to this article as a Word Document - e
advertisement

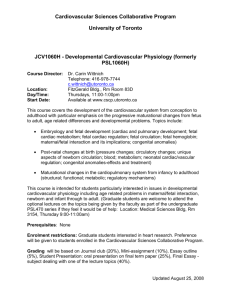
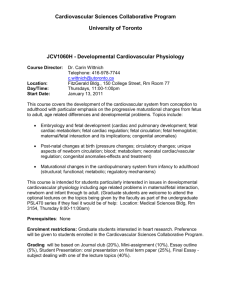
Prenatal Sonographic Diagnosis of Tuberous Sclerosis and Fetal Rhabdomyoma Authors: Lona L. Cook, BSRT, RDMS Scott W. Roberts, MS, MD Objectives: Upon the completion of this CME article, the reader will be able to: 1. List the possible tumors that might develop in the fetal heart. 2. Describe tuberous sclerosis and the medical problems and physical findings that can be seen with the disorder. 3. Discuss what is normal for the heart rate of a fetus and the types of abnormal cardiac rhythms that may occur in the presence of a cardiac tumor. 4. Describe the ultrasound findings of fetal cardiac tumors and what to watch for sonographically as a pregnancy progresses once this diagnosis is made. Introduction: Tumors of the fetal heart are uncommon findings that may be identified with obstetrical ultrasound. The most common tumor is the rhabdomyoma. Other possible fetal cardiac tumors include the teratoma, fibroma, lipoma, hemangioma, osteoma, and myxoma. These tumors can be seen as an isolated growth or as multiple solid masses arising from the fetal myocardium. Cardiac tumors in general are not malignant, but they can lead to problems as a pregnancy progresses and can also be an indicator of other underlying genetic abnormalities. The majority of rhabdomyomas occur with a genetic disorder called tuberous sclerosis, which will be discussed in more detail after the case report. Case Report: A 29-year-old white primigravid female was referred as a transfer of prenatal care at about 27 weeks gestation because of an abnormal finding seen on a routine fetal ultrasound examination. Her obstetrical history was unremarkable with no other complications noted in the pregnancy. There was no family history of birth anomalies and specifically no congenital heart defects were reported. In addition, there was no history of seizure disorders or other genetic abnormalities. The father of the fetus did have a cousin with mental retardation, but the underlying cause was unknown. Sonographic examination at the referral center revealed a live singleton female fetus in vertex presentation with normal fetal growth parameters for the expected gestational age with no abnormalities seen within the placenta and a normal amniotic fluid volume. The fetus was shown to have a “mass” in the ventricular septum of the fetal heart, which measured 1.3 cm in size (figure 1). No fetal tachycardia, arrhythmia or hydrops was identified. In addition, no other fetal abnormalities were identified. Hydrops, by definition, is the collection of fluid in more than one body compartment. The main body compartments are the abdomen (ascites), the chest cavity (pleural effusions), the pericardial sac (pericardial effusion), and the skin (skin edema). Genetic consultation and weekly biophysical profile testing was recommended. The genetic consultant recommended a follow-up fetal ultrasound evaluation with echocardiography. The fetal echocardiography revealed multiple echogenic areas within the walls of the ventricles of the fetal heart with a predominant density in the interventricular septum. The smaller echogenic areas were seen in the lateral right ventricular free wall, in the capillary muscles of both the right and left ventricles, and an isolated density in the apex of the left ventricle (figure 2). Doppler evaluation with color flow imaging revealed normal tricuspid valve and mitral valve inflow, as well as, normal pulmonary artery and ascending aortic artery outflow. Ductal flow was within normal limits. Atrial septal flow was also within normal limits. The overall impression of the fetal echocardiogram was multiple fetal rhabdomyomas with a predominant mass in the interventricular septum. Again, no hydrops was evident. These findings were discussed with the family and a recommendation for ongoing follow-up was made. Weekly biophysical profiles and periodic sonograms to assess fetal growth and to check for the development of arrhythmias and signs of cardiac failure were performed throughout the remainder of the pregnancy. Starting at approximately 31 weeks gestation, an intermittent irregular-irregular arrhythmia was noted, consistent with premature ventricular contractions (PVC’s), and this continued throughout the remainder of the pregnancy. No evidence of fetal hydrops ever developed and fetal growth continued to be normal. The patient was delivered at 39 weeks gestation by elective cesarean section under epidural anesthesia due to a cervix that was fully closed and difficulty in interpreting the fetal heart rate pattern because of the arrhythmia. Discussion: Cardiac rhabdomyomas occur in about 1 in 20,000 births with an equal distribution between males and females. They are benign growths derived from the striated cardiac muscle. These cardiac rhabdomyomas are highly associated with a medical disorder called tuberous sclerosis (which means potato-like sclerotic lesions). Tuberous sclerosis is a genetic disorder that is autosomal dominant. However, 86% of the cases are “new mutations” meaning that the parents do not carry the gene and will have no family history. However, if an individual with tuberous sclerosis has a child, there will be a 50% chance of passing it on to their offspring because it is a “dominant” genetic disorder. Tuberous sclerosis is associated with a large number of other possible abnormalities. The hallmark of tuberous sclerosis is the development of hamartomas, which are benign overgrowths of cells that normally occur in the organ, but because the growth is more than it should be, nodules or tumors develop. The most common sites for these hamartomas are in the brain, kidneys, and skin; however, they can occur in almost any organ. When they develop in the brain, it usually leads to seizures with an abnormal EEG in 90% of cases and mental retardation in 60% of cases. If they are present in the kidney, renal function is still usually normal unless there is extensive destruction. Regarding the skin, besides the development of skin nodules, patients may have white nevi (moles) and can also have characteristic areas of lack of pigment or white skin patches (called “ash leaf” spots). The worst prognosis for tuberous sclerosis is when there is central nervous system (CNS) involvement because of the potential for seizures and the high rate of mental retardation. Unfortunately, the CNS abnormalities may be subtle and therefore not detectable by prenatal ultrasound. One recent study has suggested using magnetic resonance imaging in this situation and reported a high rate of successful detection. However, it is important to understand that hamartomas in patients with tuberous sclerosis can develop at any time and therefore, a negative prenatal / neonatal evaluation of the central nervous system does not guarantee that hamartomas won’t develop in the future. Over 50% of fetuses with tuberous sclerosis will have cardiac rhabdomyomas; however, most cardiac rhabdomyomas will regress with age. Although rhabdomyomas are not malignant, their presence can lead to problems as a pregnancy progresses, especially if the tumors continue to grow in size. Therefore, the pregnancy should be followed by serial ultrasound evaluations. These tumors (or any cardiac tumor) may produce a fetal cardiac arrhythmia because they can affect the immature conduction system of the fetal heart. Explanation of the abnormalities that may occur in the fetal cardiac conduction system requires a review of what is “normal” for the heart rate of a fetus. The normal heart rate of a fetus (after the first trimester) is between 110 and 160 beats per minute (bpm) and should be regular. The fetal heart rate is usually faster in the earlier stages of pregnancy (most often between 140 and 160 bpm) and then may decrease somewhat near term. A sustained fetal heart rate between 160 and 180 bpm is considered a mild tachycardia and may have several causes, the most common of which is maternal fever. Other causes may include a normal variation for that fetus, certain drugs consumed by the mother, fetal infection, fetal anemia, fetal hypoxia, and maternal hyperthyroidism. It is important to note that when a fetus is active, the heart rate will increase for a period of time. Using fetal monitoring, these short increases in fetal heart rate seen with fetal activity are called “accelerations” (which are indirect signs that the fetus is well oxygenated). Therefore, if a fetal heart rate between 160 and 180 bpm is detected by m-mode ultrasound in association with fetal activity, this most likely is suggestive of an “acceleration” (which is normal). A true mild fetal tachycardia (due to one of the causes listed above) is one that remains sustained in the absence of fetal movement and will last for the duration of the sonographic exam. A sustained fetal heart rate above 180 bpm is considered by most authorities to be a severe tachycardia and is usually abnormal (e.g. due to certain drugs the mother may have consumed, maternal fever, fetal infection, fetal anemia, fetal hypoxia, or a tachyarrhythmia). A supraventricular tachyarrhythmia in a fetus is a heart rate that is usually above 200 bpm. The most common fetal arrhythmias that may occur in relation to cardiac tumors include atrioventricular block (AV-block), supraventricular tachyarrhythmias (SVT), and premature ventricular contractions (PVC’s). Cardiac tumors can also lead to cardiac failure and the development of fetal hydrops (figures 3 and 4). The heart failure seen with fetal cardiac tumors is usually due to obstruction of cardiac outflow because of the size of the tumor or it develops in the presence of an SVT or an AV-block. One of the first signs of cardiac failure is the development of a pericardial effusion. As cardiac failure progresses, hydrops will develop. The outcome in these hydropic cases depends somewhat on the etiology. If the hydrops is due to cardiac obstruction, the only way to potentially reverse the failure is by surgery (to relieve the obstruction). The outcome in these cases is often poor because the hydropic fetus is not a good surgical candidate. If the hydrops is related to an arrhythmia, the outcome is better because the arrhythmia can often be treated with medications that can also reverse the cardiac failure. Fetal cardiac tumors should be distinguished from the “echogenic focus” that can be seen in either the right or left ventricle (figures 5 and 6). The “echogenic focus” is caused by a reflection off the papillary muscles within the ventricles and is a normal finding. The papillary muscles are connected to the tricuspid and mitral valves. Cardiac tumors are usually much larger and even though they are more echogenic than the normal cardiac muscle, they do not reach the level of echogenicity that is commonly seen with the “echogenic focus”. In addition, (though a single isolated tumor has been reported) cardiac tumors are more commonly multiple and most often found within the cardiac muscle of the interventricular septum or the base of the left ventricle. The “echogenic focus” usually appears to be floating within the right or left ventricular chamber and is not found within the cardiac muscle itself. (Although the “echogenic focus” is not a cardiac anomaly, more recently, it has been suggested as a possible marker for some chromosomal abnormalities). Case Follow-up: After delivery, an evaluation for tuberous sclerosis was initiated. An MRI of the infant’s brain, unfortunately, did identify multiple signal abnormalities consistent with subependymal and cortical growths that are commonly found with tuberous sclerosis. Renal sonography, however, was normal. The fetal arrhythmia did not continue after delivery and the baby was discharged at 8 days of age to her parents and follow-up with the pediatrician and neurologist was recommended. This fetus was found to have both tuberous sclerosis and multiple cardiac rhabdomyomas upon delivery. The mother and father were thoroughly evaluated by genetics and it was determined that they did not have the disorder. Therefore, the findings in this case are consistent with a new mutation. The family was counseled that the risk for this occurring in a future pregnancy was extremely minimal; however, if the child with tuberous sclerosis were to have children in the future, there would be a 50% chance of passing on this genetic disorder to her offspring. Figures: 1 This image shows the 1.3 cm rhabdomyoma that was identified in the interventricular septum of the fetal heart. Note that the tumor is more echogenic than the surrounding cardiac muscle itself. 2 This image depicts some of the smaller rhabdomyomas that were seen in the capillary muscles of both the right and left ventricles. 3 Transverse scan of the fetal abdomen in a case of supraventricular tachycardia revealing ascites (this fetus did not have tuberous sclerosis or cardiac tumors). Note the distinct outlines of the loops of small bowel (which are enhanced by the intraabdominal fluid. 4 A case of severe hydrops revealing large bilateral pleural effusions and thickened skin from edema. (This fetus had hydrops for reasons unrelated to cardiac function and did not have tuberous sclerosis – note the 4-chamber cardiac view.) 5 & 6 Examples of the “echogenic focus” that may be seen within the right or left ventricle of the fetal heart. References or Suggested Reading: 1. Hegge, F: Cardiac Rhabdomyoma. A Practical Guide to Ultrasound of Fetal Anomalies. Raven Press, New York 1992 p. 143. 2. Sanders, R, Blackmon L, Hogge W, Wulfsberg E: Structural Fetal Abnormalities The Total Picture. Mosby, St. Louis 1996 P. 57. 3. Smith DW: Recognizable Patterns of Human Malformation. W. B. Saunders, Philadelphia 1982 pp. 375-376. 4. Callen, PW: Ultrasonography in Obstetrics and Gynecology. W. B. Saunders, Philadelphia 1988 p. 209. 5. Bundy, S, Evans K: Tuberous Sclerosis: A genetic study. J. Neurology Neurosurgery Psychiatry. 1969 Vol 32. p. 591 6. Shenker L: Fetal cardiac arrhythmias. Obstetrics and Gynecology Survey. 1979 Vol. 34 p. 561 7. Geipel A, Krapp M, Germer U, at al. Prenatal diagnosis of cardiac tumors. Ultrasound Obstet Gynecol 2001;17:17-21. 8. Beghetti M, Gow RM, Haney I, et al. Pediatric primary benign cardiac tumors: a 15year review. 1997;134:1107-14. 9. Tollens T, Casselman F, Devlieger H, et al. Fetal Cardiac tamponade due to an intrapericardial teratoma. Ann Thorac Surg 1998;66:559-560. 10. Sonigo P, Elmaleh A, Fermont L, et al. Prenatal MRI diagnosis of fetal cerebral tuberous sclerosis. Pediatr Radiol 1996;26:1-4. 11. Tseng JJ, Chou MM, Lee YH, Ho ES. In utero diagnosis of cardiac hemangioma. Ultrasound Obstet Gynecol 1999;13:363-5. 12. Choi JM, Jaffe R, Maidman J, Baxi LV. Multiple cardiac rhabdomyomas detected in utero. Fetal Diagn Ther 2000;15:174-6. 13. Fung TY, Lau TK, Yam MC, To KF. Prenatal diagnosis of cardiac osteoma: a case report. Prenat Diagn 1998;18:1209-11. 14. Pratt JW, Cophen DM, Mutabagani KH, et al. Neonatal intrapericardial teratomas: clinical and surgical considerations. Cardiol Young 2000;10:27-31. About the Authors: Lona L. Cook is currently a staff sonographer for the Maternal-Fetal Medicine Group that is affiliated with the Department of Obstetrics and Gynecology at the University of Kansas – Wichita. She received her BSRT in 1988 and graduated from the St. Joseph School of Radiologic Technology, in Wichita, Kansas. She then obtained her RDMS in Obstetrics & Gynecology in 1992 and her RDMS in Abdomen in 1993. Dr. Scott Roberts is board certified in Obstetrics and Gynecology and is also board certified in Maternal-Fetal Medicine. He currently is the Director of the Maternal-Fetal Medicine Division in the Department of Obstetrics and Gynecology at the University of Kansas School of Medicine – Wichita. He has authored several articles in peer-review medical journals and has lectured on many different topics across the country. Examination: 1. Possible fetal cardiac tumors include all of the following except A. teratomas B. rhabdomyomas C. hemangiomas D. lymphomas E. myxomas 2. Which of the following statements is true? A. Fetal cardiac these tumors can be seen as one isolated growth or consist of many solid masses arising from the fetal myocardium. B. C. D. E. The most common fetal cardiac tumor is the teratoma. Cardiac tumors are benign and therefore do not lead to problems as a pregnancy progresses and therefore, further ultrasound evaluations are not indicated. Cardiac tumors are isolated and therefore are not an indicator of other underlying medical abnormalities. Cardiac tumors in general are malignant. 3. In the case report presented, A. The fetus was shown to have a “mass” in the ventricular septum of the fetal heart, which measured 1.8 cm in size. B. Fetal hydrops was eventually identified. C. The fetal echocardiography revealed multiple echogenic areas within the walls of the ventricles of the fetal heart with a predominant density in the interventricular septum. D. Doppler evaluation with color flow imaging revealed normal tricuspid valve flow, but abnormal mitral valve flow. E. Doppler evaluation with color flow imaging revealed normal pulmonary artery outflow, but abnormal ascending aortic artery outflow. 4. Cardiac rhabdomyomas occur in about A. 1 in 10,000 births with a greater distribution in males over females B. 1 in 20,000 births with an equal distribution between males and females C. 1 in 20,000 births with a greater distribution in females over males D. 1 in 10,000 births with a greater distribution in females over males E. 1 in 20,000 births with a greater distribution in males over females 5. Tuberous sclerosis is A. a genetic disorder that is autosomal recessive. B. a genetic disorder that is x-linked recessive, and therefore, more often seen in males. C. a genetic disorder that is autosomal dominant and is almost always passed from one of the parents. D. a genetic disorder that is autosomal dominant, however, the majority are “new mutations” meaning that the parents do not carry the gene. E. a genetic disorder that is autosomal recessive and is almost always passed from one of the parents. 6. If an individual with tuberous sclerosis has a child, there will be a _____ chance of passing it on to their offspring. A. 5% B. 25% C. 10% D. 75% E. 50% 7. The hallmark of tuberous sclerosis is the development of hamartomas, which are benign overgrowths of cells that normally occur in the organ but because the growth is more than it should be, nodules or tumors develop. The most common sites for these hamartomas are in the A. brain and kidneys B. liver and lung C. skin D. A & B above E. A & C above 8. In tuberous sclerosis, when hamartomas develop in the brain, it leads to mental retardation in _____ of cases. A. 10% B. 20% C. 60% D. 40% E. 30% 9. Regarding the skin in tuberous sclerosis, besides the development of skin nodules, patients may have white moles and can also have characteristic areas of lack of pigment or white skin patches called A. “tuberous” spots B. “ash leaf” spots C. “paper” spots D. “sclerosis” spots E. “apigmentosa” spots 10. The worst prognosis for tuberous sclerosis is when there is ______ involvement. A. central nervous system B. renal C. cardiac D. skin E. pulmonary 11. Regarding central nervous system (CNS) involvement in tuberous sclerosis, which of the following statements is true? A. The CNS abnormalities, if present, are significant and are nearly always detectable by prenatal ultrasound. B. In evaluating the CNS, one recent study suggested using prenatal computed tomography to evaluate for subtle abnormalities, and reported a high rate of successful detection. C. Hamartomas in patients with tuberous sclerosis can develop at any time and therefore, a negative prenatal / neonatal evaluation of the central nervous system does not guarantee that problems won’t develop in the future. D. If hamartomas are detected in the kidneys, this means they are also present in the brain, so further evaluation is not necessary until after delivery. E. Prenatal diagnosis of the CNS is important, because if hamartomas are not present prenatally, then they will not develop at a later time. 12. Over _____ of fetuses with tuberous sclerosis will have cardiac rhabdomyomas. A. B. C. D. E. 5% 10% 25% 35% 50% 13. Which of the following statements is (are) true? A. Most cardiac rhabdomyomas will regress with age. B. Because rhabdomyomas are usually malignant, one should evaluate the patient for potential metastasis. C. Most cardiac rhabdomyomas will continue to grow after birth leading to future cardiac difficulties. D. A & B above are true. E. B & C above are true. 14. The normal heart rate of a fetus (after the first trimester) is between ______ beats per minute (bpm). A. 70 and 90 B. 90 and 110 C. 160 and 180 D. 110 and 160 E. 180 and 200 15. The most common cause for a mild fetal tachycardia (a sustained fetal heart rate between 160 and 180) is A. a fetal infection. B. a fetal anemia. C. maternal hyperthyroidism. D. fetal hypoxia. E. a maternal fever. 16. A fetal heart rate increase for a period of time when a fetus is active, is indicative of A. fetal hypoxia B. fetal anemia C. an acceleration D. maternal drug usage E. maternal hyperthyroidism 17. A supraventricular tachyarrhythmia in a fetus is a heart rate that is usually above A. 100 bpm B. 160 bpm C. 180 bpm D. 200 bpm E. 120 bpm 18. Because fetal cardiac tumors can lead to problems as a pregnancy progresses, serial ultrasound evaluations should occur to watch for the possible development of fetal hydrops. If hydrops occurs, it is most often caused by A. B. C. D. E. obstruction of the venous inflow to the heart a supraventricular tachyarrhythmia (SVT) tumor destruction of the cardiac muscle with failure A & B above B & C above 19. Fetal cardiac tumors should be distinguished from A. the echogenic focus that can be seen in either the right or left ventricle. B. idiopathic hypertrophic subaortic stenosis C. anomalous pulmonary venous return D. an endocardial cushion defect E. the moderator band of the right ventricle 20. By ultrasound, fetal cardiac tumors A. are usually small and more echolucent than the normal cardiac muscle. B. do not reach the level of echogenicity that is commonly seen with the “echogenic focus”. C. are usually single growths and are isolated to the surface of the cardiac muscle. D. A & B above. E. B & C above.