Document
advertisement

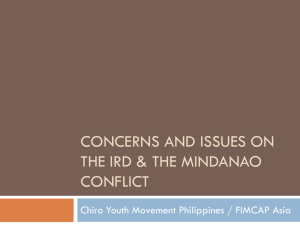
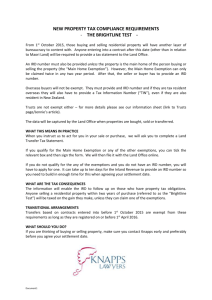
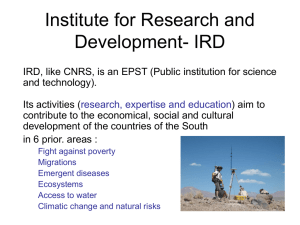
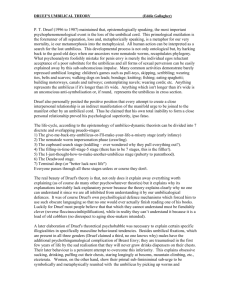
[ research report ] CYNTHIA M. CHIARELLO, PT, PhD1 • J. ADRIENNE MCAULEY, PT, DPT, OCS, FAAOMPT2 Concurrent Validity of Calipers and Ultrasound Imaging to Measure Interrecti Distance D iastasis rectus abdominis (DRA), the abnormal separation of the right and left rectus abdominis, appears as an increase in the width of the linea alba, or interrecti distance (IRD). The linea alba is a meshwork of connective tissue in which the tendinous insertions of the external oblique, internal oblique, and transversus abdominis muscles intermingle, providing structure and stability to the abdominal wall and TTSTUDY DESIGN: Clinical measurement, concurrent validity criterion standard. TTOBJECTIVE: To determine the concurrent validity of digital nylon calipers in comparison to ultrasound imaging (USI) for the measurement of interrecti distance (IRD). TTBACKGROUND: Diastasis rectus abdominis is the abnormal increase in the width of the linea alba, measured as IRD. A diastasis rectus abdominis can compromise mechanical trunk function in both genders. IRD has been accurately measured with USI but requires costly equipment and extensive examiner training. Digital nylon calipers are inexpensive and easy to use, but their use to measure IRD has not been validated. TTMETHODS: A sample of convenience of 56 individuals (11 men, 45 women) was measured. A single examiner was assigned to each tool (calipers or USI), and IRD was measured at 2 locations (above and below the umbilicus) under 2 conditions (abdominal muscles at rest and abdominal muscles contracted). All measurements were made during a single session, and examiners were blinded to measurements with the other tool. trunk.1 A DRA can indicate connective tissue alterations of the linea alba,35 an increase in muscle length with consequent altered line of muscle pull,14 damTTRESULTS: Above the umbilicus, the mea- surements of IRD with calipers were similar to those made with USI, with intraclass correlation coefficients (model 3,2) of 0.79 with abdominal muscles at rest and 0.71 with abdominal muscles contracted. The absolute mean difference between the caliper and USI measurements of IRD above the umbilicus was 0.03 cm larger with the calipers when the abdominal muscles were at rest and 0.03 cm smaller when the abdominal muscles were contracted. The values of IRD obtained with the caliper and USI techniques were not comparable when obtained below the umbilicus. TTCONCLUSION: The calipers are a valid tool for measuring IRD above the umbilicus in males and females. Measuring IRD with calipers below the umbilicus should not be considered valid, using USI as the criterion standard. This may reflect anatomical variation of the linea alba or a limitation of the calipers to assess IRD at the same depth as USI. J Orthop Sports Phys Ther 2013;43(7):495-503. Epub 30 April 2013. doi:10.2519/jospt.2013.4449 TTKEY WORDS: diastasis recti, linea alba, rectus abdominis age of the fixation of the rectus muscles in their sheaths,1 or a disruption of the entire musculofascial abdominal wall.8,13 The anisotropic, directionally dependent behavior of the linea alba,15 in conjunction with craniocaudal differences in the width and thickness of the linea alba, necessitates IRD measurements both above and below the umbilicus to document the DRA width.2 Compromising the mechanical function of the trunk, a DRA has been associated with decreased muscle strength and endurance,11,21 reduced capacity of abdominal musculature to stabilize the pelvis,2,14,32 related pelvic floor dysfunction,33,34 posture abnormalities,6 and lumbopelvic pain.29,33,37,38,42 Development of a DRA may be due to failure of the abdominal wall to withstand extreme overloading28 and may stem from different causes in males and females. In males, factors that appear to be related to DRA include increasing age,12,23,31 obesity,23 greater abdominal circumference,12 performance of full-excursion sit-ups and weight training,23 hernia,35 abdominal aortic aneurysm,24,26 and lipodystrophy in HIV-infected men.4 In addition to these same factors, in females abdominal wall stress frequently begins due to the uterus enlarging during pregnancy, with 27% of women exhibiting a DRA during their second trimester and 66% during the Program in Physical Therapy, Department of Rehabilitation and Regenerative Medicine, College of Physicians and Surgeons, Columbia University, New York, NY. 2Department of Physical Therapy, University of New England, Portland, ME. This study was approved by the Columbia University Medical Center Institutional Review Board. The authors certify that they have no affiliations with or financial involvement in any organization or entity with a direct financial interest in the subject matter or materials discussed in the article. Address correspondence to Dr Cynthia M. Chiarello, Columbia University, Program in Physical Therapy, 710 West 168th Street, 8th Floor, New York, NY 10032. E-mail: cmc3@ columbia.edu t Copyright ©2013 Journal of Orthopaedic & Sports Physical Therapy ® 1 journal of orthopaedic & sports physical therapy | volume 43 | number 7 | july 2013 | 495 43-07 Chiarello.indd 495 6/19/2013 1:01:06 PM [ ] research report TABLE 1 Participant Characteristics* Women Age, y Height, m Men (n = 11) Nulliparous (n = 22) Parous (n = 23) Total (n = 56) 37.5 9.8 (19.8-56.1) 28.5 6.0 (23.0-49.9) 39.6 9.8 (25.8-64.0) 34.8 9.8 (19.8-64.0) 1.80 0.09 (1.63-1.92) 1.63 0.06 (1.53-1.76) 1.62 0.06 (1.47-1.74) 1.67 0.10 (1.47-1.92) Mass, kg 97.2 13.7 (74.5-119.3) 62.2 11.7 (45.8-94.4) 59.5 6.7 (49.0-72.7) 67.9 17.8 (45.8-119.3) Body mass index, kg/m2 30.0 3.9 (23.7-33.9) 23.4 4.0 (17.2-34.1) 22.6 1.8 (20.1-27.8) 24.3 4.3 (17.2-34.1) *Values are mean SD (range). third.6 Although IRD decreases during the initial postpartum months, it does not completely resolve and typically remains significantly larger than IRD in nulliparous women.6,13,21 In postpartum women, Liaw et al21 found that abdominal muscle function and IRD improved at 6 months but were not restored to nulliparous values. At 12 months postpartum, Coldron et al13 reported that 48% of women had a significantly larger IRD than nulliparous controls. Ranney30 found that 39% of 1738 parous women undergoing a hysterectomy several years postpartum still exhibited a DRA. Other reported risk factors for DRA in women include multiparity, multiple gestation, older maternal age, large pregnancy weight gain, and larger babies.10,22 Although there is agreement that a DRA is abnormal, there is no consensus in the literature on the optimal IRD for all adults.3,27,31 Documentation of the size and location of a DRA is important in examining patients with any type of musculoskeletal trunk dysfunction to determine stability and load acceptance, the efficacy of exercise intervention programs, as well as the need for abdominoplasty.3,20 Typically, DRA is measured by placing palpating fingers between the medial borders of the right and left rectus abdominis muscles, parallel to the linea alba. DRA size is determined by indicating the number of fingers that fit between the 2 muscle bellies at locations above, below, and at the umbilicus while the individual performs a partial curl-up. Clinically, this palpation technique is easy to perform but has not demonstrated adequate reliability9 and validity.19 A modification of this palpation technique using nylon dial or digital calipers to measure the IRD has been shown to be reliable in pregnant and postpartum women.7,11,17 The validity of ultrasound imaging (USI) to measure IRD above the umbilicus has been established. Mendes et al25 found no statistically significant difference between supraumbilical measurements taken with USI and those directly measured during surgery for abdominoplasty. Good intrarater reliability of IRD measurements made with USI in females has also been demonstrated.21 Therefore, USI is an accurate3,13,21 and valid25 method of measuring IRD size and location; however, it requires expensive equipment and extensive examiner training and expertise.41 Given the importance of measuring IRD during an examination of abdominal function, an inexpensive, accessible, and easy-to-use tool is necessary. Digital nylon calipers meet the criteria of reliability and ease of use; however, to date, we have found no studies validating digital nylon calipers for measuring IRD. The primary purpose of this investigation was to determine the concurrent validity of digital nylon calipers in comparison to USI for the measurement of IRD. For calipers to be a clinically useful tool, they must be valid across gender, parity, and size of the IRD. A secondary purpose of the study was to describe the IRD seen in typical adult males and females. METHODS Participants A sample of convenience, consisting of an ethnically diverse group of 56 English-speaking individuals (11 men, 22 nulliparous women, 23 parous women) between 19 and 64 years of age (TABLE 1), was recruited from physical therapy private practices in New York City and the student populations at Columbia University and Touro College. The ethnicity of the sample was 66% Caucasian, 12% Asian, 9% Hispanic, 9% mixed, 2% African American, and 2% Middle Eastern. Participants were excluded if they were pregnant; had scarring from previous abdominal surgery such that, on observation of the abdomen, the linea alba or umbilicus was obscured or deformed; had rheumatological or connective tissue disease; or had any medical condition that would prohibit active abdominal muscle contraction. The study protocol was approved by the Columbia University Medical Center Institutional Review Board, and participants signed an informed-consent form following a detailed explanation of all study procedures. Instrumentation and Examiners Each tool was used by 1 examiner for all data collection, and each examiner was blinded to the measurements by the other examiner with the other tool. The measurements of IRD using the nylon digital calipers (Mitutoyo America Corporation, Aurora, IL) were made by 1 examiner, 496 | july 2013 | volume 43 | number 7 | journal of orthopaedic & sports physical therapy 43-07 Chiarello.indd 496 6/19/2013 1:01:07 PM TABLE 2 Intrarater, Within-Session Reliability Data for Interrecti Distance Measurements With Ultrasound Imaging and Calipers Ultrasound Imaging (n = 6) Measurement Condition and Location Calipers (n = 8) ICC3,1* SEM, cm MDD, cm ICC3,1* SEM, cm MDD, cm PAU 0.97 (0.95, 0.99) 0.005 0.015 0.99 (0.98, 0.99) 0.001 0.003 AAU 0.98 (0.92, 0.99) 0.012 0.032 0.98 (0.95, 0.99) 0.006 0.016 PBU 0.90 (0.89, 0.99) 0.017 0.048 0.97 (0.91, 0.99) 0.005 0.014 ABU 0.94 (0.93, 0.99) 0.009 0.024 0.94 (0.81, 0.99) 0.041 0.113 Abbreviations: AAU, activated abdominal muscles above umbilicus; ABU, activated abdominal muscles below umbilicus; ICC, intraclass correlation coefficient; MDD, minimal detectable difference; PAU, passive abdominal muscles above umbilicus; PBU, passive abdominal muscles below umbilicus; SEM, standard error of measurement. *Values in parentheses are 95% confidence interval. who had 10 years of experience with this tool. The USI measurements of IRD were performed using the LOGIQ Book XP ultrasound unit (GE Healthcare, Waukesha, WI), with a 5-MHz curvilinear transducer, by 1 examiner with advanced training and 7 years of clinical USI use. High intrarater reliability for measuring IRD for both USI and the calipers7,11 has been reported.21 To establish our own reliability, a separate study was performed, in which 8 subjects were measured with calipers and 6 subjects with USI. Three measurements for each location (above and below the umbilicus) and each condition (abdominal muscles at rest and contracted) were performed on the same day. Intrarater reliability for USI was assessed by measuring 3 separate images for each location and condition. In this preliminary work, intrarater reliability was found to be very high for each tool-examiner combination, with intraclass correlation coefficients (ICCs) ranging from 0.90 to 0.99. The minimal detectable difference (MDD) for each tool-examiner combination ranged from 0.003 to 0.113 cm (TABLE 2). Procedures IRD measurements using both tools were made during a single session. To ensure that both tools measured IRD at precisely the same location, the participant was positioned comfortably in supine and the desired measurement locations were marked with a water-soluble pen 4.5 cm above the umbilical midpoint and 4.5 cm below the umbilical midpoint. These specific locations along the linea alba have previously been used to measure IRD with 3-D photography.14 We also selected 4.5 cm above and below the umbilicus because measurements at these locations have previously been reported.6,11,12,29 No IRD measurements were made at the umbilicus due to technical difficulties with USI, which is consistent with other USI studies that have not reported measurements at the level of the umbilicus.3,13 Because the ultrasound gel can blur the water-soluble markings, making future measurements in the same location difficult, the caliper measurements always preceded the USI measurements. Previous investigations of DRA using USI have measured IRD with the abdominal muscles at rest,3,14 whereas previous studies using palpation7 and caliper techniques12 have reported IRD measurements in a hook-lying test position, with the subject actively performing a partial curl-up. In this study, we elected to perform the measurements with the abdominals both at rest and activated. For the caliper measurements with the abdominal muscles at rest, the participant was positioned in hook-lying, arms down by the side, with 1 pillow placed beneath the head. The examiner palpated the medial borders of the right and left rectus abdominis muscle bellies at the marked locations. The inside measurement jaws of FIGURE 1. To measure interrecti distance 4.5 cm above and below the umbilicus (indicated with skin markings), the inside jaws of the calipers are placed between the medial edges of the right and left rectus abdominis muscles as palpated by the examiner. the digital nylon calipers were positioned at the locations of the palpating fingers, perpendicular to the direction of the muscles, and adjusted to the perceived IRD width (FIGURE 1). The palpation and caliper measurement procedure was the same for both measurement locations, above and below the umbilicus. To measure the IRD with abdominal muscles contracted, each participant crossed the arms over the chest and raised the head until the spine of the scapulae was off the table surface. The participant maintained this partial curl-up while the examiner palpated and measured the IRD with the calipers, as described just above. Once the caliper measurements were completed, the participant remained in the same hook-lying position and the first examiner left the room. Upon entering the room, the second examiner placed the 5-MHz curvilinear journal of orthopaedic & sports physical therapy | volume 43 | number 7 | july 2013 | 497 43-07 Chiarello.indd 497 6/19/2013 1:01:08 PM [ research report TABLE 3 ] Descriptive Data for Interrecti Distance* Men (n = 11) Women: Nulliparous (n = 22) Women: Parous (n = 23) AAU 1.45 0.95 0.88 0.45 1.69 0.92 PAU 1.62 1.04 0.75 0.43 2.03 1.05 AAU 1.54 0.76 0.84 0.30 1.60 0.96 PAU 1.63 0.69 0.81 0.53 2.04 1.61 4.5 cm above umbilical midpoint Ultrasound imaging FIGURE 2. Placement of the ultrasound imaging transducer, perpendicular to the linea alba, to measure interrecti distance 4.5 cm above and below the umbilicus (indicated with skin markings). Calipers 4.5 cm below umbilical midpoint Ultrasound imaging 3.5 * 3.0 * IRD, cm 2.5 ABU 0.48 0.58 0.34 0.36 0.72 0.45 PBU 0.74 0.89 0.22 0.29 1.05 0.65 Calipers 2.0 ABU 1.39 0.37 1.18 0.33 1.63 1.04 1.5 PBU 1.68 0.54 1.69 0.68 2.36 1.43 1.0 0.5 0.0 PAU AAU USI PBU ABU Calipers FIGURE 3. Mean SD IRD measured with USI and digital nylon calipers 4.5 cm above and below the umbilicus, with abdominal muscles resting and contracted. *Statistically different between measurement tools (P<.0001). Abbreviations: AAU, activated abdominal muscles above umbilicus; ABU, activated abdominal muscles below umbilicus; IRD, interrecti distance; PAU, passive abdominal muscles above umbilicus; PBU, passive abdominal muscles below umbilicus; USI, ultrasound imaging. transducer perpendicular to the abdominal surface at each marked location along the linea alba (FIGURE 2). The onscreen image of the IRD was captured using a conventional grayscale brightness mode. The measuring feature of USI was used to measure the IRD by first capturing the image, followed by the examiner determining the location of the medial borders of the rectus abdominis muscles and using the onscreen cursor to mark the distance between the right and left muscle bellies. Participant position and instruction for the 2 conditions (with abdominal muscles at rest and with abdominal muscles contracted) were identical to those described for the caliper procedures. Abbreviations: AAU, activated abdominal muscles above umbilicus; ABU, activated abdominal muscles contracted below umbilicus; PAU, passive abdominal muscles above umbilicus; PBU, passive abdominal muscles below umbilicus. *Values are mean SD cm. Statistical Analysis Statistical analyses were performed in consultation with the Columbia University Center for Social Sciences and the Department of Biostatistics, using JMP 9.0 software (SAS Institute Inc, Cary, NC) and SPSS for Windows Version 18 (SPSS Inc, Chicago, IL). Descriptive statistics for participant characteristics and IRD at both locations and under both conditions were calculated. To determine if there was a significant difference in IRDs measured by the 2 tools, separate paired t tests were computed for each location and condition, with the statistical significance set at P<.05. To graphically examine the level of agreement between USI and caliper measurements of IRD, systematic bias, and random error, BlandAltman5 plots were constructed. We calculated the mean difference between tools and the 95% limits of agreement as 2 standard deviations of the mean differences.5 The concurrent validity of the digital nylon calipers as compared to USI was computed using ICC3,2 and standard errors of measurement, calculated as SD × 1 – ICC. MDD was calculated using a 95% confidence level (standard error of measurement × 1.96 × 2).40 ICC levels of agreement of IRD measurements were interpreted as follows: low, 0.0 to 0.5; moderate, 0.5 to 0.7; high, 0.7 to 0.9; and very high, greater than 0.9.16 For descriptive purposes and to ensure that the validity of measurements using calipers was generalizable to a greater population, the participants were divided post hoc into male, nulliparous female, and parous female subgroups. RESULTS Interrecti Distance T he mean IRDs for all subjects, as measured by both USI and calipers for each measurement condition and location, are depicted in FIGURE 3. Parous women exhibited the largest IRD above and below the umbilicus, both with and without an active abdominal muscle contraction. Nulliparous women exhibited the smallest IRD for all conditions and locations, except for the measurement with calipers below the umbilicus with the abdominal muscles at rest. Men 498 | july 2013 | volume 43 | number 7 | journal of orthopaedic & sports physical therapy 43-07 Chiarello.indd 498 6/19/2013 1:01:10 PM A B 4 AAU Difference, cm PAU Difference, cm 3 2 1 Mean = 0.03 cm 0 –1 3 2 1 Mean = –0.03 cm 0 –1 –2 –3 –2 0 1 2 3 4 5 0 1 2 Mean PAU 3 4 Mean AAU C D 4 4 2 ABU Difference, cm PBU Difference, cm 3 Mean = 1.43 cm 1 0 3 2 Mean = 0.74 cm 1 0 –1 –1 –2 0 1 2 3 4 0.0 0.5 Mean PBU 1.0 1.5 2.0 2.5 3.0 Mean ABU FIGURE 4. Bland-Altman plots of interrecti distance (cm), with difference in values between ultrasound imaging and caliper techniques on the y-axis and the average between ultrasound imaging and caliper values on the x-axis. Lines are mean differences and 95% limits of agreement. (A) PAU, (B) AAU, (C) PBU, (D) ABU. Abbreviations: AAU, activated abdominal muscles above umbilicus; ABU, activated abdominal muscles below umbilicus; PAU, passive abdominal muscles above umbilicus; PBU, passive abdominal muscles below umbilicus. TABLE 4 Level of Agreement Between Interrecti Distances Measured With Calipers and Ultrasound Imaging* Measurement Condition/Location ICC3,2 SEM, cm MDD95, cm PAU 0.79† (0.64, 0.88) 0.01 0.04 AAU 0.71† (0.51, 0.83) 0.17 0.48 PBU 0.40 (–0.02, 0.65) 0.52 1.45 ABU 0.43 (0.03, 0.67) 0.50 1.38 Abbreviations: AAU, activated abdominal muscles above umbilicus; ABU, activated abdominal muscles below umbilicus; ICC, intraclass correlation coefficient; MDD95, minimal detectable difference at the 95% confidence level; PAU, passive abdominal muscles above umbilicus; PBU, passive abdominal muscles below umbilicus; SEM, standard error of measurement. *Values in parentheses are 95% confidence interval. † P<.0001. exhibited the smallest IRD for the measurement with calipers below the umbilicus with the abdominal muscles at rest (TABLE 3). Validity The validity of the measurements made with the digital nylon calipers, as compared to those made with USI, was dif- ferent above and below the umbilicus. Above the umbilicus, there was no statistically significant difference (P>.05) in IRD values between the 2 tools under either the contracted or at-rest condition (FIGURE 3). As illustrated in the BlandAltman plots, for measurements made above the umbilicus, the majority of the data points fell within the limits of agreement (FIGURES 4A and 4B). On average, compared to the calipers, the IRD measured with USI was 0.03 cm larger with the abdominal muscles at rest and 0.03 cm smaller with the abdominal muscles contracted (FIGURE 4). Above the umbilicus, there was a high level of agreement between IRD measurements made with calipers and USI with the abdominal muscles at rest (ICC3,2 = 0.79, P<.0001) and contracted (ICC3,2 = 0.71, P<.0001) (TABLE 4). Below the umbilicus, IRD measurements using calipers were significantly larger (P<.0001) than those using USI for both abdominal muscles at rest and contracted (FIGURE 3). As indicated in the Bland-Altman plots, below the umbilicus, the mean difference in IRD between the tools was 1.43 cm with abdominal muscles at rest (FIGURE 4C) and 0.74 cm with abdominal muscles contracted (FIGURE 4D). Systematic bias was seen for measurements made below the umbilicus, as most points were located above the zero line, indicating that the calipers consistently overestimated IRD when compared to USI (FIGURES 4C and 4D). There was low agreement between the 2 measurement tools for IRD measured below the umbilicus under both the at-rest and contracted conditions of the abdominal muscles (TABLE 4). DISCUSSION T o our knowledge, this is the first study to examine the concurrent validity of measuring IRD with digital nylon calipers compared to the best available clinical tool, USI. Caliper measurements above the umbilicus were comparable to the USI measurements, journal of orthopaedic & sports physical therapy | volume 43 | number 7 | july 2013 | 499 43-07 Chiarello.indd 499 6/19/2013 1:01:11 PM [ research report FIGURE 5. Image and diagram showing the potential source of discrepancy between measurements of interrecti distance made with USI and the digital nylon calipers. As thickness of subcutaneous tissue increases, palpation of the inner edge of the RA is potentially made more difficult, leading to overestimation of the distance when using calipers. Abbreviations: RA, rectus abdominis; USI, ultrasound imaging. whereas below the umbilicus there was overestimation of the IRD size when measured with the calipers. We found good to excellent validity of measurements with the calipers when performed above the umbilicus, both with abdominal muscles at rest and contracted. The mean difference in IRD between methods was 0.03 cm, which is less than the MDD95 and not likely clinically significant. Although almost all data points were within the limits of agreement, a slightly higher measurement error was seen when IRD was measured with the abdominal muscles contracted compared to at rest (TABLE 4). This slightly greater difference between measurement techniques may be related to the variability of the intensity of muscle contraction during the measurements, as the 2 measures were done on separate trials. The high level of intrarater reliability demon- strated in this study for measurements above the umbilicus concurs with previously reported results for both the calipers7,11 and USI.21 Therefore, given these intrarater reliability and validity results, we are confident that calipers can be used as an accurate assessment of IRD for locations above the umbilicus. For IRD measurements below the umbilicus, the values obtained with the calipers were not similar to those obtained with USI (FIGURE 3, TABLE 4). Greater measurement error was also demonstrated with the abdominal muscles at rest, as a third of the points on the corresponding Bland-Altman plot were outside the limits of agreement (FIGURE 4C). Using the calipers, there may be a greater tendency to overestimate IRD for widths greater than 2.5 cm (FIGURE 4C). However, as only a few subjects exhibited such a large IRD, this requires further investigation. ] We initially thought that using calipers would lead to smaller IRD values than those obtained with USI, due to overlying skin and subcutaneous tissue. But the measurements made with the calipers were, on average, 1.43 cm greater than those made with USI with the abdominal muscles at rest (FIGURE 4C) and 0.74 cm greater with the abdominal muscles contracted (FIGURE 4D). These larger IRD measurements when using calipers may be due to the inaccurate identification of the medial edges of the right and left rectus abdominis muscles using manual palpation. It is possible that the USI and caliper measurements were not taken at equivalent depths. The measurement of IRD with USI is of the closest distance between the muscle bellies, regardless of depth from the skin. Below the umbilicus, there may be more subcutaneous tissue interfering with the examiner’s ability to detect the medial borders of the muscle by palpation. Consequently, the palpating fingers may be at a more superficial location and more lateral than the most medial aspect of the muscles (FIGURE 5). It is also possible that the caliper jaws produce a slight outward pressure against the muscle belly, thus increasing IRD—particularly if the tissue is more extensible, as is likely in those with greater IRD. This slight outward pressure may also explain why the caliper measurements were larger than the USI measurements when taken with the abdominal muscles at rest. Our results are in agreement with those by Mendes et al,25 who compared USI to direct surgical measurement and found excellent validity for measurements above the umbilicus and poor validity for those below the umbilicus. In women who had undergone a cesarean delivery, Mendes et al25 found a significantly larger IRD below the umbilicus at surgery than IRD measured with USI, which they attributed, in part, to a loss of definition of the posterior layer of the recti muscles and fibrosis, leading to difficulty in determining the medial rectus borders with USI. Gender differences in the architec- 500 | july 2013 | volume 43 | number 7 | journal of orthopaedic & sports physical therapy 43-07 Chiarello.indd 500 6/19/2013 1:01:12 PM ture2 and width1,12,31 of the linea alba in cadavers have been reported. The effect of gender on IRD has not yet been explored in living individuals. An increase in IRD postpartum compared to nulliparous women has been shown.6,12 To our knowledge, this is the first investigation to describe IRD with respect to both gender and parity. For the calipers to be clinically useful to detect a DRA, gender variation in the width of the linea alba must be considered. To facilitate comparison of our data to the few published reports on the typical IRD in adults, we chose to describe our sample by gender and parity. Modeling clinical practice, we measured IRD with the abdominal muscles under 2 conditions, at rest and contracted. To our knowledge, the only other investigation of IRD size that has included both males and females was conducted by Rath et al,31 with 60% of the 40 participants being males. However, Rath et al31 did not specifically report IRD values by gender or parity but, rather, reported a composite mean IRD of 8.3 mm midway between the umbilicus and xiphoid and 9.3 mm midway between the umbilicus and pubic symphysis, taking all measurements with the abdominal muscles at rest. The IRD values for men in our study appear similar to those reported by Rath et al31 for the location below the umbilicus, but not for the location above the umbilicus (TABLE 3). For the parous women in our study, in which 3 of the 23 participants were less than 1 year postpartum, IRD was more than double the values reported by Rath et al31 above the umbilicus and only slightly larger below the umbilicus (TABLE 3). This comparison should be made with respect to the present study’s sample of adults without disease, measured using USI, whereas the Rath et al31 study used computerized scans to measure individuals with intraabdominal disease. The IRD in women within their first postpartum year has been shown to exceed that which is considered normal in nulliparous women.13,21 The nulliparous women in this study exhibited IRD values comparable to those previously reported (TABLE 3).3,21 To identify the normal width of the linea alba in nulliparous females, Beer et al3 measured 150 women between 20 and 45 years of age. In the study by Beer et al,3 normal IRD was defined as any value between the 10th and 90th percentile, or greater than 22 mm at 3 cm above the cranial margin of the umbilicus and any value up to 16 mm at 2 cm below the caudal margin of the umbilicus. IRD measurements reported by Liaw et al21 at 2.5 cm above and below the umbilical ring in 20 nulliparous females also fell within the normal IRD range defined by Beer et al.3 The individuals in our study, and those in the study by Liaw et al,21 were within the same age range and were measured at a similar location along the linea alba.21 Coldron et al13 reported a larger IRD measurement with abdominal muscles at rest for 69 nulli­ parous females, using measurements immediately cranial to the umbilicus, where IRD is expected to be larger. Similar findings in our sample of nulliparous women give credence to the validity data for this group and provide further evidence that parity and location along the linea alba are important factors to consider when reporting IRD values. Boissonnault and Blaschak’s6 seminal research described the active curl-up assessment technique for a DRA, which is now used in common clinical practice. However, most subsequent investigations using objective measurement tools have just reported the IRD with the abdominal muscles at rest. 3,13,21,30,31 IRD measured with the abdominal muscles at rest with calipers has been shown to be more than twice the width of that measured during an active muscle contraction in women who were 11 weeks postpartum.7 In our study, to mimic clinical examination, participants were not instructed on a specific recruitment pattern or effort during the curl-up. While it was necessary to measure IRD during an active muscle contraction to validate the calipers as a clinical tool, this study was not designed to examine the variation of IRD at rest and during abdominal muscle contraction. Based on the results of this investigation and on our interpretation of the literature, we recommend that clinicians examine patients for the presence of a DRA when presenting with abdominal or lumbopelvic dysfunction. Keeler et al18 reported that 96.6% of women’s health clinicians used the finger-width technique for measuring a DRA. Finger palpation is not accurate and reliable.9 We recommend using USI when equipment and training are available. In the absence of USI, the easily obtainable and inexpensive calipers are a good alternative. Both of these tools are reliable for measuring IRD along the linea alba and lead to similar values for measurements made above the umbilicus. For measurements below the umbilicus, while recognizing that measurements made with the calipers will be greater than those made with USI, clinicians should not preclude the use of either tool at this time. To date, there is no universally agreedupon definition for DRA. It appears that measurement location, level of activation of the abdominal musculature, gender, parity, and measurement tool must be considered for the interpretation of IRD values. Future research should be designed to define DRA with respect to these variables. Limitations Measurement error may account for some of the inconsistency found below the umbilicus between the 2 tools. Measurement error might have occurred with either examiner. Though all efforts were made to minimize examiner error, our results represent not only the measurement tool but also the raters, and results may differ among raters. The results represent a first step in determining the validity of caliper measurement of IRD. Future studies should examine this technique with additional raters with varying amounts of clinical experience. Related to error among raters is journal of orthopaedic & sports physical therapy | volume 43 | number 7 | july 2013 | 501 43-07 Chiarello.indd 501 6/19/2013 1:01:14 PM [ sample size, and we recognize that a sample size of 20 or more is necessary to determine intrarater reliability for a novel tool.39 As the reliability of each tool has been previously reported in the literature,7,11,16,21 in our preliminary work we used a small but statistically appropriate sample size to determine our intrarater reliability. To accurately perform IRD measurement with calipers, the examiner must palpate the medial borders of both rectus abdominis muscles and place the calipers at the precise IRD locations palpated. The examiner perceives the edges of the muscle belly through subcutaneous tissue. If the individual has excessive subcutaneous tissue, adiposity, or a thick and rounded muscular configuration, it may be difficult to identify the actual medial extent of the muscle. When IRD is measured with USI, the examiner delineates a line between the most medial aspects of the muscle bellies, and the computer determines this exact distance. The subumbilical morphological variability previously described,1,2 along with these palpation issues, can explain how we achieved accurate measurements with each tool but how the measurements between the calipers and USI were only comparable above the umbilicus. In the design of this study, the USI examiner measured IRD without any palpation of the linea alba to most accurately represent USI. This does not represent clinical practice, and future studies may include palpation prior to transducer placement. When evaluating IRD with USI, examiner judgment, training, and consistent USI usage are vital to accurate assessment. The fascial sheaths of the rectus appear on the USI monitor as white, hyperechoic outlines, which demarcate the conical borders of the muscles against the darker, hypoechoic muscle bellies. The quality of this visual image can be affected by age and musculoskeletal dysfunctions such as atrophy, which produce a fatty fibrous muscle with diminished water content. Thus, the muscle appears whiter throughout or research report presents with greater echogenicity. 36 The participants in our study represented a range of ages and muscular development, some of which produced very poor images. In the participants with hard-todistinguish muscle edges, measurement error could have been introduced. Accurately placing the ultrasound transducer at measurement sites identical to those of the calipers was vital to ensure that IRD measurements were made by both tools in precisely the same locations. As the ultrasound gel removed skin markings, we chose to perform the caliper measurements first. Although randomized testing conditions are preferable, these would have necessitated re-marking the measurement location with the use of each tool, introducing an additional source of measurement error. ] to the calipers, especially for measurements made below the umbilicus. CAUTION: Interpretation of these results should consider that only 2 examiners, with extensive experience with these measurements, collected data for this study. ACKNOWLEDGEMENTS: The authors thank Dr David Madigan for his assistance in statistical analyses, and Drs Susan Ohlsen and Loretta Verma for assistance with data collection. We also acknowledge KIMA Center for Physiotherapy and Wellness for the use of space and equipment, as well as the support of Touro College in New York, NY, where Dr McAuley served as faculty during much of the time devoted to this project. CONCLUSION T his concurrent validity study comparing IRD measurements made with digital nylon calipers to those made with USI offers preliminary evidence to support the validity of using calipers in both males and females when measuring IRD above the umbilicus with the abdominal muscles both at rest and during contraction. Measurements with calipers, although reliable, were not comparable to those made with USI at a location 4.5 cm below the umbilicus, which may reflect anatomical variation of the linea alba or a limitation of the calipers to assess IRD at the same depth as USI. t KEY POINTS FINDINGS: Digital nylon calipers are a reli- able and valid tool for measuring IRD above the umbilicus. This is in contrast to measurements made below the umbilicus. IMPLICATIONS: The calipers are a readily available tool providing clinicians with an easy method to objectively and precisely document IRD when measured above the umbilicus. For research purposes, or when precise measurements of IRD are necessary, USI is still preferable REFERENCES 1. A xer H, von Keyserlingk DG, Prescher A. Collagen fibers in linea alba and rectus sheaths: I. General scheme and morphological aspects. J Surg Res. 2001;96:127-134. http://dx.doi. org/10.1006/jsre.2000.6070 2. Axer H, von Keyserlingk DG, Prescher A. Collagen fibers in linea alba and rectus sheaths: II. Variability and biomechanical aspects. J Surg Res. 2001;96:239-245. http://dx.doi. org/10.1006/jsre.2000.6071 3. Beer GM, Schuster A, Seifert B, Manestar M, Mihic-Probst D, Weber SA. The normal width of the linea alba in nulliparous women. Clin Anat. 2009;22:706-711. http://dx.doi.org/10.1002/ ca.20836 4. Blanchard PD. Diastasis recti abdominis in HIV-infected men with lipodystrophy. HIV Med. 2005;6:54-56. http://dx.doi. org/10.1111/j.1468-1293.2005.00264.x 5. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;327:307-310. 6. Boissonnault JS, Blaschak MJ. Incidence of diastasis recti abdominis during the childbearing year. Phys Ther. 1988;68:1082-1086. 7. Boxer S, Jones S. Intra-rater reliability of rectus abdominis diastasis measurement using dial calipers. Aust J Physiother. 1997;43:109-114. 8. Brauman D. Diastasis recti: clinical anatomy. Plast Reconstr Surg. 2008;122:15641569. http://dx.doi.org/10.1097/ PRS.0b013e3181882493 9. Bursch SG. Interrater reliability of diastasis recti abdominis measurement. Phys Ther. 1987;67:1077-1079. 502 | july 2013 | volume 43 | number 7 | journal of orthopaedic & sports physical therapy 43-07 Chiarello.indd 502 6/19/2013 1:01:15 PM 10. C andido G, Lo T, Janssen PA. Risk factors for diastasis of the recti abdominis. J Assoc Chartered Physiother Womens Health. 2005:49-54. 11. Chiarello CM, Falzone LA, McCaslin KE, Patel MN, Ulery KR. The effects of an exercise program on diastasis recti abdominis in pregnant women. J Womens Health Phys Ther. 2005;29:11-16. 12. Chiarello CM, Zellers JA, Sage-King FM. Predictors of inter-recti distance in cadavers. J Womens Health Phys Ther. 2012;36:125-130. http:// dx.doi.org/10.1097/JWH.0b013e318276f60e 13. Coldron Y, Stokes MJ, Newham DJ, Cook K. Postpartum characteristics of rectus abdominis on ultrasound imaging. Man Ther. 2008;13:112-121. http://dx.doi.org/10.1016/j.math.2006.10.001 14. Gilleard WL, Brown JM. Structure and function of the abdominal muscles in primigravid subjects during pregnancy and the immediate postbirth period. Phys Ther. 1996;76:750-762. 15. Gräβel D, Prescher A, Fitzek S, von Keyserlingk DG, Axer H. Anisotropy of human linea alba: a biomechanical study. J Surg Res. 2005;124:118125. http://dx.doi.org/10.1016/j.jss.2004.10.010 16. Hides JA, Miokovic T, Belavy DL, Stanton WR, Richardson CA. Ultrasound imaging assessment of abdominal muscle function during drawing-in of the abdominal wall: an intrarater reliability study. J Orthop Sports Phys Ther. 2007;37:480486. http://dx.doi.org/10.2519/jospt.2007.2416 17. Hsia M, Jones S. Natural resolution of rectus abdominis diastasis. Two single case studies. Aust J Physiother. 2000;46:301-307. 18. Keeler J, Albrecht M, Eberhardt L, Horn L, Donnelly C, Lowe D. Diastasis recti abdominis: a survey of women’s health specialists for current physical therapy clinical practice for postpartum women. J Womens Health Phys Ther. 2012;36:131-142. http://dx.doi.org/10.1097/ JWH.0b013e318276f35f 19. Kotarinos RK. Diastasis Recti: Clinical Assessment and Surgical Observation [thesis]. Evanston, IL: Northwestern University; 1989. 20. Lee DG, Lee LJ, McLaughlin L. Stability, continence and breathing: the role of fascia following pregnancy and delivery. J Bodyw Mov Ther. 2008;12:333-348. http://dx.doi.org/10.1016/j. jbmt.2008.05.003 21. Liaw LJ, Hsu MJ, Liao CF, Liu MF, Hsu AT. The relationships between inter-recti distance 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. measured by ultrasound imaging and abdominal muscle function in postpartum women: a 6-month follow-up study. J Orthop Sports Phys Ther. 2011;41:435-443. http://dx.doi. org/10.2519/jospt.2011.3507 Lo T, Candido G, Janssen P. Diastasis of the rectus abdominis in pregnancy: risk factors and treatment. Physiother Can. 1999;51:32-37. Lockwood T. Rectus muscle diastasis in males: primary indication for endoscopically assisted abdominoplasty. Plast Reconstr Surg. 1998;101:1685-1691; discussion 1692-1694. McPhail I. Abdominal aortic aneurysm and diastasis recti. Angiology. 2009;59:736-739. http:// dx.doi.org/10.1177/0003319708319940 Mendes Dde A, Nahas FX, Veiga DF, et al. Ultrasonography for measuring rectus abdominis muscles diastasis. Acta Cir Bras. 2007;22:182-186. http://dx.doi.org/10.1590/ S0102-86502007000300005 Moesbergen T, Law A, Roake J, Lewis DR. Diastasis recti and abdominal aortic aneurysm. Vascular. 2009;17:325-329. http://dx.doi. org/10.2310/6670.2009.00047 Nahas FX, Augusto SM, Ghelfond C. Should diastasis recti be corrected? Aesth Plast Surg. 1997;21:285-289. http://dx.doi.org/10.1007/ s002669900127 Palanivelu C, Rangarajan M, Jategaonkar PA, Amar V, Gokul KS, Srikanth B. Laparoscopic repair of diastasis recti using the ‘Venetian blinds’ technique of plication with prosthetic reinforcement: a retrospective study. Hernia. 2009;13:287-292. http://dx.doi.org/10.1007/ s10029-008-0464-z Parker MA, Millar LA, Dugan SA. Diastasis rectus abdominis and lumbo-pelvic pain and dysfunction – are they related? J Womens Health Phys Ther. 2009;33:15-22. Ranney B. Diastasis recti and umbilical hernia causes, recognition and repair. S D J Med. 1990;43:5-8. Rath AM, Attali P, Dumas JL, Goldlust D, Zhang J, Chevrel JP. The abdominal linea alba: an anatomo-radiologic and biomechanical study. Surg Radiol Anat. 1996;18:281-288. Richardson CA, Snijders CJ, Hides JA, Damen L, Pas MS, Storm J. The relation between the transversus abdominis muscles, sacroiliac joint 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. mechanics, and low back pain. Spine (Phila Pa 1976). 2002;27:399-405. Sheppard S. Part I: management of postpartum gross divarication recti. J Assoc Chartered Physiother Womens Health. 1996;79:22-24. Spitznagle TM, Leong FC, Van Dillen LR. Prevalence of diastasis recti abdominis in a urogynecological patient population. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18:321-328. http:// dx.doi.org/10.1007/s00192-006-0143-5 Szczesny W, Cerkaska K, Tretyn A, Dabrowiecki S. Etiology of inguinal hernia: ultrastructure of rectus sheath revisited. Hernia. 2006;10:266-271. http://dx.doi.org/10.1007/ s10029-006-0081-7 Teyhen DS, Gill NW, Whittaker JL, Henry SM, Hides JA, Hodges P. Rehabilitative ultrasound imaging of the abdominal muscles. J Orthop Sports Phys Ther. 2007;37:450-466. http:// dx.doi.org/10.2519/jospt.2007.2558 Toranto IR. The relief of low back pain with the WARP abdominoplasty: a preliminary report. Plast Reconstr Surg. 1990;85:545-555. Wade MD. Diastasis recti and low back pain. Orthop Phys Ther Pract. 2005;17:20-22. Walter SD, Eliasziw M, Donner A. Sample size and optimal designs for reliability studies. Stat Med. 1998;17:101-110. http://dx.doi.org/10.1002/ (SICI)1097-0258(19980115)17:1<101::AIDSIM727>3.0.CO;2-E Weir JP. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J Strength Cond Res. 2005;19:231-240. http://dx.doi.org/10.1519/15184.1 Whittaker JL, Stokes M. Ultrasound imaging and muscle function. J Orthop Sports Phys Ther. 2011;41:572-580. http://dx.doi.org/10.2519/ jospt.2011.3682 Whittaker JL, Warner MB, Stokes M. Comparison of the sonographic features of the abdominal wall muscles and connective tissues in individuals with and without lumbopelvic pain. J Orthop Sports Phys Ther. 2013;43:11-19. http://dx.doi. org/10.2519/jospt.2013.4450 @ MORE INFORMATION WWW.JOSPT.ORG DOWNLOAD PowerPoint Slides of JOSPT Figures & Tables JOSPT offers PowerPoint slides of figures and tables to accompany selected articles on the Journal’s website (www.jospt.org). These slides can be downloaded and saved and include the article title, authors, and full citation. With each article where this feature is available, click “View Slides” and then right click on the link and select “Save Target As”. journal of orthopaedic & sports physical therapy | volume 43 | number 7 | july 2013 | 503 43-07 Chiarello.indd 503 6/19/2013 1:01:16 PM