Impact of State Laws Regulating Pseudoephedrine on

Met etamine ciation of f State C d
:
Pat tricia R. F reeman, P y Talbert, PhD
Institute f for Pharmac ment of Phar rmacy Pract
Colleg acy ucky cky
©N Asso of Sta d Substances Authorities
72 B Street
Quinc MA 0
CONTENTS
I. Introduction ……………………………………………………………….3
II. Scope Work…………………………………………………………….5
III. Review of Federal and State Laws..…………….……………………...5
IV. Review of the Literature……....……………….………………………..12
A. Impact of Federal Laws……………..……………………………….14
B. Impact of State Laws………...……………………………………….17
V. Summary and Suggestions for Further Study…………………...……30
2
I. Introduction
Methamphetamine, a highly addictive drug with potent central nervous system stimulant properties, has a long history of use in the United States. Methamphetamine was first marketed by Burroughs Wellcome and Co. under the trade name Methedrine beginning in 1940 and by Abbott Laboratories under the trade name Desoxyn® in 1943. By the
1950s, methamphetamine was readily available legally and widely used for a variety of conditions, including narcolepsy, attention deficit disorder, obesity, and fatigue.
1
Methamphetamine became extensively abused and diverted during the 1960s following its use as a treatment for heroin and cocaine addiction and, in response, the US Drug
Enforcement Administration (DEA) classified methamphetamine as a Schedule II controlled substance in 1971. The scheduling of methamphetamine products had an immediate impact on reducing methamphetamine abuse in the US; however, a resurgence of abuse was noted in the 1980s following the FDA approval of ephedrine and pseudoephedrine (PSE), two common precursors used in the illicit production of methamphetamine, for use as non-prescription, or over-the counter (OTC) decongestants.
Today, methamphetamine is recognized as a major drug of abuse. According to the
United Nations Office of Drug Control (UNODC), methamphetamine abuse affects between 14 and 53 million people (0.3 - 1.2%) worldwide.
2
Data from the Substance
Abuse and Mental Health Services Administration’s (SAMSHA) National Survey on
Drug Use and Health (NSDUH) indicate that 13 million people age 12 or older in the US have used methamphetamine at some point in their lives.
3
Use of methamphetamine produces an initial period of euphoria, which may cause the user to continue using to obtain/maintain the euphoric ‘rush’. Continued use/abuse of methamphetamine is associated with anorexia, weight loss, insomnia, aggression, hallucinations, paranoia, convulsions, stroke, cardiac arrhythmia, and hyperthermia.
4
Chronic abuse can lead to irreversible brain and heart damage, memory loss, psychotic behavior, rages, violence and ultimately the inability to care for oneself and one’s children.
4
_________________________
1
Congressional Report Services, Methamphetamine: Background, Prevalence, and Federal Drug Control Policies
2007. Report No: RL33857 available at http://www.ncpc.org/cms/cms-upload/ncpc/File/Methamphetamine-
Background,%20Prevalence,%20and%20Federal%20Drug%20Control%20Policies.pdf
accessed November 20,
2011.
2
United Nations Office on Drugs and Crime. World Drug Report 2010. United Nations; 2010.
3
Substance Abuse and Mental Health Services Administration (SAMSHA). Results from the 2010
National Survey on Drug Use and Health: Detailed Tables. Available at http://www.samhsa.gov/data/NSDUH/2k10NSDUH/tabs/Sect1peTabs1to10.pdf
, accessed December 30, 2011.
4
U.S. Department of Health and Human Services (DHHS), National Institutes of Health (NIH), National Institute on
Drug Abuse (NIDA), “Methamphetamine Abuse and Addiction,” Research Report Series , NIH Publication No. 06-
4210, Revised September 2006, available at http://www.drugabuse.gov/PDF/RRMetham.pdf
, accessed November
18, 2011.
3
Global production of illicit methamphetamine is estimated at 290 tons per year with a retail value of $28 billion
5
with widespread availability in the U.S. largely fueled by illegal production and importation from Mexico, and by illicit production in large and small clandestine domestic laboratories.
6
In addition to the known harms associated with methamphetamine abuse described above, the production of methamphetamine by small labs poses significant environmental hazards such as toxic dumpsites, explosions and exposure to chemicals that can result in serious harm.
7
In 2005, an estimated 35 percent of the methamphetamine used in the United States was produced in small-scale laboratories.
8
The most recent estimates of the societal costs of methamphetamine abuse are detailed in a study conducted by the RAND Drug Policy Research Center.
9
This first national estimate suggests that the economic cost of methamphetamine use in the US reached $23.4 billion ($16.2 billion - $48.3 billion) in 2005. The authors’ analysis considers a wide range of consequences due to methamphetamine use, including the burden of addiction, premature death, drug treatment, and aspects of lost productivity, crime and criminal justice, health care, production and environmental hazards, and child endangerment.
To address the problems of methamphetamine abuse, multiple approaches have been taken by federal and state agencies. Initial approaches focused on controlling wholesale distribution of bulk precursor chemicals, including ephedrine and PSE. Subsequent efforts have largely focused on controlling access to methamphetamine precursors purchased at retail outlets such as grocery and convenience stores and pharmacies, including the reclassification of PSE as a controlled prescription drug in some states.
The illicit domestic production of methamphetamine should be sensitive to regulatory efforts that limit access to chemical precursors (ephedrine and PSE) because without them, methamphetamine cannot be readily synthesized.
_________________________
5
United Nations Office on Drugs and Crime. World Drug Report 2007. United Nations; 2007.
6
National Drug Threat Assessment, 2011. US Department of Justice, National Drug Intelligence Center;
Available at http://www.justice.gov/ndic/pubs44/44849/44849p.pdf
; accessed October 17, 2011.
7
Dan Hannan, Occupational Hazards: Meth Labs Understanding Exposure Hazards and Associated
Problems , June 2005, p. 24.
8
Testimony of Gary W. Oetje to Subcommittee on Criminal Justice, Drug Policy, and Human
Resources Committee on Government Reform , U.S. House of Representatives . Law Enforcement and the Fight Against Methamphetamine: Improving Federal, State and Local Efforts, August 23, 2005 available at http://www.justice.gov/dea/pubs/cngrtest/ct082305.html
, accessed December 22, 2011.
9
Nicosa et al. The Economic Cost of Methamphetamine Use in the United States, 2005. RAND Drug
Policy Research Center; 2009; available at http://www.rand.org/pubs/monographs/MG829.html
, accessed on October 13, 2011.
4
As states grapple with the methamphetamine abuse problem, information relative to the impact of the varying approaches states have taken to control access to methamphetamine precursors is needed. Such information will assist policy makers in crafting future precursor control regulations with the greatest impact.
II. Scope Work
The National Association of State Controlled Substance Authorities (NASCSA) engaged researchers at the University of Kentucky Institute for Pharmaceutical Outcomes and
Policy to prepare a white paper summarizing the impact of state and federal PSE laws on methamphetamine abuse. The white paper will inform public officials and legislators relative to which laws may have the greatest impact on methamphetamine abuse and guide future policy decisions relative to PSE regulation. To complete the white paper, the following components were outlined in the scope of work to be conducted:
1) Conduct a review of current state and federal laws regulating PSE
2) Conduct a review of current findings from the literature relative to PSE laws
3) Prepare a summary of successes and failures relative to state PSE laws
4) Identify suggestions of areas for further study/research
III. Review of Federal and State Laws Regulating Pseudoephedrine
Federal Laws
The first major attempt at controlling methamphetamine precursor chemicals occurred in
1988 with the passage of the Chemical Diversion and Trafficking Act (CDTA) , which regulated bulk ephedrine and PSE. The CDTA required record keeping, reporting requirements, and import/export notification requirements for bulk, pure (single entity) ephedrine and PSE products only and did not apply to OTC tablets or capsules containing ephedrine and PSE.
In 1993, Congress passed the Domestic Chemical Diversion Control Act (DCDCA) which removed the record-keeping and reporting exemption for pure (single entity) ephedrine products. It also required distributors, importers, and exporters to register with DEA and gave DEA the power to revoke a company’s registration without proof of criminal intent.
The Comprehensive Methamphetamine Control Act of 1996 (MCA) broadened federal regulation of listed chemicals to include those found in OTC cold and sinus medicines.
Under the MCA, methamphetamine precursor chemicals containing ephedrine, PSE or phenylpropanolamine (PPA) were added to Schedule II of the controlled substance act.
5
Other provisions of the MCA also increased penalties for the trafficking and manufacturing of methamphetamine and methamphetamine-related listed chemicals.
The Methamphetamine Anti-Proliferation Act of 2000 (MAPA) included provisions to address the problem of diversion of OTC drug products containing methamphetamine precursor chemicals from retail and mail order sources. MAPA established thresholds for single purchases of OTC medicines containing ephedrine, PSE and PPA at 9 grams per transaction and added the requirement that the products be packaged in containers of not more than 3 grams of precursor base chemical. Products packaged in “blister packaging” were provided a ‘safe harbor’ exemption from the threshold limits set by
MAPA.
In 2005, Congress passed the USA PATRIOT Improvement and Reauthorization Act which contained the Combat Methamphetamine Epidemic Act (CMEA). The provisions of the CMEA further regulated the domestic and international commerce of methamphetamine precursor chemicals. Specifically, the CMEA established a new set of controls for methamphetamine precursor chemicals (ephedrine, PSE and PPA) designed to control illicit diversion including the following limits on the retail sales of
OTC products containing methamphetamine precursor chemicals:
limits sales of OTC products to 3.6 grams of the precursor base per customer per day (previously limited to 9 grams per transaction) and 9 grams per customer per month in drugstores, convenience stores and grocery stores
limits mobile retail and mail-order sales to 7.5 grams of precursor base per customer per month
requires that products containing methamphetamine precursor chemicals be kept
“behind the counter” and, for mobile retailers, that the products be secured under lock and key
requires retailers to maintain a logbook that must be kept for at least two years, recording the time and date of sale, the name and quantity of the product sold, and the name and address of each purchaser
requires purchasers to present a government-issued photo identification, sign the logbook for the sale providing their name, address, and the date and time of the sale
requires retailer’s logbooks include a warning that false statements will be punishable with a term of imprisonment of up to five years and/or a fine of not more than $250,000 for an individual offender, or $500,000 in cases involving an organization
requires retailers to train employees on the methamphetamine precursor products statutory and regulatory provisions of the law
requires retailers to take measures against possible employee theft or diversion of OTC products containing methamphetamine precursor chemicals
6
Act of 2010 ted. d in the illeg al manufac w law, retai selfre in comp liance with regulation s that limit t the amou ributors are required to egistered wi A.
Figure the Con
1 below summari izes the history o attempts ulate full review ative histo ry of precursor gressional 007 Report t for Congre
10 istory of F ecursor Re gulation
• Chemica Diversion a Traffick Act TA)
• Domesti c Chemical D Co Act (D CDCA)
• Compreh Meth ine Control Act (MCA)
• Methamp A ‐ Prolifer Act MAPA)
• Combat M tamine Epid Act MEA)
• Combat M tamine Enha ct
Methamphetamin Prevalence, and
10
Congress amphetamine: Background, P port No: RL338 57 available at t http://www.nc
g Control Polic ies
Backgroun
2011
d,%20Prevale nce,%20and%
0Drug%20Cont trol%20Policies accessed 0,
7
State Law
The majority of states have enacted laws controlling the sale of PSE- and ephedrinecontaining products that are more stringent than the current federal laws. Electronic tracking and block of sales to those exceeding quantity limits is the most common approach states have taken. Additionally, some states have chosen to restrict purchase quantities to amounts that are less than currently allowed by federal regulations (CMEA restricts retail purchases to <9 grams per 30 days). Other states have chosen to reclassify PSE as a Schedule III controlled substance. More recently, some states have passed mandates to establish a registry of individuals with methamphetamine-related convictions and block the sale of PSE to these individuals.
In the following section, a review of state approaches to PSE regulation will be presented. Table 1 provides a summary of state approaches. For a full accounting of state laws regulating PSE please see Appendix A.
Table 1: State Approaches to Pseudoephedrine Regulation
Regulatory Approach States with Mandates
Electronic Tracking and Block of Sales AL, AR, FL, IL, IN, IA, KS, KY, LA, MI , MO
Prescription-only Status
NC, NE, ND, OK, SC, TX, TN, WA, WV
AR a
, MS, OR
Schedule V Controlled Substance
Schedule III Controlled Substance
AR, IA, IL, KS, LA, MN, MO, NM, OK
WI, WV
MS, OR
Greater Restrictions on Purchase
Quantities
AK, IA, IN, MN, WI
Block of Sales to Those with Previous
Methamphetamine- related Convictions
OK a
Prescription required for out of state residents only; Information current as of 12/31/11
8
Electronic Tracking and Block of Sales
Since 2006, pharmacies and retail outlets have been required to keep a log book documenting the sale of PSE to meet the provisions of the CMEA. While logging PSE sales at individual pharmacies and other retail outlets can be used to track and compare purchases within an individual outlet, this approach has been less than effective at controlling PSE purchases for illicit uses, as persons with the intent of purchasing PSE for methamphetamine production can travel from pharmacy to pharmacy making multiple PSE purchases. With electronic tracking, the purchaser’s driver’s license or other allowed identification is scanned at the point of sale of PSE-containing products.
The sale is then ‘logged’ by the electronic tracking system documenting the date and amount of the PSE purchased. Future attempts to purchase PSE will be scanned and logged in the same manner at any retail purchase outlet. Sales data is stored centrally and can be shared among pharmacies and retail outlets in a state, and, in some cases depending on the tracking system used, across state lines. Once purchase thresholds have been reached, the individual completing the sale is alerted and the sale can be blocked. Thus, the major advantage of electronic tracking over paper log books is the sharing of aggregate data in real time that allows those selling PSE to more accurately determine if a PSE purchase would exceed an individual’s legal limit. Additionally, electronic tracking systems can be used to alert law enforcement when individuals attempt to purchase more than the legal limit of a methamphetamine precursor in a more efficient and expedient manner than reviewing multiple paper logs.
Oklahoma became the first state to require electronic tracking in 2004 using an internally developed system maintained by the Oklahoma Bureau of Narcotics.
Arkansas and Kentucky soon followed suit; Arkansas has been using MethMonitor
11
to track methamphetamine precursor sales since 2006, and in 2008, Kentucky became the first state to pilot a new electronic system, MethCheck, for the tracking of PSE sales.
Since 2008, the use of electronic tracking has increased substantially with twenty states having passed laws as of July 2011 requiring the electronic tracking of PSE sales
(Table 1). Although states have implemented electronic tracking laws in a variety of ways, the most common approach taken by states has been to use the National
Precursor Log Exchange (NPLEx) described in further detail below.
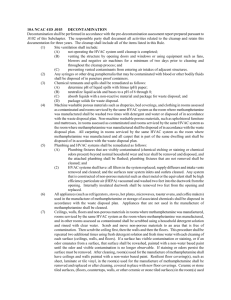
National Precursor Log Exchange
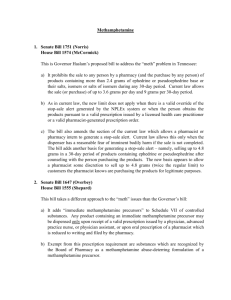
The National Precursor Log Exchange (NPLEx) is a real-time electronic logging system used by pharmacies, retail outlets and law enforcement to track sales of OTC cold and allergy medications containing methamphetamine precursors. To date, laws authorizing the use of NPLEx have been implemented in 17 states (Figure 2).
_________________________
11
Leadsonlabs available at https://www.leadsonline.com/main/services/methmonitor/methmonitor.php
, accessed December 18, 2011.
9
Figure 2: States Tracking Pseudoephedrine Sales using National Precursor
Log Exchange
Used with permission from NPLEx
11
The National Association of Drug Diversion Investigators (NADDI) is the provider of the service and Appriss, Inc., is the technology vendor whose product, MethCheck, won the competitive bid to provide the service. NPLEx is provided free of charge (sponsored by the manufacturers of PSE-containing OTC products) on a permanent basis to state governments that pass appropriate legislation and regulations. Services provided include implementation to all retailers, access to law enforcement, technical support, training for retailers and law enforcement, and maintenance and upgrades.
11
Retailers using the system voluntarily block the sale of precursors that would exceed the legal quantity limits (3.6 grams per day and 9 grams in 30 days per CMEA or more stringent requirements per relevant state laws). When a transaction is submitted by a retailer that would exceed the limits, a message is instantly transmitted recommending denial of the sale. A manual override can be used if the clerk feels in danger, and law enforcement is notified that the sale may have exceeded the limits.
11
According to NPLEx, currently
27,584 retailers and 6,591 law enforcement agents use the electronic system to log and track sales.
11
_________________________
11
National Precursor Log Exchange, available at http://www.nplexservice.com/ , accessed January 5, 2011.
10
Purchase Quantity Restrictions
Since the passage of the CMEA in 2005, retail purchases of PSE have been limited to 9 grams per 30 days. Several states, including Arkansas, Iowa, Indiana, Minnesota and
Wisconsin, have implemented more stringent laws restricting the retail purchase of PSE to 7.5 grams, or as in the case of Indiana, 7.2 grams per 30 days and Minnesota, 6 grams per 30 days. The maximum daily dose of PSE is 240 mg, thus if a person requiring PSE takes the maximum dose every day for 30 days, a quantity of 7.2 grams would be needed for the 30 day supply. Restricting quantities to a maximum of 7.2 grams per day should have no impact on persons purchasing PSE for legitimate selfcare uses. Additional states are considering legislation to restrict purchase quantities to this limit.
Schedule V Controlled Substance
Eleven states have reclassified PSE as a Schedule V controlled substance - Arkansas,
Illinois, Iowa, Kansas, Louisiana, Minnesota, Missouri, New Mexico, Oklahoma, West
Virginia and Wisconsin. As Schedule V, products are available OTC with specific requirements for purchasing, including maintaining a log of all transactions and presentation of identification showing proof of age (18 years or older). Additionally, the classification of PSE and other precursors as Schedule V substances restricts their purchases to pharmacies. States with prescription monitoring programs (PMPs) that monitor Schedule V substances may require data on Schedule V PSE sales to be transmitted to the PMP. Such is the case with Oklahoma, which has classified all PSEcontaining medications as Schedule V prescriptions and requires that they be submitted to the Oklahoma PMP database.
Prescription-only Status/ Schedule III Controlled Substance
Two states – Oregon and Mississippi – have adopted the strictest PSE laws to date, making PSE a Schedule III controlled substance available by prescription only and subject to the states’ PMP. In 2011, legislation was passed in Arkansas limiting the
OTC sales of PSE to Arkansas residents and imposing new duties on pharmacists.
Specifically, the new law makes it illegal to dispense any product containing PSE (or ephedrine or PPA) without a prescription, unless the purchaser can provide an
Arkansas-issued Driver’s License or ID card, or an identity card issued by the U.S.
Department of Defense for active-duty military personnel. Additionally, the law requires pharmacists to verify the legitimate medical need of individuals purchasing products containing PSE, based on a pharmacist-patient relationship, before allowing the purchase of a PSE (or ephedrine or PPA) containing product. Prior prescription history and/or information obtained during patient screening can be used to provide professional reassurance to the pharmacist that a legitimate medical need exists.
11
Methamphetamine Registry/Block of Sales to those with Previous
Methamphetamine-Related Convictions
Oklahoma passed legislation, effective November 2010, requiring all individuals convicted of possession, manufacture, distribution or trafficking of methamphetamine to register with the state. Pharmacies and other retail outlets who register with the state to sell or dispense PSE-related products and law enforcement agencies can access the registry through a central repository and the state’s PMP. Customers listed in the registry due to a previous methamphetamine-related conviction will be blocked at the point of sale from buying PSE and are prohibited from possessing “any detectable quantity” of the drug. When a pharmacy sells PSE OTC, the purchaser’s name is checked against the Meth Registry and the sale will be blocked if the individual has a prior methamphetamine-related conviction, without regards to quantity limits.
IV. Review of the Literature Relative to Pseudoephedrine Laws
A review of the literature was conducted to identify published studies evaluating the impact of federal and state laws regulating methamphetamine precursors on methamphetamine abuse. Published reports utilize a variety of data sources to assess impact including healthcare-related data and data collected and aggregated from lawenforcement agencies. In addition to the published literature, information from governmental agency reports, news reports, legislative policy reports and personal interviews were used as mechanisms for gathering data evaluating the impact of state and federal precursor control laws and are referenced throughout the report as appropriate. Impact can be assessed in two main ways – the use of law enforcement data (to assess changes in the manufacture of methamphetamine in domestic clandestine labs, amount of methamphetamine seized during lab raids and other law enforcement activities and methamphetamine-related crimes) and the use of healthcare data (to assess changes in the actual abuse of methamphetamine such as surveys, admissions to treatment facilities for methamphetamine abuse and emergency department (ED) visits related to methamphetamine.) The most common datasets used for assessing impact are summarized below. For the purposes of the report, the impact of federal and state laws are discussed separately.
Law Enforcement Datasets
Data from law enforcement agencies commonly utilized for assessing impact of precursor control regulations include the National Clandestine Laboratory Surveillance
System (NCLSS), the System to Retrieve Information from Drug Evidence (STRIDE) and Uniform Crime Reports (UCR).
12
The NCLSS is a national database which became operational in January 1999 and serves as a clearinghouse for all federal, state, and local clandestine laboratory seizures.
12
The El Paso Intelligence Center (EPIC) is the central repository for these data. Although commonly used, the data do have limitations, including incomplete reporting of data by states. STRIDE is the DEA’s administrative data system for collecting data on drug evidence purchased, seized or collected during investigations by the DEA, the Federal Bureau of Investigation, other federal organizations and some state and local law enforcement. Data collected includes information on type, amount, form and purity of the drug.
13
The UCR database is maintained by the Federal Bureau of
Investigation (FBI). The FBI’s primary objective in maintaining the UCR is to generate a reliable set of crime statistics for use in law enforcement administration, operation, and management.
14
Healthcare-Related Datasets
Healthcare-related datasets that provide information relative to methamphetamine use and are commonly utilized for assessing impact of precursor control regulations include the Treatment Episode Data Set (TEDS), the Drug Abuse Warning Network (DAWN) and the National Survey on Drug Use and Health (NSDUH). TEDS is maintained by the Office of Applied Studies, Substance Abuse and Mental Health Services
Administration (SAMHSA), an agency of the U.S. Public Health Service in the U.S.
Department of Health and Human Services and includes records for some 1.5 million substance abuse treatment admissions annually.
15
DAWN is a public health surveillance system that monitors drug-related visits to a sample of hospital emergency departments and drug-related deaths investigated by medical examiners and coroners.
16
The NSDUH provides national and state-level data on the use of tobacco, alcohol, illicit drugs (including non-medical use of prescription drugs) and mental health in the United States. NSDUH is sponsored by SAMHSA.
17
_________________________
12
DEA, El Paso Intelligence Center, Clandestine laboratory Seizure System. Available at http://www.justice.gov/dea/concern/map_lab_seizures.html
, accessed November 16, 2011.
13
US Drug Enforcement Agency, System to Retrieve Information from Drug Evidence, available at http://www.justice.gov/dea/stride_data.html
, accessed December 18, 2011.
14
Federal Bureau of Investigation, Uniform Crime Reports, available at http://www.fbi.gov/aboutus/cjis/ucr/ucr , accessed December 18, 2011.
15
Substance Abuse and Mental Health Services Administration, Treatment Episode Data Set, available at http://wwwdasis.samhsa.gov/webt/newmapv1.htm
, accessed December 18, 2011.
16
Substance Abuse and Mental Health Services Administration, Drug Abuse Warning Network, available at http://www.samhsa.gov/data/DAWN.aspx
, accessed December 18, 2011.
17
Substance Abuse and Mental Health Services Administration, National Survey on Drug Use and
Health, available at https://nsduhweb.rti.org/RespWeb/homepage2.cfm
, accessed December 18, 2011.
13
A. Impact of Federal PSE Laws
A review of the literature relative to the impact of Federal PSE regulations found several relevant articles. First, Nonnemaker et al. in Are Methamphetamine Precursor Control
Laws Effective Tools to Fight the Methamphetamine Epidemic estimated the impact of federal MAPA legislation (2000) that restricted PSE purchases to 9 grams per transaction.
18
The author used a conceptual model based on economic theory that precursor control is a supply side measure that should reduce supply and drive up prices of methamphetamine; because methamphetamine is price elastic (i.e., a small change in price is accompanied by a large change in the quantity demanded), increases in price will lead to fewer users and decreased consumption.
Data sources used included NCLSS to measure domestic production and availability of methamphetamine from lab seizure data, STRIDE to measure drug prices and purity, and TEDS to identify methamphetamine related admissions to drug abuse treatment facilities as a proxy for methamphetamine use. Results from the evaluation suggest that MAPA had no impact on per capita methamphetamine lab seizures but a small yet significant decline in amount of methamphetamine seized by law enforcement agencies occurred following MAPA. Additionally, results indicate that methamphetamine prices fell and average purity rose post MAPA (pre-post 2000) which was opposite of what was expected.
Finally, results indicate that methamphetamine-related treatment episodes were not significantly different pre-post MAPA implementation. From these results, the authors conclude that the net benefit of MAPA is unclear. The counterintuitive rise in methamphetamine purities and lower prices may suggest flow of finished methamphetamine from international sources and increased domestic use.
Cunningham and Liu evaluated the impact of federal precursor chemical regulations on methamphetamine-related hospital admissions
19
and arrests
20
in California. The authors found in both studies that federal regulations targeting regulation of precursor chemicals was associated with immediate declines in both methamphetamine-related hospital admissions and arrests lasting between 2 – 4 years. Ultimately, both admissions and arrests rebounded to levels greater than that observed pre-regulation.
_________________________
18
Nonnemaker, J., Engelen, M. and Shive, D, Are methamphetamine precursor control laws effective tools to fight the methamphetamine epidemic? Health Economics , 2011, 20: 519–531.
19
Cunningham and Liu, Impact of methamphetamine precursor chemical legislation, a suppression policy, on the demand for drug treatment. Soc Sci Med.
2008 Apr;66(7):1463-73 .
20
Cunningham and Liu, Impacts of federal precursor chemical regulations on methamphetamine arrests.
Addiction , 2005, 100: 479–488.
14
McKetin et al. conducted a systematic review of methamphetamine precursor regulations published in 2011.
21
The authors used 12 databases to identify studies that had evaluated the impact of methamphetamine precursor regulations on methamphetamine supply and/or use. Ten studies met the inclusion criteria with all interventions occurring between 1989 and 2008 in North America. The outcome measures included both indicators of methamphetamine use (e.g. treatment admissions, hospital admissions, arrests, toxicology) and indictors of methamphetamine supply (e.g., price, purity, seizures and detections of clandestine labs). The results are summarized in Table 2 below.
From this systematic review of the literature, McKetin and colleagues conclude that the effectiveness of legislative efforts to control methamphetamine precursors varies significantly with some effective and others not effective. Additionally, they conclude that regulations coupled with enforcement activities can have the greatest impact but warn that the importation of methamphetamine and its precursors from neighboring countries limits effectiveness of precursor regulations. Further research is needed to determine which precursor regulations work best and in what context.
Table 2: Impact of Methamphetamine Precursor Laws
Intervention (Implementation Date) Type Impact
Moderate Chemical Diversion and Trafficking Act (1989)
Domestic Chemical Diversion
Control Act (1995)
Import/export, wholesale
Import/export, wholesale, retail
Action Against Rogue Pharmaceutical Company And
Large Scale Seizure (1995)
Enforcement
Large
Large
Weak
Ephedrine Regulation (1996)
Large
Pseudoephedrine Regulation (1997)
Methamphetamine Anti-Proliferation Act (2001)
Oklahoma House Bill (2004)
Retail
Retail
Weak
Weak
Texas House Bill (2005) Retail Weak
Source: McKetin, R., Sutherland, R., Bright, D. A. and Norberg, M. M. A systematic review of methamphetamine precursor regulations. Addiction , 2011, 106: 1911–1924.
_________________________
21
McKetin, R., Sutherland, R., Bright, D. A. and Norberg, M. M. A systematic review of methamphetamine precursor regulations. Addiction , 2011, 106: 1911–1924
15
In 2008, Maxwell and Rutkowski conducted a review of available epidemiological information about methamphetamine production and use in North America using a range of sources including historical accounts, peer-reviewed papers, population surveys and large national databases.
22
Of particular interest is the authors’ review of clandestine lab data incidents and the percentage of all substances identified by forensic laboratories that were methamphetamine in the years 1999 – 2006. The results show a marked decrease in lab incidents and in the percentage of all substances identified as methamphetamine in 2006 (following passage of the CMEA). From their review, the authors conclude that “the indicators show the problem is greatest in the western parts of the North American countries and is moving eastward, but that decreased availability of PSE may have a significant impact on the nature of the epidemic in the future, as evidenced by the sharp decline in lab incidents and the percentage of all identified substances that were methamphetamine in 2006.”
22
Most recently, Maxwell and Brecht compiled historical and recent data from supply and demand indicators to provide a broad context within which to consider the changes in trends in the use of methamphetamine over the past five years.
23
To assess trends in indicators of methamphetamine supply, the authors reviewed information from CLSS and STRIDE relative to the number of lab incidents reported, the percentage of all substances identified as methamphetamine, and methamphetamine price and purity over a number of years, respectively. The authors found that lab incidents in the U.S. decreased through 2007 as an initial response to the CMEA but have steadily increased as methamphetamine “cooks” found ways to circumvent the legislation and obtain PSE and other ingredients used to produce the drug.
23
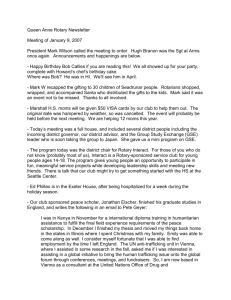
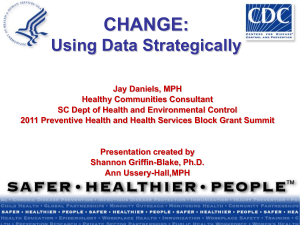
Figure 3 below, adapted from Maxwell and Brecht, depicts lab incidents and percent of all substances identified as methamphetamine by the National Forensic Laboratory Information System (NFLIS).
23
Close review of Figure 3 shows a clear relationship between methamphetamine use as evidenced by the percent of all substances identified as methamphetamine (by the
NFLIS) and the number of clandestine labs, with this indicator of methamphetamine use declining in concert with the number of clandestine lab incidents reported. This tracking relationship provides strong evidence that methamphetamine production in domestic clandestine labs fuels methamphetamine use.
To assess trends in indicators of methamphetamine demand, the authors reviewed information from surveys, including the NSDUH, and on healthcare utilization related to methamphetamine, including data from DAWN and TEDS.
_________________________
22
Maxwell and Rutkowski. The prevalence of methamphetamine and amphetamine abuse in North
America: a review of the indicators, 1992 – 2007. Drug and Alcohol Review , 2008, 27: 229 – 235.
23
Maxwell and Brecht. Methamphetamine: Here we go again? Addictive Behaviors 36, 2011, 1168-1173.
16
From their review of the trends in indicators of methamphetamine demand, the authors conclude that demand for methamphetamine decreased following precursor chemical bans. However, since 2008, trends in indicators of methamphetamine demand are increasing.
Figure 3: Methamphetamine Clandestine Laboratory Incidents and Percent
Methamphetamine Related Tests from the NFLIS, 1999-2010
20000
18000
16000
14000
12000
10000
8000
6000
4000
2000
0
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Lab Incidents % of NFLIS tests with Methamphetamine
8
6
12
10
4
2
0
18
16
14
Ultimately, the authors conclude that the supply and demand data show that methamphetamine indicators are again increasing following a few years of decline in the mid-2000s and suggest that supply-side accommodations occur in response to changes in precursor chemical restriction. The authors conclude that the results “support the need for continuing attention to control and interdiction efforts appropriate to the changing supply context and to continuing prevention efforts and increased number of treatment programs.”
23
B. Impact of State PSE Laws
Since Oklahoma in 2004, states have implemented various precursor control laws in hopes of addressing the methamphetamine abuse problem. Specifically, these regulations target the domestic production of methamphetamine in small clandestine laboratories. Little is known, however, relative to the impact of state PSE regulations.
Two early studies conducted and reviewed by McKetin et al. assessed the impact of the
Oklahoma and Texas House bills passed in 2004 and 2005 respectively. Both laws, which exerted retail controls on PSE, were deemed rather ineffective in controlling
17
methamphetamine abuse.
21
In the following section, available data relative to the impact of varying approaches taken by states to control methamphetamine precursors is summarized. When available, reports from the published literature were reviewed.
Data from other sources, including government reports, reports to state legislators, news reports and personal interviews are included.
Impact of Reclassifying PSE as a Schedule V Controlled Substance
As discussed previously, eleven states including Arkansas, Illinois, Iowa, Kansas,
Louisiana, Minnesota, Missouri, New Mexico, Oklahoma, West Virginia and Wisconsin have reclassified PSE as a Schedule V controlled substance, placing further restrictions on the retail sale of PSE over that imposed by the CMEA. A review of the published literature identified two articles that assessed the impact of making PSE a Schedule V controlled substance.
Oklahoma
In 2004, Oklahoma was the first state to reclassify PSE as a Schedule V controlled substance and impose retail sales restrictions. Brandenburg and colleagues evaluated the association of PSE sales restrictions in Oklahoma on emergency department urine drug screen results using all urine drug screen results in the Saint Francis Hospital
Trauma Emergency Center, in Tulsa, Oklahoma from January 2003 through May
2005.
24
The authors found a significant increase in the total tests performed and the percentage of positive test results for the amphetamine drug class over time. The authors conclude that while the manufacture of methamphetamine in clandestine laboratories declined following implementation of the law, methamphetamine use in the emergency department patient population did not decrease and that possibly, methamphetamine use in Oklahoma was not impacted by the passage of HB 2176 due to an increase in drug trafficking of methamphetamine into the state.
24
Iowa
Senate File 169, which classified PSE as a Schedule V controlled substance, became effective law in Iowa in May, 2005. Burke et al. conducted a study on the impact of this legislation with the outcome of interest being the impact on methamphetamine laboratory-related burns using a retrospective analysis of patients admitted to University of Iowa Burn Treatment Center 2004 and 2005 (pre-post law).
25
_________________________
24
Brandenburg MA, Brown SJ, Arneson WL, Arneson DL. The association of pseudoephedrine sales restrictions on emergency department urine drug screen results in Oklahoma . J Okla State Med Assoc.
2007, 100(11):436-9.
25
Burke BA, Lewis RW, Latenser BA, Chung JY, Willoughby C. Pseudoephedrine legislation decreases methamphetamine laboratory-related burns J Burn Care Res . 2008 Jan-Feb;29(1):138-40.
18
The results demonstrated a decrease in burn admissions related to methamphetamine from 21% in 2004 to 4% in 2005 while no change in treatment admissions to substance abuse treatment centers during same time period were noted. Thus, it appears that
Senate File 169 impacts the production of methamphetamine in clandestine laboratories as evidenced by a reduction in burns, but does not impact indicators of methamphetamine abuse.
According to a report to the Iowa legislature from the Iowa Governor’s Office of Drug
Control Policy published in January, 2006, methamphetamine-related laboratory incidents in Iowa decreased nearly 80% following implementation of the law.
26
Data from the Iowa Division of Narcotics Enforcement showed an average of 125 methamphetamine lab incidents per month during 2004 and an average of 119 per month in the first 5 months of 2005 prior to implementation of the law. Following implementation of the law, an average of 20 methamphetamine lab incidents per month were reported for the remainder of 2005.
26
Review of National Clandestine Laboratory Data
Review of data on the number of methamphetamine clandestine laboratory incidents for the years 2004 – 2010 for all states that currently have PSE classified as a Schedule V controlled substance are shown in Table 3 below. For comparison, the same data are shown for Oregon, which reclassified PSE as a Schedule III controlled substance available via prescription only in 2006.
Table 3: Methamphetamine Clandestine Laboratory Incidents in States with
Schedule V Mandates 2004 – 2010
State
Arkansas
Iowa
Illinois
Kansas
Louisiana
Minnesota
Missouri
2004
806
1441
1173
617
125
171
2820
2005
481
764
955
398
99
93
2240
2006
385
325
761
184
21
37
1300
2007
319
182
362
100
46
27
1261
2008
346
217
311
150
16
21
1477
2009
480
284
399
147
80
13
1769
2010 Trend
483
291
430
148
112
10
1917
New Mexico
Oklahoma
West Virginia
Wisconsin
Oregon (CIII)
121
679
171
90
467
59
237
216
58
190
34
194
86
33
50
36
93
42
5
21
62
134
50
11
19
58
655
52
16
12
45
485
44
25
12 bold = year Schedule V mandated (Schedule III mandate in Oregan presented for comparison)
Source: EPIC ‐ NSS www.justice.gov/dea/concern/map_lab_seizures.html
_________________________
26
Marvin L.Van Haaften. The Impact of Senate File 169 on Meth Abuse in Iowa: A Report to the
Legislature.January17, 2006 available at http://www.state.ia.us/government/odcp/images/pdf/SF169Leg.pdf
, accessed December 19, 2011.
19
In a 2006 report to the legislature, officials from Iowa documented a significant decrease in the number of clandestine lab incidents following the reclassification of PSE as a
Schedule V controlled substance.
26
Review of the data in Table 3 above for the years
2006- 2010 shows that while an initial decrease in lab incidents was observed (from a low of 182 incidents reported in 2007), the number of lab incidents in Iowa is increasing although it remains considerably lower than what was reported in 2004 and 2005 prior to implementation of the Schedule V PSE law.
The passage of Oklahoma’s 2004 law reclassifying PSE as a Schedule V controlled substance had a dramatic impact on methamphetamine clandestine laboratory incidents as shown in Table 3. Reported lab incidents dropped from a high of 679 in 2004 to a low of 93 in 2007. Since 2007, reported clandestine lab incidents have increased considerably, rebounding to levels almost equivalent to those observed prior to implementation of the Schedule V PSE law. Similar trends, suggesting an initial impact followed by some degree of rebound in reported methamphetamine lab incidents are observed in Table 3 for the majority of states that have reclassified PSE as a Schedule
V controlled substance. For comparison, the number of reported lab incidents in
Oregon, which classified PSE as Schedule III controlled substance in 2006, is reported.
The number of reported clandestine methamphetamine lab incidents in Oregon has steadily declined since implementation of the law with no rebound observed to date.
Review of Abuse Indicators
Data from TEDS shows considerable variability in methamphetamine-related treatment admissions to substance abuse treatment facilities (Table 4). In some states, admissions with methamphetamine as the primary substance reported represents up to
20% of admissions in 2010 (Oklahoma) whereas in other states it represents only 1% of admissions (Wisconsin, Illinois).
Data show that methamphetamine abuse continues to be a significant problem and is on the increase in some states after an initial period of decline.
20
Table 4: Number and (Percentage) of Methamphetamine/Amphetamine Treatment
Admissions in States with Schedule V Mandates 2002-2010
State 2004 2005 2006 2007 2008 2009 2010
Arkansas 3471 (25.2) 2943 (21.5) 2605 (17.3) 4340 (15.2) 4037 (16.4) 2544 (18)
Iowa
Illinois
Kansas
Louisiana
5558 (19.7) 5779 (20.3) 4513 (15.8) 3436 (12.8) 2652 (10.1) 2945 (10.6) 4232 (12.8)
2608 (3.2)
1808 (11.7) 2190 (13.9) 1578 (12.1) 1961 (13.1) 1815 10.8) 2036 (10.8) 1912 (12.8)
1055 (3.7)
2568 (3.3)
1229 (4.9)
2395 (2.8)
950 (4.2)
1302 (1.8)
978 (4.0)
1001 (1 .3)
718 (2.8)
892 ( 1.3)
746 (2.6)
948 (1.5)
830 ( 3.2)
Minnesota
Missouri
5934 (12.9) 7159 (15.8) 5380 (11.2) 4903 (9.8)
4914 (12.5) 6154 (14.1) 5295 (11.7) 4513 (9.5)
6386 (7.4) 3600 (6.9) 4139 (8.1)
4544 (9.2) 5056 (9.6) 5088 (10.5)
New Mexico 315 (5.7) 703 (7.7) 910 (7.3) 1018 (8.5) 846 (7.3) 698 (7.0) 668 (9.1)
Oklahoma 4007 (23.5) 4194 (25.1) 3728 (23.8) 3365 (20.4) 2687 (15.8) 2965 (17.5) 2523 (20)
77 (1.7) 175 (2.6) 187 (2.4) 138 (1.8) 147 (1.5) 68 (1.1) 46 (2.1) W.
Virginia
Wisconsin
Oregon
259 (1.1) 483 (1.9)
8561 (19)
443 (1.4) 355 (1.2) 275 (0.9) 289 (1.0) 308 (1.0)
10062 (21.1) 9226 (18.8) 8803 (16.8) 7354 (13.9) 6283 (12.9) 6650 (14.1)
Bold = year Schedule V mandated (CIII mandate in Oregon presented for comparison)
Source: http://wwwdasis.samhsa.gov/webt/newmapv1.htm
Is Reclassifying Pseudoephedrine as a Schedule V Controlled Substance Effective?
Taken together, the information suggests that implementation of state laws relative to reclassifying PSE as a Schedule V controlled substance has an initial impact on the number of clandestine lab incidents and associated hazards, but may not have an impact on indicators of abuse. A significant rebound effect in clandestine lab incidents is observed in most states that have implemented such laws, with the exception of
Minnesota and West Virginia (Table 3).
Impact of Electronic Tracking
Published data demonstrating the impact of tracking programs is somewhat lacking as the approach is relatively new. Theoretically, electronic tracking can provide an advantage over paper logs as data are centralized and can be shared among retail sellers of PSE in a state, and, in many instances, across state lines. Proponents of a national electronic tracking system cite data from NPLEx relative to block of sales in states currently using the system as evidence that NPLEx works. According to the
NPLEx website, during 2011 participating pharmacies sold 58,124,904 grams of PSE with the sale of 1,784,618 grams blocked by NPLEx.
27
_________________________
27
National Precursor Log Exchange Stats, available at http://nplexservice.com/index.html
, accessed
December 29, 2011.
21
Block of sales data for 11 of the 17 states currently using NPLEx is presented in Table 5 below. Data for 6 states which recently enacted electronic tracking laws are excluded as no 2011 data is available.
Table 5: Purchases and Block of Sales (Rate per 1,000 People) in States with
Electronic Tracking, 2011
State Purchases
Purchases
Blocked
Grams Sold
Grams
Blocked
Alabama
Florida
Illinois
Iowa
Kansas
1
1,529,300
(320)
3,950,769
(210)
3,030,382
(236)
896,292
(294)
512,249
(180)
88,141
(18)
109,093
(6)
54,548
(4)
23,262
(8)
13,494
(5)
3,234,317
(677)
7,845,934
(417)
5,662,341
(441)
1,820,827
(598)
1,110,700
(389)
219,608
(46)
289,499
(15)
137,482
(11)
61,555
(20)
39,583
(14)
Kentucky
Louisiana
1,302,254
(300)
1,139,099
(251)
29,141
(7)
28,577
(6)
2,742,849
632
2,300,520
(507)
78,188
(18)
74,801
(17)
Missouri
North Dakota
3
1,665,681
(278)
19,887
(30)
45,581
(8)
472
(1)
3,518,397
(587)
27,503
(41)
121,174
(20)
1,437
(2)
South Carolina
1,191,258
(258)
41,211
(9)
2,379,308
(514)
108,281
(23)
Washington
2
292,333
(158)
4,226
(2)
539,143
(291)
11,068
(6)
1 partial year data from May – Dec, 2011;
2 partial year data from Oct –Dec, 2011;
3 partial year data from Nov – Dec, 2011
Source: Aaron Davis, NPLEx, Manager, Creative Services via email January 5, 2011.
Review of National Clandestine Laboratory Data
Review of data on the number of methamphetamine clandestine laboratory incidents for the years 2004 – 2011 for all states that currently have enacted electronic tracking laws are shown in Table 6 below. For comparison, the same data are shown for Oregon and
Mississippi which reclassified PSE as a Schedule III controlled substance available via prescription only in 2006 and 2010, respectively.
22
Table 6: Methamphetamine Clandestine Laboratory Incidents in States with
Electronic Tracking, 2004- 2011
E ‐ Tracking States
Alabama
Florida
Illinois
Indiana
Iowa
Kansas
Kentucky
Louisiana
Michigan
Missouri
Nebraska
North Carolina
North Dakota
Oklahoma
2004
468
282
1173
1132
1441
617
589
125
300
2820
269
322
236
679
2005
290
274
955
1057
764
395
580
99
347
2240
248
322
170
237
2006
205
142
761
760
325
184
326
21
260
1300
31
190
39
194
2007
216
128
362
803
182
100
297
46
174
1261
26
153
27
93
2008
605
135
311
739
217
150
427
16
337
1477
57
196
33
134
2009
614
321
399
1139
284
147
705
80
638
1769
32
202
36
655
South Carolina
Tennessee
Texas
Washington
191
589
497
944
142
580
272
546
69
793
135
337
26
559
93
238
56
582
123
127
99
705
155
72
125
1199
111
44
Rx States
Mississippi 320 222 253 155 299 691 698
Oregon 467 190 50 21 19 12 12 bold = year electronic tracking implemented (CIII mandate in Oregon and Mississippi presented for comparison)
1070
112
679
1917
18
234
8
485
2010 Trend *2011
666
316
148
57
430
1213
291
148
481
661
260
132
770
32
293
1744
132
277
2
659
259
8
186
5
44
19
Source:EPIC ‐ NSS www.justice.gov/dea/concern/map_lab_seizures.html
*2011 data is a partial year through October 2011.
Oklahoma began electronically tracking PSE in 2006. The law was initially thought to be successful as lab incidents dropped from 679 in 2004 to 93 in 2007 (Table 6).
However, this trend quickly reversed with lab incidents increasing to a high of 655 in
2009.
Kentucky was the first state to fully implement electronic tracking with MethCheck, the system currently utilized in the NPLEx program, in 2008. As depicted in Table 6 above, the number of reported methamphetamine in clandestine laboratory incidents has climbed steadily since electronic tracking was implemented – from a low of 297 in 2007 to a high of 1070 in 2010. Trend lines for most states show an initial decline around
2005 or 2006 following retail sales control measures implemented by states and the
CMEA, with a rebound effect. Thus, electronic tracking laws do not appear to be having a sustainable impact on the domestic production of methamphetamine by clandestine labs as evidenced by the numbers of reported lab incidents.
23
Review of Abuse Indicators
Because electronic tracking laws have been enacted by states relatively recently, data on indicators of methamphetamine abuse to document impact are lacking. Using the examples of Oklahoma and Kentucky, which have the longest history with electronic tracking, review of TEDS data as an indicator of abuse shows that methamphetamine abuse continues to be a significant problem in these states and is on the increase after an initial period of decline following implementation of electronic tracking laws (Table 7).
For comparison, data for Oregon (PSE Schedule III available by prescription only) is also presented.
Table 7: Number and (Percentage) of Methamphetamine/Amphetamine Treatment
Admissions in States with Electronic Tracking Mandates, 2002-2010
State 2002 2003 2004 2005 2006 2007 2008 2009 2010
Kentucky 455
(1.7)
Oklahoma 3471
(19.3)
Oregon
(CIII)
9463
(16.9)
696
(2.2)
532
(2.6)
3555
(21.6)
4007
(923.5)
7548
(16.6)
8561
(19)
1307
(5.8)
4194
(25.1)
1249
(5.1)
3728
(23.8)
1045
(4.3)
3365
(20.4)
844
(3.8)
833
(3.9)
2687
(15.8)
2965
(17.5)
10062
(21.1)
9226
(18.8)
8803
(16.8)
7354
(13.9)
6283
(12.9)
1027
(4.6)
2523
(20)
6650
(14.1)
Bold = year electronic tracking implemented (CIII mandate in Oregon presented for comparison)
Source: http://wwwdasis.samhsa.gov/webt/newmapv1.htm
Since the implementation of electronic tracking in Kentucky in 2008, the number and percentage of methamphetamine/amphetamine admissions to substance abuse treatment facilities reported to SAMSHA has increased from 833 (3.8%) in 2008 to 1027
(4.6%) in 2010. Oklahoma, which implemented electronic tracking in 2006 showed an initial decline in the percentage of methamphetamine/amphetamine treatment admissions, from 23.8% in 2006 to 15.8% in 2008. Since 2008, the percentage of admissions related to methamphetamine-amphetamine has risen each year representing 20% of all admissions in 2010, although the number of admissions declined to 2523 in 2010.
Is Electronic Tracking Effective?
Although data are limited due to the recent nature of implementation of electronic tracking laws, review of the information available suggests that implementation of state laws relative to electronic tracking may have an initial and perhaps transient impact on indicators of abuse (admissions to substance abuse treatment facilities) but little to no impact on the number of clandestine lab incidents reported.
24
Many believe electronic tracking and block of sales to persons trying to purchase more than the legal limit of PSE may have little impact on the practice of ‘smurfing’.
28
Smurfing is a method used by some methamphetamine traffickers to acquire large quantities of PSE. Individuals purchase PSE in quantities at or below legal thresholds from multiple retail locations, with traffickers often enlisting the assistance of several associates in smurfing operations to increase the speed with which chemicals are acquired.
29
Each associate may use multiple fake identification cards to purchase quantities of PSE that exceed legal limits.
The U.S. Department of Justice, National Drug Intelligence Center’s annual National
Drug Threat Assessment reports that despite federal and state pseudoephedrine sales restrictions in the U.S., the overall incidence of smurfing has increased, facilitating the concurrent rise in domestic methamphetamine production between 2007 and 2010.
30
The DEA also does not believe that electronic tracking is an effective solution. In a testimony to the Senate Caucus on International Narcotics Control, Joseph T.
Rannazzisi, Deputy Assistant Administrator in the DEA Office of Diversion Control suggests that based on the DEA's experience, as well as numerous State and local law enforcement agencies across the country investigating methamphetamine labs, “a national electronic logbook system will not be an effective measure to prevent methamphetamine production because it represents a reactive approach to the problem that will tie up significant law enforcement resources. Additionally, smurfers will continue to circumvent any such program by means they currently employ, such as using multiple false IDs to purchase precursor chemicals.”
31
Proponents of electronic tracking suggest that it’s too early to judge the impact using abuse indicators and that block of sales data show that electronic tracking is having an impact and is stopping illegal sales.
_________________________
28
VanderWall, et al. Controlling methamphetamine precursors: the view from the trenches. National
Institute of Justice Report, May 30,2008. Available at https://www.ncjrs.gov/pdffiles1/nij/grants/223480.pdf
, accessed October 11, 2011.
29
Situation Report: Pseudoephedrine Smurfing Fuels Surge in Large-Scale Methamphetamine Production in California, available at http://www.justice.gov/ndic/pubs36/36407/index.htm
, accessed December 18,
2011.
30
National Drug Intelligence Center, National Drug Threat Assessment, 2011, available at http://www.justice.gov/ndic/pubs44/44849/44849p.pdf
, accessed January 4, 2011.
31
Written Statement of Joseph T. Rannazzisi, Deputy Assistant Administrator, DEA Office of Diversion
Control. . “The Status of Meth: Oregon's Experience Making Pseudoephedrine Prescription Only”
Presented to Senate Caucus on International Narcotics Control, April 2010, available at http://www.justice.gov/dea/speeches/s041310.pdf
, accessed January 2, 2012.
25
The most vocal proponent of electronic tracking is the Consumer Healthcare Products
Association (CHPA), a trade association representing the pharmaceutical manufacturers of OTC products. According to the CHPA, the sale of PSE-containing products represents a $600 million dollar industry (excluding sales at Wal-Mart) in the
US.
32
The CHPA provides funding for states to use the NPLEx tracking system free of charge and have lobbied heavily for implementation of a national electronic tracking system (NPLEx) to address the methamphetamine abuse problem.
32,33
Recently, support for electronic tracking was expressed by consumers in a survey conducted by the Asthma and Allergy Foundation of America (AAFA). The survey collected information from consumers regarding use of OTC PSE-containing products and gathered consumer opinions on approaches for controlling access to PSE products as a means of addressing methamphetamine abuse. The AAFA’s National
Pseudoephedrine Awareness Study, which was developed and administered by Harris
Interactive and supported by a grant from the CHPA, was conducted online in July 2010 among more than 2,000 U.S. adults age 18+ who personally suffered from asthma, allergies, cold, cough or flu in the preceding 12 months and purchased OTC medications for at least one condition during that time.
34
According to the AAFA, the study, provides evidence that 58% of consumers/patients surveyed support electronic tracking while 21% oppose it.
35
Impact of Prescription Only/Reclassification as Schedule III Controlled Substance
Oregon, the first state to adopt a law reclassifying PSE as Schedule III controlled substance making it available by prescription-only, has seen a steady reduction in the number of methamphetamine lab incidents since the rules were adopted in April, 2006.
According to the DEA, Oregon had only 12 methamphetamine lab incidents from
January 1, 2009 to December 31, 2009, a 94% decrease from the year prior to the prescription only law (Table 6).
_________________________
32
CHPA Testimony of Linda Suydam, D.P.A on behalf of the Consumer Healthcare Products Association.
U.S. Senate Caucus on International Narcotics Enforcement, April 13, 2010, available at http://drugcaucus.senate.gov/suydam-final-CHPA-4-13-10.pdf
, accessed January 5, 2011.
33
Lobbying Report, 2md Quarter 2010, Consumer Healthcare Products Association. Available at http://soprweb.senate.gov/index.cfm?event=getFilingDetails&filingID=cb4ed426-ebeb-4a35-b9d4-
62913212a3b6 , accessed January 4, 2011.
34
Asthma and Allergy Foundation of America. Patients oppose prescription mandate for OTAC medicines containing pseudoephedrine, available at http://www.aafa.org/display.cfm?id=5&sub=105&cont=725, accessed January 4, 2011.
35
Asthma and Allergy Foundation of America.
Pseudoephedrine (PSE) Awareness Study –Executive
External Report, available at http://aafa.org/pdfs/Executive%20External%20Report%20FINAL1.pdf
, accessed January 4, 2011.
26
Hendrickson et al. conducted a study to determine if the Schedule III, prescription-only legislation enacted in July, 2006, altered the number of ED visits related to methamphetamine use.
36
The study was a retrospective analysis of a database created during a prospective study that required ED clinicians to determine if a patient’s visit was related to methamphetamine and if the patient had confirmed use of methamphetamine. The authors conclude that the enactment of the legislation which limited PSE availability decreased methamphetamine-related ED visits and decreased the number of patients with confirmed use of methamphetamine in the study ED.
Information compiled by the Oregon Alliance of Drug Endangered Children indicate that since the implementation of Oregon’s law, Oregon has experienced a 96% reduction in methamphetamine lab incidents, a 32% reduction in methamphetamine-related arrests, a 33% reduction in methamphetamine-related treatment admissions, a 35% reduction in methamphetamine-related ED visits, and have seen the largest decrease in crime rates in the nation.
37
Mississippi
The Mississippi Bureau of Narcotics reports a nearly 70% decrease in methamphetamine-related cases statewide since the implementation of Mississippi’s law reclassifying PSE as a Schedule III controlled substance available by prescription only in 2010. Comparing data from the periods of July 2009 to February 2010 (prior to the prescription only law) with data from July 2010 to February 2011 (after implementation of the prescription only law) shows a reduction from 607 methamphetamine lab incidents to 203 methamphetamine lab incidents in Mississippi.
38
Additionally, as reported in the 2011 National Drug Threat Assessment, law enforcement reporting from the Jackson County (MS) Narcotic Task Force indicates a decrease in methamphetamine production and methamphetamine-related arrests in the task force’s area of responsibility since the law’s passage.
39
_________________________
36
Hendrickson et al. The association of controlling PSE availability on methamphetamine-related ED visits. Soc for Acad Emerg Med 17:1216-1222; 2010.
37
Oregon Alliance of Drug Endangered Children. Methamphetamine - Oregon Fact Sheet. Available at http://www.oregondec.org/OregonFactSheet.pdf
, accessed January 4, 2011.
38
National Association of Boards of Pharmacy, Boards of Pharmacy, State Legislators, and Law
Enforcement Continue to Tackle Methamphetamine Problem., available at http://www.nabp.net/news/boards-of-pharmacy-state-legislators-and-law-enforcement-continue-to-tacklemethamphetamine-problem/ , accessed December 29, 2011.
39
National Drug Intelligence Center, National Drug Threat Assessment, 2011, available at http://www.justice.gov/ndic/pubs44/44849/44849p.pdf
, accessed January 4, 2011.
27
Is Prescription only/reclassification as Schedule III Controlled Substance Effective?
Although data are limited to the experiences of Oregon, and more recently Mississippi, review of the information available suggests that implementation of state laws reclassifying PSE as a Schedule III controlled substance available by prescription only is extremely effective at reducing the number of clandestine lab incidents and associated hazards (Table 6)
.40
Additionally, methamphetamine-related crime and arrests have also decreased since implementation of the law. Data on indicators of methamphetamine abuse show a steady reduction in methamphetamine-related admissions to substance abuse treatment facilities reported to SAMSHA from 2006 -
2009, with a slight increase in admissions in 2010 (Table 7). Thus it appears that a prescription only/CIII controlled substance mandate may have a sustained impact on domestic clandestine lab incidents and associated hazards and crime, but further data are needed to determine if indicators of methamphetamine abuse are rebounding.
It should be noted that methamphetamine lab incidents reported to EPIC have also decreased in other states on the west coast that do not have a PSE prescription-only mandate. For example, clandestine lab incidents in Washington decreased from 337 in
2006 to 44 in 2010 (Table 6). A recent report by Stomberg and Sharma suggests that
Oregon’s prescription only PSE mandate did not reduce methamphetamine use and that a regional trend is observed relative to reductions in clandestine lab incidents across Oregon and neighboring states. The authors conclude that while the exact mechanism behind this shared decline is not known, technological or market changes unrelated to Oregon’s PSE prescription mandate would appear to be the cause.
41
Opponents of making PSE available only by prescription suggest that this measure would place undue burden on doctors, pharmacists, insurance companies and consumers. The CHPA is the most vocal opponent of prescription-only mandates.
They have undertaken an aggressive public awareness campaign – Stop Meth. Not
Meds., which highlights the advantages of electronic tracking of PSE purchases and the disadvantages of prescription only mandates.
42
_________________________
40
Oregon Alliance of Drug Endangered Children. Methamphetamine - Oregon Fact Sheet. Available at http://www.oregondec.org/OregonFactSheet.pdf
, accessed January 4, 2011.
41
Making Cold Medicine Rx Only Did Not Reduce Meth Use. Analyzing the Impact of Oregon’s
Prescription-Only Pseudoephedrine Requirement. Available at http://cascadepolicy.org/pdf/pub/Oregon_Meth_Law.pdf
, accessed March 11, 2012.
42
Stop meth. Not meds. Consumer Healthcare Products Association, available at http://stopmethnotmeds.com/ , accessed January 4, 2011.
28
The CHPA asserts that under prescription-only mandates, consumers will bear new costs for repeated doctor visits and prescriptions and healthcare payers will be forced to incur new costs or leave consumers on their own to cover all the costs associated with acquiring PSE through a prescription.
42
They also assert that moving PSE to prescription only will remove purchase limits such that methamphetamine ‘cooks’ can purchase unlimited amounts of PSE with a prescription. Representatives from Oregon, the only state with significant experience relative to a prescription-only mandate, have reported that these concerns have not been realized.
43
The CHPA also warns there is no system for real-time blocking of illegal sales for prescription drugs. However, in the case of Oregon and Mississippi, the prescription only mandates have been coupled with reclassification of PSE as a Schedule III controlled substance. Thus, as stated previously, reporting and tracking through the state’s PMP is required. When included in the PMP database with other controlled substances, healthcare providers and law enforcement can access the data as allowed under state law.
According to the previously discussed AAFA survey funded by the CHPA, the results
“provide a major indication that patients would like to see alternate measures that don't force a prescription mandate on the millions of law-abiding patients who rely on these
OTC medicines.”
44
This conclusion is drawn from the survey results which indicate that
66% of patients responding oppose prescription mandate laws, citing cost/insurance coverage issues and the inconvenience associated with needing a prescription for PSE as the main reasons for opposition.
45
Further review of the AAFA survey results show that 74% of consumers/patients fill prescriptions occasionally to frequently.
45
Although consumers surveyed voiced opinions in opposition to prescription only mandates for
PSE due in part to inconvenience, the data indicate that the majority (74%) are filling prescriptions at least occasionally, thus prescription access does not appear to be a barrier for most consumers.
Proponents of a prescription only mandate argue that the majority of PSE purchased
OTC is diverted for illicit methamphetamine production in small clandestine laboratories that create hazards for citizens, children and law enforcement officers and cost millions of dollars each year for clean-up.
_________________________
43
Oregon Alliance of Drug Endangered Children. Methamphetamine - Oregon Fact Sheet. Available at http://www.oregondec.org/OregonFactSheet.pdf
, accessed January 4, 2011.
44
Asthma and Allergy Foundation of America. Patients oppose prescription mandate for OTC medicines containing pseudoephedrine, available at http://www.aafa.org/display.cfm?id=5&sub=105&cont=725, accessed January 4, 2011.
45
Asthma and Allergy Foundation of America. Pseudoephedrine (PSE) Awareness Study –Executive
External Report, available at http://aafa.org/pdfs/Executive%20External%20Report%20FINAL1.pdf
, accessed January 4, 2011.
29
Although data on the proportion of PSE sales that are purchased for use in the illicit production of methamphetamine is lacking, recent estimates from law enforcement agents engaged in methamphetamine diversion investigations suggest that 50 - 90% of all PSE purchases are diverted to make methamphetamine.
46
Others have suggested that 50% of PSE sales are for legitimate medical needs.
47
If these estimates are, in fact accurate, then the pharmaceutical industry stands to lose between $300 – 500 million in sales annually if PSE is returned to prescription status.
Review of the data from the AAFA survey’s Executive Summary provides some additional information. When faced with having to buy PSE from behind the counter,
36% say they stop and buy it there, while more than one-half choose to buy an alternative product that is available in the regular OTC aisle and 12% choose not to buy a product at all.
45
These results may provide support for those with the opinion that the majority of PSE sales are for illegitimate purposes, if in fact, the majority of individuals requiring a decongestant choose to purchase alternative products that have unrestricted availability as suggested by the AAFA survey.
Overall, this review of the available evidence suggests that federal regulations aimed at controlling access to methamphetamine precursors have had mixed results. While early regulations targeted at the wholesale distribution of precursor chemicals had a large, sustained initial impact, more recent regulations aimed at controlling the retail sale of precursors (ephedrine, PPA and PSE) have been less effective. Data indicate an initial impact following these supply side reductions which rebounds after creative individuals find a way to circumvent new restrictions.
Most published research has focused on impact of federal legislation although a few small studies show state impact with limited data. Three main approaches to controlling access to PSE (Schedule V controlled substance, electronic tracking and Prescription only/CIII controlled substance mandates) show varying results. Mandates that classify
PSE as a Schedule V controlled substance, for the most part, have not elicited a sustained impact on indicators of methamphetamine production in small clandestine labs or methamphetamine abuse.
_________________________
46
Stop meth making meds. The truth about the Oregon Experience , Oregon Alliance for Drug Endangered
Children. Available at http://www.oregondec.org/ResponseToIndustryPowerPoint.pdf
, accessed January
5, 2011.
47
Kent Shaw, Assistant Chief, California Attorney General’s Office, Bureau of Narcotic Enforcement.
Letter to the Editor – Turlock Journal, Prescription Pseudoephedrine Policy , available at http://www.turlockjournal.com/archives/6745/ ; accessed January 4, 2011.
30
Although evidence is limited due to many states having enacted electronic tracking laws very recently, it appears the success of electronic tracking coupled with block of sales has been limited by continued ‘smurfing’. States with the most experience with this mandate, such as Kentucky, continue to report increases in the number of clandestine lab incidents and it appears smurfing in these states continues to be a problem.
Mandates that classify PSE as a Schedule III controlled substance, thus making it available only with a prescription from a licensed health care provider, appear to have the most impact to date, although again the evidence is limited as only Oregon has significant experience with this type of mandate.
Shifts across state lines in response to a state’s regulatory attempts have been documented, as is suggested by the recent adoption of Mississippi’s prescription only/CIII mandate and the increases in PSE sales observed in the states bordering
Mississippi after passage of its law.
48
These shifts ultimately limit the overall impact that an individual state approach can have and suggest that a strong federal mandate for controlling PSE precursors might have a greater impact.
From the review of the data, it appears that Oregon’s Schedule III/prescription only mandate has elicited a sustained reduction on number of clandestine lab incidents reported and, until 2010, decreases in indicators of methamphetamine abuse.
Considering the societal costs and hazards associated with the manufacture of methamphetamine in small clandestine labs, a mandate which has a sustained impact on lab incidents, even if overall indicators of methamphetamine abuse are unchanged, could have a significant public health impact.
It should be noted that the federal and state mandates relative to methamphetamine precursor control have generally focused on influencing the supply side of the methamphetamine abuse equation. These supply side interventions show initial impact which rebound after creative individuals find a way to circumvent new restrictions.
Thus, states grappling with the methamphetamine abuse problems should consider policy changes focused on prevention and treatment that impact the demand side of the methamphetamine abuse equation as well.
_________________________
48
Stop meth making meds. The truth about the Oregon Experience , Oregon Alliance for Drug Endangered
Children. Available at http://www.oregondec.org/ResponseToIndustryPowerPoint.pdf
, accessed January
5, 2011.
31
Although continued evaluation of changes in supply and demand indicators of methamphetamine abuse in response to state and federal regulatory attempts is warranted and comprehensive outcomes analyses of impact are needed, using the evidence available to date, Figure 4 summarizes the potential impact of specific approaches taken to date and provides recommendations for future policy consideration.
Figure 4: Summary of Key Findings and Recommendations for Reducing
Methamphetamine Abuse and Clandestine Laboratories
High
Federal
Of
Wholesale
Precursor
Regulation
Chemicals
State Specific
State Specific
Schedule V for PSE
E ‐ Tracking
Federal
Schedule III for PSE
State Specific
Schedule III for PSE
Low
Impact on Clandestine Laboratories
High
32
VI. Appendix
The following pages provide a summary of state laws and regulations relative to methamphetamine precursor controls, legislative initiatives in 2011, and pending legislation (as of January 2012). Additionally, information on methamphetamine laboratory incidents, methamphetamine-related admissions to substance abuse treatment facilities and the state census population is also presented.
33
State
Alabama
Alaska
Arizona
Arkansas
California
Colorado
Connecticut
District of
Columbia
2010 Meth.
Lab
Incidents (number, rate * 100,000)
666 14
2009 TEDS Meth.
Admissions
(number, rate *
100,000)
Electronic
Tracking
PSE is a
Controlled
Substance
Greater
Limit on
Purchase
Quantity
Meth
Registry/
Block Sales
1,809
38 Y N N N
11 2
324
46 N V Y N
45 1
3,575
56 N N N N
483 17
4,092
140 Y N N N
186 0
62,040
167 N N N N
17 0
7,489
149 N N N N
0 0
114
3 N N N N
0 0 0 N N N N
Pending Legislation
N
N
N
N
N
in 2012
HB 29, SB 23, SB 52.
(require Rx)
N
AB 1280, E ‐ Tracking; SB 315, require
Rx
Delaware 0 0
37
4 N N N N N
Florida 316 2
1,665
9 Y N N N N
Georgia 155 2 0 N N N N HB 437, E ‐ Tracking
Legislation
2011 but
discussed not
N
N
Require Rx
passed in
Require Rx quantity restrictions, E ‐ tracking,
Require Rx
Require Rx, Resolution to ask
Congress to make PSE Rx
N
N
N
N
Hawaii 3 0
2,564
2,190
188 N N N N HB 35 & SB 586, require Rx
N
E ‐ Tracking
Require Rx, E ‐ Tracking, quantity limits
N
Idaho
Illinois
Indiana
9
430
1,213
1
3
19
1,395
1,689
140
11
26
N
Y
Y
N
V
N
N
N
Y
N
N
N
SB 73, E ‐ Tracking
PR 3420, E ‐ Tracking
N
Require Rx
5,688
N
N
Iowa
Kansas
Kentucky
291
148
1,070
10
5
25
4,114
1,295
187
144
30
Y
Y
Y
V
V
N
Y
N
N
N
N
N
HB 2098 & SB 131, require Rx
BR 101, lowers limits; BR 396, create registry; BR 403, legend drug
Require Rx
Require Rx, quantity limits
State
Louisiana
Maine
Maryland
2010
Census
Population
2010 Meth.
Lab Incidents
(number, rate * 100,000)
4,533,372 112 2
1,328,361
5,773,552
Massachussets 6,547,629
5
2
1
0
0
0
2009 TEDS Meth.
Admissions (number, rate * 1000000)
1,267
114
201
220
28
9
3
3
Michigan
Minnesota
Mississippi
Missouri
Montana
New Jersey
New Mexico
New
North
North
York
Carolina
Dakota
9,883,640
5,303,925
2,967,297
5,988,927
989,415
Nebraska
Nevada
1,826,341
2,700,551
New Hampshire 1,316,470
8,791,894
2,059,179
19,378,102
9,535,483
672,591
679
10
698
1,917
12
148
8
6
0
45
31
106
8
7
0
24
32
1
8
0
0
0
2
0
1
1
860
6,255
573
8,977
1,431
1,872
2,725
78
259
684
1,050
1,041
393
9
118
19
150
145
103
101
6
3
33
5
11
58
Y
N
N
Y
N
N
N
Electronic
Tracking
Y
N
N
N
N
N
N
N
PSE is a
Controlled
Substance
N
N
N
N
N
V
III, requires
Rx
V
N
N
N
N
N
V
N
Greater
Limit on
Purchase
Quantity
N
N
N
N
N
Y
Meth
Registry/
Block Sales
N
N
N
N
Pending
Legislation
2012
Legislation discussed in
2011 but not passed
N N
LR 2544, E ‐
Tracking
N
N N
N N
N
N
HB 4662, PSE to prescription status
E ‐ Tracking,
Require Rx, quantity limits
N Require Rx
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
E ‐ Tracking,
Require Rx
N
E ‐ Tracking
Require Rx N
N
N
N
N
N
SB 5036 & AB
8384, E ‐
Tracking; AB
7753, penalty for quantity exceptions
N
E ‐ Tracking,
Quantity lmits
Y
Y
N
N
N
N
N
N
HB 773, establish review of meth problems
N
E ‐ Tracking, commission study of problem
E ‐ Tracking
State
Ohio
Oklahoma
Oregon
Pennsylvania
Rhode Island
2010
Census
Population
2010 Meth.
Lab Incidents
(number, rate * 100,000)
2009 TEDS Meth.
Admissions (number, rate * 1000000)
11,536,504
3,751,351
3,831,074
12,702,379
1,052,567
South Carolina 4,625,364
South Dakota 814,180
239
485
12
34
0
125
9
2
13
0
0
0
3
1
960
4,043
11,084
370
22
804
1,565
8
108
289
3
2
17
192
Electronic
Tracking
N
Y
N
N
N
Y
N
PSE
N is a
Controlled
Substance
V
III, requires
Rx
N
N
N
N
Greater
Limit on
Purchase
Quantity
Meth
Registry/
Block Sales
N
N
N
N
N
N
N
N
Y
N
N
N
N
N
Pending Legislation
2012
Legislation discussed in
2011 but not passed
HB 334, E ‐ Tracking
N
N
Require Rx, establish task force
N
N
N
N
N
N
N
N
N
N
Tennessee
Texas
Utah
Vermont
Virginia
6,346,105
25,145,561
2,763,885
625,741
8,001,024
West Virginia 6,724,540
Washington 1,852,994
1,199
111
7
3
106
44
44
19
0
0
0
1
1
2
291
5,771
3,579
32
669
8,748
76
5
23
129
5
8
130
4
Y
Y
N
N
N
Y
Y
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
HB 5, inc.
registry time; HB
181, Rx; HB 234,HB 288 &
HB 699, E ‐ Tracking; HB
1048 & SB 2020, purchase limits; HB 1537 & SB 1503,
RPh counseling; HB 1990,
CS status; SB 325, E ‐
Tracking; SB 332 & SB 561
& SB 1534, Rx
Require Rx, E ‐
Tracking, RPh counseling
Quantity limits, allow local regulation of
PSE
N
N
N
N
HB 2946, Rx
N
N
N
Require Rx
Require Rx
N
458
Wisconsin
Wyoming
5,686,986
563,626
25
7
0
1 1,281
8
227
N
Y
V
N
Y
N
N
N
AB 203, purchase limit reduction
N
N
E ‐ Tracking