Client history Form - A Touch of Balance
advertisement

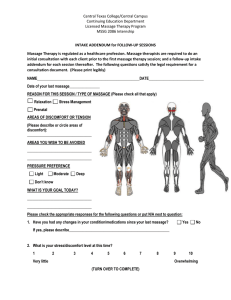
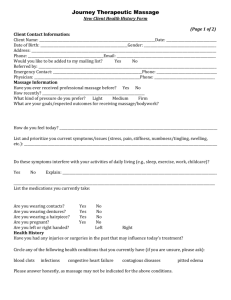
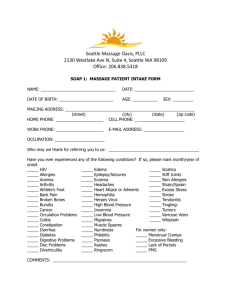
A Touch of Balance New Client History Form/Pain and Discomfort Chart In order to maximize the effectiveness and safety of massage sessions, please take the time to carefully fill out this questionnaire. This information will be treated confidentially. Your feedback is appreciated during and at the end of the sessions to help in modifying the massage session to serve in the best possible way. Please print clearly. Name:_________________________________________________ Today’s Date:____ /____ /____ Home Address:_______________________________________________ City _________________ Province_______________ Postal Code:______________________ Date of Birth:____ /____ /____ Cell #: :______________________________________ Home #:____________________________ Email: ___________________________________________________________________________ Occupation(s):____________________________________Referred by: _______________________ Is the massage covered by your insurance? ___Yes ___No *** If NO, Please inquire about special discount to make regular treatment more affordable. 1) Have you had any previous experience with massage? ___YES ___NO If yes, please explain whether for stress relief/relaxation or treatment of a specific condition diagnosed by a physician: _________________________________________________________________________________ 2) FEMALE CLIENTS: Are you pregnant? If so, due date: __________________________________ 3) Please mark an [X] for all conditions that apply now. Put a [P] for past conditions. [ ] headaches, migraines [ ] injuries to face or head [ ] sinus problems [ ] jaw pain, TMJ problems [ ] asthma or lung conditions [ ] constipation, diarrhea [ ] abdominal or digestive problems [ ] chronic pain [ ] muscle or joint pain [ ] muscle, bone injuries [ ] numbness or tingling [ ] sprains, strains, dislocations [ ] arthritis, tendonitis, bursitis [ ] scoliosis, spinal column injury [ ] osteoporosis [ ] bone or joint disease [ ] cancer, tumors [ ] diabetes [ ] heart, circulatory problems [ ] fatigue [ ] dizziness, vertigo [ ] tension, stress [ ] depression [ ] sleep difficulties [ ] allergies, sensitivity [ ] skin rash, athletes foot, nail fungus [ ] infectious disease [ ] blood clots [ ] varicose veins [ ] high/low blood pressure [ ] nervous system disorder [ ] other condition not listed 4) Explain any areas noted above and note if you are currently seeing a doctor for any of the conditions: ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ PLEASE CONTINUE ON THE BACK PAGE 1 5) Current medications, vitamins, herbs, and nutritional supplements you are taking including common nonprescription medications: ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ 6) Have you had any surgeries or injuries within the last five years? If yes please explain: ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ 7) Please explain your current exercise and stretching routine. ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ 8) What is your goal/concern for today’s session? ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ 9) Are you interested in adding prayer to your session today? ___YES___NO How can I pray for you? ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ 10) What are your long-term health goals? ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ Please check off any options you would like more information on: ( ) Nutritional Supplements ( ) Life Purpose Coaching ( ) Ioncleansing ( ) Christian Massage ( ) Stretching Routines ( ) Pathway to Purpose – Book Study Club ( ) Walking Club ( ) Prayer Chain ( ) Sign me up for Monthly Newsletters/Promo Information Preferred Email: _______________________________________________ ( ) check if same as above 2 PAIN & DISCOMFORT CHART 1) Please indicate the areas where you have pain ( X ) and/ or any Numbness ( N ). If your pain seems to refer or “shoot out” to another area of your body please indicate with arrows. 2) For how long have you experienced pain/discomfort in the areas indicated above? ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ______________________________________________________________________________________________________________ ______________________________________________________________________________________________________________ 3) Describe what you do that causes pain, and what activities make it worse: ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ______________________________________________________________________________________________________________ ______________________________________________________________________________________________________________ I HAVE STATED ALL CONDITIONS THAT I AM AWARE OF AND THIS INFORMATION IS TRUE AND ACCURATE. I WILL INFORM YOU OF ANY CHANGES IN MY HEALTH STATUS BEFORE MY NEXT MASSAGE SESSION. I UNDERSTAND THAT A HEALTH PRATITIONER CANNOT DIAGNOSE AND IS NOT A SUBSTITUTE FOR SEEING A PHYSICIAN. _______INTIAL I UNDERSTAND THAT WHEN I MAKE A BOOKING THE TIME IS SET ASIDE SPECIFICALLY FOR ME AND THEREFORE OUT OF RESPECT IF I AM UNABLE TO GIVE 24 HOURS NOTICE OF CANCELLATION I AGREE TO PAY FOR MY SESSION. ________ INTIAL Please sign here _______________________________________ _______________________ Date: _____________________ 3