Accidental Carotid Artery Catheterization During Attempted Central
advertisement

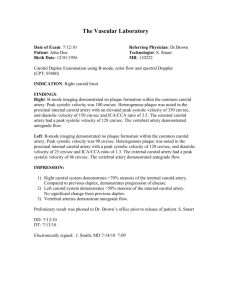
Accidental Carotid Artery Catheterization During Attempted Central Venous Catheter Placement: A Case Report Pauline Marie Maietta, CRNA, MS More than 2.1 million central venous catheters are placed annually. While carotid artery cannulation is rare, its effects can be devastating. Anesthesia providers frequently work with central venous catheters in the perioperative setting. Therefore, it is imperative that they be able to identify and react appropriately to carotid artery injury both in preexisting central lines and those that they have placed. This case report details a case of accidental carotid artery catheterization during attempted right internal jugular vein catheterization and the steps taken to treat the patient following its recognition. A discus- A nesthesia professionals commonly work with and place central venous catheters (CVCs). Although carotid artery cannulation is a rare complication associated with central line placement, its occurrence can be devastating to the patient. It is therefore important for anesthesia providers to appropriately identify and manage complications associated with an improperly placed catheter and to be knowledgeable of tools and techniques that can help prevent future carotid artery catheterizations. CVCs are commonly placed for: central venous pressure monitoring; infusion of fluids, medication, and nutrition; aspiration of air emboli; insertion of transcutaneous pacing leads; insertion of pulmonary artery catheters; and temporary hemodialysis (Table 1). The right internal jugular (RIJ) vein has been the preferred site for central venous access1,2 since the central landmark technique was first described in 1969.3 This site is often chosen over other central line insertion sites because of its readily identifiable landmarks, short direct route to the junction of the superior vena cava and right atrium, distance from the thoracic duct, and its ease of access for the anesthesia provider.1 Although CVCs placed in the internal jugular vein are associated with a high success rate, catheterization of the internal jugular vein is also associated with various techniquerelated complications.4 Complications of internal jugular cannulation include infection, embolism, dysrhythmia, hematoma, pneumothorax, cardiac perforation, cardiac tamponade, trauma to nearby nerves or arteries, thrombosis, and fistula formation (Table 2).5,6 According to www.aana.com/aanajournalonline sion of technique for central venous catheterization, indications for suspicion of arterial puncture, methods for confirming venous or arterial placement, appropriate methods for management of carotid artery cannulation, and the benefit of ultrasound in central venous cannulation follow. Through the appropriate use of equipment, early detection and management of carotid artery injury, and proper training, patient outcomes may be improved. Keywords: Carotid artery catheterization, central venous catheter, complication, ultrasound. Tom Richardson, Northeast regional district representative of CVC manufacturer, Arrow International, Boston, Massachusetts, via a phone conversation, more than 2.1 million CVCs are placed annually. While carotid artery complications are 1 of the 3 most common complications associated with central venous catheterization,7 cannulation of the carotid artery by a large bore catheter is less frequent, occurring in 0.1% to 0.5% of cases.8 Case Summary A 77-year-old male presented to the emergency department (ED) following progressive shortness of breath for several days and chest pain upon exertion. His medical history included diabetes mellitus, coronary artery disease, atrial fibrillation, chronic obstructive pulmonary disease, and chronic bronchitis. He had an 80 pack year smoking history and had been receiving 2.5 L of oxygen via nasal cannula at home for 6 months before presentaVenous access in patients with poor or no previous access Rapid fluid resuscitation (as in hypovolemia or shock) Monitoring of central venous pressure and or pulmonary artery catheterization for comprehensive cardiac monitoring Infusion of caustic drugs, vasoactive drugs, or total parenteral nutrition Temporary hemodialysis access Aspiration of air emboli in the event of venous air embolism Insertion of transcutaneous pacing leads Table 1. Indications for Central Venous Catheterization1,4-6,8 AANA Journal August 2012 Vol. 80, No. 4 251 tion to the ED. The patient’s presenting data included the following: height, 172.7 cm; weight, 68.2 kg; temperature, 98.2°F; heart rate, 102/min; blood pressure, 214/98 mm Hg; and peripheral oxygen saturation (SpO2), 93% following the administration of non-rebreather mask. Laboratory test results revealed: bicarbonate, 37 mmol/L; blood urea nitrogen, 28 mg/dL; blood glucose, 199 mg/dL; white blood cell count, 23.7 K/µL; and troponin levels, 0.09 ng/mL (> 0.03 ng/mL considered significant by hospital laboratory). The patient’s electrocardiogram was consistent with his history of atrial fibrillation and did not show changes in the ST waveform. In the ED, the patient’s arterial blood gas revealed: pH, 7.23; PaCO2, 111 mm Hg; PaO2, 77 mm Hg; HCO3-, 47 mEq/L; and SaO2, 93%. Bilateral crackles were noted upon auscultation of the patient’s lungs. He was diagnosed with acute respiratory failure secondary to chronic obstructive bronchitis with acute exacerbation and Pseudomonas pneumonia along with subendocardial infarction. One hour after admission to the ED, the patient was intubated for respiratory distress and administered continuous fentanyl and midazolam infusions for sedation. A large-bore5,6 7-French triple lumen catheter insertion was then attempted aseptically by the ED team via the RIJ under ultrasound guidance per the hospital sepsis protocol. Vital signs just prior to catheter placement were: heart rate, 98/min; blood pressure, 83/52 mm Hg, SpCO2, 100%. Difficulty with fluid infusion 1 hour after placement of the CVC prompted the ED team to transduce the central line. A pulsatile arterial waveform was noted, and arterial placement confirmed via PaCO2 of 429 mm Hg. At this time, a chest x-ray was also obtained and suggestive of catheter entrance into the innominate artery. Consults were obtained from the vascular and anesthesia services. The catheter was not removed manually because there was a high risk of adverse side effects associated with catheter removal, and surgical intervention was planned. Preoperatively the patient was assigned ASA class 4E. A plan including risks, benefits, and alternatives was discussed with the patient’s son who understood and consented to anesthesia for the procedure. The patient arrived in the operating room intubated and receiving 100% oxygen via manual ventilation. His sedative infusions were continued throughout the case. He was transferred safely to the operating room table where he was placed in the supine position by anesthesia for surgery on his RIJ and carotid artery. Standard monitors were applied with the addition of a cerebral oximeter. Initial cerebral oximetry values were obtained and maintained within normal limits throughout the procedure. Correct endotracheal tube position was confirmed via auscultation and end-tidal CO2. Sevoflurane was administered and ventilation was controlled via mechanical ventilation. An arterial line was placed and transduced before induction, which allowed for baseline activated 252 AANA Journal August 2012 Vol. 80, No. 4 Infection Air or thrombus embolism Dysrhythmia Hematomaa Pneumothorax, hemothorax, hydrothorax Cardiac perforation Cardiac tamponade Trauma to nearby nerves or arteriesa Thrombosis Fistula formation (possibly arteriovenous)a Table 2. Complications Associated with Central Line Placement in the Internal Jugular Vein5,6 a Concerns that were considered for this case. clotting time of 146 seconds and arterial blood gas values: pH, 7.38; PaCO2, 65 mm Hg; PaO2, 208 mm Hg to be established. No heparin was used during the case and no further blood specimens were necessary during the procedure. Vital signs were maintained within normal limits throughout the case with no additional pharmaceutical interventions necessary. Over the course of the surgery, the vascular team found that the catheter had entered the lateral wall of the RIJ, punctured the medial wall of the RIJ where it exited the vein, entered the right common carotid artery, and catheterized the carotid artery in a caudad direction (Figures 1 and 2). Both the RIJ and right common carotid artery were repaired by the vascular team, and the surgery was completed in less than 1 hour. Postoperatively the patient remained intubated because of his underlying respiratory status. He was transferred to the intensive care unit where he was extubated on postoperative day 1 and discharged on postoperative day 9 with no further complications. Discussion Anesthesia providers are frequently responsible for the insertion and use of CVCs in the operating room setting. Identification and management of complications associated with central line placement are an essential component of safe anesthesia practice. A brief discussion addressing the risk of carotid artery cannulation during CVC insertion in the RIJ, detection and management of carotid artery cannulation, and the use of ultrasound in the prevention of carotid artery cannulation follows. • Risk for Arterial Cannulation. The RIJ is typically the preferred site for central venous catheterization via the central landmark technique. However, this technique may not identify the middle 80% of the RIJ’s venous lumen in up to 34% of patients even with correct positioning of the patient and needle at the insertion site.9 When this occurs, the risk of carotid artery catheterization or injury is increased because of the proximity of the artery and vein. The central landmark technique is www.aana.com/aanajournalonline Figure 2. Surgical Dissection of Neck Figure 1. Surgical Dissection of Suspected Carotid Artery Catheterization also more likely to intersect the carotid artery in obese patients.9 In addition, excessive rotation or extension of the head greater than 40° may increase the likelihood of carotid artery puncture by altering cervical vascular anatomy causing the RIJ to overlie the carotid artery.10 • Detecting Cannulation. If pulsatile or high-pressure backflow occurs from the needle or catheter placed during attempted RIJ cannulation, carotid artery puncture should be suspected. Methods for confirming carotid artery puncture include comparison of blood color with an arterial sample, comparison of PaO2 from the suspected catheter with an arterial sample, transduction of the catheter and assessment for a pulsatile waveform, use of manometry, chest x-ray, use of transesophageal echocardiogram, and visualization (as with surgery) (Table 3). However, certain criteria used for determining whether carotid injury has occurred are not always accurate. Techniques such as blood color comparison and catheter transduction may produce incorrect results depending on the patient’s oxygenation status, fluid volume status, and blood pressure.8 • Management of Arterial Cannulation. Two techniques are commonly employed for the management of carotid artery cannulation with a large bore catheter (ie, 7 French or greater).5,6 These techniques consist of removal of the catheter and application of direct pressure, or surgical exploration, repair, and catheter removal. Results of large bore catheter removal and external pressure application are varied.6 Guilbert et al reported serious complications in up to 47% of patients treated by removal of the catheter and application of direct pressure, which included death in several cases. No complications from surgery or catheter misplacement were reported in those patients treated via surgical repair in the same study.5 Negative patient outcomes associated with carotid artery cannulation include stroke, www.aana.com/aanajournalonline Image displays central venous catheter exiting the medial wall of the right internal jugular and entering the common carotid artery. Abbreviations: CVC, central venous catheter; IJV, internal jugular vein. airway obstruction, hematoma, additional surgery for arterial repair, hemothorax, pseudoaneurysm, arteriovenous fistula, and death.5,7 Therefore, it is prudent to treat suspected carotid artery catheterization with immediate examination of neurological function where applicable, followed by surgical exploration, and repair of the artery to prevent negative patient outcomes. Prevention of Arterial Cannulation Several factors mitigate carotid artery injury. Insertion of a catheter by a practitioner who has placed 50 or more central lines is 50% less likely to cause a mechanical complication than an insertion by a practitioner who has not.4 Thus, practitioner experience inversely correlates with the likelihood of carotid injury. In addition, literature supports the use of real time/dynamic ultrasound guidance over the central landmark technique for cannulation of the RIJ to decrease the risk of injury (Table 4).2,11 In this method, the needle and catheter are observed at all points from insertion through placement. Ultrasound guided central venous cannulation has been endorsed by several major healthcare agencies12,13 because it can lead to improved outcomes when used appropriately. It allows providers to differentiate between venous and arterial anatomy through its ability to display arterial pulsatility, venous compressibility, and venous engorgement (as with Trendelenburg positioning). Realtime ultrasound views decrease thrombotic, infectious, and mechanical complications (eg, carotid artery trauma) associated with central venous cannulation.2 However, formal training on a standardized method of real time ultrasound use for central venous catheterization is lacking in medical education,11 as is research on the best methods for approaching central venous catheterization with ultrasound (eg, short axis vs long axis approach).14 AANA Journal August 2012 Vol. 80, No. 4 253 Reliability Method Compare blood color from suspected catheter/needle with an arterial sample.a Low Transduce the catheter and check for a pulsatile waveform congruent with arterial placementb Use of manometryc Moderate Chest x-ray confirmation Compare PaO2 from suspected catheter/needle with an arterial sample. High Use of transesophageal echocardiogram Surgical visualizationd Table 3. Methods for Confirming Suspected Carotid Artery Catheterization and/or Puncture4,6,8 a Venous blood should be darker than arterial blood. b Blood pressure dependent. c Procedure in which a piece of extension tubing is attached to the angiocatheter before wire placement to determine artery puncture by ascension/descension of blood in the tubing. d As depicted in Figure 2. The use of ultrasound guidance in CVC placement may also be limited despite promotion of its use by literature and government agencies; 67% of those surveyed by the Society of Cardiovascular Anesthesiologists report that they do not use, or rarely use, ultrasound guidance when placing CVCs.15 Increased education of nursing and medical students on the use of ultrasound for central venous cannulation could potentially increase ultrasound use by anesthesia providers and lead to improved patient outcomes. 1969 English describes the central landmark technique for internal jugular catheterization. 1978 Ullman and Stoelting describe the use of Doppler technology for detecting the internal jugular vein. 1984 Legler describes the use of Doppler ultrasound for cannulation of the internal jugular vein. 1993 Denys shows use of ultrasound may reduce risk of carotid artery puncture 1.7% (ultrasound) vs 8.3% (landmark technique). 1998 Voluntary verification process made available to surgical fellows in a statement by the American College of Surgeons to ensure they are qualified to use ultrasound and maintain quality standards. 2001 Agency for Healthcare Research and Quality (US Department of Health and Human Services) endorses the use of real-time (dynamic) ultrasound in central venous catheterization. 2007 Survey by the Society of Cardiovascular Anesthesiologists reports that despite recommendation and literature supporting the use of ultrasound in central venous pressure placement, it remains limited (with 67% of respondents reporting that they never, or almost never, use ultrasound). Conclusion Although carotid artery cannulation is a rare complication of central venous catheterization, its effects can be devastating. Therefore, it is important for anesthesia providers to be familiar with the risks involved with central venous catheterization; to have had formal training and in-servicing on tools available to prevent said risks; to be readily able to identify complications associated with CVCs; and to be prepared to manage such complications. Evidence-based policies enacted by hospitals can also help practitioners follow best practice methods for central line placement and management of complications resulting from central line placement. In addition, simple measures such as transducing CVCs and manometry may aid in the early detection of improperly placed central lines. Combining these measures with advances in central venous catheterization through the use of ultrasound technology decreases the incidence of complications associated with CVCs.1,7,15 When hospitals merge these measures to create a cohesive protocol for CVC insertion, confirmation of placement, identification of error, rapid neurological assessments, and appropriate treatment via surgical intervention, time to treatment may be decreased limiting complications associated with carotid artery injury and improving patient outcomes. 254 AANA Journal August 2012 Vol. 80, No. 4 Table 4. Chronology of Ultrasound Use2,11,12,15-19 REFERENCES 1. Ayoub C, Lavallée C, Denault A. Ultrasound guidance for internal jugular vein cannulation: Continuing Professional Development. Can J Anaesth. 2010;57(5):500-514. 2. Peris A, Zagli G, Bonizzoli M, et al. Implantation of 3951 longterm central venous catheters: performances, risk analysis, and patient comfort after ultrasound-guidance introduction. Anesth Analg. 2010;111(5):1194-1201. 3. English IC, Frew RM, Pigott JF, Zaki M. Percutaneous catheterisation of the internal jugular vein. 1969. Anaesthesia. 1995;50(12): 1071-1076. 4. McGee DC, Gould MK. Preventing complications of central venous catheterization. N Engl J Med. 2003;348(12):1123-1133. 5. Guilbert MC, Elkouri S, Bracco D, et al. Arterial trauma during central venous catheter insertion: case series, review and proposed algorithm. J Vasc Surg. 2008;48(4):918-925; discussion 925. www.aana.com/aanajournalonline 6. Shah PM, Babu SC, Goyal A, Mateo RB, Madden RE. Arterial misplacement of large-caliber cannulas during jugular vein catheterization: case for surgical management. J Am Coll Surg. 2004;198(6):939-944. 7. Domino KB, Bowdle TA, Posner KL, Spitellie PH, Lee LA, Cheney FW. Injuries and liability related to central vascular catheters: a closed claims analysis. Anesthesiology. 2004;100(6):1411-1418. 8. Ezaru CS, Mangione MP, Oravitz TM, Ibinson JW, Bjerke RJ. Eliminating arterial injury during central venous catheterization using manometry. Anesth Analg. 2009;109(1):130-134. 9. Bailey PL, Whitaker EE, Palmer LS, Glance LG. The accuracy of the central landmark used for central venous catheterization of the internal jugular vein. Anesth Analg. 2006;102(5):1327-1332. 10. Sulek CA, Gravenstein N, Blackshear RH, Weiss L. Head rotation during internal jugular vein cannulation and the risk of carotid artery puncture. Anesth Analg. 1996;82(1):125-128. 11. Thompson C, Barrows T. Carotid arterial cannulation: removing the risk with ultrasound? Can J Anaesth. 2009;56(6):471-472. 12. AHRQ issues critical analysis of patient safety practices. Qual Lett Healthc Lead. 2001;13(8):8-12, 1. 13. National Institute for Clinical Excellence. Guidance on the use of ultrasound locating devices for placing central venous catheters. Technology Appraisal Guidance No. 49. September, 2002:1-21. 14. Blaivas M, Adhikari S. An unseen danger: frequency of posterior vessel wall penetration by needles during attempts to place internal jugular vein central catheters using ultrasound guidance. Crit Care Med. 2009;37(8):2345-2349; quiz 2359. 15. Bailey PL, Glance LG, Eaton MP, Parshall B, McIntosh S. A survey of the use of ultrasound during central venous catheterization. Anesth Analg. 2007;104(3):491-497. www.aana.com/aanajournalonline 16. Ullman JI, Stoelting RK. Internal jugular vein location with the ultrasound Doppler blood flow detector. Anesth Analg. 1978;57(1):118. 17. Legler D, Nugent M. Doppler localization of the internal jugular vein facilitates central venous cannulation. Anesthesiology. 1984;60(5): 481-482. 18. Denys BG, Uretsky BF, Reddy PS. Ultrasound-assisted cannulation of the internal jugular vein. A prospective comparison to the external landmark-guided technique. Circulation. 1993;87(5):1557-1562. 19. American College of Surgeons. Ultrasound examinations by surgeons. Bull Am Coll Surg. June 1998;83(6). http://www.facs.org/fellows_info/ statements/st-31.html. Accessed April 17, 2012. AUTHOR Pauline Marie Maietta, CRNA, MS, is a staff nurse anesthetist at New York Presbyterian/Weill Cornell Medical Center, New York, New York. She was a student at Columbia University, School of Nursing Program in Nurse Anesthesia, New York, New York, and completing clinical rotations at Englewood Hospital, Englewood, New Jersey, during the writing of this article. Email: pmm2127@columbia.edu. ACKNOWLEDGMENTS I thank the administration of Columbia University, School of Nursing Program in Nurse Anesthesia, and I especially thank William Enlow, CRNA, DNP, for his support and guidance in the preparation of this article. I also thank Seth Perelman, MD, of Englewood Hospital, for allowing me to participate in this case and encouraging me to research its implications; Eleanor Dunn, RN, Englewood Hospital, for taking the beautiful photographs associated with this case; and my family and friends for their support throughout my education and writing of this article. AANA Journal August 2012 Vol. 80, No. 4 255