Supplementary Informations (doc 7286K)
advertisement
")
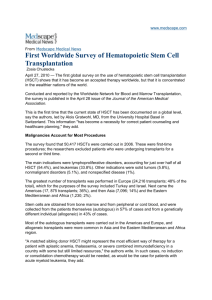
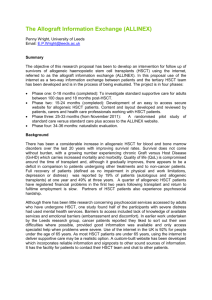
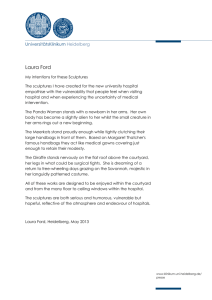
Online-only supplements Contents eMethods Page 2 eResults Page 3 eFigure 1a Page 4 eFigure 1b Page 5 eFigure 1c Page 6 eFigure 1d Page 7 eFigure 2a Page 8 eFigure 2b Page 9 eTable 1 Page 10 eTable 2 Page 11 eTable 3 Page 12 eAcknowledgements Page 13 eReferences Page 19 1 eMethods Study design All patients were assessed at diagnosis and, based on age, comorbidities and personal preference, defined as eligible or not for allogeneic hematopoietic stem cell transplantation (HSCT) with a related donor. For patients who were not eligible for HSCT, only survival probabilities were described in this analysis. For all patients considered as eligible, HLA family typing was performed; its result was used as a genetic randomization 1 between HSCT (group A; with an HLA-identical family donor) and best available drug treatment (group B; without an HLA-identical family donor). With our concept of genetic randomization, the allocation ratio between group A and group B could not be determined in advance. It was presumed that about 30% of 600 eligible patients could be transplanted with a related donor. In actual fact, 39% of 427 were transplanted. It was planned to register 1,000 evaluable patients in total. Instead, 669 patients became part of the final analysis data set. With the availability of imatinib as first-line treatment, a further continuation of study IIIA was not feasible. In the original protocol, patients with allogeneic HSCT with an unrelated donor were denoted as “group 2”. If feasible, they were supposed to be analyzed together either with group A or as part of group B but in any case, it had been intended that survival time was not censored at time of allogeneic HSCT with an unrelated donor. However, even regarding only the patients transplanted in first chronic phase, the distribution of the European Group for Blood and Marrow Transplantation (EBMT) score2 was significantly different between the 144 patients of group A and the 131 patients in group B (P<.001). In particular, while 85% of the 144 patients of group A were transplanted in the first year, it were only 60% of the 131 patients of group B (P<.001). According to these differences in their structure, it was unlikely that the two groups would show a comparable survival outcome which would allow the groups to be pooled and to have an undifferentiated interpretation of the common results. On the other hand, we had also learnt from CML-study III3 that due to early transplant-related mortality, it was not reasonable to rate survival probabilities after HSCT with an unrelated donor as survival probabilities with best available drug therapy, in general. 3 For these reasons, we found it the most appropriate approach to proceed as in CML-study III: Affiliation to group A or group B was strictly according to the genetic randomization. Survival times of patients who received an unrelated donor HSCT were censored at the day of transplantation, if patients were still in first chronic phase. Patients undergoing transplantation in accelerated phase or blast crisis were not censored, since drug treatment had failed before. Patients Unlike in CML-study IV,4 the health care setting (university based, municipal hospital based, or 36 office based) had no statistical influence on any survival probabilities. Allogeneic HSCT Preparative regimens were classified according to the CIBMTR functional definitions. 5 Standard conditioning(n = 116 [77%]) included any regimen with (i) >500 cGy of total body irradiation (TBI) as a single fraction or >800 cGy if fractionated; (ii) >9 mg/kg busulfan oral (or intravenous equivalent); (iii) >140 mg/m2melphalan; (iv) >10 mg/kg thiotepa; or (v) BEAM regimen (carmustine, etoposide, cytarabine, and melphalan); all others were classified as reduced intensity conditioning (RIC; n=35 [23%])without further subdivision into nonmyeloablative.5 Graft-versus-host disease prophylaxis and supportive therapy were conducted according to the standard practice of the individual center and classified as T-cell depletion (in vivo and ex vivo combined; n=57 [38%]), cyclosporine based (n=93 [62%]) or other (n=1). Even though it was otherwise recorded at the time of the genetic randomization, in 14 of 151 cases (9%), the related donor was not HLA-matched (eTable 1). Of 137 transplantations with an HLA-match, in 135 cases the donor was a sibling and in 2 cases a son. Further aspects of statistical analysis In line with the established ICH guidelines,6 the significance level α was chosen to be .05 two-sided in all cases. In case only few patients (less than six) were still under observation, 10-year survival probabilities were not given. In addition, we abstained from reporting the 10-year confidence intervals in some Figures in favor of the legibility of the legends. A particular focus was put on 10 years because this is the minimum time, every living patient could have been observed. Impact of events at times before 10 years might therefore be underestimated. To compute adapted EBMT scores for all 427 patients eligible for HSCT, the following algorithm was applied: Age at diagnosis was used. In accordance with the inclusion criteria, all patients were in chronic phase and supposed to be transplanted within one year from diagnosis. Of the 151 patients actually transplanted with a related donor, 8 males (5%) had a mismatched female donor and 29 males (19%) a matched female donor. Regarding the cases where either the recipient was not male or the donor not female, HSCT was unmatched in 6 2 (4%) and matched in 108 patients (72%). Taking the probabilities of these four possible combinations into account, a random outcome for the two variables was drawn for all 276 patients of CML- study IIIA who had not received an HSCT with a related donor, whereas the real data was used for the 151 transplanted patients. This random drawing was repeated 999 times. Survival probabilities between (prognostic) subgroups were compared in all resulting samples. Decision on significance was then made in dependence on the median P value of all 999 results. To be able to describe survival probabilities by the Kaplan-Meier method if they were dependent on the adapted EBMT score (Figure 3a, eFigures 2a and 2b), one out of the 999 samples had to be selected. It was decided to use the sample providing the median P value (log-rank test: P=.047) for the most relevant comparison of the survival probabilities between patients of group A with adapted EBMT scores 0-1 (10-year survival probability: 0.85 [95% CI: 0.74-0.92] and the 230 non-high-risk Euro score7 patients of group B (10-year survival probability: 0.73 [95% CI: 0.65-0.80]. The sample providing the median P value P=.047 was sample no. 813. Even though in all following cases the reported median P value came from other samples, sample no. 813 was also representative with regard to the significance (yes or no) of all other median results. eResults Treatment with tyrosine kinase inhibitors Of the 183 patients who received tyrosine kinase inhibitor (TKI) treatment, 181 started with imatinib, 1 with nilotinib and 1 with dasatinib. The median time between diagnosis and initiation of TKI therapy was 1.8 years (range, 0.1 to 12.2 years). When TKI treatment was initiated, patients were in quite different stages of disease and treatment history: Twenty of the 183 patients (11%) had experienced blast crisis before starting TKI treatment and 41 (22% of 183) had received an allogeneic HSCT before. Median duration of TKI treatment was 6.4 years (range, 18 days to 13.3 years). Starting from the day of first TKI treatment, ten-year overall survival probability for the 183 patients was 74% [95% confidence interval: 0.66-0.80]. Of the 44 patients randomized to autologous SCT, 25 patients were actually transplanted. Six patients remained TKI naïve and 19 received imatinib thereafter. Of these 19 patients, 2 received dasatinib and 1 nilotinib as a second TKI. 3 eFigure 1a: Kaplan-Meier estimates of overall survival of all 669 evaluable patients Patients at risk at different years of observation Year 0 1 2 3 5 7 8 10 12 14 Eligible for allogeneic HSCT 427 408 350 332 311 302 295 282 157 26 Not eligible for allogeneic HSCT 242 233 218 200 162 139 129 112 47 12 Patients were stratified according to eligibility for allogeneic hematopoietic stem cell transplantation (HSCT) at diagnosis. At 1, 5, and 10 years, horizontal crossbars indicate the upper and lower limits of the 95% confidence intervals for the estimated survival probabilities. The abbreviation “s.p.” stands for “survival probability”. 4 eFigure 1b: Kaplan-Meier estimates of overall survival of the 261 patients randomized to best available drug treatment (group B) Patients at risk at different years of observation Year 0 1 2 3 5 7 8 10 12 14 Unknown risk 31 26 21 18 16 15 15 15 9 1 Low risk 129 87 56 52 45 43 41 39 18 5 Intermediate risk 70 47 36 34 32 27 26 25 18 2 High risk 31 20 13 11 7 6 6 6 1 1 Patients were stratified according to disease risk (Euro score) at diagnosis. In group B, the survival time of patients receiving an allogeneic HSCT with an unrelated donor was censored at the day of transplant. The survival differences between the non-high-risk and the high-risk patients were significant (log-rank test: P=.002). At 1, 5, and 10 years, horizontal crossbars indicate the upper and lower limits of the 95% confidence intervals for the estimated survival probabilities. The abbreviation “s.p.” stands for “survival probability”. 5 eFigure 1c: Kaplan-Meier estimates of post-transplant overall survival of 151 patients in group A Patients at risk at different years of observation Year 0 1 2 3 5 7 8 10 12 14 Scores 0-1 54 51 50 49 48 48 48 42 12 1 Score 2 61 51 49 48 47 47 47 39 21 2 Scores 3-4 31 20 20 20 20 20 20 13 7 1 Scores 5-7 5 2 2 2 2 2 2 0 0 0 Of 166 patients, 151 actually received allogeneic hematopoietic stem cell transplantation (HSCT) and were stratified according to the European Group for Blood and Marrow Transplantation (EBMT) risk at time of transplant. The survival differences between the 4 curves were significant (log-rank test: overall P=.002). At 1 and 5 years, horizontal crossbars indicate the upper and lower limits of the 95% confidence intervals for the estimated post-transplant survival probabilities. The abbreviation “s.p.” stands for “survival probability”. 6 eFigure 1d: Kaplan-Meier estimates of post-transplant overall survival of 305 patients with allogeneic hematopoietic stem cell transplantation (HSCT) Patients at risk at different years of observation Year 0 1 2 3 5 7 8 10 12 14 Score 0 3 3 3 3 3 3 3 3 2 0 Score 1 55 51 50 49 48 48 48 41 12 1 Score 2 98 81 78 77 75 74 74 64 33 2 Score 3 81 54 49 48 47 47 46 36 18 2 Score 4 45 29 28 27 25 25 23 16 3 0 Score 5 14 8 5 5 4 3 3 1 0 0 Score 6 6 3 1 0 0 0 0 0 0 0 Score 7 3 0 0 0 0 0 0 0 0 0 All 305 patients actually transplanted were stratified according to the European Group for Blood and Marrow Transplantation (EBMT) risk score at time of transplant. At 1 and 5 years, horizontal crossbars indicate the upper and lower limits of the 95% confidence intervals for the estimated post-transplant survival probabilities. The abbreviation “s.p.” stands for “survival probability. 7 eFigure 2a: Kaplan-Meier estimates of overall survival of the 166 patients in group A Patients at risk at different years of observation Year 0 1 2 3 5 7 8 10 12 14 Score 0-1 68 66 61 60 58 58 58 55 25 2 Score 2 76 72 62 59 57 57 56 52 30 9 Score 3-4 22 19 16 15 15 15 15 15 8 1 Patients randomized to allogeneic hematopoietic stem cell transplantation (HSCT) were stratified according to the adapted European Group for Blood and Marrow Transplantation (EBMT) risk score at diagnosis. At 1, 5, and 10 years, horizontal crossbars indicate the upper and lower limits of the 95% confidence intervals for the estimated survival probabilities. The abbreviation “s.p.” stands for “survival probability”. 8 eFigure 2b: Kaplan-Meier estimates of overall survival of the 261 patients in group B Patients at risk at different years of observation Year 0 1 2 3 5 7 8 10 12 14 Score 0-1 86 55 32 25 24 23 22 21 12 3 Score 2 124 80 61 58 46 40 38 38 21 3 Score 3-4 51 45 33 32 30 28 28 26 13 3 Patients randomized to best available drug treatment were stratified according to the adapted European Group for Blood and Marrow Transplantation (EBMT) risk score at diagnosis. In group B, the survival time of patients receiving an allogeneic HSCT with an unrelated donor was censored at the day of transplant. At 1, 5, and 10 years, horizontal crossbars indicate the upper and lower limits of the 95% confidence intervals for the estimated survival probabilities. The abbreviation “s.p.” stands for “survival probability”. 9 10 eTable 1. Characteristics of patients with hematopoietic stem cell transplantation by allocation and phase of disease Group A In CPa 144 Not in CP 7 Total 151 Group B In CP 131 Not in CP 17 Total 148 Not eligible In CP 3 Not in CP 3 Total 6 305 Median Range EBMT-Scorea: Median Range 37 16–58 2 0–5 42 33–55 5 2–7 37 16–58 2 0–7 37 13–58 3 1–5 38 19–64 5 3–6 38 13–64 3 1–6 51, 54, 59 48, 53, 56 4, 4, naa 4, 5, na 54 48–59 4 4–5 37 13–64 2 0–7 n with standard conditioning (%) 111 77 5 71 116 77 105 80 10 59 115 78 2 67 2 67 4 67 235 77 n with GvHDa prophylaxis TCDa 55 2 57 90 10 100 2 1 3 160 (%) n with GvHD prophylaxis cyclosporine based (%) n with GvHD prophylaxis other (%) 38 29 38 69 59 68 67 33 50 52 88 5 93 41 7 48 0 1 1 142 62 1 0 71 0 62 1 0 31 0 41 0 32 0 1 33 33 1 33 17 2 33 47 3 1 n with source: Bone marrow 62 2 64 73 7 80 0 0 0 144 (%) n with matched, related donor 43 29 42 56 41 54 133 4 137 (%) 92 57 91 Number at entry Age: n with no matched, related donor (%) n with unrelated donor (%) a 11 8 0 3 43 0 14 9 0 0 0 0 Total 47 0 b b 0 0 0 0 131 100 16 94 147 99 2 67 1 1 138 33 17 45 0 0 2 67 4 67 14 5 151 50 CP: Chronic phase, EBMT-Score: European Bone Marrow Transplantation-Score, na: not available, TCD: T-cell depletion, GvHD: Graft versus host disease. Missing value for 1 patient transplanted with a related donor. b 11 eTable 2. Causes of death by treatment allocation and treatment received for 296 patients eligible for allogeneic HSCTa and not transplanted with an unrelated donor in first CPa Number at entry Group A With HSCT In CP Not in CP 144 b Without HSCT Total Group B With HSCT Not in CP Without HSCT Total Total 7 15 166 17 113 130 296 4/7 4/15 40/166 13/17 34/113 47/130 87/296 n dead 32/144 (%) n with cause of death due to disease (%) n with cause of death transplantrelated (%) n with cause of death unrelated to transplant/disease (%) 22 57 27 24 76 30 36 29 5/32 3/4 3/4 11/40 6/13 22/34 28/47 39/87 16 75 75 28 46 64 60 45 24/32 1/4 0/4 25/40 5/13 3/34 8/47 33/87 75 25 63 38 9 17 38 3/32 0/4 1/4 4/40 2/13 9/34 11/47 15/87 9 0 25 10 15 26 23 17 a HSCT: Hematopoietic stem cell transplantation, CP: Chronic phase. b 32/144 reads: n=32 of 144 dead. The corresponding interpretation holds for cells with an analog display of results. 12 eTable 3. Randomization and treatment received for 296 patients eligible for allogeneic HSCTa and not transplanted with an unrelated donor in first CPa Group A With HSCT Without HSCT Total At 10 years At 10 years 11 alive 122 alive Group B With HSCT in advanced phase After HSCT Before HSCT at 10 years 17 4 alive Total Without HSCT Total At 10 years At 10 years At 10 years 82 alive 86 alive 208b alive Number at entry Before HSCT 151 After HSCT at 10 years 111 alive n with interferon-alpha 33/151c 0/106 0/11 0/117 4/17 0/4 3/80 3/84 4/201d (%) n with tyrosine kinase inhibitor (%) n with intensive chemotherapy (%) 22 0 0 7 24 0 4 5 2 11/151 19/106 10/11 29/117 11/17 0/4 74/80 74/84 103/201d 7 18 91 25 65 0 93 88 51 1/151 0/106 0/11 0/117 3/17 0/4 0/80 0/84 0/201d 1 0 0 0 18 0 0 0 21/86 23/208 19 7 n with autologous HSCT (%) 0 0 0 0 2/17 0/4 12 0 0 e 21/82 19 e a HSCT: Hematopoietic stem cell transplantation, CP: chronic phase. Of 296 patients eligible for allogeneic HSCT, 208 patients were observed for at least 10.0 years, 5 additional patients were alive but observed for < 10 years. c 33/151 reads: n=33 of 151 received interferon-alpha. The corresponding interpretation holds for cells with an analog display of results. d Data was available for 201 of 208 patients. e Regarding autologous HSCT, the number of patients who had a transplantation any time within the 10 years was reported. b 13 14 eAcknowledgements List of the 33 transplantation centers No. of transplanted patients 56 52 40 20 17 15 13 12 11 10 10 9 8 8 7 7 7 7 6 5 4 4 3 3 2 2 2 2 2 1 1 1 1 Transplantation center Universitätsklinikum Hamburg-Eppendorf Klinikum der Universität München-Großhadern Universitätsklinikum Essen Dt. Klinik für Diagnostik Wiesbaden Universitätsklinikum Ulm University Hospital Brno Klinikum der Universität Jena Medizinische Hochschule Hannover Universitätsklinikum Düsseldorf Universitätsklinikum Freiburg Klinikum Nürnberg Nord Universitätsspital Basel Klinik für Knochenmarktransplantation Idar-Oberstein Universitätsklinikum Tübingen Charité Berlin Uniklinikum Dresden Ruprechts-Karl-Universität Heidelberg Universität zu Köln Universitätsklinikum des Saarlandes Homburg Hôpital Universitaire de Genève Universitätsklinikum Mainz Universitätsklinikum Regensburg Universität Nürnberg-Erlangen University Hospital Pilsen Klinikum Augsburg Medical University of Gdansk Universitätsklinikum Frankfurt Klinikum Minden Universitätsklinikum Münster Franziskushospital Bielefeld Universitätsklinikum Bonn St. Johannes Klinikum Duisburg Medizinische Universität Kattowice 15 List of all 143 centers participating in the study Center No. 011 034 Institution Universitätsklinikum HamburgEppendorf Klinikum Schwabing, Städtisches Klinikum München GmbH Universität zu Köln No. of recruited patients 41 Key contact persons A. Zander, Nicolaus Kröger 32 Ch. Nerl 29 C. Scheid 27 W. Hiddemann, K. Spiekermann, H.-J. Kolb 160 Klinikum der Universität München Campus Großhadern University Hospital Brno 27 J. Mayer 020 UM Mannheim 24 088 MVZ des Klinikums Nürnberg 24 R. Hehlmann, U. Berger, A. Hochhaus, S. Saussele, M. Müller, A. Reiter C. Falge 136 Universitätsklinikum Jena 23 H. - G. Sayer, A. Hochhaus 027 Universitätsklinikum Ulm 20 H. Heimpel† , D. Bunjes, H. Döhner 109 Med. Hochschule Hannover 17 A. Ganser 072 Allg. Krankenhaus St. Georg Hamburg 16 R. Kuse, S. Müller-Hagen, S. Lüb, N. Schmitz 094 Universitätsklinikum Düsseldorf 15 A. Wehmeier 019 Städt. Kliniken Karlsruhe 14 U. Stappert-Jahn, J. Fischer 179 Universitätsklinikum Heidelberg 14 A. Ho, J. Dengler 028 Universitätsklinikum Würzburg 13 H. Einsele, E. Goebeler, M. Wilhelm 081 Universitätsklinikum Essen 13 D. - W. Beelen 060 St.-Marien-Hospital Hagen 13 H. Lindemann, H. Eimermacher 065 Klinikum Bremen Mitte 12 M . Bormann, B. Hertenstein 168 Universitätsklinikum Bonn 12 T. Sauerbruch, I. Schmidt-Wolf 032 Zentralklinikum Augsburg 11 G. Schlimok, H. Hempel 045 Inselspital Bern 11 A. Tobler, B. Lämmle, G. Baerlocher 003 Universitätsklinikum Bonn 9 H. Vetter 006 St. Johanneshospital Duisburg 9 C. Aul 079 Universitätsklinik Homburg 9 M. Pfreundschuh 106 Klinikum Stuttgart 9 S. Lischke 002 054 Universitätsspital Basel St. Antonius Hospital Eschweiler 8 8 A. Gratwohl, A. Tichelli, J. Passweg, D. Heim P.Staib 086 Universitätsklinikum Regensburg 8 M. Edinger 156 St. Vincentiuskliniken Karlsruhe 8 G. Metzger, M. Schatz 118 Universitätsklinikum Mainz 7 K. Kolbe, C.Huber, Th. Kindler 126 Universitätsmedizin Göttingen 7 L. Trümper, Gerald Wulf 181 Universtitätsklinikum Essen 7 J. Novotny 183 Division d'hematology Lausanne 7 A. Rosselet 145 Medical University of Gdansk 6 A. Hellmann, W. Prejzner 165 Onkologische Schwerpunktpraxis Bielefeld Klinikum Kempten- Oberallgäu 6 M. Just, E. Schäfer 5 O. Prümmer, J. Gatter 018 021 016 16 Center No. Institution No. of recruited patients 5 Key contact persons 056 Krkh. Barmherzige Brüder Regensburg 077 Universitätsklinikum Münster 5 M. Stelljes, J. Kienast† 120 Diakonieklinikum Stuttgart 5 K. Zutavern-Bechtold 144 5 S. Custodis, G. Jacobs 173 Schwerpunktpraxis Hämatologie Saarbrücken St. Marienhospital Hamm 5 B. Soddemann-Lohmann, M. Hemeier 033 Onkolog. Schwerpunktpraxis Berlin 4 A. Koschuth 044 Vivantes Klinikum Berlin-Neukölln 4 M. de Witt 047 Westpfalzklinikum Kaiserslautern 4 H. Link 087 4 S. Kremers 103 GP für Hämatologie und Onkologie Lebach Universitätsklinikum Erlangen 4 M. Gramatzki, S. Krause 115 Johannes Wesling Klinikum Minden 4 M. Griesshammer 139 Klinikum-Hannover Siloah 4 H. Kirscher 154 Klinikum Stuttgart 4 J. Schleicher, M. Fabian 155 Franziskushospital Bielefeld 4 H.-J. Weh 161 St. Hedwigkrankenhaus Berlin 4 H.-J .Englisch, B. Oldenkott 170 Krankenhaus Düren 4 F. Henneke 180 4 Ch. Maintz 186 Hämatologisch-onkologische Praxis Würselen Laubenstein und Rendenbach GP Trier 4 H.-P. Laubenstein, B. Rendenbach 010 Zentrum für Innere Medizin Gießen 3 H. Pralle 026 Kantonsspital St. Gallen 3 U. Hess 101 3 A. Neumann 150 Krankenhaus Nord-West Frankfurt/Main Klinikum Ludwigshafen 3 M. Uppenkamp 158 Dt. Klinik für Diagnostik Wiesbaden 3 R. Schwerdtfeger, H. Baurmann 162 Marienhospital Bottropp 3 E. Musch 190 Klinik St. Antonius Wuppertal 3 M. Sandmann 208 Praxis für Innere Medizin München 3 C. Scheidegger 213 Kreisklinikum Siegen 3 S. Schanz 220 Klinikum Garmisch-Patenkirchen 3 L. Schulz 221 Kantonsspital Luzern 3 M. Gregor 008 2 B. Wassmann 2 R. Hartenstein 046 Klinikum der J. -W. Goethe Universität Frankfurt Städt. Klinikum München-Harlaching GmbH KKH Waldbröl 2 L. Labedzki 048 Klinikum Nürnberg 2 C. Falge, W. Brockhaus 049 Städt. Kliniken Oldenburg 2 C. Schweiger 067 Klinikum Herford 2 U.Schmitz-Huebner 070 Uniklinikum Dresden 2 J. Mohm, G. Ehninger 071 Onkologische Schwerpunktpraxis Lüneburg 2 B. Goldmann 036 M. Schenk 17 Center No. Institution No. of recruited patients 2 Key contact persons 102 Onkologische Praxis Oldenburg 107 Allgemeines Krankenhaus Hagen 2 T. Scholten 113 Charite-Campus Virchow Berlin 2 H. Oettle und C. Busemann 122 Gemeinschaftspraxis Onkologie Karlsruhe Praxis für Innere Medizin Dresden 2 F. Mosthaf, M. Procaccianti 2 H. Wolf 2 A. Fauser 143 Klinik für KM-Transplantation IdarOberstein Lukas Krankenhaus Bünde 2 D. Brunswig 151 Klinikum St. Marien Amberg 2 L. Fischer v. Weikersthal 157 2 S. Hahnfeld 159 Gemeinschaftspraxis Innere Medizin Jena Städt. Krkh. Dresden-Neustadt 2 R. Huhn 164 Schwerpunktpraxis Mannheim 2 W. Queisser 176 2 A. Neubauer, A. Burchert 193 Klinikum der Philipps-Universität Marburg Medizinische Klinik Recklinghausen 2 C. - P. Sodomann 195 Institut Central Hopitaux Sion 2 M. Stadler 198 2 H. Slavik 2 A. Lollert, M. Neise 200 Onkologische Schwerpunktpraxis Augsburg Schwerpunktpraxis Hämatologie/ Onkologie Krefeld Hämatologische Praxis Stuttgart 2 H. Fiechtner 201 Helios Klinkum Wuppertal 2 A. Raghavachar 202 Klinikum Krefeld 2 M. Planker 204 2 S. Schmitz 2 W. Brugger 219 Praxis für Hämatologie u. Onkololgie Köln Schwarzwald Baar Klinikum Villingen-Schwenningen Kliniken Essen Süd 2 W. Heit 227 Ärzteforum Seestrasse Berlin 2 F. Strohbach 242 2 O. Brudler 005 Praxis für Hämatologie/Internistische Onkologie Augsburg St. Joseph-Hospital Bremerhaven 1 H.-H. Heidtmann 012 Hämatolog.-onkol. Praxis Hamburg 1 U. R. Kleeberg 017 UKSH Campus Kiel 1 N. Schmitz, H. Löffler† 022 Klinikum Innenstadt München 1 I. Langenmayer 024 Helios Klinkum Bad Saarow 1 W. Schulze 030 1 H. Tesch, F. Walther 038 Onkologische Gemeinschaftspraxis Frankfurt St. Willehad-Hospital Wilhelmshaven 1 W. Augener 042 Krankenhaus München-Neuperlach 1 M. Garbrecht 055 Klinikum rechts der Isar München 1 F. Schneller 059 Dr.-Horst-Schmidt-Kliniken Wiesbaden 1 N. Frickhofen, H.-G. Fuhr 130 134 199 214 B. Otremba 18 Center No. Institution No. of recruited patients 1 Key contact persons 063 Diakonieklinikum Schwäbisch Hall 069 Onkologische Praxis Basel 1 W. Weber 074 Internistische GP Hamburg 1 A. Mohr 078 Marienkrankenhaus Ludwigshafen 1 H. Weiss 083 Jakobi-Krankenhaus Rheine 1 J. Bauer 085 Caritas Klinik Saarbrücken 1 J. Preiss 104 Praxis für Hämatologie Wuppertal 1 W. Fett 105 Praxis für Hämatol./Onkol. Lübeck 1 C. Engelmann 127 Med. Klinik St. Franziskus Mönchengladbach Innere Medizin FMH Breitenbach 1 D. Kohl 1 R. Haberthür Klinikum Mutterhaus der BorromäerinnenTrier Malteser Krankenhaus Flensburg 1 M. Clemens 1 J. - G. Saal 1 H.R. Milstrey 172 St. Irmgardis Krankenhaus ViersenSüchteln Ev. Diakoniekrankenhaus Freiburg 1 H. Arnold 175 Hämatologische Praxis Weiden 1 J. Weiß 177 Facharzt FMH für Innere Medizin Baar, Schweiz Praxisgemeinschaft Tübingen 1 M. Mannhart-Harms 1 S. H. Jacki 1 M. Sandmann 1 S. Müller 194 Kliniken St. Antonius, Petrus Krankenhaus Wuppertal Hämato-Onkol. Gemeinschaftspraxis Ansbach Städtisches Klinikum Braunschweig 1 B. Wörmann 203 Klinik Hirslanden Zürich 1 A. v. Rohr 205 Dr.-Herbert-Nieper-Krankenhaus Goslar Vinzentius Krankenhaus Landau 1 A. Hoyer 1 M. Schröder Gemeinschaftspraxis für Hämatologie/Onkologie Nürnberg Hopitaux Universitaire Geneve 1 M. Sauer 1 C. Helg 1 K. Quabeck, M. Schaefers 216 Hämato-Onkologische Gemeinschaftspraxis Duisburg Praxisnetzwerk Troisdorf 1 H. Forstbauer 218 OncoPro GbR Regensburg 1 R. Dengler 222 KKH Leer 1 G. Köchling 223 1 S. Fetscher 224 Klinik f. Hämatologie/Onkologie Lübeck Klinikum Deggendorf 1 G. Waska 225 Praxis Dr. T. Kamp Wendlingen 1 T. Kamp 226 Praxis Dr. A. Lindemann Ettlingen 1 A. Lindemann 228 Evangelisches Krankenhaus Oberhausen 1 M. Huzenlaub 133 148 166 171 185 191 192 207 209 210 211 H. H. Heißmeyer 19 Center No. Institution No. of recruited patients 1 Key contact persons 229 Onkologie Rastatt 230 Detken Gemeinschaftspraxis Northeim 1 S. Detken 232 Praxis für Hämatologie und Onkologie Freiburg Stauch Onkologische Schwerpunktpraxis Kronach Caritas Krankenhaus Bad Mergentheim 1 N. Marschner, M Zaiss, D. Semsek, T. Kirste 1 M. Stauch 1 H. - D. Bundschuh 233 236 G. Isele 20 eReferences 1. 2. 3. 4. 5. 6. 7. Archimbaud E, Thomas X, Michallet M et al. Prospective genetically randomized comparison between intensive postinduction chemotherapy and bone marrow transplantation in adults with newly diagnosed acute myeloid leukemia. J Clin Oncol. 1994;12(2):262-267. Gratwohl A, Hermans J, Goldman JM, et al. Risk assessment for patients with chronic myeloid leukaemia before allogeneic blood or marrow transplantation. Chronic Leukemia Working Party of the European Group for Blood and Marrow Transplantation. Lancet. 1998;352(9134):1087-1092. Hehlmann R, Berger U, Pfirrmann M, et al. Drug treatment is superior to allografting as first-line therapy in chronic myeloid leukemia. Blood. 2007;109(11):4686-4692. Lauseker M, Hasford J, Pfirrmann M, Hehlmann R, German CML Study Group. The impact of health care settings on survival time of patients with chronic myeloid leukemia. Blood. 2014;123(16):24942496. Warlick E, Ahn KW, Pedersen TL, et al. Reduced intensity conditioning is superior to nonmyeloablative conditioning for older chronic myelogenous leukemia patients undergoing hematopoietic cell transplant during the tyrosine kinase inhibitor era. Blood. 2012;119(17):4083-4090. International conference on harmonisation Topic E9. Note for guidance on statistical principles for clinical trials. European Medicines Agency. Document reference: CPMP/ICH/363/96, dated September 1998.http://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E9/Step4/E9_ Guideline.pdf. Hasford J, Pfirrmann M, Hehlmann R, et al. A new prognostic score for survival of patients with chronic myeloid leukemia treated with interferon alfa. Writing Committee for the Collaborative CML Prognostic Factors Project Group. J Natl Cancer Inst. 1998;90(11):850-858. 21