The surgical anatomy of the scalp
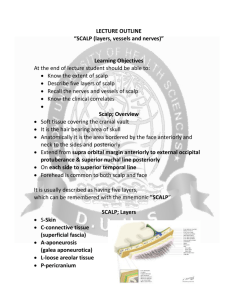
advertisement

REVIEW The surgical anatomy of the scalp of the scalp lie in this layer (see below) and the scalp has, indeed, the richest blood supply of any area of the skin in the body. When the scalp is lacerated, the divided vessels retract between the fibrous septa and therefore cannot be picked up by artery forceps in the usual way e precious time will be wasted if you try to do so. Two techniques are employed to stem the bleeding that results from lacerations to the scalp; the surgeon or his assistant presses firmly down on the underlying skull with his fingers, thus compressing the spurting vessels, or he places a series of artery forceps on the underlying third, aponeurotic, layer and flips them backwards on either side of the wound, again compressing the vessels. In closing the wound, the surgeon sutures the laceration firmly in two layers e aponeurosis and skin. A consequence of this excellent blood supply is that a flap of scalp with even a narrow pedicle has a high chance of survival compared with a similar cutaneous flap elsewhere. Aponeurosis e this fibrous sheet is found over much of the vertex of the skull, where it connects the occipitalis muscle posteriorly, (arising from the superior nuchal line), to the frontalis muscle, which inserts into the dermis of the skin in the region of the eyebrows and bridge of the nose. Laterally, the aponeurosis extends as a thin sheet overlying the temporalis fascia and becomes indistinct over the zygomatic arch. Loose connective tissue e this thin layer accounts for the mobility of the scalp on the underlying skull. It is in this layer that: the surgeon is able to mobilize a scalp flap machinery which has caught the hair may avulse the scalp Native Americans once ‘scalped’ their victims As noted above, an extensive torn flap of scalp, because of its superb blood supply, may well survive, where a similar flap elsewhere would be non-viable. Blood which collects in this loose connective tissue layer tracks freely under the scalp, but cannot pass into the occipital or temporal regions because of the posterior attachment of occipito-frontalis and the lateral attachment of the temporalis fascia. It therefore tracks forwards and accounts for the bilateral orbital haematomas that develops rapidly after a skull fracture or a cranial operation. Periosteum e this adheres to the suture lines of the skull, in the scalp region these are the coronal, saggital, temporal and lambdoid sutures. A collection of blood beneath this layer will therefore outline the affected bone. This is seen especially in birth injuries affecting the skull, (cephalohaematoma). Harold Ellis Vishy Mahadevan Abstract The scalp denotes the soft tissue that covers the cranial vault. It is a multilayered structure with a good blood supply and a rich cutaneous innervation. Scalp injuries including accidental lacerations are commonly encountered clinical problems in A & E departments. A proper understanding of the anatomy of the scalp is required for the appropriate management of such injuries, as it is for the design of craniectomies in neurosurgical practice. Full-thickness scalp flaps are frequently used in reconstructive surgery to provide soft tissue cover for facial defects. A proper appreciation of the blood supply and innervation of the scalp is a prerequisite to the design of such flaps. Keywords Cranial vault; occipito-frontalis and aponeurosis; pericranium; sebaceous cysts A good knowledge of the anatomy of the scalp and its layers is essential for a clear understanding of the management of injuries and pathologies in this region. The scalp denotes the soft tissues which cover the cranial vault. It extends from the eyebrows covering the supra-ciliary line of the frontal bone anteriorly to the superior nuchal line posteriorly. The latter is a low ridge which extends on either side from the midline external occipital protuberance of the occipital bone to the corresponding mastoid process. Laterally the scalp extends down to the level of the zygomatic arch and the external auditory meatus (Figure 1). The layers of the scalp The scalp is made up of five tissue layers, which can be remembered by the convenient mnemonic SCALP (Figure 2). The skin e is thick, variably hair-bearing and is the area of skin most richly endowed with sebaceous glands, hence its greasy feel. In consequence of this concentration of sebaceous glands, the scalp is the commonest site for sebaceous cysts, which are often multiple. Connective tissue e this is made up of fat lobules bound in tough fibrous septa. The principal blood vessels and nerves Blood supply Each side of the scalp is supplied by a total of five arteries (Figure 3). From the external carotid artery derive: occipital, whose pulse can usually be felt careful palpation above the superior nuchal line posterior auricular superficial temporal, whose pulse can be felt over the zygomatic arch immediately in front of the tragus of the ear From the internal carotid artery derive: the supraorbital artery the more medial supratrochlear artery Harold Ellis CBE MCh FRCS was Professor of Surgery at Westminster Medical School until 1989, Since then he has taught anatomy, first in Cambridge and now at Guy’s Hospital, London, UK. Conflicts of interest: none declared. Vishy Mahadevan MBBS PhD FRCS is Barbers’ Company Professor of Anatomy at the Royal College of Surgeons of England, London, UK. Conflicts of interest: none declared. SURGERY 32:S1 e1 Ó 2013 Published by Elsevier Ltd. REVIEW Epicranial aponeurosis Auricularis anterior Occipitofrontalis, frontal belly Orbicularis oculi, palpebral part Auricularis superior Depressor supercilii Occipitofrontalis, occipital belly Procerus Orbicularis oculi, orbital part Auricularis posterior Levator labii superioris alaeque nasi Nasalis Sternocleidomastoid Levator labii superioris Semispinalis capitis Zygomaticus minor Orbicularis oris Splenius capitis Zygomaticus major Orbicularis oris Trapezius Depressor labii inferioris Cervical fascia, investing layer (superficial layer) Mentalis Depressor anguli oris Parotid fascia Platysma Risorius Figure 1 Left lateral view of head showing layers of scalp. From the ophthalmic V0 e the supratrochlear and supraorbital nerves. From the maxillary V00 e the zygomaticotemporal nerve. From the mandibular V000 e the auriculotemporal nerve. The lesser occipital nerve (C2). The greater occipital nerve (C2, 3). The third occipital nerve (C3). Both of these derive from the ophthalmic artery. All these vessels are accompanied by their corresponding veins. Owing to the rich anastomoses between these vessels, the viability of the scalp may be retained when only one artery survives a major scalp avulsion. Sensory innervation (Figure 4) The cutaneous nerve supply of the scalp is derived from all three diversions of the trigeminal (V) nerve and from the second and third cervical nerves: The skull vault This comprises the frontal, parietal, occipital and squamous part of the temporal bone (Figure 5). The layers of the scalp and skull Blood vessel Hair Skin Connective tissue Aponeurosis Loose areolar tissue Periosteum Diploë of skull Dura Source: Ellis H. Clinical anatomy. 10th edition. Oxford: Blackwell Science, 2002. Reproduced with permission. Figure 2 SURGERY 32:S1 e2 Ó 2013 Published by Elsevier Ltd. REVIEW Zygomaticotemporal artery and vein Zygomaticofacial artery and vein Supratrochlear artery and vein Transverse facial artery and vein Supra-orbital artery and vein Superficial temporal artery and vein Angular artery and vein Occipital artery and vein Lateral nasal artery and vein Posterior auricular vein Superior labial artery and vein Posterior auricular artery Occipital vein Occipital artery Inferior labial artery and vein External jugular vein Facial artery Internal jugular vein Facial vein External carotid artery Figure 3 Left lateral view of head showing blood supply of scalp. SURGERY 32:S1 e3 Ó 2013 Published by Elsevier Ltd. REVIEW Ophthalmic nerve [v1] Greater occipital (C2 dorsal ramus) Zygomaticotemporal nerves Supratrochlear nerve Supraorbital nerve Auriculotemporal nerve Infratrochlear nerve Maxillary nerve [v2] Greater occipital nerve External nasal nerve C3 dorsal ramus Infraorbital nerve Lesser occipital nerve Zygomaticofacial nerve Lesser occipital and greater auricular C4 dorsal ramus Mental nerve Greater auricular nerve Buccal nerve Transverse cervical nerve Mandibular nerve [v3] Transverse cervical Figure 4 Left lateral view of head showing cutaneous innervation of scalp. Coronal suture Parietal bone Frontal bone Pterion Superior and inferior temporal lines Greater wing of sphenoid bone Squamous part of temporal bone Nasal bone Lacrimal bone Lambdoid suture Zygomatic bone Occipital bone Maxilla Mastoid process Mandible Tympanic part of temporal bone Figure 5 Bones of the cranial vault. SURGERY 32:S1 e4 Ó 2013 Published by Elsevier Ltd. REVIEW The skull vault has an adherent outer periosteal layer, or pericranium, and an inner endocranial layer. The latter is firmly fused with the dura mater (the outermost of the three meningeal layers). These two adherent layers are separated by the sagittal and the lateral venous sinuses. The periosteal and endocranial layers meet at the suture lines between the individual bones. The medullary cavities of the vault bones (the diploe) contain red bone marrow and are not uncommon sites of deposits of SURGERY 32:S1 secondary tumours and are often involved in multiple myelomatosis. The blood vessels which supply the meninges, of which the largest are the middle meningeal artery and vein, groove the inner aspect of the skull vault and lie between the bone and the dura. In addition to supplying the meninges, these vessels also supply the overlying bone and the diploe. A e5 Ó 2013 Published by Elsevier Ltd.