Normative Values for the Unipedal Stance Test with Eyes Open and
advertisement

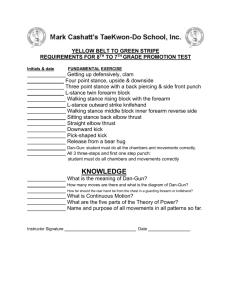
Normative Values for the Unipedal Stance Test with Eyes Open and Closed COL Barbara A. Springer, PT, PhD, OCS, SCS¹; COL Raul Marin, MD¹; Tamara Cyhan, RN, BSN¹; CPT Holly Roberts, MPT, GCS¹; MAJ Norman W. Gill, PT, DSc, OCS, FAAOMPT¹ ¹ Department of Orthopedics and Rehabilitation, Walter Reed Army Medical Center, Washington, DC ments that in whole or in part accounted for variation in length of stay and functional independence measure scores.1 Balance impairment is highly prevalent in patients with head injuries, peripheral neuropathy, or vestibular disorders.2-15 Tjon et al documented postural instability in patients with rheumatoid arthritis while others have shown that a relationship exists between age and sway, with sway increasing after age 40.16-20 Balance is not only affected in those with disease processes or trauma. Balance disturbances have also been documented in healthy senior citizens.21-24 Investigators have found a direct relationship between abnormal tests of balance and unexplained falls in older adults.24-26 For the main types of balance (static postural control, dynamic- anticipatory, and reactionary- postural control) there are numerous clinical tests to assess performance. The timed unipedal stance test (also referred to as timed single limb stance, unipedal balance test, one leg stance test, and one-leg standing balance) is a simple test for measuring static aspects of balance that can be used in a variety of settings and requires minimal equipment or training. Abnormal unipedal stance test (UPST) time with the eyes open is related to conditions such as peripheral neuropathy and intermittent claudication.9-11,27 Decreased eyes open UPST time is also associated with an increased risk for falls.8,21,22,24,26-30 Further, the UPST conducted with eyes closed may yield other valuable information. Since patients with medical conditions that impair balance may rely heavily on vision to maintain their balance, it is possible that these patients would be at an increased risk for falls in conditions where visual input is inaccurate or eliminated, such as nighttime ambulation. The UPST is described as a method of quantifying static balance ability.31 It is a valid measure32 and is useful in explaining other variables of importance such as frailty and self-sufficiency in activities of daily living,22,33 gait performance,34,35 and fall status.36 Jacobs et al recommended including the UPST with the eyes open in conjunction with several tests for patients with Parkinson disease in order to evaluate postural stability because it correlated with balance confidence and a history of falls.37 El-Kashlan et al recommended using the test as an outcome measure of static equilibrium for clinical trials of vestibular treatment.38 The UPST with the eyes open, but not closed, is also reliable for testing health-related fitness.39 Potvin and Tourtellotte recommended that UPST with the eyes closed be documented in conjunction with a battery of tests to evaluate motor function during the ‘clinical quantitative neurological examination,’ and Brinkman et al included the UPST with eyes open in their recommended battery of tests for balance assess- The views expressed in this article are those of the author and do not reflect the official policy of the Department of the Army, Department of Defense, or U.S. Government. This manuscript was produced without any sources of support. There are no competing interests. ABSTRACT Purpose: Limited normative data are available for the unipedal stance test (UPST), making it difficult for clinicians to use it confidently to detect subtle balance impairments. The purpose of this study was to generate normative values for repeated trials of the UPST with eyes opened and eyes closed across age groups and gender. Methods: This prospective, mixed-model design was set in a tertiary care medical center. Healthy subjects (n= 549), 18 years or older, performed the UPST with eyes open and closed. Mean and best of 3 UPST times for males and females of 6 age groups (18-39, 40-49, 5059, 60-69, 70-79, and 80+) were documented and inter-rater reliability was tested. Results: There was a significant age dependent decrease in UPST time during both conditions. Inter-rater reliability for the best of 3 trials was determined to be excellent with an intra-class correlation coefficient of 0.994 (95% confidence interval 0.989-0.996) for eyes open and 0.998 (95% confidence interval 0.996-0.999) for eyes closed. Conclusions: This study adds to the understanding of typical performance on the UPST. Performance is age-specific and not related to gender. Clinicians now have more extensive normative values to which individuals can be compared. Key Words: balance testing, single limb stance, normative, aging INTRODUCTION Balance impairments are a common finding among patients experiencing disease or trauma. Juneja et al reported that patients in acute inpatient rehabilitation who have experienced a stroke, head injury, non-orthopedic poly-trauma, or patients who are generally deconditioned had balance impairAddress all correspondence to: COL Barbara A. Springer, 2 Greenlane Court, Potomac, MD 20854, Ph: 202-782-6371, Fax: 202-782-3764 (Barbara.Springer@na.amedd.army.mil). Journal of Geriatric Physical Therapy Vol. 30;1:07 Study Design This study was a repeated measures, cross-sectional study. From June 2004 to December 2004, a poster advertisement describing the aims of the study was displayed in the waiting room of the PMR, PT, and OT clinics and in the lobby at our institution. The advertisement encouraged any healthy volunteer to contact the study research nurse who then explained the study in detail and obtained written informed consent which was approved by the Clinical Investigation and Human Use Committees of the Department of Clinical Investigation at Walter Reed Army Medical Center. The research nurse recorded each subject’s age, gender, race, height, weight, reason for being in the clinic, diagnosis (if any), level and location of pain (if any), limb chosen for UPST and ‘dominant limb’ on the data collection sheet. Before the UPST was performed, the subject was asked to kick a ball placed on the floor in front of him and the kicking limb was recorded as the ‘dominant’ limb. Up to 3 investigators performed the actual UPST testing and interrater reliability testing was performed by having 2 investigators test a subsample of 50 subjects. Both investigators used identical digital stopwatches and tested the same subject at the same time. An independent recorder annotated the time on their stopwatches. The third investigator began assisting with data collection after the first two had already finished with the interrater reliability testing. Eligible subjects were asked to stand barefoot on the limb of their choice, with the other limb raised so that the raised foot was near but not touching the ankle of their stance limb. Each subject was asked to focus on a spot on the wall at eye level in front of him, for the duration of the eyes open test. Prior to raising the limb, the subject was instructed to cross his arms over the chest. The investigator used a stopwatch to measure the amount of time the subject was able to stand on one limb. Time commenced when the subject raised the foot off the floor. Time ended when the subject either: (1) used his arms (ie, uncrossed arms), (2) used the raised foot (moved it toward or away from the standing limb or touched the floor), (3) moved the weight-bearing foot to maintain his balance (ie, rotated foot on the ground), (4) a maximum of 45 seconds had elapsed, or (5) opened eyes on eyes closed trials. The procedure was repeated 3 times and each time was recorded on the data collection sheet. The best and the average of the 3 trials were also recorded. Subjects performed 3 trials with the eyes open, and 3 trials with the eyes closed, alternating between the conditions. For example, 1 trial with eyes open followed by 1 trial with eyes closed equaled 1 trial set. The order of testing was randomized based on odd or even last digit in social security number. At least 5 minutes of rest were allowed between each trial set to avoid fatigue. Data collection sheets were summarized into the 8.0 release of SPSS for Windows (SPSS Inc., Chicago, Ill). ment in a routine neurological examination.40,41 Curb et al also recommended the ‘unassisted single-leg stand’ in a battery of tests to quickly assess global functional level, which adds to the validity of the measure and its usefulness in explaining other variables of importance.42 There are many other examples of how impaired UPST time is related to a variety of balance impairments. When combined with time to walk 1 meter and self-report of changed mobility status, the UPST can be used to identify preclinical disability in community-dwelling women and to screen higher-functioning populations for impairments.43 Vellas et al found that subjects who were unable to balance on one limb for 5 seconds had 2.1 times the risk of incurring an injurious fall as individuals who could balance for more than 5 seconds.36 Gehlsen and Whaley were able to distinguish between fallers and nonfallers using the UPST with eyes open and eyes closed in an elderly population.44 Also, the authors of 2 studies suggested that impaired UPST is a marker of frailty in elderly persons.22,33 Even though the UPST appears to be used often in clinical settings to test static balance for a variety of reasons, limited normative data for the eyes open and closed conditions have been established with which to compare the tested values.20,38,39,44-46 Some of the limitations of these studies include no reported age groups, the UPST not reported separately from a test battery, and small sample sizes.20,38,39,44-46 Limited normal values make it difficult for clinicians to use their measurements to detect subtle neurological or vestibular impairments. Further, establishing more extensive normative values by age group and gender would also offer clinicians and patients realistic goals to reach during a rehabilitation program. Therefore, the purpose of this study was to document normative values for the UPST with eyes open and closed in a large population by age and gender to serve as an acceptable reference standard. Our research hypothesis was that UPST would decrease as age increased. METHODS Subjects Volunteers were healthy military health care beneficiaries, ages 18 and older, recruited from among the staff members, patients, and patient family members who worked in or presented to the Physical Medicine and Rehabilitation (PMR), Physical Therapy (PT), and Occupational Therapy (OT) clinics located in a tertiary care United States military medical center. Data were collected during a 7-month period from a convenience sample of 567 consecutive volunteers. Subjects were excluded from participation if they had a known history of balance impairment (for any reason); peripheral neuropathy (clinically diagnosed or if they had symptoms of numbness/tingling in the lower extremities); orthopedic lower extremity or lumbosacral conditions requiring consultation with a health care professional (to include ligamentous injuries, osteoarthritis, or joint replacement); pain of any level presenting simultaneously in both lower extremities; or unilateral lower extremity pain >3 on the 11 point visual analog (box) scale. Pregnant women were also excluded. Journal of Geriatric Physical Therapy Vol. 30;1:07 Sample Size Estimation In a statistical analysis of methods to determine sample sizes for deriving reference values for an electrical diagnostic test, Chang et al concluded that the optimally efficient sample size is approximately 100 per group.47 For a sample size less than 100, the mean square errors were substantially increased. Based on this information, we aimed at a sample size of 30 to 50 subjects per gender per age group. Given that the study had 6 age groups (18-39 years, 40-49 years, 50-59 years, 60-69 years, 70-79 years, and 80-99 years), we aimed at a total sample size of up to 600 subjects. Statistics The best and mean of 3 trials were taken for each subject for the eyes open and eyes closed condition. Descriptive statistics were calculated for the best and mean UPST for both genders within all 6 age groups for both the eyes open and eyes closed condition. Common statistical criteria defined the reference range for normals as the mean ± 2 standard deviations. The best and mean UPST times were used for inferential statistical analysis. A 2 x 2 x 6 mixed model ANOVA with gender and age group as fixed factors and test condition (eyes open, eyes closed) as a repeated factor was calculated to identify a 3 factor interaction. Post-hoc 2 way ANOVAs were then calculated to analyze interactions present; 2 x 2 mixed model ANOVAs were calculated for gender versus testing condition, 2 x 6 mixed model ANOVAs were calculated for testing condition versus age group, and 2 x 6 fixed factor ANOVAs were calculated for gender versus age group. One way ANOVAs for each testing condition along with Tukey’s HSD were used to determine specific differences between age groups. Alpha was set at 0.05 and was appropriately corrected for multiple tests. Inter-rater reliability analysis was conducted using the intraclass correlation coefficient (ICC) and 95% confidence intervals. The ICC (2,1) was used for the best of 3 trials score and ICC (2,k) was used for the mean of 3 trials. The ICCs were calculated for both eyes open and eyes closed conditions. RESULTS A total of 567 participants consented to participate in the study. Of these, 18 were dropped from the sample because of the following reasons: 3 had pain > 3 on visual analog scale while standing on 1 limb, 4 had to leave prior to completion of testing, 1 had shoes on, 1 was too tired, 1 was younger than 18 years, and the remaining 8 belonged to an age group that had already filled its allocated quota. The final number of participants included in the analyses was 549 (female 258, 47%; male 291, 53%). The subcategories of participants were: 238 (43.4%) were patients, 135 (24.6%) were family members of patients, 39 (7.1%) were staff, 32 (5.8%) were soldiers, 27 (4.9%) saw the advertisement, and 78 (14.2%) were other. The ethnic mix of the study sample consisted of 339 (61.7%) Caucasians, 135 (24.6%) African American, 44 (8.0%) Hispanic, 18 (3.3%) Asian, and 13 (2.4%) were other. Mean height (SD) was 66.9 (6.3) inches and mean weight (SD) was 172.3 (43.7) pounds. Forty-three (7.8%) subjects reported pain in a lower extremity and 10 (1.8%) reported back pain. Level of pain for these areas (on a visual analogue pain scale of 0-10) ranged from 0-3 (mean 2.2, SD 0.90). Only 57.7% of the participants chose to stand on their right limb even though 89.4% were right limb dominant as demonstrated by the limb with which they kicked the ball. Table 1 provides the best and mean UPST times for females and males with eyes open and eyes closed for the 6 age groups as well as the values for females and males independent of age. Though a few cells show a skewed distribution due to a ceiling or floor effect, the data as a whole is normally distributed, therefore we proceeded with parametric analysis. For the inferential statistics, we report only the results of the best since that is how the test is used clinically. Further, we draw the same conclusions from the data whether the best or the mean of 3 trials is used. The 2 x 2 x 6 mixed model ANOVA showed a 3 way interaction of the factors (F=2.97, p=0.01). Post hoc 2 way ANOVAS (group vs. test, gender vs. test, and group vs. gender) revealed only one significant interaction (group vs. test; F=32.52, p < 0.001) which contributed to the overall significance of the 3 way ANOVA. However, Figure 1 shows the interaction to be an ordinal interaction. Therefore, appropriate interpretation of the main effects demonstrates a significant main effect for both test condition (F=1545.89, p < 0.001) and age group (F=109.31, p < 0.001). The 2 x 2 mixed model ANOVA (gender versus test condition) demonstrated no interaction (F=0.04, p = 0.84), a significant main effect for test condition (F=1393.70, p < 0.001), and no significant difference for gender (F=0.23, p=0.64). 2 x 6 fixed factor ANOVAs demonstrated no significant interactions (F=2.52, p=0.028 eyes open; F=1.47, p=0.119 eyes closed) at a corrected alpha of 0.025. There were significant main effects for age category (F=97.26, p < 0.001 for eyes open; F=31.57, p < 0.001 for eyes closed) and no significant main effects for gender (F=2.53, p=0.112 for eyes open, F=0.425, p=0.515 for eyes closed). One way ANOVAs for group differences demonstrated statistical significance for both eyes open (F=98.71, p < .001) and eyes closed (F=32.17, p < 0.001) and Tukey’s post-hoc comparisons revealed multiple group differences (Table 2). Inter-rater reliability testing on a subgroup of 50 participants demonstrated ICC=0.994 (95% confidence interval 0.989 to 0.996) for eyes open best of 3 trials, ICC=0.998 (95% confidence interval 0.996 to 0.999) for eyes closed best of 3 trials, ICC=0.951 (95% confidence interval 0.926 to 0.969) for eyes open mean of 3 trials, and ICC=0.832 (95% confidence interval 0.748 to 0.895) for eyes closed mean of 3 trials. DISCUSSION Our results confirm our hypothesis that there is a significant age dependent decrease in the ability to stand on 1 limb with both the eyes open and eyes closed UPST. In addition, the high inter-rater reliability supports the use of the UPST as a clinical screening tool and/or outcome measure for rehabilitation. Normative data are helpful in setting goals against a mean performance standard specifically representative of the patient. Additionally, a score that lies 1 to 2 standard deviations below the mean, in the context of the rest of the subjective or objective examination, may indicate a possible balance impairment that may require further clinical investigation with other confirmatory or complementary tests. We found that the difference in UPST times is not gender specific but is related to age, with the eyes open condition always resulting in significantly longer UPST times than eyes 10 Journal of Geriatric Physical Therapy Vol. 30;1:07 Table 1. Unipedal Stance Test Time by Age Group and Gender for Eyes Open and Closed Age & Gender Eyes Open Best of Eyes Open Mean Eyes Closed Best Groups 3 trials (sec) of 3 trials (sec) of 3 trials (sec) Mean (SE) Mean (SE) Mean (SE) Eyes Closed Mean of 3 trials (sec) Mean (SE) 18-39 Female (n = 44) Male (n = 54) Total (n = 98) 45.1 (0.1) 44.4 (4.1) 44.7 (3.1) 43.5 (3.8) 43.2 (6.0) 43.3 (5.1) 13.1 (12.3) 16.9 (13.9) 15.2 (13.3) 8.5 (9.1) 10.2 (9.6) 9.4 (9.4) 40-49 Female (n = 47) Male (n = 51) Total (n = 98) 42.1 (9.5) 41.6 (10.2) 41.9 (9.9) 40.4 (10.1) 40.1 (11.5) 40.3 (10.8) 13.5 (12.4) 12.0 (13.5) 12.7 (12.9) 7.4 (6.7) 7.3 (7.4) 7.3 (7.0) 50-59 Female (n = 50) Male (n = 48) Total (n = 98) 40.9 (10.0) 41.5 (10.5) 41.2 (10.2) 36.0 (12.8) 38.1 (12.4) 37.0 (12.6) 7.9 (8.0) 8.6 (8.8) 8.3 (8.4) 5.0 (5.6) 4.5 (3.8) 4.8 (4.8) 30.4 (16.4) 33.8 (16.0) 32.1 (16.2) 25.1 (16.5) 28.7 (16.7) 26.9 (16.6) 3.6 (2.3) 5.1 (6.8) 4.4 (5.1) 2.5 (1.5) 3.1 (2.7) 2.8 (2.2) 16.7 (15.0) 25.9 (18.1) 21.5 (17.3) 11.3 (11.2) 18.3 (15.3) 15.0 (13.9) 3.7 (6.2) 2.6 (1.7) 3.1 (4.5) 2.2 (2.1) 1.9 (0.9) 2.0 (1.6) 10.6 (13.2) 8.7 (12.6) 9.4 (12.8) 7.4 (10.7) 5.6 (8.4) 6.2 (9.3) 2.1 (1.1) 1.8 (0.9) 1.9 (1.0) 1.4 (0.6) 1.3 (0.6) 1.3 (0.6) 33.0 (16.8) 33.8 (17.1) 33.4 (16.9) 29.2 (17.4) 30.2 (17.7) 29.8 (17.5) 7.7 (9.6) 8.2 (10.8) 8.0 (10.3) 4.7 (6.0) 4.9 (6.4) 4.9 (6.2) 60-69 Female (n = 50) Male (n = 51) Total (n = 101) 70-79 Female (n = 45) Male (n = 50) Total (n = 95) 80-99 Female (n = 22) Male (n = 37) Total (n = 59) Total (all ages) Female (n=258) Male (n = 291) Total (n = 549) closed. This relationship between age and balance was also confirmed by Bohannon’s meta-analysis of single limb stance times with eyes opened.32 Our study helps establish typical performance values per respective age group for the eyes closed UPST and establishes more in-depth normative values for the eyes open UPST compared to previous studies.9,11,20,24,29 Our results are in general agreement with these investigators, however, the limited number of subjects in their reports limits their use as true normative values. Balance evaluation has importance as it pertains to safety of ambulation and transfers due to a direct relationship between balance test abnormalities and falls.24, 26 Furthermore, balance impairments have been shown to increase inpatient lengths of stay and predict poor rehabilitation outcomes.1, 2 Clinically, balance evaluations include tandem gait and Romberg testing, among others. In specialized centers, posturography is also used to test for balance impairment. However, the cost, size, and complexity of a posturography system make it impractical in some clinics, especially during a bedside evaluation. An alternative, the USPT, is not always used, yet it is an easy-to-perform clinical tool for the evaluation of static postural balance disorders. The unipedal stance allows for the evaluation of stance Figure 1. Best of three Trials Eyes Open vs. Eyes Closed Unipedal Stance Test Time (sec). Journal of Geriatric Physical Therapy Vol. 30;1:07 11 with the narrowest base of support and LaFont has positively correlated the duration of unipedal stance with posturography measured balance performance, which does measure dynamic postural control.21,38 It is important to note that the UPST does not measure the anticipatory postural control needed for selfinitiated limb movement or the reactionary postural control needed to maintain balance during unexpected perturbations or interference. The evaluation of balance with the UPST is a logical and functional approach, since transient balancing on a single limb is essential for normal gait and is critical for activities of daily living such as turning, stair climbing, and dressing. Our study further validates and expands upon previously established UPST normative values.9,11,20,24,29 In 1975, Potvin made the unsubstantiated claim that young healthy adults should be able to balance on 1 limb with eyes closed for 30 seconds and this arbitrary value does not take into consideration the effect of aging in balance.40 In a study evaluating the relationship between the UPST and aging, Bohannon obtained normative values for each decade from 20 to 79 years of age for the eyes open and eyes closed conditions.20 In the third and fourth decade, subjects were able to maintain the UPST for an average of 28 to 29 seconds for both conditions. However, from 40 to 60 years of age, the eyes closed condition showed a decrease as compared to the eyes open condition. The eyes open condition began to decrease at age 60, and a disproportionately larger decrease occurred in the eyes closed condition. In our study, Figure 1 clearly shows that UPST time decreases in both conditions, with the eyes open condition dramatically starting to decrease by the 7th decade. This is similar to Bohannon et al’s findings for the eyes open condition.20 However, the current study differs from Bohannon and colleagues as it pertains to the eyes closed condition, where our results show a fairly steady decrease in UPST time occurred across the different age groups. The difference between the current findings and those of Bohannon et al is underscored by their conclusion that the data were insufficient to classify the results as true normative values.20 Their conclusions can be explained by the fact that (1) the authors did not randomize the testing sequence of the eyes open and closed conditions, (2) they did not account for the possible effect of lower extremity muscle fatigue after 5 trials of eyes closed testing, (3) they did not account for possible substitution efforts in maintaining balance with arm movements during testing (we required patients to keep arms crossed over their chests during testing), and (4) they stopped UPST testing after 30 seconds.20 In our study, we followed the methods and rationale of Hurvitz et al by using a 45 second UPST time limit to allow for less ceiling effect and a more normal distribution of times.11 The age of the subjects in Bohannon et al’s study reached 79 where as in the current study it was 99.20 Another advantage of our study over previous work was our very large sample size–over twice as many subjects as in the Bohannon et al study.20 The current findings further define the normative values of the eyes open and eyes closed conditions of the UPST and demonstrate a significant age dependent decrease in the abil ity to stand on 1 limb with both the eyes open and eyes closed UPST. There are possible explanations for the age dependent decrease in UPST times. Jonsson et al identified 2 distinct postural phases that are necessary to perform single leg stance.48 During the dynamic phase, there was a rapid decrease of force variability amplitude as the subjects made postural adjustments to regain standing balance after transferring weight to one leg. The change in force amplitude occurred within the first 5 seconds of testing. During the second phase, static postural equilibrium was required to maintain balance on one foot, and the force variability was minimal. They concluded that elderly subjects had difficulty maintaining balance in the static phase due to difficulty adjusting postural control during the initial dynamic phase of one-leg stance. Another possibility for the decrease in stance times for elderly subjects is a decrease in lower extremity muscular strength and endurance. Although we did not test muscular strength or endurance in our subjects, there is a positive relationship between hip flexor, extensor, and abductor strength, and UPST times.46 Another measure of postural stability during single leg stance that may contribute to decreased unipedal stance time with increasing age is the assessment of time to boundary of the center of pressure excursion, which is the estimated time it would take for the center of pressure to reach the boundary of the base of support. Although several investigators have examined time to boundary measurements in double leg stance,49-51 only preliminary data have been assessed for single leg stance.52 However, time-to-boundary measures decrease with age during double leg stance, indicating decreased postural stability, and may also decrease during single leg stance.49,51 Although our study provides useful findings, the following limitations should be examined with further research. First, although we had 59 participants in the 80 to 99 years of age group, we did not reach our target sample size for this group. Second, we did not allow our subjects to use their arms to assist in maintaining balance. Elevating the arms changes the center of mass, which can aid in postural control. However, our testing protocol did allow for common movement strategies in postural sway, such the ankle sway synergy (postural adjustments are made at the ankle joint), hip sway synergy (postural adjustments are made primarily at the hip), and the suspensory synergy (flexion at the hip, knee, and ankle to lower the center of gravity toward the base of support).53 Third, we did not ask information about the level of activity or fitness, which may be an additional factor contributing to differences in performance among groups, especially if the younger groups were relatively more fit. Future research may also be helpful to examine the UPST in a subsample of subjects with known balance impairment. Also, because the UPST tests static postural control and the ability to transfer from a large base of support to a small base of support, further research should examine the relationship between the eyes closed UPST and posturography, as well as whether the UPST with the eyes open and closed is a useful test when performed in conjunction with tests that measure dynamic postural control such as the Functional Reach Test, Performance 12 Journal of Geriatric Physical Therapy Vol. 30;1:07 Table 2. Significant Differences in Unipedal Stance Test Times (sec) for Different Age Groups for Eyes Open and Closed Conditions (Best of 3 Trials) Age Groups Eyes Condition Significantly Different Mean (SE) Difference p-value (A) Age Groups (B) in seconds (A-B) 18-39 40-49 50-59 Open 60-69 70-79 80-99 12.6 (1.8) 23.2 (1.8) 35.3 (2.1) < 0.001 < 0.001 < 0.001 Closed 50-59 60-69 70-79 80-99 6.9 (1.3) 10.8 (1.3) 12.0 (1.3) 13.3 (1.5) < 0.001 < 0.001 < 0.001 < 0.001 Open 60-69 70-79 80-99 9.7 (1.8) 20.4 (1.8) 32.5 (2.1) < 0.001 < 0.001 < 0.001 Closed 50-59 60-69 70-79 80-99 60-69 70-79 80-99 4.5 (1.3) 8.4 (1.3) 9.6 (1.3) 10.8 (1.5) 9.1 (1.8) 19.7 (1.8) 31.8 (2.1) 0.008 < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 60-69 70-79 80-99 70-79 80-99 80-99 3.9 (1.3) 5.1 (1.3) 6.3 (1.5) 10.6 (1.8) 22.7 (2.0) 12.1 (2.1) 0.030 0.001 < 0.001 < 0.001 < 0.001 < 0.001 Open Closed 60-69 Open 70-79 Open 3.Lehmann J, Boswell S, Price R, et al. Quantitative evaluation of sway as an indicator of functional balance in post-traumatic brain injury. Arch Phys Med Rehabil. 1990;71:955-962. 4.Newton R. Balance abilities in individuals with moderate and severe traumatic brain injury. Brain Inj. 1995;9:455451. 5.Rubin A, Woolley S, Dailey V, Goebel J. Postural stability following mild head or whiplash injuries [see comments]. Am J Otol. 1995;16:216-221. 6.Geurts A, Ribbers G, Knoop J, van Limbeek J. Identification of static and dynamic postural instability following traumatic brain injury. Arch Phys Med Rehabil. 1996;77:639-644. 7.Mizrahi J, Groswasser Z, Susak Z, Reider-Groswasser I. Standing posture of craniocerebral injured patients: Bilateral reactive force patterns. Clin Phys Physiol Meas. 1998;10:25-37. 8.Richardson J, Ching C, Hurvitz E. The relationship between electromyographically documented peripheral neuropathy and falls. J Am Geriatr Soc. 1992;40:1008-1012. 9.Ashton-Miller J, Yeh M, Richardson J, Galloway T. A cane reduces loss of balance in patients with peripheral neuropathy: Results from a challenging unipedal balance test. Arch Phys Med Rehabil. 1996;77:446-452. 10.Richardson J, Ashton-Miller J. Peripheral neuropathy: An often-overlooked cause of falls in the elderly. Postgrad Med. 1996;99:161-172. Oriented Mobility Assessment, Timed Up and Go, or Dynamic Gait Index.48,54,55 Future research should also include examination of differences in stance times between preferred and nonpreferred extremities. SUMMARY The performance values established in this study help make the unipedal stance test (eyes open and eyes closed) a reliable, readily available and easy to perform ‘bed side’ examination tool for balance testing. These typical performance values across a variable sample will aid clinicians in understanding the age specific level of performance that is to be expected in healthy individuals during UPST evaluation. ACKNOWLEDGMENT The authors thank Tiffany Nesfield for her assistance with data collection. The first author had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. REFERENCES 1.Juneja G, Czyrny J, Linn R. Admission balance and outcomes of patients admitted for acute inpatient rehabilitation. Am J Phys Med Rehabil. 1998;77:388-393. 2.Black K, Zafonte R, Millis S. Sitting balance following brain injury: Does it predict outcome? Brain Inj. 2000;14:141-152. Journal of Geriatric Physical Therapy Vol. 30;1:07 13 29.Richardson J, Ashton-Miller J, Lee SG, Jacobs K. Moderate peripheral neuropathy impairs weight transfer and unipedal balance in the elderly. Arch Phys Med Rehabil. 1996;77:1152-1156. 30.Hill K, Schwarz J, Flicker L, Carroll S. Falls among healthy, community-dwelling, older women: a prospective study of frequency, circumstances, consequences and prediction accuracy. Aust NZ J Public Health. 1999;23:41-48. 31.Newton R. Review of tests of standing balance abilities. Brain Inj. 1989;3:335-343. 32.Bohannon R. Single limb stance times. A descriptive meta-analysis of data from individuals at least 60 years of age. Topics in Geriatric Rehabil. 2006;22:70-77. 33.Drusini A, Eleazer G, Caiazzo M, et al. One-leg standing balance and functional status in an elderly communitydwelling population in Northeast Italy. Aging Clin Exp Res. 2002;14:42-46. 34.Kinugasa T, Nagasaki H, Furuna T, Itoh H. Physical performance measures for characterizing high functioning older persons. J Aging Phys Activ. 1996;4:338-348. 35.Ringsberg K, Gardsell P, Johnell O, Jonsson B, Obrant K, Sernbo I. Balance and gait performance in an urban and a rural population. J Am Geriatr Soc. 1998;46(65-70). 36.Vellas B, Wayne S, Romero L, Baumgartner R, Rubenstein L, Garry P. One-leg balance is an important predictor of injurious falls in older persons. J Am Geriatr Soc. 1997;45:735-738. 37.Jacobs J, Horak F, Tran V, Nutt J. Multiple balance tests improve the assessment of postural stability in subjects with Parkinson’s disease. J Neurosurg Psychiatry. 2006;77:322-326. 38.El-Kashlan H, Shepard N, Asher A, Smith-Wheelock M, Telian S. Evaluation of clinical measures of equilibrium. Laryngoscope. 1998;108:311-319. 39.Suni J, Oja P, Laukkanen R, et al. Heath-related fitness test battery for adults: Aspects of reliability. Arch Phys Med Rehabil. 1996;77:399-405. 40.Potvin A, Tourtellotte W. The neurological examination: Advancements in its quantification. Arch Phys Med Rehabil. 1975;56:425-437. 41.Brinkman D, Kuipers-Upmeijer J, Oosterhuis H. Quantification and evaluation of 5 neurological equilibrium tests in test subjects and patients. Ned Tijdschr Geneeskd. 1996;140:2176-2180. 42.Curb J, Ceria-Ulep C, Rodriguez B, et al. Performancebased measures of physical function for high-function populations. J Am Geriatr Soc. 2006;54:737-742. 43.Chaves P, Garrett E, Fried L. Predicting the risk of mobility difficulty in older women with screening nomograms. Arch Intern Med. 2000;160:2525-2533. 44.Gehlsen G, Whaley M. Falls in the elderly: part II, balance strength, and flexibility. Arch Phys Med Rehabil. 1990;71:739-741. 45.Bulbulian R, Hargan M. The effect of activity history and current activity on static and dynamic postural balance in older adults. Physiol Behav. 2000;70:319-325. 11.Hurvitz E, Richardson J, Werner R. Unipedal stance testing in the assessment of peripheral neuropathy. Arch Phys Med Rehabil. 2001;82:198-204. 12.Black F, Shurpert C, Horak F, Nashner L. Abnormal postural control associated with peripheral vestibular disorders. Progress Brain Res. 1988;76:263-275. 13.Black F, Nashner L. Postural disturbance in patients with benign paroxysmal peripheral nystagmus. Ann Oto Rhino Laryn. 1984;93:595-599. 14.Horak F, Jones-Rycewicz C, Black O, Shumway-Cook A. Effects of vestibular rehabilitation on dizziness and imbalance. Otolaryngol Head Neck Surg. 1992;106:175-180. 15.Blatt P, Herdman S, Georgakakis G, Clendaniel R, Tusa R. The effect of the canalith repositioning maneuver on resolving postural instability in patients with benign paroxysmal peripheral vertigo. Am J Otol. 2000;21:356-363. 16.Tjon A Hen S, Van’t Pad Bosch P, Laan R, Mulder T. Postural control in rheumatoid arthritis patients scheduled for total knee arthroscopy. Arch Phys Med Rehabil. 2000;81:14891493. 17.Sheldon J. The effect of age on the control of sway. Gerontology Clinics. 1963;5:129-138. 18.Brocklehurst J, James-Groom F. Clinical correlates of sway in old age--Sensory modalities. Age Aging. 1982;11:1-10. 19.Thyssen H, Jansen B. Normal ranges in reproducibility of quantitative Rhomberg’s test. Acta Neurol Scand. 1982;66:100104. 20.Bohannon R, Larkin P, Cook A, Gear J, Singer J. Decrease in timed balance test scores with aging. Phys Ther. 1984;64:10671070. 21.Lafont C, Costes-Salon M, Dupui P, Nourhashemi F, Vellas B, Albarede J. The timed “up & go” test is a useful predictor of falls in community dwelling older people (Letter to the editor). JAS. 1998;46:928-929. 22.Vellas B, Rubenstein L, Ousset P, et al. One-leg standing balance and functional status in a population of 512 community-living elderly persons. Aging. 1997;9:95-98. 23.Vellas B, Wayne S, Romero L, Baumgartner R, Rubenstein L, Garry P. One-leg balance is an important predictor of injurious falls in older persons [see comments]. J Am Geriatr Soc. 1997;45:735-738. 24.Hurvitz E, Richardson J, Werner R, Ruhl A, Dixon M. Unipedal stance testing as an indicator of falls risk among older outpatients. Arch Phys Med Rehabil. 2000;81:587-591. 25.Bulbulian R, Hargan M. The effect of activity history and current activity on static and dynamic postural balance in older adults [In process citation]. Physiol Behav. 2000;70:319-325. 26.Studenski S, Duncan P, Chandler J. Postural responses and effector factors in persons with unexplained falls: Results and methodologic issues. J Am Geriatr Soc. 1991;39:229-234. 27.Gardner A, Montgomery P. Impaired balance and higher prevalence of falls in subjects with intermittent claudication. J Gerontol A Biol Sci Med Sci. 2001;56(7):M454-458. 28.Richardson J, Hurvitz E. Peripheral neuropathy: A true risk factor for falls. J Gerontol A Biol Sci Med Sci. 1995;50:M211215. 14 Journal of Geriatric Physical Therapy Vol. 30;1:07 51.Van Wegen E, Van Emmerik R, Riccio G. Postural orientation: age-related changes in variability and time-to-boundary. Hum Mov Sci. 2002;21:61-84. 52.Hertel J, Olmsted-Kramer L, Challis J. Time-to-boundary measures of postural control during single leg quiet standing. Hum Mov Sci. 2006;22:67-73. 53.Carr J, Shepherd R. Neurological Rehabilitation: Optimizing Motor Performance. Oxford: Butterworth Heinemann; 1998. 54.Pai Y, Rogers M, Hedman L, Hanke T. Alterations in weighttransfer capabilities in adults with hemiparesis. Phys Ther. 1994;74:647-657. 55.Rogers M, Pai Y. Dynamic transitions in stance support accompanying leg flexion movements in man. Exp Brain Res. 1990;81:398-402. 46.Iverson B, Gossman M, Shaddeau S, Turner M. Balance performance, force production, and activity levels in noninstitutionalized men 60-90 years of age. Phys Ther. 1990;70:348-355. 47.Chang A, Dillingham T, TYu K. Statistical methods of computing reference values for side-to-side differences in nerve conduction studies. Am J Phys Med Rehabil. 1996;75:437442. 48.Jonsson E, Seiger A, Hirschfeld H. One-leg stance in healthy young and elderly adults: a measure of postural steadiness? Clin Biomech. 2004;19:688-694. 49.Slovounov S, Moss S, Slovounova E, Newell K. Aging and time to instability in posture. J Gerontol A Biol Sci Med Sci. 1998;53:B71-78. 50.Van Emmerik R, Van Wegen E. On the functional aspects of variability in postural control. Exer Sport Sci Rev. 2002;30:177183. CALL FOR NOMINATIONS FOR SECTION ON GERIATRICS AWARDS DEADLINE: NOVEMBER 1 AWARDS RESEARCH AWARDS Clinical Educator Award This award recognizes a physical therapist or physical therapist assistant for outstanding work as a clinical educator in the geriatric health care setting. Adopt-A-Doc Award The purpose of the Section on Geriatrics Adopt-A-Doc program is to provide support to doctoral students interested in pursuing faculty positions in physical therapy education. Clinical Excellence In Geriatrics Award This award recognizes a physical therapist for outstanding clinical practice in geriatric health care settings. Any current member of the Section on Geriatrics may nominate a physical therapist who meets the award criteria. Excellence in Geriatric Research Award The individual nominated must be a physical therapist who has been the author (or co-author) of a paper dealing with clinical geriatric physical therapy research. This paper must have been published in a recognized journal (eg, Physical Therapy, Journal of American Geriatric Society, etc.) November 2002 and May 2004. Distinguished Educator Award The intent of this award is to recognize a Section on Geriatrics member for excellence in teaching. Fellowship for Geriatric Research This Fellowship is intended to provide partial financial support to physical therapists pursuing research in geriatrics. The research may be conducted as part of either a formal post-entry level academic program or a mentorship with an established investigator. The Fellowship applicant must be a physical therapist who is a current member of the Section on Geriatrics. Joan Mills Award This award, established in 1980 in honor of the Section on Geriatrics’ first President, Joan M. Mills, is presented to a member who has given outstanding service to the Section. Lynn Phillippi Advocacy for Older Adults Award This award recognizes projects or programs in clinical practice, educational, or administrative settings which provide strong models of effective advocacy for older adults by challenging and changing ageism. A member of the Section on Geriatrics must nominate individuals or organizations whose advocacy for older adults meets the intent and criteria of the award. Student Research Award This award is intended to facilitate interest in geriatric research among entry-level physical therapy students. The award recognizes outstanding research-related activity completed by entry-level physical therapy students. A member of the Section on Geriatrics must nominate the entry-level student. The nominator will submit a letter of support which addresses the extent of the student’s involvement in the research process (during a period not to exceed more than 2 years of graduation from an entry-level program). Outstanding Physical Therapist Assistant Award This award recognizes a physical therapist assistant who has significantly impacted physical therapy care in geriatric practice settings. To be eligible for this award, the nominee must be an advocate for older adults, a current member of the Section on Geriatrics, have been involved in clinical practice in geriatric settings for a minimum of 5 years, and demonstrate exemplary care and innovative teamwork in meeting the physical therapy needs of older adults. THE DEADLINE FOR ALL AWARDS NOMINATIONS IS NOVEMBER 1, 2007. We ask that all submissions be electronic. For additional information on the criteria and selection process for section awards, please visit the Section on Geriatrics web site at www.geriatricspt.org or contact the office by email at geriatrics@apta.org or by phone at 800/999-2782 ext 3238. Volunteers in Action Community Service Award The intent of this award is to highlight the significant contributions in prevention and/or intervention for elders in typically underserved populations. This may include, but is not limited to work with elders who are homeless, who are homebound, live in very rural areas, live in poverty, or those of ethnic groups facing significant cultural barriers to necessary health care. Journal of Geriatric Physical Therapy Vol. 30;1:07 Also from the Section on Geriatrics Consumer Brochure Contest for students. Submissions due December 20, 2007. *Students do not have to be APTA members. 15