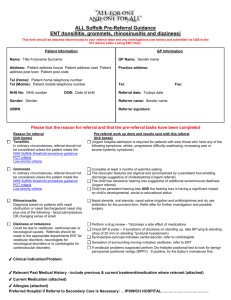
ENT REFERRAL MANAGEMENT: GUIDANCE FOR GENERAL PRACTITIONERS VERSION2 June2012 CONTENTS 1.0 Introduction Page 3 2.0 ENT Consultants and Sub-specialisation Page 3 3.0 Common Ear Conditions 3.1 Tuning Fork Tests Page 5 Page 9 4.0 Common Nasal Conditions Page 10 5.0 Common Throat Conditions Page 12 6.0 Other ENT Emergencies 6.1 Facial Nerve Palsy 6.2 Stridor Page 15 Page 15 Page 15 7.0 Emergency/ Urgent clinics 7.1 One Stop Lump & Bump Clinic 7.2 Emergency Clinic Page 15 Page 16 2 1.0 Introduction This referral management guidance document has been produced in collaboration with Barts and the London ENT Consultants and representation from Tower Hamlets PCT GPs (especially Mr Nick Eynon Lewis, Dr Rajia Khatun, Dr Shera Chok and Dr Ricardo Cabot) as well as the BLT/PCT ENT Steering Group to give GPs an overview of ENT referral management guidance. A similar document was produced in April 2002 by a joint BLT/PCT ENT Group; the aim of the document was to give GPs support in when to refer to secondary care. This remit still applies to this version; however in addition, hyperlinks to accredited websites have been inserted to each section to provide further clinical information which you can access as required. This document is intended only as guidance for management of common ENT conditions seen in primary care and when patients should be referred on to the ENT department. This guidance document also portrays the expertise and knowledge of clinical experts in Barts and the London NHS Hospital Trust. For ease of reference, the names of the consultants, their sub-specialisations and important contacts are detailed below. For further prescribing support, please refer to the BNF website on: http://www.bnf.org/bnf/ 2.0 ENT Consultants and their Sub-specialisation CONSULTANT Mr Santdeep Paun Mr Mike Dilkes Mr Mike Wareing Mr Ghassan Alusi Mr Khalid Ghufoor Mr Nick Eynon-Lewis Miss Kay Seymour Mr Yogesh Bajaj SUB-SPECIALISATION Clinical Lead Rhinology and Facial Plastic Surgery Head & Neck tumour surgery Otology, Neuro-otology, Voice surgery Thyroid surgery, Head & Neck tumour surgery, Rhinology Head & Neck tumour surgery, laser airway surgery, Paediatric ENT Otology, Voice, Rhinoplasty, Paediatric ENT, Otology Paediatric ENT, General adult ENT Paediatric patients are only seen by the stated paediatric consultants. 3 Important Contact details: Consultant ENT Surgeons Medical Secretary Mr Mike Dilkes Mike.Dilkes@bartshealth.nhs.uk 0203 594 1206 Mr Eynon-Lewis Nicholas.EynonLewis@bartshealth.nhs.uk 0203 594 1206 Mr Mike Wareing Mike.Wareing@bartshealth.nhs.uk 0203 594 1207 Mr Gus Alusi Ghassan.Alusi@bartshealth.nhs.uk 0203 594 1207 Mr Khalid Ghufoor Khalid.Ghufoor@bartshealth.nhs.uk 0203 594 1207 Mr Santdeep Paun Santdeep.Paun@bartshealth.nhs.uk 0203 594 1193 Mrs Kay Seymour Kay.Seymour@bartshealth.nhs.uk 0203 594 1193 ENT Associate Specialists Medical Secretary Mr Tapas Goswami Tapas.Goswami@bartshealth.nhs.uk 0203 594 1198/1201 Mr Pishtiwan Mirza Pishtiwan.Mirza@bartshealth.nhs.uk 0203 594 1193 REFERRALS Very urgent non cancer call on-call ENT Registrar via switchboard, 020 7377 7000 Cancer 2 week wait target referral for cancer, Urgent Choose and Book or referral letter to ENT Department Routine Choose and Book or referral letter to ENT Department Key to urgency column: * Urgent ** Cancer *** Emergency/A&E 4 3.0 Common Ear Conditions Urgency Condition 1. Acute Otitis Media GP Management Refer To Treat each attack symptomatically with analgesia. If no improvement after 72 hours, prescribe broad spectrum antibiotics e.g. amoxicillin for 5 days. Start antibiotics at presentation if systemically unwell e.g. high temperature and vomiting (SIGN 2003). If tympanic membrane not visible reexamine in two weeks. If perforation seen, further review needed. If more than 4 episodes in 6 months then refer to ENT. 2. Recurrent Acute Otitis Media http://www.sign.ac.uk/pdf/qrg66.pdf If problems continue e.g. more than 4 episodes in 6 months refer to ENT (SIGN 2003, NICE pilot). Any paeds consultant for children Consultant to consider ventilation tubes (grommets) or prophylactic antibiotics http://www.sign.ac.uk/pdf/qrg66.pdf 3. Glue ear in childhood Persistent hearing problems or language delay. Recurrent earaches. * 4. Chronic Supurative Otitis Media (with or without Cholesteatom a) Hearing loss, abnormal or Refer to the Community Paediatric Audiology Service for assessment at Steel’s Lane Any paeds consultant for children http://www.sign.ac.uk/pdf/qrg66.pdf Refer to ENT consultant for further assessment and diagnosis. Surgery may be indicated for straightforward perforation and is usually indicated for cholesteatoma. Traumatic perforations can be treated by keeping the ear dry and observing for 6 weeks, if they fail to heal, referral is indicated. 5 Wareing Eynon-Lewis Seymour Urgency Condition perforated eardrum, or offensive discharge ** GP Management http://www.gpnotebook.co.uk/simplepa ge.cfm?ID=-435814389 5. Acute Otitis Externa Discharge with oedematous painful ear canal Aural toilet then ear drops containing antibiotics and steroids for 7 days. If systemically unwell, evidence of spreading infection to the pinna or if there is no improvement with the above measures then the patient should be referred to the emergency clinic. http://www.prodigy.nhs.uk/otitis_extern a/view_whole_guidance 6. Chronic Otitis Externa Painless persistent discharge or itching with intact ear drum Advise against using buds and avoiding getting water in ears. Aural toilet. Take swab for microscopy culture and sensitivity and treat accordingly. Unilateral Earache without Otological signs Exclude obvious causes e.g. tonsillitis, temporomandibular joint or dental problems. In absence of clear cause, treat symptomatically. 7. Wax Impaction Cause of reversible hearing loss and otalgia. Wareing Eynon Lewis Seymour If unable to control refer routinely to ENT http://www.prodigy.nhs.uk/otitis_extern a/view_whole_guidance Dilkes Alusi Ghufoor Refer for ENT assessment if symptoms persist beyond 3 weeks, since there may be an underlying Head and Neck cancer, particularly if associated with dysphagia, lump in neck or hoarseness (Fax in a cancer referral form). 8. Refer To The different types of drops to soften wax such as bicarbonate and olive oil are probably all about equally effective. Wax can be removed by syringing (if the ear drum is intact) or by microsuction if equipment and expertise is available. Advice to avoid using buds should also be given. 6 Urgency Condition GP Management Refer To http://www.prodigy.nhs.uk/earwax/view _whole_guidance www.entnursing.com 9. Tinnitus Exclude obvious local causes such as wax impaction. If healthy tympanic membrane, review after 4 weeks. If symptoms persist and are troublesome refer to ENT consultant. Wareing Eynon Lewis Seymour Refer all unilateral tinnitus as rarely this can be a presentation of acoustic neuroma. http://www.gpnotebook.co.uk/simplepa ge.cfm?ID=26542053&linkID=56408&cook=yes www.tinnitus.org.uk 10. Acute vertigo Requires ENT and neurological examination by GP. Treat with vestibular sedatives such as prochlorperazine (po/ IM injection) or Buccastem. If severe and vomiting refer to A & E. If mild but persists for more than 6 weeks consider ENT or neurological referral. http://www.entuk.org/patient_info/ear/di zziness_html http://www.icms.qmul.ac.uk/chs/Docs/6 3538.pdf 11. Chronic Unsteadines s /Dizziness The history is usually the key to the diagnosis. Patients require a multisystem assessment including cardiovascular, ENT and neurological examination as appropriate. Consider referral to appropriate specialist such as ENT/ Neurology/ Elderly Care etc. 7 Wareing Eynon Lewis Seymour Urgency Condition GP Management Refer To http://www.gpnotebook.co.uk/simplepa ge.cfm?ID=-1348861947 12. Hearing loss a) *** b) c) d) Sudden unilateral conductive hearing loss caused by ET dysfunction or middle ear fluid May follow URTI/air flights/diving. Diagnose with tuning fork tests and clinical examination Topical nasal decongestant e.g. xylometazoline hydrochloride bd for 1 week with nasal steroid for 4 weeks or a combination spray e.g DexaRhinaspray bd for 2 weeks. Gentle “auto inflation” of middle ear if possible may help. Sudden unilateral sensorineural hearing loss with normal tympanic membrane Refer to ENT doctor on call. This needs to be seen urgently as early treatment may improve prognosis. Over 65 years old with bilateral hearing loss Other forms of hearing loss Refer to Hearing Aid service/clinic at the Audiology department If continued problems after 4 weeks refer to ENT consultant. (Remember Nasopharyngeal carcinoma can present with unilateral middle ear fluid) http://www.gpnotebook.co.uk/simplepa ge.cfm?ID=-389021685 Refer routinely to ENT Consultant for assessment. Wareing Eynon-Lewis Seymour http://www.gpnotebook.co.uk/simplepa ge.cfm?ID=1214971909 3.1 TUNING FORK TESTS (512 HZ TUNING FORK) 8 These can be helpful in the clinical assessment of hearing impairment but need to be taken in the context of the history, examination and audiometry if available Rinne's Test: Vibrate the fork gently by striking it on your elbow, then hold the fork parallel to the side of the head so that the end of the nearest tine is held 1cm from the entrance of the ear canal. Ask patient to compare the loudness heard when doing this compared with the loudness heard when the fork base is placed firmly on the adjacent mastoid tip. A positive test is when the former is loudest, a negative test is when the mastoid is loudest (signifies possible conductive hearing loss although can be negative in a dead ear as the sound is transmitted to the opposite cochlea i.e. false negative) Weber's Test: Vibrate the fork as before, place it with the base firmly on the forehead. If the patient hears the sound in only one ear this may indicate one of 2 things – either the ear in which it is heard has a conductive loss or the ear in which it is not heard has a sensori-neural loss. PICTURE 9 4.0 COMMON NASAL CONDITIONS Urgency *** Condition 1. Fractured Nose GP Management Refer To Following injury, check for complications such as other facial fractures, diploplia and septal haematoma. If there are none review the patient in 5 days. If there is a new deformity refer to the next day’s emergency clinic. Nasal fractures generally require manipulation within 2 weeks. Emergency clinic http://www.entuk.org/patient_info/nose/in juries_html. *** 2. Nose Bleeds a) Childhood recurrent b) Adult 1) Naseptin cream or mupirocin 2% ointment to Little’s area twice daily for 10 days. Advise against nose picking. 2) Consider performing Silver Nitrate cautery to Little’s area in GP surgery after local anaesthetic, e.g. Xylocaine spray, then prescribe Naseptin antibiotic cream. Advise against nose picking. 3) Refer to ENT consultant if not controlled. http://www.gpnotebook.co.uk/simplepag e.cfm?ID=1818951686 http://www.entuk.org/patient_info/nose/tu mours_html 1) For intermittent short-lived bleeds, manage as above if bleeding point is on the anterior septum. 2) For prolonged or severe epistaxis attempt nasal packing if possible and refer to ENT doctor or Accident & Emergency Department depending on severity, for further management. http://www.gpnotebook.co.uk/simplepag e.cfm?ID=1818951686 http://www.entuk.org/patient_info/nose/tu mours_html 10 Bajaj Seymour Ghufoor Paun Eynon Lewis Ausi Bajaj Seymour Urgency Condition GP Management 3. Sinusitis Examine nose for obvious purulent discharge and assess maxillary tenderness. a) Acute maxillary Many are viral and will resolve without antibiotics. Oral analgesia may be required. If severe or persistent, treat with augmentin or erythromycin. Refer To Refer to ENT emergency clinic if symptoms worsen in spite of medical treatment. Patient may require antral drainage. Chronic problems refer to ENT department http://www.gpnotebook.co.uk/simplepag e.cfm?ID=1678114826 http://www.gpnotebook.co.uk/simplepag e.cfm?ID=2120941596&linkID=21882&c ook=yes b) Chronic Examine as above. Treat patients with topical steroid drops such as betamethasone for 3 weeks followed by topical steroid sprays for a further 3 weeks. Consider asking to douch with alkaline salty solution (OTC such as sterimar / sinus rinse or can be made up by patient). Add antihistamines if allergic symptoms. If symptoms persist despite this, refer for specialist opinion. Paun Alusi Eynon Lewis Bajaj 4. Nasal Obstruction 11 Urgency ** Condition a) Unilateral and always on the same side GP Management Refer To Trial of topical steroid spray such as mometasone or fluticasone for at least 8 weeks with antihistamine if possible allergy e.g hay fever. Refer to ENT consultant. Often a deviated septum. Paun Alusi Eynon Lewis Bajaj Refer urgently if any worrying symptoms such as pain or bleeding which may indicate a tumour. (Fax in a cancer referral form) http://www.gpnotebook.co.uk/simplepag e.cfm?ID=241893387 b) Bilateral or alternating sides (usually allergic or vasomotor rhinitis, polyps, or adenoid) Trial of topical steroid spray such as Beclomethasone for at least 8 weeks with antihistamine if possible allergy e.g hay fever. If symptoms persist refer to ENT for assessment and allergy tests as required. http://www.ncbi.nlm.nih.gov/entrez/query .fcgi?cmd=Retrieve&db=pubmed&dopt= Abstract&list_uids=15725193&query_hl= 15 http://www.gpnotebook.co.uk/simplepag e.cfm?ID=959446990&linkID=63777&cook=yes 5.0 COMMON THROAT CONDITIONS 12 Paun Alusi Eynon Lewis Bajaj Urgency Condition 1. Acute Tonsillitis GP Management Refer To Treat with analgesics, hydration and antibiotics if failure to resolve. Choice of antibiotic is controversial but Penicillin V will cover Streptococcus pyogenes and is usually a good first line. On call as required Consider Infectious Mononucleosis . Refer to ENT for possible tonsillectomy, if a 3 year history of at least 4 attacks per year or significant disruption to life. http://www.cks.library.nhs.uk/sore_throa t_acute/in_depth/management_issues *** 2. 3. Quinsy Usually Unilateral peri-tonsillar swelling, dysphagia and “hot potato voice” Hoarseness/ loss of voice https://entuk.org/ent_patients/throat_con ditions/tonsil_surgery Refer to Emergency clinic or ENT doctor on call. http://www.gpnotebook.co.uk/simplepag e.cfm?ID=1778778125 If this arose following upper respiratory infection/laryngitis consider treatment with broad-spectrum antibiotics, voice rest for 4 days and steam inhalations. If hoarse voice persists beyond 3 weeks or is not associated with URTI refer to ENT consultant urgently. (Fax in a cancer referral form) Patients with long-standing hoarseness can be referred to a voice clinic. http://www.gpnotebook.co.uk/simplepag e.cfm?ID=1221591081 http://www.entuk.org/patient_info/throat/ hoarseness_html http://www.mrw.interscience.wiley.com/c ochrane/clsysrev/articles/CD005054/fra me.html 13 Ghufoor EynonLewis Urgency Condition 4. Sensation of lump in throat Able to swallow solids and liquids normally GP Management Examine pharynx for gross abnormality and palpate neck for lumps. If no other risk factors such as smoking, a trial of antireflux therapy such as lansoprazole for 2 weeks may be worth trying prior to referral. If history suggests the need to examine the lower throat region refer to ENT consultant for subsequent assessment. Refer To Dilkes Ghufoor Alusi If neck lump or ulceration in pharynx refer urgently to ENT consultant (Fax in a cancer referral form) http://www.gpnotebook.co.uk/simplepag e.cfm?ID=315293621&linkID=56500&cook=yes ** 5 Foreign Body Throat Acute pain and Dysphagia This usually requires referral to emergency clinic or ENT Registrar on call. It may be possible to remove a FB such as a fish bone from the oropharynx in your surgery. If patient develops stridor then will require ambulance to A & E 6. True Dysphagia For liquids or solids Usually with weight loss Refer urgently to ENT consultant if present for more than 3 weeks (fax in a cancer referral form) Dilkes Ghufoor http://www.gpnotebook.co.uk/simplepag e.cfm?ID=315293621&linkID=56500&cook=yes 14 Alusi 6.0 OTHER ENT EMERGENCIES 6.1 Facial Nerve palsy * Identify if upper or lower motor neurone (if there is sparing of the forehead, it is upper). Upper motor lesions need urgent referral to neurology; lower motor lesions need basic ENT assessment – exclude parotid gland neoplasm, middle ear abnormality. Look for vesicles on the TM or in the ipsilateral throat – these signify possible Ramsay-Hunt. If the lesion if felt to be traumatic, immediate referral to ENT is indicated, otherwise, if no pathology is found, start regular acyclovir and systemic steroids for 2 weeks. If pathology is found, urgent referral to ENT. http://www.gpnotebook.co.uk/simplepage.cfm?ID=-281739261 6.2 Stridor *** Airway obstruction can be due to ENT or chest problems. With ENT causes, there is often voice change and dysphagia. Stridor is usually inspiratory or biphasic, with chest problems it is often expiratory. Look for neck nodes to suggest an upper airway tumour. For ENT stridor call the ENT registrar on-call, administer oxygen or heliox and call an ambulance to take the patient to A&E immediately. http://www.gpnotebook.co.uk/simplepage.cfm?ID=-885719031 7.0 EMERGENCY/ URGENT CLINICS 7.1 One-stop lump and bump clinic This is a service in which referral can be made directly by GP’s telephoning the one-stop head and neck line (see above for number). Any Head and Neck lump and bump from thyroid tumour to sebaceous cyst can be referred. Referral guidance for suspected cancer should be followed and cancer patients referred using the 2WW proforma and the fax number on page 1 of this document. If suspected cancer, patients will be seen within 10 working days, and have full ENT examination, followed by ultrasound and cytology if indicated. Results of cytology will be ready within 20 minutes. It is aimed that 75% of patients will either be discharged or placed on the waiting list for surgery after 1 visit. 15 7.2 Emergency Clinic A nurse-led ENT Emergency Clinic is held each morning, Monday-Friday at Barts Hospital, from 9.30-12.00. Patients referred to the ENT Emergency Clinic need to bring with them their referral form – filled out by their GP/referring clinician. During working hours: After filling out the referral form, please tell the patient to contact Central Appointments (0207 767 3200 – open from 8.30am) to be given a time-slot to attend the clinic. Out of hours: Clinicians will need to contact the on-call SHO, who will triage the patient. If suitable for the Emergency Clinic, the referrer will then need to inform the patient that they will be seen in the Emergency ENT Clinic, and again ask them to ring Central Appointments to be given a slot. Once the patient has been seen in the Emergency ENT Clinic, patients will be given a follow up appointment if necessary. This will be done by the ENT reception staff. When referring patients to the Emergency Clinic, some clinicians may wish to send relevant patient information electronically. If this is the case, please send your emails to _ENTBartsEmergencyclinic@bartsandthelondon.nhs.uk, ensuring you include the patient’s NHS number within the email. 16
 0
0
advertisement


Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users