Diarrhoea and Dehydration In this paper we will consider What we

Diarrhoea and Dehydration
In this paper we will consider
1. What we need to know
Why treating diarrhoea is important
Understand different forms of diarrhoea
The meaning of SSS & ORS
Understand the dangers of diarrhoea
2. What we need to do
Set aims and targets
Choose a suitable method with the community
Prepare ORS appropriately
Feed ORS correctly
Teach the use of ORS to all family members
Explain how diarrhoea can be prevented
Evaluate the programme
What We Need To Know
Why treating diarrhoea is important
Diarrhoea kills at least two million children per year, making it the commonest cause of death in children under five, after pneumonia. If we manage diarrhoea correctly nine out of ten of these deaths can be prevented.
Diarrhoea usually causes death through dehydration. In addition it leads to malnutrition which further weakens health, so that diseases such as malaria and measles may prove fatal
Understand different forms of diarrhoea
Diarrhoea means passing stools which contain more water than usual. Usually they will be more frequent, but frequent stools which are otherwise normal do not count as diarrhoea. For practical purposes diarrhoea is usually defined as passing three or more loose or watery stools in 24 hours.
There are different types of diarrhoea, WHO suggests these categories:
Acute watery diarrhoea lasting 14 days or less
Persistent diarrhoea lasting more than 14 days
Dysentery, diarrhoea with blood, with or without fever
Many different germs cause diarrhoea but in practice all forms of diarrhoea are treated with Oral Rehydration
Solution (ORS). In addition, for persistent diarrhoea we should try to find a cause, e.g. Amoeba or Giardia and treat this. For dysentery we should usually use antibiotics.
The meaning of ORS and SSS
SSS stands for Oral Rehydration Therapy . This is a treatment for dehydration
Oral Rehydration Salts (ORS) , either packeted of home prepared are mixed with water and given to those with diarrhoea.
This solution which contains salt and sugar is life saving. The child needs the fluid and the salt to replace that lost in diarrhoea. Added sugar helps water and salts to be absorbed from the stomach and also gives energy.
The use of Salt-Sugar Solution (SSS) in treating diarrhoea has been described as one of the greatest medical discoveries of the twentieth century. Nearly all cases of dehydration could be prevented and nearly two million lives saved per year if parents worldwide knew how to make SSS and give it appropriately.
It has been calculated that on average it takes about 30 minutes to teach a community member about the effective use of ORS. This may seem a long time but in terms of saving lives is there any more effective way of spending half an hour?
Understand Dangers of Diarrhoea
1. Diarrhoea itself is dangerous, causing death by dehydration. In addition:
It leads to malnutrition if prolonged
It is highly infectious, rapidly spreading in communities especially where there is poverty and overcrowding
2. The wrong treatment of diarrhoea can be dangerous.
Many doctors and health workers still believe that diarrhoea should be treated by medicines and injections.
They may give intravenous fluids even when the patient is able to drink by mouth. Some know little about
ORS and many more will not use it because it brings less profit than antibiotics or injections. One reason why medicine continues to be used is because it appears to cure diarrhoea, usually however diarrhoea is self-limiting and would have stopped anyway. The greatest threat of diarrhoea is dehydration.
Medicines for diarrhoea may be dangerous in themselves, but the greatest danger is the delay the cause. Instead of starting home-based care SSS at once, parents may delay treatment of dehydration and waste valuable hours seeking the wrong remedy from a clinic or pharmacy.
3. The incorrect use of ORS may be dangerous. Although ORS potentially saves more lives worldwide than any other treatment it does have occasional dangers.
Too much salt can be given and this may occasionally cause convulsions. For this reason ORS needs careful measurement and the solution must always be tasted before it is given.
Too little fluid may be given so failing to treat the dehydration rapidly enough
It may be fed too fast or impatiently, causing vomiting or refusal in the child
4. Serious types of diarrhoea may present.
Dysentery caused by Shigella and other organisms may be present needing antibiotics
Diarrhoea may be persistent (lasting more than 14 days) needing diagnosis and further treatment.
Serious epidemic forms of diarrhoea may be present including cholera and typhoid needing a coordinated community approach.
Regardless of cause, some children may need intravenous treatment and referral to hospital. Village health promoters need to teach parents to be alert to the danger signs. Parents need to be taught how to make and give ORS as a first line measure to treating and preventing dehydration.
What We Need to Do
Set aims and targets
Our ultimate aims are these:-
1. To make sure that sure that every family member (child minder – mother, father, older sibling, grandparent, aunt, uncle, etc) in the community knows how to make and use ORS
2. To make sure that every child (or adult) with diarrhoea actually receives ORS and it is given in the appropriate manner.
Our targets could be
30% of child minders understand and use ORS appropriately after six months, 50% after one year, 90% after two years.
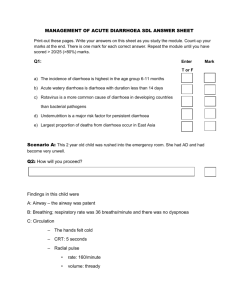
Assessing Dehydration
Condition Well, alert
PLAN A
*Restless, irritable* *Lethargic or unconscious, floppy*
B C
Look at Eyes
Tears
Normal
Present
Sunken
Absent
Very Sunken
Absent
Very Dry
*Drinks poorly or not able to drink*
Feel
Decide
Mouth and Tongue Moist
Thirst Drinks normally not thirsty
Skin Pinch
Dry
*Thirsty, drinks eagerly*
Goes back quickly *Goes back slowly*
Patient has NO signs of dehydration – Still give ORS
If patient has 2 or more sighs including even 1
*sign* there is
SOME dehydration
*Goes back very
Slowly*
If patient has 2 or more signs, including even 1
*sign* there is
SEVERE dehydration
Signs of Child with Dehydration
Choose a Suitable Method with the Community
There are many different ways of preparing ORS. Before starting a programme we must work out carefully with the community which method is most suitable. We will make our task harder if we start using one method at the beginning then change to another later.
We can follow these guidelines
1. Decide which overall method is most suitable a. Consult with the People
Discover which containers and measures are commonly used at home. Find out if ORS packets re available locally. Discover what liquid foods are fed to children. Ask for the community's suggestions. b. Follow the National Guidelines
Many countries now have national programmes. Find out about these and follow them where possible.
Even if there is no national programme, there may still be a method in use in the County, District or project area.
2. Decide whether to use packeted or home-made ORS.
Unless packets are cheap, easy to obtain and always available families should learn how to prepare their own ORS (SSS) at home. They can still use packets when available, but their children will not die when supplies of the packets run out.
Home made ORS can either be a salt-sugar solution or traditional liquid food such as rice water, soups, fruit juices, dilute tea, potato water, carrot juice or coconut milk.
Liquid foods have various advantages, they are easily available, children are familiar with them, they reduce the stool volume if some salt is added, and they provide food as well as fluid.
3. Decide on containers in which to make up the solution.
Containers used should be known by everyone, be available in the homes and always be the same size, ie beer, soft drink or water bottles, cups or glasses.
4. Decide on measuring devices for salt and sugar
Again, these must be widely known, easily available and of standard size. They must be simple to use so that mistakes are not made in the amounts measured. Here are some examples:
A 5ml teaspoon.
A human fistful of sugar and a thumb and two finger pinch of salt. Although less accurate this remains an important method in poor communities.
A bottle top
Prepare or ORS Appropriately
Having decided what is most appropriate in terms of container, measures, packets or home-made preparations, we now need to prepare the solution.
Here are some examples of how ORS can be prepared:
1. Home made sugar-salt solution
To make a one litre solution (as recommended by WHO) add six level teaspoons (5ml) of sugar plus one level teaspoon (5ml) of salt to one litre of clean water.
To make a half litre solution add one fistful (four finger scoop) of sugar plus one pinch (thumb and two fingers) of salt to half a litre of clean water.
To each of the above we can squeeze in lime, lemon or orange if available to give taste and provide potassium.
2. Home prepared liquid foods - Do NOT use in children under six months
To make one litre of rice water:
Grind any sort of ground rice into powder
Take two to three large tablespoons of the above and pour in one litre of water
Add two pinches of salt
Boil and stir for five to seven minutes
Cool and feed
Ground dried wheat, sorghum, millet, maize or potato can be prepared in similar ways. Coconut juice can be given with two pinches of salt added per litre. Do not add any potassium. Weak tea can be used to which is added salt and sugar in the same amounts as in preparing salt-sugar solution.
3. Packeted ORS
We should make sure that any packets are approved by the MoH, that they are not overpriced and that they have not expired or have damaged packaging. Packets should have written and illustrated explanations on how to mix otherwise illiterate people may not understand how to make ORS from packets and therefore could be unsafe.
Feed ORS Correctly
ORS should be given to the child by its mother or other family member. We can first demonstrate this and then observe the mother doing it herself.
How to Prepare
1. Prepare the solution as described earlier
2. Taste it, it should taste less salty than tears, if too salty it can cause harm to the child
3. Feed it to the child (see How to Feed ORS)
When to Give ORS
Start giving ORS as soon as the diarrhoea starts. Continue giving until both diarrhoea stops and a normal amount of urine is being produced.
How to Feed ORS
Feed young children from a spoon, giving one teaspoon every 1-2 minutes. Give older children frequent sips from a cup.
If the child vomits wait 5-10 minutes then try again more slowly. ORS can help reduce the feeling of nausea.
Breastfed children should continue to be breastfed.
As soon as possible start giving soft foods that are easy to digest in small amounts, eg bananas, and cereals.
As soon as the child has recovered from diarrhoea give extra food, with added vegetable oil.
(see annex – How to Treat Dehydration)
Teach the use of ORS to ALL family members
Our aim is for every community member to know about ORS, for the use of ORS to become completely accepted as the first line response to preventing dehydration.
We will need to make sure that every member of every family:
Knows how to make ORS
Knows how to use ORS
Believes in ORS so that when diarrhoea occurs ORS is given at once and with confidence.
Here are some ways of encouraging the community to use it.
1. Understand local beliefs about diarrhoea. Communities are often reluctant to use ORS. We must discover local beliefs about diarrhoea and why people are suspicious of using ORS.
For example in some parts of Africa many people belief that giving fluid makes diarrhoea last longer, therefore children with diarrhoea are not given fluids. This is quite logical when people believe that diarrhoea rather than dehydration kills the child.
Explain to parents that children die, not from the diarrhoea itself but because they dry out. You could show them a fruit that has been dried in the sun or dried up plant.
Explain that ORS does not necessarily stop the diarrhoea. Mothers may know this anyway. In fact ORS may seem to make diarrhoea worse and children will often pass a stool shortly after receiving ORS. Explain to mothers that this may happen. (this is more likely to happen with a liquid food).
Another example. People with easy access to practitioners and pharmacies often believe that the only effective treatment for diarrhoea is a medicine, injection or intravenous drip given by doctors and that home made remedies are useless.
These beliefs (wrong ideas) have to be discussed with the community until they become aware of the benefits of ORS. Unless objections and beliefs are faced up to the community will politely listen then go away and ignore our advice.
2. Demonstrate the use of ORS in the homes. This can be done by the Community Health Volunteer (CHV) how can work with the mothers until they are confident in making and using ORS. It is important that the
CHV uses ORS themselves in their families.
3. Help the community leaders to know about ORS, to use it themselves and to encourage its use in the community. Teachers, religious leaders and shopkeepers should all be aware.
4. Teach children, older siblings can give it to younger ones. Teaching of ORS can become part of the school health programme.
Explain How Diarrhoea Can be Prevented
Teaching on how to prevent diarrhoea must always go alongside teaching of how to treat it.
1. Promote breastfeeding . Up to two years and encourage exclusive breastfeeding up to six months
Breast is Best
It is the natural food for babies, having the perfect balance of nutrients and providing natural protection against illness.
It is free and easily available
It is clean, meaning the baby is less likely to get diarrhoea and so less likely to die
Breastfeeding strengthens the bond between mother and child
Breastfeeding, if regular and frequent, can act as a contraceptive and so help child spacing
Colostrum is good.
The watery milk produced in the first one or two days is not 'bad milk' but full of nutrients and antibiotics which the child really needs.
Breastfeeding should be continued where possible for at least two years. WHO now recommends it should be used exclusively up to six months.
Mothers often incorrectly believe they cannot make enough milk. Where this is the case encourage the mother to
Drink more fluids
Eat more green leafy vegetables
Allow the baby to suckle more often, day and night. The more the baby sucks the more milk is produced. This is especially important during the first few days after birth.
3. Teach good personal hygiene. Especially hand-washing. Regular hand-washing can decrease attacks of diarrhoea by one third.
4. Use the cleanest water available for drinking and preparing food.
5. Promote the use of latrines and burial of children's faeces which is much more infectious than that of adults
6. Reduce the fly population. Bury or bury domestic garbage, bury faeces or use latrines, cover food both at home and at the market. Use fly traps.
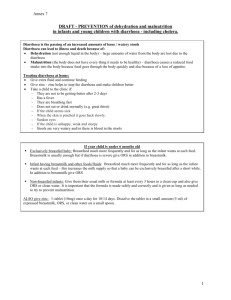
Diarrhoea Prevention – Breaking the F Cycle
FLIES
Bury faeces
Use latrines
FAECES
Cover Food
FOOD
Wash hands
After defecation
FINGERS
Wash hands before eating
Wash hand before preparing food
Evaluate the Programme
After an agreed period of time the programme should be evaluated to see if targets are being met. We can discover
Whether family members are using ORS in practice. We can do this informally by keeping alert, enquiring from community members and CHV, doing spot checks. Or we can do this more formally, preparing a questionnaire for use. We could ask: o How, when and why use ORS o How families have treated diarrhoea in the last six months
Have deaths from diarrhoea decreased, however there could be other factors responsible for a reduction in diarrhoea, improved nutrition for example.
Summary
Diarrhoea and dehydration cause millions of unnecessary deaths each year. By the simple use of homebased ORS most of these deaths could be prevented.
In preparing a programme with the community decide which forms of ORS are most appropriate for the community and which containers and measuring devices are most suitable. Any method selected must be acceptable to the community and follow the National Guidelines.
All community members should learn how to make and prepare ORS and be able to feed it to those with diarrhoea. Repeated and imaginative teaching methods are needed to raise community awareness and change incorrect beliefs.
As well as teaching how to treat dehydration we must teach methods on how to prevent diarrhoea.
The programme should be evaluated after an agreed amount of time to assess whether ORS is actually being used and used properly. A base line study needs to be conducted before the training programme starts so that you can measure the success of the programme and assess the knowledge of community members.