1_Prevalence, clinical features and drug susceptility of pulmonary

Barameht Piralam
Prevalence, clinical features and drug susceptibility of pulmonary tuberculosis among adult hospitalized patients in rural Thailand
1. Introduction
Tuberculosis is a major cause of illness and death globally. In 2011, the World
Health Organization (WHO) reported that 8.7 million new cases of tuberculosis occurred, with 1.4 million died, new acid-fast bacilli (AFB) smear–positive, pulmonary cases
Thailand is on the 18th rank of 22 countries designated by the WHO as “high burden” with regard to tuberculosis; it has an estimated annual incidence of 94 tuberculosis cases per 100,000 populations, with mortality 11 cases per 100,000.
1
One study of patients with tuberculosis in 7 public hospitals found that diagnostic delays were common in Thailand, with a median time of 2.8 weeks between first presentation to a healthcare facility and tuberculosis diagnosis.
2
Among persons admitted with active tuberculosis disease to hospitals in Thailand, transmission to healthcare workers and other patients occurs frequently.
3
As drug resistance emerges globally, the consequences of such delays might be devastating, as documented in nosocomial outbreaks of multidrug resistant tuberculosis in the United States and
Europe in the late 1980s and extensively drug-resistant tuberculosis in South Africa in
2006.
4-6
2. Objectives
1.
To examine the prevalence of tuberculosis among hospitalized patient
2.
To identify the clinical sign and symptom of hospitalized tuberculosis
3.
To determine drug susceptibility of hospitalized tuberculosis patient
3. Methods
3.1 Setting
Nakhon Phanom is located along Mekong River which 735 kms from
Bangkok in the northeastern part region of Thailand. Nakhon Phanom comprise of 12 districts in each district with a population of at least 10,000 persons. There are 13 hospitals, including 1 general hospital (345 beds), 11 community hospitals (10-120
1
Barameht Piralam beds) and 1 Ministry of Defense hospitals. For the general hospital that offers some primary-care services but also serves as the referral center for complicated medical conditions outside the scope of the community hospitals. All of these public facilities are able to perform and interpret chest radiography to indentify the radiographicallyand are able to perform and interpret chest radiography and sputum smear microscopy for AFB. The total population of year 2012 is 704,730 persons, of these populations have only a primary school education and the economy is agricultural mainly focused on rice, tobacco and rubber and the yearly capita income is 23,000 baht in 2012.
7
3. Tuberculosis Surveillance for adult hospitalized patient
In 2003, the International Emerging Infections Program (IEIP), collaboration between the Thailand Ministry of Public Health and the US Centers for Disease
Control and Prevention, conducts active, population-based surveillance for hospitalized patients with pneumonia in Nakhon Phanom provinces. An active surveillance have lunched to get an accurate measure of the incidence of radiographically confirmed pneumonia requiring hospitalization: surveillance officers
(SO) in each hospitals screened hospital admission logbooks from all hospitals daily to identify patients admitted with the potential diagnosis for pneumonia consisted with 59 diagnoses in the International Classification of Disease codes (A15-A16,
A19, A24, A37, B20, B22-24, B59, J10-22, J40, J45-46, J69, J80-81, J84, J90-93,
J96, J98, P22-26, R05-06, R09, R50). After the patient chart finding, each SO will be reviewed the medical record and collected demographic, clinical, laboratory, and radiographic findings on a standardized surveillance form. Physicians completed a data section on clinical signs and symptoms. All information will be entered into a computerized database each hospital and daily uploaded via internet into server at
MOHP in Nonthaburi. To ensure the data accuracy, data audit will be launched daily by each SO and quarterly by SO team.
8
During 2009 to 2010, IEIP Nakhon Phanom have been launched tuberculosis surveillance among adult hospitalized clinical pneumonia in all hospital in Nakhon
Phanom province to determine the prevalence of tuberculosis among these patient
Standing order to collect sputum in all clinical pneumonia patients were launched
2
Barameht Piralam
3.3 Adult hospitalized tuberculosis case definition
3.3.1 Clinical pneumonia patient
Clinical pneumonia patient was defined as a hospitalized patients who met inclusion diagnosis and presented 1) evidence of acute infection (at least 1 of the following: reported fever or chills, documented temperature higher than 38.2°C or lower than 35.5°C, white blood cell [WBC] count higher than 11,000 cells/ mm3 or lower than 3,000 cells/mm3, or abnormal differential WBCcount) ; and 2) signs or symptoms of lower-respiratory-tract illness (at least 1 of the following: abnormal breath sounds on chest auscultation, tachypnea, cough, sputum production, hemoptysis, chest pain, or dyspnea) in a resident who has lived in Nakhon Phanom at least 6 months.
3.3.2 Adult hospitalized tuberculosis patient
All clinical pneumonia patient who have either positive for AFB testing
1of 3 or TB culture
3.4 Study Population
All clinical pneumonia patient who were admitted since September 1, 2008 and December 31 st
, 2010 and either positive for AFB testing 1of 3 AFB smears or TB culture from pneumonia surveillance database will be included for this study. Patients younger than 15 years of age are excluded because the recommended diagnostic approach to tuberculosis differs for children and because infectious tuberculosis is uncommon in children.
3
Barameht Piralam
3.5 Statistical Analysis
The descriptive statics: rate, percentage will be implemented to calculate prevalence rate, clinical features and drug susceptibility of tuberculosis among adult hospitalized patients
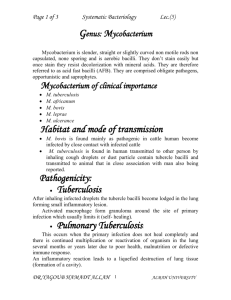
Figure 1 Conceptual frameworks:
Adult hospitalized tuberculosis
1. Prevalence of pulmonary TB
2. Clinical features
Signs of acute infection
- fever
- hypothermia
- abnormal white blood count
Respiratory Signs and
Symptoms
- cough
- sputum production
- hemoptysis
- chest pain
- dyspnea
- rhinitis
- tachypnea
Chest radiographs
- consolidation
- infiltration
- pleural effusion
- atelectasis
- cavitation
3. Drug susceptibility
4
Barameht Piralam
References
1 .
WHO Tuberculosis Report 2012. (Cited May 30, 13).
Available at: ttp://www.who.int/tb/publications/global_report/gtbr12_executivesummary.pdf
2. Rojpibulstit M, Kanjanakiritamrong J, Chongsuvivatwong V. Patient and health system delays in the diagnosis of tuberculosis in Southern Thailand after health care reform. Int J Tuberc Lung Dis 2006;10: 422– 428.
3. Yanai H, Limpakarnjanarat K, Uthaivoravit W, Mastro TD, Mori T, Tap- pero JW. Risk of Mycobacterium tuberculosis infection and disease among health care workers, Chiang Rai, Thailand. Int J Tuberc Lung Dis 2003; 7:
36 – 45.
4. Menzies D, Fanning A, Yuan L, Fitzgerald M. Tuberculosis among health care workers. N Engl J Med 1995; 332: 92–98.
5. Centers for Disease Control. Epidemiologic Notes and Reports: nosocomial transmission of multidrug-resistant tuberculosis among HIV-infected persons-Florida and New York, 1988-1991. MMWR Morb Mortal Wkly Rep
1991; 40: 585–591.
6. Gandhi NR, Moll A, Sturm AW, et al. Extensively drug-resistant tubercu- losis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. Lancet 2006; 368: 1575–1580.
7. Nakhon Phanom Province Office. Nakhon Phanom province briefly information, year 2012 . (Cited May 28, 2013). Available from URL: http://103.28.101.10/ briefprovince/filedoc/48000000.pdf
8. Olsen SJ, Laosiritaworn Y, Siasiriwattana S, Chunsuttiwat S, Dowell SF.
The incidence of pneumonia in rural Thailand. Int J Inf Dis 2006; 10:439 –
445
9. World Health Organization (WHO). TB manual: National Tuberculosis
Programme guidelines. Geneva: World Health Organization; 2001. (Cited May
30 th
, 2013) Available from URL: http://www.euro.who.int/document/e75464.pdf.
5