Stress, Coping, and Family Health
advertisement

;Il,' l:J2-1 lICt-1'1dbts:>cfJ
k- of
C'fDI' 1"'If I Q..H ...l
GHAPfER
Sf> ~
I
lie o.L .{~
12
Stress, Coping, and
Family Health
Rosanna DeMarco, Marilyn Ford-Gilboe,
Marie-Luise Friedemann, Hamilton I. McCubbin,
and Marilyn A. McCubbin
he ways in which people cope is
the most significant mediating
that families have on the healthpotential of
future generations.(p. 80)
factor in determining consequences of life stress on their health (Bomar,
1996). To date, much of the stress,coping, and
health research has focused on the individual
as the unit of analysis. Rarely, however, does a
person manage life's demands on his or her
own. Individuals also belong to a family, and it
is within this context that they deal with dayto-day life stressors. Of necessity, what the individual does or feels can affect the whole
family unit, just as the family unit is an imp ortant influence on individual behavior. Pender
(1996) wrote,
..>Health ~alues,atti~des, and behaviorsare
learned In the family context.The place of
health in the family value structureand the
extent to which health-promoting knowledge and [coping] skills are transmittedto
offspring determine the degree of impact
Helping families to learn to cope successfully
with the stressors that they face in their dayto-day lives is a formidable task as family
practitioners examine the many perspectives
and interpretations of family stress, coping,
and health. In this chapter, theoretical models
of family stress, coping, and health are detailed and critiqued. Conceptual definitions
are presented, issues of measurement and
logical and empirical adequacy are reviewed,
and the contributions of respective research
findings to nursing knowledge are evaluated.
TRADITIONAL
FRAMEWORKS
OF FAMILY STRESS COPING
"
AND HEALTH
Interest in family stress and coping originated
within the social sciences. Formal theorizing
295
296 ~
INTERACTIONAL AND TRANSACTIONAL MODELS
can be traced to Reubin Hill's (1949, 1958)
classic ABCX modelof family stress.On the
basis of researchconducted with families
who had experiencedseparationduring war,
Hill proposedthree interrelated factors that
were thoughtto precipitatefamily crisis. The
concept of "crisis" (or "X" factor), Hill argued,wasintendedto markthe point at which
a family unit is disruptedand disorganizedin
the face of both normativeand nonnormative
stressor-inducedsituations.The three critical
factors that best explain the "crisis proneness" of families are the stressorand related
hardships("A" factor),the family's resources
neededto managethe stressor("B" factor),
and the family's definition of the stressor
("C" factor). According to the theory,families who are crisis prone tend to experience
more stressors,particularly those that pose
major challenges.In addition, thesefamilies
tend to havefewercoping resourcesavailable
to them and are more likely to view stressors
as crisesin family life ratherthanasmanageable events.Within the ABCX model,families are proposedto follow a roller-coaster
course of adjustmentwith a trajectoryof disorganization, crisis, reorganization,and recovery (Hill, 1949, 1958). Not all families,
however,progressto the point of a family crisis in which the family systemchangesand
reorganizationis necessary.~e ABCX componentsof the Hill modelwere introducedas
explanatoryor predictorvariablesto account
for the variability in family functioning in the
face of a stressor and to determine which
families deterioratedto the point of experiencing a crisis and which families did not.
Thus, Hill's model focuseson precrisisvariabIesor whathas beenreferredto in the later
literature asprotectivefactors.
On thebasisof bothqualitativeandquantitative longitudinal investigationsconducted
on families faced with war-inducedseparations, Hill's ABCX model evolved into the
double ABCX model (McCubbin & Patters<:>n,
1983a).This evolutionwasbasedon several fundamentalobservations.First, in the
face of conditionsof chronic stress,families,
operatingas a system,are forced into a crisis
and called on to reorganizeand changetheir
patternsof operation.Second,the ABCX factors defined in the Hill model were not sufficient to explain the variability in postcrisis
family functioning involving reorganization
and recovery. Therefore, additional factors
wereidentified. Third, the outcomeof family
postcrisisbehaviorandprocessesappearedto
be that of adaptation.Familiesneedto achieve
a different level of functioning as a result of
changesin the family system.This level of
functioning, referred to as adaptation (XX
factor),reflectsthe family's effort to balance
demandsplacedon the family unit referredto
as "pileup" (AA factor) with the family's resourcesand capabilities(BB factor). Family
appraisal(CC factor) involves an overall assessment
of the family situation,including the
stressorand its hardships,changesmade,the
family's capability,the compatibility of family changeswith memberneedsand development,and the coordinationand synergismof
thesefamily changeswith all aspectsof family functioning and systemneeds.Coping is
the family's operatingarmfor producingthese
changes,
reducingtension,andachievingfamily harmonyandbalance.
With the addedfocus on the family processesinvolved in adaptation, namely, the
family's postcrisis behaviors, the double
ABCX model took on a subsequenttransformationreferredto as the Family Adjustment
and Adaptation Response (FAAR) model
(McCubbin & Patterson, 1983b). In this
framework,family processesinvolved in adaptation are introduced and described.The
family's movementthroughpostcrisisrecovery involves a set of processesinclusive of
change,synergism,congruency,coordination,
assimilation,accommodation,
andcoping.Interestingly,researchon family protectivefactors and processesemerged as the FAAR
modelwasbeingintroducedand subjectedto
scrutinyand additionalstudy. Family protective processesgained prominenceas family
scientistsexaminedthe patternsof functioning that servedto protectfamilies from being
"crisis prone" and that also servedto foster
theeaseof family recoveryin the faceof a cri-
r
c",
,
Stress,Coping,and FamilyHealth'"
sis situation (McCubbin, 1987; Olson et aI.,
1984). The FAAR model also was being
tested for its applicability to the study of families faced with childhood chronic illnesses,
297
cause families do not live in a vacuum, the'
context of family life is critical in shaping experiences of stress. The Contextual Model of
Family Stress (Boss, 1987) develops the con-
namely, cystic fibrosis, myelomeningocele,
and cerebral palsy. Family patterns or
typologies (T factor) of family functioning
emerged as important predictors of family
postcrisis adaptation and functioning. Most
prominent among the typologies were family
patterns ofregenerativity, resiliency, traditionalism, and rhythmicity. With these sets of dramatic findings, depicting both protective and
recovery patterns of family functioning that
served to predict family adaptation, the TDouble ABCX model, which was inclusive of
the FAAR elements, was given recognition
and advanced for additional study and application for practice.
The development and evolution of family
stress theory took another bold step with the
emergence of the Resiliency Model of Family
Stress, Adjustment, and Adaptation. Not only
did risk, protective, and recovery factors gain'
prominence in the resiliency model but also
the conceptual framework evolved as a result
of research on families of different ethnic
groups and cultures as well as emerging inter.est in multiple levels of family appraisal found
to be relevant in understanding and explaining
family adaptation (McCubbin & McCubbin,
1993; McCubbin, McCubbin, Thompson, &
Thompson, 1995/1996). In the Resiliency
Model of Family Stress, Adjustment, and Adaptation, the assumption that families manage
stressful situations over time emphasizes the
family's ability to recover from stressful
events and crises by drawing on patterns of
cept of family context, situated as two concentric circles surrounding the concepts of the
ABCX model. In the innermost circle, internal context relates to factors that the family
can change and control and includes three dimensions: (a) structural context, including the
family boundaries, roles, and rules; (b) psychological context-the family's perception
(both cognitive and affective) of the stressful
event; and (c) philosophical context, or the
family's values and beliefs. Unlike the internal context, the family has little or no control
over its external context-~e
broader environment in which the family is situated. This
outermost circle includes the elements of culture, history, economics, development, and
heredity. Boss also differentiates between
family stressand crisis. Family stressis a neutral concept that simply describes pressure experienced by families that changes family
equilibrium in some way. Two outcomes of
stress are possible within Boss's model: crisis
or coping. Crisis is a serious disturbance in
the functioning of the family such that the
family is immobilized. Coping refers to the
family's management of the stressful event
such that there are no detrimental effects on
family members. Although this definition of
coping is tied to effectiveness or success in
management (an outcome), Boss also refers to
coping as a process of managing the stressful
situation, leading to confusion about the nature of this concept.
Burr, Klein, and associates(1994) devel-
!
functioning, strengths, capabilities, appraisal
processes, coping, resources, and problem
solving to facilitate adaptation. Because of the
centrality of the resiliency model in the study
of family stress and coping in nursing, it is reviewed in depth later.
Using a symbolic interactionist perspective, Boss (1987) proposed that although the
meaning of an event to the family is the most
important factor influencing family stress,it is
the least well understood. Furthermore, be-
oped a systems-oriented model of family
stress as a means of addressing inconsistency
between family theories that emphasize systerns processesand the deterministic assumptions of the ABCX model and theories that
have evolved from it that have guided much of
the research about family stress and coping.
For these theorists, stress is viewed as a process that is intnnsically linked to other family
systems processes.F~mily s~ess.occ~rs when
usual rules for managmg famIly lIfe (I.e., rules
i
:1
:1
i
~
'I
~
,\
I
I
~,
1
"j,
I::
i
'I
i
!,!
,
Jf
298 ..INTERACTIONAL
AND TRANSACTIONAL
of transfoffi1ation)are not sufficient for the
family to handlechangeor a new input to the
system.As a result,noffi1alactivitiesandroutinesare disrupted,and attentionis focusedon
the stressfulsituationand how the family will
manageit. Using this perspective,Burr et al.
studiedstressprocessesof 50 families experiencing six different stressful events: bankruptcy, institutionalized handicappedchild,
troubled teenager,chronically ill child (muscular dystrophy),infertility, and displacement
as a homemaker.Data were collected using
in-depth interviews, observation,and questionnaires in participants'homesduring a 3month period. Study findings provided support for complexity and variation in family
stress and coping processes.The following
theoreticalinsightshave beenproposedfrom
this work: (a) families exhibit many different
patternsof responseto stressfulsituations;(b)
families that are quick to allocate resources
for managinga stressfulsituationtendto cope
more effectively than those that wait; (c) the
emotional subsystem(communication,cohesion,bonding,and togetherness)
mayimprove
as a resultof experiencingstress;(d) if families focus on changesin their emotionalsystemsduring stress,theytend to copemore effectively; (e) although specific coping
strategies tend to be generally helpful or
harmful, this deteffi1inationis context specific; and (t) there are some generaldifferences in men's and women's ~pproachesto
coping with stressful events (Burr et al.,
1994).
In summary,this brief overviewof family
stressand coping theories that have evolved
within social scienceprovidesa glimpse into
foundational work in this area. For in-depth
descriptionsof thesetheories,the readeris directed to the original texts. Although much
theorizing about family stress and coping
evolved from the ABCX model, there is a
clear indication that scholarshipwithin this
domainis shifting its focusto considerthe impact of systemsthinking, the role of family
strengthsand resiliency,and the role of context in family stressexperience.Foundational
work conductedwithin the socialscienceshas
MODELS
beeninfluential in nursing'sapproachto family stressand coping. Although family stress
and coping theoriesthat haveevolved within
nursingbearsomesimilarity to social science
perspectives,they have been less bound to
thesetheoriesand, therefore,provide unique
waysof understandingfamily stressarid coping.
>- EVOLVING PERSPECTIVES
IN NURSING
It is no accidentthattheoriesof family stress,
coping, and resiliency emergedwithin nursing. The durability of the family systemin the
face of adversityhas profound implications
for both the short- and 10ng-teffi1health and
well-being of family members,who may be
living with diseaseor disability. Nurses are
challengedto promote the health and developmentof both family membersandthe family as a unit. In the following sections,three
theoriesthat haveadvancednursing's ability
to understand,predict, and work with families understressare examined.The theories
reviewedvary in both perspectiveand stage
of developmentand are presentedas exampIes of nursing's unique contribution to understandingfamily stressandcoping.
The ResiliencyModel of Family Stress,
Adjustment,and Adaptation
Origins and Evolution
One of the important developmentsin
family stresstheory is advancementof theories that explainresiliencyin the family unit.
Family resiliency theory,a natural extension
of family stresstheory,wasdevelopedto shed
light on our understandingof how and why
somefamilies, whenfaced with the adversity
of illnessesand traumaticconditions,are able
to cope,endure,andsurvive.It alsoplaysa vital andpositiverole in explainingsupportand
in-home care to promote the well-being of
family memberswho may be threatenedor af-
~;
J!
I;
':,~
Stress,Coping,and FamilyHealth ~
fectedby the situation. For the purposeof developing and applying interventionstrategies,
nursing and other disciplines are cultivating
the developmentof resiliencytheoriesthatanswerthe complexquestionof whichcombination of risk factors,protectivefactors,andrecovery factorsdetermineswhich families are
more likely to adaptto a family crisis involving a traumatizing illness or medicalcondition.
The combinedresearchandtheory-building efforts of nursing and family scientists,
encompassinga period of 15 yearsat the endowedInstitute for the Study of Resiliencyin
Families and the Family Stress,Coping,and
Health Projectatthe Universityof WisconsinMadison, have resulted in the Resiliency
Model of Family Stress,Adjustment,andAdaptation (McCubbin & McCubbin, 1993,
1996).This frameworkhasbeenusedto guide
researchby nursing and behavioralscientists
throughoutthe world working both individually and collectively to isolateprotectiveand
recoveryfactorsin the family unit thatmayaffect physical and psychologicaloutcomesof
family membersaffected by medicalconditions. In addition,the resiliencymodeland derived findings have fostered the parallel researchefforts directedat the developmentand
testing of reliableandvalid measures
to assess
risk, protective, and recovery factors to be
used in family and health-relatedinvestigations. The developmentof family measuresto
study stress,coping, and resiliencyhas been
in progressfor the past20years(McCubbin&
Thompson, 1987, 1991; McCubbin, Thompson,& McCubbin, 1996; Olsonet al., 1984).
I
Resiliencyand Family Nursing
In the context of family nursing,family
resiliencyis defined as the property of the
family systemthat enablesthe family unit to
respond constructively to (a) a stressor(in
combinationwith risk factors) and,in so doing, maintainits positive functioning and ensure the well-being and developmentof the
family unit and its members(i.e., protective),
and (b) disorganization(family crisis brought
,
299
aboutby a stressorin combinationwith risk
factors)and,in doing so,bounceback and restore its positive functioning and ensurethe
well-beingand developmentof the family unit
and its members(i.e., recovery).
The conceptof family resiliency has a
rich history embeddedin the longitudinal research on resilience in children (Werner,
1984;Werner& Smith, 1982),the studyof resiiiency in children at risk for adversedevelopmentaloutcomes(Garmezy,1991a,1991b;
Rutter, 1990), investigations of children's
competenceas a protective factor in the face
of risk situations(Garmezy,1987;Garmezy&
Masten,1991;Luthar&Zigler, 1992),andthe
study of resiliency in inner-city adolescents
(Luthar,1991;Luthar, Doernberger,& Zigler,
1993).
Therehasbeena proliferationof research
on resiliencyin childrenand youth with investigationsdesignedto determinewhich aspects
in the family milieu emergeas centralprotective factorsin the developmentof resiliencyin
children(Baldwin, 1990;Conrad& Hammen,I
1993; Richters & Martinez, 1993; Wyman,
Cowen,Work,& Parker,1991).In the pastdecade,nursing and family scientistshave expandedthis earlierfocusto investigateand advance theories to explain variability in
resiliencyof the family systemin the face of
normative(McCubbin, 1999)and nonnormative life events and changes (McCubbin,
McCubbin,Thompson,Han,& Allen, 1997).
Drawing from two decadesof family
stress, coping, and resiliency research to
which they are sustained contributors,
McCubbin and McCubbin (1993, 1996) in
collaborationwith their colleagues(McCubbin et al., 1995/1996,1997) developedand
testedthe ResiliencyModel of Family Stress,
Adjustment,and Adaptation.This conceptual
frameworkhasbeenusedto guide both family
scienceand nursing studies throughout the
world. The 36 copyrighted researchinstruments developed by the McCubbin and
McCubbinteamand testedfor reliability and
validity havebeenusedto measurevariousdimensionsof the resiliencyframework,particularly risk, protective,and recovery factors.
c
~
c':
I_~
.
300 ..INTERACTIONAL
AND TRANSACTIONAL
Nonnative data are available for many of
these measures,and some have been"translated into foreign languages,including Korean, Chinese, Spanish, Hebrew, Japanese,
and Russian for applicationin cross-cultural
studies(McCubbin et al., 1996).
As described previously,the Resiliency
Model of Family Stress,Adjustment,andAdaptation is rooted in Hill's (1949, 1958)
ABCX model and hasevolvedsystematically
for a period of 20 years.This evolution has
beenfosteredby bothqualitativeandquantitative studiesof families faced with life events
such as war-induced separation(McCubbin,
Dahl, Hunter, & Plag, 1975),having a child
memberwith a chronic illness (McCubbin&
McCubbin, 1993),and nonnative transitions
and changes(McCubbin, Thompson,Pirner,
& McCubbin, 1988).The inductivelyderived
conceptualmodelof family resiliencyfocuses
on the role of risk, protective,and recovery
factors in the prediction and explanationof
family resiliency (McCubbin et al., 1997).
The McCubbin and McCubbin framework
seeksto explain why some families endure
life's hardshipsand traumaswith minor adjustmentand appearto be bufferedby protective factors.The frameworkis alsointendedto
explain why families in crisis, or those who
experience disorganizationand a need for
changedue to life events,are able to bounce
back,recover,and adaptthroughthe useof recovery factors in the process.of restoring,
changing, and introducing new patterns of
family functioning.
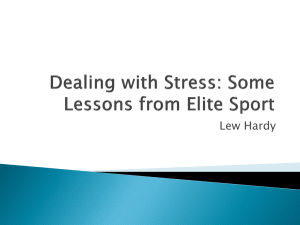
A more completediagram of the family
resiliency model (McCubbin & McCubbin,
1996),which hasalso beendevelopedto have
predictive and explanatoryvalue in the study
of families of different ethnic groups,is presentedin Figure 12.1 (adjustmentphase)and
Figure 12.2 (adaptationphase).
FamilyAdjustment:
A Short-TermResponse
in the face of a diagnosis and the demandsof caring for a memberwith anillness
or disability, the family's initial reaction is
MODELS
predictablyto maintainthe "statusquo" with
minimal changesin how the family typically
operatesand behaves.In this "adjustment
phase"of the resiliencymodel,the family system draws from its existing patternsof functioning, strengths,andprotectivefactors(e.g.,
accord,hardiness,time and routines,celebrations,and traditions).The interactingcomponents in this phaseof family resiliency are
seenas (a) the stressorevent(e.g., diagnosis,
illness, and disability); (b) the family's vulnerability (risk factorsand the pileup of concurrentlife changes,suchas marital conflict,
abuse,and history of violence); (c) the family's establishedpatternsof functioning (e.g.,
family time and routines and family tradi-,
tions); (d) thefamily's resources,both internal
and externalto the family unit (e.g.,cohesivenessand socialsupport);(e) the family's appraisalof the stressorand its severity;and (t)
the family's coping repertoireand problemsolving communication(e.g.,seekingconsultation,opennessto medicaladvice,and seeking supportfrom supportgroups).In the short
term,the family directsits energyanddoesall
thatis possibleto keepfamily systemchanges
to a minimum and attempts to maintain
healthy functioning in the family unit. The
family seeksto maintainharmonyandbalance
among its four basic components-namely,
the family's interpersonalrelationships,the
family's development
and memberwell-being
(including spirituality), the family's structure
and functioning,andthe family's relationship
with the community.
The confirmationof a diagnosis or disability or both,combinedwith ever-increasing
demandson the family unit to modify its establishedpatternsof functioning,to introduce
new patterns,and to find harmony and balancein the family systemwill often movethe
family into a crisis situation. Family crisis is
not a pejorativeterm. Rather,it representsa
stateof temporarydisorganizationaccompanied by a demandfor changesin the family's
expectations,rules, and overall patterns of
functioning.At this point,the family struggles
to modify the old and introduce new patterns
of functioningto achievefamily adaptation-
I
I
"
I,
rd
~
~ ~
Q) ~
s 0
.~
~~
~~
..14.~
~ ==
.~
IoV
""i
fJ)
00..
..M
~
Q) ~
~ ~
~
00 ~
~ .-4
~ ~
.~ M
~
~
SCI-I
..
IoV0
~ ""'"
~
0 ""00
,"
~
~
~
Q)
~"O
~
.~~£
~~.-4
~~
=~
Q) 0
.~ .~
...~
IoV
Q) ~
"'-
-~
.~,~
~ ~
~~
.d..=
~ ~
IoV
.:I:
(
4
;;:;.
.g
Sbil
t
p.°'"5a1o
~ ~ U)
bD
~.~
~
Q
'-' Q) ~> -~
~...
~
U).o
...0.
a bO~~.'t::
~
~ ...~
?;-.S-o>
a~
.s z
§ ~~
8~~
~
0>-.-a
~
~5
~
~
Q)
iiJ~
er..
0>5
;~
~~"'c)~
~"'.
W Po
0
~~rfi
oS;9.C;
Po'~
E
-0
~
,
~
...~.
Q
~-a.
'" '"
~ .;
«
~s.
VJ -~._~...
~
.v
.-=
>.~
-'"
...~
~
~
-~
~
8 In
o~
~
~~ ?'~
-oc...bD
Q)o.g
~
°=
a
~
=
t.s
"0
~
0
~
£
~
]v
.-=0
v
~
t.s
~
"8
[
.§
-0
t.s
<I:
a-
"0
V
-=
~
~
a
:& ;
~
b
~'""'
~\O
~~
0 ,c
.S
~ -'
~u
~:.s
~.g
g~
.~ =
~~
.g:3
-,c
aI~~
.a0>""~
~CG
~rn~
..-~."".-.
F! ° c
~~~
t
:>..
:
-i!
=
v ~(.)
-5
° a
~
0"0:
;.:=
.D
Q)
fJ)
..~
IoV M
I
I
ji
l'
I'
-=
'"
v °
Co..S!
E
~
v .s
:l:.=
.s
~
:>
:&-5
1
J!
"
'!
1
<I: .-,
~
&
~
(.)
~'V "0
=
~o.
"":3
N
~~ v
00
O
~
Q)~
00<;~"8
t
Q)
~c
~~
~~
.~
0
.d
~
oW ~
~ ~
~ ~
S~
~~
fI) "i
=s
.~
-~
\J
~
"i
00
301
"'I
M
t1)
t1)
Q)
Q)~
~
;
~
.~
' ~
t
I
S ~
.:
..'
.g
~
~..~
.~
2
~.
;
5
'"
~,
.i
.g
I
,
.~
I
I
I
1
I
:
:
1
:
1II
I
0
=
E
V
~
V
'"
'"
8
e
Q.
,g
~=
-1U
V
~
-
"0
=
~
~
I
I
I
I
,0
::3
"0
go
~~
I
I
:
1
:
~
-«
"0
=
--1
1
-,-
I
,',.."
I
"
.."0
~..
§
-:='
--1:0-
-s,a
0.
a<
-@
,
'=0~0
,-
u
~
'08
-5~
v u
~ u
~.o
:=.0
=
v
"t;'c/d
'""~'""
~
0 u:='
"0 .0
,5
.0
r;)
.?:-G'
..
~
'".
~
-«
"0
.'?"
8
-on
~
.
1
I
:
,
,'--',
"
1
,
e ',:°e:; ,I
"-')'
'- bO '
..'
'i ° 5 '
I ".
'£
'- bO'
.g
!:o-..o. 5
-ltrZ 8
s~
~
..~
~:§.
~'"
.I
~..
."
,
I>.]~'§"
,za~§~1
'
]
'-~rz."
'
"-'
,
'
,
I.,G/ -1l ~ ~
'
,
I
')
~
I
I
,-bO
'/'
rz. I
'-0°5
"
'
t1)-
,
Q) ~
~
Q) Q)
,
'~Ee,2e:;
I ., '., 1l -E'-
:
.I
"
-
'
8
'-
--,
I
-~s:s
,"'~
,-0
ve
"' =
Q.
,-
"O~
0-0-
~
""
:>
V
8
..
= ~
o
,1U
~
-«,~
~b
.-v
Of) 0-
~ ..
0
=
""
:='
~"O
N U
.v
-<
I
I
4
,
--'
~
.~
I
-'
..~
,..
'
,
§O
-.:
,I
,~.'
f
10 ~
03.6
,
t
I.
,.,.'.:
I ,.:eo"
I 3$'~C
" ~ ~ §
,
rz.
~
..'--'
0 'tj
Q)
t1)
0
~ =
..c:
~~
,
"
~
~'~..=
~
3
0
=~
0"
I --
cI
i3~~E'-
I
I
I
,
,]rz.
'cod,
,
,-
.
..~
I 'OQ)~,,~
~
~'tj
~
I
~ fo
N"O
~I:~
cn
"
',.s'a9'
,cI~,_d
I
..~
~<
'tj
I
\
<-I
..~~
..~
'--'
't1)
,
I I"'" .'~,,'
0 ...~
~'tj§
302
V
c"-
SOl
~ ---§~.>-g
= '""'
Q) =
~ a
'tj~
t1) ~
= ~
..." ~
'tj
~=
t1) '"
"'"
I
.U
..~"
~
Q)Q)
~
~
~
...!!-.
II
'"
".I
-,
.."
~
,--,
'""'
~
-'"
~
~
t1)
~~,,~
~
M'tj O O
-t1)
0
r~
'(ij 0
a
,
1I
,...,...
~~
Q) Q)
-:5 -:5
...=
..0
~ ~
=~~>.
~
~
-
,
"7111111111
Ii.
~
Stress, Coping, and Family Health
the point at which harmony and congruency at
the interpersonal, developmental, structural,
and community levels of family functioning
are achieved.
303
The level and ease of family adaptation,
according to McCubbin and McCubbin
(1988a, 1988b, 1993, 1996), is determined by
many interacting factors. These moderating
and mediating factors include the pileup of
family demands and risk factors extant'to the
family unit (e.g., prior marriage with
and adopt new and necessarypatterns of functioning are important to consider in an
assessmentof family resiliency. For example,
the family's ability to comprehend and integrate a home care medical regimen into their
pattern of functioning, while maintaining or
restoring family harmony and balance is an
important consideration in the family's ability
to achieve a satisfactory level of adaptation.
The family unit may need to establish a supportive network of friends and associates to
help them to cope with the situation. The
medical community of physicians and nurses
may be a new part of the family's network of
support-a social. group that did not exist or
stepchildren in the household) and its history
as well as demands created by an illness situation (e.g., home care regimen and treatment
plans). The family continues to develop, and
normal family life cycle transitions (e.g., having an adolescent in the home), prior strains
(e.g., conflict regarding religious beliefs and
spending money), unresolved conflicts and issues (e.g., marital conflict), the positive and
unexpected side effects of a family's efforts to
cope (e.g., conflict because spouse takes on
additional work to make ends meet) also come
into play and influence the family's response
and adaptation. The concurrent nonnal and
abnormal life events (e.g., death in the extended family) and the ambiguity regarding
what the future will hold for the family unit
must all be taken into account in evaluating
the family's capability for managing the diagnosis and future course of treatment for the ill
member. The accumulation of life changes
and hardships determines the extent to which
the family's capabilities and protective
resources (e.g., income, psychological and interpersonal strengths, and established patterns
of family functioning that serve to creates stability and predictability) are disrupted, deteriorated, drawn down, or depleted and what remains of these patterns to be applied to
helping the family to adapt to the current family crisis situation.
Family recovery factors are also important in the resiliency model. Efforts to create
that was not previously important. Family systern resources of flexibility and problem-solving communication that ensure a mutually
supportive and encouraging rather than a
conflictual pattern of communication may become even more important to the family unit
in a crisis situation.
The resiliency model, which also draws
from Aaron Antonovsky's exemplary theory
building and research on "sense of coherence"
(see Chapter 8 of this book) also underscores
the importance of the family's appraisal processesin achieving a satisfactory level of family adaptation. Families are also called on to
reconcile differences and conflicts that may
emerge when the family unit, through a trialand-error process, adoptspatterns of functioning to cope that may not be congruent with the
family's strongly held beliefs and values. The
family's worldview, or what McCubbin and
McCubbin (1996) call family schema, must
also be congruent with the family's newly instituted patterns of functioning. For example,
McCubbin and McCubbin note that family
members may find meaning and value in raising the nation's consciousness about a disease
or disability a family member may have with
the hope that more research funding could
lead to new and effective treatments. To
champion this national cause, however, may
move a family unit farther apart becausesome
members may be "on the road" while the remaining members struggle to achieve balance
Family Adaptation: The
Long-Term Response
!
~
~
i
!
'
I
i
i
,
,-
-,."",.
-i
--~
304 ~
INTERACTIONAL
AND TRANSACTIONAL
.andhannonyo~ th~irown.This maycreatean
Incongruous slt~ation betweenthe ~amily's
sch~maof working togetheras a UnIt and a
famIly member'sefforts to make the disease
or disability a nationalpriority.
~e family unit is also called on to give
~eamng to the healthproblem.Family meanmgs.arethecollectiveviewsof the family unit
cultivated, developed,and adopted (actively
and passively)by family membersto render
legitimacyand acceptabilityto the currentsituation (e.g.,illness anddisability). Thesevaluesrelateto the family's effortsto cope,to the
family's adoptedpatternsof functioning,and
to the family's hopes and beliefs for the future, given the crisis that hasalteredthe family's original life courseto a substantialdegree.
Family paradigms may also changeto
give legitimacy and meaningto the new patterns of functioning. Families may have
shapedand adopted a family paradigm for
work thataffinns family members'individuality to do what is necessaryto promote their
own professionalor work careers.In the face
of a family healthproblem,this paradigmmay
be cast aside and replacedby a sharedcommitment to have one memberdevote his/her
full-time efforts to the careof a memberwho
is ill or disabled with the agreementthat, at
sometime in the future,this membermaypursuehis or her own careergoals.Family paradigms, according to the resiliency model,
servea vital role in stabilizingandgiving predictability to the family unit. They are most
commonly createdand adoptedto guide the
family's central areas of functioningnamely,the family's marital or partnercommunication,sexualrelationship,parentingrelationship, work and family relationships,financial management,in-laws and relatives
relationships,and socialrelationships.
The resiliency modelincludesa family's
cultural andethnic historythat may beembedded in the personal history of its members.
McCubbin and McCubbin (1996) argue that
culture and ethnicity playa critical role in
shapingthe family's responseto family crises
and the adoption of patternsof functioning
MODELS
neededto achievea satisfactorylevel of adaptation. By drawing from and conducting
studiesof African American, Filipino, Asian
American,and Native Hawaiian families under stress,McCubbin and McCubbin isolate
the importanceof culture and ethnicity in the
family schema(e.g., values,beliefs,and rules)
and senseof coherence(e.g., trust, control,
and manageability),both of which are confirmed to be importantto the family processof
adaptationin the face of family crises.
InstrumentDevelopmentand Use
The ResiliencyModel of Family Stress,
Adjustment, and Adaptation emerged from
and continuesto be shapedby an inductive
processwith researchinforming theory.Consequently,the developmentof family measuresto study risk, protective,and recovery
factorsin the processof adaptationhas been
continuoussince the introduction of the initial versionsof the theoretical framework in
1978. Throughout the years, the Family
Stress, Coping, and Health Project has
generated36 reliableandvalid self-reportand
family system-focused research instruments.In testingtheevolving theory,a host of
family adaptationmeasureshave been used,
including the family APGAR (Adaptation,
Partnership, Growth, Affection, Resolve)
(Smilkstein, 1978),FACES (Family and Cohesion Evaluation Scales I, II, IIA, III)
(Olson,Portner,& Bell, 1978, 1982),Family
Indexof Regenerativityand Adaptation-General (McCubbin& Thompson,1987),Family
Member Well-Being Index (McCubbin &
Patterson,1982/1996),Family Distress Index
(McCubbin, Thompson, Thompson, &
McCubbin, 1993), and Family Attachment
and ChangeabilityIndex (McCubbin,Thompson,& Elver, 1995/1996a).In addition,measuresof family risk factors,family protective
factors,andfamily recoveryfactors,presented
in the book Family Assessment:Resiliency,
Coping and Adaptation-Inventories for Research and Practice (McCubbin, Olson, &
Larson,1996)includethe following:
~ c~
,:
Stress, Coping, and Family Health'"
1. Risk factors or pileup: the Family Inventory
of Life Eventsand Changes(FILE; McCubbin & Patterson,1983a),the AdolescentFamily Inventory of Life. Events and
Changes&(AFlLE;
McCubbm, thPatterson,
H
.
1981/1996)
"
Bauman,
Ad
I F
.
arns,
,
e
loung
1 I
t
f L .ti E ts d
u t amI y nvenory 0 I even
an
Strains (YAFlLE; McCubbin, Patterson,&
Grochowski, 1984/1996),and the Family
PressuresScale-Ethnic(McCubbin,Thompson,& Elver, 1993/1996)
2. Protectivefactors: the Family HardinessIndex (McCubbin, McCubbin, & Thompson,
1988), the Family Inventory of Resources
for Management(McCubbin, Comeau, &
Harkins, 1991),the Family lime and Routines Index (McCubbin, McCubbin, &
Thompson, 1988), the Family Traditions
Scale (McCubbin & Thompson, 1986a/
996)
1
,
h
t e
F
.1
amI y
C
I b
.
e e rations
I d
n ex
(McCubbin & Thompson,1986b/1996),the
Social Support Index (SSI; McCubbin,
Patterson,& Glynn, 1981/1996),and the
Young Adult Social SupportIndex(YA-SSI;
McCubbinet al., 1984/1996)
3. Recoveryfactors: the Coping Health Inventory for Parents (McCubbin, McCubbin,
Nevin, & Cauble,1983/1996;McCubbin et
al., 1983),the Family Crisis OrientedPersonal EvaluationScales(McCubbin, Olson,
& Larsen, 1981/1996),the Family Coping
Index (McCubbin, Thompson, & Elver,
..n
1995/1996b),the AdolescentCopIng Onen..pecla
tattonfor ProblemExpenences(patterson&
McCubbin, 1983/1996),the Youth Coping
Index (McCubbin, Thompson, & Elver,
1995/1996c),the Family Problem Solving
Communication (McCubbin et al., 1988),
the Dual-EmployedCoping Scales(Skinner
& McCubbin, 1981), and the Family
Schema-Ethnic Inventory (McCubbin,
Thompson,Elver, & Carpenter,1992/1996)
Nursing Research
The evolution of nursing research using
the resiliency model resulted from the profession's interest in exploring family change and
adaptation over time. Although the theoretical
framework had its origin in war-induced family traumas, the resiliency model gained currency by virtue of its relevance to the study of
305
families coping with many health problems,
including myelomeningocele (McCubbIn,
1988a, 1989), handicaps (McCubbin, 1988b),
cystic fibrosis (McCubbin, McCubbin, MischI
& S
.. m press), and cerebral
er,
vavarsdottIr,
1 (M C bb.
1 198 )
pa sy
cum
et a .,
1.
..Carr (1995) affi~ed the value of the resillency model as a guide to nursing research.
Many nursing studies have examined family
stressand adaptation within the framework of
the resiliency model, For example, the resiliency model has been used to guide research
on families coping with acute health problems, such as myocardial infarction (Carr,
1995), severe trauma, and head injuries
(Kosciulek, McCubbin, & McCubbin, 1993;
Leske & Jiricka, 1998). The model has also
.
been
used
to
study
family
responses
to
hr . h ' ldh d
di .,
c om~ c I. 00 con ~ons m.many c~ntexts, IncludIng those caring for Infants with
chronic apnea at home, children withcongenital heart conditions, and children with a variety of illnesses participating in early discharge
programs after rehabilitation (Svavarsdottir &
McCubbin, 1996; Youngblut, Brennan, &
Swegart, 1994). In addition, the model has
been used to examine life changes such as retirement (Smith, 1997).
C .t .,l"
I ue oJ the M 0 deI a nd
~ I C .d .
S
onsl eratlons
Originally, Hill's ABCX model offered
simplicity and a charted, linear approach to
knowledge development about family ~tress
and family crises. McCubbin, McCubbin, and
associates (McCubbin & McCubbin, 1988a,
1988b, 1996; McCubbin et al., 1997) have
made the case for looking beyond family crises. They have fostered a line of research designed to isolate those risk, protective, and recovery factors that provide nursing with the
best possible predictors of family adaptation
in the face of a range of illnesses, disabilities,
and life situations. Ironically, although the
complexity of the Resiliency Model of Family
Adjustment and Adaptation has shed new
light on critical factors that shape the outcome
of family adaptation, particularly for those
~:f':
306 ~
INTERACTIONAL
AND TRANSACTIONAL
families of different ethnic backgrou9ds,the
model has also been difficult to test as a
whole. Although a few investigationshaveexaminedthe model in a comprehensive
way by
defining dimensionsof the model as latent
variablesunderlying broaderconstructs,there
is much to be learnedaboutthe direct andindirect effects of risk factors and about the
moderatingand mediatinginfluencesof protective and recovery factors (Lavee,
McCubbin, & Patterson,1985; McCubbin &
McCubbin, 1988a,1988b,1996).
As noted by the developingauthors,but
also emphasizedhere,there is much to learn
about families under stress,including why
and under what conditionsfamilies "bounce
back." The resiliency model needsto be expandedor competitiveframeworksintroduced
or both to explain the variability in perceptions and meaningsof eventsby the family
and individual members. Furthermore,the
contribution of daily hasslesto the clusterof
risk factors that families must deal with on a
day-to-day basis needs to be examined.
Studiesthat addressthe complexityof coping
behaviorsand repertoiresand identify when
they serve as protectiveand recoveryfactors
in the processesof family adjustmentand adaptationare also needed.Finally, the issueof
potential deliberateness
of family crisesneeds
to be studied.Do somefamilies allow themselvesto entera crisis asa plannedstrategyso
as to change and transform.themselvesfor
their own good?Nursinghasmuchto offer the
advancementof the resiliency theory as we
move toward greaterunderstandingof family
risk, protective,and recoveryfactors and the
conditions under which they operatemosteffectively.
The Framework of
SystemicOrganization
Origins and Evolution
, A secondfamily model,the Framework
, of Systemic Organization,draws on principIes derived from opensystemstheory (Von
':
MODELS
Bertalanffy, 1968)and social ecology(Bronfenbrenner,1977).In contrastto othermodels
discussedin this chapter, its origin is not
rootedin theoriesof stressandcoping.In fact,
neithertermappearsin Friedemann'stheoretical articles or textbook (Friedemann,1989a,
1989b,1995). Instead,the framework presents an explanationand visualizationof general family functioning. Within the total family process,coping is seen as a series of
actionsundertakento resolveincongruenceor
disharmonywithin family members,between
members,and betweenthe family and its environment.Friedemann(1995)claims that everyone affected feels incongruence; it can
therefore be defined as stress. Friedemann
offersthe idea that copingis embeddedin the
family process (Anderson & Tomlinson,
1992)and suggeststhat coping represents
the
entire family processas it unfolds day after
day. This implies that the processis indivisible and respondsto an innate, often unconscious,needof the systems(family and individuals) to gain congruence.Coping is not
linear or circular but ratherthree-dimensional
in its complexity;it is not a responseto a stimulus but rathera seriesof strategiesof the entire family systemandits membersto respond
to changesfrom within or from the environment.
The developmentof the Frameworkof
Systemic Organizationstarted with the discoveryof four distinct dimensionsof family
functionipg as a result of a factor analysis
donefor the purposeof testing an instrument
to measurefamily functioning (Friedemann,
1991a). Family maintenanceand coherence
addressthe stability of the systemor homeostasis,whereasfamily changeand individuation referto family growth or morphogenesis.
Thesefour dimensionsare easily detectedin
family therapyliterature.Homeostasisis discussedas the outcomeof two groups of behaviors. The first, described by Bowen
(1976), representssystem maintenance,or
collective behaviorpatterns suchas decision
making,enforcingrules,caring for the sick,or
screeninginformation. These behaviorsare
groundedin a setof valuesandbeliefs thatare
"
Stress,Coping,and FamilyHealth ~
307
)~~;~~~~~~.I--~~Ge.
',~.~ CO~...~XEnvironment
StabiUty
EnVironment
i *Cf
~,'~
0
Coherence
System
Maintenance
a
U
In
SpirituaUty
;
,~
.[~!~~~=J~
\
n
Control
Individ~ons::: Change! .I
'. ~ "::::
.-/~"
~&
EnVironm~t '+0;:,
a~
/
~...~ -~
EnVi~onment
Growth
Figure 12.3. Frameworkof SystemicOrganization
learnedand taught to each new generation.
The secondgroup of behaviors,coherence,is
playedout atthe interpersonallevelandrefers
to sharingtime, space,emotionalenergy,and
materialgoods(Kantor& Lehr, 1975).
Growth or morphogenesisis also easily
divided into two groups of behaviors-those
thatareenactedatthe family systemleveland
thoseenactedatthe individuallevel. At theindividuallevel, family membersengagein individuationas they developinterests,commit
themselvesto goals outside the family, and
connect with other people. At the system
level, the family then adjuststo the diversity
of its membersthrough systemchange.It acceptsinformation from outsideandintegrates
it by making the necessaryorganizational
changes(Kantor& Lehr, 1975).
In addition to stability and growth,
Friedemanncomplementsthe modelwith two
othersystemictargets,controlandspirituality.
Theseshe conceptualizedinductively by examining her own family and nursingpractice
and deductivelybased them on the work of
Kantor and Lehr (1975). From this perspective,the family is seenas a systemcomposed
of individuals and interpersonal units, all
having unique qualities of their own. The
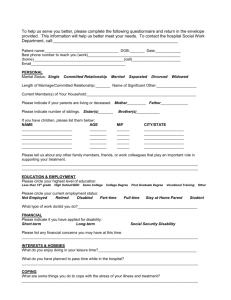
interactionsof family membersoccur as sequencesof actsand purposefulrepetitivepatterns.The notionthat family strategicpatterns
are relativelystableandbasicto a largeroverall family life processis centralto the framework of systemicorganization(Friedemann,
1989a, 1991a). This life process is representedgraphicallyin Figure 12.3.
TheModel
Accordingto Friedemann(1995),coping
with any type of changeis intimately fused
with the life processesof the family and its individuals. All systems seek congruence,a
statein which all interactingsystemsandsubsystemsfunction harmoniouslyin that their
rhythms and spatial patternsare attuned to
each other. Becausechangeis ongoing and
occurring at a rapid pace,a state of congruenceis utopian. Nevertheless,systemsstrive
to at least approachcongruenceto the extent
of feeling its effect as peaceof mind, calmness,and well-being. Friedemannclaims that
~;~~
1-,
t'i,:,
308 ..INTERACTIONAL
AND TRANSACTIONAL
MODELS
a major motivator for change is the need to
control anxiety that results from incongruence. Anxiety can become evident as physical
and mental distress in any form. Consequently,
and families
strivecontrol,
to find
a
desiredindividuals
level of stability
and growth,
problem negotiation patterns (Haley, 1976);
family structure and generational boundaries
(Minuchin, 1974); coalitions, rules, and roles
(Haley, 1976; Lewis, Beavers, Gossett, &
Phillips,
1976);& and
family
organization
control (Moos
Moos,
1984).
Coherenceand
en-
and spirituality to ward off anxiety and reacha
sense of congruence that is defined as health.
The emphasis individuals and families place
on each of the targets differs among families
and defines the family's style of functioning.
Health, therefore, is the subjective experience
of congruence. It increases as families reach
an approximation of their desired balance between stability and growth, control, and spirituality.
Coping with change, therefore, pertains
to four distinct processes.The first process is
maintaining stability through the continuation
of values, traditions, and daily routines.
Growth, the second process, occurs through
adaptation and readjustment of the system's
operation to changes from within and outside.
Growth implies a change of attitudes and values (second-order change) and not simply a
readjustment of roles and minor behaviors to
keep the family functioning (first-order
change) (Watzlawick, Weakland, & Fisch,
1974). The third process is control, a reaction
to change that attempts to eliminate or minimize threats to stability, with homeostasis being the goal. Examples are disciplining children, screening information, or seeking
medical care. Finally spirituality is defined as
changing one's own system (individual or
family) to find meaning and congruence. As a
result, the family accepts the change and incorporates it into its overall life process. Spirituality implies connecting with and becoming
a part of other systems,be it other individuals,
organizations, nature, or a higher being, and
thereby finding a new identity and meaning
(Friedemann, 1995).
In the family, these processes of coping
can be observed as behaviors that pertain to
the process dimensions in the inner circle of
'the model (Figure 12.3). System maintenance
tails behaviors used to establish and maintain
emotional bonds. Related concepts are closeness and empathy (Lewis et al., 1976), cohesion (Moos & Moos, 1984; Olson et al.,
1984), and enmeshment (Minuchin, 1974).
System change behaviors are necessaryto adjust to change from within and the environment. Concepts such as morphogenesis
(Buckley, 1967), adaptability (Olson et al.,
1984), and family growth and flexibility
(Kantor and Lehr, 1975; Lewis et al., 1976)
address these processes. Individuation consists of behaviors that individuals employ to
follow their interests and search for meaning.
On the family level, individuation relates to
the family's accommodation to members' differences in values, opinions, lifestyles, and
schedules. Individuation is implied in concepts such as self-differentiation (Bowen,
1976), self-disclosure, and expressiveness
(Lewis et al., 1976).
involves organizational strategies and includes concepts such as power structure and
client-driven, holistic, and in-depth approach
to individuals and families. Nurses assess
I'
The Nursing Process
The task of categorizing behaviors according to these process dimensions may be
formidable because the same behavior could
be categorized in more than one process dimension, depending on the reason why it is
undertaken. For example, a family walk in the
woods could be system maintenance if done
for the sake of physical exercise, coherence if
its purpose is to find togetherness, individuation if a family member seeks a co~nection to
nature in his or her search for meam~g, or system change if the walk is to provIde a new
identity and reorganization of priorities for the
family. Consequently, nurses need the family's interpretation of their own behaviors to
reach conclusions. Nursing within the Framework of Systemic Organization is therefore a
cc-C"
I
i
I
Stress,Coping,and FamilyHealth ~
309
with the family its life processbefore the
change (illness, crisis, etc.), its life process
afterthe change,and the optimal life process
theywould like to achieveconsideringthe situation.
Friedemann(1995) explains that for a
family to be healthy,all membersneedto expressa reasonablelevel of satisfactionwith
the family or well-being.To achievewell-being, eachperson'sdevelopmentalneedshave
to be honoredby the family. Althoughdevelopmentalneeds differ with age, all refer to
growth and change. Friedemannclaims that
everycrisis in a family occurswhengrowthis
inhibited, and thus every crisis is a developmentalcrisis.
Be it for the sake of crisis resolutionor
simplyto enhancethe life process,the goalof
nursingis notthe family's healthbutthefacilitation of the processthe family choosesto
achieve its health (congruence)and allow
eachpersonto grow and developfreely. The
entireprocessis coping and occurswithin the
dimensionsof the life processdescribedpreviously.Thechallengefor the nurseis to make
an assessment
that representsthe family's reality, not the nurse's.
Friedemann(1995) promotes open discussionin which the nurserevealsher or his
theoreticalthinking by explaining the major
conceptsof the model in simple terms and
thenencourages
the family to explorehoweverydaystrategiesandspecificcoping attempts
may fit into the four processdimensions.An
agreementaboutnecessarychangesis reached
jointly. Strategiesto enhancethe family processthat lead to a balanceof targetsthat the
(Friedemann,1995;Friedemann,Jozefowicz"
Schrader,Collins,& Strandberg,1989).
The Frameworkof Systemic Organization is appropriatefor families of variouscultures, structures,and/oreconomicsituations.
Whereasthe generallife processdepicted in
Figure 12.3is generallyapplicableto all families, vastdifferencesarefound in the specific
strategiesusedand in the emphasisplaced on
certain targetsamongvarious types of families. Within the Frameworkof SystemicOrganization,culture is defined as two processes
occurring simultaneously-namely, culture
maintenance and culture transformation.
Theseprocessesare inherentin the pursuit of
stability versusgrowth or the maintenanceof
cultural traditionversusadaptationof life patterns to a changed environment. Consequently,cultureis lived within the family life
process.To assesscultural patterns,the nurse
simply follows the dimensionsof the life processand examineshow certainstrategiesare
used to pursue family targets (Friedemann,
1991b,1995).Becausemanyof thesemay be
unfamiliar to the nurse,the unbiaseduse of
the modelhasthe potentialfor promotingcultural awareness.
The use of the framework reduces the
comparisonof client families along preset
normsthat may not be valid for all. Insteadof
using norms, the nurse can let the family
judge its own level of healthor effectiveness.
He/shemaydisagreewith the family's self-assessmentbased on signs of congruence orI
stress within the system. In such cases,the
nurseis encouragedto point out inconsistencies and suggestreevaluationof the situation.
family considersoptimalaredevelopedby examiningthe family's successes
in usingstrategies in the past. The nurse then assiststhe
family in using familiar strategiesor in the
creationof new ones. Interventionssuch as
teaching,practicing interactions,or procuring
newresourcesareusedif the family discovers
a need for new strategies.Friedemannhas
specifieda step-by-stepapproachin an interventionmodel for substanceabusingfamilies
(Friedemann,1989b,1992).This model also
has been applied in other areasof nursing
Ultimately, however, it is the family who
makes the decisionto changeand to make
changehappen.
InstrumentDevelopmentand Use
To usethe major conceptsof the Framework of SystemicOrganizationas a theoreticat basis for research, they need to be
operationalizedand measured.Key concepts
are family health and congruence.Friedemann(1995)statesthat healthcan only be es-
,
-
,
I
310 ...INTERACTIONAL
AND TRANSACTIONAL
MODELS
timatedand thatthe sole expertof healthis the
family. According to the framework,thereis
evidenceof health if (a) the family pursues
strategiespertainingto all four processdimensions, (b) the family is reasonablysatisfied
with family functioning, (c) the anxietylevel
of family membersis low,and (d) thereis congruencebetweenthe family's pursuitsandenvironmentalexpectations.
The Assessmentof Strategiesin Families-Effectiveness (ASF-E) instrument is
availablefor ini.tialscreeningof fam~lyhealth.
The ASF-E (Fnedemann,1991a; Fnedemann
& Smith, 1997)represents
a subjectiveassessmentof family effectivenessin all fourdimensions.Respondents
mark statements
of family
functioning ranked accordingto levels of effectivenessthatare mostlike their family. The
latest versionhas 20 items and subscoresfor
the targets of stability, growth, spirituality,
and individuation (Friedemann1998). The
ASF-E has beenexaminedfor content,construct, and concurrentvalidity (Friedemann,
1991a, 1998). Internal consistencyof the
ASF-F is satisfactory,with Cronbach'salpha
coefficientsranging from .69 to .78 for the
to seeka clarification of a desiredlife process
that satisfies all members.Having defined
suchan ideal, the nurse can then work with
the family in determiningwhatcoping strategiesto useto arrive at their goal.
The family APGAR (Smilkstein, 1978)
hasalso beenused successfullyas a complementarymeasureof satisfaction.A varietyof
existing standardizedanxiety measuresand
measuresof negativeemotions,suchas anger
or depression,are recommendedto explore
the e.xistenceof personal and int~rpersonal
conflicts thatmayor may notbe family based.
Within the Frameworkof SystemicOrganization,the family processis also seenasthe
majordeterminingfactor of outcomessuchas
qualityof parenting,caregiving,or adjustment
to difficult situations.A tool to measurethe
family processat this level needsto delineate
strategieswithoutjudging their effectiveness.
Sucha tool (ASF-F [Function]) is underdevelopment by Friedemannand others but
needsrefinement.Challengesfaced in developmentof the ASF-F include the needto ensurecross-culturalrelevanceof the items and
difficulty relatedto categorizingeachactivity
subscalesand .82 for the total scale.Furthermore,respondents'scoreson the ASF-E have
beenfound to convergewith theirdescriptions
of family processdimensionsspecifiedin the
framework(Friedemann& Smith,1997).The
ASF-E hasalso beentranslatedinto threeforeign languagesand tested iri four countries
with families experiencingdifferent life and
health situations. The four targets of the
framework were clearly defined throughexploratory factor analysis in all studies.This
provides substantialevidenceof the instrument's cultural applicability. Because the
evaluationof family effectivenessis subjective, a high scorealsoimplies satisfaction.
In addition to its use in research,the
ASF-E has shown merit as a clinical tool. It
providesa basisfor generaldiscussion,theselection of a focal dimension (scored lower
th~n the others), and the detenninationof
neededchanges.The tool may alsobe usedto
facilitate discussionaboutdifferencesin perceptionsamongvarious family membersand
with a specificprocessdimension.
'
I
I
I
I
ResearchTestingthe Framework
of SystemicOrganization
Throughouther book,Friedemann(1995)
cites hundredsof studiesthat provide support
for theoretical tenets of the Framework of
Systemic Organization. In addition, many
studieshave been undertakenspecifically to
test propositions deduced from the theory.
Thereare threeissuesof concernto researchers working with this and other systemic
frameworks.First, systemicmodels defy linear causality,which is the basisof empirical
research.Second,the frameworkusesa reciprocal interactionworldview (Fawcett,1995).
Therefore,the family processis constantly
evolving. This implies that there is no objective truth of the kind that empirical research,
seeksto discover.Finally, the frameworkof
systemicorganizationstressesthe importance
of understandingdiversity,whereasmoststa-
,
~~~.
Stress,Coping,and FamilyHealth ~
i
:
,
311
tistical methods that are based on central tendency neglect the exploration of differences
from the norm.
Unfortunately, there is no research
method that circumvents these issues. Friedemann (1995) advocates between-methods triangulation to group data generated by more
than one method, thereby converging partial
truths. While using innovative approaches,in-
results by showing that families tried to maintain their family style even in the nursing
home and desired involvement that was congruent with the emphasis they placed on the
four family process dimensions. Whereas coherence was important to most and maintained through visiting, direct care was related
to an emphasis on system maintenance. Activities of learning and patient advocacy were re-
cluding qualitative methodology guided by
the framework, close attention to the sampling
procedures, sequencing of the methods, and
interpretation of the data is imperative (Floyd,
1993). A few examples of such researchexist.
Pierce (1998) conducted an ethnographic
study of African American families to examine their experience of caring and the meaning
they found in the process. The Framework
was used as a template along which emerging
themes and behaviors of caregivers were
grouped. The experience of caring involved
eight caring actions pertaining to the four process dimensions (physical work, sacrifice,
taught and shared actions, structure of caring,
communication, accommodation, mutuality,
and learning). Meaning was described by the
way the caregivers pursued and balanced the
four targets to find congruence. The meaning
of caring encompassed 13 expressions (emotional burden, evasion of conflicts, motivations concerned with love and duty, approval
of the care recipient, philosophical introspection, self-development, fairness, filial ethereal
value, self-contemplation, Christian piety, living in the moment and hoping for the future,
and purpose). The findings supported the nocion of culture in that patterns were maintained and transformed within the domains of
caring actions, family functions, and expressions of caring of these caregivers.
Similarly, Friedemann's study of family
involvement in nursing homes showed that
family functioning measured with the ASF-E
and certain items of the Family Environment
Scale (Moos & Moos, 1984) were the strongest predictor of families' expectations to be
involved (Friedemann, Montgomery, Rice, &
Farrell, 1999). A qualitative inquiry associated with the same study complemented these
lated to families' emphasis on growth and
connecting with their environment (Friedemann, Montgomery, Maiberger, & Smith,
1997).
Smith and Friedemann (1999) showed
that the framework is well suited to the development of family process models at the
midrange level in a study involving families
with members who suffered from chronic
pain. Both the ASF-E and in-depth interviews
were used to assessfamily functioning and the
role that pain plays in the family and in regulating interactive patterns, (Friedemann &
Smith, 1997). The interviews were minimally
structured, and the Framework of Systemic
Organization was used mainly for interpretation of the results. Dominant themes pointed
to the struggle of the family in finding congruence-a struggle that was played out by the
individual with pain and on the family level.
The informants with pain reported a great
need to belong and to be heard. In their family
life, this need remained unmet resulting in
distress, loneliness, and confusion. This emotional climate set the stage for ensuing family
strategies. Several processes were evident. A
cycle of obligations was evident as the individuals with pain sacrificed themselves for
others, thereby gaining charismatic power and
the ability to bind others through obligation to
serve and reciprocate. A second dynamic was
extreme closenessat the expense of individuation of the family members and the third was
family isolation from the environment. From
these phenomena, it was evident that healing
as defined by the respondents meant approaching congruence by breaking the cycle
of obligat.ion and freeing the individual from
the emotional bondage. In support of the
framework, families that reported healing en-
~\1'~t!
312 ..INTERACTIONAL
AND TRANSACTIONAL
gaged in individuation and allowing each
otherto grow. They shiftedthe emphasisfrom
the targetof controlto spiritualityandfound a
new senseof healthand happiness.The pain
was no longer the dominantforce in the family evenif it still existed.
DeMarco (1997)extendedthe framework
by applying it to staffteamsin acutecarehospita! units. Without prior theorizing, focus
groupswereusedto explorethe natureof staff
nurses'interactionalbehaviors.Resultswere
used to create items that were organizedaccording to the four processdimensionsof the
Framework of Systemic Organization and
then tested conventionally (DeMarco &
Friedemann,1995).This approachresultedin
a valid andreliableinstrument.In herdissertation, DeMarco (1997)refined the instrument
and testeda model that she explicatedusing
the Frameworkof Systemic Organizationin
which relationshipsbetweenfamily function
and workgroup function and betweenfamily
intimacyand work relationshipswerehypothesized.Significant positive correlationswere
found betweenrelationalpatternsin the family and at work. Silencingthe self in the family was related to keeping silent at work and
being compliant with expectedfeminineroles
which subsequentlyled to inner hostility.
Theseemotionswereconceptualizedasnegative coherence or lack of individuation.
Nurseswho found personalmeaningin their
work and incorporatednew knowledgeexperienced personal growth and demonstrated
positive individual coherenceor individuation
at the workplace.DeMarco'sfindings clearly
speakto the processof seekingcongruenceor
failing to do so.
MODELS
folds. The approachto practiceand research
needsto be family process-specificand,therefore,sensitiveto thefamilies' subjectivestress
appraisal. Research and practice methods
must accommodatevast differencesin reactions related to cultural, developmental,and
economicfactors that can be assessedonly
throughopen-ended,in-depthinterviewing.
Unfortunately,linear approachesto nursing care that are preferred by nursesfor the
sakeof simplicity and easeof applicationare
not congruentwith this framework.Thus, any
situationthat appearsto be easymay become
immenselycomplexwhenmultiple confounding factors are added. Nevertheless,Friedemann's(1995) bookprovidesassessment
and
interventionexamplesso thatnursescan learn
to shift their thinking from cause-and-effect
decisionmaking to a more complexsystems
approach.
Researchstudies with the framework
havethe potentialof revealingnoveltypes of
information,but the dangerof getting lost in a
complexmazeof mutually interactingforces
exists. Designsneedto maintain a fine balanceof simplicity and depthto be usefuland
interpretable.Few guidelines currently exist
for the convergence
of variousresearchmethods,and the resultsderived from suchmethods and carefullyplanneddesignsare greatly
needed.Researchwith the Frameworkof Systemic Organizationis still in the experimental stage,and its quality needsto be carefully
monitored. Nevertheless, this framework
tendsto appealto independentthinkers who
dareto take their researchefforts beyond existing parametersand experimentwith new
approachesin the searchfor newsolutions.
Critique and Summary
The DevelopmentalHealth Model
The approachto nursing practice within
the Framework of Systemic Organization
leadsaway from a narrowfocus on the causes
of distress and methods to deal with the
stressorsto a direct interventionwith the systerninfluenced by the stressorsin the context
of the entire situation.Likewise,researchuses
multiple methodsto interpretprocessas it un-
Origins and Evolution
Another family theory,the Developmental Health Model (DHM), is a theoreticalextensionand refinementof the McGill Model
of Nursing, a curriculum model first developed by Moyra Allen and faculty at the
.
I
: