Supplementary Material (doc 2282K)
advertisement
")
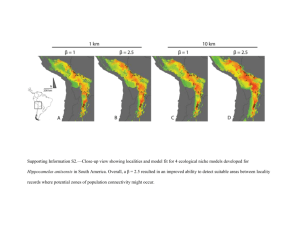
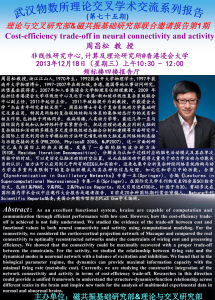
Supplementary Material for “Resting-State Connectivity Predictors of Response to Psychotherapy in Major Depressive Disorder” Andrew Crowther, Moria J. Smoski , Jared Minkel, Tyler Moore, Devin Gibbs, Chris Petty, Josh Bizzell, Crystal Edler Schiller, John Sideris, Hannah Carl, & Gabriel S. Dichter* Supplementary Materials I: Cross-correlations among BDI subscale scores in the MDD sample Pre-treatment BDI scores: Total BDI Score Anhedonia Subscale Somatic Subscale Anhedonia Subscale 0.80 Somatic Subscale 0.88 Cognitive Subscale 0.84 - 0.69 - 0.69 0.49 Post-Treatment BDI scores: Total BDI Score Anhedonia Subscale Somatic Subscale Anhedonia Subscale 0.83 Somatic Subscale 0.41 Cognitive Subscale 0.47 - 0.24 - 0.25 0.84 1 Supplementary Materials II: Within groups connectivity maps Figure 1 illustrates, for each seed used in the between groups analysis, the within-groups rs-fcMRI connectivity maps on the left accompanied by the pattern of group differences in seed- based connectivity for that seed on the right (color-bars illustrate the degree to which the within groups maps are greater than 0). This figure illustrates the extent to which group differences in connectivity are related to connectivity maps within the control and MDD samples. Figure 1. Within-groups rs-fcMRI connectivity maps for each network and seed region (left); Group differences for that seed (right) 2 Supplementary Materials III: Between-groups results excluding four participants who completed fewer than eight therapy sessions Although this study was designed as an intent-to-treat trial, it is possible that participants who received fewer psychotherapy sessions did not received the intended full benefit of the treatment. Four patients with MDD completed fewer than eight therapy sessions (i.e., one each completed 1, 3, 5, and 7 sessions), and Figure 2 and accompany activation tables below we present findings for group differences in functional connectivity excluding these four patients. As is evident from the figure, primary findings of group differences in the DAN remained significant, as did group differences using the right insula and dorsal anterior cingulate seeds in the salience network. However, group differences in the DMN, ECN, and using the left insula seed were no longer evident. Although these findings should be interpreted with caution given the small number of participants who received fewer than eight therapy sessions, these results suggest that rs-fcMRI-based group differences in the salience network below may be particularly robust (i.e., they remained significant even after the removal of four participants). Figure 2. Group differences in rs-fcMRI in the default mode network; the dorsal attention network; and the salience network (cluster-corrected p<.05; compare to Figure 1 in the main paper). 3 Table 3: Between groups differences in rs-fcMRI connectivity (cluster-corrected p<.05) with removal of four patients with MDD who completed fewer than eight therapy sessions (cluster-corrected p<.05; compare to Table 4 in the main paper). MDD>Control MNI Coordinates Seed (network) Region (BA) X Y Z Peak z-score Right Anterior Insula (Salience Network) Left Visual Cortex (BA17) -2 -88 -8 3.82 Dorsal ACC (Salience Network) Left Visual Cortex (BA17) -20 -98 10 3.95 BA: Brodmann Area Control>MDD MNI Coordinates Seed (network) Region (BA) X Y Z Peak z-score Right Anterior Insula (Salience Network) Right Anterior Insula (Salience Network) Dorsal ACC (Salience Network) Left Middle temporal lobe (BA21) -60 -44 4 4.23 Right Middle temporal lobe (BA22) 50 -38 8 4.19 Left Parahippocampal gyrus -12 -34 -16 4.6 Left IPS (Dorsal Attention Network) BA: Brodmann Area Left Orbitofrontal cortex (BA47) -32 24 -18 3.71 4 Supplementary Materials IV: Predictions of treatment response defined as post-treatment minus pretreatment BDI scores To supplement our hierarchical linear model predictions of treatment response, we conducted simple correlations between connectivity in the nine pairs of regions listed in Table 4 (in the main manuscript) that differentiated MDD and control groups and change in total BDI score calculated by subtracting the BDI acquired on the scan day with the BDI score collected on the last day of treatment. One significant association was found. As illustrated in Figure 3, connectivity between the right insula and the left middle temporal gyrus was a significant predictor of treatment response such that greater pre-treatment connectivity correlated with greater improvement after BA psychotherapy. There were no other significant Figure 3. Pretreatment connectivity between the right insula and the left middle temporal gyrus was a significant predictor of treatment response. associations between baseline connectivity and treatment response measured this way. 5 Supplementary Materials V. Prediction of psychotherapy motivation from intrinsic connectivity MDD participants also completed the Situational Motivation Scale (SIMS) at each therapy session to assess how motivated patients were in their therapy sessions. The SIMS is based on selfdetermination theory, which Figure 4. Biweekly SIMS scores from individual MDD participants (thin lines) and average biweekly SIMS scores from all MDD participants (thick line). posits that the motivations for different human behaviors vary in their level of self-determination, with self-determination defined as a true sense of choice, a sense of feeling free in doing what one has chosen to do. The SIMS may be broken down into subscales, reflecting a continuum of self-determination. From high to low self-determination the subscales are intrinsic motivation, extrinsic motivation (which is further separated into identified regulation and external regulation), and amotivation. Intrinsic motivation involves doing an activity for its own sake. Identified regulation involves choosing to do an activity as a means to an end. External regulation is when a behavior is determined by rewards or a desire to avoid negative consequences. Lastly, amotivation involves behavior without a sense of purpose or expectation of reward (Guay, Vallerand, & Blanchard, 2000). The first SIMS assessment was at week two of treatment, and biweekly SIMS subscale scores from individual MDD participants (thin lines) and average biweekly scores from all MDD participants (thick line) are illustrated in the figure above. 6 We used a hierarchical linear model (HLM) estimated via SAS “proc mixed” (SAS version 9.3, Cary, NC) to analyze the capacity of baseline resting state fMRI data to predict change in SIMS scores using nine timepoints over 15 weeks. We used a model that tested the possibility that linear change in SIMS scores over time was moderated by baseline connectivity included as a time-invariant variable (examining all connectivity metrics that differentiated MDD and control groups at baseline). The model included main effects for time and connectivity plus their interaction. Data were centered such that the main effect for connectivity is estimated at time = 0 (i.e., before treatment) and the main effect for time was estimated at the mean of connectivity metrics. Three models yielded significant connectivity × time interaction effects, as described here: Prediction of change in SIMS identified regulation scores from dACC connectivity with hippocampus: Tests of random effects indicated significant effects for the intercept (z = 2.80, p<.003, but not for time (z = 1.15, p>.10). The fixed effects indicated a significant positive effect for time (t=2.44, p < .03), indicating that SIMS identified regulation scores increased with time for all participants, and a marginal positive effect for connectivity (t=1.98, p = .051), indicating that connectivity was marginally positively associated with SIMS identified regulation scores. The critical connectivity × time interaction was significant as well (t=-2.75p < . 01) indicating that varying levels of connectivity were associated with differential change in SIMS identified regulation scores over time, and more specifically that the amount of change in SIMS identified regulation scores was greatest for those with greater connectivity and least for those with lower connectivity. 7 Prediction of change in SIMS intrinsic motivation scores from intraparietal sulcus connectivity with orbitofrontal cortex: Tests of random effects indicated significant effects for the intercept (z = 2.51, p=.006, but not for time (z = 1.10, p>.10). The fixed effects indicated a significant positive effect for time (t=6.36, p < .0001), indicating that SIMS intrinsic motivation scores increased with time for all participants, and no effect for connectivity (t=-1.00, p > .30), indicating that connectivity was not associated with SIMS intrinsic motivation scores. The critical connectivity × time interaction was significant (t=3.14, p < . 003) indicating that varying levels of connectivity were associated with differential change in SIMS intrinsic motivation scores over time, and more specifically that the amount of change in SIMS intrinsic motivation scores was greatest for those with greater connectivity and least for those with lower connectivity. Prediction of change in SIMS external regulation scores from left insula connectivity with intraparietal sulcus: Tests of random effects indicated significant effects for the intercept (z = 2.86, p<.002, but not for time (z = 0.61, p>.30). The fixed effects indicated a significant negative effect for time (t=-5.83, p < .0001), indicating that SIMS external regulation scores decreased with time for all participants, and for connectivity (t=3.79, p > .0003), indicating that connectivity was not associated with SIMS external regulation scores. The critical connectivity × time interaction was significant (t=-3.63 p < . 005) indicating that varying levels of connectivity were associated with differential change in SIMS external regulation scores over time, and more specifically that the amount of change in SIMS external regulation scores was greatest for those with greater connectivity and least for those with lower connectivity. 8