. Assessment included pain, sedation and delirium using the Cornell Assessment of Pediatric Delirium (CAP-D) tool. If CAP-D scores were elevated and
symptoms were consistent with delirium, the protocol called for identification
of potential causes of delirium. If delirium persisted despite initial treatment to
address potential causes, non-pharmacological treatments were initiated followed
by pharmacological antipsychotic treatment. In addition, monthly case conferences were held to discuss delirium cases and enhance staff delirium knowledge.
Screening and treatment practices were analyzed 6-months following the intervention. Results: In 2012-2013, the PICU did not screen for delirium and only
4 cases were identified in a retrospective review. Six months following protocol
implementation, 559 patients were screened and 120 (21.5%) delirium cases
identified. Ten patients (aged 6 months-17 years) received pharmacological treatment. All patients were intubated, 6 with primary respiratory, 2 cardiovascular,
and 2 oncologic disease. Conclusions: An IPC approach to pediatric delirium
which combines a clinical practice protocol with education and monthly case
conferences is effective in increasing the rates of delirium screening, detection
and treatment.
287
HIGH-FIDELITY SIMULATION RESOLVES KNOWN AND
UNKNOWN MILESTONE GAPS IN SURGICAL CRITICAL
CARE
Matthew Moorman1, Tony Capizzani1; 1Cleveland Clinic, Cleveland, OH
Learning Objectives: Simulation based training (SBT) has become universal in residency and is costly. No validated curricula for surgical critical care
exists. Local competency gaps should drive training goals. Unlike traditional
paradigms, SBT can address known gaps and identify unanticipated weaknesses in learners. Pre-identified and emergent milestone deficiencies can be
eliminated with high-fidelity SBT. Methods: SimMan 3G (Laerdal Medical)
was used for simulation. Initial needs assessment targeted trauma resuscitation. Expected data capture included: identification of shock physiology,
resuscitation products used, volume delivered, use of endpoints of resuscitation, knowledge of massive transfusion protocols. Training applied deliberate
practice methodology over one academic year, replacing experience-based with
competency-based training. Learner feedback was given after each scenario,
4-5 times per year. Performance was trended for improvement and retention.
Faculty inter-rater variability was analyzed. Results: Unexpected gaps seen
during initial training included: airway assessment and adjuncts, recognition
of tension pneumothorax (tPTX), and prompt decompression of tPTX. Airway management was appropriate by only 10% of residents in initial training. Second exposure resulted in improvement. Junior residents (PGY2,3)
showed subsequent decay (10% to 40% then 19%). Senior residents (PGY4,5)
retained skills (10% to 60% then 55%). These same trends were seen with
tPTX and shock resuscitation. Volume resuscitation skills showed similar patterns of initial performance-improvement-decay: 13%-29%-15% PGY2,3
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
and 33%-68%-55% PGY4,5. Conclusions: SBT improves surgical resident
competency in trauma and critical care. Training curricula can be modified
based on emergence of unanticipated milestone gaps seen in early training.
Planned and emerging gaps can be successfully eliminated. PGY2,3 residents
show improvement but dramatic decay in skills over time. PGY4,5 residents
improve and retain. This should affect training schedules and intervals. SBT is
a cost-effective use of resources warranting continued investigation.
288
HIGH-FIDELITY SIMULATION IMPROVES RESIDENT
LEARNING FOR THE PECARN HEAD TRAUMA RULE
Ilana Harwayne-Gidansky1, Kevin Ching2, Kristen Critelli2, Jennifer Garnett2,
Son Mclaren2; 1New York Presbyterian Hospital - Weill Cornell Medical College,
New York, NY, 2New York Presbyterian Hospital, New York, NY
Learning Objectives: Procedural skills acquired through simulation training
have been shown to transfer into clinical practice. Evidence for the transfer of medical decision-making skills is more limited. Pediatric residents are
expected to learn and utilize a clinical prediction rule derived and validated
by PECARN (Pediatric Emergency Care Applied Research Network) to
determine whether children with head trauma need neuroimaging to identify a traumatic brain injury (TBI). We predicted that interns participating
in a high-fidelity simulation exercise illustrating the use of this PECARN
rule would utilize this rule more correctly when applying it to real children
in our pediatric emergency department (PED), than residents who did not
participate in this simulation. Our primary outcome was the correct identification and utilization of the PECARN rule criteria. Methods: Single center, blinded, prospective randomized-controlled pilot trial implemented for
one year. All interns completed a written pretest and were randomized to
participate in a PECARN head trauma simulation or an unrelated simulation control of acute intracranial hypertension. For the next 12 months, any
utilization of this rule by interns or senior residents in the PED was compared using a structured observation tool. Results: Interns were similar in
demographics, prior experiences, and general knowledge of TBI. Interns in
the PECARN simulation group were able to correctly identify a median of
71% of the PECARN criteria, as compared with senior residents (57%), and
interns in the control group simulation (43%) (p=0.011). Conclusions: Our
preliminary proof of concept data suggests that interns participating in simulation training may demonstrate clinical performance competencies involving
the use of the PECARN clinical prediction rule that are measurably similar
to more experienced senior level residents. This study suggests that we may
improve the efficiency of information delivery through simulation, and has
promising implications for future larger studies.
289
EFFICACY OF A STREAMLINED EDUCATION PROGRAM
FOR NURSING TRANSITION INTO CRITICAL CARE AREAS
Ron Della Valle1, Maresa Glass1; 1Tampa General Hospital, Tampa, FL
Learning Objectives: The Critical Care Transition Course (CCTC) is designed
to prepare the registered nurse to assume the role of a critical care nurse at
Tampa General Hospital, a large acute care, tertiary, teaching facility. This
course is a combination of multidiscipline instructor led lectures, skill workshops and modules developed by the American Association of Critical Care
Nurses. Historically, the course was 12 weeks in duration and included discussion on advanced critical care topics. This course was streamlined to only 9
weeks in duration and focuses on topics that a novice critical care nurse would
likely be exposed to. The number of patient case studies was increased, and
an electrocardiography (ECG) and an advanced cardiac life support (ACLS)
module was added. The purpose of this review is to evaluate the effectiveness of
this streamlined course in preparing nurses to work in the critical care setting.
The streamlined CCTC 9 week course is as effective at preparing nurses to work
in the critical care setting as the original 12 week course. Methods: Retrospective comparison of exam results from the Basic Knowledge Assessment Tool
(BKAT-8) for Adult Critical Care Nursing in both original and streamlined
CCTC course groups. Students in each group were evaluated on knowledge
through the BKAT-8 that was administered upon completion of the course.
Results: A total of 155 nurses completed the original (12 week) CCTC from
January 2011-April 2012. A total of 150 nurses completed the streamlined (9
week)CCTC from Feb 2013-Feb 2014. The mean posttest score of the students
completing the original 12 week course was 84.21+/-5.9. The mean posttest
score increased significantly to 87.80+/-4.5 for the students in the streamlined
9 week course (P < 0.05). Conclusions: The streamlined CCTC course resulted
in a significant improvement in standardized test scores compared to the original course. This improvement in scores was seen despite a reduction in total
course duration from 12 to 9 weeks.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
290
ASSESSING KNOWLEDGE AND CONFIDENCE OF THE NURSE
PRACTITIONER AND PHYSICIAN ASSISTANT RESIDENT
Heather Meissen1, David Carpenter2, Rob Grabenkort1, Timothy Buchman3,
Craig Coopersmith4; 1N/A, Atlanta, GA, 2EUH, Atlanta, GA, 3Emory University
Hospital, Atlanta, GA, 4Emory University School of Medicine, Atlanta, GA
Learning Objectives: As Nurse Practitioners(NP) and Physician Assistants(PA)
increase in the intensive care unit(ICU) workforce, residencies have grown to give
new providers the skills needed to practice in the ICU. Despite this, there has been
limited data on changes in knowledge, confidence or orientation time from these
residencies. Methods: We designed an NP/PA residency program based on Society
of Critical Care Medicine (SCCM) and European Society of Intensive Care Medicine competencies as well as internally developed competencies. Over 30 months a
total of 20 residents have matriculated. 10 residents graduated and were included in
this study. Initially residents were evaluated using SCCM Residency Intensive Care
Unit (RICU) pre and post tests. Due to a lack of up to date testing material, we
transitioned to a self developed pre and post test. A Likert scale assessment (1-10)
was added measuring confidence in procedures, cardiovascular and pulmonary conditions as well as overall confidence. 6 months after graduation, a survey was completed by the graduate’s employer. The survey was used to compare orientation time
of the resident-trained to the last 6 non-resident trained hires in the Emory Critical
Care Center (ECCC). Results: Of 10 residents, 4 residents completed RICU, 2
residents completed the ECCC test, and 4 residents completed both. Residents
who completed the RICU had a mean pretest score 62% and a mean posttest score
79% (p<0.0007). Residents completing the ECCC test had a mean pretest score
65% and a mean posttest score 86% (p=0.03). 5 residents completed the confidence assessment. Overall, residents had a mean pre-training confidence level of 5.1
and a mean post-training confidence level of 8 (difference 2.9 p=0.013). For procedures the difference was 3.4 (p=0.011) the cardiac difference was 3.1 (p=0.012)
the respiratory difference was 2.1 (p=0.072). Comparing non-residency trained and
residency trained NPs and PAs, the orientation was 5.8 months vs 1.4 months (p=
0.036). Conclusions: A residency program for NPs and PAs produces proficient
and confident bedside providers who need minimal orientation.
291
EFFECT OF VIDEO LARYNGOSCOPY WITH SUPERVISOR
FEEDBACK ON TRAINEE INTUBATION EDUCATION
Julia Noether1, Adam Dodson1, Paul Phrampus2, Joseph Carcillo3, Erik Su1;
1
Johns Hopkins Hospital, Baltimore, MD, 2University of Pittsburgh Medical
Center, Pittsburgh, PA, 3Children’s Hospital of Pittsburgh, Pittsburgh, PA
Learning Objectives: Airway protection is vital during resuscitation of critically ill
children and adequate intubation practice for pediatric trainees in older children is
episodic in the ICU. Video laryngoscopy (VL) with supervisor feedback is a promising
contemporary technology that could improve education. This study evaluates success
rate, time to intubation, and educational experience of trainees with direct laryngoscopy (DL) vs. VL in supervised simulation. We hypothesize VL, even when only visible to a supervisor, improves intubation success rate and educational experience and
decreases time to intubation. Methods: The Johns Hopkins University IRB approved
this study. PGY 1-3 pediatric residents intubated a difficult airway simulation device
in easy and difficulty airway modes with each laryngoscope under supervision. Only
the supervisor was allowed to see the VL screen (C-MAC, Karl Storz, Tuttlingen).
Time to successful intubation, accuracy of vocal cord identification, and endotracheal
tube placement were recorded. Participants were surveyed on intubation experience
and education during the airway scenarios. Results:Enrollment in this study is currently ongoing, with twelve residents completing evaluation to date (6 PGY-1). Time
to intubation was 21 ± 3 (s) with DL vs. 38 ± 10 with VL (mean±SEM, p=0.13) in the
easy airway, and 40 ± 15 with DL vs. 41 ± 10 with VL (p=0.97) in the difficult airway.
Time differences were not statistically significant. 10 of 12 residents preferred VL; of
the two remaining residents, one preferred DL and the other preferred DL for the
easy airway but VL for the difficult airway. More supervisor feedback events occurred
during VL (12) than DL (0). Reported advantages of VL included confirmation of
anatomy (4 residents, 33%) and confirmation of tube passage through the vocal cords
by supervisor (4 residents, 33%). Conclusions: VL provided a more positive teaching
experience for pediatric trainees than DL; benefits included confirmation of anatomy
and tube passage through vocal cords. Further investigation is warranted regarding
educational outcomes in this approach.
292
CAN YOU INTUBATE BETTER THAN A 5TH GRADER: THE
VALUE OF VIDEO LARYNGOSCOPY IN MED STUDENT
TEACHING
Dave Milzman1, daisy choi2, Alex Kherdi3, sara rao4, Anthony Napoli5, Patti
Pang6; 1N/A, Washington, DC, 2Georgetown U School of Medicine, washington,
DC, 3Georgetown U School Of Medicine, Wash, DC, 4georgetown U School of
Medicine, washington, DC, 5N/A, N/A,6Georgetown U Schoool of Medicine/
Cornell Anesthesia Residency, NY, NY
Learning Objectives: During training med students may receive introductory
experience with advanced resuscitation skills. ETI (endotrach intubation) is
important advanced skill that many students never attempt. Recent studies on
Video Laryngoscopy (VL) have demonstrated improvements in both the safety
and success of intubation in the ED and ICU. Prior studies on both physician
and medical student endotracheal intubation (ETI) have not compared multilevel success of VL in simulation studies. Methods: 3 groups with differing
experience in intubation were selected, one group of of non medical students
aged 10-18 (5th Grd) were compared to first year medical students(1stMed) and
intubation experienced EM and anesthesia residents (EMA Rez). A 20 min brief
teaching on-line course was devised and made available to all study participants.
Exclusion criteria included any person in the 5th Grd or 1 Med who had prior
intubation attempts and EMA rez who did not have 25 successful ETI. metrics
included 8 critical actions for ETI and mean time (best of 3 attempts) for successful manikin ETI placement. Power analysis found 32 subjects were need in each
group and 1 SD was 22 sec difference. Results: 88 subjects completed study: 20
5th grad, 50 1Med and 18 EMA Rez. for knowing critical actions EMA Rez had a
mean score of 98% (SD 7%) compared to 85.% (SD 11%) for 5thGrd and 90%
(SD 8.5%) for 1 Med: EMA Rez VS non MD was P < 0.02. Time for successful
placement of ETT with VL was not different for meas between the three groups
with single best time of 3 tries actually showed marked improvement for the inexperienced groups: EMA rez 21(SD 10 sec) 1 Med 27 sec (SD 15) and 5thgrad
29 sec (SD 14). Conclusions: By using VL, the actual skill of ETI can be learned
by nearly anyone. Certainly, sim success does not guarantee clinical success in
actual patients but it is an important start and better than no useful experience.
The ease and simple understanding of VL makes it an important step in taking
the mystery out of ETI.
294
IMPLEMENTATION AND EXPANSION OF AN ONLINE CRITICAL CARE PHARMACY JOURNAL CLUB
Aimee LeClaire1, April Quidley2, Jorie Frasiolas3, Karen Berger3, Lance Oyen4;
1
N/A, Gainesville, FL, 2Vidant Medial Center, Greenville, NC, 3N/A, N/A,
4
Mayo Clinic, Rochester, MN
Learning Objectives: Members of the Society of Critical Care Medicine Clinical
Pharmacy and Pharmacology (SCCM CPP) Section implemented a teleconference journal club to provide an audience with opportunities for networking and
learning. Evolving interest and methods over 7 years has resulted in a SCCM supported, web-based platform. Methods: In 2007, a critical care pharmacy journal
club was conducted by a few pharmacists as a quarterly teleconference in a limited
geographic area. Participation was facilitated through personal networks and word
of mouth. Since 2009, the CPP Education Committee has coordinated a monthly,
web-based critical care pharmacy journal club without geographic bounds. Presenters and moderators volunteer following an annual solicitation for participants. Articles are selected by the presenters and approved by journal club charge leadership.
The journal club is promoted monthly through announcements by SCCM. E-mail
announcements are made at least 1 week prior to the scheduled journal club and
include citations of articles to be presented as well as instructions for pre-registration
through SCCM. In July 2014, e-mail promotion was extended to all SCCM members. Results: Presenter participation has increased 480% from 5 to 24 speakers
with 24 timely articles discussed annually. All speakers are residents in a critical care
pharmacy residency program from 24 unique programs. The audience has grown
from 4 institutions participating in the teleconferences to an average of 61 unique
registrants per month for the 2013-2014 residency year. Expansion of the journal
club to all SCCM members resulted in an increase to 80 attendees. Conclusions: A
critical care pharmacy journal club has expanded from regional roots and engaged
a boundless audience using an online platform. The journal club program has seen
steady growth with primary benefits of networking and education across disciplines.
293
EVALUATION OF KEY WORDS CITED IN CRITICAL CARE
MEDICINE PUBLICATIONS
Nao Umei1, Benjamin Berg2, Shingo Ichiba3, Atsuyoshi Iida4, Yoshihito Ujike5;
1
Okayama University, Osaka, Japan, 2N/A, Honolulu, HI, 3Okayama University,
okayama, Japan, 4N/A, Okayama, Japan, 5Okayama University, Okayama, Japan
Learning Objectives: Key Words are essential tools for bibliographic research.
Key Words enable authors to extend the representation of manuscript content
beyond that presented in the title and abstract. Key Words impact the retrievability process that can contribute to the frequency with which a publication will be
cited. In our previous study, we found that it was not possible to retrieve publications related to patient simulation if authors did not choose appropriate strategies to incorporate Key Words in manuscript text. The objective of this study
is to evaluate the use of key words in articles of the Critical Care Medicine, to
determine if characteristics of published Key Words impact retrievability. Methods: Feature articles published in Critical Care Medicine from 2013 to 2014
were reviewed manually to identify Key Words. The key words used by authors
were compared to the medical subject heading (MeSH) terms as defined in the
MeSH website, 2014 version. In addition, we studied whether PubMed searches
using the key word specified by authors yielded the article. Results: Fifty feature
articles published in the study period used a total of 258 key words. According
to the MeSH database, the total of MeSH consistent key words was 148 (57%)
and MeSH inconsistent key words was 63 (24%). Examples of MeSH inconsistent key words include the following:antibiotic (MeSH -Anti-Bacterial Agents),
cardiopulmonary arrest (MeSH-Heart Arrest), and acute respiratory distress syndrome (MeSH-Respiratory Distress Syndrome, Adult). Suitable MeSH terms
were not available for 47 key words (18%). A Key Word based PubMed search
showed that 67(26%) key words did not yield original article; 37 (14%) of author
identified keywords were not included in the text of manuscript. Conclusions:
57% of Key Words in Critical Care Medicine were used correctly, in accordance
with MeSH vocabulary. A PubMed search using author selects Key Words failed
to retrieve 26% of articles. MeSH compatible terms should be used as Key Words,
and should be included in the text of manuscripts to optimize literature search
retrievability.
295
USING AN AUDIENCE RESPONSE SYSTEM SMARTPHONE
APP TO IMPROVE RESIDENT EDUCATION IN THE PICU.
Hoyoung Chung1,2, Tom Kallay1,2, Nick Anas3, Diana Bruno1, Jose Decamps1,
Darci Evans1, Niveditha Vilasagar1, Richard Mink1,2; 1Harbor-University of California Los Angeles Medical Center, Torrance, CA, 2LA Biomedical Institute, Torrance, CA, 3Children’s Hospital of Orange County, Orange, CA
Learning Objectives: Technological advances are changing medical education. We
used an Audience Response System (ARS) smartphone app in the Pediatric Intensive
Care Unit (PICU) to identify resident knowledge gaps and utilized this information
to guide teaching. We hypothesized that using ARS education in the PICU would
improve resident knowledge. Methods: 3rd year residents in the PICU were randomly
selected to use ARS. Prior to making rounds, study subjects completed an ARS quiz
using the Socrative® app on a topic selected by the principal investigator (PI) based on
diagnoses of patients in the PICU. At the same time, the fellow predicted resident performance on the quiz. Then, the PI texted the test scores to the fellow along with points
for discussion based on the incorrect answers. The fellow directed his/her teaching on
rounds to address these knowledge gaps. Controls (CTL) did not use ARS and received
traditional teaching. All residents completed pre- (PRE) and post-rotation (POST)
tests based on the topics and a survey evaluating ARS. The POST-PRE difference was
analyzed with a t-test. Kappa was used to determine the agreement between fellow’s
prediction of resident performance and actual results. Data are mean±SD. Results: 13
residents have participated in ARS and 9 in CTL. The PRE scores between the two
groups were similar (ARS 70 ± 10%, CTL 71 ± 9%; p>0.05). On the POST, the study
group did not perform better than CTL (POST-PRE difference 6 ± 11% vs. 7 ± 10%,
respectively; p>0.05). The fellows’ prediction on resident performance improved over
time (% agreement in week 1=10%, week 2=20% & week 3= 29%). All residents
thought that ARS had educational value, and fellows felt that it enhanced their teaching. Conclusions: Although all participants felt that ARS is a useful teaching tool, the
ARS group did not perform better on the POST than CTL. Initially, fellows underestimated resident knowledge but the gap improved over time as evident by 3 fold increase
in % agreement. ARS education may still be an effective teaching method in the PICU
but other outcome measures may be needed to demonstrate its efficacy.
Poster Session: Education 2
296
EVIDENCE-BASED ICU FELLOW TRACHEAL INTUBATION
SKILL MILESTONES
Maki Ishizuka1, Donald Boyer1, Wynne Morrison1, Justin Lockman1, Natalie
Napolitano1, Robert Berg1, Vinay Nadkarni1, Akira Nishisaki2; 1The Children’s
Hospital of Philadelphia, Philadelphia, PA, 2The Children’s Hospital Philadelphia, Philadelphia, PA
Learning Objectives: Tracheal intubation (TI) is a core technical skill for critical
care medicine fellows (CCM). The Accreditation Council for Graduate Medical
Education has requested the development of clinical skill milestones; however,
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
limited data exist to describe current CCM fellow skill acquisition over time.
We hypothesized that TI success rates by CCM fellows improve predictably
over time. Methods: We queried the National Emergency Airway Registry for
Children (NEAR4KIDS) local database at a large academic PICU for all TIs
attempted by pediatric CCM fellows from 7/2011-6/2013 (12 quarters). All data
were collected prospectively using a standard reporting system with high compliance (>95% capture rate). TI success was defined as a successful TI with one or
more attempts. We adjusted for factors associated with difficult TI (history of difficult airway, upper airway obstruction, limited mouth opening, and patient age).
Fisher’s exact and multivariate logistic regression were used with p<0.05 as significant. Results:774 primary TIs were reported; CCM fellows performed TI in 398
(51%). TI success rates were 87% during the first quarter and 92% during the last
quarter of fellowship, which improved over time (odds ratio:OR for successful TI
per quarter: 1.11, CI95:1.02-1.22, p=0.02). After adjusting for covariates, the
TI success rate remains significantly associated with training duration (OR for
successful TI per quarter: 1.12, CI95:1.02-1.24, p=0.02). The estimated TI success rates for the first quarter of each training year were: 83% (1st year, CI95:7689%), 89% (2nd year, CI95: 85-92%), and 93% (3rd year, CI95:88-96%), and
95% in the last quarter of 3rd year, (CI95: 89-98%). Conclusions: The TI success rate significantly improved over time. Such data improves understanding
of CCM fellowship skill acquisition and may be used for skill-based milestone
development. Generalizability needs to be evaluated in other CCM settings.
297
EFFECT OF SIMULATION BASED CURRICULUM ON THE
UTILIZATION OF RAPID RESPONSE TEAM ACTIVATIONS
(RRT)
Shashikanth Reddy Ambati1, Todd Sweberg2, Peter Silver3, Sandeep Gangadharan4; 1Cohen Children’s Medical Center of New York, New Hyde Park, NY,
2
Cohen Children’s Medical Center, New Hyde Park, NY, 3Cohen’s Children’s
Hospital, New Hyde Park, NY, 4Cohen Children’S Medical Center, New Hyde
Park, NY
Learning Objectives: When a child in an inpatient unit decompensates, the
first responders are nurses and residents. Early appropriate interventions have
the potential to improve a child’s clinical status before it irreversibly deteriorates.
The aim of the study is to assess a PASS (Pediatric Acute Care Assessment and
Stabilization) program that improves the initial assessment, recognition of escalation triggers for RRT, and initial stabilization skills, and its impact on RRT
utilization. Methods: The PASS curriculum was developed in 2011, and was
targeted to tertiary children’s hospital medical/ surgical floor nursing staff and
junior pediatric residents. Simulation scenarios included common clinical deteriorations observed on a pediatric floor such as respiratory failure, shock, seizures
and apnea. The hospital CPR committee maintains a database of all CPR and
RRT events in de-identified form for quality improvement purposes. Results:
Compared to the year of PASS initiation (2011) when there were 182 RRT activations, the number of RRTs increased to 198 in 2012(9% increase), 240 in 2013
(32% increase) and 276 annualized for 2014(52% increase). Conclusions: Rapid
response teams have been adopted widely in children’s hospitals as a system for
rapidly escalating and triaging care for clinically deteriorating patients. Successful
implementation of these programs requires a change in the safety culture and an
educational curriculum to educate primary providers in both initial assessment
and stabilization of deteriorating children, and criteria for escalation/activation
of the RRT. We believe our dedicated simulation based educational curriculum
familiarizing front-line staff about the triggers for RRT was an effective resource
in improving the utilization and accuracy of RRT events.
298
ANNUAL FIELD EPIDEMIOLOGY COURSE: A SIMULATED
INVESTIGATION OF A FEBRILE ILLNESS IN TUMBES, PERU
Suchitra Pilli1, Amit Kumar2, Andres Lescano3, Patricia Lozano2, Sharon Onguti2,
Juan Sanchez4, Clinton White2; 1University of Texas Medical Branch Hospitals,
Galveston, TX, 2University of Texas Medical Branch, Galveston, TX, 3Naval and
Medical Research unit - 6, Lima, Peru, Lima, Peru, 4Naval and Medical Research
unit - 6, Lima, Peru, Lima, Peru
Learning Objectives: The Field Epidemiology course in Peru is designed to train
students of public health, infectious disease and epidemiology in the planning,
conduct and analysis of an outbreak investigation. Methods: We completed this
course in Lima, Peru at the NAMRU-6 location from Aug 5-Aug 16, 2013, investigating a simulated febrile outbreak in Tumbes, Peru. Participants conducted a
12-day-field investigation with epidemiological, laboratory, entomological and
zoonotic components. This involved information gathering, logistical planning,
study design and travel with on-site installation at a local Cysticercosis health
center and a visit to the Zarumilla primary health center. The methods included
house-hold population surveys, biological sample collection, vector studies,
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
collection of larvae, pupae, adults of Anopheles, Aedes and Culex mosquitoes
from rural and urban environments, reservoir studies, mosquito trapping, insecticide sensitivity testing, rodent trapping, bat trapping and necropsies of rodents
and pigs, bird stool sampling and training in cohort study design and basic parasitological and virological testing techniques. Results: Human population survey
analysis with geo-spatial mapping of the surveyed area and entomological studies
of the larvae and adults of Anopheles, Culex and Aedes mosquitoes collected in
both rural and urban setting was done. Mosquitoes were tested for insecticide
sensitivity with Cipermethrin, Deltamethrin and an ethanol control. Rodents
and bats were trapped and necropsies were performed on mice and pigs infected
with cysticercosis. Conclusions: This course is a successful example of integration
and complementary efforts to build global capacity for response to pandemics
and global health emergencies as well as international collaborative research and
increased our knowledge of practical aspects of epidemiological field investigations. Limitations include traveler’s diarrhea and limited pre-course knowledge of
tropical medicine and epidemiology among the participants.
299
INTERN PERCEPTION OF CODE BLUE SIMULATION TRAINING IN RESIDENCY
Adam Mora1, Bijas Benjamin2, Jennifer Duewall2, Britton Smialek2; 1N/A, Dallas, TX, 2Baylor University Medical Center, Dallas, TX
Learning Objectives: In some educational institutions, interns are expected to
participate and even manage codes as early as day one of residency. Simulation
training is becoming a main stay in medical school education yet this modality
doesn’t seem to be substantially utilized to train future doctors in one of the
most crucial skills required early on in their careers. Methods: During orientation week, the entering intern class of Baylor University Medical Center’s internal
medicine residency program were surveyed to assess their experience with simulation training, code experience, attitude toward simulation in their medical education and perception of readiness to participate or lead a code. Residents then
received a didactic lecture reviewing the mechanics of running a code which was
augmented by code simulation with a 3G SimMan. A post-code assessment followed. Results: A total of 16 residents were asked to participate in surveys and 16
responded for a response rate of 100%. While 100% of those surveyed reported
their medical schools provided simulation training of which 15 out of 16 (93%)
specifically had code blue simulation training and 10 out of 16 interns (62.5%)
reported participation in an actual code (none as code leaders), 0% felt prepared
to run a code on day one. All believed formal code training was necessary. Furthermore, all believed that specific training in code debriefing and addressing
code status should be taught in both medical school and residency. Following
specific code training in a simulation lab, 100% felt more comfortable about
participating in a code and 93% felt more prepared to lead a code on day one of
internship. Post education, all interns thought formal code training to be helpful, a necessary part of medical education/training and mandatory in residency
training. Conclusions: Simulation is common in medical education, but doesn’t
provide new physicians a vital skill set needed early in training. New physicians
are not comfortable participating in codes but have a dramatic change in their
perception with simulation training and they are open to this training modality.
300
DEVELOPMENT OF INTERNATIONAL PEDIATRIC FUNDAMENTALS OF CRITICAL CARE SUPPORT (PFCCS)
INSTRUCTORS
Beth Ballinger1, Sheri Crow1, Giorgi kvitsinadze2, David Tsibadze3, Grace
Arteaga1; 1Mayo Clinic, Rochester, MN, 2Maternal and Child Health Health, D.
Tvildiani Medical University, Tblisi, Georgia, 3D. Tvildiani Medical University,
Tblisi, Georgia
Learning Objectives: PFCCS trains providers to manage acutely ill children.
Our goal was to evaluate PFCCS as a tool to develop a consistent and sustainable
critical care educational system in the Republic of Georgia while using a “train
the trainer” educational strategy. Methods: Over 18 months and 4 visits, Mayo
Clinic and Georgian Pediatric Critical Care leadership collaborated to: 1. Survey
health care needs within the Republic of Georgia: 2. Preview PFCCS lectures and
simulation scenarios to evaluate interest and win “buy-in” from key stake-holders
throughout the Georgian medical infrastructure, 3. Identify PFCCS instructor
candidates. Training for Georgian PFCCS instructors was achieved as follows: 1.
PFCCS course consultants presented PFCCS course Day 1 materials to Georgian
instructor candidates. 2. Simulation learning principles were taught to instructor
candidates and basic equipment was acquired. 3. Instructor candidates presented
PFCCS Day 1 to Georgian learners while mentored by PFCCS consultants.
4. Evaluation and debriefing with instructor candidates using PFCCS course
evaluation forms. 5. Translation of PFCCS slides into Georgian. Steps 1-4 were
repeated for Day 2 content. 6. Learner evaluation of PFCCS course utility with
novel form. Results: Six candidates were identified and completed the PFCCS
instructor training. They presented PFCCS to 15 Georgian medical students.
Student PFCCS test scores improved for students (n=14) (pretest: 38.7 ± 7 vs
post-test 62.7 ± 6, p<0.05). A Likert scale of 1 to 5 (1=not useful; 5=extremely
useful) was used to evaluate the responses for a)Relevance of PFCCS content to
clinical work: Very useful (mode=9); b)Effectiveness of lecture delivery: Effective
(mode=8); and c)Value of skill stations for clinical practice: Very useful (mode=8).
Conclusions: Our model of PFCCS instructor training is an effective tool that
can be tailored to the local needs of an international setting with demonstrated
user satisfaction. Further studies are needed to show improved patient outcomes
through translation of PFCCS principles into the Georgian healthcare system.
301
NURSING PERCEPTIONS AND ASSOCIATION
APPROACH RATES IN THE THAPCA TRIALS
WITH
Brittan Browning1, Renee Kuhn2, Ann Pawluszka3, Mary Ann DiLiberto4, Evin
Golson5, Jendar Deschenes6, Eileen Taillie7, Kent Page1; 1University of Utah, Salt
Lake City, UT, 2University of Utah Health Care, Salt Lake City, UT, 3Childrens Hospital of Michigan, Detroit, MI, 4Children’s Hospital of Philadelphia,
Philadelphia, PA, 5Children’s Medical Center Dallas, Dallas, TX, 6University of
Arizona, Tucson, AZ, 7University of Rochester Medical Center, Rochester, NY
Learning Objectives: The THAPCA Trials are multicenter randomized trials
evaluating the effect of active temperature control on survival and neurobehavioral outcome after pediatric cardiac arrest. Since PICU nurses care for and
interact with families enrolled in research, their perceptions may impact trial
recruitment. The goal of this project was to determine whether nurses’ perceptions of the THAPCA trials were associated with rates at which eligible families
were approached for consent and successfully enrolled in the trial. Methods: At
the 16 (of 38 total) THAPCA sites participating, a 38 item investigator-developed, IRB-approved survey was distributed electronically to PICU/CICU nurses.
Demographic and Likert scale questions elicited responses about perceptions
of training, the trials and the study team. Pearson correlations were calculated
between average institution-wide response to each Likert scale question and site
approach rates (number approached/number eligible) and site enrollment rates
(number randomized/number eligible) for the THAPCA trials. Results: Of 2241
eligible nurses, 1387 (62%) completed the survey. The majority of respondents
(93%) had cared for a patient in research studies and 92% agreed that research
is an important component of care in the PICU/CICU. In THAPCA, higher
center-specific subject approach rates were significantly correlated with nurses’
perception that their institution values research (r=0.53, p=0.040), that their
PICU/CICU supported the THAPCA trials (r=0.63, p=0.011), and that the
THAPCA trials should be done in children despite previous cooling data that
show benefit in adults (r=0.61, p=0.016). No significant correlation was found
between nurses’ perceptions and THAPCA enrollment rate. Conclusions: We
found that the majority of nurse respondents felt that research was an important
part of care in the PICU/CICU. In addition, study teams should be aware that
nursing attitudes may have an impact on the completion of trials, and this should
be considered during trial planning and execution of a large study.
302
included: 1) Use of language and communication (53%) ie. “how words, expressions and actions affect the family;” 2) Team building (38%); ie. “learned more
about the roles of others”; 3) Improved knowledge of protocols (22%); ie. “how
to interact with OPO and who brings up DCD”; and 4) Opportunities not found
in the clinical setting (11%); ie. “never participated in DCD and this helped me
understand the process.” Conclusions: Simulation effectively provides the means
for team training in EOL and organ donation discussions. Improved knowledge
of protocols and communication between ICU teams and OPO personnel occurs.
303
ACHIEVING COMPETENCY IN ULTRASOUND GUIDED
CENTRAL VENOUS CATHETER INSERTION FOR INCOMING
HOUSE STAFF
Zafar Akram Jamkhana1, Brian Reichardt2, John Mwangi3, Nirav patel4, Aditya
Uppalapati4; 1saint Louis univeristy, Saint Louis, MO, 2Saint Louis University
School of Medicine, 3Saint Louis University, St. Louis, MO, 4Saint Louis University, Saint Louis, MO
Learning Objectives: Ultrasound guided central venous catheter (CVC) insertion
is now the standard of care. There are no specific recommendations for training or
assessing house staff competency. The purpose of our study was to assess whether a
simulation based workshop could improve ultrasound knowledge and understanding of sterile CVC insertion technique among the incoming house staff. Methods: New incoming internal medicine residents participated in the workshop as
part of their hospital orientation. They first filled out a questionnaire as a pretest
which contained 3 parts – basic ultrasound knowledge and anatomy, ultrasound
images, and 10 video clips showing errors in insertion technique. The residents then
received a one hour presentation followed by hands-on training consisting of sterile
technique, vascular ultrasound use, and ultrasound guided CVC placement technique on a mannequin. Immediately following the workshop they retook the same
questionnaire as a post-test. Descriptive statistics and paired t tests were used to
compare the results. Results: Of the 29 house staff participants 10% had experience
with ultrasound guided CVC insertion, 66% had some ultrasound knowledge, and
24% with no ultrasound experience. There was a significant difference in pretest
and post-test scores for ultrasound knowledge and anatomy (3.52 vs 5, t=2.05,
p=0.001); ultrasound image identification (7.14 vs 8.86, t=2.05, p=<0.001); and
error detection on video clips (11.86 vs 14.52, t=2.05, p=<0.001). There was
improvement in total score from 66.2% in pretest to 83.5% in post-test (t=2.05,
p=<0.001). Conclusions: Our data suggests that a standardized education protocol
with a didactic lecture based on the ACCP guidelines and hands-on simulation
increases resident understanding of ultrasound guided CVC insertion. Our novel
approach utilising ultrasound images and questions based on video clips improved
and assessed their knowledge. We conclude that a brief educational workshop
paired with a structured assessment is an effective way to enhance the knowledge of
incoming house staff in performing ultrasound guided CVC insertion.
304
COMPUTER SOFTWARE DEPICTS DYNAMIC SHIFTING OF THE OXYHEMOGLOBIN DISSOCIATION CURVE
VIDEOGRAPHICALLY
SIMULATION TRAINING FOR ICU TEAMS FOR APPROACH
TO DONATION AFTER CARDIAC DEATH
Robert Demers1, Otaniel A. Castillo2; 1Southern California Permanente Medical Group, Pasadena, CA, 2Anesthesia Technology Program, Kaiser Permanente
Anesthesia, Pasadena, CA
Learning Objectives: The ICU team frequently faces family meetings and end of
life (EOL) discussions that involve the opportunity for organ donation. Oftentimes donation discussions occur without the proper personnel and training to
effectively follow protocols. Simulation training was used for teams of ICU providers and our local organ procurement organization (OPO), to further understand protocols and improve teamwork around organ donation after cardiac death
(DCD). Methods: A simulation curriculum was developed for the neurosurgical,
cardiac, surgical and medical ICU’s with 3 parts: 1) a chance hallway encounter
with the RN, MD and the family, who requested to withdraw life support in an
adult patient with limited brain stem activity; 2) a huddle (MD, RN, FA (family
advocate), OPO); and 3) a family meeting (MD, RN, OPO, FA) that included
introduction of personnel and discussion about DCD, followed by a facilitated
debriefing. Actors were used to portray family members. The sim was repeated
for teams of Fellows and RNs and Attendings and RNs. A qualitative analysis was
performed on learner feedback. Results: Thirty seven scenarios were completed
during 2 sessions, 8 months apart. Six Attendings, 12 ICU Fellows; 10 RNs, 9
FA, 20 OPO staff attended. The sim encounters were 1.5 hours each. Over 81%
of participants had previous sim experience and 92% had previous EOL discussions with family members. with 57% < 5 years of experience. Common themes
Learning Objectives: The oxyhemoglobin dissociation curve (OHDC) can be
modeled mathematically, but the equation for that sigmoid curve is formidably
complex. In the process of teaching about the OHDC, I wanted to portray, in
dynamic fashion, the curve’s tendency to shift in response to alterations in blood’s
pH and carbon dioxide tension (pCO2). Methods: A polynomial equation
which faithfully models the OHDC has been described by G. Richard Kelman
(J Appl Physiol 1966; 21: 1375-1376). His methodology incorporates correction
factors for variations in pH and pCO2. One can solve the equation manually,
but its’ complexity renders this a tedious and time-consuming process. Kelman’s
equation was incorporated within a computer spreadsheet (Numbers® software;
Apple, Inc., Cupertino, CA) in order to generate data pairs which accurately
express oxygen saturation as a function of oxygen tension. Spreadsheet functionality allows users to generate plots of numerical parameters incorporated within
any tables which it creates. The software was employed to generate the plot of
percent saturation (ordinate) versus oxygen tension (abscissa) for oxygen tension
values ranging between 10 and 200 torr. Results: Because the software solves
the Kelman equation so rapidly, it virtually scribes the OHDC in real-time. As a
result, we can depict dynamic shifting of the OHDC in silico within a timeframe
which is comparable to the curve-shifting dynamics which take place in vivo.
Those who attend this presentation will view a video loop which depicts dynamic
shifting of the OHDC videographically, so that they can ascertain if this tool
might be useful in their own practice as clinical educators. Conclusions: Some
Sandy Swoboda1, Clint Burns1, Maggie Neal2, Pamela Lipsett3; 1Johns Hopkins
Hospital, Baltimore, MD, 2Johns Hopkins University School of Nursing, Baltimore, MD, 3Johns Hopkins Medical Institutions, Baltimore, MD
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
physiologic concepts are as formidably complex as they are elegantly beautiful.
The ability of spreadsheet software to generate high-resolution graphics at the
stroke of a key liberates the educator from the chore of creating elaborate diagrammatic representations manually. Screen-capture software can then be used to
confer a more visceral appreciation of this dynamic physiologic process.
305
USING A “FLIPPED CLASSROOM” MODEL TO TEACH BEDSIDE ECHOCARDIOGRAPHY IN A SURGICAL ICU
Christopher Tainter1, Gaston Cudemus1, Edward Bittner1; 1Massachusetts General Hospital, Boston, MA
Learning Objectives: Challenges to education in the ICU include the wide range
in level of training and experience among learners, competing clinical demands,
and duty hour restrictions. The traditional model of teaching may be improved
with a “flipped classroom” design. Methods: A curriculum was designed to teach
Critical Care Echocardiography. Four modules were designed around core concepts, each consisting of a 5-minute video watched prior to a “hands-on” teaching session led by experienced providers at the bedside. The four modules were:
Principles of Ultrasound (background information, ultrasound physics, inferior
vena cava); Basic Views (parasternal long- and short-axis, apical four-chamber,
and subcostal views, pericardial effusion); Doppler and Valves (Doppler measurements, velocities, pressure gradients); and Functional Assessment (ejection
fraction estimation, stroke volume, diastolic function). To assess the efficacy of
the curriculum, pre- and post-testing was performed, consisting of knowledge
questions and a Likert Scale assessment of confidence with the content area, usefulness of the skills and likelihood that they would use the skills in their clinical
practice. Participants also evaluated the quality of the videos and hands on sessions, and provided feedback for improvement. Results: There were significant
improvements in scores for knowledge (p<0.004), confidence with ultrasound
use (p<0.002), and applicability to clinical practice (p<0.05) with all of the modules. There were non-significant increases in perceived usefulness scores for modules 1 and 2 (p=0.096, p=0.086), but significant increases in modules 3 and 4
(p=0.041, p=0.021). Median reported quality score for each the videos was 8
out of 10, and 9 out of 10 for the hands-on experiences. Conclusions:Residents
reported increased satisfaction with the “flipped classroom” experience compared
to the traditional lecture method. They showed improvements in knowledge,
confidence, and perceived transferability of this knowledge to clinical practice.
The “flipped classroom” educational model is well-suited for teaching echocardiography in the ICU.
Poster Session: Education 3
306
VALIDATING PEDIATRIC CRITICAL CARE TRAINING
WITH KNOWLEDGE, CONFIDENCE, AND SIMULATION
COMPETENCY
Daniel Bruzzini1, Heidi Sallee2, Jeremy Garrett2, Jason Werner2; 188th Medical
Group, Wright-Patterson AFB, OH, 2Saint Louis University, Saint Louis, MO
Learning Objectives: Objective: Validate the two-day Society of Critical Care
Medicine’s (SCCM’s) Pediatric Fundamental Critical Care Support (PFCCS)
course as an effective pediatric critical care training platform using measures of
objective learning, learner self-reports of perceptions of confidence, and performance on high-fidelity simulations, a quantitative Knowledge, Confidence,
Competency (KCC) tool. Methods: Design: Prospective repeated measures
assessment. Setting and Subjects: First year and third year pediatric residents from
St. Louis University and the University of Missouri at Columbia. Interventions
and Measurements: Pre-test and post-test exams assessed knowledge of PFCCS
participants. A survey of ten ten-point Likert scale questions on managing critically ill children was taken before and after the course to assess confidence in caring for critically ill children. Two videotaped and pediatric intensivist-debriefed
high-fidelity simulations were used to assess clinical competency of residents.
Pediatric residents actively completing the PFCCS program (first year residents
N=73) were compared to pediatric residents without PFCCS training. (third year
residents N=15). Results: 1. The PFCCS course experience improved knowledge. Pre-test PFCCS mean 60.5% std. dev. 15.4 versus PFCCS Post-test 85.6
std. dev. 7. p < 0.0001 2. Self-confidence improved 38% overall in all ten key
pediatric critical care tasks, (range 25-60%). 3. Psychomotor skills improved
significantly following intensivist led videotaped debriefing (32% for PFCCS
engaged residents) as a measured by Pediatric critical care high-fidelity simulation
performance. . 4. PFCCS course effect: PFCCS certified residents required less
time (421 sec.) to recognize and treat cardiopulmonary failure on the high-fidelity
simulation as compared to residents without PFCCS training (596 sec.). Conclusions: The KCC tool proves PFCCS training results in significant Knowledge,
Confidence, and Competency improvement by first year pediatric residents that
is equal to or better than third year pediatric residents without PFCCS training.
307
DESIGNING & IMPLEMENTING A WEB-BASED “QUESTION OF THE DAY” MODULE IN A BUSY CRITICAL CARE
FELLOWSHIP
Avinash Kumar1, Jennifer Morse1, Lisa Weavind1; 1Vanderbilt University Medical
Center, Nashville, TN
Learning Objectives: A majority of critical care fellowship programs use the Multidisciplinary Critical Care Knowledge Assessment Program (MCCKAP) examination as a valuable preparation tool for the final board examination in Critical
Care Medicine. We designed, tested and implemented a voluntary, web-based,
upgradable, mobile-centric automated module of questions to be delivered at specific time intervals to meet this need. Methods: We designed a secure questions
and answers database using REDCap - a secure database application supported
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
by the National Center for Advancing Translational Sciences/National Institute
of Health (NCATS/NIH). The topics were identified by evaluating deficiencies in
the previous MCCKAP examinations. Single questions were available on mobile
devices at 11AM each workday to all fellows and attendings. Immediate feedback
and explanations were available on answering the questions. Data was analyzed by
calculating the percentage of questions answered and the percentage of attempts
for each topic and for the overall group of questions. A correlation statistic was
calculated to compare the data. Results: A total of 175 questions were deployed
over a period of 5 months starting in 10/2013. The mean percentage of questions
answered by our 7 fellows was 54.3% ± 17.3%. Overall, the fellows fared best
on general surgical questions (81.9% ± 11.5% correct), followed by toxicology
(81.1% ±16.8%), nephrology (69.2% ± 20.6%), general critical Care (66.9% ±
15.8%) and neurologic critical care (58.3%±19.2%). The number of questions
attempted did not correlate with the number of correct responses (R2=0.09). 11
of 20 attending physicians participated regularly in the module. However the
faculty attempted the questions only 22.45% of the time with 80.4% accuracy
in correctly answering the questions on the first attempt. Conclusions: Question
of the day is an engaging learning strategy and a valuable adjunct to traditional
lecture based content. Identifying learning gaps helped us address deficiencies
prior to the end of the 2013-14 academic year and refocus the curriculum plan
for 2014-15.
308
REINFORCING ABCDE BUNDLE CONCEPTS THROUGH
INTERPROFESSIONAL SIMULATION AND TEAM STEPPS
TRAINING
Cara McDaniel1, Nethra Ankam2, Alan Forstater3, Elizabeth Speakman2, John
Duffy2, Lauren Collins2, Dimitrios Papanagnou2, Michael Weinstein2; 1Thomas
Jefferson University Hospital, Philadelphia, PA, 2Thomas Jefferson University,
Philadelphia, PA, 3Thomas Jefferson University, Philadephia, PA
Learning Objectives: The ABCDE bundle is an evidence-based tool designed to
implement pain, agitation, and delirium guideline recommendations into routine practice. However, health-system wide implementation of bundle components demands effective coordination of care and team-based communication to
optimize patient and safety outcomes. This educational program was designed to
promote effective teamwork and patient safety skills, while removing barriers to
successful implementation of the ABCDE bundle. Methods: Sixty interprofessional ICU providers representing five healthcare disciplines from nine ICU areas
of practice participated in a four hour workshop to augment unit-based ABCDE
education. The workshop utilized simulation and Team STEPPS training combined with brainstorming and debriefing sessions to promote interprofessional
communication and teamwork. Participants completed a pre-and post-workshop
questionnaire to assess effectiveness of the workshop at improving communication skills and optimizing patient safety. Results: This interprofessional workshop allowed participants to interact with all health professions across varying
ICU settings to review ABCDE skills and to identify actionable solutions to
address implementation barriers. Although participants identified many barriers
and issues related to bundle implementation, they eagerly matched those with
constructive solutions to bring back to their individual ICUs. As a result of the
workshop, 94% of participants reported an increase in confidence in implementing ABCDE bundle components and 90% reported an increase in confidence
regarding communication related to patient safety issues. Conclusions:The
hands-on workshop provided an ideal format for interprofessional training. By
introducing Team STEPPS vocabulary and skills, participants felt empowered to
advocate for patient safety and optimize patient care and less hesitant to implement ABCDE bundle components. Creating opportunities for teams to work
together to identify issues and solutions is essential to successful implementation
of new protocols and to affect change to the culture of practice.
average pre-test score was 61% that improved to an average score of 85% correct answers on post-test (p<0.0001). The average improvement score comparing
the pre and post-test was 24%. 35 out of 36 participants improved their scores.
Conclusions: The Simulation-Based Central Venous Catheter Placement training program for Internal Medicine residents was able to improve knowledge base
on central venous catheter placement and should be an integral part in the training of all internal medicine residents.
309
ASSESSMENT OF DISASTER-PREPAREDNESS AMONGST
PEDIATRICIANS
311
EVALUATION OF FCCS IN CRITICAL CARE EDUCATION IN
JAPAN: A SURVEY OF INSTRUCTORS AND PARTICIPANTS
Kazuaki Atagi1, Shigeki Fujitani2, Takamitsu Kodama3, Jun-Ya Ishikawa4, Masahiko Kawaguchi5; 1Nara Medical University, Kashihara-city JAPAN, 2St Marianna
University, Kawasaki-city, Kanagawa, 3University of Texas Southwestern Medical
Center, Dallas, TX, 4Advanced Critical Care & Emergency Center, Yokohama,
Japan, 5N/A, Kashihara-Shi, Nara-Ken
Learning Objectives: A Fundamental Critical Care Support (FCCS) program
specific to Japanese clinical settings has been introduced after minimal adaptation
of the original course in the United States. The American FCCS course is often
used to prepare residents for rotations in the intensive care unit; therefore, this
program can be used for basic critical care training in Japan to standardize critical
care management. The purpose of this study was to evaluate whether the Japanese FCCS course is effective and potentially useful in critical care management
in Japan through a survey of FCCS instructors and participants. Methods: The
FCCS program was conducted in the form of lectures and skill stations. Pre- and
post-training knowledge was assessed. After completion of a 2-day FCCS course,
a questionnaire survey was administered to all participants, who were asked to
respond to questions regarding the course. FCCS instructors (n = 51) also were
asked to respond to questions regarding the usefulness of the course in critical care
education in Japan. Results: Over the past four years, the number of participants
in the FCCS program has increased to 2200. Nearly 70% of the participants
are physicians, and most others are nurses. When the course was first offered,
more than half of the participating physicians had >5 years of clinical experience;
however, this percentage has gradually decreased. Meanwhile, the proportion of
residents and nurses has increased. Regarding the usefulness of the course, nearly
half of the participants thought that the session on mechanical ventilation (MV)
was the most useful. More than 80% of the instructors acknowledged some misunderstandings after becoming FCCS instructors. The instructors also responded
that the session on MV was the most useful session of the course, and practical
application of the training was seen in their changes in the MV setting in their
clinical practice after becoming FCCS instructors. Conclusions: The Japanese
FCCS course was considered useful by the participants and instructors alike, and
is potentially useful for critical care management in Japan.
310
Shantaveer Gangu1, Sonea Qureshi2, Kozue Shimabukuro3; 1Loma Linda University, Loma Linda, CA, 2Loma Linda Children’s Hospital, Loma Linda, CA,
3
Loma Linda, Los Angeles, CA
Learning Objectives: The purpose of this survey-based study was to assess
pediatricians knowledge of disaster-preparedness in natural disasters, domestic
terrorism, and other forms of disasters. Methods: An online multiple-choice
questionnaire designed to assess knowledge about disaster plans was distributed
to pediatricians working in academic institutions, community hospitals, and
private practices. Participants also included residents and fellows. Collected
data included participant’s comfort levels in various aspects of disaster management, including team formation, team leadership, skill sets required for patient
stabilization, knowledge of resources available to them, and their own role
during a disaster within their community. Results: The survey was administered using Qualtrics, an online survey tool. The response rate was 14.5% (146
out of 1007) over 10 weeks. By clinical setting, the majority of participants
were from academic pediatric hospitals (65%), and by profession, most were
general pediatricians (54%). 98% of respondents were willing to respond in
the event of a disaster within their community, but only a quarter reported
receiving pediatric-specific disaster training. Only one-third of the physicians
participated in annual disaster drills. More than two-thirds of respondents were
not familiar with their hospital’s and/or clinic’s disaster response plan and felt
they needed further training. The majority of our participants reported being
comfortable managing airways (73%), shock (63%) and disaster triage (56%).
However, many other aspects reported low comfort including familiarity with
emergency communication devices (25%), knowledge of stocks of equipment
for disasters (37%), techniques for victim identification (24%), processes for
family reunification (27%), and managing bioterrorism (24%) and radiation
exposures (10%). Conclusions: This study reveals an immediate need for pediatric-specific disaster training among general pediatricians, physicians in training, and sub-specialists including pediatric emergency physicians and critical
care practitioners.
312
COMMUNICATION & PROFESSIONALISM: VALIDATION
OF AN ASSESSMENT TOOL IN A PEDIATRIC FELLOWSHIP
PROGRAM
SIMULATION-BASED CENTRAL VENOUS CATHETER PLACEMENT TRAINING PROGRAM FOR INTERNAL MEDICINE
RESIDENTS.
Shilpa Balikai1, Ken Wallston2, Stacey Williams2, Geoffrey Fleming3, William Cutrer4;
1
Vanderbilt Children’s Hospital, Nashville, TN, 2Vanderbilt University, Nashville,
TN, 3Vanderbilt Children’S Hospital, Nashvillle, TN, 4N/A, Nashville, TN
Learning Objectives: Simulation-based training of central venous catheter
(CVC) placement has been shown to improve operator procedural competence,
decrease complication rates and reduce incidence of catheter-related bloodstream
infection. The aim of this project was to provide a simulation-based education
course for all incoming Internal Medicine (IM) Residents and further enhance
their knowledge and procedural skills in CVC placement. Methods: A 4 hr simulation-based education course was developed for incoming IM residents prior to
starting their residency training at our institution. This training began in 2012
and has been part of incoming medicine resident orientation since. It consisted
of a pre-training test to assess basic knowledge on CVC placement followed by
a 30 minute presentation about important evidence-based information pertaining to CVC placement. It was followed by One-on-one instruction on proper
sterile barrier technique i.e. sterile gown and sterile gloves prior to a hands on
procedure technique and vascular ultrasound use on a part-task trainer mannequin. A team of instructors comprising of 2 attendings and 5 pulmonary/ critical
care fellows, who were proficient in ultrasound-guided central venous catheter
placement technique, administered the course. Each instructor was assigned to 3
trainees. The equipment includes ultrasound machines along with 5 Blue phantom mannequins. Expired CVC kits were obtained from our central supply and
utilized in the simulation training. Results:There have been a total of 36 1st year
residents that had been trained in this course since the program started. The
Learning Objectives: The Accreditation Council for Graduate Medical Education (ACGME) has outlined six core competencies that trainees should demonstrate proficiency in during their residency training. No standardized methods or
set of tools to evaluate and assess trainee progression during training currently
exist. Pediatric Critical Care (PCC) Fellows are one trainee group without valid
communication assessment measures. This study examined the validity evidence
for the use of the Communication and Interpersonal Skills (CIS) Tool in a realtime clinical setting to assess the interpersonal and communication skills competency in PCC Fellows (trainees). Methods: Patient family members completed
CIS tool surveys about the PCC fellow they interacted with during their child’s
admission to the Pediatric Intensive Care Unit. As a comparison tool for the CIS,
we selected the previously validated Communication Assessment Tool (CAT)
based on its success in the adult outpatient setting. Patient family members also
completed the CAT at the time of completing the CIS tool. Additionally, for
patient encounters with direct faculty observation, faculty completed both the
CIS and CAT tools assessing fellow performance. Results: The overall total score
for both the CIS and CAT tools correlated highly at 0.82 (p < 0.001). The CISCS (Communication skills) subscale correlated 0.88 (n = 75; p < 0.001) with the
CAT while the CIS-IS (Interpersonal skills) subscale correlated 0.72 (n = 78; p
< 0.001) with the CAT. The final CIS Global question “Given a choice, I would
choose this fellow as my personal physician” correlated with CIS-CS subscale
0.69 (p < 0.001) and the CIS-IS subscale 0.81 (p < 0.001). Conclusions: The
CIS tool is valid for use by families to assess PCC fellows in the competency of
interpersonal and communication skills.
Killol Patel1, David Shiu2, Keith Guevarra3; 1Newrak Beth Israel Medical Center,
Newark, NJ, 2Newark Beth Israel Medical Center, Newark, NJ, 3UMDNJ - Newark,
Newark, NJ
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
313
RISE AND SHINE EVERYONE: HOSPITAL WIDE EARLY
MOBILITY PROGRAM
Chris Wells1,2, Krystal Lighty2, Julie Pittas2, Kristie Snedeker2, Kathryn Von
Rueden3, Meredith Huffines2, Daniel Herr2; 1University of Maryland School of
Medicine, Baltiomre, MD, 2University of Maryland Medical Center, Baltimore,
MD, 3University of Maryland School of Nursing, Baltimore, MD
Learning Objectives: The ABCDE Bundle can improve critically ill (ICU)
patient outcomes by focusing on targeted sedation, ventilation liberation, mobility, and delirium. The E is early mobility and exercise. An interdisciplinary team
at a large academic medical center was formed for the purpose of developing
and implementing a hospital-wide guideline categorizing patient mobility levels to promote out of bed (OOB) activity. Hypothesis: An interdisciplinary
guideline that defines mobility level for patients will improve rehabilitation and
nursing coordination, facilitate safe OOB activities with no increase in falls or
staff patient handling related injuries and improve patient outcomes. Methods:
As part of an initiative to fully implement the ABCDE bundle, rehabilitation
therapists and ICU nurses, collaborating with physicians and other disciplines
(Rise and Shine Team), developed a Mobility Guideline (MG). The MG includes
assessment of medical stability, sedation level, and a functional screening tool
to determine patient readiness and safest method to facilitate OOB transfers by
nurses. Results: The first outcome was the development of a two-step MG. First
the medical team determines the daily appropriateness of OOB activities. The
assessment considers cardiopulmonary, neurological, skeletal, and integumentary
systems. Step two involves sedation level assessment with RASS, and mobility
screening to assign a mobility level (1-5). The mobility level determines the specific safe patient handling technique to be used by nurses to facilitate OOB.
Second outcome was the education of over 800 ICU nurses and 70 rehabilitation
therapists to use of the MG, RASS and the Mobility Screen. Rehabilitation therapists are conducting education in each ICU on using the MG, Mobility Screen
safe patient handling techniques, and activity documentation. Conclusions: The
interdisciplinary effort to develop a hospital wide early mobility program promoting OOB has successfully resulted in the adoption of MG. Use of this guideline
supports full ABCDE bundle implementation and facilitates staff collaboration
to improve patient outcomes.
314
IMPLEMENTATION OF A SUCCESSFUL INTENSIVE CARE
NURSING STAFF DEVELOPMENT PROGRAM IN HAITI
Jennifer Lutz1, Marc Augustin2, Christy Chua Patel3, Marie Fenestor4, Angela
Patel5, Shella Rock4, Janice Rorabeck6, Hollie Thornton6; 1Mayo Clinic Hospital,
N/A, 2St. Luke Family Hospital, Port-au-Prince, Haiti, 3Mayo Clinic, Rochester, MN, 4St Luke’s Hospital, Port au Prince, Haiti, 5University of Notre Dame,
South Bend, IN, 6Mayo Clinic, Phoenix, AZ
Learning Objectives: Critical care nurses in developing nations are challenged
with limited time and access to educational resources. Despite this Haitian nurses
strive to know practice guidelines and provide quality care. Optimal educational
strategy to meet this need is unknown. A unique approach to global nursing
education involving expert embedded assessment, a collaboratively developed
curriculum and implementation strategy guided by local administrators and
providers can be successful creating a sustainable ICU nursing staff development model. Methods:Qualitative methods were used to describe the process
of education prioritization, teaching methods selected and to determine success of the educational initiative. Preliminary web-based virtual meetings were
conducted with medical and nursing leaders to develop mutual goals. Onsite,
active participant observer embedded assessments and tracer observations were
used to learn and analyze hospital processes and nursing practices. Emphasis was
placed on respectful, authentic and responsive participation to establish rapport. Imperative educational topics and teaching methods were collaboratively
identified from direct observations and interviews with interprofessional staff.
Learning was evaluated by direct observation and return demonstration post
education and 9-12 month later. At 12 months, satisfaction surveys were distributed. Results: Case scenarios were identified as foundational to the curriculum. Train the trainer teaching methods included bedside education, interactive
simulation learning stations, and lectures. Evaluation of learning confirmed
the retention of primary educational topics. Surveys indicated that nurses and
administrators were highly satisfied with the initiative. Conclusions: A nursing
staff development program can be created, implemented, and sustained in developing nations with proper planning and interprofessional collaboration using
active participant observers and contextualized training to identify learning gaps
and reinforces critical knowledge and skills. This may be an effective model in
other global health environments.
315
TOWARD ECHOCARDIOGRAPHY AND CRITICAL CARE
ULTRASOUND INTEGRATION INTO CRITICAL CARE
FELLOWSHIP
Abbas Ali1, Karen Korzick1, Angela Miller1, Luis Urrutia1, Robert Strony1;
1
GMC, Danville, PA
Learning Objectives: It is essential to create a conducive environment for establishment of a curriculum for Critical care echocardiography and ultrasound (US).
Training of intensivists in practice is a major facilitator to reach this goal. Methods: We integrated an echocardiography and critical care US curriculum into
our critical care and pulmonary/critical care fellowships. During the two years
of fellowship we have a dedicated three months echocardiography rotation, the
first month is spent in the echo lab and the other two months in the ICU under
supervision of intensivists with advanced training in echocardiography. The fellow performs an independent echocardiography examination on all patients on
whom an official echocardiography examination is requested. The images captured by the fellow are compared with the official ones and a target of 90% agreement is required to approve the exam. In a two year period the fellow is required
to perform at least 150 examinations and interpret additional 150 studies To
reach this goal we have established a 6 monthly echocardiography and critical
care US course to train the intensivists and mid-levels in practice. The training involved 16 hours didactic lectures and hands on training on live models.
The topics covered include handling the ultrasound machine, echocardiography,
lung, pleural, vascular and FAST exams. The candidates were trained in how to
obtain echocardioraphy standard views, identification of pleural slide, lung A and
B lines. Identification of four points for FAST exam and vascular access Results:
A total of 26 candidates were enrolled in July two day courses. A pre and post
test was performed. The change in pre to post scores was significant (p<0.0001).
The average change was an increase of 4.23 points (95% CI: 2.92, 5.54). One
fellow completed the two years and his echocardiography skills are comparable
to certified echocardiographers Conclusions: Training of intensivists in practice
will create a conducive environment for integration of echocardiography and US
into critical care fellowship. A certifying echocardiography examination is needed
Poster Session: Education 4
316
ICU ROUNDS AND MENTAL FATIGUE
Matthew Friedman1, Christine Park2, Mary McBride3; 1Ann & Robert H Lurie
Children’s Hospital of Chicago, Chicago, IL, 2Northwestern Memorial Hospital,
Chicago, IL, 3Ann and Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL
Learning Objectives: Medical decision-making in the ICU is difficult due to the
acuity, complexity, distractions and temporal pressures inherent to the ICU. Mental fatigue, ego depletion and decision fatigue are phenomena that describe impairment in cognitive work after previously engaging in other executive processes.
Individuals who perform acts of self-control, decision-making or problem-solving
later show increased bias, decreased persistence, poorer self-control and poorer
cognitive function. Emergency room physicians have been shown to be susceptible
to these phenomena. The hypothesis is that rounds induce mental fatigue, manifested on cognitive tasks after rounds, compared to prior to rounds Methods: This
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
is a prospective study of pediatric residents during their ICU rotation. Two tests,
the Cognitive Estimation Test (CET) and the Repeatable Episodic Memory Test
(REMT), will be given before and after rounds. CET scores and the total words
recalled on REMT are the main outcomes. After rounds, the participants will
complete a subjective workload survey. A paired t-test will be used to evaluate for
difference between pre and post rounding testing. Pearson correlation coefficient
will be used to test for correlation between variables. Results: To date 18 subjects
have been enrolled, toward a goal of 30. There are no significant differences in the
main outcomes. On the REMT, subjects recalled less words after rounds compared
to before, 30.8 vs 31.9. (p=0.1) There is a nonsignificant decrease in CET scores
after rounds, 4.3 vs 4.7. (p=0.27) The total number of intrusions, or falsely recalled
words, on the REMT is 0.7 before and 1.2 after rounds (p=0.07). Performance on
tests was not correlated with any of the subjective or objective measures of workload. Conclusions: At this point, there are no statistically significant differences in
cognitive performance suggesting that residents have an ability to maintain good
executive function despite engaging in the mentally taxing process of rounds. The
number of falsely recalled words is near significance at partial enrollment, which is
a connection previously established.
317
INTRODUCTION OF A DEGREE COURSE IN CRITICAL CARE
FOR UNDERGRADUATE MEDICAL STUDENTS
John Kinsella1, Tara Quasim2; 1University of Glasgow, Glasgow Scotland, United
Kingdom, 2University of Glasgow, Glasgow, United Kingdom
Learning Objectives: In the UK medical students are not required to undertake
a primary university degree prior to entering medical school. Many universities
in the UK offer the opportunity to extend the course by one year in order to
undertake a science degree (intercalated BSc). As critical care is an expanding
specialty we hypothesized that an intercalated BSc.Med.Sci in Critical Care and
Perioperative medicine would be a popular and successful innovation. Methods:
A specialist critical care and perioperative medicine BSc course curriculum was
devised and approved, with teaching of physiology and pharmacology at the level
expected for postgraduate exams. The course was designed as an option in the
intercalated degree for Glasgow medical students and started in 2012. The course
provided 30 credits for the core medical sciences, 20 credits for statistics, 30 credits for the specialist course and 40 credits for a research project. The research project supervisors created projects which were related to the current research themes
of the academic department. The total number of student places was limited to
8. Results: The course is now in its 3rd year. In each year it has been heavily
oversubscribed and it has been the most popular option. In the first year, 4 students gained First Class Honors and 4 gained 2:1s. In year 2, 6 students gained
Firsts. The majority of students have now presented at national or international
meetings and several have published in peer-reviewed journals. Conclusions: An
undergraduate degree course in critical care has proven to be very popular. It
attracts the highest caliber of students and the performance of the students is
excellent. There was an unmet need for a specialized degree in critical care. The
future career choices of these students and their career progression will be studied.
318
COLLABORATIVE TEACHING OF MEDICAL AND NURSING
STUDENTS IN ACUTE CARDIAC ARREST SIMULATION
Dave Milzman1, michelle dugan2, Wendy Thompson3; 1N/A, Washington, DC,
2
Georgetown U School of Medicine, washington, DC, 3Georgetown U School of
Nursing, Washington, DC
Learning Objectives: The importance of effective collaboration among health
care professionals from each specialty field is fundamental to successful patient
care. When contributions from both nurses and physicians are well coordinated,
the individual patient benefits from the communication. The objective of this
study is to evaluate the experiences of both medical and nursing students after
joint collaboration in a simulated cardiac arrest scenario. It is anticipated that
constructive communication between health care professionals with different
specialty training will enhance patient care and safety, as well as foster cost savings and less overlap of services. Nursing and medical students have minimal
experience learning in an interprofessional environment, without initial communication until much later in their careers. With early exposure to team-oriented
professional training, students will gain a deeper understanding of the roles
required of themselves and their colleagues. Methods: Both medical and nursing students were exposed to a cardiac arrest educational model in a simulated
environment, and then completed a survey of their experiences before and after
the simulation. Any student with significant prior experience or a prior degree
in health care was excluded. Results: A total of 55 medical and 42 senior nursing students were included in the cardiac arrest training simulation. Pre =event
confidence in success was moderate with mean 3.5 on 5 point likert scale by
med students and 3.2 by nursing students with noted success of program, with
increased numbers at completion; 4.8 and 4.9, respectively, (p<0.01). After the
simulation was completed, students documented an increased understanding of
the benefits of interprofessional education. They also felt more positive about
their collaboration and problem solving skills. Conclusions: Interprofessional
education between nursing and medical students fosters important principles in
effective collaboration for high quality patient care. Students showed improved
skills and positive attitudes after training in this education model.
319
ASSESSING PARENT UNDERSTANDING OF THE “ASTHMA
ACTION PLAN” EDUCATION USING INTERACTIVE MOBILE
APP.
Renuka Mehta1, Kyle Johnsen2, Edwin Perry3; 1Medical College of Georgia at
Georgia Regents University, Augusta, GA, 2University of Georgia, Athens, GA,
3
Medical College of Georgia, Augusta, GA
Learning Objectives: Asthma is a preventable illness affecting nearly 7 million
children/year. The education given to parents via “Asthma Action Plan (AAP)”
introduced in 2008 had very little effect in decreasing rate of admission. Ineffective communication between healthcare Providers (HCPs) and parents may
be one the factor contributing factor. Improvements in communication between
parents and their child’s HCPs could lead to better understanding of treatment
plans, prevention, and management of their health. We recently developed Virtual patient interactive tool and took several measures to improve communications between parents and HCPs. However, we have not addressed how much
information is retained by the parents after they receive education on AAP. Active
interaction in comparison to passive teaching may retain more information.
Computer-based interactive Apps have been recently evolving. The aim of this
tool is to look into enhancing parent-patient understanding of AAP using teach
back method and interactive communication tools. Methods: AAP is a specific
educational tool and written document for parents of children with asthma. And
follow the instructions for their child’s daily asthma care at home. The current
AAP was modified using appropriate Health Literacy principles making it simpler
for parents to understand. 13 questions were created for the mobile App using
the Unity3D game engine, which could run on web or mobile device and would
provide assessment and feedback to parents in real time at the point of care or
at home. A sequence of slides, containing question and multiple choice answers,
with audio and visual component. The correct answer is presented with feedback.
Parents can only move to the next question after they have answered it correctly.
Each sessions log into a remotely accessible database for the analysis. Results:
This App will be implemented this fall to the parents who children are seen in
hospital with asthma. Conclusions: This intervention is expected to have positive
affect in improving care of children with asthma. This app will be accessible to the
largest audience in future
320
ACCIDENT PREVENTION AND FIRST AID KNOWLEDGE
AMONG PRESCHOOL CHILDREN’S PARENTS
Balint Banfai1, Emese Pek1, Krisztine Deutsch1, Balázs Radnai1, Jozsef Betlehem1;
1
University of Pecs Faculty of Health Sciences Inst of Emerg Care and Health
Ped, Pecs, Hungary
Learning Objectives: Based on international and national health statistics, accidents from various mechanisms are among the most common causes of death
which affect children seriously. Our aim was to examine the first aid and accident prevention knowledge and attitude of the parents. In this study parents
of 3-7 years old children were involved in six kindergarten located in Hungary
Methods: A self-fill-in questionnaire applying standardized items was used to collect data. In the investigation 307 parents (N=307) were included. Out of them
234 persons filled out the questionnaire correctly (n=234). The statistical analysis
was made with SPSS 20.0 statistical software. For analyses descriptive statistics,
Chi-square-test and ANOVA were used. Results:Three-quarter of the children
have suffered at least one accident in his past life (74.3%). Most of the accidents
occurred at home (88.5%). 174 parents attended first aid course earlier (74.4%),
the previous knowledge is based mainly on the driving license (81.6%). Based
on parents’ answers there is a need for teaching first aid (70.5%) and accident
prevention (89.7%) to children in the kindergarten. There were only 10 parents,
who answered all the featured first aid situations correctly (4.3%). Between the
subjective judgment of the financial status and the correct answers we found a
significant correlation (p=0.03). The previously accomplished first aid training
(p<0.05) and the educational attainment (p=0.029) had a positive impact on the
correct answers. Conclusions: The level of first aid knowledge among kindergarten children’s parents is lower than expected. With an offer to participate in a first
aid course the level of knowledge on both sides (children and parents) could be
increased. This could contribute to a better and more effective accident prevention and first aid practice among parents.
321
QUALITY OF YOUTUBE VIDEOS ON CENTRAL LINE
PLACEMENT
Oveys Mansuri1, Grace Chang2, Brittany England1, Kelly Fenn1; 1University of
Nebraska Medical Center, Omaha, NE, 2Advocate Good Samaritan Medical
Center, Downers Grove, IL
Learning Objectives: Central line placement is a common procedure in various clinical situations. There has been an increased focus on the methods used
to teach this procedural skill. We examine the role of YouTube as one common
resource used by trainees to review clinical procedures. Methods: The YouTube
site was queried using multiple search terms related to central line placement. The
results were filtered by views and screened for duplicates and series. Videos were
reviewed for key demographic data points. Two independent clinical reviewers
then scored all the videos for Usefulness (US: 3 to -1), Quality (QV: 5 to 1), and
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Sterile Technique (ST: 3 to -1). Statistical analysis was then done on the demographic data video ratings. Results: There were 24 unique videos or video series
that had at least 100 views in aggregate. These were posted from 2006 through
2014. The average number of views for each individual video was 45345.2, and
the average video length was 7:24. Location of central line placement were broken down as 57.1% IJ, 23.8% femoral, and 19.1% subclavian. 26.7% had no
formal institutional affiliation, where 73.3% did. 54.5% videos used at least a live
person versus 45.5% that used a mannequin or simulation. The comments for
videos ranged from some with no comments, to a maximum of 152 comments
for one video in particular, the average was about 12 comments per video. The
average and median US score was 2.235 and 2.5, average and median QV score
was 3.43 and 3.5, and average and median ST score was 2.34 and 2.8. The videos
using mannequin or simulation scored better in all three scoring areas versus
those that used live persons. Videos with institutional affiliations scored better
in QV and ST, and were about the same for US when compared to those videos
without institutional affiliation. Conclusions: There is a broad range of videos
with varying usefulness and quality of video. The characteristics of the video do
impact US, QV, and ST scores. Further research is necessary to determine the
utility of YouTube as a repository for critical care procedural videos.
322
EVALUATING PALLIATIVE CARE EDUCATION IN PEDIATRIC
CRITICAL CARE TRAINING PROGRAMS
Arun Singh1,2, Jeffrey Klick3, Courtney McCracken4, Kiran Hebbar5,2; 1Children’s
Healthcare of Atlanta, Atlanta, GA, 2Emory University School of Medicine,
Atlanta, GA, 3Children’s Healthcare of Atlanta - Egleston Campus, Atlanta, GA,
4
Emory University, Atlanta, GA, 5Egleston Children’S Hospital, Atlanta, GA
Learning Objectives: In 2009, the ACGME recognized the importance of
palliative care (PC) medicine and emphasized that pediatric trainees be taught
the “impact of chronic disease, terminal conditions and death on patients and
their families”. We aim to assess current PC education in pediatric critical care
medicine (PCCM) training programs. We hypothesize there is a continued deficit of formalized PC education in PCCM training. Methods: We surveyed 64
PCCM fellowship program directors (PD) using Research Electronic Data Capture (REDCap) software. The survey consisted of 3 sections in which PCCM
PDs were asked about their background, current practices and perceptions/
evaluation of PC education. Results: 29 out of 64 (45.3%) surveyed PCCM
PDs responded. 26 of 29 (90%) PCCM PDs reported the presence of a multidisciplinary PC team in their institution, and 17.2% report PCCM physicians
who received additional years of PC training. 13 of 29 (45%) PDs reported the
availability of a formal PC curriculum and 5 (17%) reported that PC rotations
are available to trainees. Of those, 4/5 stated that the PC rotation was offered as
an elective. 100% of programs that lack a PC rotation (n = 24) report that one
was never previously in place. The most common reason for the lack of a PC rotation was that one had never been established, followed by lack of funding, faculty
& trainee interest. The majority of PCCM PDs felt that a formal PC curriculum
would enhance trainees’ general ability to care for any patient (74.1%), enhance
their expertise (88.9%) and comfort levels (84.6%) with dying patients and their
families, establishing goals of care (81.5%) and communication skills (92.3%).
Overall, 82% of PCCM PDs felt that a PC rotation would enhance their trainees’
education. Conclusions: While a significant number acknowledge the benefits
of formalized PC education, there remains a paucity of PC curriculum and formal rotations. Barriers to formalized PC education are trainee’s time restraints,
funding, lack of interest from trainees and faculty, but not from lack of teaching
opportunities or availability of PC providers.
323
KNOWLEDGE AND SKILL GAPS IN HIGH QUALITY CPR ARE
PREVALENT IN THE PEDIATRIC INTENSIVE CARE UNIT
Robert Bishop1, Tensing Maa2; 1Nationwide Children’s Hospital At Ohio State
University, Columbus, OH, 2Nationwide Children’s Hospital, Columbus, OH
Learning Objectives: There is variability in the quality of cardiopulmonary
resuscitation (CPR) in children, but real-time feedback can improve adherence
to current guidelines. Patient outcomes can be improved by performance of
high quality CPR. The purpose of this study was to collect baseline performance
data for our pediatric intensive care unit (PICU). We hypothesized that PICU
staff would have poor retention of and be unable to demonstrate high quality
CPR metrics during a two-minute interval of CPR without feedback. Methods:
PICU staff who may perform CPR during an arrest were invited to participate
in a multiple-choice quiz and CPR challenge. Staff performed two minutes of
CPR without feedback on a manikin and then again, using a defibrillator with
audiovisual feedback. A CPR sensor measured rate, depth and recoil. CPR was
considered in range if depth was at least 2 inches, rate 100-120 per minute and
full recoil between compressions. The number of providers able to maintain CPR
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
in target range for >70% of 2 minutes without/with audiovisual feedback was
analyzed by Fisher’s exact test. Results: 63 staff members participated in the CPR
challenge (36 RN, 12 MD, 8 PharmD, and 7 RT). Incorrect knowledge of adequate compression depth and ventilation rates including pediatric compression to
ventilation ratios was common at baseline across disciplines: % correct answers:
MD: 81%, RN: 65%, RT: 78%, PharmD: 57%. Only 31% of RNs performed
CPR in range without feedback, compared to 97% with feedback (p<0.0001).
75% of physicians performed CPR in range without feedback and 92% with
feedback (p=0.59). Pharmacists and RTs improved from 13% and 14% respectively to both 100% with feedback (p = 0.001 & p=0.005). Conclusions: Gaps
in knowledge and skill in performing high quality CPR exist in our PICU. This
deficit is most pronounced amongst nurses, the most frequent CPR provider in
our unit. CPR feedback can greatly improve adherence to quality CPR metrics.
Future quality improvement interventions in our PICU should focus on training
nursing staff to use CPR feedback devices during real cardiac arrests.
324
TRANSITION TO FIRST JOB: AN IN TRAINING SECTION
RESEARCH SURVEY
Laura Watkins1, Krzysztof Laudanski2; 1Cohen Childrens Medical Center, New
Hyde Park, NY, 2University of Pennsylvania, Philadelphia, PA
Learning Objectives: We evaluated the subjective feeling of preparedness and the
needs of the current Trainees and recent Graduates from Critical Care Training
in regards to first employment. Methods: A web accessible survey was deployed
by the Society of Critical Care Medicine In training Section, made available by
email. The study population included In Training Members of SCCM, along
with any SCCM member who is currently a trainee or graduated from a Critical Care Training Program within the previous 3 years. Results: We surveyed
approximately 3000 members, with a final response number of 180 (6%). 160
(89%) responders were physicians, 125 (69%) were currently In Training. The
majority of responders (64%) trained in Critical Care Internal Medicine or Pediatrics. 67% had recently interviewed for a job. Northeast was the preferred location (85 responders) and academia was favored over private practice (80% vs
15%). The sources most often used were direct contact, word of mouth or suggestions offered by mentor/Program Director. 62% of interviewees felt prepared
for the interviewing process. 69% felt prepared to build an adequate job portfolio
but only 34% received formal guidance from mentor/training program. Only
42% describe their training program facilitating building the resume during the
training period. 57% and respectively 53% received guidance from the mentor/
training program in searching for or deciding what position to choose. Of all
responders, 89% agreed it is important to participate in a formal training course
in job search, portfolio development and details of the interviewing process. The
preferred sources of training were equally distributed between home institution
courses, webinars and courses at the SCCM Congress. Conclusions: Young Critical Care Professionals describe a need in education regarding first employment.
The Society of Critical Care Medicine is ideally situated to respond to this need
by courses offered at the Annual Congress, Webinar dissemination and working
with Program Directors in creating local courses.
325
ARE RESIDENTS PREPARED TO ENTER THE “REAL
WORLD”?: SURVEYING BOTH ATTENDING AND RESIDENT
VIEWPOINTS.
Amanda Celii1, Alisa Cross2; 1Allegheny General Hospital, Pittsburgh, PA,
2
Allegheny General Hospital, N/A
Learning Objectives: The purpose of this project was to survey attending physicians and general surgery residents to better understand current viewpoints regarding surgery training programs since the 80 hour work week was implemented over
10 years ago. Methods: Participation in this study required answering an anonymous short online survey which consisted of about 60 questions. These surveys
were then distributed via an email with a link to the survey on Survey Monkey.
Potential respondents were from: Allegheny General Hospital and Emory University. Following the initial email, a reminder email and a ‘final request to participate’
email was sent at approximately 21 days; the survey closed approximately 4 weeks
after initial email. Results: Responses from 40 attending physicians and 30 residents from two institutions were analyzed. There was a 53% response rate from
the attendings at AGH and a 47% response rate from the residents at AGH. Out
of the 58 questions asked there was a statistically significant difference between
attending and resident responses regarding post graduation preparedness, reasons
for pursuing a fellowship, work hour restrictions, reasons for staying over hours,
effects of the hour restrictions, OR preparedness/experience, free time, and case
volume. Conclusions: The training for general surgery has changed significantly
over that last 10 years. More and more general surgery residents are pursuing fellowship opportunities; however we have also found ourselves in a time of increased
need for general surgeons. In order to make up for the 6 to 12 months of time
that has been purposed is now lost with the 80 hour work restriction; we find our
residents training more through simulations, online modules, and “self-directed”
learning. Whether this can make up for actual experience is still being determined,
as we are searching for more ways to increase our educational experience without
violating our hours. The perception is that more residents are choosing to enter
fellowship in order to gain this experience that is now lacking in residency, as the
confidence in their clinical and operative ski
Poster Session: Endocrine/Nutrition 1
326
THE EFFECT OF GUT-ORIENTED COMPREHENSIVE NUTRITIONAL THERAPY ON NOSOCOMIAL INFECTIONS.
Takeaki Sato1, Shigeki Kushimoto2; 1Tohoku University Hospital Emergency
Center, Sendai-shi, Japan, 2Tohoku University Hospital Emergency Center,
Sendai-city, Japan
Learning Objectives: The “normal flora” of the intestinal tract responsible for
protecting the body from infection can be disturbed by the therapeutic administration of antibiotics, resulting in nosocomial infections including Clostridium
difficile-associated diarrhea (CDAD) and multi-drug resistant Pseudomonas
(MDRP) infections. We evaluated the effect of gut-oriented comprehensive
nutritional therapy on the detection rates of CDAD and MDRP and physiological severity. Methods: We established the original protocols for comprehensive
nutritional support in 2010. The protocols were designed based on up-to-date
guidelines and a gut-oriented strategy, primarily focused on controlling diarrhea.
The principal components of each protocol include avoiding fasting, enhancing
enteral feeding, prophylactic administration of synbiotics, diarrhea monitoring,
and the restriction of obstipation, irritating laxatives and antacid agents, in addition to the restricted use of broad spectrum antibiotics. Patient characteristics
and endpoint parameters were compared between the pre-protocol cohort (20082009, 794 patients) and the post-protocol cohort (2010-2012, 1633 patients).
Results: There were no differences in patient characteristics, including age, sex,
comorbidities, APACHEII and SOFA scores between the two groups. In the
post-protocol cohort, the mean length of ICU stay and duration of mechanical
ventilation significantly reduced (15.0 to 12.0 days, p=0.002; 7.7 to 5.6 days,
p=0.013, respectively) compared to the pre-protocol cohort. The incidences of
CDAD and MDRP were also reduced (31 cases/2 years versus 3 cases/3 years;
46 times/2 years to 3 times/3 years, respectively). Moreover, the frequency of
MDRP detected in the entire hospital reduced in parallel with that detected in
the ICU (R=0.950, p=0.004). Conclusions: Gut-oriented comprehensive nutritional support, particularly focused on the management of diarrhea, may reduce
the incidence of CDAD and MDRP detection and the duration of mechanical
ventilation and ICU stay.
327
IMPLEMENTATION OF AN AGGRESSIVE ENTERAL NUTRITION PROTOCOL AND THE EFFECT ON CLINICAL
OUTCOMES
Daniel Yeh1, Catrina Cropano1, Sadeq Quraishi1, Eva Fuentes1, Haytham Kaafarani1, Jarone Lee1, Yuchiao Chang1, George Velmahos1; 1Massachusetts General
Hospital, Boston, MA
Learning Objectives: Macronutrient deficiency in critical illness is associated
with suboptimal clinical outcomes. We hypothesized that an aggressive enteral
nutrition (EN) protocol would be associated with higher calorie as well as protein
delivery and a lower risk of late infections in surgical ICU patients. Methods: We
enrolled adult surgical ICU patients who received >72 h of EN from 09/201305/2014. Our intervention consisted of increasing protein prescription targets
(2.0-2.5 vs. 1.5-2.0 g/Kg/day) and implementing compensatory feeds around the
time of EN interruption. We compared the intervention group to historical controls. To test the association of EN protocol with the risk of late infections (defined
as >96 h after ICU admission), we performed a logistic regression analysis, while
controlling for plausible confounders including, age, sex, body mass index (BMI),
acute physiology and chronic health evaluation (APACHE) II score, exposure to
gastrointestinal surgery, and ICU length of stay. Results: There was no difference in age, sex, BMI, admission category, or Injury Severity Score between the
intervention (n=119) and control groups (n=94). Mean APACHE II score was
higher in the intervention group (17 ± 8 vs. 14 ± 6, p=0.002). The aggressive EN
group received more calories (19 ± 5 vs. 17 ± 6 kcal/kg/day, p=0.005) and protein
(1.2 ± 0.4 vs. 0.8 ± 0.3 g/kg/day, p<.001); received higher percentage of prescribed
calories (77% vs. 68%, p<.001) and protein (93% vs. 64%, p<.001); and accumulated lower overall protein deficit (123 ± 282 vs. 297 ± 233 g, p<.001), when
compared to controls. The aggressive EN protocol was associated with a lower
risk of late infection [adjusted odds ratio 0.34 (95%CI 0.14-0.83)]. Conclusions: In our cohort of surgical ICU patients, implementation of an aggressive
EN protocol was associated with greater macronutrient delivery and lower risk of
late infections. Randomized, controlled trials are required to determine whether
aggressive feeding protocols improve outcomes in surgical ICU patients.
328
A COMPARISON OF BOLUS VERSUS CONTINUOUS FEEDING
METHODS IN MECHANICALLY VENTILATED CHILDREN
Ann-Marie Brown1; 1Akron Children’s Hospital, Akron, OH
Learning Objectives: Malnutrition increases the risk of mortality and morbidity in the Pediatric Intensive Care Unit (PICU). Barriers to adequate delivery of
enteral nutrition (EN) include hemodynamic instability, feeding interruptions,
feeding intolerance and lack of standardized feeding protocols. The purpose of
this study was to compare the effect of two gastric feeding methods, continuous
(C-GF) versus bolus (B-GF), on nutritional goals and feeding interruptions in
mechanically ventilated patients. We hypothesized that EN in intubated children
would be increased using B-GF compared to C-GF with a comparable safety
profile. Methods: This prospective, randomized, controlled comparative effectiveness study included ages 1m corrected gestational age - 12y intubated within
24h and started EN within 48h of admission. Subjects were randomized to C-GF
or B-GF. EN volume was advanced in a weight-based manner every 3h to target volume; Caloric density was increased every 12h to target. Feeding intolerance (emesis, elevated gastric residual volumes (GRV) x 2, or elevated GRV x1
plus elevated abdominal girth (AG) was assessed every 3h. Lung injury acuity
was measured every 3h using the Oxygen Saturation Index (OSI). All feeding
interruptions were recorded. Significance was defined p<0.05. Results: Twentyfive subjects (B-GF = 11) were enrolled. There were no demographic or severity
of illness differences between groups. The B-GF group attained higher energy
(p=.001) and protein (p=.006) intake in the first 24h compared to the C-GF;
there was no difference at 48h. Though not significant, the B-GF group reached
goal EN volume faster (median 15h vs 29.5h p=1.00). No relationship was identified between emesis, GRV or AG; few interruptions were recorded in either
group. No aspiration events or difference in OSI was noted between the groups
(p=0.866). Conclusions: B-GF enhanced delivery of EN intake with a comparable safety profile when compared to C-GF. Further study is needed to compare
both EN methods in other PICU populations.
329
COMPARISON OF INSULIN INFUSION METHODS IN CRITICALLY ILL PATIENTS: BASAL/BOLUS AND MULTIPLIER
Carrie Zechmeister1, Amanda Fesko2, Rachel Leis3, Deidre Rohaley3; 1Spectrum
Health, Grand Rapids, MI, 2University of Findlay, Findlay, OH, 3Mercy St. Vincent Medical Center, Toledo, OH
Learning Objectives: Glycemic control remains a difficult issue in critically
ill patients. Although numerous insulin infusion protocols are available, there
exists a paucity of studies comparing different methods. This study aimed to
demonstrate that an insulin multiplier based protocol is safe and efficacious
when compared to a basal/bolus infusion method in critically ill patients with
a target blood glucose (BG) of 140-180 mg/dL. Methods: This retrospective,
observational before and after study evaluated adult intensive care unit (ICU)
patients admitted to a 450 bed Level 1 tertiary care center with at least six
hours of continuous intravenous insulin. Two time frames were studied: the
pre-implementation group (May 2013 to October 2013) utilized a basal/bolus
infusion method, and the post-implementation group (November 2013 to February 2014) utilized a multiplier method. Categorical variables were described
using frequency distributions and continuous variables as means with standard
deviations. Multivariate analysis was conducted to adjust for confounding variables. Results: A total of 52 patients (31 basal/bolus and 21 multiplier) were
included. Crude analysis showed a decreased time to goal BG in the multiplier
group (4.1 versus 6.1 hours, P = 0.0016). This effect persisted after adjustment for potential confounding variables. No differences existed for average
insulin infusion rate (5.1 units/hour for basal/bolus versus 5.7 units/hour for
multiplier, P = 0.50) or percent time in goal range (42.6% for basal/bolus versus 50.7% for multiplier, P = 0.23). Hypoglycemic episodes (including severe
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
hypoglycemia) were infrequent and similar between both groups. Additionally
ICU length of stay, hospital length of stay, and discharge disposition did not
differ. Conclusions: The multiplier method is safe and efficacious for insulin infusions when targeting a goal BG of 140-180 mg/dL which resulted in a
quicker time to goal BG in the study population. Further studies are needed to
continue to assess safety data.
330
INSULIN GLARGINE COMPARED TO INSULIN NPH FOR
THE MANAGEMENT OF HYPERGLYCEMIA IN THE CRITICALLY ILL
Joseph Trang1, Marlena Fox1, Valerie Danesh1, Timothy Jones1; 1Orlando Health,
Orlando, FL
Learning Objectives: Insulin glargine and insulin NPH are both routinely utilized in the management of hyperglycemia in critically ill patients. Currently,
there is no safety or efficacy data to support the use of one agent over the
other. Methods: Critically ill adult patients admitted to the Intensive Care
Unit (ICU) requiring long-acting insulin for management of hyperglycemia
were prospectively identified. Outcomes were compared between patients who
received insulin glargine and insulin NPH. Safety was evaluated by comparing hypoglycemic (blood glucose (BG) <70 mg/dL) and severe hypoglycemic
(BG <40 mg/dL) episodes. Efficacy (BG <180 mg/dL) was evaluated with mean
BG readings, percentage of BG readings > 180 mg/dL, and 24 hour sliding
scale insulin (SSI) requirements. Data was recorded until long-acting insulin
was discontinued, patient transferred out of the ICU, or for up to 14 days
following insulin initiation, whichever occurred first. Data was reported as
median (IQR). Pearson’s chi-square and Mann Whitney U tests were utilized
for dichotomous and continuous data, respectively. Results: Demographics
were similar between insulin glargine (N=97) and insulin NPH (N=65) groups,
including age, history of diabetes, and reason for ICU admission. Results show
no difference in number of patients with hypoglycemic episodes [glargine=25,
NPH=24; p=0.548] and no difference in number of patients with severe hypoglycemia [glargine=3, NPH=5; p=0.332]. The glargine group had similar mean
BG readings [163(147-189) vs 156(142-178); p=0.468] and percent of BG
readings >180 mg/dL [36(18-55) vs 29(17-44); p=0.367] as the NPH group.
The daily SSI requirements were similar [14(6-22) vs 8(5-24); p=0.352 between
the glargine and NPH groups, respectively. There was no difference in ICU or
hospital length of stay. Conclusions: Results suggest insulin glargine and insulin NPH are equally safe and effective for the management of hyperglycemia
in the critically ill.
331
ROUTE OF NUTRITIONAL SUPPORT AFFECTS METABOLIC
OUTCOMES IN AN ENDOTOXEMIA MODEL OF SEPSIS
Faraaz Shah1, Srikanth Singamsetty1, Sherie McDonald1, Lanping Guo1, Brett
O’Donnell1, Christopher O’Donnell1, Bryan McVerry1; 1University of Pittsburgh
Medical Center, Pittsburgh, United States
Learning Objectives: Sepsis is common in critically ill patients and the development of hyperglycemia during sepsis is associated with increased morbidity
and mortality. Critically ill patients receive nutritional support in intravenous
dextrose infusions and in enteral tube feeds but the effects of these interventions on metabolic function in sepsis are unknown. Methods: 10 week old
C57/BL6 mice (n=64) were randomized to (1) surgical implantation of either
gastric cannula for enteral or venous catheter for parenteral infusions, (2) lipopolysaccharide (LPS) challenge (1mg/kg) or vehicle, and (3) saline (100uL/
hr) or dextrose infusion (equivalent to 10% daily caloric needs) immediately
following septic insult. Frequently sampled intravenous glucose tolerance test
(FSIVGTT) was performed five hours after LPS to assess metabolic function.
Results: Control (vehicle) mice receiving saline by either enteral or parenteral
routes exhibited normal glucose disposal and insulin response with return to
baseline in 20 minutes during FSIVGTT. Mice in saline-LPS groups demonstrated mild hypoglycemia prior to and higher peak insulin secretion during FSIVGTT but similar glucose tolerance compared to controls. Mice in
vehicle-dextrose groups, by both enteral and parenteral routes, also maintained
normal glucose tolerance. Mice receiving parenteral dextrose and LPS demonstrated profound glucose intolerance with blood sugars reaching over 600 mg/
dL, inappropriately low insulin secretion, and marked insulin resistance during FSIVGTT. In contrast, mice receiving enteral dextrose and LPS demonstrated normal glucose disposal and insulin secretion similar to control mice.
Conclusions: While parenteral dextrose induces severe metabolic dysfunction
in endotoxemic mice, enteral dextrose administration does not compromise
glucose disposal or insulin secretion. Further studies will determine the role of
gut derived insulin secreting and sensitizing hormones in mediating improved
glycemic control.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
332
ENTERAL NUTRITION ADMINISTRATION IN THE ICU:
ACHIEVING GOALS WITH BETTER STRATEGIES
Roopa Kohli-Seth1,2, Sara Wilson1, Bridget Twohig3, Ylaine Aldeguer1, John Oropello2,1, Anthony Manasia1,2, Adel Bassily-Marcus1,2; 1Mount Sinai Hospital, New
York, NY, 2Icahn School of Medicine at Mount Sinai, New York, NY, 3Mount
Sinai Hospital, NY, NY
Learning Objectives: Nutrition support is a key element of managing ICU patients.
Enteral nutrition (EN) is preferred over parenteral, as it maintains GI integrity and
attenuates the inflammatory response. Despite these benefits, providing adequate
nutrition is a challenge. The goal of this study is to asses whether a feeding protocol
improves time to goal rate and administration of nutrients to patients. Methods:
With IRB approval adult patients who received EN support in the SICU from July 1,
2012 - June 30, 2013 were screened for inclusion. An EN protocol was implemented
on January 1, 2013 with the pre period defined as six months preceding implementation and the post period six months after. Patients who received feeds for less than 24
hours or were on EN support prior to ICU admission, were excluded. Patients whose
EN was discontinued within 48 hours of initiation due to procedure, complication,
poor prognosis or withdrawal of care, were also excluded. A retrospective chart review
was completed and data analyzed to determine how quickly goal rate was achieved
and whether feeds met the daily volume recommended. Results: 624 charts were
screened, 150 of which had orders for EN support. A total of 38 were excluded,
leaving 112 (57 pre, 55 post) patients. Seventy three patients did not reach goal (41
pre, 32 post). For patients that met goal a Kaplan-Meier curve was calculated for
the overall time, which was significantly shorter in the post period compared to the
pre, as confirmed by the log rank test (p=0.01). A significantly higher mean percent
of daily volume was achieved in the post period for days two (51.2% versus 42.1%,
p=0.0003) and three (55.9% versus 42%, p=0.04) of EN administration. Conclusions: The benefits of nutrition support in the treatment of ICU patients are well
known. Enteral feeding protocols aim to guide practitioners on the appropriate timing of initiation and quick advancement to goal rate. This study shows that use of a
protocol for provision of EN facilitates shorter duration of time to attain goal rate and
can result in an increase in overall administration of nutrition to patients.
333
NUTRITION PRACTICE PATTERNS IN ADULT ECMO
PATIENTS: RESULTS OF AN INTERNATIONAL SURVEY
Veena Nandwani1, Amanda Tauber1, Paul McCarthy1, Daniel Herr1; 1University
of Maryland Medical Center, Baltimore, MD
Learning Objectives: Nutritional support in critically ill patients is essential and
guidelines do exist, however, there is no consensus for adult patients on extracorporeal membrane oxygenation (ECMO). Current Extracorporeal Life Support Organization (ELSO) guidelines recommend full caloric and protein support but offer
no specifics on practice. This survey was done to examine practice patterns to help
identify areas for future study. Methods: We emailed a survey pertaining to nutritional support practice patterns in this patient population to the directors of ELSO
centers worldwide. We analyzed data from centers caring for adults. Results: We had
a 28% response rate. 50% of the respondents were from North America and 25%
from Europe. The rest were from Asia, Australia/New Zealand, and South America.
Most care for a diverse adult ECMO population including respiratory, cardiac, and
ECPR. Most U.S. centers perform fewer than 50 cases/year, while European and
Australian perform more. Post pyloric is the preferred enteral route in the U.S. while
gastric is preferred elsewhere. U.S. centers initiate feeding later than other countries.
Most measure gastric residual volumes (GRV) and hold enteral feeds for GRV of 250
to 450ml. In the U.S. patients on vasoactive agents are fed via small bowel vs. gastric
in other countries. Standard enteral feeds are the most common type of tube feeding
worldwide. Nutritional status is assessed primarily by pre-albumin in the U.S. vs.
Subjective Global Assessment (SGA) in Europe, Asia, Australia. Most use ideal body
weight to assess patients’ kcal needs. Europe, Asia, South America target a goal of 20
to 25kcal/kg while the U.S. and Australia target 25 to 30kcal/kg. Protein goals were
lower in Europe and Australia. Conclusions: There are differences among centers in
nutritional support practice patterns for adult ECMO patients. Non - US centers
tend to manage more ECMO cases than US centers. Non - US centers feed earlier,
use SGA to assess nutritional status, favor gastric feeding and have different nutritional goals. Further study of nutrition support in ECMO patients is warranted.
334
EVALUATION OF A BASAL–BOLUS INSULIN PROTOCOL
FOR CONTINUING DOSING EFFICACY AND SAFETY
OPTIMIZATION
Maureen Greene1; 1Wheaton Franciscan Healthcare-St Joseph, Milwaukee, WI
Learning Objectives: Approximately one third of all patients admitted to the hospital
have hyperglycemia. Glycemic control has been linked to fewer infections, decreased
length of stay, improved mortality and cost-savings. Studies have shown Basal Bolus
Insulin (BBI) dosing better reflects natural human insulin release levels throughout
the day and leads to better control with decrease hyper/hypoglycemic events. In
response to clinical guidelines developed by AACE in 2009, a clinical pilot test of a
weight-based BBI protocol was developed for use in hospitalized patients at the time
of admission. Purpose: The purpose of this study was to determine if hospitalized
patients, who present with hyperglycemia (glucose greater than 180mg/dl) and who
meet algorithmic selection criteria placed on a nurse/pharmacist admission weightbased BBI protocol demonstrate better glycemic control than a historic control
group Methods: This exploratory, descriptive study was exempt from human subjects review. Inclusion criteria was extracted from the EHR by registered nurses and
pharmacists on selected demographic and physiologic variables for a weight-based,
adjusted dose of basal/bolus insulin management ranging from 0.2-0.4 units/kg/day.
Subject Selection: Between May 2012 and May 2013, adult hospitalized patients on
a single cardiopulmonary unit, age 18 and older, were screened by nursing using protocol criteria. 201 subjects were screened for inclusion. 92 were placed “on protocol”
with 37 noted “missed” opportunities. Results: In the “on protocol” group, 60%
of the sample achieved normo-glycemia (70-180 mg /dl) with only 5% hypoglycemic event compared to the “not in protocol” group of 51%. The “not in protocol”
group had average of 21% severe hyperglycemia (> 250 mg/dl) compared to 15%
of the “on protocol” group. The descriptive results of this pilot show that using an
inclusion algorithm to treat hyperglycemia at the time of hospital admission has the
potential for better glycemic control during early hospital management of patients.
Conclusions:Future improvement efforts will focus on insulin dosing and resistance.
335
NUTRITIONAL SUPPORT AND CLINICAL OUTCOMES OF
CHILDREN IN A PEDIATRIC INTENSIVE CARE UNIT
Christopher Babbitt1, Amanda Legro1, Emily Burritt1; 1Miller Children’s Hospital, Long Beach, CA
Learning Objectives: Children who are critically ill are at high risk for
energy and protein imbalances due to inflammatory responses, catabolic
processes, and increased metabolic demands.1 During metabolic stress it is
important that patients receive adequate calories and protein for metabolic
support. However, many medical conditions in the PICU inhibit this process and delay the initiation of early enteral nutrition (EEN). Methods: A
retrospective chart review was performed for patients admitted to a 20 bed
PICU at a tertiary children’s hospital during an 18 month period. Patients
mechanically ventilated, enterally fed and had a PICU LOS greater than
48 hours were included in the study. The patients were fed according to a
feeding protocol developed in our PICU. Data abstracted from the chart
review included: patient’s age, sex, PICU LOS, hospital LOS, MV days,
admission weight, admission height, admission BMI, discharge weight, discharge height, discharge BMI, pediatric risk of mortality (PRISM 3) score,
prescribed calories, prescribed protein, formula order, and daily volume of
formula received. Results: 87 patients with a median age of 1.15 yrs were
included in this study. Patients that received prescribed calories within 72
hours of admission had a shorter duration of MV compared to those who
did not (4.5 vs 6.6 days, p = 0.007), a shorter PICU LOS (8.6 vs. 14.4 days,
p=0.003) and overall hospital LOS (18.8 vs. 34.1 days, p=0.01). Patients
that received prescribed goal protein within 72 hours, had a shorter duration
of MV (4.4 vs. 7.6 days, p=0.005), PICU LOS (8.3 vs. 15 days, p=0.002)
and overall hospital LOS (18.7 vs 34.1 days, p=0.001). There was no difference in the two group’s median admit BMI. Conclusions: This retrospective
study demonstrated that EEN is associated with decreased LOV, PICU LOS
and overall hospital LOS. Feeding protocols that help establish standardized feed advancements may be helpful in reaching goal feeds early during
a PICU admission. 1. Skillman H and Mehta N. Nutrition therapy in the
critically ill child. Curr Opin Crit Care 2012; 18:192-198. doi: 10.1097/
MCC.0b013e3283514ba7
Poster Session: Endocrine/Nutrition 2
336
EVALUATION OF GLUCOSE MANAGEMENT SOFTWARE IN
CRITICALLY ILL PATIENTS WITH HYPERGLYCEMIC CRISES
Maresa Glass1, Kevin Ferguson1, Mark Rumbak2; 1Tampa General Hospital,
Tampa, FL, 2University of South Florida, Tampa, FL
Learning Objectives: The American Diabetes Association recommends the use of
a continuous intravenous (IV) infusion of regular insulin as one of the main components in the treatment of hyperglycemic crises, including diabetic ketoacidosis
(DKA) and hyperosmolar hyperglycemic states (HHS). These recommendations
also advocate achievement of a blood glucose (BG) reduction of 50-75 mg/dl/hr.
Studies exist addressing the safety and efficacy of glucose management software
programs, however there are limited data using these programs in DKA and/
or HHS patient populations. The purpose of this review was to determine if a
computerized glucose management system (Endotool®) would lower BG levels
effectively in DKA patients while minimizing incidents of hypoglycemia and
severe hypoglycemia. The hypothesis is Endotool® can safely and effectively lower
blood glucose in critically ill patients with DKA and HHS. Methods: This safety
and efficacy evaluation was conducted as a retrospective chart review of adult
patients with a diagnosis of DKA or HHS. Safety measures examined included
the incidence of hypoglycemia (BG less than 60mg/dl) and severe hypoglycemia
(BG less than 40mg/dl). Efficacy was measured by the rate of decrease of BG
levels in mg/dL/hr. Results: Fifty patients were included in the results. There
were 44 patients with a diagnosis of DKA and 6 with HHS. Of the 2912 recorded
BG measurements, 0.79% (23) were categorized as hypoglycemia and 0.17% (5)
categorized as severe hypoglycemia. The mean rate of blood glucose reduction
was 87 mg/dl/hr (95% CI [72.56-101.41]). A BG reduction of at least 50 mg/
dl/hr was achieved in 84% (42) of patients. Conclusions: The management of a
continuous intravenous infusion of regular insulin utilizing a computerized glucose management system (Endotool®) is both safe and effective at lowering BG in
DKA and HHS patients.
337
EFFECTS OF VITAMIN C AND E ON THE OUTCOME OF
CRITICALLY ILL PATIENTS REQUIRED MECHANICAL
VENTILATION
Samir Hegazy1, Tamer Helmy2, Humadi Zaher2; 1Faculty of Medicine, Alexandria University, alexandria, Egypt, 2Faculty of Medicine, Alexandria university,
alexandria, Egypt
Learning Objectives: Critical illness and injury are associated with oxidative
stress because of cytokine release and systemic inflammation. The generation of
reactive oxygen and nitrogen-oxygen species leads to mitochondrial dysfunction,
tissue injury, organ failure, and death Methods:This randomized, prospective
cohort study conducted on 54 mechanical ventilated patients divided blindly
into two groups: group 1 received antioxidant supplementation (vitamin E in
the form of α -tocopherol 400 IU (50 mL) 8h and vitamin C in the form of
ascorbic acid (50ml) 8h through enteral rout) and group 2 receiving placebo.
Both groups are followed for 28 days or till ICU discharge. The primary endpoint
for analysis was duration of mechanical ventilation, length of ICU stay. Secondary endpoints included the development of multiple organ failure and mortality
Results:Patients randomized to antioxidant supplementation had a significant
shorter duration of mechanical ventilation (p= 004), shorter length of ICU stay
(p= 009), and reduction of rate of multiple organ failure (p=0. 005), There was
no significant reduction in mortality. (p= 276) Conclusions: Administration of
antioxidant supplementation using α -tocopherol and ascorbic acid reduces duration of mechanical ventilation, ICU stay and the incidence of organ failure in
critically ill mechanically ventilated patients
338
USE OF PH AS AN INDICATOR OF NASOGASTRIC FEEDING
TUBE PLACEMENT IN CRITICALLY ILL INFANTS
Kathleen Meert1, Mary Caverly2, Lauren Kelm2, Norma Metheny3; 1Wayne State
University, Detroit, MI, 2Children’s Hospital of Michigan, Detroit, MI, 3Saint
Louis University Health Sciences Center, Saint Louis, MO
Learning Objectives: pH testing of feeding tube aspirates is an often recommended bedside method to determine tube location. However, clinicians are
unsure about the pH method’s effectiveness in determining gastric feeding tube
placement in infants who are receiving gastric acid inhibitors and frequent feedings. Our objective is to describe the pH of feeding tube aspirates obtained
from critically ill infants and evaluate the effect of gastric acid inhibitors and
recent feedings on aspirate pH. Methods: Critically ill infants <1 year of age
with blindly inserted feeding tubes were eligible for the study. Aspirates were
withdrawn from feeding tubes within one hour of a radiograph that described
the tube location. Aspirate pH was tested using a colorimetric pH indicator. Use
of gastric acid inhibitors within the past 24 hours and time since last feeding
were recorded. Data represent means and standard deviations; groups were compared using t-tests. Results: 100 aspirates were obtained from 60 infants (age
14.1 ± 13.9 weeks). Of these, 96 aspirates were obtained from infants with tubes
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
in the stomach, 2 from infants with tubes in the esophagus and 2 from infants
with tubes in the proximal duodenum. 47 (49%) gastric aspirates were obtained
from infants receiving gastric acid inhibitors and 33 (34%) from infants that
had been fed in the 4 hours prior to aspirate collection. Although pH values
were higher in gastric aspirates from infants who received gastric acid inhibitors
(4.56 ± 1.0 vs. 3.95 ± 1.1, p<.01) or recent feedings (4.64 ± 0.89 vs. 4.05 ± 1.2,
p<.01), 87 (91%) of all gastric aspirates had pH values ≤5.5. 23 gastric aspirates
were obtained from infants who received both gastric acid inhibitors and feedings
within 4 hours of aspirate collection; all had pH values ≤5.5. Aspirates with pH
values ≤5.5 were also collected from 2 tubes in the duodenum and one in the
esophagus. Conclusions: Gastric tube placement was correctly classified with an
aspirate pH ≤5.5 in the majority of cases. Use of gastric acid inhibitors and recent
feedings had minimal effect on the pH method’s effectiveness in determining
gastric tube placement.
339
EFFECT OF OPIOIDS AND BENZODIAZEPINES ON TOLERANCE OF ENTERAL NUTRITION IN PICU
Jithinraj Edakkanambeth1, Harsheen Kaur2, Sandeep Tripathi3, Ryan Hurt1;
1
Mayo Clinic, Rochester, United States, 2Mayo Cliic, Rochester, United States,
3
Mayo Clinic, Rochester, MN
Learning Objectives: Critically ill children in PICU very often require narcotic
or benzodiazepines (BZD) for sedation and analgesia. While effective in the primary goal, they have several side effects, with decreased gastrointestinal (G.I)
motility being one of the most common. It is not clear to what extent decreased
G.I motility contributes to feeding intolerance and other G.I complications. This
study was done with the hypothesis that patients who receive more cumulative
morphine equivalent or cumulative benzodiazepines would have more intolerance to feeds and as a result would get less enteral nutrition (EN). Methods:
Electronic medical records of all patients < 18 years of age admitted to the PICU
between Jan 2011 and Dec 2012 were examined to identify patients who were on
mechanical ventilator for at least 48 hours and received any sedative medication.
Patients with surgical contraindication to EN were excluded. Data was entered
into Redcap® software and analyzed using JMP® statistical program. Standard opioid conversion tables were utilized to calculate morphine equivalents. Results:
Data from EN delivery and opioid and sedative medication usage was analyzed.
There was no significant difference in the cumulative morphine or benzodiazepines doses in the first 10 days between patients who reached 1/3rd goal enteral
nutrition vs. those who did not. Patients who had GI complications (abdominal
distension, >2 vomiting/day, bleeding, Necrotizing enterocolitis (NEC) or constipation) received more opioids and Benzodiazepines (Cumulative over a 10 day
period 24.2 ± 23 mg/kg morphine equivalent and 18.5 ± 22mg/kg BZD equivalent vs. 15.9 ± 27 mg/kg and 12.5 ± 20 mg/kg), although the difference did not
reach statistical significance (p=0.1 and 0.15 respectively). We did not find any
correlation between morphine and benzodiazepines dosing and average calorie
intake or frequency of stools. Conclusions: In this retrospective study, use of
opioids and benzodiazepines was not associated with feeding intolerance. There
was a trend towards higher G.I complications in those receiving higher doses.
340
INCREASING WEIGHT-BASED DOSING OF INSULIN IS
ASSOCIATED WITH HYPOGLYCEMIA IN CRITICALLY ILL
PATIENTS
John Radosevich1, Asad Patanwala2, Paul Frey3, Yong Gu Lee4, Holly Paddock2,
Brian Erstad2; 1St. Joseph’s Hospital and Medical Center, Phoenix, AZ, 2University of Arizona College of Pharmacy, Tucson, AZ, 3The University of Arizona
Medical Center, Tucson, AZ, 4Banner Good Samaritan Hospital, Phoenix, AZ
Learning Objectives: Blood glucose control in critically ill patients is usually
performed using continuous infusions of insulin. There is a lack of data regarding
the effect of weight-based dosing on the incidence of hypoglycemia in this patient
population. The purpose of this study was to evaluate the association between
weight-based insulin infusion rates on hypoglycemia. Hypothesis: Increasing
weight-based dosing of insulin is associated with hypoglycemia in critically ill
patients receiving continuous intravenous insulin infusions. Methods: This was
a retrospective, case-control study conducted at a tertiary care, academic medical center. Adult patients admitted to the intensive care unit (ICU) receiving
intravenous insulin infusions for the management of hyperglycemia between
January 2008 and March 2013 were included. Each patient who developed
hypoglycemia (blood glucose <70 mg/dl) was matched with a non-hypoglycemic
control subject, based on age and sex. The primary outcome was highest insulin
infusion rate (units/kg/hour) measured on the day of hypoglycemia in cases and
same day in controls. Continuous variables were compared between the groups
using a Students t-test and categorical variables were compared using the Fisher’s
exact test. Logistic regression was used to assess the relationship between insulin
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
infusion rate and hypoglycemia. Results: A total of 122 patients were included
in the study (61 cases, 61 controls). The mean weight-based insulin infusion rate
was higher in the cases than in the controls (0.11 versus 0.07 units/kg/hour,
p=0.009). The risk of hypoglycemia increased with increasing dose (OR 2.2, 95%
CI 1.2 to 4.3, p=0.015, per 0.1 unit/kg change). The proportion of patients in
each group (cases versus controls) based on 24-hour insulin consumption (units/
kg/day) was as follows: less than 0.20 (11% versus 5%), 0.20-0.39 (5% versus
21%), 0.40-0.59 (20% versus 16%), 0.60-0.79 (10% versus 16%), 0.80 or more
(54% versus 41%) (p=0.036 for overall group). Conclusions: Increasing weightbased doses of insulin are associated with hypoglycemia in the ICU.
341
ASSOCIATION OF EARLY ENTERAL NUTRITION DELIVERY
AND CLINICAL OUTCOME IN CRITICALLY ILL CHILDREN.
Harsheen Kaur1, Jithinraj Edakkanambeth2, Sandeep Tripathi3, Ryan Hurt2;
1
Mayo Cliic, Rochester, 2Mayo Clinic, Rochester, United States, 3Mayo Clinic,
Rochester
Learning Objectives: Optimal nutrition in critically ill children has been shown
to be important for sustaining organ function and promoting wound healing.
However there is equipoise in the existing literature regarding the impact of
early enteral nutrition (EN) on patient outcomes. This study was undertaken
with the hypothesis that patients who receive optimal EN have better outcomes.
Methods: Electronic Medical Records of all patients < 18 years of age, admitted
to PICU between Jan 2011 and Dec 2012, were examined to identify patients
who were on mechanical ventilation for at least 48 hours and received sedation.
Patients with surgical contraindication to feeding were excluded. Predefined data
was entered into a Redcap® software and analyzed using JMP statistical program®.
Results: Out of the 106 patients meeting the inclusion and exclusion criteria,
only 11% received >75% of the prescribed enteral calories and 50% met 1/3rd of
the goal in the first 10 day of PICU admission. A total of 38% of the patients did
not receive full EN on any day of their first 10 days. No significant difference was
observed on any outcome variable (ICU or hospital length of stay, ventilator days
or mortality) or incidence of hospital acquired conditions between the groups.
There was no correlation between average calorie intake and PICU length of stay
(r=0.16). Patients, who achieved at least 1/3 of the enteral calorie intake, had less
G.I complications (46% vs. 69.2% p=0.01). Use of any vasoactive medication
was not associated with increased instance of G.I complication. Conclusions:
In this single center retrospective study we did not find any beneficial impact of
early enteral nutrition on patient outcomes. Use of enteral nutrition may have a
favorable impact on G.I complications.
342
EVALUATION OF A GLYCEMIC CONTROL PREVENTATIVE
MEASURES PROTOCOL IN THE INTENSIVE CARE UNIT
Mahmood Ali1, Alba Gonzalez2, Sandra Van Horn3, Julie PEPE4, Eugene Go5;
1
Florida Hospital Orlando Pulmonary Critical Care Department, Orlando, FL,
2
Florida Hospital, Orlando, FL, 3Florida Hospital Orlando, Orlando, FL, 4FH,
Orlando, FL, 5florida Hospital, Orlando, FL
Learning Objectives: Hypoglycemia, either spontaneous or occurring as a
complication of insulin therapy, is a frequent occurrence in critically ill patients
Hypoglycemic events were associated with increased risk of mortality and length
of stay in ICU patients. Severe hypoglycemia, usually defined as blood glucose
level (BG) < 40 mg/dL, and mild hypoglycemia–BG < 70 mg/dL. The purpose of
this study is to determine the effectiveness and safety of a standardized preventive
measure, order set/template in order to reduce hypoglycemic events in critically
ill patients who are NPO for > 4 hours, tube feedings on hold for greater than
4 hours, or decrease oral intake less than 50 percent of the goal. Methods: All
patient with orders of Nothing by mouth or tube feeding on hold for more than
4 hours or low Po intake were included in the study, and accuchecks every 3 hours
initiated. Patients were placed on intravenous Dextrose (D10W) at 30 ml/hour
when blood glucose was less than 150. If blood glucose was higher than 150, then
we hold D10W. Hypoglycemia protocol was initiated if blood glucose was less
than 70 mg/dl. Data collection on all patients included in the study between July
2012 to March 2013. Results: Data of 125 patients were collected, their average age of the patients were 65 years, 70% of the patients were male. The average low blood glucose level was 93.6 mg/dL and the average high blood glucose
level was 180.8 mg/dL. The events of severe hypoglycemia before implementing
the preventive order set was significantly higher where sixteen patients developed
severe hypoglycemia in 8 month period, as compared to only 1 patient in the
8 months after. The number of patients who experienced a mild hypoglycemic
event before the preventive order set was 59 patients in an 8 month period, as
compared to 17 patients in the 8 months after the preventive order set was placed.
Conclusions:The implementation of the preventive measure order set in ICU is
feasible and associated with significant reduction of hypoglycemic events in ICU
patients. Which will positively impact the outcome and cost of care.
343
EFFICACY AND SAFETY OF INSULIN GLARGINE VERSUS
INSULIN INFUSIONS IN INTENSIVE CARE UNIT PATIENTS
Christina Rose1, Marissa Casagrande1, Brittany Conahan1, Benjamin Pullinger1,
Kristen Schmerbeck1, Hannah Spinner2, Sarah Yeager3; 1Temple University, Philadelphia, PA, 2Baystate, Springfield, MA, 3Thomas Jefferson University Hospital,
Philadelphia, PA
Learning Objectives: Blood glucose (BG) variability in critically ill patients
has been associated with increased mortality. The administration of longacting insulin products is an increasing trend in critically ill patients. Longacting insulin may decrease monitoring and reduce glucose variability but the
efficacy and safety in intensive care unit (ICU) patients has not been well
described. Methods: A retrospective cohort of ICU patients on either continuous infusions of short acting insulin (II) or insulin glargine (IG) was conducted from January 2010 through February 2014. Patients receiving insulin
for DKA⁄HHNK, insulin for< 48 hours or receiving oral hypoglycemics or >
1 type of insulin besides correction in the IG group were excluded. The primary objective was to compare the efficacy of II and IG using day-weighted
mean BG and the % of BG in goal range of 70- 180 mg/dl. The safety of each
regimen was also compared using the % of patient-days with any BG <60 mg/
dl. Results: 17 patients in the II group and 28 patients in the IG group were
included. The mean age of both groups was 65 years with a median APACHE
II score of 23 in the II group and 22 in the IG group. The average days on II
was 4 compared to 5.7 in IG group. The day weighted-mean BG was higher
in the IG group (164 +/-16 vs 137 +/- 19 mg/dL, p<0.0002). Similarly, the
mean of all BG of each cohort was higher in the IG group (166 vs 153 mg/
dL, p < 0.001). BG readings in the II group were more frequently in the goal
range of 70-180 mg/dL compared to the IG group (75% vs 63%, p < 0.001).
% patient-days with BG < 60 was higher in the II group at 6.6% compared
to 3% in the IG group but was not significant (p<0.294). Conclusions: The
day−weighted mean BG was lower in the II group compared to IG, though
both were within the goal range of 70-180 mg/dl. The patients in the II group
were in the goal range for a higher percentage of time compared to the IG
group but the incidence of hypoglycemia was higher in the II group. This small
retrospective cohort shows there may be a potential role for insulin glargine in
critically ill patients with hypoglycemia.
344
SYNBIOTICS THERAPY IMPROVES GUT DYSBIOSIS IN
SEVERE SEPSIS PATIENTS: A RANDOMIZED CONTROLLED
TRIAL.
Tomoki Yamada1, Kentaro Shimizu1, Hiroshi Ogura1, Takeyuki Kiguchi2, Takashi
Asahara3, Koji Nomoto3, Satoshi Fujimi2, Takeshi Shimazu1; 1Osaka University
Graduate School of Medicine, SUITA, OSAKA, Japan, 2Department of Emergency and Critical Care, Osaka General Medical Center, Osaka, Japan, 3Yakult
Central Institute, Tokyo, Japan
Learning Objectives: The gut is an important target organ after severe injury.
We previously reported that altered gut microbiota and environment was associated with infectious complications and mortality in patients with severe systemic
inflammatory response syndrome (SIRS). However, the effects of synbiotics therapy in severe sepsis patients has not been thoroughly clarified. The objective of
this study was to evaluate if synbiotics therapy can maintain the gut microbiota
and environment in patients with severe sepsis. Methods: Severe sepsis patients
with mechanical ventilation were randomized to receive synbiotics or no synbiotics (control group). Infectious complications (such as ventilator associated
pneumonia, enteritis and blood stream infections), gastrointestinal dysmotility,
length of ICU stay, and death were recorded. Fecal samples were acquired from
the subjects by swabs of the rectum within 3 days after admission and weekly.
Microbiota were detected by ribosomal RNA-targeted reverse transcriptase-quantitative polymerase chain reaction (RT-qPCR) method and organic acids by highperformance liquid chromatography. Results: Eighteen severe sepsis patients
were included. There was no significant difference between the two groups in
patient characteristics and about infectious complications and outcome. Total
bacterial counts were higher in Synbiotics group than in control group in 1st
week(Median;9.35vs7.46 as log10cells/g feces, p=0.07). Concentration of fecal
total organic acid in 1st week were significantly higher in Synbiotics group than in
control group(Median;125.21vs39.72 as µmol/g feces, p=0.01). Moreover, there
were significant differences between the two groups by the analysis of changes
over time in number of total bacteria(p=0.04), Bifidobacterium(p=0.02), and Lactobacillus (p=0.04), and concentration of acetate(p=0.02) and butylate(p=0.03).
Conclusions: Synbiotics therapy can maintain the gut microbiota and environment in patients with severe sepsis. That would be a fundamental mechanism of
synbiotocs to keep a normal host response through gut microbiota in critically
ill patients.
345
METABOLOME ALTERATION IN CRITICAL ILLNESS
ACCORDING TO VITAMIN D STATUS: A PROSPECTIVE
COHORT STUDY
Kenneth Christopher1, Angela Rogers2, Rebecca Baron3, Laura Fredenburgh3,
Lee Gazourian3, Anthony Massaro4, Augustine Choi5, Augusto Litonjua3; 1Renal
Division, Brigham and Women’s Hospital, Boston, MA, 2Division of Pulmonary
and Critical Care Medicine, Stanford University Medical Center, Stanford, CA,
3
Pulmonary and Critical Care Medicine Division, Brigham & Women’s Hospital,
Boston, MA, 4Pulmonary and Critical Care Medicine Division, Brigham and
Women’s Hospital, Boston, MA, 5Department of Medicine, Cornell University
Weill Medical College, New York, NY
Learning Objectives: We hypothesized that differential metabolic profiles exist
in the critically ill with regard to vitamin D status. Methods: We performed
metabolomic profiling of plasma from 31 MICU subjects (68% septic) within 72
hours of ICU admission. Plasma metabolomic profiles were generated from 411
metabolites, via gas and liquid chromatography and mass spectroscopy. Metabolites with the lowest inter-quartile range of variability were removed, leaving 308
metabolites. 25(OH)D levels were determined via chemiluminescence immunoassay. Adjusted associations were estimated with multivariable logistic regression models including potential confounders. The primary outcome was 28-day
mortality. Results: Metabolomic profiles differed in critically ill patients with
vitamin D deficiency (25(OH)D<20 ng/ml) relative to those 25(OH)D≥ 20 ng/
ml. 12 of the metabolites were significantly associated with vitamin D deficiency,
after adjusting for age, gender, race, malignancy status, sepsis, and renal function
(p<0.05). Low levels of 3 of these metabolites were significantly associated with
both vitamin D deficiency and 28 day mortality: the amino acid trans-urocanate, the nucleotide 7-methylguanine and the carbohydrate 1,5-anhydroglucitol
(p<0.05). A model with adjustment for APACHE II, age, gender, race, 25(OH)
D and sepsis diagnosis showed good calibration (Hosmer-Lemeshow χ2 P = 0.70)
and discrimination for 28 day mortality (AUC=0.82). Evaluation of the addition of metabolites (trans-urocanate,7-methylguanine, and 1,5-anhydroglucitol)
to the model, demonstrated good calibration and improved discrimination for
28-day mortality (AUC of 0.98). Differences in model discrimination with and
without metabolites were significant (χ2 P = 0.03). Further, the net reclassification improvement was estimated at 0.46 (P= 0.005) and the integrated discrimination improvement was estimated at 0.39 (P<0.001). Addition of metabolites
improved classification for a net of 46% of individuals with 28-day mortality.
Conclusions: Metabolite profiles significantly differ in critically ill subjects
according to vitamin D status.
Poster Session: Endocrine/Nutrition 3
346
EDUCATION AND ALGORITHM IMPROVE NUTRITION OF
CRITICALLY ILL PATIENTS IN THE SURGICAL INTENSIVE
CARE
Janet Weisz1, Kyle Bunton1, Tahnee Thibodeau1, Katherine Petrin1, Harry Anderson, III1; 1St. Joseph Mercy Ann Arbor, Ann Arbor, Michigan
Learning Objectives: Enteral nutrition (EN) initiated within the first 24-48
hours of SICU admission has been associated with a reduction in infectious complications, ICU (intensive care unit) and hospital lengths of stay, and mortality.
Ensuring optimal and consistent nutrition is challenging and studies have shown
that, on average, 60% of prescribed calories are actually delivered to patients.
Methods: In 2011, a benchmarking survey in the SICU (International Nutrition Survey, INS 2011, n=21) revealed that only 42% of our EN patients had
nutrition initiated within 48 hours of admission, and an even smaller percentage
received the prescribed amounts of calories and protein. The INS 2011 questionnaire demonstrated that our barriers to effective nutrition delivery included lack
of knowledge on how to optimally feel patients, misconceptions about contraindications to EN, and numerous interruptions due to perceived intolerance. In
response, we first developed a quality improvement initiative providing education
to critical care nursing staff and physicians. We then introduced a nutrition support algorithm to guide timely delivery of nutrition. Goals included initiation of
EN within 48 hours of SICU admission and achieving calorie goal within the
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
next 72 hours. Appropriate contraindications to EN were delineated, and the
gastric residual policy was revised to prevent unnecessary interruptions. Results:
In 2013, a follow-up study in the SICU (n = 25) showed improvement. Nutrition was initiated within 48 hours of admission in 75% (improved from 42%)
of EN patients, while 51% of calories and 48% of protein prescribed (up from
37% and 36%, respectively) were successfully delivered. Conclusions: Introduction of critical care team education and a nutrition algorithm have heightened
awareness of the importance of nutrition in the SICU, and have provided strategies and identifiable goals, leading to improved delivery of nutrition. We propose that additional improvement will be accomplished by feeding patients with
ileostomies and colostomies sooner, and by inserting nasoduodenal feeding tubes
intraoperatively.
347
ULTRASOUND GUIDED NASOGASTRIC FEEDING TUBE
PLACEMENT IN CRITICAL CARE PATIENTS
Funda Gok1, Alper Kilicaslan1, Alper Yosunkaya1; 1Necmettin Erbakan University, Konya, Turkey
Learning Objectives: Nasogastric feeding tube (NGT) placement is the most
frequently used method for enteral feeding and drug administration in critical
care patients. Complications can develop at a rate of 0.3- 8% due to the nature of
method. Therefore, we aimed to prospectively evaluate the effectiveness of ultrasound-guided NGT placement in intensive care units and to evaluate procedurerelated parameters in the present study. Methods: 56 mechanically ventilated
patients monitored in the intensive care unit who received US-guided NGT
placement were included in the study. The patients were placed in the supine and
sniffing position before the procedure. High frequency linear USG probe which
was transversely placed over the suprasternal notch, an attempt was made to visualize the esophagus by sliding the probe to the left. If the image was not achieved
in this manner, an image of the esophagus was obtained by cricoid pressure application. Meanwhile, a second individual inserted a polyurethane NGT of 10-14
Fr in thickness was inserted. The NGT was gently advanced and an attempt was
made to visualize its passage from the esophagus lumen with US. At the end of
the procedure, US was performed on all patients to obtain a sonographic image of
the esophagus before removing the guide wire of the NGT. Furthermore, gastric
placement of the NGT tip was confirmed with abdominal x-ray. Results: A total
of 56 patients were included in the study. In 53 (94.6%) out of 56 patients, the
NGT image was obtained during placement within the esophagus (Figure 1). In
23 patients (41%), cricoid pressure was applied to achieve a sonographic image
of the esophagus. In three patients (5.3%), the nasogastric feeding tube was
blindly placed, as the esophagus was not visualized. No other complications were
observed in the patients. At the end of the intervention, it was seen that NGT was
in the esophagus in 53 patients (94.6%). Conclusions: As a result, in the present
case series composed of critically ill patients, the transmission of NGT through
the esophagus could be visualized in real time at a high rate.
348
EFFICACY OF A NURSE-DRIVEN, ELECTRONIC, DIABETIC
KETOACIDOSIS PROTOCOL – A COMPARATIVE ANALYSIS
Marybeth Boudreau1, Megan Hudacek2, James McCarthy1, Renee Ford3, Robert
Hand4; 1Eastern Maine Medical Center, Bangor, ME, 2Eastern Maine Medical
Center, Bangor,ME, 3Eastern Maine Medical Center, Brewer, ME, 4Penobscot
Respiratory, Bangor, ME
Learning Objectives: Diabetic ketoacidosis (DKA) is a serious and complicated
health crisis. As a response to its often time-intensive, multifaceted treatment,
numerous standardized protocols led by endocrinologists at large urban teaching hospitals have been studied and have demonstrated improvement in patient
outcomes. Eastern Maine Medical Center is a rural tertiary hospital where endocrinology services are not always available. As such in 2012, a previously published protocol was adapted into a nurse driven, electronic order set and titration
calculator. We conducted a subsequent review of patient cases to determine if
our electronic, nurse-driven DKA protocol and electronic titration calculator
resulted in similar outcomes as the endocrinologist-designed, physician-led protocol upon which it was based. Methods: This was a single-center, retrospective,
observational trial conducted at a rural tertiary care center, with data collection
occurring over a 16 week period. The study was approved by our IRB. The electronic medical records of eligible patients were analyzed for endpoint data. The
primary endpoint was time to anion gap closure (defined at a value <13 mmol/L).
Secondary endpoints were critical care unit length of stay (hours), hospital length
of stay (hours), incidence of anion gap re-opening (>12 mmol/L) and incidence
of hypoglycemia on the protocol (<55 mg/dL) Results: Twenty-six patients were
included in the data analysis. Time to anion gap closure was 10.36 hrs at the
study institution, vs. 10.3 hrs in the model protocol (p = 0.95). ICU length of
stay was 32.39 hrs vs. 34.2 hrs (p = 0.57), hospital length of stay was 56.71 hrs
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
vs. 64.3 hrs p = 0.25), recurrence of anion gap was 23.1% vs. 3% (p = 0.06), and
hypoglycemic episodes occurred in 3% vs. 14% of patients (p =0.76). Conclusions: Our data indicate that adapting a DKA protocol developed and overseen
by endocrinologist and fellows at an academic teaching institution into an electronic, nurse-driven protocol can result in similar patient outcomes.
349
EVALUATION OF HYPOGLYCEMIA WITH 2 DIFFERENT
INSULIN PROTOCOLS IN THE NEURO INTENSIVE CARE
UNIT(NICU)
Brittany Pelsue1,2, Elizabeth Isaac2, Susanne Muehlschlegel3, Jeffrey Fong2, Kristen
Ditch2; 1PharmD, Worcester, MA, 2UMass Memorial Medical Center, Worcester,
MA, 3MD, MPH - UMass Memorial Medical Center, Worcester, MA
Learning Objectives: Intensive insulin therapy (IIT) is defined as a blood glucose (BG) of 80-110 mg/dL. Studies on benefits of IIT in critically ill neurologic
patients have been inconclusive despite an association with poor patient outcomes
from both hyperglycemia and hypoglycemia. At our institution a nurse-driven
paper protocol is used to achieve a BG of 80-140 mg/dL using intravenous and
subcutaneous insulin. The performance of this protocol was evaluated to determine
the rate of hypoglycemic events which led to the creation of a pilot glycemic protocol targeting a BG of 100-140 mg/dL. We aimed to compare the hypoglycemic
event rate in the NICU between patients in the pre-pilot (target BG 80-140 mg/
dL) and pilot groups (target BG 100-140). Methods:This is a retrospective review
of adult patients admitted to the NICU at our institution who experienced a
hypoglycemic event (BG < 60 mg/dL). Data was collected between October 2012
and December 2012 for the pre-pilot phase and from November 2013 to June
2014 for the pilot phase. Hypoglycemic event rates were compared between the
two protocols. Results: Seventy-five hypoglycemic events were included in the
analysis; 45 in the pre-pilot phase and 30 in the pilot phase. Five patients (11%) in
the pre-pilot group had non-insulin dependent diabetes vs. 10 (33%) in the pilot
group (p=0.018). Ischemic stroke was the most common diagnosis in the pre-pilot
phase [16(35%)] vs. the pilot phase [3(7%)] (p=0.002). Intracerebral hemorrhage
was less common in the pre-pilot phase [2(4%)] vs. the most common diagnosis
in the pilot phase [13(31%)] (p=0.001). Other baseline characteristics were similar
between groups. Hypoglycemic events occurred at a rate of 4.2 events per 100
patient-days in the pre-pilot phase vs. 1.2 events per 100 patient-days during the
pilot phase (p<0.0001). Complete adherence to the protocol was achieved in 5
(13%) patients in the pre-pilot phase vs. 11 (37%) patients in the pilot group
(p=0.017). Conclusions: In this retrospective chart review the pilot glycemic protocol was associated with a statistically significant decrease in hypoglycemic events.
350
RADIOLOGIC INTERPRETATION OF NUTRITION AT BASE
OF SPINE (RIBS) - NOVEL MARKER FOR NUTRITIONAL
STATUS
Ilya Shnaydman1, Jacqueline McLatchy2, Rafael Barrera3; 1Long Island Jewish
Medical Center, N/A, 2NorthShore LIJ Health System, N/A, 3Long Island Jewish
Medical Ctr, New Hyde Park, NY
Learning Objectives: Critically ill patients suffer from nutritional deficiency
resulting in poor wound healing, prolonged ventilator dependence and decreased
survival. Currently no objective method to accurately assess a patient’s nutritional exists.The purpose of this study was to create a simple, effective and accurate nutritional scoring system by radiologic interpretation of nutrition status.
Computerized calculations at the base of spine created a scoring system which
correlated with nutrition and outcome. Methods: The RIBS application using
technologies from facial reconstruction; created by one of the authors, guides
users through a few simple steps to upload a lumbar slice from a routine CTAP
and select the boundaries of fat and muscle adjacent to the spine. Then a RIBS
score, the percent fat of the target tissues (fat and muscle), is calculated. This
application is cross-platform compatible on mobile as well as desktop devices.
This study retrospectively compared albumin, prealbumin, BMI, BSA, and RIBS
score among 20 SICU patients using CT scans obtained at least four weeks apart.
End goals were ICU length of stay, ventilator dependence and survival. Results:
A two year retrospective chart review yielded twenty patients that met inclusion
criteria. Early results demonstrated increased RIBS scores following at least one
month of hospitalization. Increasing RIBS score correlates to worsening nutritional status. The RIBS scores correlated with albumin, prealbumin, ICU stay
and need for ventilator support (p=0.05). Conclusions: Preliminary results demonstrate the effectiveness of the RIBS scoring system for assessing nutritional
support in the critically ill surgical patient. Increasing RIBS scores, indicating a
proportional loss of muscle tissue compared to fat tissue, likely catabolic, were
found in nutritionally compromised patients. This study showed that like albumin, BMI/BSA, a RIBS score could be a valid nutritional marker that positively
correlates with ICU length of stay and ventilator dependence.
351
EFFECTS OF INSULIN INFUSION RATE CHANGES ON GLUCOSE OSCILLATIONS FOR STRESS HYPERGLYCEMIA
Richard Strilka1,2, Stewart McCarver1,3, Scott Armen1, Matthew Indeck1; 1Pennsylvania State Hershey Medical Center, Hershey, PA, 2San Antonio Military Medical Center, San Antonio, TX, 3Walter Reed National Military Medical Center,
Bethesda, MD
Learning Objectives: Stress hyperglycemia (SH) of critical illness is multifaceted;
it involves elevated stress hormones, insulin resistance (IR), and insulin deficiency
(ID). The effect of insulin drip adjustments on glucose can be mathematically
modeled for various IR and ID combinations, providing insight into the glucoseinsulin dynamics found in SH. Methods: A glucose-insulin model was used to
simulate two groups of 20 virtual patients: those receiving, or not receiving, a
continuous nutritional source; SH was created by doubling the gluconeogenesis
rate, varying IR from borderline to high, and changing insulin secretion from a
normal to severely deficient state. This produced pre-insulin glucose oscillations
with maximum (Gmax) values between 160-170 mg/dl with minimum (Gmin)
values between 80-115 mg/dl. Next, an insulin infusion was titrated to produce
two tight glycemic control (TGC) goals with Gmax values of 110 and 125 mg/dl;
the insulin was then abruptly stopped. After the glucose oscillations returned to
pre-insulin levels, the insulin infusions were restarted at the same TGC rates. The
effects on glucose oscillations were studied. Results: Abruptly stopping an insulin
infusion caused significant temporary rebound hyperglycemia (RH) when TGC
110 mg/dl infusions were the starting point, provided IR was high (largest increase
20 mg/dl) without dependence on ID. Abruptly restarting an insulin infusion
resulted in Gmin values that were temporarily lower than those in the steady state
insulin infusions (largest decrease 20 mg/dl); this was most pronounced when the
TGC 110 mg/dl rates were used with severe ID. With no nutritional source, RH
was not produced; however, mild hypoglycemia occurred when the insulin infusions were restarted when IR was high. Conclusions: Glucose-insulin dynamics
are nonlinearly affected by IR, ID, and the nutritional source; each of which may
change over time. It is unlikely that a traditional insulin drip protocol, based on
a single simple algorithm, could optimally handle such complexity. Mathematical
glucose-insulin models may prove the most adaptive in the critical care setting.
352
CALORIFIC DEFICIT IN PATIENTS WITH MULTIPLE SEVERE
TRAUMA AND MORBIDITY ASSOCIATED
R. Gutierrez-Rodriguez1, J.F. Fernandez-Ortega1, M.J. Furones-Lorente1, M.V.
Garcia-Martinez1, I Macias-Guarasa1; 1Hospital Regional Carlos Haya, Malaga,
Spain
Learning Objectives: Our objetive is to establish morbidity associated with delay
in nutrition and the increase in calorific deficit on the 10th day in patients with
multiple severe trauma Methods:Prospective descriptive study of patients admitted to ICU for multiple severe trauma in 2013-2014. Variables: demographics,,
hospital and ICU mortality, gravity according to different scores on admission
(APACHE II, SOFA, Data Bank score, ISS, GCS). Previous treatment. Complications Turing admisión, pulmonary, renal according to RIFLE, nosocomial infection. Day on which diet commenced, enteral or parenteral, calculations according
to weight and our protocols, calorific deficit on day of admission. Significance
rated at P < 0.05. X2 for análisis of qualitative variables and T-Student for quantitative variables. Results: 87 patients were studied. Mean age 47.2 ± 17 years.
Average stay 18.6 days ± 15. Data Bank mean score 2.8 ± 1.55, GSC, Glasgow
come scale, 8.4 ± 4, APACHE II 18 ± 7, SOFA 3.1 ± 1.6. ISS 21 ± 12. TRISS 13.4.
Hospital mortality 18.4%. Renal insufficiency during admission 15%, pulmonary
complications 20%, nosocomial infections, 41.7%. Mean calorific deficit on 10th
day of admission, -4.888 ± 3.98 kcal, 14.3% presented a deficit greater than -8000
kcal. 65.1% started their diet before the third day, above all on the second day,
(58,7%), enteral, 93% of cases. In the univariable analysis we found there were
no significant differences between groups with regard to hospital mortality and
a calorific deficit above 8000 kcal/ There was a significant difference in the rate
of hospital prolonged stay, 88.9%, increase in the number of days of mechanical ventilation, > 7 days, 66.4%, pulmonary complications (respiratory distress
and pneumonia), 44,4%, and nosocomial infections, 76.7%. Conclusions: It is
necessary to establish new protocols to optimize nutrition in patients with severe
multiple trauma who already present an significant accumulated deficit, given that
though it does not increase mortality, it does increase co-morbidity
353
EARLY TRANSITION TO SUBCUTANEOUS INSULIN FOR
GLYCEMIC CONTROL IN CARDIAC SURGERY
Peter Terry1, Kush Dholakia2, Gregory Fontana2, Jonathan Hemli3, Hugh Lawrence3, Nirav Patel2, Minisha Sood2, Jamie Taylor2; 1N/A, N/A, 2Lenox Hill Hospital, New York, NY, 3Lenox Hill, New York, NY
Learning Objectives: We proposed that early transition to SQ insulin would
reduce the duration of CII compared with a strategy of continuing CII for 24
hours after surgery. Methods: We retrospectively reviewed 73 consecutive cardiac
surgery patients (36 diabetic) for EA time, time of first dosing of SQ insulin,
blood glucose (BG) values obtained between 18 and 24 hours after EA. Patients
received CII immediately after cardiac surgery. When patients first tolerated oral
feeding, SQ insulin was substituted. Diabetic patients received basal, prandial,
and correctional insulin. Non diabetics received correctional insulin. Additionally, for any BG > 180 mg/dL obtained between 18-24 hours after end of anesthesia, at least 5 Units regular insulin IVP was given and BG repeated. Results: 20
patients could not tolerate oral intake within 24h from EA and were maintained
onCII for at least 24 hours. 4 did not require CII. 48 transitioned from CII to
SQ insulin with 24 h after EA. Cases with EA time prior to 16:00: mean time
of the first dosing of SQ insulin was 09:18 the day after surgery. Duration of
CII was 19.69h (range 9.5 to 27.75h). Cases which ending after 1600: mean
EA time was 18:09, mean time of first dosing of SQ insulin was 09:48. Duration of CII was 14.03h (range 3 to 18.75h). Patients in both early and late cases
transitioned to SQ insulin at a similar mean time on the day after surgery. The
mean BG 18-24 hours after EA was 117.95mg/dL. There were 8 BG < 70 mg/
dL (3.5%), and none < 50 mg/dL. The glycemic control target was met in all but
two patients whom did not receive indicated additional IVP insulin dosing when
a BG > 180mg/dL was obtained. Conclusions: Early transition from CII to SQ
insulin is safe and effective for glycemic control after cardiac surgery and reduces
the duration of CII to well under 24h, particularly for cases ending after 1600.
This strategy potentially improves resource utilization and patient satisfaction.
Training and compliance of staff is important for efficacy of this multidisciplinary
protocol.
354
PARENTERAL NUTRITION IN CRITICAL CARE: OBSERVATIONS AND CHALLENGES IN A PRACTICE PATTERN
ASSESSMENT
Yoanna Skrobik1,2, John Drover3, Asmaa Khamsi4; 1N/A, Ontario, Canada, 2Université de Montréal, Montreal, Canada, 3Queen’s University, Kingston, ON,
4
Maisonneuve Hospital, Montreal, Quebec
Learning Objectives: Nutritional support determines outcome in critically
ill children and adults1,2. Parenteral nutrition (PN) is administered more frequently in critically ill, and ICU and non-ICU adult and pediatric patients in
whom gastrointestinal dysfunction is a primary diagnosis3, than in any other
patient population. We sought to establish which PN practices are considered
useful in critically ill patients by consulting expert multidisciplinary practicing
clinicians, and by reviewing relevant publications and guidelines. clinical practice
audits serve to reflect whether guidelines or best practice are, in fact, applied to
current clinical care. Methods: A multidisciplinary panel of provincial experts
independently described key clinical features they considered to be significant
triggers, and prescription modifiers, for PN in critical illness using a nominal
process. A modified Delphi Method was then used to develop a list of quality
indicators. A list of clinically relevant parameters was generated based on expert
opinion and on a review of the relevant literature. The panel of experts subsequently reviewed and approved these parameters, which served to construct the
practice survey. This survey was then sent to critical care caregivers in every intensive care unit providing PN in the province. Its content described site-specific
clinical practice and PN determinants, based on the identified clinically relevant
parameters. Results: The respondents represented caregivers looking after 75%
of Quebec’s critical care patient population and were mostly from academic institutions. PN prescribing practice was highly variable in all parameters surveyed
and inconsistent with guidelines or parameters based on observational data at
least 40% of the time. Conclusions: The variability and inconsistency in parenteral nutrition practice in critically ill adults and children in Quebec mirrors the
paucity of randomized controlled trial based evidence and the resulting limited
guidelines recommendations.
355
ENTERAL FEEDING TIMING AND OUTCOMES AFTER
SIMULTANEOUS TRACHEOSTOMY AND PEG PLACEMENT
IN THE ICU
Christa San Luis1, Ravirasmi Jasti2, Tammi Tam1, Nasir Bhatti2, Vinciya Pandian1; 1Johns Hopkins University School of Medicine, Baltimore, MD, 2Johns
Hopkins University School of Medicine, Baltimore, United States
Learning Objectives: Studies have shown that enteral tube feeds decrease
intensive care unit (ICU) related stress ulcers, promote comfort, maintain
nutrition, and aid in wound healing. The timing of enteral feeding initiation
and their outcomes have not been described adequately in patients requiring simultaneous tracheostomy and percutaneous endoscopic gastrostomy
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
(STPEG) in the ICU. The purpose of this project was to assess the outcomes of
various timings of enteral feeding initiation. Methods: Between October 2011
and November 2012, as part of a quality improvement project, patients undergoing STPEG tube placement were randomized into starting enteral tube feeds
within 4 hours (A), 4-12 hours (B) or greater than 12 hours (C). Patient demographic and clinical characteristics were collected. Primary outcome measured
was presence of high gastric residual volume (>250cc), and secondary outcomes
included peri-procedural complications, mortality (<72 hours), and intensive
care unit (ICU) and hospital lengths of stay. Comparative descriptive statistics
were used. Results: Seventy seven patients were included in the study. The
three groups had comparable baseline demographic and clinical characteristics
including disease severity scores. There were no statistical differences in residual volumes, or lengths of stay between three groups. There was no difference
in various procedural complications except for a significantly higher rate of
tube feed leakage via the stoma in group C (A =25% vs B=0 vs C=32.65%,
p=.03). Moreover, a 5% overall short-term mortality rate was also noted in
this study group. Conclusions: To our knowledge this is the first randomized
controlled quality improvement project analyzing patients’ outcomes and timing of enteral feeds of patients undergoing STPEG in the ICU. This project
revealed that there were no disadvantages to starting enteral feeds as early as 4
hours. Findings from this project support early initiation of enteral tube feeds
after STPEG among critically ill patients.
Poster Session: Epidemiology 1
356
ALL-TERRAIN VEHICLE ACCIDENTS: NINE YEARS OF EXPERIENCE AT A LEVEL 1 TRAUMA CENTER
John Bethea1, Julton Tomanguillo Chumbe2, Damayanti Samanta3; 1Charleston
Area Medical Center, Charleston, WV, 2Charletson Area Medical Center Health
Education and Research Institute, Charleston, WV, 3Charleston Area Medical
Center Health Education and Research Institute, Charleston, WV
Learning Objectives: The popularity of all-terrain vehicles (ATV) in the US
has caused an “epidemic of injuries and mortality” among ATV users. The US
Consumer Product Safety Commission reported 107,500 ATV-related injuries in
2011. The purpose of this study was to examine the impact of safety equipment
and illicit substance exposure on outcomes of ATV accident victims admitted to a
level 1 trauma center. Methods: A retrospective, single center study of ATV accident victims were evaluated from 2005 to 2013. Subjects and data were obtained
from the institution’s Trauma Registry. Appropriate statistical analyses were performed. Results: There were 1,857 ATV crashes resulting in 719 (38.7%) ICU
admissions and 36 (1.93%) deaths. Of the patients requiring ICU admission, 472
(65.6%, p = 0.00) had a positive serum or urine drug screen. Injury Severity Score
(ISS), length of stay (ICU and hospital), and hospital costs were all significantly
higher for patients who had positive toxicology screens upon admission. Mortalities and discharges in a vegetative state were also significantly higher for those
with positive drug screens (3% vs.1%, p = 0.002). Patients who were not wearing
safety equipment were more likely to require ICU admission (86% vs. 14%, p
= 0.00) and had a higher incidence of traumatic brain injury (85.4% vs. 14.6%,
p = 0.000). Hospital length of stay, ISS, and cost of hospitalization were also
significantly higher in this group. Mortality and discharges in a vegetative state
were significantly higher as well (2.4% vs. 0.6%, p = 0.045). Additional analyses
indicated that patients who were positive for substances were approximately 10%
less likely to utilize safety equipment (14% vs. 24.4%, p = 0.00). Conclusions:
Positive drug screens and a lack of utilization of safety equipment were associated
with a significant increase in markers of morbidity and mortality following an
ATV accident. Findings suggest that substance exposure may predispose riders
to be less likely to utilize safety equipment. Accordingly, rigorous efforts should
be made to raise awareness among ATV riders and discourage unsafe practices.
357
SIZE OF SEPSIS IN WALES: FEASIBILITY PILOT
Tamas Szakmany1, Gemma Ellis2, Robert Lundin2, Llaria Pignatelli2, Judith
Hall3, Paul Morgan4; 1Cwm Taf NHS LHB, Llantrisant, United Kingdom, 2Cardiff University, Cardiff, United Kingdom, 3NHS Wales, Cardiff, United Kingdom, 4University Hospital of Wales, Cardiff, United Kingdom
Learning Objectives: The incidence of sepsis on the general wards is unknown
in Wales, whilst sepsis accounts for 30% of all admissions to the ICUs. The introduction of the National Early Warning Score and the Sepsis Screening Tool makes
it possible to estimate the true incidence. We performed a feasibility pilot study to
estimate the incidence of sepsis and severe sepsis on the general wards. Methods:
1 day point prevalence study conducted in 4 hospitals (2 tertiary centres and 2
university affiliated general hospitals) on all general and obstetric wards using an
anonymised pro-forma data collection sheet. Information was obtained by medical students who were trained in recognising the signs of sepsis. All patients with
NEWS 3 or above were screened. Sepsis and severe sepsis was defined according to SSC criteria. Demographics, co-morbidities and significant drug therapy
data was collected along with data on severity of sepsis, organ dysfunction and
applied treatment. Results: 393 patients scored 3 or above on the NEWS. 16% of
patients (n=62) had clinical signs of sepsis and 7.9% of patients (n=29) had severe
sepsis with at least one organ dysfunction. Sepsis patients were similar age: 71
(61-84) years and NEWS 4 (3-6) compared to the non-sepsis patients. M/F ratio
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
was 60/40. 23% of the patients had at least one significant co-morbidities. Out of
the 62 sepsis patients only 4 had received the complete Sepsis 6 bundle. Critical
Care input was obtained only in 5 patients with severe sepsis. Conclusions: The
prevalence of sepsis and severe sepsis is high on the general wards and the problem
is highly unrecognised. The lack of critical care referral of severe sepsis patients
highlights the educational problem on ward level. Despite national effort, the
delivery of the simple and effective Sepsis 6 treatment is lacking. The feasibility
pilot showed that the research model employing the medical students as data
collectors is workable and we are preparing to launch a nation-wide survey to get
a true reflection about the size of the problem in different areas of the country.
358
OVERLAP OF COGNITIVE, PHYSICAL AND MENTAL HEALTH
IMPAIRMENTS IN THE POST-INTENSIVE CARE SYNDROME
Nathan Brummel1, Said Sidiqi1, Pratik Pandharipande2, Jennifer Thompson1,
Eduard Vasilevskis2, Timothy Girard3, E. Wesley Ely1, James Jackson1; 1Vanderbilt University School of Medicine, Nashville, TN, 2Vanderbilt University Medical Center, Nashville, TN, 3Vanderbilt University, Nashville, TN
Learning Objectives: The extent to which impairments in cognitive and physical
functioning and mental illness overlap in post-intensive care syndrome (PICS)
is unclear. Moreover, factors associated remaining free of PICS are unknown.
Methods: We conducted a prospective cohort study of ICU survivors, excluding
those with pre-illness cognitive or physical impairment. At 3 and 12 months after
discharge, we assessed cognition with the Repeatable Battery for the Assessment
of Neuropsychological Status, physical functioning using the Katz Activities of
Daily Living Scale and depression using the Beck Depression Inventory-II. We
then categorized patients into seven mutually exclusive groups, ranging from
no impairments to impairments in all 3 PICS domains. We used logistic regression to model the association between age, education, frailty, and durations of
delirium, severe sepsis and mechanical ventilation with the odds of remaining
free of PICS. Results: Our cohort included 406 patients who were a median 61
(51-70) years old. At 3- and 12-months, 130 (40%) and 101 (35%) survivors,
respectively, were impaired in 1 domain, 61 (19%) and 47 (16%) were impaired
in 2 domains and 19 (6%) and 12 (4%) were impaired in all 3 domains. Years of
education were independently associated with an increase in the odds of remaining free of PICS at both follow-up time points [14 vs 12 years, OR 1.6, 95% CI
(1.3 to 1.9) and OR 1.6 (1.3 to 2.0), respectively]. Conversely, greater frailty was
associated with lower odds of remaining free of PICS at 3 months [vulnerable vs
well, OR 0.6 (0.3 to 0.9)], with a trend towards lower odds at 12 months [OR 0.6
(0.4 to 1.02)]. Finally, duration of severe sepsis was associated with lower odds
of remaining PICS free at 3 months, but not 12 months [0 vs 6 days, OR 0.6
(0.4 to 1.0) and OR 0.9 (0.4 to 1.9), respectively]. Conclusions: Newly acquired
impairments in PICS domains are common after critical illness, but overlapping
impairment in all 3 domains is rare. More education is protective against the
development of PICS, but not modifiable. Identification of modifiable risk factors for PICS is needed.
359
CONTEMPORARY TRENDS OF ICU UTILIZATION AMONG
PATIENTS WITH DEMENTIA: A POPULATION-BASED
COHORT STUDY
Lavi Oud1, Phillip Watkins2; 1Texas Tech University Health Sciences Center,
Odessa, TX, 2Texas Tech University HSC, Lubbock, TX
Learning Objectives: The benefits of intensive care in dementia (D) patients
remain debated, while the number of the affected population continues to
rise; there are no population-level data on the trends of ICU utilization among
patients with a diagnosis of D. Methods: We used the Texas Inpatient Public
Use Data File to identify, using ICD-9-CM codes, patients with a diagnosis of
D among hospitalizations aged ≥65 years, during the years 2001-2010. We then
identified those admitted to ICU among hospitalizations with and without diagnosis of D (ND). US Census data were used for censal and intercensal population
estimates of those ≥65 years over similar period. We then examined trends of ICU
admissions among D hospitalizations vs. the general population, hospitalizations
among ND with and without ICU admission, and overall D hospitalizations.
Regression analysis was used to examine trends. X2 test & descriptive statistics
were reported. Results: There were 876,994 hospitalizations with D, with ICU
admission in 276,056 of those, during study period. The rates of ICU admission
among D hospitalizations rose between 2001 & 2010 from 21.4% to 37.8%
(p<0.0001). The following trends were noted in the number of elderly hospitalizations & general population between 2001 vs. 2010, and their respective annual
changes: D hospitalizations with ICU admission 333% (14%/yr; p<0.0001);
state population 24.4% (2.5%/yr; p<0.0001); all ND hospitalizations -1%
(-0.4%/yr; p=0.0170); ND hospitalizations with ICU admission 26.9% (2.4%/
yr; p<0.0001); all D hospitalizations 87.9% (7.6%/yr; p<0.0001). Conclusions:
The number of ICU admissions among elderly hospitalizations with D rose more
than 3-fold over the past decade, outpacing that of all D hospitalizations, as well
as that of ND hospitalizations with and without ICU admission, and state elderly
population growth. The rate ICU admission among D hospitalizations increased
from 1 in 5 to more than 1 in 3 over the same period. The factors underlying the
observed trends merit further study.
360
LONG-TERM INTENSIVE CARE UNIT (ICU) OUTCOME
TRENDS AMONG A NATIONWIDE COHORT OF TELE-ICU
PATIENTS
Jiachen Zhou1, Omar Badawi1, Erkan Hassan1, Michael Breslow1, Brian Rosenfeld1, Craig Lilly2, Xinggang Liu1; 1Philips Healthcare, Baltimore, MD, 2University of Massachusetts Memorial Medical Center / EICU Support Center,
Worcester, MA
(ED) visits attributed to injuries due to legal interventions. Methods: We performed an analysis of Nationwide Emergency Department Sample for the years
2008-2010 including all ED visits for Injuries due to Legal Interventions (ILI).
Characteristics of patients, ED disposition, and subsequent hospitalization outcomes were examined (Hospital charges [HC], Length of stay [LOS] and inhospital mortality [IHM]). Results:170,599 ED visits were due to ILI. Legal
interventions included: firearms(3.6%), explosives(0.05%), gas(1.1%), blunt
objects (3.8%), cutting and piercing instruments(2.9%), blow or manhandling
(73.4%), unspecified means(14%). Late effects of legal interventions accounted
for 1.7% of all ED visits. Characteristics of ED visit included: age: <18 yrs(9.1%
of all ED visits), 18-29yrs(40.1%), 30-39yrs (23.2%), 40-49yrs(17.4%),
50-59yrs (8%), and >60 yrs(2.1%); males(86%); weekends (33%). Disposition following ED visit included: discharged routinely(87%), admitted to same
hospital(4.3%), transferred to another short term hospital(2.1%) or long term
facility(3%). 459 patients died in the ED. Of the 7373 inpatient admissions,
subsequent outcomes included: discharge routinely(71%), transferred to long
term care (13.4%), discharged to home health care(3.4%), and discharged against
medical advice(3.7%). 144 patients died as an in-patient. Payers included private
insurance(20.3%), Medicare (4.4%), Medicaid(15.6%), uninsured(40%). About
64% resided in areas with low income levels. Close to 39% had multiple injuries.
Mean ED charge was $1,988 and total ED charges was $244.9 million. Amongst
those admitted as inpatients, the mean HC was $57,653 and the total HC was
$422.2 Million. Conclusions: Legal intervention leading to injuries and necessitating medical care is not an uncommon cause of ED visit. Hospital resource
utilization is considerable. Certain high risk groups are identified.
362
CHARACTERISTICS AND OUTCOMES OF CANCER PATIENTS
ADMITTED TO THE INTENSIVE CARE UNIT: A 5-YEAR
STUDY
Lama Nazer1, Awad Addassi1, Dalia Rimawi2, Khaled Jamal1, Feras Hawari1;
1
King Hussein Cancer Center, Amman, Jordan, 2King Hussein Cancer Center,
Amman, Jordan
Learning Objectives: Tele-ICU programs have been associated with lower mortality and shorter length of stay (LOS). However, the impact of tele-ICU on a
large cohort of patients (pts) over a sustained time period is lacking. The goal
of this study was to evaluate changes in ICU outcomes in the years (yrs) following tele-ICU implementation. We hypothesize that the changes in mortality and
LOS are sustained in the yrs following implementation. Methods: Data were
obtained from the Philips eICU Research Institute data repository and represented 307 ICUs managed with tele-ICU program in the United States. The
analysis included pts with an ICU admission between 2004 and the first quarter
of 2014. Patient outcome changes over calendar (2004-2013) yrs were estimated
in multivariable linear/logistic regression models adjusting for APACHE IV
(Acute Physiology and Chronic Health Evaluation IV) prediction. For trends
over yrs since tele-ICU implementation, further adjustment was made for program implementation calendar year after indexing patient unit stays at the time of
tele-ICU implementation. Results: The analysis included 1,115,710 ICU patient
stays. APACHE IV acuity increased continuously as a function of calendar yrs
(2004-2013, APACHE score: 47.0 to 55.0, p<0.001), while actual mortality and
LOS showed continuous decrease (2004-2013, ICU mortality: 6.3% to 5.3%;
hospital LOS: 9.1 to 7.6 days; all p<0.001). The improvements in ICU outcomes
were also evident over yrs since program implementation: after adjustment, multivariable regression models estimated an 18.1% reduction in ICU mortality
and 19.3% reduction in hospital mortality over the first 8 yrs reflecting a 0.16%
(p<0.001) and 0.29% (p<0.001) absolute yearly decrease in respective mortality.
ICU and hospital LOS decreased 17% (2.2 hrs/yr; p<0.001) and 14.2% (4.4 hrs/
yr; p<0.001) respectively. Conclusions:Implementation of a comprehensive ICU
telemedicine program is associated with lower mortality and shorter length of
stay characteristics that continue to improve many years after implementation.
Learning Objectives: This study describes the characteristics and outcomes of
cancer patients admitted to the intensive care unit (ICU) of a comprehensive
cancer teaching center. In addition, it evaluates the impact of the several patientrelated characteristics on mortality. Methods: The ICU database was used to identify all cases admitted to the adult ICU at King Hussein Cancer Center between
January 2009 and December 2013. The demographics and baseline characteristics of those patients were recorded. In addition, we determined the ICU length
of stay, ICU and hospital mortality, as well as 28-day mortality. Univariate and
multivariate analysis were conducted to evaluate the association between ICU
mortality and the following factors: APACHE II, gender, type of malignancy,
admission diagnosis, neutropenia, thrombocytopenia, and mechanical ventilation. Results: Over the study period, we recorded 3371 ICU admissions for
2439 patients. The mean age was 54.3 years ±16.5(SD), mean APACHE II was
20 ± 7.8(SD), the majority of the cases had solid tumor (72.8%), 31.6% had
thrombocytopenia upon admission, and 18.8% had neutropenia upon admission. The most common admission diagnoses were sepsis (n=725, 23.9%) and
respiratory distress/failure (n=868; 28.6%). Mechanical ventilation was required
for 1082 (53.8%) cases. The median length of stay was 3 days (IQR 2-6). ICU
Mortality for the reviewed cases was 36.5% and the majority of the deaths
(72.4%) occurred within the first week of ICU admission. Hospital and 28-day
mortality were reported in 1695 (51.1%) and 1659 (49.2%) cases, respectively.
The following factors were associated with increased ICU mortality: APACHE
II, neutropenia or thrombocytopenia upon admission, mechanical ventilation,
and the ICU length of stay. Conclusions: In an oncology ICU with a closed-unit
model and high intensity staffing, ICU mortality was reported in about onethird of the cases. Thrombocytopenia and neutropenia upon admission were two
cancer-related factors associated with ICU mortality
361
363
INJURIES DUE TO LEGAL INTERVENTION AND EMERGENCY DEPARTMENT VISITS.
INCIDENCE AND OUTCOMES OF ARDS IN RWANDA USING
MODIFIED BERLIN CRITERIA FOR RESOURCE-POOR
SETTINGS
Sankeerth Rampa1, Natalia Martinez-Schlurmann2, Romesh Nalliah3, Veerasathpurush Allareddy4, Karen Lidsky5, Alexandre Rotta6, Veerajalandhar Allareddy6;
1
University of Nebraska Medical University, College of Public Health, Omaha,
NE, 2Rainbow Babies & Childrens Hospital, Cleveland, OH, 3Dental Medicine,
Harvard University, Boston, MA, 4College of Dentistry, University of Iowa, Iowa
City, IA, 5Rainbow Babies & Children’s Hosp., Cleveland, OH, 6Rainbow Babies
& Children’s Hospital, Cleveland, OH
Learning Objectives: Violence necessitating legal interventions is not uncommon, yet outcomes of subsequent injuries are poorly described. We sought to provide a nationally representative estimate of hospital based emergency department
Elisabeth Riviello1,2, Daniel Talmor1, Victor Novack3, Willy Kiviri2, Theogene
Twagirumugabe4, Valerie Banner-Goodspeed1, Laurent Officer1, Robert Fowler5;
1
Beth Israel Deaconess Medical Center, Boston, MA, 2University Teaching Hospital of Kigali, Kigali, Rwanda, 3Soroka University Medical Center, Beer Sheva,
Israel, 4University Teaching Hospital of Butare, Butare, Rwanda, 5Sunnybrook
Hospital, Toronto, ON
Learning Objectives: Incidence and outcomes of the Acute Respiratory Distress Syndrome (ARDS) have not been reported for a resource-poor setting.
We hypothesize that a scarcity of mechanical ventilators, arterial blood gas
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
equipment, and radiographic resources will cause the Berlin definition of ARDS
to underestimate ARDS incidence in a resource-poor setting. Methods:This
single-center prospective observational study screened every adult patient
admitted to a public referral hospital in Rwanda for hypoxemia for four weeks.
For every patient with an oxygen saturation <90% or receiving oxygen, we
collected data on demographics and ARDS risk factors. We evaluated these
patients for ARDS using pulse oximetry, ultrasound, and chest radiograph
when available. ARDS was defined by modified Berlin criteria using a validated
estimate of the PaO2/FiO2 ratio based on oxygen saturation, waiver of the
positive end expiratory pressure (PEEP) requirement, and bilateral opacities
defined as “B lines” or consolidation by ultrasound. We performed testing for
agreement between ultrasound and radiograph findings. Results: 1046 adults
were admitted to the hospital in one month. 126 (12.0%) screened positive for
hypoxemia. Using our modified Berlin criteria, 56 of 1046 patients (5.4%) met
criteria for ARDS. ARDS risk factors were: infection 44.3%, trauma 23.7%,
surgery 22.7%, and stroke 9.3%. Hospital mortality for ARDS patients was
59.3%. Since only 47.9% of all hypoxemic patients had a chest radiograph at
any time during the study, confining the criteria to bilateral opacities on chest
radiograph led to an ARDS incidence of only 2.7%. Requiring a minimum
PEEP level reduced the incidence to 1.1%. Of the 158 patient-days in which
both a chest radiograph and ultrasound examination were available, there was
agreement in 101 (63.9%). Conclusions: Our survey of a referral hospital in
Rwanda suggests that ARDS is a common and fatal syndrome. Use of modified Berlin criteria is necessary to capture all affected patients in resource-constrained settings. These criteria need to be validated in a resource-rich setting
with gold standard comparisons.
Poster Session: Epidemiology 2
364
RACE IS AN INDEPENDENT RISK FACTOR FOR MORTALITY
DURING ECMO FOR RESPIRATORY SUPPORT
Titus Chan1, Jane Di Gennaro1, Reid Farris1, David McMullan1; 1Seattle Children’s Hospital, Seattle, WA
Learning Objectives: Non-Caucasian race has been described as a risk factor
for mortality in patients supported with extracorporeal membrane oxygenation
(ECMO) for cardiac failure. This study aims to determine if racial variations exist
in patients supported with ECMO for respiratory failure. Methods: All adult
and pediatric patients (excluding neonates) in the ELSO registry who received
ECMO for respiratory support between 1989 and 2012 were included and categorized as bacterial or viral pneumonia, ARDS, sepsis, other respiratory disease
and unknown. Logistic regression models examining race/ethnicity and hospital
mortality, adjusting for cannulation site, pre-ECMO acidosis, type of ECMO
support, ECMO complications and year, were constructed. Results: Of 9,812
patients (4001 adults, 5,811 children), Caucasian race was the predominant
racial group (60% in adults, 42% in pediatrics) while Black (8% in adults, 14%
in pediatrics), Hispanic (4% in adult, 9% in pediatric) and Asian (13% in adult,
5% in pediatrics) were the other identifiable race/ethnicities. Multivariate analysis
identified Black race (Odds Ratio (OR): 1.29, 95% Confidence Interval (CI):
1.01-1.66), and Hispanic ethnicity (OR: 1.49; 95% CI: 1.04-2.13) as independent risk factors for mortality in adults. In contrast, Hispanic ethnicity (OR 1.44;
95% CI 1.17-1.79) was associated with mortality in children. Neither Black race
nor Hispanic ethnicity were associated with increased odds of experiencing an
ECMO complication in children or adults. In children, Black race and Hispanic ethnicity were not independent risk factors for prolonged time to ECMO
cannulation, pre-ECMO acidosis, or higher pre-ECMO vasopressor usage. In
adults, Black race was associated with pre-ECMO acidosis (OR 1.44; 95% CI
1.11-1.86) while Hispanic ethnicity was associated with higher pre-ECMO vasopressor usage (OR 2.30; 95% CI 1.48-3.56). Conclusions: Hispanic ethnicity
in children and Hispanic ethnicity and Black race in adults are independently
associated with mortality in patients who require respiratory ECMO. Pre-ECMO
care may influence outcomes in adults.
365
CHARACTERISTICS OF LONG STAY PATIENTS IN PEDIATRIC
INTENSIVE CARE UNITS IN THE UNITED STATES
Orkun Baloglu1, Sergey Tarima2, Shi Zhao2, Matthew Scanlon3; 1The Medical
College of Wisconsin, Milwaukee, WI, 2Medical College of Wisconsin, Milwaukee, WI, 3N/A, Milwaukee, WI
Learning Objectives: Length of stay (LOS) is one of the parameters of cost-effective utilization of intensive care units. Historically, long-stay patients (LSPs) are
defined as patients who stay in pediatric intensive care unit (PICU) longer than
12 days which was calculated as 95th% cut-off of the LOS. In light of advances in
healthcare, it is unclear whether the 12-day cut-off is still accurate. Additionally,
disproportionate use of PICU days by LSPs was reported and predictors of LSP
are largely unknown. Aim of the study was to determine 95th% of length of stay
for PICU patients and determine factors associated with longer LOS in PICUs.
Methods: Retrospective, analytic cohort study. All patients admitted to PICUs in
the Virtual Pediatric Intensive Care Unit Systems (VPS) database from 1/1/2009
to 1/1/2012 and discharged from PICUs between 1/1/2009 and 6/30/2012 were
included in analysis. Patients older than 18 years of age at time of PICU admission or those who were still hospitalized in PICU by 6/30/2012 were excluded.
Intercept only quantile regressions were used to estimate 95%-level quantiles and
their 95% confidence intervals. Logistic regression analyses were performed to
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
determine predictors for LSPs. Results: 224,960 unique patient encounters in
PICUs were identified. The 95th% of LOS for all encounters was 15 days. As the
number of previous PICU admissions increases, the 95th% of LOS for subsequent PICU admissions increases up to 25 days. Age< 1 year, need for mechanical ventilation and renal replacement therapy, being admitted from another
hospital`s PICU, general care floor and step down unit, being post-operative and
trauma status were associated with longer length of stay (p<0.001). Although
LSPs were 5% of all patients, they used 38.8% of all PICU days. Conclusions:
LOS in PICUs has been prolonged compared to historical reported cohorts. 15
days should be used as the new cut off to define LSPs. Disproportionate use of
PICUs by LSPs continues to exist. Risk factors for being LSPs may potentially be
used for better patient allocation and resource use in PICUs.
366
COST ANALYSIS OF THE PANGEA STUDY
Breonna Slocum1, Kenneth Smith2, Robert Clark2, Rudolph Richichi3, Derek
Angus4, Patrick Kochanek5, R Watson6, Ericka Fink7; 1University of Pittsburgh
School of Medicine, Pittsbur, PA, 2University of Pittsburgh, Pittsburgh, PA,
3
Statistical Analysis and Measurement Consultants, Inc., Lanexa, VA, 4University of Pittsburgh Critical Care Medicine CRISMA Laboratory, Pittsburgh, PA,
5
Safar Center for Resuscitation Research, Pittsburgh, PA, 6Children’s Hospital
of Pittsburgh of UPMC, Pittsburgh, PA, 7Children’s Hospital of Pittsburgh,
Pittsburgh, PA
Learning Objectives: Neurological injuries are a leading cause of death and morbidity. We describe hospital costs associated with children admitted to pediatric
intensive care units with 7 types of acquired brain injury (ABI) in 107 centers
(922 subjects) from the PANGEA study. ABI categories included traumatic
brain injury (TBI), stroke, brain mass, cardiac arrest (CA), spinal cord injury,
status epilepticus, and central nervous system (CNS) infection/inflammation. We
hypothesized that hospital costs will differ by ABI category. Methods: ABI type
was matched to corresponding Clinical Classification Software (CCS) code from
the Kids Inpatient Database (KID), assigned by age group and multiplied by
hospital length of stay (LOS). All costs are reported in 2009 U.S. dollars from a
third-party payer perspective. Data are reported as mean ± standard deviation.
Results: CA was associated with the highest hospital cost per day as assigned
by KID ($6,365/day) and had the highest hospital cost of all ABI’s in PANGEA ($282,840± $323,019). Hospital costs were higher if the patient survived
TBI or CA and higher if the patient did not survive stroke, status epilepticus, or
CNS infection. Hospital characteristics were not associated with cost. The Pediatric Index of Mortality 2 was weakly correlated with cost (ρ=0.12, p<0.001). In
multivariate regression, longer hospital LOS, older age, and subjects with white/
Hispanic or ‘other’ race were associated with higher cost (β=0.894, 0.088, 0.033,
and 0.032, p<0.05). Relative to CA, other ABI had lower cost (p<0.001) as well
as children who died (β=-0.039, p<0.05). Conclusions: Children with ABI constitute a cohort that requires significant financial and clinical resources. CA, the
most common ABI, had the longest LOS and hospital cost compared to the
other ABIs. Future work will examine differences in practices and interventions
between countries that could affect costs.
367
EPIDEMIOLOGY OF HOSPITAL BASED ED VISITS DUE TO
AIR & SPACE TRANSPORT ACCIDENTS IN THE USA.
Sankeerth Rampa1, Romesh Nalliah2, Veerasathpurush Allareddy3, Veerajalandhar Allareddy4; 1University of Nebraska Medical University, College of Public Health, Omaha, NE, 2Dental Medicine, Harvard University, Boston, MA,
3
College of Dentistry, University of Iowa, Iowa City, IA, 4Rainbow Babies &
Children’s Hospital, Cleveland, OH
Learning Objectives: Air travel is one of the most common modes of locomotion
in USA. Injuries related to air travel necessitating medical care are poorly described.
We sought to provide nationally representative estimates of hospital based emergency department visits (ED) attributed to air & space transport accidents(AST).
Methods: We performed a retrospective analysis of the Nationwide Emergency
Department Sample(2008-2010). All ED visits with an external cause of injury
code for AST were selected. Characteristics of patients that had AST, ED disposition, and subsequent hospitalization outcomes(Hospital charges-HC, Length
of stay-LOS) were examined. Descriptive statistics were used. The study was
IRB exempt. Results: A total of 12,716 ED visits were attributed to AST. Different AST’s included: accidents to powered aircrafts at takeoff or landing(18.5%
of ED visits), accidents to powered aircraft – unspecified(11%), accidents to
unpowered aircraft (5.5%), fall in(on or from) aircraft(12%), other air transport
accidents (46.6%), and accidents involving space crafts(6.6%). Characteristics of
ED visits include mean age(40.3y), males(64.8%), weekends(37%), and monthsJuly-Sept(31%). 83 patients died in ED while 45 died following hospitalization.
Outcomes following ED visit include discharged routinely(73.7%), admitted as
inpatients (20.5%, N= 2608), transferred to other hospitals(3.1%), mean ED
charges($2,996) & total ED charges across the entire USA($29.1 Million). Outcomes following hospitalization include discharged routinely(63.3%), transferred
to long term facilities (19.7%),discharged to home health care(9.6%), mean HC
($90,239), total HC($233.7 Million), mean LOS(6.1 days) & total hospitalization
days across the entire United States(15,803 days). Close to 39% had multiple injuries. Conclusions: This large epidemiological study describes the national estimates
of Air/space travel injuries necessitating ED visits. Certain risk factors are identified.
AST injuries are associated with considerable hospital resource utilization.
368
EPIDEMIOLOGICAL ESTIMATES OF EMERGENCY DEPARTMENT VISITS ATTRIBUTED TO STORMS & FLOODS
Sankeerth Rampa1, Romesh Nalliah2, Veerasathpurush Allareddy3, Veerajalandhar Allareddy4; 1University of Nebraska Medical University, College of Public
Health, Omaha, NE, 2Dental Medicine, Harvard University, Boston, MA, 3College of Dentistry, University of Iowa, Iowa City, IA, 4Rainbow Babies & Children’s Hospital, Cleveland, OH
Learning Objectives: One of the key components of natural disaster management is to assess the impact of disasters on medical care. We sought to provide
nationally representative epidemiological estimates of hospital based emergency
department visits (ED) attributed to storms and floods. Methods: We performed
a retrospective analysis of the Nationwide Emergency Department Sample(years
2008-2010). All ED visits with an external cause of injury code for “cataclysmic
storms, and floods resulting from storms” were selected. Multiple demographic
characteristics were examined. Outcomes examined included: disposition from
ED, ED charges, and hospitalization outcomes(hospital charges-HC, Length of
stay-LOS, In-hospital mortality-IHM). Descriptive statistics were used. Results:
During the study period, a total of 3,970 ED visits were attributed to storms
and floods. These included hurricanes (2.3%), tornadoes(48%), floods(12.4%),
snow blizzards(10.3%), dust storms (2%), other cataclysmic storms(6.7%), and
unspecified storms and floods (18.2%). ED visit characteristics include: mean
age(38.4y), males(55%), weekends(39%), Southern regions(49.4%), and Midwestern regions(34.7%). Outcomes following ED visit include: mortality in
ED(41 patients), discharged routinely(79.6%), mean ED charge($2,609), total
ED charge across entire USA ($9.5 Million) and admitted as inpatients into
the same hospital(14.2%, N=563). Outcomes of hospitalized patients include:
IHM(21 patients), discharged routinely(56.6%), transferred to another short
term hospital(4.7%) or long term facilities(23.4%), discharged to home health
care(11.5%), mean HC($77,176), total HC across entire USA ($43.4 Million),
mean LOS(6.4 days), and total LOS(3,606 days). Insurance type include private(39.6%), Medicare(14.7%), Medicaid(17.3%), and uninsured(18%). About
67% resided in geographic areas with low income levels. About 37% had multiple
injuries with the injury severity score ranging from a low of 0 to a high of 75.
Conclusions: The present study highlights the impact of certain natural disasters
on medical care. Hospital resource utilization is considerable.
369
DYSNATREMIAS IN CRITICALLY ILL CHILDREN: EPIDEMIOLOGY AND ASSOCIATED OUTCOMES
Gabriel Bredin1, Kevin Bock2, Todd Sweberg3, Meredith Akerman4, James
Schneider5; 1Hospital For Sick Children, Toronto, Canada, 2Long Island Jewish
Medical Center, New Hyde Park, NY, 3Cohen Children’s Medical Center, New
Hyde Park, NY, 4North Shore LIJ Health System, Manhasset, NY, 5Cohen’s Children’s Medical Center, New Hyde Park, NY
Learning Objectives: To describe the incidence of and outcomes associated with
dysnatremia in a large heterogeneous group of patients admitted to a tertiary
PICU. We hypothesize that both hyponatremia and hypernatremia are independently associated with use of mechanical ventilation (MV), longer Pediatric ICU (PICU) Length of Stay (PLOS), Hospital Length of Stay (HLOS), and
mortality. Methods: We retrospectively identified 3746 consecutively admitted
PICU encounters between 8/1/11 and 11/6/13 of which 2301 had ≥1 serum
sodium levels measured. Mann-Whitney U, Fisher Exact, Cochran-Armitage
and/or Spearman correlation test were used to analyze the association of dysnatremia with the outcomes of interest, as appropriate. Dysnatremias were defined
as serum sodium outside 135-145mmol/L. The incidence of dysnatremias were
described, as well as the association with MV, PLOS, HLOS, and mortality.
Results: 61.4% of all PICU encounters had at least 1 sodium value assessed.
973/2301 (42.3%) were dysnatremic during their PICU stay, 532/2301 (23.1%)
had hyponatremia, 650/2301 (28.2%) had hypernatremia and 209/2301 (9.1%)
had both hypo and hypernatremia during their stay. Any dysnatremia at the time
of PICU admission or during the PICU stay was associated with younger age,
smaller weight, longer PLOS and HLOS, and higher PIM2 (all p<0.01). Each
5mmol/L increment in sodium below 135 mmol/L was associated with a significant increase in MV, PLOS, HLOS, and mortality. (p<0.01) Each 5 mmol/L
increment in sodium above 145 mm/L was associated with a significant increase
in MV, PLOS, HLOS, and mortality. (p<0.01) A significant association was
found between severity of hypo- or hypernatremia and worsening outcomes.
(p<0.01) Conclusions:Dysnatremia intially, or at any point during the PICU
stay, is strongly associated with increased MV, PLOS, HLOS and mortality. Furthermore, as the dysnatremia worsens, so does the association with poor outcome.
370
INTERNATIONAL COLLABORATION IN PEDIATRIC CRITICAL CARE RCTS: A SOCIAL NETWORK ANALYSIS
Mark Duffett1, Karen Choong1, Lisa Hartling2, Lehana Thabane3, Deborah
Cook3; 1McMaster Children’s Hospital, Hamilton, ON, 2University of Alberta,
Edmonton, AB, 3McMaster University, Hamilton, ON
Learning Objectives: Our objective was to describe the degree and patterns
of international collaboration among pediatric critical care researchers who coauthored at least one randomized controlled trial (RCT). Methods: We considered coauthors or study sites from 2 or more countries to indicate international
collaboration. We used the Evidence in Pediatric Intensive Care database (epicc.
mcmaster.ca) to identify RCTs, the authors’ affiliations from trial publications
to identify country of origin, and the World Bank’s classification of country
income levels. Results: We included 276 RCTs and 1507 researchers from 35
countries. 54 (19.6%) trials reported international collaboration. Of the 51
(18.5%) trials with coauthors from 2 or more countries, 31 (60.8%) were from
only high-income countries (HIC), 19 (37.3%) were from at least one HIC and
a middle-income country (MIC) or low-income country (LIC) and 1 (2.0%) was
from only a MIC or LIC. 19 (6.9%) trials included study sites in more than 1
country. Although 77 (27.9%) trials included study sites in at least one MIC or
LIC, only 2 (2.6%) of these trials included also included at least one study site
in a HIC. Trials with international collaboration were more often multicentered
(50.0% vs. 11.3%, p<0.001), but not larger (median [IQR] children randomized:
49 [26, 119] vs. 50 [30, 84], p=0.56) than other trials. In a network analysis of
coauthorship, we identified a large cluster of 512 (33.9%) researchers (85.2%
from HIC) publishing 81 (29.3%) of the trials. There were 22 smaller unconnected clusters of researchers publishing a median of 3 (minimum 2, maximum
10) trials each. There were also 106 (38.4%) trials published by researchers who
were not connected by co-authorship to any other researchers. Conclusions: A
minority of trials in pediatric critical care are the product of international collaboration. Co-authorship networks are fragmented. Although there is a large
cluster of researchers who are linked by coauthorship, most trials are conducted
by researchers who have limited or no coauthorship links to researchers who have
published other RCTs.
371
THE INCIDENCE OF VENTILATOR-ASSOCIATED PNEUMONIA IN THE UNITED STATES FROM 2008 TO 2011
Bryan Lizza1, Sean Smith2, Raj Shah2, Curtis Weiss2, Grant Waterer3,2, Richard
Wunderink2; 1Northwestern Medicine, Chicago, IL, 2Northwestern University,
Chicago, IL, 3University of Western Australia, Perth, WA
Learning Objectives: Ventilator-associated pneumonia (VAP) is a frequent nosocomial infection associated with a high degree of morbidity and mortality. Modifications in reporting methods have been developed by the Centers for Disease Control
and Prevention (CDC) to minimize variation in reporting. Early data suggests
these modified definitions may not capture the full disease spectrum. We report
the incidence and epidemiology of VAP in the United States using the Nationwide
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Inpatient Sample (NIS) from the Healthcare Utilization Project (HCUP) developed
by AHRQ. Methods: We queried the NIS database for cases coded for VAP using
the ICD-9 code of 997.31. Data were analyzed according to year from 2008-2011,
representing the years data was available from AHRQ. Incidence rates are reported
per 100,000 persons based upon US census data. Results: From 2008 to 2011,
73,215 cases were coded as VAP in the US. The incidence rate ranged from 1.6 to
7.3 per 100,000 persons across study years. The majority Caucasians and Hispanics
were noted to have a 2-fold lower rate of VAP development compared to African
Americans across study years. The incidence rate for men (8.9-9.6%) was significantly higher than women from 2009 to 2011. A higher rate of documentation of
VAP was noted in the south region of the United States (37.6%) compared to the
northeast (16.6%), mid-west (23.3%) and west (22.7%) regions. The overall rate of
death across cohorts was 19.2% and improved from 2008 (20.8%) to 2011 (18.0%).
Patients aged >80 years accounted for the smallest group of patients (11.3%) but had
the highest rate of death (30.6%, RR 3.71, 95% CI 3.10-4.44, p<0.001) compared
to patients <40 years of age. Rates of death for patients coded with VAP did not
differ significantly according to gender, race, hospital type, or geographic location.
Conclusions: The incidence of VAP has remained stable across study periods with
a trend towards improved rates of death. African Americans may have a higher incidence rate of VAP compared to their Caucasian and Hispanic counterparts. Further
research of the effect of racial disparities on VAP is warranted.
372
CHANGING TRENDS IN THE USE OF VASOPRESSORS IN
INTENSIVE CARE UNIT: A 7-YEAR STUDY
Narat Srivali1, Charat Thongprayoon2, Wonngarm Kittanamongkolchai2, Wisit
Cheungpasitporn2, Aysen Erdogan3, Perliveh Carrera4, Kianoush Kashani2;
Division of Pulmonary and Critical Care Medcine, Mayo Clinic, Rochester,
MN, 2Division of Nephrology and Hypertension, Mayo Clinic, Rochester, MN,
3
Department of Anesthesiology, Mayo Clinic, Rochester, MN, 4Mayo Clinic
Department of Anesthesiology, Rochester, MN
1
Learning Objectives: The use of vasopressors was common in intensive care unit
(ICU). Due to the lack of conclusive evidence in superiority in efficacy among
various types of vasopressors, the choice of vasopressor use mainly depends on the
physician preference. This study aims to describe the prevalence of vasopressor use
and the trend in the use of each vasopressor medication in ICU over the past 7
years. Methods: This is a descriptive study conducted at a tertiary referral hospital.
All ICU admissions, including both medical and surgical ICU, at our institution
between January 2007 and December 2013 were included in this study. The use of
vasopressors within given ICU day (12.00 am – 11.59 pm) during ICU stay was
reviewed. Vasopressors were defined as the continuous intravenous administration
of norepinephrine, epinephrine, dopamine, phenylephrine, or vasopressin regardless of duration and dosage. Results: A total of 52410 unique patients had 72005
ICU admissions in the course of study, (272271 patient*ICU day). Vasopressors
were used in 17767 (24.7%) ICU admissions and on 53898 (19.8%) patient*ICU
day, resulting in a total of 76564 vasopressor day. Vasopressin was used on 21955
(41%), epinephrine on 20958 (39%), norepinephrine on 17919 (33%), dopamine
on 8636 (16%) and phenylephrine on 7096 (13%) patient*ICU day. Over 20072013, there was an upward trend in the use of norepinephrine (the proportion of
ICU day on norepinephrine over total ICU day with vasopressor 0.24 in year 2007
to 0.45 in year 2013), and a downward trend in phenylephrine (the proportion of
ICU day on phenylephrine over total ICU day with vasopressor 0.20 in year 2007
to 0.10 in year 2013). There was no specific trend in the usage of vasopressin, epinephrine, and dopamine. Conclusions: The vasopressors were used in about one
fourth of ICU admission and about one fifth of ICU days. Vasopressin is the most
commonly used vasopressor. The use of norepinephrine is in upward trajectory.
Poster Session: Epidemiology 3
373
SIMULTANEOUS PREDICTION OF MORBIDITY (M), MORTALITY (D), AND INTACT SURVIVAL (S)
Murray Pollack1, Richard Holubkov2, Funai Tomohiko2, Collaborative Pediatr Crit
Care Research Network (CPCCRN),3; 1Children’s National Health System, Washington, DC, 2University of Utah, Salt Lake City, UT, 3Eunice Kennedy Shriver
National Institute of Child Health and Human Development, Bethesda, MD
Learning Objectives: D rates adjusted for physiological status have been the standard for ICU quality assessments for decades. But D is decreasing and therapies
are increasingly focused on reducing M. We hypothesized that M risk, like D risk,
is associated with physiological dysfunction and M, D, and S can be predicted
simultaneously. Methods: Pts. < 18 yrs. in medical/surgical and cardiovascular
PICUs in the CPCCRN were randomly selected. Descriptive information, physiological status (4-hr. PRISM III score) and the Functional Status Scale (FSS) were
collected. M was a ≥ 3 worsening in the FSS. Trichotomous logistic regression was
used to model 3 outcomes at hospital discharge: M, D, and S. The modeling used
development (75%) and validation sets (25%). Results: There were 10,078 pts.
from 7 sites (1252 to 1617 pts./site). Pt. characteristics varied among sites (p<.001
for all comparisons). The crude D rate was 2.7% (site range 1.3% - 5.0%) and
the crude M rate was 4.6% (range 3.3% to 7.7%). Increasing PRISM III scores
were associated with increasing M as well as D risks (p<.001). Modeling PRISM
III vs. the 3 outcomes indicated that M risks increased and then decreased as
high-risk M’s died. Trichotomous logistic regression using variables selected from
univariate M and D odds ratios identified PRISM III and 7 pt. modifiers as independent variables. In the validation set, there were 108 M observed vs. 110.5 M
predicted, and 61 D observed vs. 66.8 D predicted. Trichotomous goodness-of-fit
tests were excellent (p>.20 for both development and validation sets). Discrimination as assessed by the 3-dimensional ROC was also excellent (volume under the
surface of = .49 development and .50 validation sets, chance performance = .17).
Conclusions: New M’s were associated with many of the same factors as D including physiological status. Trichotomous modeling uncovered the phasic association
of M risk with physiological status as well as produced an excellent simultaneous
prediction model for M, D, and S. This unique severity of illness advance is a new
paradigm for critical care outcomes and quality assessment.
Rotta6; 1Rainbow Babies & Children’s Hosp., Cleveland, OH, 2University of
Nebraska Medical University, College of Public Health, Omaha, NE, 3Rainbow
Babies and Childrens Hospital, Cleveland, OH, 4Dental Medicine, Harvard University, Boston, MA, 5College of Dentistry, University of Iowa, Iowa City, IA,
6
Rainbow Babies & Children’s Hospital, Cleveland, OH
Learning Objectives: Lightning injuries have been associated with high mortality and morbidity. Current national estimates and demographics associated with lightning injuries are unclear. We conducted this study to describe
nationally representative epidemiological estimates of hospital-based ED visits
attributed to lightning injuries in United States. Methods: We performed a
retrospective analysis of the Nationwide Emergency Department Sample for
the years 2008-2010 to include all ED visits with an external cause of injury
code for lightning. Outcomes included disposition from ED, ED charges,
and hospitalization outcomes(hospital charges-HC, Length of stay-LOS).
Descriptive statistics were used. Results: During the study period, a total of
4,786 ED visits were attributed to lightning. Characteristics included: mean
age(34.6yrs), males(62%), weekends(27%), months(June:23.8%, July 28.8%,
August 16.7%). Outcomes following ED visit: mortality(18 patients), discharge routinely(84.5%), admitted as in-patients to same hospital(9.2%,
N= 443). Following admission as inpatients, outcomes included: discharged
routinely(76.7%), transferred to another short term facility(5%), long term
facility(8.7%) or discharged to home health care(4.9%). In-hospital mortality included 18 patients following admission. Primary payers included private
insurance(44.9%), Medicare(6%), Medicaid (10%), uninsured (17%). About
58% resided in low income. About 57% of all ED visits occurred in the Southern regions. The mean ED charge was $2,441 and total ED charges across the
entire United States was $11.3 Million. Amongst those who were admitted
as inpatients, the mean HC was $49,430 and the total HC across the entire
United States was $21.88 Million. The mean LOS was 4.8 days and the total
hospitalization days across the entire US was 2,127 days. Conclusions: In this
national ED estimate,lightning injuries were associated with lower mortality rates compared to prior studies, which could be due to appropriate triage,
advances in care or preventive program effectiveness. Certain risk factors and
hospital resource utilization is described.
374
375
EPIDEMIOLOGICAL ESTIMATES OF HOSPITAL BASED
EMERGENCY DEPARTMENT VISITS ATTRIBUTED TO
LIGHTNING.
EFFECT OF METHODOLOGY: DETERMINING DISPARITIES
IN MORTALITY OF TRAUMA PATIENTS BASED ON PAYER
SOURCE
Karen Lidsky1, Sankeerth Rampa2, Natalia Martinez-Schlurmann3, Romesh
Nalliah4, Veerasathpurush Allareddy5, Veerajalandhar Allareddy6, Alexandre
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Gina Berg1, Felecia Lee2, Ashley Hervey2, Robert Hines2, Paul Harrison1; 1Wesley
Medical Center, Wichita, KS, 2KU School of Medicine-Wichita, Wichita, KS
Learning Objectives: Payer source is commonly associated with disparities in
health outcomes. However, because payer source has not been universally defined
in trauma literature nor consistently merged and analyzed, differences in outcome, therefore disparities, may be biased and conclusions inaccurate. The objective was to determine if in-hospital mortality as associated with payer sources
vary based on methodology employed (inclusion/exclusion; referent group in
modeling; categorization of mixed payer [Medicaid: socioeconomic or Medicare:
physiologic reserve definition], and subjective statistical interpretation). Methods: Retrospective, registry study of admitted adult patients between 2005- 2010
at a Midwestern Level I trauma facility was completed to assess in-hospital mortality. Eligible patients were categorized based on payer source, then stratified
by four literature-based definitions: Definition 1-insured [commercially insured
{CI}, Medicare, Medicaid, mixed insured payer sources] and uninsured; Definition 2-CI, publicly insured (PI) [Medicare, Medicaid, mixed payer Medicare/
Medicaid], and uninsured; Definition 3-CI, Medicaid, Medicare, and uninsured;
Definition 4-CI, Medicaid, and uninsured. Results: Only in Definitions 2 and
3, using CI as referent group, was there a difference in mortality: PI (AOR 2.05;
CI 1.2-3.4) and Medicare (AOR 3.41; CI 1.5-7.8). When reclassifying the mixed
payer Medicare/Medicaid according to socioeconomic definition, there was an
increased risk of mortality for Medicaid (AOR 1.86; CI 1.1-3.2) and Medicare
(AOR 2.62; CI 1.3-5.4). When reclassifying into physiologic reserve definition,
there was increased risk of mortality for Medicare (AOR 3.63; CI 1.6-8.2). Conclusions: Variations in methodology culminated in results that could be interpreted with differing conclusions. Payer source varied as a significant variable
depending on literature definition, referent group, and categorization of mixed
payer. To accurately determine disparities in health outcomes, it is critical there
are consistently defined stratification of payer sources.
376
THE ASSOCIATION OF AGE WITH SHORT-TERM AND LONGTERM MORTALITY IN ADULTS ADMITTED TO THE ICU
Raghu Seethala1, Peter Hou1, Susan Wilcox2, Haytham Kaafarani2, Daniel Yeh2,
Imo Aisiku1, J. Perren Cobb2, Jarone Lee2; 1Brigham and Women’s Hospital, Boston, MA, 2Massachusetts General Hospital, Boston, MA
Learning Objectives: Recent studies have demonstrated that the age of ICU
patients is increasing. The significance of this observation is unclear. The literature
is mixed on whether advanced age leads to higher mortality or whether it is due
to the greater number of comorbidities in the aging population. We hypothesized
that increasing age would significantly increase the odds of short-term and longterm mortality after adjusting for comorbidities in patients admitted to the ICU.
Methods: We performed an IRB approved retrospective cohort study of patients
aged 18 or older who were admitted to any ICU over a 5-year period (2007
– 2012) at two urban, academic tertiary care centers. Patients were divided into
four age groups, 18-39, 40-59, 60-79, and ≥ 80. The primary outcomes were
30-day mortality and 360-day mortality. We used multivariate logistic regression
to assess for an association between age group and outcomes adjusting for gender,
race, Charlson Comorbidity Index and Elixhauser index. Odds ratios (ORs) and
95% confidence intervals (CIs) are reported. Results: 57,335 patients were analyzed. 42.8 % were female and the mean age was 64.2 ± 16.1 years. 30-day mortality was 5.9%, 8.6%, 11.8%, and 17.4% for age groups 18-39, 40-59, 60-79
and ≥ 80 respectively (p < 0.001). 360-day mortality was 13.5%, 20.4%, 27.2%,
and 32.8% for age groups 18-39, 40-59, 60-79 and ≥ 80 respectively (p<0.001).
The adjusted 30-day mortality ORs were 1.26 (95% CI 1.10-1.45), 1.57 (95%
CI 1.37–1.80), and 2.51 (95% CI 2.17 - 2.91) for age groups 40-59, 60-79 and
≥ 80 respectively, using age group 18-39 as the reference. The adjusted 360-day
mortality ORs were 1.11 (95% CI 1.01-1.23), 1.20 (95% CI 1.08–1.32), and
1.50 (95% CI 1.35 – 1.67) for age groups 40-59, 60-79 and ≥ 80 respectively,
using age group 18-39 as the reference. Conclusions: We observed an increasing proportion of short-term and long-term death with increasing age after ICU
admission. After correcting for important clinical variables this trend remained.
Further study is needed to assess the contribution of age on outcomes in ICU
patients.
377
years. The aspirated food consisted of bread (n=8), rice cake (mochi) (n = 8),
rice (n = 7), meat (n = 4). Forty-six patients (64%) had witnesses to aspiration.
Fourteen patients had a favorable outcome, which was defined as cerebral performance category scale (CPC) 1 or 2 at hospital discharge. Patients with favorable
outcomes had witnesses (72% vs. 33%, P = 0.0163). Three cases were opened
their airway at the site of aspiration by caretakers and all patients were discharged
with favorable outcomes. Patients with favorable outcomes had significant differences in arterial blood pH (7.33 ± 0.12 vs. 6.97 ± 0.21, P < 0.0001), PaCO2
(44 ± 22 mmHg vs. 85 ± 39 mmHg, P = 0.001), lactate (51 ± 50☐mg/dL vs.
134 ± 56 mg/dL, P < 0.0001); however, no significant difference in PaO2 was
observed (162 ± 117 vs. 148 ± 156 mmHg, P = 0.77). Among 52 patients who
suffered cardiac arrest, 17 survived to hospital discharge. Survival group patients
were more frequently intubated at the site of aspiration (28% vs. 58%, P = 0.021)
and were treated by emergency doctors (15% vs. 50%, P = 0.012) before hospital
admission more than non-survival group patients. All survival group patients had
return of spontaneous circulation before hospital arrival. Conclusions: Patients
of airway obstruction due to food aspiration with favorable outcomes more frequently had witnesses than those with unfavorable outcomes, and cardiac arrest
survivors were intubated more often at the scene. Elderly persons who have a
high risk of aspiration should be observed during meals and caretakers should be
trained for emergency resuscitation.
378
RBC TRANSFUSION RATES WITHIN MECHANICALLY VENTILATED, MEDICAL ICU SHOCK PATIENTS REQUIRING
CRRT
Michael Young1, Rita Bakhru2, DC Files1, Sanjay Dhar3, L Flores1, James Lovato1,
Peter Morris2; 1Wake Forest, Winston Salem, NC, 2Wake Forest, Winston-Salem,
NC, 3Wake Forest, Winston Salem, NY
Learning Objectives: The risk of death within the ICU is influenced by premorbid factors, severity of acute illness & side effects of ongoing treatments. The
need for active kidney replacement treatment for severe kidney injury represents
up to a threefold increase risk of death vs. no acute kidney injury. Methods: We
reviewed all adult patient (pt) admissions over 21 months to a university hospital
medical intensive care unit (MICU) to determine mortality of pts in receipt of
continuous renal replacement therapy (CRRT) for ≥1 ICU day. Additionally,
we sought the relationship between receipt of CRRT and total # red blood cell
(RBC) transfusions within the same hospitalization. Of MICU pts, records were
queried by CPT code and by direct data extraction for demographics, mechanical ventilator (MV), CRRT, & death. Shock was assessed by the administration
of norepinephrine, dopamine, vasopressin, or phenylephrine in a continuous
infusion. Total hospital RBC transfusions were tallied. Results: From Sep 2012
to May 2014, 2976 separate pts required 3599 hospitalizations with ≥1 ICU
day. The % pts requiring MV, pressor agents, or CRRT were 44%, 34% & 5%,
respectfully. The # hospitalizations with combined MV, shock & CRRT were
129 (4%). Mortality was 7% for any MV pt, 9% for any shock pt, & 17% for
any CRRT pt. Mortality for combined MV-shock-CRRT was 21%; age-adjusted
odds ratio of death vs vent alone was 16. The mean RBC transfusions for MVshock-CRRT pts was 7 units/hospitalization. Of 101 (78%) CRRT pts who
received ≥1 RBC transfusion, only 8 (8%) had an ICD-9 code for GI hemorrhage or retroperitoneal hemorrhage. There was no alteration in mortality for
MV-shock-CRRT pts when reviewed over time by quarter. Conclusions: CRRT
was overall uncommon but associated with a high mortality particularly in MVshock-CRRT pts. RBC transfusions occurred in a majority (78%) of these pts.
Lack of GI/retroperitoneal hemorrhage may represent opportunity for improved
filter-access management to reduce blood loss. Prospective filter-access management studies may show reductions in RBC transfusions in this high mortality
MICU pt subset.
379
A MODEL TO PREDICT DURATION OF VENTILATION
AND 30-DAY MORTALITY IN PATIENTS WITH TRAUMATIC
INJURIES
WITNESSES AND INITIAL RESPONSE ARE CRUCIAL FOR
POSITIVE OUTCOMES IN PATIENTS ASPIRATING FOOD.
Ed Barnard1, Vikhyat Bebarta2; 1University Hospital Birmingham NHS Foundation Trust, Barnstaple, United Kingdom, 2San Antonio Military Medical Center/
US Army ISR, San Antonio, TX
Learning Objectives: Rapid aging of the population is a large problem in Japan.
The number of patients with food aspiration has been growing. Methods: The
objective is to clarify the risk factors affecting the outcomes in elderly patients
with airway obstruction due to food aspiration who are transferred to the tertiary
emergency center. Results: Among 72 patients, the mean age was 80.2 ± 13.5
Learning Objectives: Scoring systems are widely used in civilian practice to predict intensive care patient outcomes. Tools to predict outcomes from combat
trauma are not available; specifically prediction tools for aeromedical evacuation
from theater. The objective was to identify pre-flight variables associated with an
increased requirement for ventilation time and 30-day mortality. Methods: This
IRB-approved, retrospective cohort study included all patients evacuated from
combat theaters by the U.S. Air Force Critical Care Air Transport Team (CCATT)
between 2007 and 2011. Pre-flight physiological variables and treatments were
Yoshino Yudai1, Yutaka Igarashi1, Hiromoto Ishii2, Jun Hagiwara2, Shoji Yokobori2, Tomohiko Masuno2, Akira Fuse2, Hiroyuki Yokota2; 1N/A, Tokyo, Japan,
2
Nippon Medical School, Tokyo, Japan
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
assessed for associations and examined in stepwise regression models. The primary outcome was total ventilator time (≤72 hours vs >72 hours); the secondary
outcome was 30-day mortality. Receiver operating characteristic (ROC) curves
were produced for both outcomes. Data are presented as percentages, median
[IQR], and odds ratio (OR [95% CI]). Results: 1308 combat trauma patients
(24 years, 98% male) were included: 72% blast, 17% penetrating, 9% blunt, and
2% burns. Pre-flight systolic blood pressure was 121 [109-143] mmHg, pulse 100
[84-116] bpm, and base deficit 0 [-2-2]. The median number of blood products
administered pre-flight were 4 [0-13] units packed red blood cells (PRBC), and
3 [0-12] units fresh frozen plasma. When modeling for ventilator time, injury
severity score (ISS) (OR 1.04 [1.03-1.06]), pre-flight PRBC units transfused (OR
1.05 [1.04-1.07]), and pre-flight intubated status (OR 11.9 [8.53-16.89]) were
independently associated with increased ventilator days. A composite of the variables produced an AUC of 0.85 with 86% sensitivity and 56% specificity. Using
mortality as the outcome, ISS (OR 1.06 [1.03-1.09]), prothrombin time (OR
2.13 [1.18-4.47]), pre-flight intubated status (OR 9.2 [1.88-166.11]), and whole
blood (OR 3.18 [1.38-7.04]) were associated with death. The combination of
variables produced an AUC of 0.84 with 71% sensitivity and 57% specificity.
Conclusions: In our large study of critical care aeromedical patients a number of
pre-flight variables are a
380
OUTCOME OF BONE MARROW TRANSPLANTATION IN
CHILDREN: AN ANALYSIS OF KID’S INPATIENT DATABASE.
Mahreen Siddiqui1, Madhuradhar Chegondi2, Balagangadhar Totapally1; 1Miami
Children’s Hospital, Miami, FL, 2Miami Children’s Hospital, Miami,FL
Learning Objectives: Bone marrow transplant (BMT) is used as treatment
for various malignant and non-malignant conditions. Outcome of BMT procedure depends on various factors including the patient’s condition and the
type of transplant (allogeneic, autologous, or cord blood). The objective of this
study was to evaluate demographics and outcomes of children who received
BMT procedure using Kid’s Inpatient Database (KID) during 2009. Methods: We have filtered all patients from the KID using ICD codes for BMT and
analyzed the data. We evaluated various parameters such as age, gender, race,
comorbid diagnosis, mechanical ventilation, type of BMT and their effect on
mortality and length of stay (LOS). To obtain the nationally representative
estimates of the procedure, discharge weighting was applied towards the data.
Chi-square test and student t-test were used to analyze the data. Results: A
total of 2656 children received BMT during 2009. Mean age was 8.62 years
and females were 41%.Most cases of patients who received BMT were Caucasians (47%), followed by Hispanics (16%) and African American (10 %).
Children requiring mechanical ventilation were younger (7yrs), had a longer
LOS (78 vs 40 days; p<0.001), had more co-morbid conditions and higher
mortality (58% vs. 2.8%; p<0.001). Presence of renal failure increased mortality (39% vs. 5.7%; p<0.001). Most common type of BMT was Allogeneic
(47%) followed by autologous (40%) and cord blood (12%). Children with
cord blood BMT were younger (7.4 vs. 8.7 yrs.), had APRDRG extreme risk of
mortality (19%, P<0.001) compared to allogeneic (10%) or autologous (5%),
had longer LOS (65 days, P<0.001), and higher mortality (17%, P<0.001).
Lowest mortality was seen in autologous group (1.5%). Conclusions: Our
study analyzes children who received BMT during a year using a large national
data base. Overall hospital mortality of BMT procedure is 6.2% and is higher
in patients who received mechanical ventilation, had renal failure or received
cord blood.
Poster Session: Epidemiology 4
381
NEW PROGNOSTIC PREDICTION SYSTEM IN CRITICAL
CARE BASED ON NETWORK ANALYSIS
Toshifumi Asada1, Yuta Aoki2, Kent Doi2, Naoki Yahagi3; 1N/A, N/A, 2Tokyo
University Hospital, Tokyo, Japan, 3The University of Tokyo Hospital, Tokyo,
Japan
Learning Objectives: Several prognostic scoring systems including APACHE II
score have been developed and widely used. However, the accuracy and generalizability is not sufficient. This is partly because these systems evaluate each organ
separately although the measured variables used in the scoring systems reflect the
interactions of each organ or biological response. We hypothesized that network
analysis of the interaction of the measured variables will enable to develop a better
prognosis perdiction. Methods: Patients 18 years of age or older who had been
admitted to our intensive care unit at the University of Tokyo Hospital during 9
months were included. 17 clinical variables were analyzed using network analysis.
Variables with high betweenness centrality were detected by calculating Spearman’s rank correlation coefficient, adjusted with Bonferroni correction. Association of the indentificial variables with high betweenness centrality (“hubs”)
with the clinical outcomes were further evaluated by multivariate regression and
receiver operating characteristic analysis. Results: NT-proBNP, %prothrombin,
hemoglobin, NGAL (a new AKI biomarker), platelet count and serum albumin
had significantly high centralities and were identified the “hubs” in the network.
The area under the ROC curve (AUC-ROC) of outcome prediction with these 7
variables was significantly higher as compared with that APACHE II score (AUCROC=0.911, IQR 0.798-0.964 vs. 0.790, IQR 0.676-0.873, p=0.0491). Conclusions: Network analysis could identify several clinical “hubs” that enable to
predict prognosis in critically ill patients with high accuracy.
382
PATIENT-SPECIFIC RISK MODEL OF BACTERIAL CO-INFECTION IN CHILDREN WITH SEVERE VIRAL BRONCHIOLITIS
Michael Spaeder1, Refik Soyer2; 1Children’s National Medical Center, Washington,
DC, 2The George Washington University School of Business, Washington, DC
Learning Objectives: Up to 24% of children hospitalized with viral lower
respiratory tract infection (LRTI) will require admission to the intensive care
unit. Among children with respiratory failure from LRTI caused by respiratory
syncytial virus (RSV), between 17% and 39% will develop pulmonary bacterial
co-infection yet nearly all will receive antibiotics. We sought to reduce antibiotic overuse in children with LRTI by identifying those patients at low risk of
bacterial co-infection through the use of a patient-specific risk model. Methods:
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Retrospective cohort study of children with laboratory confirmed RSV LRTI
requiring mechanical ventilation over a two-year period. Bacterial co-infection
was defined using previously published microbiological criteria. Multiple candidate variables were assessed for association with co-infection and potential
inclusion in the final model. Model was constructed using a weighted partial
correlation method. Model output of risk was assessed using receiver operating
curve (ROC) characteristic analysis. Results:Forty-five patients were included in
the study, 19 (42%) with bacterial co-infection (four (9%) with probable infection, 15 (33%) with possible infection). Candidate variables associated with coinfection: elevated white blood cells (WBC) for age, Gram stained (GS) WBC
and bacteria (both ordinal variables). By partial correlations, weighted values for
each model variable were elevated WBC (13%), GS WBC (52%), and GS bacteria (35%). By ROC analysis, optimal model cut-offs correctly classified 94%
of patients with an area under the curve of 0.83. Model would have decreased
unnecessary antibiotic use in 18-51% of patients. Conclusions: Patients with
RSV LRTI at low risk for bacterial co-infection can be identified using mathematical models, potentially decreasing antibiotic overuse. Efforts to expand
patient-specific modeling to other respiratory viruses are needed.
383
PATTERN OF HOSPITAL ADMISSIONS AND OUTCOME
OF ACUTE ALUMINIUM PHOSPHIDE POISONING IN AN
INDIAN ICU
RANVIR SINGH1, diptimala agrawal2, vivek badada3, anirbhanhom chaudhary4, arushi goel5, mayank jain6, Rakesh Tyagi7; 1Indian Society of Critical Care
Medicine, AGRA, India, 2pushpanjali hospital and research center, agra, DC, 3s
n medical college, agra, agra, India, 4g.b.pant hospital, new delhi, India, 5subharti
medical college merrut, merrut, India, 6pushpanjali hospital and research centre,
agra, India, 7Pushpanjali Hospital & Research Centre, Agra, India
Learning Objectives: Acute aluminium poisoning is a major problem in India.
This retrospective study was undertaken to describe the epidemiological features
of aluminium phosphide poisoning in all patients who were admitted in Pushpanjali Hospital, Agra, India. The specific objectives included the determination
of the age range most vulnerable, the annual pattern of occurrence, the clinical
features at the time of presentation, duration and course of ICU stay and the outcome Methods: Data was extracted from the medical records of 62 patients with
aluminium phosphide poisoning admitted between January 2009 and March
2014. Results: 62 patients were admitted for suicidal poisoning. The age ranged
from 14 years to 63 years. Females of age group 20 to 35 years accounted for 37
(59.6%) cases. There were 21 males and 41 females with a male: female ratio of 1:
2. Forty seven (75.8%) out of 62 patients were from low social backgrounds. Ga
strointestinal symptoms (nausea, vomiting) dominated the clinical presentation
in 39 (62.9%) patients followed by respiratory distress in 9 (14.5%) and unconsciousness in 7 (11.2%) patients. Sixty patients (96.7%) were admitted in the
ICU and out of them 44 (70.9%) required mechanical ventilation. Fifty patients
(80.6%) were in shock despite adequate fluid resuscitation and required adrenaline and dobutamine.36 patients (58.0%) died during the course of ICU stay.
The cause of death was heart failure in all cases. Thirty four (54.8%) patients had
severely low bicarbonate levels (< 10 mmol/L). The mean duration of ICU stay
was 0.86 ± 1.2 days. Conclusions: Aluminium phosphide poisoning is an important cause of mortality in Indian ICU. The young females of the age group of 20
to 35 years are the most vulnerable group. A majority of the patients remain in
shock despite fluid resuscitation and require vasopressors and mechanical ventilation. Cardiac failure is the most common cause of death.
384
ELIXHAUSER COMORBIDITY INDEX BETTER PREDICTS
ICU MORTALITY THAN CHARLSON COMORBIDITY INDEX
Kevin Zhao1, Karim Ladha1, Sadeq Quraishi2, Christopher Tainter1, Raghu
Seethala3, Haytham Kaafarani1, Matthias Eikermann4, Jarone Lee1; 1Massachusetts General Hospital, Boston, MA, 2N/A, Boston, MA, 3Brigham and Women’s
Hospital, Boston, MA, 4Departmnt of Anesthesia, Critical Care, and Pain Medicine, Boston, MA
Learning Objectives: The Charlson and Elixhauser comorbidity indices have
been used to predict long-term mortality based on patient comorbidities from
admistrative databases, but have not been well studied among ICU patients. The
objective was to test whether both comorbidity indices were adequate predictors of ICU survival and if one index was superior to the other. Methods: An
electronic chart review of all admissions to the ICU at two major academic centers from January 2007 to December 2011, totaling 59,816 admissions across
12 ICUs. Receiver operator curves were constructed for both the Charlson and
Elixhauser indices at 30, 90, 180, and 365 days. Results: The average Charlson Comorbidity Index score was 7.22 (SD 3.80) and the average Elixhauser
Comorbidity Index score was 16.30 (SD 11.60). At 30-days, the ROC area for
the Charlson index was 0.65 while the ROC area for the Elixhauser index was
0.66 (p = 0.0148). These ROC areas improved at one year to 0.72 for Charlson
and 0.72 for Elixhauser (p = 0.46). Conclusions: Both the Elixhauser and Charlson comorbidity indexes predict mortality among ICU patients at 365 days with
ROC values >0.70. Elixhauser outperformed Charlson at predicting mortality at
30, 90, and 180 days, but they were both equally predictive at 365 days.
385
TOXIC COLITIS: SURGICAL OUTCOMES AND RISK FACTORS FOR MORTALITY.
Anand Dayama1, Dordaneh Sugano2, Melvin Stone2, John McNelis3; 1Jacobi
Medical Center,, NY, 2Jacobi Medical Center, Bronx, NY, 3N/A, Bronx, NY
Learning Objectives: Toxic colitis (TC) is a potentially lethal complication of
inflammatory bowel disease and infectious colitis. Intensive medical management
is the first line of the treatment however; surgical salvage remains the cornerstone
treatment in medically refractory patients. We aim to evaluate surgical outcomes
of TC and clinical factors associated with mortality. Methods:National Surgical
Quality Improvement Project, a national data set which includes data from >300
hospitals, was queried to identify emergent colectomies for a primary diagnosis
toxic colitis using ICD-9 codes. Thirty-day postoperative mortality and other
postoperative complications were identified as the study end point. We performed multivariate logistic regression analyses to study clinical factors associated
with 30-day mortality. Results: Out of 95 TC patients, 85.3% were in sepsis
preoperatively; 53.7% were in ASA IV class and 9.5% in ASA V; 33.7% patients
were on chronic steroids. Mean time for operation from admission was 6 days.
Mortality for colectomy was 24.2%; 16.8%-experienced renal complications;
14.7% wound complications; 22.1% sepsis complication; 43.2% pulmonary
complications and 17.9% experienced cardiovascular complications. Our multivariate analysis demonstrated advancing age, uremia, respiratory failure with
ventilator dependence and malnutrition as a strong predictor of mortality with
concordance index 83%. Conclusions: Patients with toxic colitis are very ill.
Surgical options should be considered earlier in the management.
386
RETROSPECTIVE MULTICENTER STUDY OF IN-HOSPITAL
CARDIOPULMONARY ARREST (CPA) IN JAPAN
Shinsuke Fujiwara1, Shigeki Fujitani2, Koike Tomotaka3, Megumi Moriyasu3,
Kazuaki Atagi4, Masashi Nakagawa5, Takamitsu Kodama6; 1Ureshino Medical
Center, Ureshino City, Saga Pre, Japan, 2St Marianna University, Kawasaki-city,
Kanagawa, 3Kitasato University Hospital, Sagamihara, Japan, 4Nara Medical
University, Kashihara-city, Japan, 5Social Insurance Kinan Hospital, Tanabe-ckty
Wakayama, Japan, 6University of Texas Southwestern Medical Center, Dallas, TX
Learning Objectives: RRS has been implemented internationally and studies
to improve clinical outcomes has been reported. In Japan, RRS is also gradually
spreading. However, the data of in-hospital CPA is limited in order to compare
before and after introduction of RRS. Therefore, a multicenter study to evaluate
in-hospital CPA before and after introducing RRS was conducted. Methods: 10
facilities were selected to extract one year of the date of in-hospital CPA before
and after introducing RRS. Data were collected using three keywords from DPC
(Diagnosis Procedure Combination) data; “closed-chest compression”, “epinephrine” and “defibrillation”. Patients who were under 18-year-old, and who became
cardiac arrest in ER and ICU were excluded. Possible preventable death was evaluated by 2 board certified physicians of Japanese Acute Care Medicine. Results:
A total of 228 cases in 10 facilities were collected. Average age was 72.8 ± 13.0
years old. Ratio of male/female was 1.78(146/82). Survival ratio with hospital
discharge was 7.0%. Ratio of possible preventable death was 7% (16/228) and
varied from 3.2% to 30.0%. Medical safety issues were found in 8%(17/228).
Abnormal vital signs was found in 63.3%(138/216). Conclusions:Cases with
abnormal vital signs were observed before CPA accounted for about 60%. RRS
might decrease the ratio of possible preventable death.
387
HOSPITAL BASED EMERGENCY DEPARTMENT VISITS DUE
TO RAPE: A PUBLIC HEALTH ISSUE.
Sankeerth Rampa1, Veerajalandhar Allareddy2, Romesh Nalliah3, Veerasathpurush Allareddy4; 1University of Nebraska Medical University, College of Public
Health, Omaha, NE, 2Rainbow Babies & Children’s Hospital, Cleveland, OH,
3
Dental Medicine, Harvard University, Boston, MA,4College of Dentistry, University of Iowa, Iowa City, IA
Learning Objectives: The impact of rape on medical care and outcomes is
unclear. We sought to provide nationally representative epidemiological estimates
of hospital based emergency department visits (ED) attributed to rape. Methods:
We performed a retrospective analysis of the Nationwide Emergency Department
Sample(years 2008 to 2010). All ED visits with an external cause of injury code
for rape were selected for analysis. Characteristics of patients, ED disposition, and
subsequent hospitalization outcomes including hospital charges(HC), Length of
stay(LOS)were examined. Results: During the study period, a total of 49,047
ED visits were attributed to rape. Females comprised 94.7% of all ED visits. Age
groups included: <18 yrs(28.9% of all ED visits), 18 to 29 yrs (42.3%), 30 to 39
yrs (15%), 40 to 49 yrs (9.5%), 50 to 59 yrs (3.2%), and >60 yrs (1.3%). About
34% of all ED visits occurred over weekends. 28% of all visits occurred between
July to September. Following an ED visit, 89.1% were discharged routinely, 4.2%
were admitted as in-patients, 2.1% were transferred to another short term hospital, and 1.4% were transferred to a long term facility. Following admission as
in-patients (total N=2,080), 79.8% were discharged routinely while 11.7% were
transferred to long term facilities, 2.5% were discharged to home health care,
and 3% were discharged AMA. 18 patients died in hospital following admission
as an in-patient. Primary payers included private insurance(25.9%), Medicare
(3.8%) and Medicaid (25.5%). About 22% were uninsured. About 65% resided
in geographical areas with low income levels. Close to 24% had multiple injuries.
The mean ED charge was $2,034 and total ED charges across the entire USA
was $85.5 Million. Amongst those who were admitted as inpatients the mean
HC was $31,588 and the total HC across the entire USA was $65.1 Million.
The mean LOS in hospital was 5 days and the total hospitalization days across
the entire USA was 10,349 days. Conclusions: Rape is a significant cause of ED
visitation and is a public health issue. High risk groups are identified. Hospital
resource utilization is substantial.
388
EPIDEMIOLOGICAL STUDY FOR CASES WITH IRREVERSIBLE HYPOXIC ENCEPHALOPATHY AND BRAIN DEATH
Wakatake Haruaki1, Shigeki Fujitani2, Yuka Kitano3, Yasuhiko Taira4; 1St. Marianna University, Kawasaki-Shi, Kanagawa-Ken, 2St Marianna University, Kawasaki-city, Kanagawa, 3St. Marianna University School of Medicine, Emergency
and Critical Care Medicine, Kanagawa, Japan, 4St. Marianna University School
of Medicine, N/A
Learning Objectives: In Japan, despite Japanese Association for Acute Medicine
end of life care guideline in 2007, many physicians are reluctant to withdraw
of life support care even patients have own living will. The epidemiological and
economical data of irreversible hypoxic encephalopathy (IHE) after CPA and
brain death in Japan is limited. Our objectives are to elucidate the epidemiological prognosis and the impact to medical expense for cases with IHE secondary to CPA and brain death. Methods: All cases with IHE secondary to CPA
and probable brain death secondary to CPA or CVA were recruited from April,
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
2008 to April, 2014(study ongoing). Primary outcome was overall mortality and
functional prognosis during hospitalization in each group. Secondary outcomes
were length of stay (LOS) in ICU after diagnosis, LOS of hospitalization after
diagnosis, and medical expense. Results: Total cases with 215 were reviewed:
150 cases with CPA survivors, 47 with intrinsic cerebral hemorrhage, 16 with
extrinsic cerebral hemorrhage, and one with cerebral infarction and one with
encephalitis. Average age was 65.3 years old. Cases were composed of 81 cases
of brainstem reflex positive, 129 cases of brainstem reflex negative, and only 5
cases with legal brain death. Median LOS of hospitalization after diagnosis for
brainstem reflex positive cases was 6.5 days, while that of brainstem reflex negative was 2 days (p<0.01). 58 cases were solicited for organ donation and organ
donation were performed in17 cases. Average expense per case was 17,850 US
dollar. Only 10 % of cases were desired for withdrawal and only half of 10% had
actual withdrawal from life support care. Conclusions: Clinical function and life
prognosis for most of cases with brainstem reflex positive were poor as previously
reported studies. In Japan, it is not yet socially accepted to withdraw life support
care, which indicates only few percentage of patients/family are given options of
medical withdrawal by physicians.
Poster Session: Ethics/End of Life/Palliative Care 1
389
VARIABILITY IN END-OF-LIFE PRACTICE AMONG U.S. TERTIARY CARE PEDIATRIC INTENSIVE CARE UNITS (PICUS)
Kathleen Meert1, Linda Keele2, Amy Clark2, Collaborative Pediatric Critical Care
Research Network3; 1Wayne State University, Detroit, MI, 2University of Utah,
Salt Lake City, UT, 3Eunice Kennedy Shriver National Institute of Child Health
and Human Development, Bethesda, MD
Learning Objectives: In the U.S., most pediatric deaths occur in intensive care
settings. Our objective is to describe the extent of variability in end-of-life practice
among PICUs affiliated with the seven tertiary care clinical centers comprising the
NICHD Collaborative Pediatric Critical Care Research Network (CPCCRN).
Methods: We conducted a secondary analysis of data prospectively collected
from a random sample of patients (n=10,078) admitted to CPCCRN-affiliated
PICUs between December 4, 2011 and April 7, 2013.1 Patients were eligible
for inclusion during the first PICU admission of their hospital stay; moribund
patients were excluded. Data are expressed as absolute counts and percentages
(overall and range across sites), and means and standard deviations. We evaluated
the association between key characteristics and site using Pearson chi-square or
Fisher’s exact test. Results: 275 (2.7%, range across sites 1.3%-5.0%) patients
(age 4.5 ± 5.6 years) died during their hospital stay; of these, 252 (92%, 76%100%) died in a PICU. Discussions with family regarding limitation/withdrawal
of support (LWS) were documented during the initial PICU stay for 173 (63%,
47%-76%, p=0.27) patients who died. Of these, palliative care was consulted
for 67 (39%, 12%-46%); pain service for 11 (6%, 10 of which were at a single
site); and ethics committee for 6 (3%, from 3 sites). Mode of death did not differ
significantly by site (p=0.57) and was LWS for 187 (68%, 56%-76%) patients,
failed CPR for 53 (19%, 12%-28%), and brain death for 35 (13%, 8%-20%).
Organ donation was offered for 101 (37%, 17%-88%, p<0.001) patients; of
these, 20 (20%, 0%-64%) donated. 62 (23%, 10%-53%, p<0.001) deaths were
deemed medical examiner (ME) cases. Of non-ME cases (n=213), autopsy was
requested for 79 (37%, 17%-75%, p<0.001). Of autopsies requested, 53 (67%,
50%-100%) were performed. Conclusions: Across CPCCRN-affiliated PICUs,
most deaths occur after life support has been limited or withdrawn. However,
wide practice variation exists in requests for organ donation and autopsy. 1Pollack
MM, et al. JAMA Pediatr 2014
390
USE OF ICU DURING END-OF-LIFE HOSPITALIZATIONS OF
PATIENTS WITH DEMENTIA: A POPULATION-BASED STUDY
Lavi Oud1, Phillip Watkins2; 1Texas Tech University Health Sciences Center,
Odessa, TX, 2Texas Tech University HSC, Lubbock, TX
Learning Objectives: The benefits of intensive care among dementia (D) patients
remain debated, while their number continues to rise; there are no populationlevel data on the use of ICU during end-of-life (EOL) hospitalizations among
patients with a diagnosis of D. Methods: We used the Texas Inpatient Public
Use Data File to identify, using ICD-9CM codes, patients with a diagnosis of
D among hospitalizations aged ≥65 years during the years 2001-2010, & identified those admitted to ICU. We defined EOL hospitalizations as those with
either hospital death or discharge to hospice (H). We then examined the rates
of ICU admission among D hospitalizations and use of ICU among EOL hospitalizations. Regression analysis was used to examine trends. X2 test & descriptive statistics were reported. Results: There were 876,994 hospitalizations with
D, with ICU admission in 276,056, and 84,843 EOL hospitalizations during
study period. The rates of ICU admission among D hospitalizations rose between
2001 & 2010 from 21.4% to 37.8% (p<0.0001). Among EOL hospitalizations, the rate of ICU admission between 2001 & 2010 rose from 31.1% to
50.2% (p<0.0001) [6.2%/yr (p<0.0001)]. When only hospital mortality rate
was examined, no change was noted among D hospitalizations with ICU admission (-1.4%/yr; p=0.1764), while their rate of EOL hospitalizations rose 4.5%/
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
yr (p=0.0002). The rate of discharge to H among EOL hospitalizations admitted
to ICU rose from 15.8% to 51.9% (p<0.0001) between 2001 & 2010. Conclusions: Use of ICU rose overall & reached 1 in 2 over the past decade among
EOL D hospitalizations. Use of H rose markedly among EOL hospitalizations
admitted to ICU, likely reflecting increase in EOL discussions by their clinicians. Trends of hospital mortality can be misleading among D hospitalizations
as a measure of EOL hospitalizations. The prevalent use of ICU among EOL D
hospitalizations in our cohort underscores the need to improve our understanding about D patients who are likely to benefit from critical care interventions.
391
THE IMPACT OF ADVANCED DIRECTIVES ON NON-SURVIVORS WHO ARE INTUBATED IN THE EMERGENCY
DEPARTMENT
Lawrence DeLuca1, Donald Davidson2, Tyler Durns2, Erik Gerlach2, Kurt Denninghoff3; 1University of Arizona Dept. of Emergency Medicine, Tucson, AZ,
2
University of Arizona, Tucson, AZ, 3Emergency Medicine, Tucson, AZ
Learning Objectives: Patients who are intubated in the Emergency Department
(ED) have a high rate of mortality prior to hospital discharge. It is not known
what the impact of advance directives are on this mortality. We sought to characterize the proportion of patients who were non-survivors who received a full code
or whose resuscitative efforts were limited by a Do Not Resuscitate (DNR) order
and/or withdrawal of care. Methods: This study was performed in an academic
emergency medicine department and Level I trauma center with an annual ED
census of 77,000. A cohort of patients intubated in the ED who died before
hospital discharge was identified. The proportion of patients who received at least
one code, had a DNR, and who had care withdrawn were calculated. It was possible for patients to be in multiple groups depending upon their hospital course.
Injuries and illnesses that frequently occurred were identified and the relative
rates of full codes (CODE) to withdrawals of care (WD) were described. Results:
A total of 547 patients were identified, with 151 non-survivors (28% mortality).
Twenty-eight patients were excluded for incomplete documentation, leaving 123
patients in the final analysis. 63/123 (51%) were trauma patients. Eighty-nine
patients (72%) died within the first 48 hours after admission. Forty-nine patients
(40%) received at least one code (CODE), and 72 (59%) ultimately had care
withdrawn (WD). Twenty-one (17%) had a DNR order placed at some point
during their hospital course. Motor vehicle accidents (15 CODE, 12 WD), falls
(1 CODE, 9 WD), ICH (2 CODE, 8 WD), and septic shock (4 CODE, 12
WD) were among the most common presenting illnesses. Conclusions:Among
patients intubated in the ED who are non-survivors, the vast majority expire
within 48 hours. The majority of patients who expire after intubation in the ED
ultimately have care withdrawn. Non-survivors intubated in the ED for septic
shock, intracranial hemorrhage, and falls were more likely to have care withdrawn
than to have expired during a code.
392
IMPROVING ACCESS TO PALLIATIVE CARE SERVICES IN
THE PEDIATRIC ICU.
Jeffrey Lutmer1, Kelli Kurtovic2, Tanya Maria Kempton2, Lisa Humphrey2;
1
Nationwide Children’s Hospital, Columbus, OH, 2Nationwide Children’s Hospital, Columbus, United States
Learning Objectives: While critically ill pediatric patients should be screened for
unmet palliative care (PC) needs, we perceived these services were under-utilized
in our PICU. We designed a quality improvement (QI) project to prospectively
screen for and improve access to PC services in our unit. We hypothesized that
a unit-specific PC consultation trigger list would improve access to PC services
in our PICU. Methods: Utilizing QI methodology, we identified key drivers focusing on PC education, staff communication, and early identification of
PC-eligible patients. Using an iterative plan, do, study, act (PDSA) approach,
PICU and PC faculty developed screening criteria that were piloted and revised
until consensus was obtained. PC triggers focused on severe, potentially life limiting conditions, e.g. devastating traumatic and hypoxic-ischemic brain injury,
progressive oncological disease, and severe chromosomal anomalies. Using a consultation-based integration method, the PICU clinical care coordinator screened
the PICU census daily and sought consults for eligible patients. Results: During
the first quarter of implementation, 45/623 (7%) PICU admissions met criteria
for PC consultation. Trigger list compliance was poor in the first month (57%)
but improved to 80% by the third month, representing a seven-fold increase in
PC consults compared to pre-intervention baseline, despite an unchanged average PICU PRISM probability of death and mortality rate. Patients eligible for
PC consultation had significantly longer median PICU LOS (8.6 d vs 1.6 d,
p < 0.001), hospital LOS (14 d vs 4 d, p < 0.001) and total charges ($101,749
vs $22,580, p < 0.001). Conclusions: Utilizing a multidisciplinary approach,
QI methodology can be utilized to improve access to PC services in the PICU.
Notably, patients eligible for PC services consumed a disproportionate amount
of healthcare resources. Early identification of PC needs may improve patient/
family satisfaction and encourage innovative approaches to identify strategies to
reduce associated resource consumption. Further study is warranted.
393
IMPACT OF A PEDIATRIC HOSPITAL ORGAN DONATION
COMMITTEE ON OPO REFERRAL AND CONSENT
Sally Vitali1, Samantha Endicott2, Diego Martinez2, Megan Barrett1, Monica
Kleinman1, Jeffrey Burns1; 1Boston Children’s Hospital, Boston, MA, 2New England Organ Bank, Waltham, MA
Learning Objectives: Programmatic efforts to improve the pediatric organ donation process are challenged by the small number of potential donors in individual
hospitals. We sought to evaluate the impact of a multidisciplinary organ donation
committee on referral and consent statistics at a pediatric hospital. Methods:
Boston Children’s Hospital (BCH) appointed physician and nursing leaders from
medical, surgical, cardiac and neonatal ICUs to an Organ Donation Oversight
Committee (ODOC) in July 2012. The ODOC was directed to collaborate with
the New England Organ Bank (NEOB) to evaluate referral, approach, and donation data from all deaths at BCH and strategize for improvement. We evaluated
referral and consent statistics for 18 months before and after introduction of the
ODOC. Results: Before the ODOC, 41 (20.6%) of 199 deaths at BCH were
referred to the NEOB prior to death, while afterward 115 (60.5%) of 189 deaths
were pre-mortem referrals. The percentage of referrals that were deemed medically suitable for donation remained similar before (12.2% or 5/41) and after
(14.8% or 17/115) the ODOC. Of the medically suitable referrals, 1 of the 5
before the ODOC was a potential donation after circulatory determination of
death (DCDD) candidate (20%) while 7 of the 17 after were DCDD candidates
(41.2%). None of those approached for DCDD consented for donation before or
after the ODOC initiative, while 2 of the 4 brain dead donation (BDD) pathway
candidates (50%) became donors before and 5 of 10 BDD candidates (50%)
became donors after the ODOC started. Several families that declined DCDD
agreed to donate tissues, leading to an increased tissue donation conversion rate
from 25% before to 38% after the ODOC began. Conclusions: The collaborative work of the ODOC and NEOB has increased the number of opportunities
for families to consider DCDD and the number of tissue donors. Efforts are
now focused on modifiable factors (e.g. timing and communication) that cause
interested families to decline consent so that eligible families who would benefit
from donating the organs of their dying child have every opportunity to do so.
394
OUTCOME EXPECTATIONS AND GOALS OF CARE AMONG
MDS, RNS, AND FAMILY SURROGATES FOR CCI ADULTS
Sara Douglas1, Barbara Daly2, James Rowbottom3, Rana Hejal4, Elizabeth
O’Toole5; 1Case Western Reserve University, Cleveland, OH, 2University Hospitals of Cleveland, Cleveland, OH, 3Univ. Hospital of Cleveland, Cleveland, OH,
4
N/A, Akron, OH, 5MetroHealth Hospital, Cleveland, OH
Learning Objectives: Expectations for treatment outcome influence treatment
decisions in situations of chronic critical illness (CCI). The purpose of the study
was to: (a) measure the extent to which expectations regarding survival, functional status, cognitive status, need for mechanical ventilation, and ADLs differ
among MDs, RNs, and FSs of CCI patients;(b) assess accuracy of expectations
for survival; and (c) examine degree of concordance between MDs and FSs in
their identified goals of care. It was hypothesized that there would be a lack of
agreement among MDs, RNs, and FSs regarding expectations and goals of care.
Methods: There were 264 ICU patients and FSs, 159 RNs and 67 MDs in this
descriptive correlational study. Data regarding the current goal of care and predicted outcomes at 6 months post-ICU stay were collected from FSs, MDs and
RNs caring for the CCI patient every 5 days. Results: FSs were significantly
the most optimistic in their prediction of outcomes (survival, cognitive status,
ventilator dependence, ADLs) with MDs ranking second, and RNs ranking last.
MDs and RNs had the highest degree of agreement for expectations of cognitive
function (76%) and expectation for ADLs (76%) while MDs and FSs had the
highest degree of agreement for expectation of survival (71%). For mortality prediction, MDs and RNs accuracy rate was identical at 68.4%. MD sensitivity was
50.8% and specificity was 84.9% while RN sensitivity was 55.3% and specificity
was 80.8%. FS accuracy rate was 59.3%. There was a lack of concordance in goal
identification at all time points and MD expectations of survival were significant
predictors of goals at all time points. Conclusions: Consensus regarding expectations for outcomes is a key component of family satisfaction with decision making. The large discrepancy between groups (MD, FS, RN) regarding expectations
for survival and the primary goal of care points to the need to develop strategies
to clarify expectations early in the ICU experience.
395
UTILIZATION OF PALLIATIVE CARE CONSULTS IN CIRRHOTIC PATIENTS IN THE MICU
Piyush Gupta1, Lauren de Leon2, Gerardo Carino3; 1Brown University School
of Medicine, N/A, 2Brown University, Providence, RI, 3Miriam Hospital, Providence, RI
Learning Objectives: Given the high mortality rates of patients with decompensated cirrhosis, more awareness and understanding of the appropriateness of palliative care (PC) referrals is necessary. Our project aimed to determine the impact
of PC consultation on the length of stay of ESLD patients in a MICU. Methods:
A retrospective chart review was completed for patients admitted to the MICU
between Jul 2010 - Dec 2012 who carried a diagnosis of cirrhosis. Data collected
included: age, gender, length of stay (LOS), PC consult day, and disposition.
MELD, CTP, and Maddrey function scores were calculated to score liver disease
severity. Results: Out of 220 patients, 39 had PC consults. The average LOS
for those with a PC consult was 10.46 days, while the average LOS for patients
without a consult was 8.91 days. Once PC was consulted, disposition for patients
was reached within 3.5 days on average. However, those patients who had a PC
within 7 days had the shortest length of stay (5.96 days). Patients who had a PC
consult had higher severity of liver disease (CTP 11.05, MELD 25.09, Maddrey 49.8) compared to those without a consult (9.5, 17.35, 37.26 respectively).
Conclusions: PC was consulted infrequently (17.7% of patients) and more likely
to be consulted in patients with more severe disease. If PC was consulted within
7 days of admission, the average length of stay was 5.96 days compared to 8.91
days. If PC was consulted, a disposition plan was able to be reached in 3.5 days,
regardless of consult date. Patients who did receive a consult were more likely to
be discharged to a hospice center. This data suggest that timely PC consultation
can decrease the length of stay of ESLD patients in the MICU and facilitate
appropriate discharge. Moreover, MELD, CTP, and/or Maddrey function can
guide timing and appropriateness of PC consultations. Given the mortality rates
of patients with ESLD, it appears prudent to develop criteria for appropriate
consultation of PC, much like those that exist for end stage CHF, COPD, and
dementia. Further research will be needed to more precisely define these criteria.
396
RESOURCE UTILIZATION DURING END-OF-LIFE HOSPITALIZATIONS AMONG DEMENTIA PATIENTS ADMITTED
TO ICU
Lavi Oud1, Phillip Watkins2; 1Texas Tech University Health Sciences Center,
Odessa, TX, 2Texas Tech University HSC, Lubbock, TX
Learning Objectives: The benefits of intensive care among dementia (D) patients
remain debated; there are no population-level data on resource utilization among
patients with a diagnosis of D who are admitted to ICU during end-of-life (EOL)
hospitalizations. Methods: We used the Texas Inpatient Public Use Data File
to identify, using ICD-9-CM codes, patients aged ≥65 years with D & ICU
admission, between 2001 & 2010. We defined EOL hospitalizations as those
with either hospital death or discharge to hospice (H). We examined the share
of use of selected resource utilization measures by ICU admissions with EOL
hospitalization out of all D ICU admissions. X2test & descriptive statistics were
reported. Results: There were 276,056 hospitalizations with a diagnosis of D
who were admitted to ICU, with 36,671 EOL hospitalizations. Between 2001
& 2010 the rate of EOL hospitalizations among D ICU admissions rose from
10.9% to 14.9% (p<0.0001), while the rate of discharge to H among EOL hospitalizations rose from 15.8% to 51.9% (p<0.0001). The following changes were
noted between 2001 vs. 2010 in the share of use of selected resource utilization by
EOL hospitalizations out of all D ICU admissions: total hospital charges 12.7%
vs. 16.8% (p<0.0001); total days of hospitalization 11% vs. 15.5% (p<0.0001);
use of mechanical ventilation 43.2% vs. 45.8% (p=0.1971); use of hemodialysis
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
19.3% vs. 28.3% (p=0.2009). Conclusions: EOL hospitalizations among D
patients admitted to ICU consumed disproportional components of examined
resources, with no improvement over the past decade, with use especially pronounced for life support interventions. The marked increase of EOL hospitalizations with H may reflect increased EOL discussions, but those have likely
occurred late in the clinical course, given lack of effect on the examined resource
utilization measures. Further studies are needed to improve our understanding
about D patients who are likely to benefit from critical care interventions.
397
IS THE ICU/STEP-DOWN UNIT AN APPROPRIATE TRIAGE
LOCATION FOR THE PRESPECIFIED DNR-DNI PATIENT?
Andrew Miller1, Tarak Rambhatla1, Bushra Mina1, Georgia Panagopoulos1;
1
Lenox Hill Hospital, New York, NY
Learning Objectives: Admissions to ICU and step-down units represent a disproportionately large percentage of total hospital charges. Understanding the
outcomes of patients classified as DNR-DNI prior to ICU admission is vital
in the setting of an aging population and our limited hospital resources. As a
consequence of their advanced age and multiple comorbid diagnoses, we believe
this population may well be unique from others and that the use of Apache II or
other scoring systems may be inadequate to stratify them appropriately. Understanding the variables that are associated with mortality in this group may help
in the appropriate triage of this population. Methods: We performed a retrospective chart review of 52 patients classified as DNR-DNI prior to ICU or ICU
step-down admission. A panel of 50 variables describing the patients just prior
to their unit admission was made. Descriptors included admission location just
prior to the unit, outcomes data, biographical data, admission diagnosis, comorbid diagnoses, length of stay on each unit/ward, and major medical interventions made during the hospital admission. A database was created and statistical
analysis was performed. Results: Data were examined for significant associations
between all variables and the need for non-invasive ventilation (NIV) and all variables with resultant mortality. Significant findings with NIV included antibiotics
use (P= 0.03), tube feeding (P=0.024), and admission diagnoses of: pneumonia
(p=0.019), COPD (P=0.01), and chest tube placement (P=0.039). Significant
associations with mortality included antibiotics use (p=0.029), electrolyte abnormalities (p=0.01), hemodialysis (P=0.027), TPN (P=0.02), and having a pastoral
care visit (P=0.003). Mortality in the overall group was 15.4% with 5/8 occurring
in the step-down unit. Conclusions: The 15.4% mortality seen in our sample
was within the average mortality reported by multiple studies of all ICU/stepdown patients (8%-16%). This suggests that the triage of prespecified DNR-DNI
patients to the ICU/step-down units is appropriate. NIV use in this population
was not associated with mortality.
398
NURSES’ PERSPECTIVE ON END OF LIFE ISSUES
Ginger Tsai-Nguyen1, Britton Blough2, Adam Mora3; 1Texas A&M University
Health Science Center, N/A, 2Baylor University Medical Center, Dallas, TX,
3
N/A, Dallas, TX
Learning Objectives: End of life issues are moving increasingly more to the forefront of patient care. However, while these issues are of utmost importance in
caring for patients, there has yet to be a formal education medium in place to
help nurses navigate implementation of themes involved with end of life issues.
This is an area of medicine that carries with it many psychosocial issues and comfort levels may vary between providers. Prior to developing a tool to help nurses
deal with this topic, it is important to assess the current status of their views and
comfort levels. Methods: Our survey was sent to ICU nurses across the North
Texas Baylor Health Care System. Nurses were asked via email to answer an
anonymous 23 question survey from a “MonkeySurvey” link. The survey asked
general non-identifying demographic information as well as questions assessing comfort level with various end of life issues. Results: We received 78 total
responses. Demographics: 92% female, 8% male. Age ranges were evenly distributed between 20-29, 30-39, 40-49, 50-59. 40% of nurses had greater than 10
years of experience and greater than 60% worked in mixed ICUs. 81% of nurses
worked in a hospital with a formal palliative care service but only 44% knew
about a formal withdrawal of life sustaining therapy protocol. Almost 70% of
nurses were comfortable discussing code status and with initiating WLST Orders.
In regards to pain control, anxiety, and air hunger in a terminally ill patient, 90%,
81%, and 68% of nurses respectively felt comfortable addressing these issues.
Greater than 80% of nurses were comfortable requesting a hospice evaluation.
71% of nurses reported comfort addressing questions and concerns from family
members. When asked about the death of family members, 85% of nurses had a
close family member die and 56% were at the bedside when a close relative died.
88% of nurses think formal education on end of life issues is important. Finally,
2/3 of the nurses did not have an advanced directive. Conclusions: Nurses are
comfortable addressing end of life issues but believe that implementing formal
education is important.
Poster Session: Ethics/End of Life/Palliative Care 2
399
400
THE CRITICAL ILLNESS MORTALITY INFLECTION POINT
DURING PROLONGED SURGICAL ICU LENGTH OF STAY
VALIDATION OF A PEDIATRIC BEDSIDE TOOL TO PREDICT
TIME TO DEATH AFTER WITHDRAWAL OF LIFE SUPPORT
Niels Martin1, Tara Ramaswamy1, Joshua Marks1, Tara Collins1, Nina O’Connor1,
David Casarett1, Daniel Holena1, Lewis Kaplan1; 1University of Pennsylvania,
Philadelphia, PA
Learning Objectives: The purpose of this study is to determine the relationship
between ICU length of stay (LOS) and mortality in a surgical population and
evaluate predictors of mortality at an inflection point. We hypothesis that the
mortality curve based on surgical ICU LOS will have an inflection point that will
identify predictors of mortality and guide decision making. Methods: All patients
admitted to the surgical ICU at a mature, urban, academic medical center from
July 2003 through June 2014 were reviewed retrospectively. Mortality rates were
determined and plotted for each ICU LOS day through the first 6 weeks. Identified mortality curve slope change was used to identify an at-risk cohort. Using
the most recent one year data, risk factors including APACHE II were recalculated on the inflection point day to assess metric validity. Results: 19,061 ICU
admissions were assessed. Mortality followed a sigmoid curve with a major rise
occurring during the second week that plateaued by day 14. Mortality rates based
on LOS < 14 days vs. ≥14 differed significantly, 3.99% to 17.61%, p<0.0001.
There were 130 patients with a >14 day LOS in the most recent year cohort.
Re-calculated APACHE II scores on ICU day 14 were significantly predictive of
mortality, 23.64 for deaths (95% CI: 21.36-25.92) vs. 16.35 for survivors (95%
CI: 15.50-17.20), p<0.0001. Additional independent Day 14 predictors of mortality included pressor use (44.0% vs. 21.9%, p<0.02), bacteremia (44.0% vs.
16.2%, p<0.002), active malignancy (40.0% vs. 16.2%, p<0.005), and dialysis
use (36.0% vs. 10.5%, p<0.001). Conclusions: Mortality significantly increases
after 14 days in a surgical ICU. Recalculation of APACHE II score at this inflection point is valid and correlative of mortality. This methodology can be helpful
for directing decision making in patients who remain in the ICU after two weeks.
Crit Care Med 2014 • Volume 42 • Number 12 (Suppl.)
Ashima Das1, Ingrid Anderson1, David Speicher2, Richard Speicher3, Steven
Shein3, Alexandre Rotta4; 1Rainbow Babies and Childrens Hospital, Cleveland,
OH, 2Rainbow Babies and Children’s Hospital, Cleveland, OH, 3N/A, Cleveland, OH, 4Rainbow Babies & Children’s Hospital, Cleveland, OH
Learning Objectives: Successful organ donation after circulatory determination
of death (DCDD) requires short time intervals between withdrawal of life support (WS) and cessation of circulation to minimize the effects of hypoxic-ischemic
organ damage. The recently developed Dallas Predictor Tool (DPT) has an overall
classification accuracy of 74.5% and 87.3% for death within 30 and 60 min after
WS, but external validation is needed. We evaluated the ability of the DPT to
accurately predict death within 30 and 60 min of WS in a remote pediatric cohort.
Methods:Pertinent variables for all pediatric deaths (age Results: There were 8829
PICU admissions resulting in 132 (1.5%) deaths. Death followed WS in 70 patients
(53%). After excluding subjects with insufficient data to calculate DPT scores, 62
subjects were analyzed. Average age of patients was 5.3 yrs +/- 6.9, median time
to death after WS was 25 min (7 min–16hr 54 min). Respiratory failure, shock
and sepsis were the most common diagnoses. Thirty-seven patients (59.6%) died
within 30 min of WS and 52 (83.8%) died within 60 min. DPT-30 scores ranged
from -17 to 16. A DPT-30 score >0 was most predictive of death, with sensitivity=
0.76, specificity= 0.52, AUC= 0.69 and an overall classification accuracy= 64.5%.
DPT-60 scores ranged from -21 to 28. A DPT-60 score>-1 was most predictive
of death, with sensitivity= 0.75, specificity= 0.8, AUC= 0.847 and an overall classification accuracy= 74.2%. Conclusions: In this external cohort, DPT is clinically
relevant in predicting time from WS to death. DPT is more useful in predicting
death within 60 min than within 30 min of WS. Even with our proposed optimal
cut-off scores, further calibration and modifications of this important tool could be
beneficial to families and health care professionals considering DCDD.
401
ORGAN DONATION: A VALUES EXPLORATION EXERCISE
Sandy Swoboda1, Ali Hall2, Pamela Lipsett1; 1Johns Hopkins Medical Institutions, Baltimore, MD, 2Ali Hall Training and Consulting, San Francisco, CA
Learning Objectives: The greatest obstacle to organ donation is a shortage of donors
and a lack of communication of donor status to family members. While a 2012 Gallup poll showed 95% of respondents are donor willing, only 60% have designated
their intent or shared their intent with family. To further understand one’s motivation, readiness and commitment to change and personal values around donation, we
utilized Motivational Interviewing (MI), a participant centered approach to understand ambivalence and elicit change, with a personal values card sort (VCS) exercise
to improve outreach for organ donation. We sought to understand these issues in a
non-crisis setting.Our hypothesis: MI and a VCS exercise would identify values and
elicit change talk, interest and commitment to organ donation Methods: A convenience sample of nursing students and employees of a large university participated in
focus groups with MI and VCS. This was a pre-post design with Likert scales (1-10)
for attitude, importance, confidence and commitment to donation intent and family
communication. Demographics, knowledge and VCS data were collected. Donor
status was blinded until analysis. Results: All of the 25 participants were female,
72% white, 64% age < 40, and 68% single, with 68% designated donors. Of the
32% non-donors change talk toward intent to donate increased for importance and
confidence 1.5 on a Likert scale, 66% increased commitment language and 100%
communication to family. More than 90% of donors expressed increased importance
and confidence in change talk for intent to donate and communicate with family,
with an average range of 0.5-1.6 on a Likert scale. Three of the top 5 sorted values
around donation included values of family (>77%), health (>47%) and being loved
(>41%) for both donors and non-donors. Conclusions: MI and the VCS exercise
strengthens change talk and commitment language toward intent to donate and to
communicate donor intention among both non-donor and donor participants. This
exercise can be used to improve and target educational strategies to increase donor
designation and communication of intent to family.
402
EFFICACY OF THE “SURPRISE” QUESTION TO PREDICT
6-MONTH MORTALITY IN ICU PATIENTS.
Saad Khan1, Sarah Hadique1, Stacey Culp1, Asma Syed2, Corbin Hodder3, John
Parker4, Alvin Moss5; 1West Virginia University School of Medicine, Morgantown,
WV, 2West Virginia UNiversity School of Medicine, Morgantown, WV, 3West Virginia University Pulmonary/ Critical Care Medicine, Morgantown, WV, 4West Virginia University, Morgantown, WV, 5West Virginia University, Morgantown, WV
Learning Objectives: Researchers are seeking to improve prognostic accuracy for
patients in the medical intensive care unit (MICU) by developing an integrated
model that combines clinical predictions and other prognostic factors. The Surprise
Question “Would I surprised if this patient died in the next 6 months”? is one such
clinical prediction tool which has been validated in cancer and dialysis patients, but
its utility has not previously been tested in MICU patients. Increased prognostic
accuracy of 6-month mortality could lead to an improvement in palliative and endof-life care in this population. Methods: DESIGN: Prospective Cohort Study in
Academic MICU PATIENTS: 500 consecutive adult MICU patients MEASUREMENTS: Surprise Question classification; patient status at 6 months (alive or
dead); Charlson Comorbidity Index (CCI) score; Karnosfsky Performance Status
score; Apache 3 Score and demographics. Results: Intensivists answered the Surprise Question for 500 prospective patients admitted to the MICU classifying 238
(47.6%) into the ‘‘No, I would not be surprised’’ group and 262 (52.4%) into the
‘‘Yes, I would be surprised’’ group. Mortality at 6 months was 36% overall, 62.2%
for the “No” group, and 12.2% for the “Yes” group P< .001. In multivariate logistic
regression analysis, the odds ratio (OR) of dying within 6 months for those patients
for whom the Surprise Question was answered “No” was 7.290 (95%CI, 4.515 to
11.770) greater than for those for whom the Surprise Question was answered “Yes”
P< .001. The CCI score,OR 1.094 P= .033 and the Apache 3 score OR 1.021,
P <.001 were also significant but weaker predictors in the stepwise multivariate
logistic regression model. Mean survival time calculated using the log-rank test and
censored at 180 days was 91.1 days for the “No” group and 169.1 days for the
“Yes” group P<.001. Conclusions: The Surprise Question is a simple, feasible and
effective tool to predict 6-month mortality for MICU patients. Additional study is
required to validate these findings and to develop an integrated prognostic model
including the surprise question with a strong C-statistic.
403
PALLIATIVE CARE CONSULTATION AND END-OF-LIFE CARE
IN AN ONCOLOGIC ICU
Christine Freise1, Alison Wiesenthal1, Lisa Canecchia1, Ilde Lee1, Natalie
Kostelecky1, Louis Voigt1, Stephen Pastores1, Neil Halpern1; 1Memorial Sloan
Kettering Cancer Center, New York, NY
Learning Objectives: Palliative care consultations (PCC) are used in many ICUs
to assist healthcare providers in their discussions with patients/families regarding
end-of-life (EOL) care issues. Limited data are available on the frequency of PCC
in critically ill patients with cancer. Our objective was to compare the characteristics of cancer patients who died in the ICU with or without PCC. Methods: We
retrospectively analyzed all adult cancer patients who died in a med-surg ICU at
a cancer center from 01/01/13 to 12/31/13. ICU decedents were divided into 2
groups: Group I: decedents who received PCC before or during their ICU stay
(PCC) and Group II: decedents who did not receive PCC (no-PCC). Data collected included demographics, reasons for ICU admission, weekday or weekend
admission, medical or surgical service, MPM II score and lactate level on ICU