Systematic review with meta-analysis of the
advertisement

Systematic review with meta-analysis of the
epidemiological evidence relating smoking to COPD,
chronic bronchitis and emphysema
Barbara A Forey, Alison J Thornton and Peter N Lee
Additional File 2 : Studies
-1-
Contents
Systematic review with meta-analysis of the epidemiological evidence relating
smoking to COPD, chronic bronchitis and emphysema ................................................ 1
Table 1
The 218 studies ...................................................................................... 4
Table 2
Overlapping and linked studies .............................................................. 8
Table 3
Study characteristics ............................................................................ 11
Table 3 (continued – COPD studies) ....................................................................... 14
Table 3 (continued – CB studies)............................................................................. 19
Table 3 (continued – Emphysema studies) .............................................................. 23
Table 4
Study populations and exclusions ........................................................ 26
Table 5
Disease outcomes - summary.............................................................. 34
Table 6
Disease outcomes – detailed ................................................................ 37
Table 6A : COPD based on ICD .............................................................................. 37
Table 6B : COPD based on LF (lung function) only ............................................... 38
Table 6C : COPD based on LF and symptoms ........................................................ 40
Table 6D : COPD not further defined ...................................................................... 41
Table 6E : COPD defined as COPD, CB or Emphysema ........................................ 41
Table 6F : COPD defined as CB or Emphysema ..................................................... 42
Table 6G : COPD defined as CB, Emphysema or AST .......................................... 42
Table 6H : COPD other............................................................................................ 43
Table 6I : CB based on ICD ..................................................................................... 44
Table 6J : CB based on diagnosis ............................................................................ 44
Table 6K : CB based on self-report ......................................................................... 45
Table 6L : CB based on symptoms .......................................................................... 45
-2-
Table 6M : CB other ................................................................................................ 48
Table 6N : Emphysema based on ICD ..................................................................... 49
Table 6O : Emphysema based on visual comparison .............................................. 50
Table 6P : Emphysema based on diagnosis ............................................................. 50
Table 6Q : Emphysema based on self-report ........................................................... 51
Table 6R : Emphysema other ................................................................................... 51
Grading systems used throughout Table 6: .............................................................. 52
References – see main paper
-3-
Table 1
The 218 studies
REF
Brief description of study
Original study name
ALDERS
ALESSA
AMIGO
ANDER1
ANDER2
ANDER3
AUERBA
BANG
BECK1
BECK2
BEDNAR
BEST
BJORNS
BROGGE
BROWN
CERVER
CHAPMA
CHEN1
CHEN2
CHEN3
CHENG
CLEMEN
COATES
COCCI
COLLEG
DEAN1
DEAN2
DEANE
DEJONG
DEMARC
DETORR
DICKIN
DOLL1
DOLL2
DONTA1
DONTA2
DOPICO
EHRLIC
English hospital inpatient CC 1977-82
Roman outpatients CC 1992-93
Santiago clinic CC 2001-03
British Columbian (Chilliwack) CS 1963
Florida autopsy CS study ca 1964?
Southern Polish plasma sample CC ca 1997?
New Jersey/New York CS autopsy study 1963-70
HHANES US hispanic CS 1982-84
Lebanon US baseline CS 1972
Lebanon US follow-up PS 1972-78
Warsaw sleep apnea CS 2000-2002
Canadian veteran PS 1955-62
Swedish ECRHS young adults 1990
Bergen hospital+cohort CC 2003
Birmingham elderly men CS 1956
Italian ISAYA young adult CS 1998-2000
Utah sulfur oxide exposed parents CS 1976
Shanghai factory PS 1972-1993
Canadian NPHS middle-aged CS 1994/5
Canadian (CCHS) CS 2000-1
China (Beijing, Hubei, Liaoning) CS 1992
Belgian Airmen PS 1960-75
Detroit middle-aged post office employees CS 1962
Italian (Pisa?) hospital patients CC ca 2000?
UK GP patients CS ca 1960?
Cleveland mortality risk factors CC 1969-1973
UK (GB) adults CS 1972
California telephone co employees CS 1963
Kalamazoo COPD screening/intervention CS ca 2003?
Multi-country (ECRHS) young adults CS 1991-93
Spain high-risk smoker screening CS 2001-03
Barton elderly patients CS ca 1997?
UK male doctors PS 1951-91
UK female doctors PS 1951-73
Cretan male villagers CS baseline 1960
Cretan male villagers PS 1960-70
Minnesota/Wisconsin grain handlers CS ca 1982?
S African household CS 1998
EKBERG
ENRIGH
ENSTRO
FERRI1
FERRI2
FERRI3
FIDAN
FINKLE
FLETCH
FORAST
FOXMAN
FUKUCH
GEIJER
GODTFR
Malmo cardiovascular risk baseline 1974-1992
US Cardiovascular Health elderly CS 1989-90
Californian households (CPS I) PS 1960-98
Berlin (US) air pollution CS 1961
Berlin (US) air pollution CS 1967
Berlin (US) air pollution CS 1973
Izmir coffeehouse workers CS 2000-1
Chicago military recruits CS 1969-70
UK middle-aged post office workers CS 1956-7
Sonoma female occupational CS 1993-4
US HIE adults CS ca 1981?
Japanese (NICE) CS 2000
IJsselstein PS 1998-2003
Copenhagen and Glostrup CCHS/GPS/CMS PS 1964-97
GOLDBE
GULSVI
HAENSZ
HAMMO2
HARDIE
HARIKK
HARRIS
HAWTHO
HAYES
HEDMAN
HIGGI2
HIGGI3
HIGGI4
HIGGI6
HIRAYA
New York parents CS 1970
Oslo two-phase CS 1972-74
Norwegian population/sibling adults CS 1964
US households (CPS I) PS 1959-65
Bergen elderly CS 1998-99
Baltimore long-term adults PS 1962-ca 2000?
Nigerian soldiers CS ca 1992?
Paisley/Tiree/Renfrew male occupational PS 1965-77
US Rocky Mountains parents CS 1970
Southern Finland asthma/aspirin CS 1996
UK Vale of Glamorgan adults CS 1956
UK Annandale middle-aged adults CS 1956
Tecumseh PS 1962-87
Tecumseh CS 1962-65
Japanese adults PS 1965-82
Chilliwack Respiratory Survey
New Jersey Lung study
HHANES
Canadian Veterans
ECRHS, first stage
ISAYA study
National Population Health Survey 1st cycle
Canadian Community Health Survey
Belgian Air Force study
Post office employees
College of General Practitioners Study
ECRHS study, second stage
British male doctors study
British female doctors study
part of Seven Countries Study
part of Seven Countries Study
South African Demographic and Health
Survey
Malmo Preventive Program
Cardiovascular Health study
CPS I
Berlin study
Berlin study
Berlin study
SPPARCS study
Rand Health Insurance Experiment
NICE study
IJsselstein cohort study
Copenhagen City Heart/ Glostrup/
Copenhagen Male studies
CPS I
Baltimore Longitudinal Study of Aging
Vale of Glamorgan study
Annandale study
Tecumseh Community Health Study
Tecumseh Community Health Study
Six prefecture study
-4-
Outcomes included
COPD
CB
EMP
0
x
0
x
0
0
x
0
0
x
x
0
0
0
x
x
0
0
0
0
x
0
x
0
0
x
0
0
x
0
x
0
0
x
x
x
0
x
0
x
0
0
0
x
0
0
x
0
0
x
0
x
0
0
x
0
0
x
0
0
x
0
0
x
0
0
0
x
0
x
0
0
0
x
0
x
0
0
0
x
0
0
x
0
x
0
0
x
x
0
x
0
0
x
0
0
x
x
0
x
x
0
x
0
0
0
x
x
0
x
0
0
x
0
x
0
x
x
x
x
x
0
0
x
0
x
x
x
0
x
0
x
0
0
0
x
x
0
x
0
0
0
0
x
0
0
0
0
0
0
0
0
0
0
0
0
0
x
0
x
x
x
0
x
0
x
0
0
x
0
0
x
0
x
0
x
0
x
x
x
0
x
x
0
x
x
0
x
0
x
x
0
0
0
0
0
0
0
0
0
x
REF
Brief description of study
HO
HOLLA2
HOLLNA
HOUSE
HOZAWA
HRUBEC
HUCHON
HUHTI1
HUHTI2
HUHTI3
ITABAS
JACOBS
JAENDI
JENSEN
JINDA2
JOHANN
JOSHI
JOUSI1
KACHEL
KAHN
KAHN2
KARAKA
KATANC
KATO
KHOURY
KIM
KIRAZ
KLAYTO
KOJIMA
KOTAN1
KOTAN2
KRZYZA
KUBIK
KULLER
LAI
LAM1
LAM2
LAM3
LAMBER
LANGE
LANGE2
LANGHA
LAVECC
LEBOWI
LEE
Hong Kong elderly CS 1991
US middle-aged male telephone employees CS 1962
Glostrup 40 year old CS 1976-7
US sulfur oxide exposure parents CS 1970
US 4 centre ARIC baseline CS 1987-89
US Veterans Twin Registry adults CS ca 1972?
French adults CS ca 2001?
Harjavalta middle-aged CS 1961
Harjavalta middle-aged CS 1971
Hankasalmi rural men CS 1968-70
Sendai elderly CC ca 1989?
Seven Countries middle-aged men PS 1957-89?
Toledo general practice CS 2001-02
Danish bronchial reactivity adults CS ca 1996?
Indian urban/rural adults CS ca 2004?
Hordaland community PS 1985-1997
Indian male factory workers CS ca 1974?
North Karelia/Kuopio CS 1972 + 1977
Bielsko-Biala factory workers CS ca 2002?
US Veterans PS 1954-80
US Veterans PS 1954-62
EPIC (Athens) air pollution NCC up to 1996
Pittsbgh/Tennessee elderly periodontal CS 1997-98
Japanese baseline cancer CS 1985
Baltimore familial component study (1970s)
Korean NHANES II CS 2001-2
Kayseri biomass fumes CS 1999
San Francisco MM research workers CS ca 1974?
Aichi Health Centre CS 2001-02
Finnish outdoor workers/skiers CS 1995-96
North Finland clinical CS 1996-97
Polish (Cracow) population PS 1968-1981
Kolin lung cancer adults CS 1972
US MRFIT all screenees 1972-74 with 6 yr follow-up
Hong Kong CS 2001-2003
Xi'an factory workers PS 1976-96
Xi'an retired military men CS 1987 (baseline)
Xi'an retired military men PR 1987-2005(follow-up)
English/Welsh/Scottish adults CS 1965
Copenhagen PS 1976-78 to 1989
Danish elderly population CS 1991-4
Norwegian HUNT adults CS 1995-97
Italian National Health Survey CS 1983
Tucson white adults PS (baseline) 1972-3
Great Britain migrants' siblings PS 1964 to 1977
LIAW
LINDBE
LINDST
LIU1
LIU2
LUNDB1
LUNDB2
MADOR
MAGNUS
MANFRE
MANNI1
MANNI2
MANNI3
MARAN1
MARAN2
MARCUS
Taiwan multicentre screening PS 1982-1993
Norrbotten OLIN PS 1996-2003
Sweden/Finland FinEsS CS ca 1998?
China retrospective mortality CC study 1986-91
Guangdong urban/rural CS 2002-03
North Sweden OLIN CS 1996
Swedish OLIN adults CC 1986
New York veterans exercise CC (ca 2002?)
Icelandic male CS 1993
Canadian Rural Adults CS 1978-9
US (NHANES III) adults CS 1988-94
US (NHANES I) adults CS 1971-75
US (NHANES I) adults PS 1971-92
Bangkok elderly baseline 1998
Bangkok elderly PS 1998-9
Oahu (HHP) Japanese men PS 1965-84
MATHES
MELLST
MENEZ1
MENEZ2
MENEZ3
MENEZ4
MENEZ5
MENEZ6
Melbourne genotyping CS (ca 2005?)
Goteborg 70 year old men CS 1971-72 and 1976-77
Brazilian Urban Adults CS 1990
Sao Paulo PLATINO CS 2003
Santiago PLATINO CS 2003
Mexico City PLATINO CS 2003
Montevideo PLATINO CS 2003
Caracas PLATINO CS 2003
Original study name
Glostrup Population Study
Salt Lake Basin study
ARIC study
Harjavalta study baseline
Harjavalta study follow-up
Seven Countries study
Hordaland County study
North Karelia/Kuopio study
US Veterans - Dorn study
US Veterans - Dorn Study
EPIC study (nested case-control)
Health ABC study
Johns Hopkins familial component study
Korean NHANES II
Cracow study
MRFIT study (all screenees)
Copenhagen City Heart Study (prospective)
Copenhagen City Heart Study 3rd round
HUNT study
second National Health Survey
Tucson study
British sibling sample, USA-UK-Norway
Migrant stdy
OLIN study
FinEsS study
Million deaths study
OLIN study
OLIN Study 1986
NHANES III Survey
NHANES I Survey (baseline prevalence)
NHANES I Survey (22 years follow-up)
Honolulu Heart Program/Japan-Hawaii
Cancer Study
70 Year Old People in Goteborg
Pelotas study
PLATINO study
PLATINO study
PLATINO study
PLATINO study
PLATINO study
-5-
Outcomes included
COPD
CB
EMP
x
x
x
0
x
0
0
x
0
0
x
0
x
0
x
0
x
0
0
x
0
x
x
x
x
x
0
x
x
0
x
0
0
x
0
0
x
0
0
0
x
0
0
x
0
x
0
0
0
x
0
0
x
0
x
0
0
x
x
x
x
x
x
x
0
0
x
0
0
0
x
0
x
0
0
x
0
0
x
x
0
x
0
0
x
0
0
0
x
0
x
0
0
x
0
0
0
x
0
x
0
0
x
0
0
x
0
0
x
0
0
x
0
0
0
x
0
x
0
0
0
x
0
0
x
0
0
x
x
x
x
x
x
0
0
x
x
x
x
x
x
0
x
0
0
x
x
x
x
x
x
0
0
x
0
0
0
x
0
x
x
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
x
0
0
x
x
x
x
x
0
x
x
0
0
0
0
0
0
0
0
0
0
0
0
0
REF
Brief description of study
MEREN
MILLER
MILNE
MOLLER
MONTNE
MUELLE
NAWA
NEJJAR
NIEPSU
NIHLEN
NILSSO
OGILVI
OMORI
OSWAL1
OSWAL2
PANDEY
PEAT
PELKON
PEREZP
PETO
Estonian postal CS 1995-6
Michigan PBB contaminants adults CS 1978
Edinburgh Elderly adults baseline CS 1968-70
German adults CC ca 1999?
Malmo postal survey baseline 1992
Glenwood Springs household CS 1967
Japanese workers/retired men CS 1998-2000
French elderly CS ca 1991?
Zabrze adults CS 2001
Malmo family history PS 1992-2000
Swedish smoking habits PS 1963-1996
Newcastle adults CC 1955-56
Japanese male screening CS ca 2004?
UK adult patients/civil servants CC 1951-3
London adult civil servants CS 1954-5
Nepalese rural adults CS 1979-80
Busselton LS 1966-84
Finland rural PS 1959-2000
Mexico City women CC 1992-4
UK male mortality PS 1954-81
PRATT
PRICE
REID
RENWIC
RICCIO
RIMING
RYDER
SARGEA
SAWICK
SCHWAR
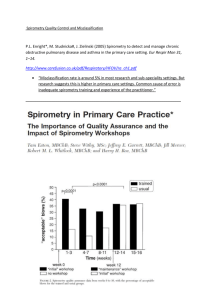
SHAHAB
SHARP
SHIMUR
SHIN
SICHLE
SILVA
SOBRAD
SPEIZE
STERLI
US autopsy CS ca 1978?
UK (Aberdeen) & USA (Denver) CS ca 2004?
US migrants/native born CS 1962-3
Manchester white adults CS 1992-4
Chieti hospital CS 2002
UK radiography volunteers CS 1970
Welsh? autopsy CS ca 1969?
UK EPIC-Norfolk diet CS 1993-96
Polish (Cracow) population CS baseline 1968
US national adults CS 1976-80
England nationwide health CS 2001
Chicago electric company male workers 1960-1
Japanese autopsy CC ca 1994?
Ansan City residents CS 1999-2000
Northern Greece CS 2000-01
Tucson white adults PS 1972-ca 1992?
Spanish IBERPOC CS 1996-97
US 6 cities PS 1974-86
US (NMFS/NHIS) adult decedents CC 1986/87
STJERN
STROM
SUADIC
SUTINE
TAGER
TAGER2
TANG
Swedish sulphite exposed adults CS 1981
Malmo male risk factors CS 1982-3
Copenhagen middle-aged men CS 1985-6
Finnish necropsy CS 1971-72
East Boston family (1 deg relatives) CS 1973-74
East Boston adults CS 1973-74
Pooled analysis 4 UK PS 1967-82, max 19y follow-up
THUN
TODD
US (CPS II) household PS 1982-88
Great Britain PS 1965 followed to 1977
TROISI
TRUPIN
TSUSHI
TVERDA
URRUTI
VESTBO
VIEGI1
VIEGI2
VIKGRE
VINEIS
VOLLM1
US female nurses PS 1980-90
US telephone survey CS 2001
Nagano lung cancer screening CS 2003-2004
Norwegian mortality PS 1972-88
Spanish ECRHS young adults CS ca 2004?
Copenhagen baseline 1976-78
Northern Italian low pollution CS 1980-82
Po delta CS 1988-91
Swedish elderly men PS 1994-2001
EPIC multicentre PS 1993-ca 2003?
Portland screening clinic volunteers CS 1971-2
VOLLM2
Portland screening clinic volunteers PS 1971-82
VONHER
WAGEN2
WALD
WANG2
WATSON
Finnish (MFHS) CS 1978-80
Dutch employees CC 2001
London professional/businessmen PS 1975-93
Japanese cancer screening CS 1996-98
Southampton GP CC study (ca 2000?)
Original study name
Edinburgh Elderly study: baseline
PAQUID cohort
1963 smoking habit survey
Busselton study
Seven Countries study (Finland centres)
Leigh/Staveley/Rhondda/Vale of
Glamorgan/London studies (follow-up)
EPIC study
Cracow study
NHANES II Survey
Health Survey for England
Western Electric Company study
Tucson study
IBERPOC study
Six cities study
1986 NMFS (National Mortality Followback
Survey)/ 1987 NHIS (National Health
Interview Survey)
Men born in 1914
Copenhagen Male study
BUPA/Whitehall/Paisley-Renfrew/UKHD
prevention
CPS II
British pop sample, USA-UK-Norway
Migrant study
Nurses' Health Study
ECRHS study (based on Spanish data only)
Copenhagen City Heart Study (baseline)
Men born in 1933 in Goteborg - follow-up
EPIC study
Portland/screening centre cohort study baseline
Portland/screening centre cohort study follow-up
Mini-Finland Health Survey
Maastricht Cohort Study
BUPA study
-6-
Outcomes included
COPD
CB
EMP
0
x
0
0
x
x
0
x
0
0
x
0
x
0
0
x
x
0
0
0
x
0
x
0
x
0
0
x
0
0
x
0
0
0
x
0
0
0
x
0
x
0
0
x
0
0
x
0
x
0
0
x
x
0
x
x
0
x
0
0
0
x
0
x
x
0
0
x
x
0
x
0
0
x
x
x
0
x
x
0
0
x
0
0
x
0
0
x
x
0
x
x
0
0
x
x
0
0
x
0
0
0
0
0
x
0
0
0
0
0
0
0
0
x
0
0
0
0
x
0
0
x
0
x
x
0
x
0
0
x
0
0
0
0
x
0
0
0
x
x
0
0
0
0
0
x
x
x
0
x
0
x
0
x
x
x
0
0
0
x
0
x
0
0
0
0
0
0
0
0
0
0
0
0
x
0
0
x
0
0
x
0
x
0
x
0
x
0
0
0
0
0
0
x
0
REF
Brief description of study
Original study name
WEISS
Philadelphia lung cancer project men CS 1961
Philadelphia Pulmonary Neoplasm Research
Project
WEN
WIG
WILHEL
WILSO1
WILSO2
WOJTYN
WOODS
WOOLF
XIAO
XU
YAMAGU
YUAN
ZIELI1
ZIELI2
ZIETKO
ZOIA
Taiwan community & civil service PS 1982-2000
Indian urban/rural adults CS ca 1963?
Swedish 54 year old men CS 1967
Northwest Adelaide Health Study Baseline 2000
South Australian adults CS 1998
Polish (Cracow) population CS 1968,1973 combined
Melbourne and Riverina young adults CS ca 1998?
Canadian employed women CS ca 1970-1973?
Beijing Hospital CC ca 2003?
Nanjing urban/rural CS 2000-01
Beijing air pollution CS 1986
Shanghai middle-aged men PS 1986-93
Polish 12 cities screening CS 1999
Poland nationwide screening CS 2000-2003
Bialystok nitric oxide CC ca 2003?
Lombardy dietary CS ca 1993?
Men born in 1913 in Goteborg
Northwest Adelaide Health Study
South Australian Health Omnibus Survey
Cracow study
Beijing Respiratory Health study
Know the Age of Your Lung Study 1
Know the Age of Your Lung Study 2
-7-
Outcomes included
COPD
CB
EMP
x
0
x
x
0
0
x
0
x
0
0
x
x
x
x
x
x
x
0
x
x
x
0
x
x
x
x
0
0
x
0
0
0
0
x
x
0
0
0
x
0
0
0
0
0
0
0
0
0
0
0
Table 2
Na
1
TypebREF
B AMIGO
1
2
B MENEZ3
A BECK1
2
3
A BECK2
C DEMARC
3
4
C URRUTI
B EKBERG
4
A/B MONTNE
4
A/B NIHLEN
4
B STROM
5
B ENRIGH
5
5
6
B HARIKK
B HOZAWA
C FERRI2
6
6
7
C FERRI1
C FERRI3
C GODTFR
7
7
7
7
7
8
A/C
A/C
A/C
A/C
A/C
C
LANGE
HOLLNA
SUADIC
VESTBO
LANGE2
HAMMO2
8
9
C ENSTRO
B HARDIE
9
9
B/C JOHANN
B/C BROGGE
Overlapping and linked studies
REFGPb Princ/Subsidb COPDc CBc Empc Comment
AMIGO Principal
i
Possible overlap between study AMIGO (2001-03 clinic cases of COPD
with outpatient controls) and MENEZ3 (household survey 2003) both in
Santiago
MENEZ3 Principal
p
BECK1 Principal
p
BECK1 is cross-sectional analysis of Lebanon survey at baseline,
BECK2 is incidence analysis based on 6 years of follow-up in those
disease-free at baseline
BECK2 Principal
i
DEMARC Principal
p
p
DEMARC is multinational study, treated as principal. URRUTI is
Spanish sample only but gives data for cigarettes per day. Study
DEMEER based on Dutch sample only but rejected as unexposed group
unsatisfactory.
DEMARC Subsidiary
p
EKBERG Principal
p
Study EKBERG includes persons attending screening in Malmo and born
approx 1913-65, so may overlap with NIHLEN (random sample of
persons living in Malmo area and born approx 1933-72) and with
STROM (50% of all men living in Malmo and born 1914)
MONTNE Principal
p
Study MONTNE includes a random sample of persons living in Malmo
area and born approx 1933-72, so may overlap with EKBERG (persons
attending screening in Malmo and born approx 1913-65). Disease-free
subjects from this study were followed up in study NIHLEN
NIHLEN Principal
i
Study NIHLEN includes a random sample of persons living in Malmo
area and born approx 1933-72, so may overlap with EKBERG (persons
attending screening in Malmo and born approx 1913-65). NIHLEN is a
follow-up of the disease-free subjects from study MONTNE.
STROM Principal
p
Study STROM includes 50% of all men living in Malmo and born 1914,
so may overlap with EKBERG (persons attending screening in Malmo
and born approx 1913-65)
ENRIGH Principal
p
p
HOZAWA was conducted in 1987-89 in four communities, including
Washington county MD and Forsyth County NC. ENRIGH also included
those two counties but as it started in 1989 and included only age 65+ any
overlap will be minimal. HARIKK was conducted in Washington/
Baltimore MD and continuously recruited subjects since 1958
HARIKK Principal
i
HOZAWA Principal
p
p
FERRIS Principal
p
Study FERRI1 consists of original sample surveyed in 1961. Study
FERRI2 is follow-up survey in 1967 which also included newly recruited
second sample. Study FERRI3 is further follow-up cross-sectional survey
in 1973. Study FERRI2 chosen as principal because based on largest
sample.
FERRIS Subsidiary
p
p
FERRIS Subsidiary
p
GODTFR Principal
i
Study GODTFR is pooled analysis of 3 prospective studies, with
outcome COPD hospitalization and excluding subjects with previous
hospitalization. Study VESTBO is baseline prevalence of GOLD-COPD
in the Copenhagen City Heart Study, SUADIC is cross-sectional analysis
of MRC-CB at 15-year follow-up in the Copenhagen Male Study, and
HOLLNA is baseline prevalence of CB in the Glostrup Study. All have
been marked as principal although some overlap with GODTFR is likely.
Study LANGE is follow-up to COPD-related mortality from the CCHS this is marked as subsidiary to GODTFR, and some overlap with
VESTBO is likely. LANGE2 is a cross-sectional analysis of CB at 15year follow-up in the CCHS - this is marked as subsidiary to VESTBO,
and some overlap with GODTFR is likely
GODTFR Subsidiary
m
HOLLNA Principal
p
SUADIC Principal
p
VESTBO Principal
p
VESTBO Subsidiary
p
HAMMO2 Principal
m
m
HAMMO2 is based in 25 states, ENSTRO is based on subset of subjects
in one state only but follow-up is longer
HAMMO2 Subsidiary
m
HARDIE Principal
p
p
p
Half of subjects in study BROGGE were drawn from survivors of study
JOHANN (ongoing community cohort study up to age 82 in county
Hordaland incl Bergen since 1985) and the remainder from hospital
records in Bergen. Also possible overlap with study HARDIE (conducted
in Bergen in 1998-9 age 70+)
JOHANN Principal
p
JOHANN Subsidiary
p
-
-8-
Na
10
TypebREF
C HIGGI4
10
11
C HIGGI6
C HOUSE
11
12
C CHAPMA
C HUHTI1
12
13
C HUHTI2
C JACOBS
13
13
13
14
C
C
C
C
14
15
C KAHN2
C KOTAN1
15
16
C KOTAN2
A KRZYZA
16
16
17
A/C SAWICK
A/C WOJTYN
A LAM2
17
18
A LAM3
B LEBOWI
18
19
B SILVA
A LINDBE
19
19
20
A/C LUNDB1
A/C LUNDB2
A MANNI2
20
21
A MANNI3
A MARAN1
21
22
A MARAN2
B OSWAL2
22
23
B OSWAL1
C PETO
23
24
C HIGGI2
A TAGER
24
A TAGER2
DONTA1
DONTA2
PELKON
KAHN
REFGPb Princ/Subsidb COPDc CBc Empc Comment
HIGGI4 Principal
m
HIGGI6 is a baseline prevalence study, with follow-up mortality in all
subjects entered as HIGGI4. Prevalence at an interim follow-up with
additional community sample (METZNE1983) has been mentioned as
alternative outcome in HIGGI6
HIGGI4 Subsidiary
p
HOUSE Principal
p
HOUSE is baseline (1970) cross-sectional analysis of Salt Lake Basin
communities, study CHAPMA presents results of 1976 survey in same
communities. HOUSE includes higher number of subjects, so is treated as
principal study.
HOUSE Subsidiary
p
.
HUHTI1 Principal
p
p
p
Studies HUHTI1 and HUHTI2 are cross-sectional surveys conducted on
same subjects 10 years apart
HUHTI1 Subsidiary
p
p
JACOBS Principal
m
JACOBS is multinational study. Subjects from one centre (Crete/Greece)
are also included in studies DONTA1 (baseline prevalence of COPD) and
DONTA2 (10-year incidenc), and subjects from West and East Finland
centres are included in study PELKON
JACOBS Subsidiary
p
JACOBS Subsidiary
i
i
JACOBS Subsidiary
i
i
KAHN
Principal
m
m m
Study KAHN is based on 26 years follow-up but gives minimal results
for CB and EM. Study KAHN2 is based on only 8.5 years follow-up but
gives detailed results for CB and EM
KAHN
Subsidiary
m
m m
KOTAN1 Principal
p
Study KOTAN1 was a postal cross-sectional survey. Study KOTAN2
comprises a random subsample from part of the study area invited to
clinical study
KOTAN1 Subsidiary
p
KRZYZA Principal
i
Study SAWICK is baseline analysis using outcomes FEV1/FVC <60%
and MRC-CB. Follow-up study KRZYZA excludes subjects with
baseline FEV1/FVC <70% (so no overlap with SAWICK) but analyses
outcome FEV1/FVC <65% at 13 years. Results entered as study
WOJTYN defines outcomes as FEV1/FVC<70% and MRC-CB both at
baseline and at 5-year follow-up, and is marked as subsidiary study
SAWICK Principal
p
p
SAWICK Subsidiary
p
p
LAM2
Principal
p
Study LAM3 is prospective follow-up of disease-free subjects from
LAM2
LAM3
Principal
m
LEBOWI Principal
p
p
p
Study LEBOWI is baseline study of subjects who were prospectively
followed-up in study SILVA. As the outcomes studied are not identical,
some cases may be included in both studies. Results from paper
LEBOWI1977 omitted due to considerable inconsistencies in data
presented
SILVA
Principal
i
i
i
LINDBE Principal
i
Study LUNDB2 was the first wave (1986) of the OLIN study, analysed
as CC with a subset of symptom-free subjects as controls for CB cases.
The full cohort but males only was also analysed cross-sectionally (data
not entered but mentioned as alternative CB outcome in LUNDB2), and
also served as a control group in a study of miners (study HEDLUN,
subsequently rejected). A subset of the original full cohort was contacted
again in 1996 and analysed for both prevalent COPD (study LUNDB1)
and subsequent incidence (study LINDBE). LUNDB2 is marked as
subsidiary to LUNDB1
LUNDBA Principal
p
LUNDBA Subsidiary
p
MANNI2 Principal
p
Study MANNI2 is baseline prevalence, MANNI3 is follow-up of COPDfree subjects
MANNI3 Principal
m
MARAN1 Principal
p
Study MARAN1 includes prevalence at baseline and study MARAN2
includes incidence in 1 year follow-up of those disease-free at baseline
MARAN2 Principal
i
OSWAL2 Principal
p
36% of cases in CC study OSWAL1 were civil servants, and some
overlap with OSWAL2, a cross-sectional study in civil servants, cannot
be ruled out
OSWALD Principal
p
PETO
Principal
m
Study PETO includes 5 samples, one of which is also reported as a
subsidiary study (HIGGI2)
PETO
Subsidiary
p
TAGER Principal
p
Study TAGER refers to 1st degree relatives and is based on a random
sample of subjects aged 45-54 years while study TAGER2 refers to
cluster sample of households and includes subjects aged 5+ years
TAGER2 Principal
p
-
-9-
Na
25
TypebREF
C TANG
25
25
26
C HAWTHO
C WALD
C TODD
26
27
C LAMBER
C VINEIS
27
27
28
C KARAKA
C SARGEA
C VOLLM2
28
29
C VOLLM1
C WEN
29
30
C LIAW
B WILSO1
30
B WILSO2
REFGPb Princ/Subsidb COPDc CBc Empc Comment
TANG
Principal
m
Study TANG is marked as principal study and is a pooled analysis of 4
samples, 2 of which are also entered as subsidiaries. Study HAWTHO
includes 3 samples one of which (survey 3) was drawn from Paisley in
1974-5 thus also included in TANG (Renfrew and Paisley 1972-76).
Study WALD (the BUPA study) is also included in the TANG analysis.
TANG
Subsidiary
m
p
TANG
Subsidiary
m
TODD
Principal
m
Study LAMBER is baseline study of prevalent CB. Study TODD is 12year follow-up of CNSLD mortality (not excluding subjects with baseline
CB)
TODD
Subsidiary
p
VINEIS Principal
m
VINEIS is the multi-national EPIC study, conducted in 10 countries and
is marked as principal. SARGEA (UK) and KARAKA (Greece) were
analyses using the data from one country only and are marked as
subsidiary
VINEIS Subsidiary
p
VINEIS Subsidiary
p
VOLLME Principal
m
Study VOLLM1 is baseline, and VOLLM2 is prospective follow-up of
all subjects
VOLLME Subsidiary
p
WEN
Principal
m
m m
Study WEN includes two cohorts (community and civil service/teachers)
followed until 2000, with results available only for males. Study LIAW
reports both sexes for the community cohort only, with follow-up to
1993, and is marked as subsidiary
WEN
Subsidiary
m
WILSO1 Principal
p
WILSO1 was conducted in northwest Adelaide among persons age 18+
in 2000, WILSO2 in metropolitan Adelaide and country towns among
persons age 15+ in 1998, so some overlap cannot be ruled out
WILSO2 Principal
p
p
a
N identifies linked studies (the numbering is based on alphabetical order of the first principal study in
each set).
b
If the studies are independent (Type A), or the overlap between studies is deemed minor (Type B),
then each study is marked as principal and has a separate value of REFGP. Where the overlap is
deemed major (Type C), the studies share a common value of REFGP, and only one study within
REFGP is marked as principal. The principal study is chosen on the basis of factors such as largest
study size, widest geographical coverage or longest follow-up, and not on assessment of study quality.
A/B indicates a type A link with at least one study in the set and a type B with another, and similarly
for A/C and B/C – see Comment for details.
c
Availability of each outcome is indicated by m=mortality, i=incidence and p=prevalence
-10-
Table 3
Study characteristics
All studiesa
Variablec
Levelsc
Total
CC
Prosp
20
39
Study Typeb
CrossSec
Subsid
Total
134
25
218
Study type
case/control
prospective
cross-sectional
nested case/control
20
0
0
0
0
39
0
0
0
0
134
0
2
8
14
1
22
47
148
1
Study sex
both
male
female
17
2
1
20
17
2
108
23
3
20
5
0
165
47
6
Lowest age in study
no limit
<15
15 or adult NOS
16-19
20-29
30-39
40-49
50-59
60-69
70+
4
0
1
0
3
6
5
0
1
0
0
1
0
3
10
15
7
0
3
0
5
4
21
12
32
11
29
8
8
4
0
0
2
1
9
6
5
1
1
0
9
5
24
16
54
38
46
9
13
4
Highest age in study (at baseline
for prospective study)
unknown
0
0
1
0
1
0
0
2
4
2
0
12
2
4
9
6
1
2
15
6
8
29
19
5
4
62
1
1
5
8
2
1
7
9
13
45
37
10
7
96
60-69
-
6
-
0
6
70-79
80-89
90-98
no limit
-
2
9
3
19
-
2
3
0
4
4
12
3
23
Region
USA
Canada
S/C America
UK
Western Europe
Scandinavia
E Europe
SE Europe/Balkans
Middle East/S Asia
SE Asia/Pacific
Far East
Australia/NZ
Africa
multi
2
0
2
5
4
0
2
0
0
0
4
1
0
0
13
1
0
6
2
6
1
0
0
1
6
1
0
2
35
5
6
12
11
26
8
3
4
1
16
3
2
2
7
0
0
5
1
7
1
3
0
0
1
0
0
0
57
6
8
28
18
39
12
6
4
2
27
5
2
4
National cigarette tobacco type
Blended
Virginia
Mixed
Unknown
12
6
0
2
25
8
2
4
100
26
2
6
19
5
1
0
156
45
5
12
Start year of study
unknown
<1960
1960-69
1970-79
1980-89
1990-99
>1999
10
2
1
1
2
2
2
0
7
12
9
5
6
0
24
4
17
23
13
29
24
2
3
8
6
2
3
1
36
16
38
39
22
40
27
<50
50-59
60-69
70-79
80-89
90-98
no limit
Highest age in study at final
follow-up (prospective study)
-11-
All studiesa
Variablec
CC
Prosp
Study Typeb
CrossSec
Subsid
Total
10
3
24
1
38
<1960
1960-69
1970-79
1980-89
1990-99
>1999
2
0
1
2
3
2
4
9
10
5
8
0
4
13
23
13
30
27
3
6
7
3
4
1
13
28
41
23
45
30
unknown
-
5
-
0
5
1960-69
1970-79
1980-89
1990-99
>1999
-
2
5
12
9
6
-
1
2
1
4
1
3
7
13
13
7
Principal publication year
<1960
1960-69
1970-79
1980-89
1990-99
>1999
2
0
1
1
6
10
0
3
2
11
10
13
4
12
23
16
19
60
1
1
5
6
4
8
7
16
31
34
39
91
Type of Population
general
household
long-term resident
household + long-term resident
phone subscriber
employed
health insurance member
military veterans
military veteran + twin
other military
mixed
specfic race
volunteer
parent
siblings of migrants
clinic patients
16
1
0
0
0
1
0
1
0
0
1
0
0
0
0
0
13
6
3
0
0
5
0
3
0
1
3
1
3
0
1
0
61
26
6
1
1
13
1
2
1
2
6
1
6
3
0
4
14
3
1
1
0
1
0
1
0
0
1
0
2
1
0
0
104
36
10
2
1
20
1
7
1
3
11
2
11
4
1
4
Type of controls (for CC studies)
population
hospital
decedents
mixed
13
5
1
1
-
-
2
0
0
1
15
5
1
2
Type of population - controls
same as cases
(differences from case population)
no respiratory symptoms
no respiratory disease
no respiratory symptoms/disease
normal LF
normal LF, no respiratory
symptoms
normal LF, no major disease
household members
9
-
-
2
11
1
2
1
2
1
-
-
0
0
1
0
0
1
2
2
2
1
2
2
-
-
0
0
2
2
Any proxy use
3
1
6
0
10
Any major study weakness
9
4
13
6
32
5
8
20
2
1
1
-
-
1
1
3
0
0
0
6
9
23
2
1
1
End year of study (of baseline for
prospective study)
Final follow up year (prospective
study)
Levelsc
unknown
Matching factors: (CC studies):
sex
age
race
location (within study area)
socioeconomic status
hospital admission (ward, date
etc)
-12-
All studiesa
Variablec
Levelsc
Results available by :
current vs never
ex vs never
ever vs never
current vs non
amount smoked
age started smoking
pack-years
duration of smoking
duration of quitting (vs never)
inhalation level
filter plain
tar level
nicotine level
other aspects of smoking
CC
Prosp
Study Typeb
CrossSec
Subsid
Total
14
12
16
14
7
5
10
2
3
2
2
1
0
4
34
29
29
28
23
7
5
4
8
5
3
2
1
16
98
93
113
101
47
5
43
6
7
6
4
0
0
27
23
19
18
17
14
3
5
2
4
2
3
1
0
9
169
153
176
160
91
20
63
14
22
15
12
4
1
56
14
7
0
35
9
7
67
71
19
17
14
2
133
101
28
13
6
0
1
0
0
0
28
2
1
2
1
1
4
52
55
8
8
3
4
4
11
7
0
5
0
1
1
104
70
9
16
4
6
9
Results also available for other
disease definitionsd
Results also available by severity
of COPDd
0
9
38
9
56
1
2
10
1
14
Results by stratifying factors
available (other than sex)
5
14
62
9
90
2
7
2
3
1
2
1
1
1
5
10
5
1
4
2
9
3
0
16
26
20
13
9
29
15
4
2
3
4
2
1
1
5
6
1
2
26
47
29
18
15
38
31
9
5
Outcomes available in study
COPD
CB
Emphysema
COPD only
CB only
Emp only
COPD and CB
COPD and Emp
CB and Emp
COPD, CB and EMP
Number of relative risks
1-2
3-4
5-6
7-8
9-10
11-20
21-50
51-100
>100
-13-
Table 3 (continued – COPD studies)
COPD studiesa
Variablec
Levelsc
Total
CC
Prosp
Study Typeb
CrossSec
Subsid
Total
14
35
67
17
133
Study type
case/control
prospective
cross-sectional
nested case/control
14
0
0
0
0
35
0
0
0
0
67
0
1
7
8
1
15
42
75
1
Study sex
both
male
female
11
2
1
18
16
1
60
5
2
13
4
0
102
27
4
Lowest age in study
no limit
<15
15 or adult NOS
16-19
20-29
30-39
40-49
50-59
60-69
70+
4
0
1
0
1
3
4
0
1
0
0
0
0
3
10
14
6
0
2
0
5
1
5
7
17
6
16
3
4
3
0
0
1
1
5
4
5
1
0
0
9
1
7
11
33
27
31
4
7
3
Highest age in study (at baseline
for prospective study)
<50
0
2
1
0
3
0
1
2
1
0
10
3
8
6
1
2
13
1
11
11
4
1
38
1
2
6
2
1
5
5
22
25
8
4
66
60-69
-
4
-
0
4
70-79
80-89
90-98
no limit
-
2
9
3
17
-
2
2
0
4
4
11
3
21
Region
USA
Canada
S/C America
UK
Western Europe
Scandinavia
E Europe
SE Europe/Balkans
SE Asia/Pacific
Far East
Australia/NZ
multi
2
0
2
2
2
0
2
0
0
3
1
0
11
1
0
6
2
5
1
0
1
5
1
2
14
3
5
3
4
13
6
3
1
12
1
2
5
0
0
3
0
5
1
2
0
1
0
0
32
4
7
14
8
23
10
5
2
21
3
4
Start year of study
unknown
<1960
1960-69
1970-79
1980-89
1990-99
>1999
8
0
1
0
2
2
1
0
7
11
8
4
5
0
7
0
7
7
6
16
24
1
2
5
5
1
2
1
16
9
24
20
13
25
26
End year of study (of baseline for
prospective study)
unknown
8
3
7
0
18
<1960
1960-69
1970-79
1980-89
1990-99
>1999
0
0
1
1
3
1
4
8
9
4
7
0
0
6
6
5
18
25
2
3
6
2
3
1
6
17
22
12
31
27
50-59
60-69
70-79
80-89
90-98
no limit
Highest age in study at final
follow-up (prospective study)
-14-
COPD studiesa
Variablec
Levelsc
CC
Prosp
unknown
-
5
1960-69
1970-79
1980-89
1990-99
>1999
-
Principal publication year
1960-69
1970-79
1980-89
1990-99
>1999
Type of Population
Type of controls (for CC studies)
Study Typeb
CrossSec
Subsid
Total
-
0
5
2
4
11
8
5
-
1
1
1
4
1
3
5
12
12
6
0
1
0
5
8
3
2
9
9
12
3
8
2
8
46
1
3
4
3
6
7
14
15
25
72
general
household
long-term resident
household + long-term resident
phone subscriber
employed
military veterans
other military
mixed
specfic race
volunteer
siblings of migrants
clinic patients
13
0
0
0
0
0
1
0
0
0
0
0
0
11
6
2
0
0
4
3
1
3
1
3
1
0
31
14
6
1
1
3
1
0
3
0
4
0
3
8
2
1
1
0
1
1
0
1
0
2
0
0
63
22
9
2
1
8
6
1
7
1
9
1
3
population
hospital
decedents
mixed
10
2
1
1
-
-
1
0
0
1
11
2
1
2
Type of population - controls
same as cases
(differences from case population)
no respiratory symptoms/disease
normal LF
normal LF, no respiratory
symptoms
normal LF, no major disease
household members
7
-
-
2
9
1
2
1
-
-
0
0
0
1
2
1
1
2
-
-
0
0
1
2
Any proxy use
3
1
0
0
4
Any major study weakness
7
4
8
4
23
Matching factors (for CC studies) :
sex
age
location (within study area)
2
5
1
-
-
1
1
0
3
6
1
1
2
10
1
14
Final follow up year (prospective
study)
Results also available by severity
of COPD
Disease definition (subtype)
mortality
lung function
other
3
7
4
25
5
5
0
47
20
6
4
7
34
63
36
Disease definition
ICD
LF only
LF and symptoms
CB or EM
COPD CB or EM
CB, EM or AST
other COPD
COPD undefined
3
7
2
0
1
0
0
1
26
5
1
0
1
0
2
0
0
47
1
6
2
2
7
2
6
4
0
1
1
0
5
0
35
63
4
7
5
2
14
3
Diagnostic criteria
GOLD
MRC
ATS
ERS
2
0
3
2
2
0
1
0
23
1
2
1
2
1
0
0
29
2
6
3
-15-
COPD studiesa
Variablec
Levelsc
ICD
Mixed
unspecified
Thoracic Society of Thailand
Van Schayck
Enright
Chinese Soc Resp Dis
BTS
CC
3
0
3
0
0
0
0
1
Prosp
21
1
9
1
0
0
0
0
Study Typeb
CrossSec
0
3
32
1
1
1
1
1
Subsid
5
4
5
0
0
0
0
0
Total
29
8
49
2
1
1
1
2
ICD7 codes
501-502,527.1,(527.2 later)
500-502,527.1
241,500-502,527.1
502,526,527.1
unspecified
-
1
2
0
2
2
-
0
1
1
0
1
1
3
1
2
3
ICD8 codes
490-492
490-492,519
490-493
466, 490-493
490-493,518,519.3
491-492,519
unspecified
0
0
1
0
0
0
0
2
1
0
1
1
1
1
-
1
0
2
0
0
0
1
3
1
3
1
1
1
2
ICD 9 codes
491,492,496
490-492,496
490-492,496,416.7
490-496
416,491,492,496,519
466, 490-493
unspecified
0
1
1
0
0
0
0
1
1
0
7
0
1
2
-
0
0
0
1
1
0
2
1
2
1
8
1
1
4
ICD 10 codes
J40-J44
unspecified
-
1
2
-
0
1
1
3
Analysis type for asthma
include irrespective of asthma
excluding all asthmatics
cases include but controls
exclude asthmatics
COPD definition includes
asthma
unkn if COPD defn includes
asthma
cases exclude but controls
include asthmatics (cannot have
both diagnoses)
3
5
4
16
3
0
50
10
0
9
1
0
78
19
4
1
9
4
6
20
1
6
2
1
10
0
1
1
0
2
FEV1/FVC <70%
FEV1/FVC<70% and
FEV1<80% predicted
FEV1/FVC<88%M, 89%F
FEV1/FVC<normal (ATS value
nk)
FEV1<65% predicted or
FEV/FVC<65%
FEV1% <60
FEV1/FVC <80%
FEV1 <75% predicted
FEV1/or VC <70%predicted
FEV1 <65% predicted
FEV1/FVC<70% +
reversibility<15%
FEV1/FVC<88% +
reversibility<12%
FEV1<5th%ile +
reversibility<9%
FEV1/FVC <65%
FEV1 or MMEF <2SD below
predicted
FEV1 or DLCO <80% predicted
FEV1/FVC <68%
FEV1/FVC <60%
GOLD2+ (FEV1/FVC<70%,
FEV1<80%)
2
1
2
0
30
2
3
1
37
4
1
2
0
0
1
1
1
0
3
3
0
1
0
0
1
0
0
1
0
0
0
0
0
0
1
1
1
1
1
0
0
1
1
1
0
0
0
0
0
2
1
1
1
2
2
0
0
1
0
1
0
0
1
0
1
0
0
0
0
1
1
0
0
1
1
0
0
0
1
1
0
0
1
0
2
5
2
0
0
2
1
1
2
7
5
Lung function criteria
-16-
COPD studiesa
Variablec
Levelsc
FEV1 < 85% predicted
ATS NOS
FEV1/FVC<75%
FEV1/FVC<70%, FEV1<80%
predicted, reversibility <12
FEV1 > 2SE below predicted
unspecified
CC
0
1
0
1
Prosp
0
0
0
0
Study Typeb
CrossSec
1
0
1
0
Subsid
0
0
0
0
Total
1
1
1
1
0
0
0
0
1
1
0
0
1
1
Spirometry with bronchodilator
post-bronchodilator
without/pre/unknown
pre + post-bronchodilator
0
9
1
1
6
1
11
39
5
2
7
0
14
61
7
Source of diagnosis
Hospital/GP records
Questionnaire: physician
diagnosis
Questionnaire: other
Spirometry
Death certificate/ registry
Mixed
1
0
2
1
0
7
0
1
3
9
0
8
2
3
0
5
21
6
3
47
0
10
0
4
6
6
3
64
29
25
Questionnaire
none
MRC
NHLI
ATS
FinEsS
Harvard
OLIN
NHS
MRC/ATS
ATS/NHLBI
unnamed/ unspecified
14
-
32
0
1
1
0
0
1
0
0
0
0
48
3
0
2
1
1
1
1
1
1
8
11
4
0
0
0
0
0
0
0
0
2
105
7
1
3
1
1
2
1
1
1
10
Type of outcome
prevalence
mortality
incidence
10
3
1
2
25
8
67
0
0
10
6
1
89
34
10
Number of COPD cases
unknown
1-100
101-200
201-500
501-1000
>1000
Median
Range
Median (based on principal studies
only)
Range
1
10
1
0
1
1
64.00
19:32822
0
19
8
4
2
2
91.00
13:3483
0
19
18
17
3
10
178.00
34:21506
0
7
3
4
1
2
195.00
24:2243
1
55
30
25
7
15
134.00
13:32822
131.00
13:32822
1
0
0
0
1
5
0
0
0
5
2
0
0
0
2
4
1
10
2
17
0
5
10
4
19
2
29
47
11
89
200.00
7633.00
1727.00
1530.00
2032.50
29:261535 399:78638 207:10538 336:24819 29:786387
7
0
5
Median (based on principal studies
2033.00
only)
Range
- 29:786387
Total number of subjects
unknown
1-100
101-200
201-500
501-1000
>1000
Median
Range
Total number of adjustment
factors used
none
9
10
33
6
58
1
2
3
4
5
6
7
8
9
1
0
2
1
0
1
0
0
0
10
5
4
1
1
2
2
0
0
12
3
5
5
2
3
1
1
1
7
1
1
0
1
0
1
0
0
30
9
12
7
4
6
4
1
1
-17-
COPD studiesa
Variablec
Levelsc
13
Adjusted for :e
sex
age
race
location within study (1)
location within study (2)
aspects of study design
family (parent/sibling)
medical history
household composition
SES/education (1)
SES/education (2)
occupation (1)
occupation (4)
cooking/heating/aircon/ventila
tion (1)
cooking/heating/ aircon/
ventilation (3)
housing quality
exposure to allergens (4)
other medical
history/symptoms (1)
other medical
history/symptoms (2)
other medical
history/symptoms (3)
obesity/BMI
exercise
diet/alcohol (1)
diet/alcohol (2)
diet/alcohol (7)
ETS exposure (1)
other aspects of smoking (1)
other aspects of smoking (2)
other aspects of smoking (5)
Other confounders considered but
rejected
Smoking results available for
COPD :
current vs never
ex vs never
ever vs never
current vs non (as well as curr
vs never)
current vs non (and not curr
vs never)
amount smoked
age started smoking
pack-years
duration of smoking
duration of quitting (vs never)
duration of quitting (vs
current)
-18-
CC
0
Prosp
0
Study Typeb
CrossSec
1
Subsid
0
Total
1
0
5
0
1
1
0
1
3
25
0
3
0
5
1
15
30
3
6
0
0
5
2
11
0
3
0
0
0
20
71
3
13
1
5
7
0
2
0
1
0
1
1
1
0
1
0
0
1
9
2
7
0
1
0
2
0
0
1
0
2
14
2
9
1
2
0
0
1
0
1
0
0
0
0
1
0
1
0
4
0
0
0
1
1
4
0
1
0
0
1
0
3
1
0
4
1
0
1
0
0
1
1
0
0
2
1
3
0
0
0
4
1
0
6
1
1
2
1
1
1
0
1
0
0
1
0
0
0
1
0
0
9
2
6
2
1
2
7
1
1
0
0
2
1
3
9
7
11
8
30
27
27
25
50
48
57
48
15
11
11
11
104
93
106
92
1
2
3
0
6
3
3
9
2
2
1
19
6
3
1
4
3
17
4
30
3
2
2
7
2
5
1
2
2
46
15
47
7
10
8
Table 3 (continued – CB studies)
CB studiesa
Variablec
Levelsc
Total
CC
Prosp
Study Typeb
CrossSec
Subsid
Total
7
9
71
14
101
Study type
case/control
prospective
cross-sectional
7
0
0
0
9
0
0
0
71
1
4
9
8
13
80
Study sex
both
male
female
6
0
1
3
4
2
53
16
2
11
3
0
73
23
5
Lowest age in study
<15
15 or adult NOS
16-19
20-29
30-39
40-49
50-59
60-69
70+
0
0
0
2
3
2
0
0
0
1
0
0
3
4
1
0
0
0
2
14
5
20
5
14
4
4
3
0
1
1
5
3
2
1
1
0
3
15
6
30
15
19
5
5
3
Highest age in study (at baseline
for prospective study)
unknown
0
0
1
0
1
<50
50-59
60-69
70-79
80-89
90-98
no limit
0
0
1
2
1
0
3
0
1
0
0
1
1
6
6
7
20
10
1
2
24
1
1
4
5
1
0
2
7
9
25
17
4
3
35
60-69
-
1
-
0
1
70-79
80-89
90-98
no limit
-
0
0
1
7
-
2
2
0
0
2
2
1
7
Region
USA
Canada
S/C America
UK
Western Europe
Scandinavia
E Europe
SE Europe/Balkans
Middle East/S Asia
Far East
Australia/NZ
Africa
multi
0
0
1
3
2
0
0
0
0
1
0
0
0
4
1
0
2
0
0
0
0
0
2
0
0
0
20
3
1
8
7
16
3
1
4
3
2
2
1
4
0
0
3
1
4
1
1
0
0
0
0
0
28
4
2
16
10
20
4
2
4
6
2
2
1
Start year of study
unknown
<1960
1960-69
1970-79
1980-89
1990-99
>1999
2
2
0
1
0
1
1
0
4
1
2
2
0
0
14
4
14
16
8
15
0
1
3
6
2
1
1
0
17
13
21
21
11
17
1
End year of study (of baseline for
prospective study)
unknown
2
1
14
1
18
<1960
1960-69
1970-79
1980-89
1990-99
>1999
2
0
0
1
1
1
4
1
1
1
1
0
4
11
17
9
15
1
3
4
4
1
1
0
13
16
22
12
18
2
Highest age in study at final
follow-up (prospective study)
-19-
CB studiesa
Variablec
Levelsc
CC
Prosp
unknown
-
1
1960-69
1970-79
1980-89
1990-99
>1999
-
Principal publication year
<1960
1960-69
1970-79
1980-89
1990-99
>1999
Type of Population
Type of controls (for CC studies)
Study Typeb
CrossSec
Subsid
Total
-
0
1
1
2
2
2
1
-
1
2
0
0
1
2
4
2
2
2
2
0
0
1
2
2
0
2
0
3
2
2
4
10
16
14
12
15
1
1
4
4
1
3
7
13
20
22
17
22
general
household
long-term resident
employed
health insurance member
military veterans
military veteran + twin
other military
mixed
specfic race
volunteer
parent
clinic patients
4
1
0
1
0
0
0
0
1
0
0
0
0
2
1
0
3
0
2
0
0
1
0
0
0
0
32
14
2
10
1
0
1
2
3
1
1
3
1
8
2
1
0
0
1
0
0
1
0
0
1
0
46
18
3
14
1
3
1
2
6
1
1
4
1
population
hospital
mixed
3
3
1
-
-
1
0
0
4
3
1
Type of population - controls
same as cases
(differences from case population)
no respiratory symptoms
no respiratory disease
no respiratory symptoms/disease
normal LF, no major disease
3
-
-
0
3
1
2
0
1
-
-
0
0
1
0
1
2
1
1
Any proxy use
0
0
3
0
3
Any major study weakness
2
0
3
2
7
Matching factors (for CC studies) :
sex
age
location (within study area)
socioeconomic status
hospital admission (ward, date
etc)
3
3
1
1
1
-
-
0
0
0
0
0
3
3
1
1
1
Final follow up year (prospective
study)
Disease definition
CB based on ICD
CB based on symptoms not LF
CB self-reported
CB diagnosed
CB other
0
5
0
1
1
6
1
0
1
1
0
53
3
11
4
1
10
0
1
2
7
69
3
14
8
Diagnostic criteria
MRC
ATS
ICD
Mixed
unspecified
Rose
Fletcher
2
0
0
1
4
0
0
1
1
5
0
2
0
0
18
3
0
0
47
1
2
2
0
1
1
10
0
0
23
4
6
2
63
1
2
ICD7 codes
500-502
unspecified
-
3
2
-
1
1
4
3
ICD8 codes
unspecified
-
-
-
1
1
-20-
CB studiesa
Variablec
Levelsc
CC
Prosp
Study Typeb
CrossSec
Subsid
Total
ICD 9 codes
unspecified
491
-
0
1
-
1
0
1
1
ICD 10 codes
unspecified
-
-
-
1
1
Analysis type for asthma
include irrespective of asthma
excluding all asthmatics
cases include but controls
exclude asthmatics
2
2
3
8
1
0
68
3
0
10
3
1
88
9
4
Lung function criteria
FEV1 <80% predicted
FEV1/FVC <88% predicted
-
1
0
0
1
-
1
1
Spirometry with bronchodilator
without/pre/ unknown
-
1
1
-
2
Source of diagnosis
Hospital/GP records
Questionnaire: physician
diagnosis
Questionnaire: other
Death certificate/registry
Other
Mixed
Unspecified
3
0
0
1
0
8
0
0
3
9
2
0
0
1
1
2
6
0
0
0
53
0
4
6
0
9
1
0
4
0
66
7
4
11
1
CB: Questionnaire
none
MRC
ECRHS
NHLI
ATS
NHLBI
WHO
Rose
FinEsS
ECSC
Harvard
NHANES
OLIN
NHS
MRC/ATS
MRC/ECRHS
Health Omnibus Survey
CECA
unnamed/ unspecified
4
0
0
0
1
0
0
0
0
0
0
0
0
0
0
0
0
0
2
6
0
0
1
0
0
0
0
0
0
0
0
0
1
0
0
0
0
1
7
23
3
1
4
2
1
1
2
1
1
2
1
0
1
2
1
1
17
1
9
1
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
3
18
32
4
2
5
2
1
1
2
1
1
2
1
1
1
2
1
1
23
Type of outcome
prevalence
mortality
incidence
7
0
0
0
6
3
71
0
0
11
1
2
89
7
5
Number of cases
unknown
1-100
101-200
201-500
501-1000
>1000
Median
Range
Median (based on principal studies
only)
Range
0
2
1
3
1
0
300.00
6:973
1
5
2
0
1
0
85.00
2:798
2
17
16
18
7
11
209.00
8:4769
0
2
4
6
1
1
254.00
40:1119
3
26
23
27
10
12
198.50
2:4769
193.50
Total number of subjects
2:4769
2
0
0
0
1
0
2
1
2
8
600.00 53091.00
10:5255 901:26511
8
1-100
101-200
201-500
501-1000
>1000
Median
Range
Median (based on principal studies
only)
Range
-21-
1
0
3
1
0
1
10
1
12
9
2
14
50
11
71
2435.00
2857.00
2826.00
85:72284 460:24819 10:265118
5
2826.00
10:265118
CB studiesa
Variablec
Total number of adjustment
factors used
CC
Prosp
Study Typeb
CrossSec
Subsid
Total
none
5
1
24
3
33
1
2
3
4
5
6
7
8
2
0
0
0
0
0
0
0
6
1
0
0
0
1
0
0
21
7
4
4
2
5
3
1
8
0
1
0
1
1
0
0
37
8
5
4
3
7
3
1
0
1
0
0
0
0
0
0
1
8
0
0
0
1
0
0
18
38
2
13
2
0
1
3
1
9
0
3
0
0
0
0
20
56
2
16
2
1
1
3
0
0
1
0
1
0
0
0
0
0
0
0
0
13
7
0
4
0
1
1
0
13
8
1
4
0
0
1
0
0
0
1
1
7
0
0
0
1
1
8
0
0
1
1
2
0
1
0
0
1
0
0
0
0
0
0
0
0
0
0
0
0
2
0
2
1
1
4
0
1
0
0
0
1
2
1
2
1
1
5
0
0
4
1
5
5
5
6
4
8
6
5
3
57
54
60
53
14
13
12
11
84
78
83
71
1
0
5
0
6
4
2
2
0
1
1
5
0
0
2
2
2
35
1
11
2
4
3
9
1
1
0
1
1
53
4
14
4
8
7
Levelsc
Adjusted for :e
sex
age
race
location within study (1)
location within study (2)
aspects of study design (1)
aspects of study design (3)
family (parent/sibling)
medical history (1)
family (parent/sibling)
medical history (2)
SES/education
occupation (1)
occupation (4)
cooking/heating/aircon/ventila
tion
housing quality
exposure to allergens
other medical
history/symptoms (1)
other medical
history/symptoms (2)
other medical
history/symptoms (4)
obesity/BMI
diet/alcohol (1)
diet/alcohol (2)
diet/alcohol (3)
ETS exposure
other aspects of smoking
Other confounders considered but
rejected
Smoking results available for CB:
for current vs never
for ex vs never
for ever vs never
for current vs non (as well as
curr vs never)
for current vs non (and not
curr vs never)
amount smoked
age started smoking
pack-years
duration of smoking
duration of quitting (vs never)
duration of quitting (vs
current)
-22-
Table 3 (continued – Emphysema studies)
Emphysema studiesa
Variablec
Levelsc
Total
CC
Prosp
Study Typeb
CrossSec
Subsid
Total
-
7
19
2
28
Study type
prospective
cross-sectional
-
7
0
0
19
2
0
9
19
Study sex
both
male
-
3
4
15
4
0
2
18
10
Lowest age in study
<15
15 or adult NOS
16-19
20-29
30-39
40-49
50-59
60-69
70+
-
0
0
0
1
4
1
0
1
0
1
8
1
1
0
3
2
1
2
0
0
0
1
1
0
0
0
0
1
8
1
3
5
4
2
2
2
Highest age in study (at baseline
for prospective study)
60-69
-
1
5
0
6
70-79
80-89
90-98
no limit
-
0
1
1
4
1
0
3
10
1
1
0
0
2
2
4
14
60-69
-
1
-
0
1
80-89
90-98
no limit
-
0
1
5
-
2
0
0
2
1
5
Region
USA
Canada
UK
Western Europe
Scandinavia
SE Europe/Balkans
Far East
Australia/NZ
-
3
1
0
0
1
0
2
0
8
0
1
1
4
0
4
1
1
0
0
0
0
1
0
0
12
1
1
1
5
1
6
1
Start year of study
unknown
<1960
1960-69
1970-79
1980-89
1990-99
-
0
3
1
1
1
1
4
0
3
4
3
5
0
1
1
0
0
0
4
4
5
5
4
6
End year of study (of baseline for
prospective study)
unknown
-
1
4
0
5
<1960
1960-69
1970-79
1980-89
1990-99
>1999
-
2
2
0
0
2
0
0
2
5
2
5
1
1
1
0
0
0
0
3
5
5
2
7
1
unknown
-
1
-
0
1
1960-69
1970-79
1980-89
>1999
-
2
0
2
2
-
1
1
0
0
3
1
2
2
1960-69
1970-79
1980-89
1990-99
>1999
-
3
0
1
0
3
3
5
3
2
6
1
0
1
0
0
7
5
5
2
9
Highest age in study at final
follow-up (prospective study)
Final follow up year (prospective
study)
Principal publication year
-23-
Emphysema studiesa
Variablec
CC
Prosp
Study Typeb
CrossSec
Subsid
Total
-
1
2
1
0
2
1
0
9
4
1
1
1
1
2
1
0
0
0
1
0
0
11
6
2
1
4
2
2
Any proxy use
-
1
4
0
5
Any major study weakness
-
0
2
1
3
Type of Population
Levelsc
general
household
long-term resident
health insurance member
military veterans
mixed
volunteer
Emphysema definition
EM based on visual comparison
EM diagnosed
EM deaths (with ICD code)
EM self-reported
other EM
-
1
0
5
0
1
9
7
0
2
1
0
1
1
0
0
10
8
6
2
2
Diagnostic criteria
ICD
unspecified
Japanese Respiratory Society
-
4
3
0
0
18
1
1
1
0
5
22
1
ICD7 codes
527.1
-
4
-
1
5
ICD 9 codes
492
-
1
-
-
1
Analysis type for asthma
include irrespective of asthma
excluding all asthmatics
-
6
1
18
1
1
1
25
3
Lung function criteria
FEV1/FVC <70%
FEV1 or DLCO <80% predicted
-
0
1
1
0
-
1
1
Spirometry with bronchodilator
without/pre/ unknown
-
1
1
-
2
Source of diagnosis
Questionnaire: physician
diagnosis
Questionnaire: other
X-ray
CT scan
Death certificate/registry
Autopsy
Mixed
-
1
7
0
8
-
0
0
1
5
0
0
2
1
3
0
5
1
0
0
0
1
0
1
2
1
4
6
5
2
Questionnaire
none
MRC
NHLI
ATS
Health Omnibus Survey
unnamed/unspecified
-
6
0
1
0
0
0
10
1
1
2
1
4
1
1
0
0
0
0
17
2
2
2
1
4
Type of outcome
prevalence
mortality
incidence
-
0
5
2
19
0
0
0
1
1
19
6
3
Number of cases
1-100
101-200
201-500
501-1000
>1000
Median
Range
Median (based on principal studies
only)
Range
-
4
0
3
0
0
57.00
2:473
9
5
2
2
1
101.00
6:1384
1
0
1
0
0
220.50
15:426
14
5
6
2
1
96.50
2:1384
96.50
1-100
101-200
201-500
501-1000
>1000
-
Total number of subjects
-24-
2:1384
1
0
0
0
6
0
3
1
3
12
0
0
1
0
1
1
3
2
3
19
Emphysema studiesa
Variablec
Levelsc
Median
Range
Median (based on principal studies
only)
Range
Total number of adjustment
factors used
Study Typeb
CC
Prosp CrossSec
Subsid
Total
- 78000.00
1476.00 124327.50
2433.00
- 66:100322 164:72284 460:24819 66:100322
9
5
9
2433.00
66:100322
9
none
-
1
8
1
10
1
2
3
6
-
4
1
0
1
7
1
2
1
1
0
0
0
12
2
2
2
-
1
6
0
1
0
1
4
10
2
0
3
0
0
1
0
0
0
0
5
17
2
1
3
1
-
0
1
0
1
-
5
3
3
1
10
9
17
8
2
2
2
2
17
14
22
11
-
4
1
1
2
1
0
6
0
2
1
1
0
2
0
0
0
0
0
12
1
3
3
2
0
Adjusted for :e
sex
age
location within study
aspects of study design
SES/education
other medical
history/symptoms (4)
diet/alcohol (2)
Smoking results available for
Emphysema:
for current vs never
for ex vs never
for ever vs never
for current vs non (as well as
curr vs never)
amount smoked
age started smoking
pack-years
duration of smoking
duration of quitting (vs never)
duration of quitting (vs
current)
a
All studies are counted in the first section of the Table. In subsequent sections, studies with at least
one relative risk for each of the disease outcomes are counted; outcome-specific fields (including
description of the outcome definition and availability of results for the major and dose-related smoking
indices) are included only in those sections. The availability of results for other disease definitions and
stratified results, as well as the number of relative risks per study, are included only in the first section
b
Principal studies are categorized as CC (case-control, including nested CC), Prosp (prospective) or
CrossSec (cross-sectional). Subsidiary studies are categorized separately.
c
For presence/absence variables, the “Levels” column is left blank and counts for only the “presence”
level are shown. “Not applicable” levels are not shown (e.g. for variables specific to case-control
studies)
d
"Results also available for other disease definitions" refers to all disease definitions qualifying for
this project but not entered, with the exception of different levels of severity of COPD which are
counted separately (see following variable “Results also available by severity of COPD”)
e
Factors adjusted for – by 1 variable except where shown in brackets.
-25-
Table 4
REF
Study populations and exclusions
Population
ALDERS all (general population)
ALESSA all (general population)
Medical exclusionsa
Other exclusions
Pulmonary embolism, metabolic acidosis, cancer, acute
inflammatory, immunological, renal or peripheral vascular disease,
thrombosis, hypertension, diabetes, antiplatelet/anticoagulant drugs
in last 15d, hematocrit>50%
History of tuberculosis, silicosis, cancer, asthma, other respiratory
disease
AMIGO
all (general population)
ANDER1
ANDER2
ANDER3
AUERBA
BANG
BECK1
all (general population)
all (general population)
all (general population)
all (general population)
all (general population)
Died during subsequent 6-year follow-up
BECK2
all (general population)
Died during follow-up
Snuff users
Hispanics
BEDNAR all (general population)
BEST
military veterans
BJORNS
BROGGE
BROWN
CERVER
CHAPMA
CHEN1
CHEN2
all (general population)
all (general population)
all (general population)
all (general population)
parents
workers at 11 factories
household members
CHEN3
household members
CHENG
all (general population)
Non whites, never smokers who started smoking pipe/cigar only
during subsequent 6-year follow-up
Non-whites, baseline smokers who started smoking pipe/cigars
only during follow-up
Non-Caucasian
Additionally includes a few non-veterans who received Canadian
war veteran pensions
Asthma
Long-term hospitalization
AATD, previous chronic lung disease, dementia, HIV, hepatitis
Living >2 miles from air monitoring station
COPD, heart disease or rheumatoid arthritis diagnosed before the
age of 25 years
Cardiopulmonary disease (identified by electrocardiogram and
chest slides
CLEMEN Air Force personnel
COATES
COCCI
COLLEG
DEAN1
DEAN2
DEANE
Post Office employees
all (general population)
all (general population)
all (general population)
all (general population)
Non-Caucasian
Residents of Indian reserves and remote areas of Quebec and
Ontario
Residents of Indian reserves and remote areas
Subjects with fewer than 3 measurements of lung function during
study period
a
telephone company employees
-26-
REF
DEJONG
DEMARC
DETORR
DICKIN
Population
all (general population)
all (general population)
clinic or GP patientsb
all (general population)
doctors
DOLL1
doctors
DOLL2
DONTA1 all (general population)
DONTA2 all (general population)
DOPICO outdoor workers for City and power company
EHRLIC household members
EKBERG all (general population)
ENRIGH
health insurance members
Medical exclusionsa
Other exclusions
Positive bronchodilator response
Died within 12 month study period. Asthma or other restrictive
disease
Died during subsequent follow-up period
Baseline COLD (i.e. CB, EM, asthma or other lung disease). Died
during follow-up
Subjects with self-reported current/previous cancer, stroke, angina
pectoris, heart infarction or diabetes at baseline
Terminal illness, inability to walk, communicate or give informed
consent
ENSTRO household members
FERRI1
FERRI2
FERRI3
FIDAN
household members
households+long term residents
households+long term residents
FINKLE
FLETCH
FORAST
military recruits
Institutionalization, likely to move from area in next 3 years
Subjects in institutions or military service, migrant workers and
similar subjects who would be difficult to trace, households in
which no-one was aged at least 45 years
Regularly work away from home
Regularly work away from home
Regularly work away from home
Restricted to coffeehouse and small shop workers, but excluding
current employees in hair salons, barbershops, and bakeries, exemployees in shoe-making, painting, mining, textile and other
occupations with possible respiratory risks
Recruits from states other than Illinois and Indiana
coffeehouse or shop workers
men - postmen, women - clerical workers
all (general population)
FOXMAN all (general population)
FUKUCH household members
GEIJER
all (general population)
GODTFR
GOLDBE
GULSVI
HAENSZ
Emigrated or made dramatic changes to smoking habits during
subsequent follow-up period
Emigrated or made dramatic changes to smoking habits during
follow-up
Spending <50% of work day on functions outdoors
Asthma diagnosed before age 18; asthma (diagnosis as adult) or
CB/EM without symptoms in last year
Disabled subjects eligible for Medicare
Subjects for whom a proxy interview was obtained
Subjects in military or various institutions, high income families
Previous lung disease diagnosis or GOLD II at baseline, died or
severe illness during followup (5yrs)
all (general population)
parents
all (general population)
Non-white subjects
nationwide sample plus siblings of migrants to
USA still resident in Norway
HAMMO2 household members
Subjects in institutions or military service, migrant workers and
similar subjects who would be difficult to trace, households in
which no-one was aged at least 45 years
-27-
REF
Population
HARDIE all (general population)
HARIKK all (general population)
HARRIS soldiers
HAWTHO Occupational groups (from industry, not
Medical exclusionsa
Other exclusions
Baseline FEV1 <65% predicted, asthma, acute bronchitis,
bronchiectasis, baseline diagnosis of COPD (with or without
abnormal spirometry)
Proven pulmonary tuberculosis or bronchial asthma
Non-whites
otherwise specified) and census-identified
sample
HAYES
parents
HEDMAN
HIGGI2
HIGGI3
HIGGI4
HIGGI6
HIRAYA
HO
HOLLA2
HOLLNA
HOUSE
all (general population)
all (general population)
all (general population)
all (general population)
all (general population)
all (general population)
long-term residents
HOZAWA
HRUBEC
HUCHON
HUHTI1
HUHTI2
all (general population)
military veterans and twins
household members
all (general population)
long-term residents
HUHTI3
ITABAS
JACOBS
JAENDI
JENSEN
all (general population)
all (general population)
all (general population)
clinic or GP patientsb
clinic or GP patientsb
telephone company employees
Prolonged occupational exposure to coal dust, cutting oils,
asbestos, mine dust, smelter fumes or raw cotton dust
TB, bedridden from stroke, incapable of participating
Recent cardiac infarction
Subjects who had worked in mining or other dusty occupation
Sickness + absence from work on day of survey
all (general population)
parents
Lived in community <2 years, occupational exposure to irritating
fumes, dusts or aerosols
race other than white or African American
Non-whites
history of CHD or stroke
TB and "other" respiratory diseases
TB and other respiratory diseases, excluding asthma and
emphysema
TB and other respiratory diseases, but not emphysema or asthma
Asthma
Started or restarted smoking in last 10 years
Airway infection within previous 2 weeks, asthma with at least
20% increase in FEV1 after terbutaline inhalation
JINDA2 household members
JOHANN long-term residents
employees at machine tool factory and woollen
JOSHI
hosiery mill
JOUSI1
KACHEL
KAHN
KAHN2
KARAKA
all (general population)
Reported history of MI or stroke before survey
workers at 5 factories
military veterans
military veterans
all (general population)
Non-whites
Non-whites
History of heart disease, asthma or episodic wheezing in childhood
or adulthood, or other respiratory diseases (e.g. bronchiectasis, TB)
-28-
REF
Population
KATANC whites from Medicare, blacks from general
population
Medical exclusionsa
Difficulty in walking quarter of mile, climbing 10 steps without
resting or performing basic activities of daily living, need of
assistive walking device, active treatment for cancer in previous 3
years
KATO
all (general population)
KHOURY Relatives of COPD cases (cases having been
Other exclusions
Planning to move out of study area in next 3 years
Non-whites
identified through Johns Hopkins Hospital
respiratory laboratory), relatives of lung cancer
and non-pulmonary patients, or communitybased samples (neighbours and teachers)
KIM
KIRAZ
household members
KOJIMA
KOTAN1
KOTAN2
KRZYZA
KUBIK
KULLER
LAI
LAM1
LAM2
LAM3
LAMBER
all (general population)
all (general population)
all (general population)
all (general population)
all (general population)
self-selected volunteers
all (general population)
LANGE
LANGE2
LANGHA
LAVECC
LEBOWI
all (general population)
all (general population)
all (general population)
household members
household members
LEE
LIAW
siblings of migrants
self-selected volunteers
LINDBE
LINDST
LIU1
LIU2
long-term residents
all (general population)
all (general population)
all (general population)
rural group using biomass cookers and urban
group using fuel oil
KLAYTO employees at 2 research facilities
Subjects with MZ phenotype
Asthma and TB
Died during study period
employees in a machine factory
military veterans
military veterans
household members
LUNDB1 long-term residents
LUNDB2 all (general population)
COPD at baseline
Subjects with unknown daily smoking amount, and occasional
smokers
Non-whites and Mexican-Americans, subjects with <6 months full
time employment history and men with occupational exposure for
COPD endpoint only
Restricted to siblings of migrants to USA
Previous history cancer or major diseases (eg cardiovascular
disease, diabetes mellitus, hypertension)
Died during follow-up
Subjects born outside the years 1919-20, 1934-5 and 1949-50
neurological disease, serious arteriosclerosis, chest or eye surgery
in last 2 months, detached retina, acute respiratory infection
Subjects born outside the years 1919-20, 1934-5 and 1949-50
a
-29-
REF
MADOR
MAGNUS
MANFRE
MANNI1
Population
military veterans
all (general population)
all (general population)
all (general population)
MANNI2
MANNI3
MARAN1
MARAN2
household members
household members
all (general population)
all (general population)
MARCUS
MATHES
MELLST
MENEZ1
MENEZ2
Japanese ancestry
all (general population)
all (general population)
household members
household members
MENEZ3 household members
MENEZ4 household members
MENEZ5 household members
MENEZ6 household members
MEREN
MILLER
MILNE
MOLLER
MONTNE
MUELLE
NAWA
NEJJAR
NIEPSU
NIHLEN
NILSSO
OGILVI
OMORI
all (general population)
household members
all (general population)
all (general population)
all (general population)
household members
Medical exclusionsa
Significant underlying diseasea
Other exclusions
Restricted to subjects aged 50 and 80 years
Exposure to grain in farming
Recent chest/abdominal surgery, heart attack, angina or congestive Subjects who classified their race as neither black nor white
heart failure
Subjects with COPD (GOLD)
Upper respiratory tract infection on day of study
Upper respiratory tract infection on day of study, died during study
period
a
Mental disease,thoracic/abdominal surgery,MI,eye surgery,
hospitalization for any cardiac problem, current TB, pregnancy,
heart rate >120 beats/minute
Mental disease,thoracic/abdominal surgery,MI,eye surgery,
hospitalization for any cardiac problem, current TB, pregnancy,
heart rate >120 beats/minute
Mental disease,thoracic/abdominal surgery,MI,eye surgery,
hospitalization for any cardiac problem, current TB, pregnancy,
heart rate >120 beats/minute
Mental disease,thoracic/abdominal surgery,MI,eye surgery,
hospitalization for any cardiac problem, current TB, pregnancy,
heart rate >120 beats/minute
Mental disease,thoracic/abdominal surgery,MI,eye surgery,
hospitalization for any cardiac problem, current TB, pregnancy,
heart rate >120 beats/minute
Nonwhite subjects
a
healthy workers/retired persons
household members
all (general population)
long-term residents
all (general population)
household members
all (general population)
Died during follow-up
Moved away during follow-up
Asthma or other pulmonary diseases
-30-
REF
Population
OSWAL1 general clinic patients, and civil servants
referred after repeated sickness due to
bronchitis
OSWAL2 civil servants
PANDEY all (general population)
PEAT
all (general population)
PELKON all (general population)
PEREZP
all (general population)
PETO
transport and clerical workers, and censusidentified sample
PRATT
PRICE
military veterans
all (general population)
REID
general group, and migrants from UK and
Norway
RENWIC all (general population)
RICCIO
clinic or GP patientsb
RIMING
self-selected volunteers
RYDER
SARGEA
SAWICK
SCHWAR
SHAHAB
SHARP
all (general population)
all (general population)
all (general population)
household members
all (general population)
Medical exclusionsa
Other exclusions
a
Absent from work due to sickness
Away on leave or temporary duty
Working away from home
History of asthma, died during study period
Subjects with asthma, TB, bronchiectasis, pulmonary fibrosis and
thorax deformity were excluded from CB analysis
Asthma, bronchiectasis or any respiratory diagnosis other than CB
or CAO. Radiographic abnormalities
Subjects who worked in cotton textile industry
Non-obstructive lung disease (eg sarcoidosis, TB, lung cancer),
acute symptoms suggestive of unstable heart disease
Non-whites from native-born sample
History of ischaemic heart disease, currently receiving beta
Non-white subjects
blockers, anticholinergic medications or oral steroids, evidence of
myocardial ischaemia on ECG, housebound, confused or unsuitable
for other reasons according to GP
Asthma, bronchiectasis, interstitial lung disease, acute sinusitis,
pregnancy, gastro-oesophageal reflux, positive reversibility test
Disease or abnormality detected on chest x-ray thought likely to be
cause of sputum e.g. certain tuberculous disease, lung cancer and
bronchiectasis
Coal miners
Subjects in the military services or who resided in institutions
clerical and light assembly workers at power
company
SHIMUR all (general population)
SHIN
household members
SICHLE all (general population)
SILVA
household members
SOBRAD
SPEIZE
STERLI
STJERN
all (general population)
household members
all (general population)
all (general population)
a
Lung injury or operation, cardiac disease, TB, asthma or pulmonary
neoplasms
Subjects with CB/EM at baseline, or those who underwent heart or Non-whites and Mexican-Americans
lung surgery before or during study period, subjects with
concurrent CB and emp for CB analyses only
Non-white subjects
Non-civilian and institutionalised subjects from living sample
Employees at sulphite pulp factory
-31-
REF
STROM
SUADIC
Population
long-term residents
SUTINE
TAGER
TAGER2
TANG
all (general population)
all (general population)
household members
THUN
household members
TODD
TROISI
household members
Medical exclusionsa
Other exclusions
Armed Forces, Customs service, railway,
telephone, post, banking and construction
companies
businessmen/professionals, civil servants,
general population from socially deprived area,
industrial workers
nurses
TRUPIN telephone subscribers
TSUSHI self-selected volunteers
TVERDA all (general population)
URRUTI
all (general population)
VESTBO
VIEGI1
VIEGI2
VIKGRE
all (general population)
household members
all (general population)
long-term residents
VINEIS
VOLLM1
VOLLM2
VONHER
WAGEN2
self-selected volunteers
self-selected volunteers
self-selected volunteers
all (general population)
heterogeneous population of employees from
different companies and organisations
professional/business men
WALD
WANG2 self-selected volunteers
WATSON all (general population)
WEISS
self-selected volunteers
Subjects in institutions or military service, migrant workers or
similar who would be difficult to trace, households where all
members were aged <45 years
Physician's diagnosis of chronic bronchitis or emphysema before
1980, or diagnosis of cancer except nonmelanoma skin cancer,
cardiovascular disease or diabetes at each biennial examination, or
any diagnosis of asthma
asthma, bronchiectasis, panbronchiolitis, TB
Users of cigars only or other combinations of smoking products, or
missing smoking data
Asthma related symptoms (woken in night due to lack of air or
asthma attack in last 12 months or taking asthma medication)
Self-reported asthma (at baseline or follow-up)
Presence of any pulmonary disease requiring medical attention,
Quit smoking before examination or moved away during study
history of congestive heart failure or unstable angina pectoris at
period
baseline, presence of any other severe disease at baseline or followup, died during follow-up (although no deaths were from COPD),
emphysematous lesions at baseline
Asthmaa
Subjects who worked less than 16 hours/week, temporary workers
Restricted to men with NHS numbers
History of IHD, diabetes, gastrointestinal diseasea
-32-
Smoked <=10 pack years
REF
WEN
Population
WIG
WILHEL
WILSO1
WILSO2
household members
all (general population)
household members
household members
WOJTYN
WOODS
WOOLF
XIAO
XU
YAMAGU
YUAN
ZIELI1
ZIELI2
ZIETKO
all (general population)
all (general population)
ZOIA
all (general population)
Medical exclusionsa
Other exclusions
community cohort were volunteers invited for Previous history of major disease (eg cardiovascular diseases,
screening and comprised 25% of population in diabetes mellitus, or hypertension) for community cohort only
study areas; other cohort were civil servants
and teachers in government employee
insurance scheme
Participants in 1963 survey who died before 1967
Residents of hotels, motels, hospitals, nursing homes and other
institutions
Subjects who changed smoking habit during study
employees of large commercial firms
Asthma, heart disease, obesity or chest wall deformities
all (general population)
long-term residents
long-term residents
all (general population)
self-selected volunteers
self-selected volunteers
all (general population)
History of cancer
50 "unreliable" subjects
History of asthma, bronchiectasis, TB
Patients treated with inhaled or systemic corticosteroids during the
past 3 monthsa
Did not consent to 7-day dietary assessment (65% of original
sample)
a
For case-control studies, the criteria shown apply to the cases. Additional criteria for the controls, if any, are as follows:
Normal LF. No controls reported history of lung disease or occupational exposure
COCCI
No self-reported asthma, CB or respiratory symptoms suggestive of CB or asthma
LUNDB2
Normal LF
MADOR
Normal LF and no respiratory symptoms
MATHES
Normal LF, no respiratory or cardiovascular disease
MOLLER
No pulmonary disease
OSWAL1
No respiratory disease
SHIMUR
No respiratory symptoms
WAGEN2
Normal LF and no lung disease in GP records
WATSON
No chronic or recurrent respiratory symptoms, no past history of significant pulmonary disease
ZIETKO
b
Studies with population "clinic or GP patient" have also been marked as having a study weakness (see Table 2 of paper)
-33-
Table 5
Disease outcomes - summary
Study REFs are listed in columns corresponding to the sections in Table 6, where more detail is given.
A
ICDa
B
LF only
BEST
CHEN1
DEAN1
DOLL1
DOLL2
ENSTRO
GODTFRa
HAMMO2
HAWTHO
HIGGI4
JACOBS
KAHN
KAHN2
KULLER
LAM1
LAM3
LANGE
LEE
LIAW
LIU1
MANNI3
MARCUS
NILSSO
PETO
SPEIZE
STERLI
TANG
THUN
TODD
TVERDA
VINEIS
VOLLM2
WALD
WEN
YUAN
ANDER3
BEDNAR
BROGGE
CHENG
CLEMEN
DEJONG
DEMARC
DETORR
DICKIN
EKBERG
FUKUCH
GEIJER
HOZAWA
HUHTI2
HUHTI3
ITABAS
JAENDI
JOHANN
KACHEL
KATANC
KHOURY
KIM
KLAYTO
KOJIMA
KOTAN2
KRZYZA
LAI
LEBOWI
LINDBE
LIU2
LUNDB1
MADOR
MANNI1
MANNI2
MATHES
MENEZ2
MENEZ3
MENEZ4
MENEZ5
MENEZ6
MUELLE
NIEPSU
PEAT
PEREZP
PRICE
RENWIC
RICCIO
SAWICK
SHAHAB
SHIN
STROM
TAGER
TSUSHI
VESTBO
VIEGI2
WATSON
WEISS
WILSO1
WOJTYN
YAMAGU
ZIELI1
ZIELI2
ZIETKO
C
LF+
symptoms
ALESSA
COCCI
KIRAZ
SILVA
COPD
D
E
COPD
COPD, CB,
undefined
Emp
HO
AMIGO
LAM2
CHEN3
XIAO
KARAKA
NIHLEN
TRUPIN
-34-
F
CB, Emp
CHEN2
FORAST
LINDST
MONTNE
VOLLM1
VONHER
XU
G
CB, Emp,
Asthma
HARDIE
HUHTI1
H
Other
ANDER1
DONTA1
FERRI1
FERRI2
FERRI3
FIDAN
GULSVI
HARIKK
HEDMAN
MARAN1
MARAN2
PELKON
SARGEA
SICHLE
CB
I
ICDa
BEST
DOLL1
DOLL2
HIRAYA
KAHN
KAHN2
WEN
J
Diagnosis
ALDERS
BANG
BROWN
COLLEG
DONTA2
ENRIGH
HARDIE
KOTAN1
LEBOWI
MILLER
SCHWAR
TROISI
VIEGI1
WILSO2
K
Self-report
HO
KATO
LAVECC
L
Symptoms
ANDER1
BECK1
BECK2
BJORNS
CERVER
CHAPMA
COATES
DEAN2
DEANE
DEMARC
DOPICO
EHRLIC
FERRI1
FINKLE
FLETCH
FOXMAN
GOLDBE
HAENSZ
HARRIS
HAWTHO
HAYES
HIGGI2
HIGGI3
HIGGI6
HOLLA2
HOLLNA
HOUSE
HRUBEC
HUCHON
HUHTI1
HUHTI2
HUHTI3
JINDA2
JOSHI
JOUSI1
KUBIK
LAMBER
LANGE2
LANGHA
LINDST
MAGNUS
MANFRE
MENEZ1
MEREN
MILNE
MOLLER
MUELLE
NEJJAR
OGILVI
OSWAL1
OSWAL2
PANDEY
PEREZP
REID
RIMING
SAWICK
SHARP
SOBRAD
STJERN
SUADIC
TAGER2
URRUTI
WAGEN2
WILHEL
WOJTYN
WOODS
WOOLF
YAMAGU
ZOIA
-35-
M
Other
JENSEN
KIRAZ
LUNDB2
MELLST
PELKON
SHIMUR
SILVA
WIG
Emphysema
O
P
Q
R
Visual
Diagnosis
Self-report
Other
Comparison
BEST
ANDER2
DONTA2
HO
HUHTI1
HAMMO2
AUERBA
ENRIGH
LAVECC
SILVA
HIRAYA
NAWA
GULSVI
KAHN
OMORI
HARDIE
KAHN2
PRATT
HOZAWA
WEN
RYDER
LEBOWI
SUTINE
MILLER
VIKGRE
WILSO2
WANG2
WEISS
Outcomes based on ICD codes are mortality studies, with the exception of GODTFR (COPD) which is incidence.
N
ICDa
a
-36-
Disease outcomes – detailed
Table 6
Sections in this table correspond to the columns in Table 5, and footnotes are given at the end of each section.
Table 6A : COPD based on ICD
REF
Outcome type
ICD7a ICD8 a ICD9 a ICD10 a Defn
DIAGSC a Description of disease
incl
asthma
Source of diagnostic information
BEST
CHEN1
mortality
mortality
3
-
-
6
-
No
Yes
c
Mixed
Bronchitis/emphysema mortality (ICD7 500-02,527.1)
COPD : ICD 9 490-496
DEAN1
DOLL1
mortality
mortality
9
6
-
9
-
Yes
Unkn
c
c
DOLL2
ENSTRO
GODTFR
HAMMO2
HAWTHO
HIGGI4
mortality
mortality
incidence
mortality
mortality
mortality
9
5
3
-
6
2
6
-
6
9
2
-
Unkn
Yes
No
No
Yes
Unkn
c
c
r
c
c
c
JACOBS
mortality
-
9
-
-
Unkn
Mixed
Chronic bronchitis (sic): ICD 8 490-493
COLD: ICD 7 or ICD 9 (underlying cause, codes unspecified but
includes chronic bronchitis and emphysema)
Chronic bronchitis and emphysema: ICD 7 (codes unspecified)
COPD (ICD 7: 241, 500-2, 527.1; ICD 8: 490-3; ICD 9: 490-6)
First hospitalisation for COPD (ICD 8: 490-492 or ICD 10: J40-J44)
COPD: ICD 7 500-502, 527.1
Chronic bronchitis (sic) (ICD 8: 490-493)
Underlying or contributing COPD (ICD 9: codes unspecified. Probably
CB,EM,COPD and asthma as shown in Table 3 of HIG GIN1989)
COPD (ICD 8: codes unspecified)
Death records of Dept of Veterans Affairs
Death certificates (supplemented if necessary by hospital records and
inquiry of family members and factory medical staff)
Death certificates
Death certificates
KAHN
mortality
2
-
-
-
No
c
KAHN2
KULLER
LAM1
LAM3
LANGE
LEE
LIAW
LIU1
mortality
mortality
mortality
mortality
mortality
mortality
mortality
mortality
3
6
-
2
-
6
6
9
3
9
-
No
Yes
Yes
Unkn
No
No
Unkn
No
c
c
Mixed
r
c
c
c
Mixed
Underlying COPD (ICD 7:501-502,527.1 from 1954-68; 501-502,
527.1, 527.2 from 1969-80). ICD code 500 (acute bronchitis) was
additionally included only in dose-related analyses of current smoking
by amount smoked
Underlying COPD (ICD 7: 500-502, 527.1)
COPD (ICD9 490-496) underlying cause of death
COPD (ICD 9: 490-496)
COPD (ICD 10, codes unspecified)
COPD underlying or contributing mortality (490-2)
CNSLD (ICD 7 502=CB, 526=Bronchiectasis, 527.1= emphysema)
ICD9-COPD (codes unspecified)
COPD (ICD 9):ICD 9 (490, 491, 492, 496 and 416.7)
MANNI3
mortality
-
-
6
-
Yes
c
COPD (ICD 9: 490-496) as underlying cause
-37-
Death certificates
Death certificates
Hospital admission and discharge diagnoses
Death certificates
Mortality registry
Death certificates
Death certificates, medical records, interview with physicians and
relatives of deceased
Death certificates
Death certificates
Death certificates
Medical records, death certificates
Hospital records
Death register
Death certificate
Computerized national mortality register
Local administrative records, supplemented by medical records and
discussions with health workers and family
Death certificates
REF
Outcome type
MARCUS mortality
NILSSO
PETO
SPEIZE
STERLI
TANG
THUN
TODD
TVERDAb
mortality
mortality
mortality
mortality
mortality
mortality
mortality
mortality
VINEIS
VOLLM2
WALD
WEN
YUAN
mortality
mortality
mortality
mortality
mortality
ICD7a ICD8 a ICD9 a ICD10 a Defn
DIAGSC a Description of disease
incl
asthma
8
Yes
c
COPD (ICD 8: 490-493, 518, 519.3) underlying or contributory. (ICD8
519.3 is defined by MARCUS as chronic obstructive disease not
elsewhere classified, although this code is not listed in the ICD8
Manual)
2
No
c
Bronchitis and emphysema (ICD 8: 490-492)
4
No
c
COPD (ICD 8: 490-492,519)
6
Yes
c
COPD (ICD 9: 490-496)
2
No
c
COPD (ICD 9: 490-492, 496)
a
No
c
chronic obstructive lung disease ICD-8 491-492,519
2
No
c
COPD (ICD 9: 490-492, 496)
6
No
c
CNSLD (ICD 7 502=CB, 526=Bronchiectasis, 527.1= emphysema)
7
a
Yes
c
Asthma, bronchitis and emphysema (underlying, ICD 8, 466, 490-493;
ICD 9: 466, 490-493)
9
Unkn
c
COPD or emphysema (ICD 10, no codes specified)
6
Yes
c
Underlying and contributory COPD (ICD 9: 490-496)
8
No
c
COPD (ICD 9: 416,491,492,496,519)
1
No
c
CB (ICD9 491), Emphysema (ICD9 492) or CAO (ICD9 496)
6
Yes
c
COPD (ICD 9: 490-496)
Source of diagnostic information
Hospital records, death certificates
Death certificates
Death certificates
Death certificates
Death certificates
Death certificates
Death certificates
Death certificates
Death certificates
Cancer and mortality registries
Death certificates
Mortality register
Computerized national mortality register
Death certificates
a
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
b For study TVERDA, this COPD outcome was accepted despite lacking the core condition ICD9-496. As the study follow-up period was 1972 to 1988, and Norway adopted the 9th revision in
1986, the 8th revision was in force for the majority of the study. As code 496 only gradually came to be used for COPD, it is unlikely that omission of this code for the final 3 years of the study
would have had much impact.
Table 6B : COPD based on LF (lung function) only
REF
Outcome type
Diagnostic
Criteriaa
LUNGFNb SPBRONc Description of disease
Source of diagnostic information
ANDER3
BEDNAR
BROGGE
CHENG
CLEMEN
prevalence
prevalence
prevalence
prevalence
prevalence
ATS
BTS
GOLD
unspec
unspec
q
2
n
2
a
no/unkn
no/unkn
post
no/unkn
no/unkn
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
DEJONG prevalence
DEMARC prevalence
GOLD
GOLD
2
2
no/unkn
no/unkn
COPD (ATS criteria NOS)
COPD/airflow limitition (ERS FEV1/FVC<70%)
COPD (GOLD II postbronc'r FEV1/FVC<70% FEV1<80%pr)
FEV1/FVC < 70%
Reduced FEV1 and/or VC (<70% predicted at least once and average below normal)
Endpoint not originally defined as COPD, but based on FEV1 and/or VC value
<70% predicted, with average over the study period also below normal
Obstructive lung disease (FEV1/FVC <70%)
COPD (FEV1/FVC <70% = GOLD 2001 I-IV)
-38-
Spirometry
Spirometry
LUNGFNb SPBRONc Description of disease
Source of diagnostic information
prevalence
Diagnostic
Criteriaa
GOLD
2
post
Spirometry
DICKIN
EKBERG
FUKUCH
GEIJER
HOZAWA
HUHTI2
HUHTI3
ITABAS
JAENDI
JOHANN
KACHEL
KATANC
prevalence
prevalence
prevalence
incidence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
Van Schayck
GOLD
GOLD
GOLD
unspec
unspec
unspec
ATSd
unspec
GOLD
unspec
ATS
f
2
2
n
p
7
7
5
n
2
n
5
revers
no/unkn
no/unkn
post
no/unkn
no/unkn
no/unkn
no/unkn
post
post
no/unkn
no/unkn
KHOURY
KIM
KLAYTO
KOJIMA
KOTAN2
KRZYZA
LAI
LEBOWI
LINDBE
LIU2
LUNDB1
MADOR
MANNI1
MANNI2
MATHES
MENEZ2
MENEZ3
MENEZ4
MENEZ5
MENEZ6
MUELLE
NIEPSU
PEAT
prevalence
prevalence
prevalence
prevalence
prevalence
incidence
prevalence
prevalence
incidence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
unspec
GOLD
unspec
GOLD
GOLD
unspec
GOLD
unspec
GOLD
Chinese
GOLD
ATS
unspec
GOLD
GOLD
GOLD
GOLD
GOLD
GOLD
GOLD
unspec
GOLD
unspec
k
2
h
2
2
b
2
8
2
2
2
5
3
2
n
2
2
2
2
2
l
2
6
no/unkn
no/unkn
no/unkn
no/unkn
post
no/unkn
no/unkn
no/unkn
no/unkne
post
reverse
no/unkn
no/unkn
no/unkn
no/unkn
post
post
post
post
post
no/unkn
no/unkn
no/unkn
PEREZP
PRICE
prevalence
prevalence
unspec
GOLD
9
2
no/unkn
post
REF
Outcome type
DETORR
Post-bronchodilator FEV1/FVC <0.7 (Patients with documented positive
bronchodilator response were excluded))
COPD (FEV1 <5th centile + reversibility <9%)
COPD (GOLD criteria FEV1/FVC<70%)
Airflow limitation (FEV1/FVC <70%)
Incident GOLD II FEV1/FVC<70% FEV1<80%pred)
FEV1 <85% predicted
Chronic airflow obstruction (FEV1% < 60)
Chronic obstructive lung disease (FEV% < 60)
COPD (abnormal expiratory flow for several months)
post-bronchodilator FEV1/FVC<70% and FEV1<80%pred
COPD (post-bronchodilator FEV1/FVC<0.7 =GOLD I-IV)
Airflow limitation (FEV1/FVC <0.70, FEV1 <80%pred)
Obstructive airway disease (ATS criteria: reduced FEV1/FVC and FEV1 <100%
predicted)
Airways obstruction (FEV1/FVC <68%)
COPD (FEV1/FVC <70%)
COPD (FEV1 or MMEF rate <2 SD below predicted)
COPD (FEV1/FVC <70%)
Post-bronchodilator FEV1/FVC <0.7
COPD (FEV1 <65% predicted)
prebronchodilator FEV1/FVC <70%
Predicted FEV1/FVC <80%
COPD (GOLD modified no bronchodilator)e
post-bronchodilator FEV1/FVC <70%
COPD (GOLD postbronchodilator FEV1/FVC<70%)e
COPD (ATS, FEV1 <70%)
Low lung function (FEV1/FVC <0.7 and FEV1 <80%) predicted
COPD (FEV1/FVC <0.7)
FEV1/FVC <0.7 and FEV1 <80% predicted
COPD (postbronchodilator FEV1/FVC <0.7)
COPD (postbronchodilator FEV1/FVC <0.7)
COPD (postbronchodilator FEV1/FVC <0.7)
COPD (postbronchodilator FEV1/FVC <0.7)
COPD (postbronchodilator FEV1/FVC <0.7)
Chronic airway obstruction (FEV1/FVC < 60%)
COPD (GOLD 2001 criteria)
Chronic airflow limitation (FEV1/FVC <65% or FEV1 <65% predicted in at least
two surveys. If age >75 CAL started before age 75 or also FEV1 <65% predicted)
Chronic airway obstruction (FEV1 <75% predicted)
Postbronchodilator FEV1/FVC <0.70
-39-
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
spirometry
Spirometry
Spirometry
LUNGFNb SPBRONc Description of disease
Source of diagnostic information
prevalence
Diagnostic
Criteriaa
Enright
g
no/unkn
Spirometry
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
GOLDf
unspec
Mixed
ATS
unspec
unspec
GOLD
GOLD
unspec
BTS
unspec
GOLD
unspec
unspec
ERS
GOLD
ERS
2
l
2
r
2
b
2
2
2
3
u
2
2
k
4
2
t
no/unkn
no/unkn
no/unkn
no/unkn
no/unkn
no/unkn
post
no/unkn
no/unkn
no/unkn
no/unkn
revers
no/unkn
no/unkn
no/unkn
no/unkn
revers
REF
Outcome type
RENWIC
RICCIO
SAWICK
SHAHAB
SHIN
STROM
TAGER
TSUSHI
VESTBO
VIEGI2
WATSON
WEISS
WILSO1
WOJTYN
YAMAGU
ZIELI1
ZIELI2
ZIETKO
Chronic airways obstruction (FEV1/FVC <65% for subjects aged <65 years,
predicted and lower limit of normal FEV1/FVC calculated for those aged 65+ years
by Enright formula)
Bronchial obstruction (GOLD criteria)f
FEV1/FVC <60%
ATS/ERS FEV1/FVC <0.7
Airway obstruction (FEV1/FVC <75%)
Airflow limitation (FEV1/VC <70%)
Obstructive airways disease (FEV1 <65% predicted)
Post-beta2 stimulant FEV1/FVC <70%
COPD (GOLD stage 1+ FEV1/FVC <0.7)
COPD ('clinical' criteria FEV1/FVC<70%)
BTS (FEV1<=80%pred and FEV1/FVC <=70%pred)
COPD (FEV1 > 2 SE below mean predicted for height)
COPD (GOLD FEV1/FVC <70.0%)
FEV1/FVC<70% at both baseline and 5-year follow-up
Airways obstruction (FEV1/FVC <68%)
Bronchial obstruction (ERS: FEV1/FVC<85% pred)
Airflow limitation (Gold: FEV1/FVC <0.7)
COPD (ERS criteria: FEV1/FVC <70%, FEV1 <80% predicted, <12% reversibility)
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
Spirometry
a
As named by original author.
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
c Field SPBRON refers to spirometry used post-bronchodilator, no (=without bronchodilator) or unknown, and reversibility criteria.
d Reference given for definition of disease status relates to ATS document, so it is assumed these criteria were used.
e Although Lundbäck (2003) [185] states that GOLD criteria were applied to values after reversibility test, Lindberg (2006) [180] (describing both baseline and follow-up) states that no
reversibility test was performed.
f Bronchodilator was used and reversibility is mentioned but it is not clear how it relates to use of the GOLD criteria.
b
Table 6C : COPD based on LF and symptoms
REF
Outcome type Diagnostic
Criteriaa
DIAGSCb
Questionnaire LUNGFN
SPBRON Description of disease
Source of diagnostic information
ALESSA
prevalence
unspec
Mixed
-
2
no/unkn
Clinical history, physical examination, x-ray, ECG, spirometry
COCCI
prevalence
ERS
s
-
4
no/unkn
COPD (attending outpatients with CB and irreversible AO, clinically
confirmed as COPD and FEV1/FVC < 70% predicted)
COPD (hospitalized for COPD and FEV1/VC <88% predicted)
-40-
Not stated, but spirometry results available
REF
KIRAZ
Outcome type Diagnostic
Criteriaa
prevalence
unspec
SILVA
incidence
ATSc
DIAGSCb
Questionnaire LUNGFN
SPBRON Description of disease
Source of diagnostic information
Mixed
MRC/ATS
e
revers
Questionnaire: ATS/MRC, physical examination, spirometry
Mixed
NHLI
i
no/unkn
COPD (chronic bronchitis, decreased respiratory sounds or increased
expiration time on physical examination, FEV1/FVC <88% predicted
and reversibility <12%)
COPD (chronic bronchitis (cough/phlegm for 3 months for 2
consecutive years) and/or physician-diagnosed emphysema, and FEV1
or DLCO <80% predicted)
Questionnaire, spirometry
a
As named by original author.
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
c ATS criteria refers to chronic bronchitis part only.
b
Table 6D : COPD not further defined
REF
Outcome type
Diagnostic
Criteriaa
DIAGSCb Defn
Description of disease
incl
asthma
Source of diagnostic information
HO
LAM2
XIAO
prevalence
prevalence
prevalence
unspec
unspec
unspec
Mixed
q
Mixed
Questionnaire and physician diagnosis
Questionnaire
Spirometry, x-ray, CT scan, blood gases
Unkn
Unkn
Unkn
COPD (physician diagnosis)
Chronic obstructive pulmonary disease (criteria unspecified)
Hospital patients with COPD (unspecified criteria)
a
As named by original author.
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
b
Table 6E : COPD defined as COPD, CB or Emphysema
REF
Outcome type
Diagnostic
Criteriaa
DIAGSCb Questionnaire
LUNGFNb SPBRONc Description of disease
Source of diagnostic information
AMIGO
incidence
GOLDd
r
-
2
no/unkn
Clinical diagnosis (unspecified)
CHEN3
prevalence
KARAKA prevalence
unspec
Mixed
q
Mixed
unnamed/unsp
unnamed/unsp
4
no/unkn
NIHLEN
TRUPIN
unspec
unspec
d
d
OLIN
unnamed/unsp
-
incidence
prevalence
Clinical diagnosis of COPD in last 2 years, GOLD 2001, (said to be
equivalent to ICD J44.8-44.9 which includes chronic bronchitis and
pulmonary emphysema)d
COPD (either emphysema, CB or COPD) starting from age 25
COPD (ERS criteria=FEV1/VC<88% pred M, 89% pred F) and/or
chronic bronchitis (chronic cough and chronic phlegm for 3 months for
at least 2 years) and/or physician diagnosed CB, emphysema or COPD)
Chronic bronchitis and/or emphysema and/or COPD
COPD (physician diagnosis of chronic bronchitis, emphysema or
COPD)
-41-
Questionnaire
Questionnaire, spirometry, physician diagnosis
Questionnaire: physician diagnosed
Questionnaire
a
As named by original author.
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
c Field SPBRON refers to spirometry used post-bronchodilator, no (=without bronchodilator) or unknown, and reversibility criteria.
d Disease definition is unclear as it mentions both clinical diagnosis and GOLD 2001. It also states that ICD J44.8-44.9 include chronic bronchitis and pulmonary emphysema which they do not.
b
Table 6F : COPD defined as CB or Emphysema
REF
Outcome type
Diagnostic
Criteriaa
DIAGSCb Questionnaire
Description of disease
Source of diagnostic information
CHEN2
FORAST
LINDST
MONTNE
VOLLM1
VONHER
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
unspec
unspec
unspec
unspec
unspec
unspec
d
d
d
q
d
Mixed
unnamed/unsp
ATS/NHLBI
FinEsS
OLIN
MRC
unnamed/unsp
XU
prevalence
MRC
d
unnamed/unsp
COPD (physician diagnosis of chronic bronchitis or emphysema)
Chronic bronchitis/emphysemac
Physician diagnosed chronic bronchitis/emphysema
Self-reported chronic bronchitis and/or emphysema
Chronic bronchitis and/or emphysema
Examining physician's assessment of CB (=cough and phlegm for at
least 3 months for 2 consecutive years excluding other explanations) or
emphysema
COPD (physician diagnosed chronic bronchitis or emphysema
Questionnaire
Questionnaire: physician-diagnosed in last yearc
Questionnaire: FinEsS, physician diagnosis
Questionnaire
Questionnaire: physician diagnosed
Screening (questionnaire, spirometry, x-ray) confirmed by clinical
examination by physician. (Spirometry only used for severity, not for
case status)
Questionnaire (verified from medical records)
a
As named by original author.
b Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
c The outcome categories as defined originally (adult asthma diagnosed, CB/EM, asthma-like symptoms without diagnosis) were stated to be mutually exclusive, so it is assumed that no subject
had both asthma and CB/EM. It is stated that CB/EM diagnosis was in last year, but it seems more likely that this means ever-diagnosed and disease active in last year. Results used refer to
CB/EM versus all others. However no information is available on subjects with a history of inactive respiratory disease (diagnosis but no symptoms in last year, 68 subjects) or with childhood
asthma (diagnosed before age 18, 18 subjects) so those subjects are omitted.
Table 6G : COPD defined as CB, Emphysema or AST
REF
Outcome type
Diagnostic
Criteriaa
Defn
DIAGSCb Questionnaire
incl
asthma
Description of disease
HARDIE
HUHTI1
prevalence
prevalence
unspec
unspec
Yes
Yes
Chronic bronchitis, emphysema or asthma (physician-diagnosed)
Questionnaire: ATS
Chronic non-specific lung disease (CB (phlegm most days for 3 months Spirometry, x-ray and questionnaire
for 2 years), emphysema (FEV/FVC <60% or FEV/FVC <70% and xray changes) and/or asthma)
a
d
Mixed
ATS
MRC
As named by original author.
-42-
Source of diagnostic information
b
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
Table 6H : COPD other
REF
Outcome type
Diagnostic
Criteriaa
Defn
DIAGSCb
incl
asthma
Questionnaire
LUNGFNb SPBRONc Description of disease
Source of diagnostic information
ANDER1
prevalence
unspec
Yesd
Mixed
Harvard
l
DONTA1
prevalence
MRC
Yes
Mixed
MRC
-
FERRI1
prevalence
Mixed
Yes
Mixed
MRC
l
no/unkn
Questionnaire: Harvard, and
spirometry
Questionnaire, physical
examination
Questionnaire, spirometry
FERRI2
prevalence
Mixed
Yes
Mixed
MRC
l
no/unkn
FERRI3
prevalence
Mixed
Yes
Mixed
MRC
l
no/unkn
FIDAN
prevalence
unspec
No
Mixed
ATS
2
no/unkn
GULSVI
prevalence
unspec
No
Mixed
unnamed/unsp
j
no/unkn
HARIKK
incidence
Mixed
No
Mixed
ATS
2
no/unkn
HEDMAN prevalence
unspec
No
d
NHS
-
MARAN1 prevalence
Thai
No
Mixed
-
d
revers
MARAN2 incidence
Thai
No
Mixed
-
d
revers
PELKON
Mixed
Unkn
Mixed
-
2
no/unkn
incidence
no/unkn
Obstructive lung disease (wheezing most days or nights, dyspnea
walking at own pace on level, or FEV1/FVC <60%) or asthma
Chronic bronchitis and/or emphysema, or other lung diseases (5% of
subjects)
Chronic non-specific respiratory disease (chronic bronchitis (phlegm for
3+ months for previous 3 years), asthma (physician-diagnosed) or
chronic obstructive pulmonary disease (wheezing/whistling in chest
most days/nights, breathlessness while walking at own pace, and/or
FEV1/FVC <60%))
Chronic non-specific respiratory disease (chronic bronchitis (phlegm for
3+ months for previous 3 years), asthma (physician-diagnosed) or
chronic obstructive pulmonary disease (wheezing/whistling in chest
most days/nights, breathlessness while walking at own pace, and/or
FEV1/FVC <60%))
Chronic non-specific respiratory disease (chronic bronchitis (phlegm for
3+ months for previous 3 years), asthma (physician-diagnosed) or
chronic obstructive pulmonary disease (wheezing/whistling in chest
most days/nights, breathlessness while walking at own pace, and/or
FEV1/FVC <60%))
Airway disease (chronic bronchitis and/or pathologic signs in
auscultation and at least two respiratory symptoms and/or FEV1/FVC
<70%)
COLD (chronic bronchitis with obstruction, emphysema, asthmatic
bronchitis, obstructive lung disease further classification not possible)
COPD (emphysema, chronic bronchitis, chronic airways obstruction
and FEV1/FVC <70%)
COPD : Doctor diagnosed COPD
Questionnaire, spirometry
Questionnaire, spirometry
Questionnaire: ATS, physical
examination, spirometry
Questionnaire, physical
examination, lung function, chest
x-ray
Questionnaire, physical
examination, spirometry, chest xray
Questionnaire: physiciandiagnosed
Spirometry, x-ray
COPD (FEV1/FVC <70%, reversibility of <15%), no x-ray
abnormalities
COPD (FEV1/FVC <70%, reversibility of <15%), no x-ray
Spirometry, x-ray
abnormalities
Incident FEV1/FVC <70% persisting at all subsequent examinations, or Spirometry at 5-yearly examination
COPD mortality (ICD codes not specified)
or death cert
-43-
Questionnaire
LUNGFNb SPBRONc Description of disease
unspec
Defn
DIAGSCb
incl
asthma
Yes
Mixed
unnamed/unsp
3
no/unkn
Mixed
No
MRC
3
no/unkn
REF
Outcome type
Diagnostic
Criteriaa
SARGEA
prevalence
SICHLE
prevalence
Mixed
Source of diagnostic information
Obstructive airways disease (physician-diagnosed bronchitis,
Questionnaire: physician
emphysema or asthma, or FEV1 <80% predicted and FEV1/FVC<70%) diagnosed, spirometry
COPD (BTS criteria from spirometry and/or MRC criteria for chronic Spirometry, questionnaire: MRC
bronchitis from questionnaire)
a
As named by original author.
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
c
Field SPBRON refers to spirometry used post-bronchodilator, no (=without bronchodilator) or unknown, and reversibility criteria.
d Cases of pure asthma (i.e. without OLD) were very rare, 0.4% of males and 0.7% of females.
b
Table 6I : CB based on ICD
REF
Outcome type
ICD7a ICD8a ICD9a ICD10a DIAGSCa Description of disease
Source of diagnostic information
BEST
DOLL1
DOLL2
HIRAYA
KAHN
KAHN2
WEN
mortality
mortality
mortality
mortality
mortality
mortality
mortality
7
9
9
7
7
7
-
Death records of Dept of Veterans Affairs
Death certificates
Death certificates
Death certificates
Death certificates
Death certificates
Death certificates
-
b
-
c
c
c
c
c
c
c
Bronchitis mortality (ICD7 500-502)
Chronic bronchitis (underlying cause, ICD codes unspecified)
Chronic bronchitis (underlying cause, ICD codes unspecified)
Bronchitis (ICD 500-502)
Chronic bronchitis deaths (underlying) (ICD7 500-502)
Underlying chronic bronchitis deaths (ICD 7: 500-502)
Chronic bronchitis (ICD 9: 491)
a
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
Table 6J : CB based on diagnosis
REF
Outcome type
Diagnostic
Criteriaa
DIAGSCb Questionnaire
Description of disease
Source of diagnostic information
ALDERS
BANG
BROWN
COLLEG
prevalence
prevalence
prevalence
prevalence
unspec
unspec
unspec
unspec
r
d
Mixed
Other
NHANESc
-
Hospital records (final diagnosis if available)
Questionnaire (NHANES?): physician-diagnosed
Physical examination, x-ray
Physician diagnosis
DONTA2
ENRIGH
HARDIE
KOTAN1
incidence
prevalence
prevalence
prevalence
MRC
unspec
unspec
unspec
Mixed
d
d
d
MRC
ATS
ATS
FinEsS
Chronic bronchitis: Hospital diagnosis
Chronic bronchitis: Self reported physician- diagnosed CB
Chronic bronchitis : Medical diagnosis of CB
Chronic bronchitis (diagnosed by physician using standard
questionnaire)
Clinical diagnosis of chronic bronchitis (using MRC criteria)
Chronic bronchitis (physician-diagnosed)
Current physician-diagnosed chronic bronchitis
Chronic bronchitis (physician-diagnosed)
-44-
Questionnaire, physical examination, spirometry
Questionnaire: ATS
Questionnaire: ATS
Questionnaire: FinEsS
DIAGSCb Questionnaire
Description of disease
Source of diagnostic information
prevalence
prevalence
Diagnostic
Criteriaa
unspec
unspec
d
Other
NHLI
-
Questionnaire: NHLI
Physical examination; physician diagnosis, criteria unspecified
prevalence
incidence
prevalence
prevalence
unspec
unspec
unspec
unspec
d
d
d
d
NHANES
NHS
NHLBI
HealthOmnibus
Chronic bronchitis (physician diagnosed)
Chronic bronchitis (examining physician's impression of chronic
bronchitis)
Bronchitis (ever diagnosed by physician and still has condition)
Chronic bronchitis (CB based on physician diagnosis)
Chronic bronchitis (confirmed by physician)
Bronchitis (physician-diagnosed)
REF
Outcome type
LEBOWI
MILLER
SCHWAR
TROISI
VIEGI1
WILSO2
Questionnaire: physician diagnosed
Questionnaire: physician diagnosed
Questionnaire: physician diagnosed
Questionnaire: Health Omnibus Survey
a
As named by original author.
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
c Assumed that HHANES used same questionnaire as NHANES studies.
b
Table 6K : CB based on self-report
REF
Outcome type
Diagnostic
Criteriaa
DIAGSCb Questionnaire
Description of disease
Source of diagnostic information
HO
KATO
LAVECC
prevalence
prevalence
prevalence
unspec
unspec
unspec
q
q
q
Chronic bronchitis (self-reported)
History of chronic bronchitis (criteria unspecified)
Chronic bronchitis (self-reported)
Questionnaire (unnamed)
Questionnaire (unspecified)
Questionnaire
unnamed/unsp
unnamed/unsp
unnamed/unsp
a
As named by original author.
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
b
Table 6L : CB based on symptoms
REF
Outcome type
Diagnostic
Criteriaa
DIAGSCb Questionnaire
Description of disease
Source of diagnostic information
ANDER1
prevalence
unspec
q
Harvard
Questionnaire: Harvard
BECK1
BECK2
BJORNS
prevalence
incidence
prevalence
MRC
MRC
unspec
q
q
q
unnamed/unsp
unnamed/unsp
MRC/ECRHS
CERVER prevalence
CHAPMA prevalence
COATES prevalence
MRC
unspec
MRC
q
q
q
ECRHS
MRC
MRC
Chronic bronchitis (phlegm on 4 days/week for 3 months/year for 3
years)
Chronic bronchitis (cough and phlegm for 3 months for at least 2 years)
Chronic bronchitis (cough and phlegm for 3 months for at least 2 years)
Bronchitis symptoms (phlegm and long-term cough and/or morning
cough in recent years)
Chronic bronchitis (cough and phlegm most days for at least 2 years)
Persistent cough and phlegm (for at least 3 months every year)
Chronic bronchitis (combined chronic cough and phlegm on most days
-45-
Questionnaire
Questionnaire
Questionnaire: ECRHS/MRC
Questionnaire: ECRHS
Questionnaire: MRC
Questionnaire: MRC
REF
Outcome type
Diagnostic
Criteriaa
DIAGSCb Questionnaire
DEAN2
prevalence
unspec
q
MRC
DEANE
prevalence
DEMARC prevalence
unspec
unspec
q
q
MRC
MRC/ECRHS
DOPICO
prevalence
unspec
q
ATS
EHRLIC
prevalence
MRC
q
unnamed/unsp
FERRI1
prevalence
unspec
q
MRC
FINKLE
FLETCH
prevalence
prevalence
MRC
unspec
q
q
MRC
unnamed/unsp
FOXMAN
GOLDBE
HAENSZ
HARRIS
HAWTHO
HAYES
HIGGI2
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
unspec
MRC
MRC
unspec
MRC
MRC
unspec
q
q
q
q
q
q
q
WHO
MRC
MRC
MRC
MRC
MRC
unnamed/unsp
HIGGI3
prevalence
unspec
q
unnamed/unsp
HIGGI6
HOLLA2
prevalence
prevalence
unspec
unspec
Mixed
q
unnamed/unsp
MRC
HOLLNA
prevalence
MRC
q
unnamed/unsp
HOUSE
prevalence
MRC
q
MRC
HRUBEC
prevalence
MRC
q
MRC
HUCHON prevalence
HUHTI1
prevalence
unspec
MRC
q
q
ECSC
MRC
HUHTI2
prevalence
unspec
q
MRC
HUHTI3
prevalence
unspec
q
MRC
JINDA2
prevalence
unspec
q
unnamed/unsp
Description of disease
Source of diagnostic information
for at least 3 months every year)
Bronchitis syndrome (shortness of breath, prolonged cough and
prolonged phlegm)
Chronic bronchitis (persistent cough and phlegm)
Chronic bronchitis (regular cough with phlegm for at least 3 months
every year)
Chronic bronchitis (phlegm usually daily or twice a day 4 days/week,
for 3 months of year for 2 or more years)
Chronic bronchitis (cough with phlegm for 3 months for at least 2
years)
Chronic bronchitis (phlegm on 4+ days per week for 3 months per year
for 3 years)
Chronic bronchitis (Cough and phlegm for 3+ months each year)
Chronic bronchitis (production of phlegm on rising on most days for at
least 3 months each year)
Chronic bronchitis (phlegm most days 3 months in last year)
Chronic bronchitis (cough and phlegm for 3+ months each year)
Chronic bronchitis (termed MRC but symptoms unspecified)
Chronic bronchitis: MRC questionnaire but criteria unspecified
Bronchitis syndrome (MRC but exact criteria not given)
Chronic bronchitis (Cough and phlegm for 3+ months each year)
Chronic bronchitis (persistent phlegm for at least 3 months of year + at
least 1 chest illness with increased cough and sputum during past 3
years)
Chronic bronchitis (persistent phlegm and 1+ bronchitic chest illness in
past 3 years)
Chronic bronchitis (cough and phlegm for at least 3 months each year)
Persistent cough and phlegm (assumed to be defined as cough and
phlegm, either morning or day, in winter for 3 months each year
Chronic bronchitis (cough and/or phlegm for 3 months for the past 2
years)
Chronic bronchitis (cough and phlegm most days for at least 3 months
every year)
Bronchitis (regular or extended periods of cough, and phlegm from
chest for more than 3 months)
Chronic bronchitis (cough + phlegm for 3 months for at least 2 years)
Chronic bronchitis (production of phlegm on most days for at least 3
months of year for at least 2 consecutive years)
Chronic bronchitis (production of phlegm on most days for at least 3
months of year)
Chronic bronchitis (Production of phlegm on most days for at least 3
months of year)
Chronic bronchitis (cough with phlegm for 3 months for at least 2
years)
-46-
Questionnaire: MRC
Questionnaire: MRC
Questionnaire: MRC/ECRHS
Questionnaire: ATS
Questionnaire
Questionnaire: MRC
Questionnaire: MRC
Questionnaire (unnamed)
Questionnaire: WHO
Questionnaire: MRC
Questionnaire: MRC
Questionnaire: MRC
Questionnaire: MRC
Questionnaire: MRC
Questionnaire
Questionnaire
Questionnaire (unnamed), physician examination
Questionnaire: MRC
Questionnaire (unnamed)
Questionnaire: MRC
Questionnaire: MRC
Questionnaire: ECSC
Questionnaire: MRC
Questionnaire: MRC
Questionnaire: MRC
Questionnaire (unnamed)
DIAGSCb Questionnaire
Description of disease
Source of diagnostic information
prevalence
prevalence
Diagnostic
Criteriaa
MRC
Rose
q
q
MRC
Rose
Questionnaire: MRC
Questionnaire: Rose
KUBIK
prevalence
MRC
q
unnamed/unsp
LAMBER
prevalence
unspec
q
MRC
LANGE2
prevalence
unspec
q
unnamed/unsp
LANGHA prevalence
ATS
q
unnamed/unsp
LINDST
prevalence
unspec
q
FinEsS
MAGNUS prevalence
MANFRE prevalence
ATS
unspec
q
q
ECRHS
NHLBI
MENEZ1
prevalence
unspec
q
ATS
MEREN
prevalence
unspec
q
OLIN
MILNE
MOLLER
prevalence
prevalence
unspec
MRC
q
u
MRC
-
MUELLE
NEJJAR
prevalence
prevalence
unspec
Fletcher
q
q
MRC
unnamed/unsp
OGILVI
prevalence
unspec
Mixed
unnamed/unsp
OSWAL1
prevalence
unspec
r
-
OSWAL2
prevalence
unspec
q
unnamed/unsp
PANDEY
prevalence
MRC
Mixed
-
PEREZP
prevalence
unspec
q
ATS
REID
prevalence
unspec
q
unnamed/unsp
RIMING
prevalence
unspec
q
unnamed/unsp
SAWICK
prevalence
unspec
q
MRC
Chronic bronchitis (phlegm for 3+ months/year for at least 2 years)
Chronic bronchitis symptoms grade 2 (cough with phlegm most days or
nights for 3 months each year)
Chronic bronchitis (cough with phlegm for 3 months for at least 2
years)
Chronic bronchitis (cough and phlegm lasting 3+ months,
breathlessness on walking and period of increased cough and phlegm
lasting 3+ weeks in past 3 years)
Chronic bronchitis (phlegm for at least 3 months per year for at least 2
consecutive years)
Chronic bronchitis (cough and phlegm for 3+ months for the past 2
years)
Chronic productive cough (cough with phlegm most days for at least 3
months for at least 2 successive years)
Chronic bronchitis (phlegm from chest for 3 months for 2 years)
Chronic bronchitis (cough and/or phlegm most days at least 3 months
every year)
Chronic bronchitis (cough and phlegm most days for 3 months for at
least 2 years)
Chronic productive cough (phlegm when coughing or phlegm on chest
at least 3 months in 2 successive years)
Persistent cough and phlegm
Chronic obstructive bronchitis (cough and phlegm for 3 months during
2 previous years)
Chronic bronchitis (phlegm from chest for 3+ months every year)
Chronic bronchitis (phlegm most days for 3 months for previous 2
years)
Chronic bronchitis (daily cough with phlegm for 3 months for at least 2
years) without other causative respiratory disease
Chronic bronchitis (cough/phlegm/breathlessness with some degree of
disability persisting for at least 1 year)
Bronchitis (habitual cough and phlegm with disability due to
exacerbations and/or breathlessness in previous 5 years)
Chronic bronchitis (MRC criteria: cough and sputum most days for at
least 3 consecutive months of 2 successive years)
Chronic bronchitis (cough or phlegm on most days for more than 3
months of year for at least 2 consecutive years)
Chronic bronchitis (persistent cough and phlegm (most days for at least
3 months each year), with shortness of breath while walking with other
people at ordinary pace, and at least 1 period of increased cough and
phlegm lasting 3+ weeks during previous 3 years)
Chronic bronchitis (coughed up phlegm for 3 months for at least 2
years)
Chronic bronchitis (cough and phlegm most days for 3 consecutive
months for at least 2 years)
REF
Outcome type
JOSHI
JOUSI1
-47-
Questionnaire (unspecified)
Questionnaire: MRC
Questionnaire (unnamed)
Questionnaire (unspecified)
Questionnaire: FinEsS
Questionnaire: ECRHS
Questionnaire: NHLBI
Questionnaire: ATS
Questionnaire: OLIN
Questionnaire: MRC
Unspecified
Questionnaire: MRC
Questionnaire (unspecified)
Questionnaire, confirmed by physical examination
Hospital diagnosis
Questionnaire (unnamed)
Questionnaire: MRC, usually confirmed at field clinic
Questionnaire: ATS
Questionnaire (un-named)
Questionnaire
Questionnaire: MRC
DIAGSCb Questionnaire
Description of disease
Source of diagnostic information
prevalence
prevalence
Diagnostic
Criteriaa
unspec
unspec
q
q
MRC
CECA
Questionnaire: MRC
Questionnaire: CECA
STJERN
prevalence
ATS
q
MRC
SUADIC
TAGER2
prevalence
prevalence
MRC
unspec
q
q
MRC
MRC
URRUTI
prevalence
unspec
q
ECRHS
WAGEN2 prevalence
MRC
q
unnamed/unsp
WILHEL
WOJTYN
prevalence
prevalence
MRC
unspec
Other
q
MRC
WOODS
prevalence
unspec
q
ECRHS
WOOLF
prevalence
YAMAGU prevalence
unspec
MRC
Mixed
q
MRC
ZOIA
unspec
q
unnamed/unsp
Persistent cough and phlegm for at least 3 months per year
Chronic bronchitis (cough and phlegm for 3+ months per year for at
least 2 consecutive years)
Chronic bronchitis (excessive mucous secretion and chronic recurrent
cough for 3 months for at least 2 years, excluding other causes)
Chronic bronchitis (cough and phlegm for 3 months for at least 2 years)
Chronic bronchitis (cough and phlegm for 3 months per year for 2+
years)
Chronic bronchitis (cough and phlegm for 3 months for last 2 years),
and no asthma-related symptoms (woken in night due to lack of air or
asthma attack in last 12 months, or taking asthma medication)
Chronic bronchitis (cough and phlegm most days for 3 months during 2
previous years)
Chronic bronchitis (cough and phlegm for 3 months each year)
Chronic bronchitis (cough and phlegm most days for at least 3
consecutive months for 2 or more years) at both baseline and 5-year
follow-up
Chronic bronchitis (cough with phlegm for 3 months for at least 2
successive years)
Chronic bronchitis (chronic cough and phlegm)
Chronic bronchitis (cough and phlegm most days for 3 months each
year)
Chronic bronchitis (chronic cough and phlegm)
REF
Outcome type
SHARP
SOBRAD
prevalence
Questionnaire: MRC
Questionnaire: MRC
Questionnaire: MRC
Questionnaire: ECRHS
Questionnaire (not specified)
Physical examination
Questionnaire: MRC
Questionnaire: ECRHS
History and physical examination
Questionnaire: MRC
Questionnaire (unspecified)
a
As named by original author.
b Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
Table 6M : CB other
REF
Outcome type
Diagnostic
Criteriaa
DIAGSCb Questionnaire
LUNGFNb SPBRONc Description of disease
JENSEN
prevalence
unspec
Mixed
MRCd
-
KIRAZ
prevalence
unspec
Mixed
MRC/ATS
v
no/unkn
Source of diagnostic information
Bronchitis (physician diagnosis of bronchitis, asthmatic bronchitis or
Questionnaire (MRC?): physician diagnosis/other
asthma, <20% increase in FEV1 after terbutaline inhalation and/or daily
cough and/or expectoration for at least 3 months a year)
Chronic bronchitis (Cough and sputum most days for at least 3 months Questionnaire: ATS/MRC, physical examination,
for at least 2 years plus chest rales, decreased respiratory sounds or
spirometry
increased expiration time and FEV1/FVC <88% predicted, with or
e
without COPD (reversibility of <12%))
-48-
DIAGSCb Questionnaire
LUNGFNb SPBRONc Description of disease
Source of diagnostic information
prevalence
Diagnostic
Criteriaa
unspec
Mixed
MRC
-
Questionnaire: MRC, spirometry, physical examination
MELLST
prevalence
Fletcher
Other
-
-
PELKON
incidence
Mixed
Mixed
MRC
-
SHIMUR
prevalence
Mixed #
r
ATS/MRC
-
SILVA
incidence
ATS
q
NHLI
c
WIG
prevalence
unspec
Mixed
unnamed/unsp
-
REF
Outcome type
LUNDB2
no/unkn
Self-reported respiratory disease/symptoms confirmed at examination as
chronic bronchitis (cough/sputum most days for at least 3 months for at
least 2 years, or impaired lung function of obstructive type and FEV1
<80% predicted with history typical of chronic bronchitis)
Chronic bronchitis (Phlegm most days for 3+ months each year and/or
diagnosis of asthmatic bronchitis in previous 10 years)
Incident chronic bronchitis (cough with phlegm for at least 3 months
each year), or CB mortality (ICD codes not specified)
Chronic bronchitis (ATS/MRC criteria), chronic obstructive
mucopurulent bronchitis, with phlegm for at least 5 years and chronic
airflow limitation, death from chronic respiratory failure
Chronic bronchitis (cough and phlegm most days for 3 months for at
least 2 consecutive years and FEV1 <80% predicted) and no physician
diagnosis of emphysema
Chronic bronchitis (criteria unspecified)
Physical examination
Questionnaire: MRC or death certificate
Medical records
Spirometry, questionnaire: NHLI
Questionnaire (unnamed), physical examination, x-ray
a
As named by original author.
b Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
c Field SPBRON refers to spirometry used post-bronchodilator, no (=without bronchodilator) or unknown, and reversibility criteria.
d Questionnaire used stated to be British Committee on Research into Chronic Bronchitis, assumed to be MRC.
e CB cases appear to have been split according to the presence of COPD, although this is not made clear. Therefore, both groups combined to form CB endpoint.
Table 6N : Emphysema based on ICD
ICD7a ICD8a ICD9a ICD10a DIAGSCa Description of disease
Source of diagnostic information
BEST
mortality
HAMMO2 mortality
8
8
-
-
-
c
c
Death records of Dept of Veterans Affairs
Death certificates
HIRAYA
KAHN
KAHN2
WEN
8
8
8
-
-
c
-
c
c
c
c
REF
Outcome type
mortality
mortality
mortality
mortality
Emphysema mortality (ICD7 527.1)
Emphysema (ICD 7 Code 527.1, modified to include bronchitis and
emphysema as joint cause)
Emphysema (ICD 527.1)
Emphysema deaths (underlying) (ICD7 527.1)
Underlying emphysema deaths (ICD 7: 527.1)
Emphysema (ICD 9: 492)
a
Death certificates
Death certificates
Death certificates
Death certificates
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
-49-
Table 6O : Emphysema based on visual comparison
REF
Outcome type
Diagnostic
Criteriaa
DIAGSCb Questionnaire
Description of disease
Source of diagnostic information
ANDER2
prevalence
unspec
a
-
Autopsy
AUERBA
NAWA
OMORI
prevalence
prevalence
prevalence
unspec
unspec
Japanese
a
t
t
-
Emphysema(visual comparison with pre-set standard, Grade 1+ vs
none)
Emphysema (visual comparison against standard (Grade 1+))
Emphysematous changes (visual comparison)
Emphysema (visual comparison with pre-defined grading system)
PRATT
prevalence
unspec
a
-
RYDER
SUTINE
VIKGRE
prevalence
prevalence
incidence
unspec
unspec
unspec
a
a
t
-
WANG2
prevalence
unspec
t
-
WEISS
prevalence
unspec
x
-
Centrilobular emphysema (visual comparison with standard pointcounting technique, including trace only)
Emphysema (airspace of 0.1cm diameter or greater)
Emphysema (air spaces >0.1 cm, grade 5+)
Emphysema (areas of low attentuation and/or presence of stretched
narrow vessels)
Emphysema (low-attenuation areas with disrupted vasculature but
without discernible surrounding walls in the pulmonary parenchyma)
Emphysema (low flat diaphragm with little difference demonstrable
photofluorographically between inspiration and expiration films,
increased general radiolucency of the lungs and widening of the
interspaces)
Autopsy
Low dose spiral CT scan
Low dose CT scan plus high resolution CT at 3 locations in current and
ex-smokers only
Autopsy
Autopsy
Autopsy
CT scan
CT scan
X-ray
a
As named by original author.
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
b
Table 6P : Emphysema based on diagnosis
REF
Outcome type
Diagnostic
Criteriaa
DIAGSCb Questionnaire
Description of disease
Source of diagnostic information
DONTA2
ENRIGH
GULSVI
HARDIE
HOZAWA
LEBOWI
MILLER
WILSO2
incidence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
prevalence
unspec
unspec
unspec
unspec
unspec
unspec
unspec
unspec
Mixed
d
d
d
d
d
d
d
Clinical diagnosis of pulmonary emphysema
Emphysema: physician diagnosed
Emphysema (physician diagnosis/hospitalisation)
Ever diagnosed with emphysema by physician
Emphysema (physician-diagnosed)
Emphysema (physician diagnosed)
Emphysema (ever diagnosed by physician)
Emphysema (physician-diagnosed)
Questionnaire, physical examination, spirometry
Questionnaire: ATS
Questionnaire (unspecified)
Questionnaire: ATS
Questionnaire (unnamed)
Questionnaire: NHLI
Questionnaire (physician diagnosis)
Questionnaire: Health Omnibus Survey
a
MRC
ATS
unnamed/unsp
ATS
unnamed/unsp
NHLI
MRC
HealthOmnibus
As named by original author.
-50-
b
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
Table 6Q : Emphysema based on self-report
REF
Outcome type
Diagnostic
Criteriaa
DIAGSCb Questionnaire
Description of disease
Source of diagnostic information
HO
LAVECC
prevalence
prevalence
unspec
unspec
q
q
Emphysema (self-reported)
Emphysema or respiratory insufficiency (self- reported)
Questionnaire (unnamed)
Questionnaire (unspecified)
unnamed/unsp
unnamed/unsp
a
As named by original author.
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
b
Table 6R : Emphysema other
REF
Outcome type
Diagnostic
Criteriaa
DIAGSCb Questionnaire
LUNGFNb SPBRONc Description of disease
Source of diagnostic information
HUHTI1
prevalence
unspec
Mixed
-
2
no/unkn
Spirometry, x-ray
SILVA
incidence
unspec
d
NHLI
i
no/unkn
Emphysema (FEV1/FVC <60% or FEV1/FVC 60-69% plus 2 or more
of following chest x-ray changes: deficiency of peripheral vascular
pattern, prominent main pulmonary artery and hilar blood vessels,
narrow vertically situated heart, low position or poor mobility of
diaphragm, large retrosternal space)
Emphysema (physician-diagnosis, and FEV1 or DLCO <80%
predicted)
a
Spirometry, questionnaire: NHLI
As named by original author.
Codes are explained at the end of Table 6 (although the information is generally repeated in text form in columns "Description of disease" and " Source of diagnostic information "; the levels
are the same for all 3 outcomes).
c Field SPBRON refers to spirometry used post-bronchodilator, no (=without bronchodilator) or unknown, and reversibility criteria.
b
-51-
Grading systems used throughout Table 6:
DIAGSC
ICD7
ICD8
ICD9
ICD10
r
d
q
s
x
t
c
a
o
m
u
1
2
3
4
5
6
7
8
9
a
1
2
3
4
5
6
7
8
9
a
1
2
3
4
5
6
7
8
9
a
b
c
2
3
9
LUNGFUN
Hospital/GP records
Questionnaire: physician diagnosis
Questionnaire: other
Spirometry
X-ray
CT scan
Death certificate/registry
Autopsy
Other
Mixed
Unspecified
502,527.1
501-502,527.1,(527.2 later)
500-502,527.1
501,502,526,527.1
241,500-502,527.1
502,526,527.1
500-502
527.1
unspecified
502.0, 527.1
491-492
490-492
490-492,518
490-492,519
491-493
490-493
466, 490-493
490-493,518,519.3
unspecified
491-492,519
491,492,496
490-492,496
490-492,496,416.7
491-493
490-493
490-496
490-492,494,496
416,491,492,496,519
unspecified
466, 490-493
491
492
J40-J44
J43-J44
unspecified
2
3
4
5
6
7
8
9
a
b
c
d
e
f
g
h
i
j
k
l
m
n
o
p
q
r
s
t
u
v
-52-
FEV1/FVC <70%
FEV1/FVC<70% and FEV1<80% predicted
FEV1/FVC<88%M, 89%F
FEV1/FVC<normal (ATS value nk)
FEV1<65% predicted or FEV/FVC<65%
FEV1% <60
FEV1/FVC <80%
FEV1 <75% predicted
FEV1/or VC <70% predicted
FEV1 <65% predicted
FEV1 <80% predicted
FEV1/FVC<70% + reversibility <15%
FEV1/FVC<88%+ reversibility <12%
FEV1<5th percentile + reversibility <9%
FEV1/FVC <65%
FEV1 or MMEF <2SD below predicted
FEV1 or DLCO <80% predicted
unspecified
FEV1/FVC <68%
FEV1/FVC <60%
FEV1/FVC<70% + FEV1<80% predicted +
reversibility <10%
GOLD2+ (FEV1/FVC<70%,FEV1<80%)
FEV1/FVC<70% + FEV1<70% predicted +
reversibility <12%
FEV1 < 85% predicted
ATS NOS
FEV1/FVC<75%
FEV1/FVC<85%
FEV1/FVC<70%, FEV1<80% predicted,
reversibility <12%
FEV1 > 2SE below predicted
FEV1/FVC <88% predicted