OCCP Fall Meeting 2014 Abstract Guidelines
advertisement

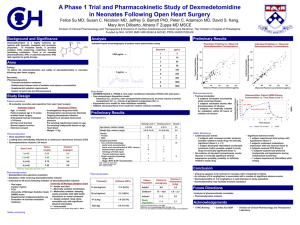
Ohio College of Clinical Pharmacy Abstract Guidelines Fall Meeting – Friday November 7, 2014 Cleveland Airport Marriott 4277 West 150th Street · Cleveland, Ohio 44135 Podium presentations are reserved for pharmacy residents (PGY1 and 2) and fellows. Students and faculty cannot be accommodated at this time. Abstract Construction 1. Submit abstracts using the template on the following page. Abstracts must be typed in “Microsoft Word” arial size 10 font or larger and must fit on a single 8.5 x 11 inch page of paper with no less than 0.5 inch margins. Please left justify all text for formatting purposes. 2. Abstracts should include the following information: title, authors names, degrees, institution(s) where work was performed, PGY-X & specialty if applicable, contact email for the first author (trainee), structured abstract (see template and example provided), and 3-5 references. Please do not use EndNote to prepare the reference section of the abstract. 3. All abstracts will be posted, as submitted, to the OCCP website (www.occpweb.org) on or before the week of the meeting for downloading by attendees. 4. All file names should be in the following format: Last name_First Name Abstract Submission Due Date 1. The due date for abstract submission for this year’s program is Friday October 10, 2014. Abstracts should be submitted via the OCCP website (occpweb.org). If you have any problems with uploading the abstracts through the website, please email Alia Poore at alia.daghstani@gmail.com. Meeting Registration 1. Please note that all poster presenters must register for the meeting and pay the registration fee. Early registration is encouraged. Title (in bold) Full names of authors and author degrees (resident’s name listed first and in bold): Resident’s email address PGY-___ & specialty (if applicable) Research Site Background: Objectives: Methodology: Results and conclusions: References: 1. 2. 3. 4. Please review the example abstract on the following page. Evaluation of dexmedetomidine for acute alcohol withdrawal syndrome in the intensive care unit Ellen Immler, PharmD; Alia Poore, PharmD, BCPS hazelee@ccf.org PGY-1 Fairview Hospital 18101 Lorain Avenue, Cleveland, OH 44111 Background: Dexmedetomidine, a selective alpha-2 receptor agonist, can provide sedative, anxiolytic, and sympatholytic effects without respiratory compromise. Despite theoretical benefits, there is a lack of evidence supporting the use of dexmedetomidine in the treatment of acute alcohol withdrawal syndrome (AWS). A few small retrospective analyses have been completed; however, these studies lacked a control group.1,2,3 Additionally, only one prospective trial has been completed to date.4 Interest in the use of dexmedetomidine in severe AWS is increasing, and compared to conventional benzodiazepine therapy, dexmedetomidine is significantly more expensive. This study evaluates dexmedetomidine use for acute alcohol withdrawal syndrome in the ICU. Objectives: (1) To determine if the use of adjunctive dexmedetomidine in patients with alcohol withdrawal will shorten ICU length of stay. (2) To determine if the use of adjunctive dexmedetomidine in patients with alcohol withdrawal will shorten hospital length of stay, reduce intubation/mechanical ventilation, and reduce the requirement for benzodiazepines administration. Methodology: Prior to commencement, this study will be submitted to the Institutional Review Board for approval. The hospital’s electronic medical record system will be utilized to identify patients admitted to the ICU for acute alcohol withdrawal syndrome, as indicated by alcohol withdrawal protocol order. Patients will be divided into two groups, based on presence or absence of an order for dexmedetomidine, and compared. Patients will be excluded from analysis if there is a concurrent order for clonidine or if, through review of clinician documentation, it is determined dexmedetomidine was not received solely for management of alcohol withdrawal symptoms. The following data will be collected: age, gender, weight, history of delirium tremens or drug abuse, total number of doses received of antipsychotic drugs, need for intubation, ICU and hospital length of stay, and deaths. Minimum and maximum Clinical Institute Withdrawal Assessment of Alcohol scores will be recorded. Dexmedetomidine use will be characterized by total duration of infusion and minimum and maximum infusion rates per day. Use of benzodiazepines will be expressed by cumulative doses. Data will be collected until intubation or until ICU discharge, whichever is first. All data will be recorded without patient identifiers and maintained confidentially. Results and conclusions: To be determined. References: 1. DeMuro et al. Use of dexmedetomidine for the treatment of alcohol withdrawal syndrome in critically ill patients: a retrospective case series. J Anesth. 2012;26:601-605 2. Muzyk et al. The use of dexmedetomidine in alcohol withdrawal. J Neuropsychiatry Clin Neurosci. 2012;24(3):E45-46. 3. Rayner et al. Dexmedetomidine as adjunct treatment for severe alcohol withdrawal in the ICU. Annals of Intensive Care. 2012;2:2-6. 4. Tolonen et al. Dexmedetomidine in addition to benzodiazepine-based sedation in patients with alcohol withdrawal delirium. European Journal of Emergency Medicine. 2012 [Epub ahead of print].