1/19/2016
History/ Mechanism
1. Chief Complaint
Elbow Evaluation
Tell me about your problem
Athletic Medicine
History/ Mechanism
History/ Mechanism
2. History of Present Problem
3. Time Sequence
a. When did you first notice the symptoms?
b. Have you had any history of this problem or other related
problem areas?
c. Has anyone in your family had similar symptoms?
d. What activity were you engaged in at onset of symptoms?
e. Was there any change in activity recently? (running, diet,
sleep)
f. Did you hear or feel anything at time of onset?
g. Any specific mechanism (cause) you were aware of at the
time?
a.
b.
c.
d.
Was onset of symptoms sudden or gradual?
How long did symptoms last?
Have symptoms been constant or intermittent?
When do symptoms typically occur? (during activity,
after?)
History/ Mechanism
History/ Mechanism
4. Location of Symptoms
5. Symptom Characteristics
a. Point with one finger to area where symptoms most
severe.
b. Is there more than one area of symptoms?
a. Characterize the pain? (dull, sharp, throbbing,
burning, aching)
b. Does the pain radiate and where?
c. What relieves the pain?
d. What increases the pain?
e. How do symptoms affect your activity level?
1
1/19/2016
History/ Mechanism
History/ Mechanism
6. Participation Characteristics
7. Personal Management
a. What sport?
b. What position or event?
c. What are the frequency, duration and intensity of
your practice?
d. Could equipment be related to your symptoms? If
yes, what type, kind, vintage?
e. What type of playing environment?
f. What type of warm-up pattern?
Observation
a. Have you attempted any treatment?
b. Have you taken any medication?
c. Have you seen anyone else for the problem? If yes,
who and what was their impression?
d. Do you have any opinions of your own as to what is
your problem?
Elbow - HOPS
1. Remove clothing bilaterally (use discretion)
2. Deformity
3. Bleeding
4. Scars
5. Discoloration
6. Coloration
7. Swelling
8. Compare bilaterally (compare to other side)
9. Observe body movement
10. Arm swing
11. Carrying angle
12. Olecranon bursa
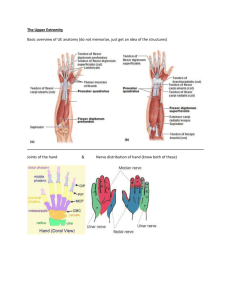
• History: same general questions
• Observation:
– Carrying angle: angle from humerus to ulna
• Usually 10-15 degrees
– Triangle formed by epicondyles and olecranon
process
• Observations
– Deformities and swelling?
– Carrying angle
• Cubitus valgus versus cubitus
varus
– Flexion and extension
• Cubitus recurvatum
– Elbow at 45 degrees
Figure 23-5
• Isosceles triangle (olecranon
and epicondyles)
Figure 23-8
Figure 23-7
© 2011 McGraw-Hill Higher Education. All
rights reserved.
2
1/19/2016
Palpation
1.
2.
3.
4.
Medial epicondyle
Lateral epicondyle
Olecranon process/fossa
Radial head
2
1
3f
2
4
1
3p
Palpation
5. Bicep tendon
6. Brachial artery
5
6
5
Palpation
Palpation
8. Flexors
7. Olecranon bursa
8
9. Extensors
7
9
3
1/19/2016
Palpation
10. Pronators
10
11. Supinators
11
Palpation
Palpation
10. Radius
11. Ulna
14. Tricep Tendon
15
14
15. Ulnar Nerve
10
11
4
1/19/2016
Palpation
Palpation
17. UCL (MCL)
18
17
16. Humerus
18. RCL (LCL)-AREA.
(LIGAMENT NOT
DIRECTLY PALPABLE)
Palpation
19. Radial Artery
20. Coronoid (Cubital)
fossa
19
Range of Motion
• *Should test in active, passive, and resistive
motions and compare bilaterally.
•
1. Flexion
•
2. Extension
•
3. Supination
•
4. Pronation
20
Stress Tests
1. Valgus/varus stress (Ulnar/Radial collateral ligaments), 0 and 30 Degrees’
2. When elbow in flexion:
a. olecranon, lateral epicondyle, and medial epicondyle = triangle
If this is not so = possible fx.
3. When elbow in extension:
a. olecranon, lateral epicondyle, and medial epicondyle= straight line
If this is not so= possible fx.
4. Medial Epicondylitis--Little League/Golfer’s elbow
5. Lateral Epicondylitis--Tennis Elbow
6. Tinel Sign
5
1/19/2016
Elbow – HOPS (cont.)
• Special/Stress Tests:
– Valgus/Varus Stress Test
• Assess injury to the medial and lateral collateral
ligaments, respectively
• Looking for gapping or complaint of pain
– Circulation
– Tinel’s sign:
•
•
•
•
Designed to determine ulnar nerve compromise
Ulnar nerve test
Tap on ulnar nerve (in ulnar groove)
Positive test is found when athlete complains of
sensation along the forearm and hand
– Valgus/Varus ligament tests
Figure 23-10
• Same as knee collateral tests
© 2011 McGraw-Hill Higher Education. All
rights reserved.
Elbow – HOPS (cont.)
• Special/Stress Tests:
– Medial/Lateral Epicondylitis Tests
• Elbow flexed to 45 degrees and wrist extension is
resisted (increases pain on lateral epicondyle) or resist
wrist flexion (increases pain on ?)
Elbow Injuries
Athletic Medicine
Sprains
• Often happen with throwing sports (baseball,
javelin, fastpitch, etc.)
• Can occur with a person that held onto
someone as they ran passed them.
• Valgus and varus tests just like the knee
– Make sure that you test at 0 and 30.
Care
• 1st-rest, ice, possible bracing
• 2nd-refer. Check for avulsion fx, especially in
young people.
• 3rd-surgery to reattach ligament. “Tommy
John” surgery.
• Might need to clean up the area. Joint mice
• 45-degree angle- flex & extend wrist. Pain=
capsular problem/maybe ligament
6
1/19/2016
Olecranon bursitis
•
•
•
•
Lies between the skin and the olecranon process
S/S: pain, swelling, lack of ROM
Aspiration- (taking fluid out) may need to be done
Care: RICE. Must compress this ASAP
Epicondylitis
• Inflammation of muscular
attachments
• Extensors- lateral
– “tennis elbow”
• Flexors- medial
– “little league elbow/golfers
elbow”
• S/S: pain around
epicondyles with mild
swelling
• Care: IM, rest, antiinflammatory
Osteochondritis Dissecans
• Rare
• Poor/impaired blood supply
• Can leave a loose body in
the joint- loosens articular
cartilage & bone (joint
mice)
• Cause is unknown
• S/S: locking symptoms
when moving, clicking, pain
• Care: Refer for surgery
Ulnar Nerve
• Nerve
subluxes/dislocates
over the medial
epicondyle (trochlea)
• Care: Rest, ice (careful
to not freeze nerve),
anti-inflammatory,
referral for possible
nerve transposition
Cubital Tunnel
• Nerve entrapment in cubital space (anterior side of the
forearm)
• S/S: tingling, parasthesia to 4th & 5th digits from ulnar
nerve being trapped or dislocated
• Care: Refer. Can be problems from ulnar nerve
transposition
Dislocation
•
•
•
•
High incidence with falling on
outstretched hand or severe twist
while in flexion
Posterior is most common
Can injure major nerves/blood
vessels
Care: Splint, Refer
7
1/19/2016
Fractures
• Look for straight line
between condyles and
olecranon process on
extension and a triangle
in flexion
• If this is not seen
suspect a fx
• Care: Splint and refer
Volkmann’s contracture
• Fx above the condyles of
humerous
• Can cut off the brachial
artery
• S/S: pain in forearm when
fingers are passively
extended, no brachial or
radial pulse, muscle
contracture
• Care: Refer
Forearm injuries
• Blood supply is the
ulnar/radial artery
• Pulse should be taken
on the radial artery
• Muscles
– flexors/pronatorsanterior
– Extensors/supinatorsposterior
Hyperextension
Forearm splints
• Most commonly see in
gymnastics
• Results from fatigue &
poor conditioning
• Care: Rest, check
technique, ice, antiinflammatory, change
event
• MOI: FOOSH or blow to elbow
– Ligament sprain or muscle strain
– Bony compression of olecranon process
w/humerus
• Treatment
– PRICES
– ROM, strength of elbow flexors
– Tape
8
1/19/2016
History/ Mechanism
1. Chief Complaint
Hand, Wrist, Thumb Evaluation
Tell me about your problem
Athletic Medicine
History/ Mechanism
History/ Mechanism
2. History of Present Problem
3. Time Sequence
a. When did you first notice the symptoms?
b. Have you had any history of this problem or other related
problem areas?
c. Has anyone in your family had similar symptoms?
d. What activity were you engaged in at onset of symptoms?
e. Was there any change in activity recently? (running, diet,
sleep)
f. Did you hear or feel anything at time of onset?
g. Any specific mechanism (cause) you were aware of at the
time?
a.
b.
c.
d.
Was onset of symptoms sudden or gradual?
How long did symptoms last?
Have symptoms been constant or intermittent?
When do symptoms typically occur? (during activity,
after?)
History/ Mechanism
History/ Mechanism
4. Location of Symptoms
5. Symptom Characteristics
a. Point with one finger to area where symptoms most
severe.
b. Is there more than one area of symptoms?
a. Characterize the pain? (dull, sharp, throbbing,
burning, aching)
b. Does the pain radiate and where?
c. What relieves the pain?
d. What increases the pain?
e. How do symptoms affect your activity level?
9
1/19/2016
History/ Mechanism
History/ Mechanism
6. Participation Characteristics
7. Personal Management
a. What sport?
b. What position or event?
c. What are the frequency, duration and intensity of
your practice?
d. Could equipment be related to your symptoms? If
yes, what type, kind, vintage?
e. What type of playing environment?
f. What type of warm-up pattern?
a. Have you attempted any treatment?
b. Have you taken any medication?
c. Have you seen anyone else for the problem? If yes,
who and what was their impression?
d. Do you have any opinions of your own as to what is
your problem?
Observation
Palpation
1. Remove clothing bilaterally (use discretion)
2. Deformity
3. Bleeding
4. Scars
5. Discoloration
6. Coloration
7. Swelling
8. Compare bilaterally (compare to other side)
9. Observe body movement
10. Guarding
11. Carrying
10. Radius
11. Ulna
10
11
Palpation
Palpation
Carpal bones
1. Navicular
(scaphoid)
2. Lunate
3. Triquetrum
4. Pisiform
5. Trapezium
6. Trapazoid
7. Capitate
8. Hamate
5
6
7
8
4
1
2
3
8
6
7
3
1
5
2. Metacarpals (5)
3. Phalanges (14)
4. Joints
a. Metacarpalphalangeal (MCP)
b. Proximal Interphalangeal (PIP)
c. Distal Interphalangeal (DIP)
5. Radial styloid
6. Ulnar styloid
c
b
3
a
a
2
2
5
6
10
1/19/2016
Palpation
7.
Palpation
8. Ligaments
a. collaterals on all
interphalangeal joints
b. ulnar collateral- in web
of thumb
Anatomical snuff box
b
a. extensor pollicis longus
(ulnar side/top)
b. extensor pollicis brevis
(middle)
c. abductor pollicis longus
(radial side/bottom)
d. navicular/scaphoid is
floor of snuff box
a
a
a
a
c
b
b
a
c
Palpation
Thenar Muscles
9. Muscles
THENAR EMINENCE
• Abductor pollicis brevis
(most radial)
• Flexor pollicis brevis
• Opponens pollicis
a. thenar eminence
b. hypothenar
eminence
a
HYPOTHENAR EMINENCE
• Abductor digiti minimi
(most ulnar)
• Flexor digiti minimi
• Opponens digiti minimi
b
Palpation
c. Extensors
back of hand
d. Flexors palm
of hand
c
d
11
1/19/2016
Range of Motion
•Blood and Nerve Supply
• Three major nerves
– Ulnar, median and
radial
• Ulnar and radial
arteries supply the
hand
– Two arterial arches
(superficial and deep
palmar arches)
Figure 24-11
*Should test in active, passive, and
resistive motions and compare
bilaterally.
1. Wrist
a. flexion
b. extension
c. radial/ulnar deviation
d. pronation
e. Supination
f. raider nation
2. Fingers
a. metacarpalphalangeal joints
- flexion/extension
- abduction/adduction
b. interphalangeal joints
- flexion/extension
3. Thumb
a. carpalmetacarpal joint
-palmar abduction
-palmar adduction
-opposition
-flexion
-extension
b. metacarpalphalangeal joint
-flexion/extension
c. interphalangeal joint
-flexion/extension
© 2011 McGraw-Hill Higher Education. All
rights reserved.
Stress Tests
*Remember: Do not reduce fingers or thumb!
1.
2.
3.
4.
Pinch strength (OK sign)
Opposition pinch
Grasp strength
Carpal Tunnel Syndrome- compression of the median nerve
a. Tinel sign
b. Phalens test
5. Finkelstein’s test - irritation to the tendons (tenosynovitis) of the
anatomical snuff box.
6. Extend and abduct thumb (Ulnar collateral ligament)
7. Valgus/varus stress ( collateral ligaments of phalanges)
8. Twist test (for fx)
9. Tap test (for fx)
10. Lost MCP joint (FX)
• Special Tests
– Finklestein’s Test
•
•
•
•
•
Test for de Quervain’s syndrome
Athlete makes a fist w/ thumb tucked inside
Wrist is ulnarly deviated
Positive sign is pain indicating stenosising tenosynovitis
Pain over carpal tunnel could indicate carpal tunnel
syndrome
Figure 24-12
© 2011 McGraw-Hill Higher Education. All
rights reserved.
• Special Tests
– Tinel’s Sign
• Produced by tapping over transverse carpal
ligament
• Tingling, paresthesia over sensory distribution of
the median nerve indicates presence of carpal
tunnel syndrome
Figure 24-13
© 2011 McGraw-Hill Higher Education. All
rights reserved.
• Phalen’s Test
– Test for carpal tunnel
syndrome
– Position is held for
approximately one
minute
– If test is positive, pain
will be produced in
region of carpal tunnel
Figure 24-14
© 2011 McGraw-Hill Higher Education. All
rights reserved.
12
1/19/2016
– Valgus/Varus and Glide Stress Tests
• Tests used to assess ligamentous integrity of joints
in hands and fingers
• Valgus and varus tests are used to test collateral
ligaments
• Anterior and posterior glides are used to assess the
joint capsule
– Circulatory and Neurological Evaluation
• Hands should be felt for temperature
– Cold hands indicate decreased circulation
• Pinching fingernails can also help detect circulatory
problems (capillary refill)
• Allen’s test can also be used
– Patient is instructed to clench fist 3-4 times, holding it on
the final time
– Pressure applied to ulnar and radial arteries
– Patient then opens hand (palm should be blanched)
– One artery is released and should fill immediately (both
should be checked)
Figure 24-15
• Hand’s neurological functioning should also be
tested (sensation and motor functioning)
© 2011 McGraw-Hill Higher Education. All
rights reserved.
© 2011 McGraw-Hill Higher Education. All
rights reserved.
Hand, Wrist, Thumb Injuries
Wrist Injuries
Athletic Medicine
Sprains & Strains
• Hard to distinguish between the two
• Main support to the hand is posterior &
anterior ligaments
Carpal Tunnel Syndrome
Tunnel is located on the anterior aspect of the wrist
Made from the carpal bones & the transverse ligaments
Inflammation of tendons & synovial sheaths apply compression on median
nerve.
MOI: repeated wrist flexion or a blow
s/s: sensory/motor changes over the thumb & index fingers
Care: rest, anti-inflammatories
MOI:
• falling on a hyperextended wrist
• violent flexion
13
1/19/2016
DeQuervain’s Disease
Narrow tendon passage in
the thumb causing
tenosynovitis
MOI: constant wrist
flexion
s/s: pain radiating to the
forearm
Care: immobilization,
cryotherapy, rest
Fractures
Most common at heads of
radius/ulna, scaphoid, hamate
Scaphoid
• MOI: force on an outstretched
hand
• compression between radius &
second row of carpal bones
• recognized as a sprain
• necrosis may occur w/o proper
splinting
• s/s: swelling, pain in snuff box &
with radial deviation
Hamate
• MOI: gripping an object
Dislocations
Very rare
MOI: hyperextension at distal ends of radius/ulna (lunate, not a true
dislocation)
s/s: pain, swelling, difficulty w/ index finger flex, numbness in median
nerve
Care: acute
Colles’ Fx
• Occurs on the lower end of
the radius and or ulna
• Most commonly results
from a fall on an
outstretched hand that
drives the radius/ulna up &
back – hyperextension
• Secondly can result from
falling on the back of a
hand, driving it down and
foreword (silver fork
deformity)
Wrist Ganglion (Ganglion cyst)
Herniation of joint capsule,
synovial sheath or a cyst
Appears after a strain around
tendon points
Care:
• new
Hand, Thumb Injuries
– leave it alone and decrease
activity that will cause it
– surgically remove it, drain
fluids with syringe
• old
– drop book on it (bible bump)
14
1/19/2016
Contusions
Due to little padding
Subungual Hematoma
Bruising under the finger
nail
Trigger finger (thumb)
Tenosynovitis
Thickening of the flexor
tendons, can’t
straighten
Mallet Finger
• Torn (avulsed) extensor tendon
• Occurs at the DIP joint
• s/s: finger at 30 degree angle, bone chip
Sprains
“Jammed” fingers
Sprains to ligaments/ joint
capsule
Boutonniere Deformity
Torn (avulsed)
extensor tendon
Occurs at the PIP joint
Button sewers
thought it was great
15
1/19/2016
Gamekeepers Thumb
Dislocation
Tear of collateral ligament in thumb
Couldn’t hold chickens
Fractures
TFCC
• Triangular Fribrocartilage Complex Injury
– Problem with wrist sprains
– Piece of cartilage located between the ulna and
carpal bones
– MOI: Forceful rotation or hyperextension of wrist
– Tx: immobilization, rehab (ROM & strength),
surgery?
16