Anatomical Basis for Repair of Ulnar and Median Nerves in the
advertisement

Copyrighl 1986 by The Journal of Bone and Joint Surgery, Incorporated
Anatomical Basis for Repair of Ulnar and MedianNerves
in the Distal Part of the Forearm
*t*
by GroupFascicular Suture and Nerve-Grafting
rk.
)2,
the
~in
the
BY JIMMY
Z.
JOHN
A.
BILOS,
CHOW§,
M.D.§,
LIEUTENANT
COLONEL,
MEDICAL
WASHINGTON,
DAVID
L.
MEYER§,
AND
MARTHA
C.
JOHNSON,
CORPS,
UNITED
LIEUTENANT
PH.D.§,
STATES
COLONEL,
ARMY,
MEDICAL
WASHINGTON,
ALLEN
L.
CORPS,
VAN
BEEK,
UNITED
M.D.§,
STATES
ARMY,
D.C.
FromWalter ReedArmyMedicalCenter, Washington,D.C., Uni~brmed
Services University School of Medicine,Bethesda, Maryland,and
CookCountyHospitaland HektoenInstitute of MedicalResearch,Chicago,Illinois
-.l[S.
27,
ABSTRACT:The topography of the intraneural
fascicular groups must be understood if the treatment of
acute lacerations of the major nerves in the forearm is
to be successful. Most lacerations in the upper extremity
occur at the wrist and in the distal half of the forearm.
With microsurgical
longitudinal dissections
and serial
sections, we studied the intraneural
topography of the
fascicular groups of the median and ulnar nerves utilizing forty-five fresh frozen or refrigerated specimens. We
devised a new technique of light photography to demonstrate the distinct boundaries of the fascicular groups.
The intraneural
fascicular
groups provide the anatomical basis for the recommended surgical techniques of
group fascicular repair and nerve-grafting.
In 1945, Sunderland reported his classic study, "The
Intraneural
Topography of the Radial, Median and Ulnar
Nerves"5, and in 1968 his book 6Nerves and Nerve Injuries
was published. Since then, his description of the intraneural
fascicular
pattern has been widely quoted and has been
confirmed by the studies of Jabaley et al. and Williams.
For our purposes, two points may be drawn from Sunderland’s reports.
I. The funicular pattern in both the ulnar and median
nerves is continually modified along the length of each nerve
by repeated divisions, anastomoses, and changes in the relative positions of the funiculi. The changes in position of
individual funiculi may take place within a short expanse
of the nerve, often in a segment of 2.5 millimeters or less.
2. The funiculi (also called fascicles or bundles) arrange themselves in definite groups that are usually identifiable along the course of the nerve for distances of several
centimeters, especially in the distal portions of the two
nerves. Sunderland reported that the bundles in the branches
of each nerve course as separate and distinct groups within
the nerve, and despite the changing patterns of the individual
funiculi in cross section, the bundle groups, during their
course in the nerve, are individually identifiable for variable,
and often considerable, distances above the site of branching.
ManycIinicians have cited our first point to support
claims that a precise anatomical realignment of fascicles in
the~ repair of lacerated peripheral nerves is impossible. Our
second point generally has been overlooked, as it relates to
surgical treatment.
The present study was prompted by clinical observations by the principal one of us (J. A. C.) made at the Cook
County Hospital between July I978 and June 1979. Of fiftysix cases of laceration of the major peripheral nerves of the
.upper extremity, forty-one were lacerations of the median
or ulnar nerve, or both, at the wrist or in the distal half of
the forearm.
These observations emphasized the significance of intraneural fascicular group topography in the tte-atment of
acute lacerations of the major nerves at the wrist and distal
half of the forearm. Also, the fascicular group arrangement
is more constant distally in the major nerves of the upper
and lower extremities.
We decided to attempt to reconfirm Sunderland’s observations on the intraneural topography of the median and
ulnar nerves, with special attention to the fascicular groups,
and to amplify his studies. Our purpose was to investigate
the anatomical feasibility of suturing the groups of fascicles
individually.
Materials
and Methods
We used forty-five fresh refrigerated or fresh frozen
* Thisarticle wasacceptedfor publicationprior to July I, 1985.No specimens of the upper extremity, and in seventeen speciconflict-of-interest statementwasrequestedfromthe authors.
+ Theopinionsor asse,--r,i;.’,~s coa~ained
hereinare the privateviews mens we did a microsurgical longitudinal dissection of the
(’::,.:i:’:.,.!ar
groups o;: ’&~media~and ~ir<u" ,~rve~: Wetraced
274
J. A,
CHOW ET AL.
ULNAR
15MM
DORSAL
F~, 1-A
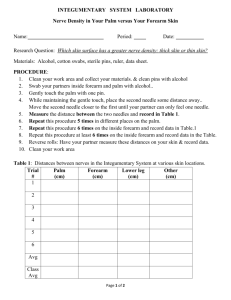
Figs. I-A through l-D: Histological sections of the left ulnar nerve, one centimeter
Fig. l-A: At a level fifteen millimeters proximal to the radial styloid process.
of the medianand ulnar nerves in the proximaI part of the
forearm were followed in the proximal direction, utilizing
a similar microsurgical dissection technique, tn ten specimenswe madea series of sections at five-millimeter inter-
apart (hematoxyii~ and eosin, × 10),
vals and studied themby a methodsimilar to that described
by Sunderland~. Weused hematoxylin and eosin and Masson trichrome stains. Special attention was directed to the
group fascicular patterns of the median and ulnar nerves
AIqAT~3~6~C-AL
BASIS
FOR REPAIR
OF ULNAR AND MEDIAN NERVEg
275
FI~,
Th(rty-fi,~e millimeters proximal to the raOi~l s~yloid process.
scribed by VanBecketal, -~ in. 1979(Fig. 3).
(Figs. t-A through I-D and 5), This empt~asis was different
In, addition to the data obtainefi from t~e,~e fort~-fw~
~:rom those of previously published anatomical stugies,
whichfocused their attention on the individual fascicles of fresh specimens, additional information was obtained from
dissection of sixty-si~ f~rmalin-fixed specimens f~m ca~!~enerves.
Wealso devised a newpt~otographic technique to study davera to determine the locations and c~urses of the motor
a series of consecutive segments of the median and ulnar fascic~lar groups of the ulnar nerve at the wrist and in the
distal part of the forearm.
nerves in sixteen specimens (Pigs. 2-A and 2-B). The lostitular group topography of tl-te median and alaar nerves
Results
was studied in two specimensutilizing a series of sections,
from the edge of the palmto tt~e proximal part of the arm, Ulnar Nerve
The ulnar nerve gives rise to three terminal branc/Tes
by scanning electron microscopy. The technique was de-
276
J. A. CHOWET AL.
FIG. 2-A
Figs. 2-A and 2-B: Conventionalphotographs of cross-sectional surfaces of segmentsof the left ulnar nerve madewith a camera that had a bellows
attachment (x 5).
Fig. 2-A: Fifty millimeters proximalto the radial styloid process.
at the level of the proximaledge of the palm-- one muscular
and twocutaneous(Fig. 4). The first is a branchthat supplies
the hypothenar muscles and interosseus muscles. One cutaneous branch proceeds to the fourth web space as the
common
digital nerve, while the other supplies the hypoth-
frown~hesensor3’ fascicular groui~~S!.
enar skin and the ulnar side of the little finger. Thesethree
branches can be followed proximally as three distinct fascicular groupsfor fifty millimeters from the radial styloid
process (Figs. 1-A through l-D). The two sensory groups
mergeat that level. Fromthe fifty-millimeter to the ninety-
ANATOMICALBASIS FOR REPAIR OF ULNAR AND MEDIAN NERVES
277
ULNAR
150MM
FIG. 3
Scanningelectron micrographof the left ulnar nerve, 150 millimeters proximalto the radial styloid process. Note the intraneural epineurium(arrows)
and the fascicular group from the dorsal cutaneous branch located at the ulnar portion of the nerve.
hree
fas ,loid
~ups
tety-
millimeter level, the mergedsensory and the motorfascicles
can be identified as two distinct fascicular groups separated
by a firm condensationof connectivetissues (the intraneural
epineurium) (Figs. 2-A and 2-B). At the ninety-millimeter
level, these two groups merge. The motor fascicular group
maytherefore be identified as a distinct entity from the tip
of the radial styloid process to a point ninety millimeters
proximal to the palm. In all but two of the 111 specimens
that Werestudied, the motor fascicular group of the ulnar
nerve at the distal part of the forearm was located at the
ulnar-dorsal position or central dorsal position. In the exceptional two specimens,it was located at the radial-dorsal
nerve(left forearm).
’.GERY
VOL. 68-A, NO. 2. FEBRUARY
1986
278
J.A.
CHOWET AL.
RADIAL
20MM
DORSAL
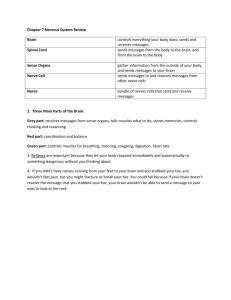
F~G. 5
Histological section of the right mediannerve at a level twenty millimeters proximalto the radial styloid process. Aindicates the radially located
combinedmotorand sensory group. The motor fascicles to the thenar musclesare on the volar aspect of this group. B and C are the sensory fascicular
groups from the common
digital nerves of the second and third web spaces, respectively (hematoxylin and eosin, x 10).
position. At the level of the distal third of the forearm,the
motorfascicular group constituted 30 to 35 per cent of the
total fascicular cross-sectional area of the ulnar nerve.
The dorsal cutaneous branch is separate from the main
trunk of the ulnar nerve at, and distal to, the junction of the
middle and distal thirds of the forearm (eighty to ninety
millimeters from the palm). It was followed proximally as
a separate fascicular group, running side by side with the
combinedfascicular group from the three terminal branches,
from the ninety-millimeter level to the 250-millimeterlevel
proximal to the palm (Fig. 3).
In the proximal half of the forearm, the fascicular
groups that ~correspondto the three terminal branchesat the
proximal edge of the palm becomedistinct. However, at
the elbow,the specific fascicular groups that form the motor
branchesto the flexor carpi ulnaris and the ulnar half of the
flexor digitorum profundus can be readily identified. They
remainas distinct entities for approximatelyten centimeters
proximal to the elbow.
Median Nerve
cles are in the volar-radial position.
Themotorfascicles to the two radial lumbrical muscles
are also located in the mixed sensory-motor fascicular
group, situated ulnar to the motor fascicular group to the
thenar muscles.Moredistally, in the palm, the motorbranch
to the index lumbrical muscleaccompaniesthe radial digital
nerve of the index finger. The motorbranch to the lumbrical
muscle of the long finger accompaniesthe commondigital
nerve to the second webspace. The motor fascicles of the
medianner*e at the distal end of the forearmconstitute only
10 per cent of the total fascicular cross-sectional area of the
nerve.
The palmar cutaneous branch is separate from the main
part of the median nerve at approximately seventy millimeters proximalto the radial styloid process, and its sensory
fascicular groupcan be traced proximallyas an entity to the
150-millimeterlevel; that is, to the middlethird of the forearnq.
In the proximal half of the forearm, the fascicular
groups that correspond to the terminal branches become
indistinct, but the motorfascicular groups that terminate as
branches to the muscles of the forearm maybe traced for
about ten centimeters proximallyfrom the site of branching.
At the level of the wrist and in the distal quarter of the
forearm, three fascicular groups maybe identified in the
median nerve, and they can be traced as separate entities
Discussion
for five to seven centimeters proximal to the proximaledge
of the palm. At the ulnar side, there are two sensory fasBecausethe majornerves at the distal part of the forecicular groups (Fig.-5), which form the two common
digital
arm are lacerated so frdquently, a study of the topography
nerves to the third and second web spaces. On the radial
of the intraneural fascicular groupsat these levels has special
side, there is one large fascicular groupconsisting of sensory clinical significance.
andmo~#r
--’:~:,:cicies....... t~e :;e~sorvfasciclescontinue
d{:;taI!y
Our findings are basedon st. ~.die~ c;f f~’>.~’~’efresh
as ’&ccadi’~.!~igitalnerve:)f ~heindex~:ic.:2=.:~:
ANATOMICALBASIS FOR REPAIR OF ULNAR AND MEDIAN NERVES
the distinct entities of the fascicular groupsat serial levels
(Figs. 2-A and 2-B).
The surgical relevance of our findings should be emphasized because they provide an anatomical basis for group
fascicular repair. In 1917, Langleyand Hashimoto,of Cambridge University, suggested the idea of separate suture of
fascicular groups, and advised cutting open the inner, dense
epineurial sheath (intraneural epineurium). The technique
of group fascicular repair has been described by Van Beck
and Kleinert8 as well as by Sunderland7 (Fig. 6). Utilizing
the operating microscope, one mayreadily identify, match,
align, and repair the fascicular groups.
Groupfascicular repair maybe conceptualized as inner
279
segmentof nerve is lost, the fascicles at the two nerve ends
will not correspond, so that fascicle-to-fascicle repair by
perineurially placed sutures is precluded. Undersuch conditions, one should be able to identify corresponding fascicular groups rather than individual fascicles at the nerve
ends, and then microsurgical group fascicular repair will be
possible because the fascicular groupsremainas identifiable
entities for several centimeters proximalto the wrist.
In the surgical treatment of acute lacerations of the
major peripheral nerves, we advocate microsurgical group
fascicular repair or microsurgicalepineurial repair with correct alignment of the fascicular groups. Wedo not advocate
fascicular (perineurial) repair.
F~. 6
Groupfascicular repair.
"/
F~. 7
Groupfascicular nerve-grafting,
epineurial repair. The epineurium maybe divided into external epineuriumand intraneural epineurium. The external
epineuriumsurrounds the entire nerve, while the intraneural
epineurium separates and surrounds individual fascicular
groups or individual fascicles (Figs. 1-B and 2-B). The
epineurium,either external or intraneural, lends itself to
separate suturing without injury to the encased fascicular
groups. Utitizir~ the operating microscope, sutures maybe
car.:g:~i!)’ap?ii::<c~<sizec.~.:.:::
thet’ascicuIar
gr~>:ps.
’.,; i~.>.’.~,t
The fascicular group arrangementof major peripheral
nerves is also important for the techniqueof interfascicular
3’4.
nerve-grafting as described by Millesi and Millesi et al.
Theypointed out that, using the operating microscope,nerve
grafts can be utilized to bridge the gap betweenthe corresponding fascicular groups (Fig. 7).
Webelieve that the relatively constant location of the
motorfascicular group of the ulnar nerve at the distal part
of ..~ f~;,:." ~-mi:.~ >av:i,::’.’~ " i~~,~.:.~:...t. In all buttwoof
t~te i11 ~:;<>c:cic~~ens
t!,:x~ ,.~..~: .tudied, that fasciculargroup
~, :: :~ : .::.’ "2t ~},: :i:: ¯ .’,.," cer,.tral dorsalpositi.op., in
~ess surgical traumaand resuita~.<a,.’ri;~g. If a signii:~ ::~nt
in~r~ .ic rrmsck:s;;;. ~i:e ha~=,d, one should makea special
280
J. A. CHOWET AL.
effort duringnervesutureto correctlyidentify andalign this
motorfascicular group.
We recognize the value of the early work of
5 andthe later contributionsof Jabaleyet al. and
Sunderland
Williams, and most of the points that they madehave been
confirmedin our study. Ourdissections constitute a larger
numberof specimensthan do the previously published reports, and we further highlight the privileged anatomical
fact of the moreconstant fascicular grouparrangementin
the intraneural topographyof the ulnar and mediannerves
at the distal part of the forearm,wherethe majorityof acute
lacerationsoccurclinically.
NOTE:
Lieutenant
Colonel
Chow
is indebted
to Sir Sydney
Sunderland
for proofreading
the
manuscript
andto Dr. Michael
Jabaley,Dr. BraceWilliams,
andDr. Hanuo
Millesifor advice
andencouragement
duringthepreparation
of this work.TheauthorsthankMr.George
Holborow.
Mr.Gregory
Holmes,
Mr.PaulNiner,andMs.lngridLynch
for technicalassistance.Theyalso
thankGaryG.Wind,
M.D.,for preparation
of theline drawings.
References
t.
2.
3.
4.
5.
6.
7.
8.
9.
10.
JABALEY, M. E.; WALLACE, W. H.; and HECKLER,
F. R.: Internal Topography of Major Nerves of the Forearm and Hand: A Current View. I.
Hand Surg., 5: 1-18, 1980.
LANGLEY,
J. N., and HASHIMOTO,
M.: Onthe Suture of Separate Nerve Bundles in a Nerve Trunk and on Internal Nerve Plexuses. J. Physiol.,
51: 318-346, 1917.
:
MILLESI,H.: Nerve Grafts -- Indications, Techniques and Prognosis. In Managementof Peripheral Nerve Problems, p. 417. Edited by G. E.
Omer, Jr., and MortonSpinner. Philadelphia, W. B. Saunders, 1980.
MILLESI,H.; MEISSL,G.; and BERGER,
A.: The Interfascicular Nerve-Grafting of the Medianand Ulnar Nerves. J. Boneand Joint Surg., 54..A:
727-750, June 1972.
SUNDERLAND,
SYDNEY:
The Intraneural Topographyof the Radial. Median and Ulnar Nerves. Brain, 68: 243-298, 1945.
SUNDERLAND,
SYDNEY:
Nerves and Nerve Injuries. Edinburgh, Churchill Livingstone, 1968.
SUNDERLAND,
SYDNEY:
Nerves and Nerve Injuries. Ed. 2. Edinburgh, Churchill Livingstone. 1978.
VANBEEK,ALLEN,and KLEINERT,
H. E.: Practical Microneurorrhaphy. Orthop. Clin. North America, 8: 377-386, 1977.
VANBEEK,A. L.; JACOBS,
S. C.; and ZOOK,
E. G.: Examinationof Peripheral Nerves with the ScanningElectron Microscope.Plast. and Reconstr.
Surg., 63: 509-519, 1979.
WILLIAMS,
H. B.: Peripheral Nerve Injuries in Children. In Symposium
on Pediatric Plastic Surgery, pp. 266-282. Edited by D. A. Kernahan, H.
G. Thompson,and B. S. Bauer. St. Louis, C. V. Mosby, 1982.