Three Documentation
Tools That Work
Our progress note form, pocket guide
and quick-reference list will help you put the revised
Medicare documentation guidelines into practice.
Leigh Ann Henry
each level of exam. To further complicate matters, the number of systems and
body areas recognized by HCFA in the
exam guidelines has changed, from 19
to 14. (No, the human anatomy hasn’t
changed — just HCFA’s view of it.)
The changes mean that in addition to
Leigh Ann Henry is an
associate editor of Family
Practice Management.
Reproduced with permission
from Family Practice Management.
Copyright© by the American Acdemy of
Family Physicians. All rights reserved.
Downloaded from the Family Practice Management Web site at www.aafp.org/fpm. Copyright © 2003 American Academy of
Family Physicians. For the private, noncommercial use of one individual user of the Web site. All other rights reserved.
SUZETTE BAR BIER
A
s we’ve explained in
our last two issues, the
revised Medicare documentation guidelines
from HCFA necessitate
significant changes in
the way you document exams. The Jan.
1 enforcement date has been postponed,
however.
At press time, HCFA has granted
a request from the AMA to extend
the grace period by six months, to July
1. The random, prepayment medical
reviews of E/M codes that HCFA has
planned will use both the original guidelines and the revised guidelines until that
date. As many as 3 percent of E/M claims
may be subject to review.
Briefly, here’s how the guidelines
for exam documentation have changed:
Under the original guidelines, the level
of exam depended on the number
of organ systems and body areas you
examined and documented in the medical record. The revised guidelines go
much farther, identifying the clinical
elements that constitute comprehensive
multisystem and single-organ-system
exams and establishing precisely how
many of those elements must be performed and documented to substantiate
SPEEDBAR ®
HCFAhasextended
the grace period for
implementation of
the revised guidelines to July 1.
With the revised
guidelines, documenting exams
has become much
more complicated.
A progress note
form that includes
checklists of systems and body
areas can help
to relieve at least
some of the exam
documentation
burden.
Negative
responses on the
ROS and negative
findings on the
exam that are relevant to the presenting problem must
be documented.
CC:
counting the
HPI:
systems and body
areas you examine, now
you must also count the number
of clinical elements you perform and
document for each of those systems and
body areas.
Yes, the revised guidelines are confusing, but time, practice and, we hope,
our articles on the subject will help you
to make sense of them. Here we offer
three tools designed to help you implement the guidelines.
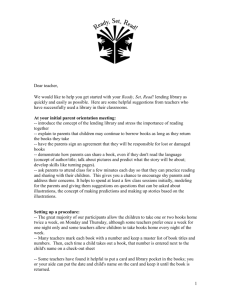
1. The progress note form
The first tool is a revised version of a
form that we first published in 1995,
when the original documentation guidelines were introduced. The checklist is
designed to make it easier to count systems and body areas. We’ve revised the
list of systems and body areas to match
those that HCFA now recognizes for the
general multisystem exam, and we’ve
done some rearranging to allow more
room for the note. To count clinical elements (referred to as “bulleted elements”
in the guidelines), you’ll have to work
through your note.
To use the checklist, put a check
mark in the appropriate column for every
system you cover in the ROS, every area
of the PFSH you touch on and every
system or body area you examine. In circumstances where you would normally
write, for example, “GI normal” with no
further elaboration, a check mark in the
“nl” column should suffice. Remember
that the guidelines still require that you
note explicitly any negative responses on
the ROS and negative findings on the
exam that are relevant to the presenting
problem.
You should be able to quickly determine the number of systems covered
in the ROS and the number of areas
covered in the PFSH by counting the
check marks in those sections of the
form. Before you can determine the level
of history, you’ll also need to count the
elements of the HPI that appear in the
note. The elements of the HPI are listed
on the form to help you remember what
to look for. (Note that the HPI has a new
3 0 ■ F A M I LY P R AC T ICE MANAGEMENT / January 1998
element now, too:
“status
of chronic
diseases.” It’s
important to track
how many such diseases
you ask about.)
To determine the level of
exam, you’ll be able to count the
number of systems and body areas
by counting check marks. Then you’ll
need to compare your note with the
We’ve done some
rearranging to allow
more room for the note.
exam chart developed by HCFA and the
AMA and count the number of clinical
elements in the note. (The pocket guide
and quick-reference list discussed later
in this article both include a version of
the general multisystem exam chart. For
additional resources, see page 32.)
Note that the form provides no
checklist for documenting medical decision making; to assess that, you’ll need to
refer to your note.
Like the original, this form also
provides a shortcut for documenting
encounters dominated by counseling or
coordination of care. Simply check the
box labeled “Couns/coord > 50%” (i.e.,
“Counseling and/or coordination of care
took more than 50 percent of the visit”),
enter the total time (face-to-face or floor
time, as appropriate) of the encounter
and the time devoted to counseling and/
or coordination of care, and describe in
the note the counseling and/or activities
to coordinate care that you provided.
2. The pocket guide
You’ll find a revised version of our original “Pocket Guide to the Documentation
Name: _________________________________________________________________________________________
DOB: _____________________
H: ______
W: ______
T: ______
P: ______
BP: ______
R: ______
Nurse’s Note:_____________________________________________________________
HPI
Location, quality, severity,
duration, timing, context,
modifying factors, associated
signs and symptoms OR status
of chronic diseases.
ROS
nl
See
note
Const
❏
❏
Eyes
❏
❏
ENT/mouth
❏
❏
CV
❏
❏
Resp
❏
❏
GI
❏
❏
GU
❏
❏
Musc
❏
❏
Skin/breasts
❏
❏
Neuro
❏
❏
Psych
❏
❏
Endo
❏
❏
Hem/lymph
❏
❏
Allerg/immun
❏
❏
No
chng
See
note
PFSH
Date: _____________________
Past
❏
❏
Family
❏
❏
Social
❏
❏
Exam
nl
See
note
Const
❏
❏
Eyes
❏
❏
ENT/mouth
❏
❏
Neck
❏
❏
Resp
❏
❏
CV
❏
❏
Chest (breasts)
❏
❏
GI (abdomen)
❏
❏
Lymph
❏
❏
GU
❏
❏
Musc
❏
❏
Skin
❏
❏
Neuro
❏
❏
Psych
❏
❏
___________________ ______
No ✔: no review/exam
Couns/coord > 50% ❏
Total time: _________ min.
Physician’s Signature: ____________________________________________________________
Couns/coord time: _________ min.
Copyright © 1995, 1998 American Academy of Family Physicians. Physicians may photocopy for use in their own patients’ charts; all other rights reserved.
SPEEDBAR ®
The FPM Pocket
Guide is a useful
memory aid, not a
substitute for thorough reading and
assimilation of the
guidelines.
Once you
understand the
new guidelines, the
pocket guide can
help you work from
your note to the
appropriate code.
Guidelines” facing page 89. Before you
continue reading this article, you may
want to remove the pocket guide along
the perforation, cut out the shaded areas
and fold the guide as indicated in the
instructions.
With the pocket guide folded correctly, the front should show the two
Code selection tables at the top with a
History table below. The words Exam
and Decision making should be showing above the history table, each next to
the head of a broad gray arrow. The gray
arrow in the History table indicates that
the History table contributes information
to the History column of the code selection tables. Open the first flap and on
the right you should see an Exam table
with a gray arrow indicating its relationship to the Exam column of the Code
selection tables. Lift up the small flap
carrying the exam table and you should
see a two-column table that lists the clinical content of the comprehensive gen-
eral multisystem exam as it’s defined in
the new documentation guidelines. (We
chose to include the general multisystem
exam because of its prevalence in family medicine.) Close the small flap, open
the third flap, and you should see three
tables that contribute information to the
Decision making table and a gray arrow
indicating the relationship of decision
making to the Code selection tables.
Keep in mind that the pocket guide is
designed to jog your memory, not to teach
you everything you need to know about
the guidelines. To consult the unabridged
version of the tables or the requirements
for single-system exams, you’ll need to
refer to the guidelines themselves.
While the checklist form described
earlier is designed to help you as you write
or dictate your note, the pocket guide
is intended to help you determine the
appropriate code, based on what you have
documented in the note. You might want
to consult the pocket guide before coding
Educational resources
The pocket
guide is perhaps
most useful as a
self-audit tool and
a way of fine tuning
your seat-of-thepants coding.
Use the table of
exam requirements
on the pocket guide
to assess the systems and bulleted
elements covered
in your note.
T
o obtain the revised guidelines or the earlier articles in our series on exam documentation, see the instructions below. As this issue goes to press, the Academy is also accepting orders for the second edition of “Mastering Medicare’s
Documentation Guidelines,” the FPM publication designed to help you understand
the guidelines and improve your coding. The second edition has been revised to
make it easier to use. It includes up-to-date information about documenting history,
exam and medical decision making as well as the tools included in this article.
To obtain“Mastering Medicare’s Documentation Guidelines,”which includes the
pocket guide, or to obtain single copies of the pocket guide: Call the AAFP order
department (800-944-0000) and ask for item number 574 (“Mastering Medicare’s
Documentation Guidelines” with the pocket guide) or item number 557 (single copies of the pocket guide). At press time, pricing had not yet been determined.
To obtain back issues of FPM: Call the AAFP order department (800-944-0000),
ask for item number 539 and specify the date for the issue you want to purchase
(“Exam Documentation Just Got Harder,”October 1997,focuses on the guidelines for
multisystem exams;“More HelpWith Exam Documentation,”November/December
1997, explains the guidelines for single-system exams). The cost is $5 an issue in the
United States, $7 in Canada and elsewhere.
To obtain the documentation guidelines themselves: Call theAAFP order department (800-944-0000) and ask for item number 736.The price, which covers shipping
and handling, is $3. Copies of the guidelines are also available from Medicare carriers
and via the HCFA web site (http://www.hcfa.gov/medicare/ mcarpti.htm).
3 2 ■ F A M I LY P R AC T ICE MANAGEMENT / January 1998
a visit, but you’ll probably find it more
useful as a way of fine-tuning your “seat of
the pants” coding. If you use it to help you
in a self-audit from time to time, checking
the codes you’ve submitted for selected
visits, you can identify areas where you
may be coding too high or too low.
Let’s use the pocket guide to evaluate the following sample note, which
represents a common type of Medicare
visit — the routine follow-up visit for a
patient with multiple chronic problems
and no new complaints:
S: Mr. Doe returns today for a routine
four-month F/U for evaluation and
management of his NIDDM, hypertension and OA. No new complaints.
He denies headache, visual changes,
chest pain, SOB or extremity numbness. No increased joint pain. Dietary
compliance good, and his BP and
home glucose monitoring records indicate acceptable control of both.
O:CONST: BP 138/84, Wt 175, P 82
and regular.
HEENT: PERRLA, EOMI; EACs and
TMs nl; oropharynx benign.
NECK: supple w/o JVD, bruits or
thyromegaly.
RESP: bs clr to P and A w/o retractions or rubs.
HEART: WNL w/o gallop, murmur,
rub, click or irregularity.
EXT: distal pulses intact w/o cyanosis,
clubbing or edema.
NEURO: deep tendon reflexes WNL
and symmetric; no decreased lower
extremity sensation noted.
LABS: FBS 132, UA WNL.
A: 1. Stable NIDDM
2. Stable hypertension
3. Stable osteoarthritis
P: 1. Glucotrol 5 mg daily q.a.m.
2. Procardia XL 30 mg daily.
3. Relafen 1,000 mg daily.
4. Continue home glucose monitoring.
5. SMA-7 and glycosylated hemoglobin today.
6. RTC for routine F/U in 4 months.
If you’ve read the other two articles
in this series, you ought to be able to use
the pocket guide to evaluate this note
and come up with a suggested coding
level. Before we go on, you might want
to re-read the note and decide how to
code it without consulting the pocket
guide or the guidelines, then read on to
compare your analysis with ours.
History: The History table on the
front of the pocket guide doesn’t include
a column for chief complaint, since that
is required for all levels of history and
not likely to be missing from any progress note. Even though the patient in our
example has no new complaints, there
is a chief complaint in the first sentence
of the note. The guidelines define chief
complaint very broadly as a statement
“describing the symptom, problem,
condition, diagnosis, physician-recommended return or other factor that is
the reason for the encounter” (emphasis
added).
Determining how to score the HPI
in this note would have been difficult
under the original guidelines, since the
patient has no new complaints to characterize. Now that HCFA has redefined the
extended HPI as four or more elements
of the HPI or the status of three or more
chronic conditions, the HPI score is clear.
Because the patient is returning for a routine evaluation of three chronic diseases
— diabetes, hypertension and osteoarthritis — the HPI is extended.
Documentation Tools
The pocket guide is designed
to jog your memory, not to teach
you everything you need to
know about the guidelines.
The ROS includes questions about
at least six systems and body areas: eyes,
cardiovascular, respiratory, musculoskeletal, neurologic and endocrine. The History table of the pocket guide, then, tells
us that the ROS is detailed.
Because the note doesn’t really touch
on past, family or social history, there is
no PFSH. Consequently, although the
HPI and ROS seem to point to a detailed
January 1998 / FAMILY PRACTICE MANAGEMENT ■ 35
history, the actual level is limited to
expanded problem focused. As the History table indicates, expanded problem
focused is the highest level possible without a PFSH. Note that simply reviewing
the patient’s medication list and documenting that fact in the note would have
counted as past history, therefore raising
the PFSH to detailed and, therefore, the
overall level of history to detailed.
Exam: Opening the first flap of the
pocket guide exposes on the right the
table devoted to the exam, and on the
back of the small flap is the table that
lists the clinical content of the comprehensive general multisystem exam. The
sample note documents findings for
eight systems and body areas, which, as
the table indicates, meets the requirement for a detailed exam, provided that
at least 12 bulleted elements are documented in the note.
Here’s how the note and the bulleted elements in the general multisystem exam table match up:
• Constitutional: Measurement of
any three of the following seven vital
signs ... (“BP 138/84, Wt 175, P 82 and
regular”);
• Eyes: Examination of pupils and
irises (HEENT: “PERRLA, EOMI”);
• ENT/mouth: Examination of oropharynx (HEENT: “throat clr, oropharynx benign w/o pallor”);
• ENT/mouth: Otoscopic
examination of external auditory canals and tympanic membranes (HEENT: “EACs and
TMs nl”);
• Neck: Examination of
neck (NECK: “supple w/o JVD,
bruits or thyromegaly”);
• N e c k : E x a m i n ation of thyroid (NECK:
“ s u p p l e w / o J V D, b r u i t s o r
thyromegaly”);
• Respiratory: Assessment of respiratory effort (RESP: “bs clr to P and A w/o
retractions or rubs”);
• Respiratory: Auscultation of lungs
(RESP: “bs clr to P and A w/o retractions
or rubs”);
• Respiratory: Percussion of chest
(RESP: “bs clr to P and A w/o retractions
or rubs”);
• Cardiovascular: Auscultation of
heart with notation of abnormal sounds
and murmurs (HEART: “WNL w/o gallop, murmur, rub, click or irregularity”);
• Cardiovascular: Examination of
pedal pulses (EXT: “distal pulses intact
w/o cyanosis, clubbing or edema”);
• Cardiovascular: Examination of
extremities for edema and/or varicosities
(EXT: “distal pulses intact w/o cyanosis,
clubbing or edema”);
• Musculoskeletal: Inspection and/or
palpation of digits and nails (EXT: “distal
pulses intact w/o cyanosis, clubbing or
edema”);
• Neurologic: Examination of deep
tendon reflexes with notation of pathological reflexes (NEURO: “deep tendon
reflexes WNL and symmetric”);
• Neurologic: Examination of sensation (NEURO: “no decreased lower
extremity sensation noted”).
In addition to noting the exam of
eight systems and body areas, the sample
note documents a total of 15 bulleted elements, clearly making the exam detailed.
Medical decision making: Because
the history and the exam differ in level
and this is an established-patient visit,
the level of medical decision making will
determine the level of the visit. As the
Code selection tables indicate, the level
of the visit is determined by the highest two of the three components. Open
Medicare isn’t the only entity
with a reason to be interested in
your documentation habits.
3 6 ■ F A M I LY P R AC T ICE MANAGEMENT / January 1998
the pocket guide fully, and we’ll use the
decision making tables to evaluate the
note.
First, the score for number of diagnoses and management options involved
works out to be 3: No new problems are
reported, and each established, previously
diagnosed problem (diabetes, hypertension and osteoarthritis) counts for one
point because they’re all stable. Second,
in evaluating the amount and complex-
ity of data to be reviewed, we have only
lab tests to consider. That gives a score
of 1 (the guidelines say no matter how
many tests of a given class are requested
or reviewed, the note earns no more than
one point per class). Finally, the level of
risk seems to be moderate, both because
the visit involves prescription drug therapy and because it concerns three stable chronic illnesses. Because the level
of decision making is determined by the
highest two of the three components, the
level for this encounter is moderate complexity.
To review, then, we have an expanded problem-focused history, a detailed
exam and moderately complex decision
making to evaluate on the Code selection table at the top of the pocket guide;
because two of the three are enough to
determine the level for an establishedpatient visit, we end up with a code of
99214.
The new guidelines for documenting exams make coding E/M visits even
more complicated than before. However,
the specificity of the exam guidelines
helps to remove at least some of the
uncertainty from the coding process. The
pocket guide should help you to code
with greater confidence that the documentation in your notes justifies the
level of service.
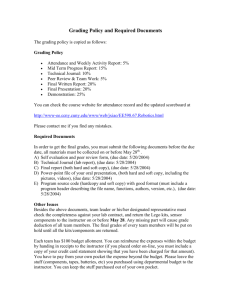
3. The quick-reference list
The third tool we developed is really an
abbreviated version of the pocket guide,
designed simply to help familiarize you
with the revised guidelines for multisystem exams. You’ll want to duplicate
it, preferably on card stock, to make it
easier to handle. The quick-reference
list reproduces from the pocket guide
the exam table and the list of clinical
elements that comprise the general multisystem exam, providing you with an
easy way to consult the guidelines as you
write or dictate your note.
Good luck
The revised documentation guidelines,
albeit anxiety provoking, can be a useful tool for evaluating your documentation. If you’re thinking, “Why bother?”
remember that Medicare will be review-
Documentation Tools
Quick-Reference List:
The General Multisystem Exam
Content and Documentation Requirements
Systems/
Areas
Bulleted
elements
PF
1+
1-5
EPF
1+
6-11
D
2+
12+
C
9+
18+
Note: For the comprehensive exam, all
bulleted elements must be performed.
Constitutional
• Any three vital signs
• General appearance of patient
Eyes
• INSP of conjunctivae & lids
• EX of pupils & irises
• Ophthalmoscopic EX of optic discs
& posterior segments
Ears, Nose, Mouth & Throat
• External INSP of ears & nose
• Otoscopic EX of external auditory canals &
tympanic membranes
• ASSMT of hearing
• INSP of nasal mucosa, septum
& turbinates
• INSP of lips, teeth & gums
• EX of oropharynx: oral mucosa,
salivary glands, hard & soft palates, tongue,
tonsils & posterior pharynx
Neck
• EX of neck
• EX of thyroid
Respiratory
• ASSMT of respiratory effort
• Percussion of chest
• PALP of chest
• Auscultation of lungs
Cardiovascular
• PALP of heart
• Auscultation of heart with notation of
abnormal sounds & murmurs
EX of:
• carotid arteries
• abdominal aorta
• femoral arteries
• pedal pulses
• extremities for edema &/or
varicosities
Chest (Breasts)
• INSP of breasts
• PALP of breasts & axillae
Gastrointestinal (Abdomen)
• EX of abdomen with notation of
presence of masses or tenderness
• EX of liver & spleen
• EX for presence or absence of hernia
Gastrointestinal (Abdomen) (continued)
• EX of anus, perineum & rectum,
including sphincter tone, presence of hemorrhoids, rectal masses
• Obtain stool sample for occult blood test
when indicated
Genitourinary
Male:
• EX of the scrotal contents
• EX of the penis
• Digital rectal EX of prostate gland
Female:
Pelvic EX, including:
• External genitalia & vagina
• Urethra (masses, tenderness, scarring)
• Bladder
• Cervix
• Uterus
• Adnexa/parametria
Lymphatic
PALP of lymph nodes in two or more areas:
• Neck
• Axillae
• Groin
• Other
Musculoskeletal
• EX of gait & station
• INSP &/or PALP of digits & nails
EX of joint(s), bone(s) & muscle(s) of one or
more of the following six areas: 1) head &
neck; 2) spine, ribs & pelvis; 3) right upper
extremity; 4) left upper extremity; 5) right
lowerextremity;&6)leftlowerextremity.The
EX of a given area includes:
• INSP &/or PALP with notation of
presence of any misalignment,
asymmetry, crepitation, defects,
tenderness, masses, effusions
• ASSMT of range of motion with
notation of any pain, crepitation or
contracture
• ASSMT of stability with notation of any
dislocation, subluxation or laxity
• ASSMT of muscle strength & tone with
notation of any atrophy or abnormal
movements
Skin
• INSP of skin & subcutaneous tissue
• PALP of skin & subcutaneous tissue
Neurologic
• Test cranial nerves with notation of any
deficits
• EX of deep tendon reflexes with
notation of pathological reflexes
• EX of sensation
Psychiatric
• Description of patient’s judgment & insight
Brief ASSMT of mental status, including:
• orientation to time, place & person
• recent & remote memory
• mood & affect
Copyright © 1998 American Academy of Family
Physicians.
January 1998 / FAMILY PRACTICE MANAGEMENT ■ 41