A ptotic kidney with multiple arteries, one from a common renal
advertisement

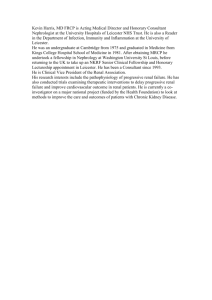
318 Asian Pacific Journal of Reproduction 2012; 1(4): 318-319 Contents lists available at ScienceDirect Asian Pacific Journal of Reproduction Journal homepage: www.elsevier.com/locate/apjr Document heading A ptotic kidney with multiple arteries, one from a common renal artery stem * Gokhan Tulunay, Isin Ureyen , Alper Karalok, Taner Turan, Nurettin Boran Etlik Zubeyde Hanim Women’s Health Reseach and Teaching Hospital, Gynecologic Oncology Division, 06010, Kecioren, Ankara, Turkey ARTICLE INFO ABSTRACT Article history: Received 3 October 2012 Received in revised form 5 October 2012 Accepted 4 December 2012 Available online 20 December 2012 Anomalies of major retroperitoneal vascular structures have been showed up in many reports so far. Here, a group of vascular anomalies of retroperitoneum were reported, all of which were encountered during the staging surgery of a 65-year-old woman with endometrium carcinoma. There was no vascular injury during the surgery associated with these vascular abnormalities. Since they are met quite frequently, it is important for surgeons dealing with retroperitoneum to be aware of the possible anomalies of vascular and renal structures in this region. Keywords: Renal artery Renal vein Vascular anomaly 1. Introduction 2. Case report Anomalies of major retroperitoneal vascular structure are not uncommon. With a prevalence of 13.6% to 30.2%, they are mostly diagnosed either during surgery or by imaging techniques since they are mostly asymptomatic[1-3]. Renal vascular anomalies are responsible for more than half of these anomalies[1]. In a study, simple renal anatomy with a solitary artery and vein was present in 72% of kidneys[4]. Renal venous anomalies are seen on the right side more commonly, since renal arterial anomalies have a predilection to left side[5,6]. Pelvic and paraaortic lymphadenectomy is an essential part of staging surgery done for most gynecological malignancies. Therefore, it is a necessity for a gynecologic oncologist to have a command of the anatomy of the retroperitoneum and to be aware of the high incidence of vascular anomalies of this region. Otherwise, hazardous complications such as nephrectomy and vascular injury requiring blood transfusion are inevitable. Here, we reported a group of anomalies of renal vessels, some of which are seen rarely. We described vascular anomalies of retroperitoneum encountered during the surgery of a 65-year-old woman with grade II endometrium carcinoma in November 2011. Since the frozen section analysis of the hysterectomy material revealed a tumor filling all the cavity and tumoral invasion more than half of the myometrium, pelvic and paraaortic lymph node dissection was performed. During dissection of retroperitoneum, vascular and renal anomalies were recognized (Figure 1). The findings are as follows: (i) The right kidney was below the level than that it should be (a ptotic kidney). (ii) There were three arteries, one for the lower pole and two for the upper pole, supplying the right kidney while two veins were draining it. (iii) One of the arteries supplying the upper pole was a branch of an artery originating from abdominal aorta at a level below inferior mesenteric artery and giving branches to both kidneys by ascending upwards. (iv) The artery supplying the lower pole was originating from the right common iliac artery. (v) Right ovarian vein was a tributary of right renal vein. (vi) There were two renal veins on the right side; one in the original place, the other one was anterior to it. (vii) All three renal arteries on the right side were overpassing the inferior vena cava (precaval renal arteries). (viii) There was no abnormality in the left side except the unusual course of the left renal artery, supplying the left kidney by ascending upwards after originating from a common renal artery stem. The left renal vein was single and coursing over the aorta as expected. There was no vascular injury during the surgery associated with these vascular abnormalities. *Corresponding author: Isin Ureyen, Etlik Zubeyde Hanim Women’s Health Reseach and Teaching Hospital, Gynecologic Oncology Division, Etlik Street, Post code: 06010, Kecioren, Ankara, Turkey. Tel: +90 312 3220180 Fax: +90 312 3238191 E-mail: isin.ureyen@gmail.com Gokhan Tulunay et al./Asian Pacific Journal of Reproduction (2012)318-319 The final pathological finding was stage IB grade 2 endometrioid adenocarcinoma. All removed 91 retroperitoneal lymph nodes, 39 of which were dissected from paraaortic region, were pathologically free of disease. Therefore, it is not erroneous to say that the vascular anomalies mentioned above did not interfere with the adequacy of the surgery. 319 of cases[7,8]. Although multiple renal vessels are usually asymptomatic, they may cause hydronephrosis, hematuria and asymptomatic proteinuria[8]. A special risk associated with multiple renal vessels is the ligation of accessory renal arteries, because these are end arteries and ligation of these arteries may cause partial ischemia, renal function loss, and renal hypertension[2,3]. In a study by Yeh et al., 35% of precaval right renal arteries arose from the anterior aspect of aorta, while 6% of these arteries arose from right common iliac artery[9]. In our case, one of the renal arteries arose from anterior aspect of aorta, one arose from the common renal artery stem originating from left side of the aorta, and one arose from right common iliac artery. In our case, the right ovarian vein was a tributary of right renal vein in spite of the vena cava. This is a rare anomaly seen in 1.3% of population[3]. Although a common renal artery stem has been defined and known for more than 130 years, it is an unusual vascular anomaly of the retroperitoneal region as can be seen in the literature[10]. To our knowledge, this is the first case in which such an anomaly was showed up during surgery. If there had been any injury to this common artery, there would be ischemia in both kidneys. It is important for surgeons dealing with retroperitoneum to be aware of the possible anomalies of vascular and renal structures in this region, since they may cause serious complications if the attention they deserve is not given. Conflict of interest statement We declare we have no conflict of interest. References Figure 1. Anomaly of major retroperitoneal vascular structure. K: Kidney; VCI: Vena cava inferior; ARRV: Anterior right renal vein; SRRA: Superior right renal artery; MRRA: Middle right renal artery; IRRA: Inferior right renal artery; CS: Common stem; LRA: Left renal artery; IMA: Inferior mesenteric artery. Written informed consent was obtained from the patient for publication of this case report and accompanying image. 3. Discussion The vascular and renal anomalies of retroperitoneum were reported in many researches and case reports. In the literature, retroperitoneal vascular anomaly rates range between 0.1% and 43% for veins and 9% and 31% for arteries[2]. This abnormal vasculature is important because of the possible increased injury to these vascular structures during retroperitoneal surgery. It was shown to be important to define these vascular anomalies in aorta-iliac surgery, renal transplantation surgery and renal nephron-sparing surgery preoperatively, while Kose et al. and Klemm et al, reported that vascular injuries were not more common in the cases with retroperitoneal vascular anomalies in a study population composed of gynecologic oncology cases[1,2]. Multiple renal vessels are a part of these vascular a nomalies. T hes e an om alies ar e d u e to v a ri o u s developmental positions of kidneys and are seen more frequently in the kidneys not ascended or rotated normally. Multiple renal veins are shown to have a prevalence of 19% and multiple renal arteries are found to be as high as 25% [1] K ose MF, Turan T, Karasu Y, Gundogdu B, Boran N, Tulunay G. Anomalies of major retroperitoneal vascular structure. Int J Gynecol Cancer 2011; 21(7): 1312-1319. [2] K lemm P, Fröber R, Köhler C, Schneider A. Vascular anomalies in the paraaortic region diagnosed by laparoscopy in patients with gynaecologic malignancies. Gynecol Oncol 2005; 96(2): 278-282. [3] Benedetti-Panici P, Maneschi F, Scambia G, Greggi S, Mancuso S. Anatomic abnormalities of the retroperitoneum encountered during aortic and pelvic lymphadenectomy. Am J ObstetGynecol 1994; 170(1 Pt 1): 111-116. [4] K ok NF, Dols LF, Hunink MG, Alwayn IP, Tran KT, Weimar W, et al. Complex vascular anatomy in live kidney donation: imaging and consequences for clinical outcome. Transplantation 2008; 85(12): 1760-1765. [5] Bordei P, Sapte E, Iliescu D. Double renal arteries originating from the aorta. Surg Radiol Anat 2004; 26(6): 474-479. [6] Janschek EC, Rothe AU, Hölzenbein TJ, Langer F, Brugger PC, Pokorny H, et al. Anatomic basis of right renal vein extension for cadaveric kidney transplantation. Urology 2004; 63(4): 660-664. [7] Koc Z, Ulusan S, Oguzkurt L, Tokmak N. Venous variants and anomalies on routine abdominal multi-detector row CT. Eur J Radiol 2007; 61(2): 267-278. [8] R anade AV, Rai R, Prahbu LV, Mangala K, Nayak SR. Arched left gonadal artery over the left renal vein associated with double left renal artery. Singapore Med J 2007; 48(12): e332-334. [9] Y eh BM, Coakley FV, Meng MV, Breiman RS, Stoller ML. Precaval right renal arteries: prevalence and morphologic associations at spiral CT. Radiology 2004; 230(2): 429-433. [10]Macalister A. Multiple renal arteries. J Anat Physiol 1883; 17(Pt 2): 250-252.