Read the full article. - Trends in Urology & Men's Health
advertisement

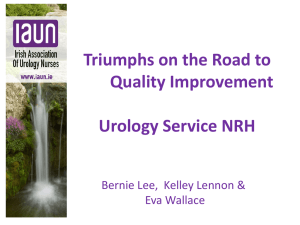
Modgil Epididymo-Orchitis_Layout 1 15/03/2012 15:01 Page 1 SEXUAL HEALTH 17 Epididymo-orchitis in primary care: is management adequate? VAIBHAV MODGIL, PAUL STURCH, TARIG ABDELRAHMAN, ANGIE RILEY, SUMIT BHADURI, CHRIS HEATH, JOSHUA PHILLIPS AND PAUL RAJJAYABUN Acute epididymo-orchitis is a common and increasing problem for GPs, which, if untreated, carries risks of significant sequelae, including infertility. Recent literature suggests widespread suboptimal management of epididymo-orchitis in secondary care, in spite of published guidelines. In this article, the authors evaluated adherence to these guidelines in primary care. cute epididymo-orchitis is a clinical diagnosis consisting of pain and swelling of the epididymis and/or testes (Figure 1). The most common route of infection is local extension from the urethra (sexually transmitted pathogens) or bladder (urinary pathogens).1 It is the fifth most common urological diagnosis in the 18–50 age range, responsible for more lost man hours in the US military than any other urological condition.2 A AETIOLOGY OF EPIDIDYMO-ORCHITIS In the UK, acute epididymo-orchitis is a common and increasing problem, with patients frequently presenting to their GP. A recent study using the NHS General Practice Research Database identified more than 12 000 patients presenting with epididymo-orchitis over a five-year period, 57 per cent of whom were treated entirely in primary care.3 TRENDS IN UROLOGY & MEN’S HEALTH MARCH/APRIL 2012 Epididymo-orchitis is predominantly an acute inflammatory process; however, if left untreated, chronic inflammation may develop, with sequelae of abscess formation, testicular infarction, testicular atrophy and infertility.4 The aetiology can be categorised largely by patient age, with a peak incidence in the third decade and 70 per cent of cases occurring between 20 and 39 years.5 In most patients aged 35 years or less, infection is sexually transmitted, with Chlamydia trachomatis isolated in approximately 85 per cent of cases, followed by Neisseria gonorrhoea.5 In spite of substantial evidence of the growing public health problem caused by untreated C. trachomatis, a recent study highlighted that secondary epididymo-orchitis is poorly managed by urologists in hospital.6 It should also be recognised that cases of epididymoorchitis related to sexually transmitted infections offer an opportunity to perform sexual health screening and contact tracing. On this background, in 2001 the National Strategy for Sexual Health and HIV encouraged a greater role for primary care physicians in the treatment of sexually transmitted infections. Figure 1. Acute epididymo-orchitis, showing inflammation of the testes. ”Dr P. Marazzi/ Science Photo Library Vaibhav Modgil, BM, MRCS, ST3 Urology, West Midlands Deanery; Paul Sturch, MB ChB, BSc, MRCS, Core Surgical Trainee, Wessex Deanery; Tarig Abdelrahman, BM, MRCS, ST3 General Surgery, Wales Deanery; Angie Riley, MB ChB, GPVTS, North West Deanery; Sumit Bhaduri, MB ChB, FRCP, Consultant in Genitourinary Medicine, Worcestershire Acute NHS Hospitals Trust; Chris Heath, MB ChB, DCH, DRCOG, MRCGP, GP, St John’s Surgery, Bromsgrove; Joshua Phillips, MD, FRCS(Urol), Consultant Urological Surgeon, Royal Bournemouth Hospital; Paul Rajjayabun, MD, FRCS(Urol), Consultant Urological Surgeon, Worcestershire Acute Hospitals NHS Trust. www.trendsinurology.com Modgil Epididymo-Orchitis_Layout 1 15/03/2012 15:01 Page 2 SEXUAL HEALTH 18 GUIDELINES FOR MANAGEMENT OF EPIDIDYMO-ORCHITIS Published guidelines from the British Association for Sexual Health and HIV (BASHH)1 and the European Association of Urology7 offer clear and specific recommendations for investigation and management of urinary/genital tract infections. Standard No. of patients (%) Nucleic acid studies on first-catch urine for chlamydia testing All patients to have midstream urine sent for enteric organisms Doxycycline or ofloxacin Duration of treatment: 14 days 2 (3) 8 (14) 13 (23) 0 Table 1. Investigation of epididymo-orchitis in 57 primary care patients Following the exclusion of testicular torsion, in suspected cases of epididymoorchitis, nucleic acid amplification testing should be used to diagnose C. trachomatis or N. gonorrhoea infection, in combination with microscopy and culture of a midstream urine sample. Opportunistic screening of patients with sexually transmitted epididymo-orchitis should be undertaken and all patients with a urinary tract pathogen should be referred for urological assessment to exclude structural abnormalities or urinary tract obstruction. Empirical treatment should include doxycycline if sexually transmitted organisms are the most likely aetiology, or ofloxacin if enteric organisms are suspected. Partner notification and treatment is recommended for all patients with epididymo-orchitis secondary to sexually transmitted organisms. STUDY TO EVALUATE ADHERENCE TO GUIDELINES The aim of this study was to evaluate adherence to established guidelines in the management of epididymo-orchitis identified in primary care. A comprehensive retrospective review of electronic records held in three primary care centres across the country was performed (Bromsgrove, West Midlands; Portsmouth, Hampshire; Oldham, Lancashire). All patients presenting with testicular or scrotal pain over a 12-month period were initially included. From this group, 57 patients (median age 26 years, www.trendsinurology.com Standard No. of patients (%) Referral to hospital for follow-up Referral to urology for follow-up Referral to genitourinary medicine 18 (31) 14 (25) 5 (8) Table 2. Follow-up care in 57 primary care patients range 15–34) with a final diagnosis of epididymo-orchitis were identified (Bromsgrove, n=23, Portsmouth, n=14, Oldham, n=20). Consultation details were reviewed, along with microbiological request/results and prescribed antibiotic regimens. Additional clinical information was extracted from case notes, including supplementary investigations, treatment and follow-up recommendations. These data were then scrutinised for adherence to published guidelines.1,7 Results of the study From the 57 patients identified, two (3 per cent) were formally investigated for chlamydia with a urethral swab or firstcatch urine, one of which tested positive (Table 1). Midstream urine samples were sent in eight cases (14 per cent); one tested positive for enteric organisms. Chlamydia studies were inappropriately requested on a midstream urine specimen in one case. Microbiological confirmation of an infective organism was achieved in only two cases (3 per cent). The most commonly prescribed antibiotic was ciprofloxacin (28 per cent). Twentythree per cent of patients were prescribed a recommended antibiotic (doxycycline or ofloxacin); however, none of the patients received treatment for 14 days (Table 1). Only 31 per cent of cases were referred onwards for secondary care assessment (25 per cent had urology follow-up arranged). In spite of clear recommendations that all patients treated for epididymoorchitis be referred to genitourinary medicine (GUM) clinics at the earliest opportunity, only 8 per cent of cases were referred, and only half of these attended (Table 2). Diagnosis of sexually transmitted infections Because of the long-term sexual health implications of chlamydia infection and the potential impact on the NHS, a national chlamydia screening programme was introduced in 2003.8 Rising public awareness of chlamydia has resulted in an increased uptake of screening.9 The cost-effectiveness of these screening programmes is yet to be proven. Young men presenting with epididymoorchitis represent an important group of patients in whom prompt treatment could reduce the adverse health for both the index case and associated sexual contacts. Unfortunately, our data suggest that TRENDS IN UROLOGY & MEN’S HEALTH MARCH/APRIL 2012 Modgil Epididymo-Orchitis_Layout 1 15/03/2012 15:01 Page 3 SEXUAL HEALTH 20 management of epididymo-orchitis in the community falls markedly short of recommended guidelines. General practitioners appear to be failing to diagnose sexually transmitted infections, including chlamydia, when faced with secondary complications such as epididymo-orchitis. Suboptimal treatment We identified suboptimal treatment regimens, including incorrect choice of antibiotic and duration of the course of treatment. This could lead to risk of residual and recurring infection with further sexual transmission. Limiting the choice of antibiotic to ofloxacin alone, which covers both sexually transmitted and enteric organisms, may help to simplify the management of epididymo-orchitis in primary and secondary care before referral to GUM services.10 REFERENCES 1. 2. 3. 4. 5. Inadequate referral Few patients in our cohort were appropriately referred on to GUM/urology clinics for review, with even smaller numbers attending their appointments. This leads to inadequate follow-up and also prevents a second chance to enable contact tracing. 6. 7. CONCLUSION Poor management of epididymo-orchitis is not isolated to healthcare in the community. A study carried out in various UK teaching hospitals confirmed that urologists remain poor at managing epididymo-orchitis in sexually active young men in secondary care.6 Our evidence suggests that collaboration between primary care, GUM teams and urologists is required to develop programmes of education and training to improve the management of this important patient group and enhance compliance with existing guidelines and recommendations. Declaration of interests: none declared. www.trendsinurology.com 8. 9. 10. British Association for Sexual Health and HIV. 2010 United Kingdom national guideline for the management of epididymo-orchitis. www.bashh.org/ guidelines Tracy CR, Costabile RA. The evaluation and treatment of acute epididymitis in a large university based population: are CDC guidelines being followed? World J Urol 2009;27:259–63. Nicholson A, Rait G, Murray-Thomas T, et al. Management of epididymo-orchitis in primary care: results from a large UK primary care database. Br J Gen Pract 2010;60:579. Garthwaite MAE, Johnson G, Lloyd S, Eardley I. The implementation of European Association of Urology guidelines in the management of acute epididymoorchitis. Ann R Coll Surg Engl 2007; 89:799–803. Drury NE, Dyer JP, Breitenfeldt N, et al. Management of acute epididymitis: are European guidelines being followed? Eur Urol 2004;46:522–5. Phillips JT, Giebaly D, Gillham T, et al. Urological management of acute epididymo-orchitis in sexually active young men: too great a public health risk? Sex Transm Infect 2010;86:328. European Association of Urology. Guidelines on the management of urinary and male genital tract infections. www.uroweb.org/fileadmin/user_ upload/Guidelines/15%20Male% 20UTI.pdf NICE. Revised rapid review of evidence for the effectiveness of screening for genital chlamydial infection in sexually active young women and men, 2006. www.nice.org.uk/nicemedia/pdf/ Chlamydia_Screening_Revised_Review_ of_Effectiveness.pdf Thomson-Glover R, Mandal D. Chlamydia screening. Trends Urol Mens Health 2011;2(1):34–7. O’Mahony C, Evans-Jones J. Urological management of epididymo-orchitis: simple, ofloxacin for all! Sex Transm Infect 2011;87:43. TRENDS IN UROLOGY & MEN’S HEALTH MARCH/APRIL 2012