No muscular activation by the patient
advertisement

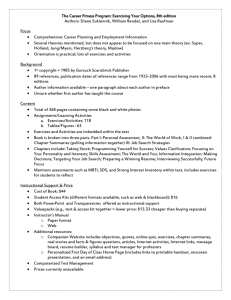
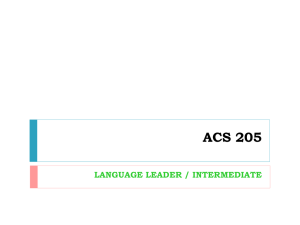
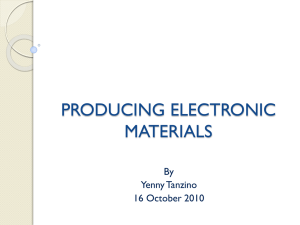
THERAPEUTIC EXERCISE THEORY AND PRACTICE First Edition 2005 Faculty of Physical Therapy Cairo University PART I -1- Preface Physical therapy as part of practice medicine involves treating disease and injury with different modalities. The use of therapeutic exercise in treatment is an important part of physical therapy. The ultimate goal of any therapeutic exercise program is achievement of symptoms free movement and improvement of function. The positive effect of therapeutic exercise include the development, improvement, restoration, or maintenance of normal range of motion, strength, endurance, mobility and flexibility. This book includes five chapters, which could provide a theoretical bases and practical application of therapeutic exercise which enables effective and safe administration of those exercises. Chapter one, introduce the student to the concept of therapeutic exercises, its importance, classifications and the different types of therapeutic exercises. Chapter two, views the dofferent positions from which the exercises is started and how to choose the appropriate position to the selected exercise. Chapters three describe the exercises needed to increase range of motion and includes traditional exercises as passive exercises and active exercises Chapter four deals with muscle performance exercises with explanation of muscle performance and its components. The chapter also demonstrate isometric exercises with its clinical application The final chapter presents the principles and guidelines for abdominal and back exercises with brief presentation of the abdominal and back muscle anatomy. -2- CONTENTS Chapter1 Introduction To Therapeutic Exercises 9 Chapter 2 Positions For Starting Exercises 15 Chapter 3 Range of Motion Exercises - Passive Range of Motion Exercises 25 29 - Continuous passive Motion Active Range of Motion Exercises Active Assisted Range of Motion Exercises Active Free Range of Motion Exercises Chapter 4 Muscle performance exercises 47 51 53 67 73 Isometric Exercises 76 Chapter 5 Abdominal and Back Exercises * * -3- 83 * -4- Introduction to Therapeutic Exercise -5- THERAPEUTIC EXERCISE Therapeutic exercise is an integral part of the practice of physical therapy. One of the most difficult tasks for a physical therapists is to design and apply an exercise program. Exercise presents both benefits and risks. This balance can be easily achieved towards the benefit side of the equation with the optimal exercise prescription. Definition Therapeutic exercise is the systematic and planned performance of body movements or exercises which aims to improve and restore physical function. Exercise is defined as “activity that is performed or practiced in order to develop or improve a specific function or skill for the sake of developing and maintaining physical fitness” Importance Of The Therapeutic Exercise 1- The ultimate goal of a therapeutic exercise program is the 2345- achievement of an optimal level of symptoms free movement during basic to complex physical activities. To improve and restore physical function. To enhance a patient’s functional capabilities and prevent loss of function. To prevent and decrease impairment and disability To optimize overall health status, fitness and sense of well-being -6- Prerequisites For Designing Exercise Program For the designing of successful and effective exercise program the followings should be fulfilled: 1- The therapist must have knowledge of anatomy, physiology, kinesiology and pathology and can integrate and apply this knowledge to each condition. 2- The therapist must understand the different forms of exercises and how these exercises affect body system. 3- The exercise program should be individualized to the special needs of each patient. Steps For Designing Exercise Program 1- Start with comprehensive examination of the patient. 2- Determine the problems and functional disabilities that the patient has. 3- Set the aims and objectives of the treatment program. 4- Select the proper exercise program that can solve the patient’s problems and improve functional capabilities. 5- Periodic e-evaluation and examination of the patients should be carried out weekly or monthly depending on the program. 6- According to the result of the re-evaluation, modifications of the program should be made to attain the optimal degree of improvement 7- The purpose and goal of the exercise program should be very clearly identified to the patient. -7- Classification of Therapeutic Exercises Therapeutic exercises in general are classified into two main categories from which many types are branched each for which has its own effects and benefits Therapeutic Exercises Active Exercises Passive Exercises Relaxed passive Exercise s Forced Passive Exercises Active assisted Exercises Static Exercises Active Free Exercises Active resisted Exercises Passive exercise: is exercise in which movement is performed entirely by an external force without any voluntary participation of the patient, The external force may be from another individual, a machine, or another part of the patient’s body. Relaxed passive exercise: is exercise in which movement is performed by an external force in the available pain free range of motion in order to maintain range of motion. Forced passive exercise: is exercise in which movement is performed by an external force within the tolerance of pain in order to increase limited range of motion. Active exercise: is exercise in which movement is performed by the voluntary effort of the patient. -8- Active assisted exercise: is exercise in which movement is performed by the voluntary effort of the patient with assistance of external force to complete the range of motion. Active free exercise: is exercise in which movement is performed by the voluntary effort of the patient through full range of motion omitting gravity or against gravity. Active resisted exercise: is active exercise in which the movement is resisted by an external force. Types of Therapeutic Exercises The therapeutic exercises are also categorized according to the aim and purpose of the exercises into many types 1- Range of motion exercises which aims to maintain and increase range of motion as traditional ROM exercises (passive- active and active assisted ROM exercises) and other techniques of joint mobilization and soft tissue stretching 2- Muscle performance exercises to increase muscle 3456- strength, power and endurance as resisted exercises, endurance exercises Postural exercises to improve posture and correct faulty posture Balance and coordination exercises to improve balance and coordination Relaxation exercises to induce relaxation Area specific exercises as breathing exercises and circulatory exercises -9- -10- Positions For Starting Exercises -11- POSITIONS FOR STARTING EXERCISES There are fundamental positions which are usually described along with their derivatives as the starting positions from which exercises start. Selection of the starting position When selecting a starting position for an exercise, the following points should be considered 1- The ability of the patient to assume the position. 2- The need to stabilize one segment of the body to permit safe and efficient movement. 3- The use of gravity for assistance or resistance. 4- The presence of pain or discomfort ( the position should be pain free to assure relaxation of the patient). 5- The use of a short lever arm versus a long lever arm. Fig. (1): Lying (supine or backlying). Characteristics It is the easiest of the whole positions. The body is most supported with a large base of support and low center of gravity. -12- Description: The body is erect with - Eyes look up, ears at the same line ( head in neutral position). - Shoulders at the same level. Trunk is relaxed on bed. - Arms by the side of the body palms in contact with table. Pelvis at the same level. - Lower limbs ( hips and knees) straight. - The feet free from the bed or in neutral position. Positions derived from lying Prone lying (Face lying) (Fig. 2) - The body is face down rested on the forehead with chin tucked in. also the head may be turned to one side for ease of respiration. - Shoulders at the same level. Trunk is relaxed on bed. - Arms by the side of the body palms facing up. Pelvis at the same level. Lower limbs ( hips and knees) straight. The feet free from the bed or in planter flexion. Fig. (2): Prone lying position. -13- Side lying (Fig. 3) - The body is lying on the side with the arms by the side and the legs straight. This position is difficult to assume as the base of support is small and rounded, some modification is made to make this position suitable for exercises performance. - The under arm is bent forward or placed under the head. The upper arm is for balance and to prevent trunk rotation. - The under leg is bent forward ( flexed 45 degrees at hip and knee) for balance and increase base of support. The upper leg is extended. Fig (3): Sid lying position. Hook lying (Crook lying) (Fig. 4) As supine lying position but hips and knees are flexed with the feet rested on the table. Fig (4): Crook lying position. -14- Sitting Characteristics It is comfortable, natural and very stable position. The center of gravity is low but near to the edge of the base of support which is the area between both the legs of the seat and the feet. Description: The body is resting on a chair ( with back support) or stool (without back support) - Eyes look forward, ears at the same line ( head in neutral - position). Shoulders at the same level. - Back is straight. The back is supported in case of sitting on chair with back support. While when sitting on stool the back is unsupported making the position less stable and need effort of the subject to maintain back straight. Arms by the side of the body. - Pelvis at the same level. Thighs fully supported and together on the chair ( hips, - knees, and ankles at right angle flexion). The feet rested on the floor. In case of sitting on stool, according to the height of the stool the feet may be rested or not on the floor. Positions derived from sitting Long Sitting (Fig. 5) As in supine position but the body is bent at the hips and the trunk is raised from lying to an angle of 90 degree. -15- - Eyes look forward, ears at the same line ( head in neutral position). Shoulders at the same level. - Back is straight. - Arms by the side Knees are extended - Ankles are relaxed. Fig (5): Long sitting position. Forward Lean Sitting (Fig. 6) Trunk is inclined forwards and the head is supported on pillows on a table at the front. Fig (6): Forward Lean Sitting Position. -16- Kneeling Characteristics The position is unstable and difficult to maintain as the center of gravity is high and the line of gravity falls close to the edge of the base which the area of the legs only Description: The body is upright from the knees which are held at right angle - Eyes look forward, ears at the same line ( head in neutral position). - Shoulders at the same level. Arms by the side of the body palms facing inward. - The back is straight. Pelvis at the same level. Lower limbs ( hips straight and knee right angle flexion). Knees and legs are together and supported on the floor The feet are planter flexed Positions derived from kneeling Kneel Sitting The position is stable. From kneeling to sitting back on the heels. Prone Kneeling (cat position) (Fig. 7) Kneeling supported by the four limbs. The arms should be straight and the hands in line below the shoulders. Right angle should be maintained at the hips and knees. The ankles are planter flexed. -17- Fig (7): Prone Kneeling Position. Standing Characteristics The base of support is very small and the center of gravity is high. Description: The body is erect with - Eyes look forward, ears at the same line ( head in neutral position). Shoulders at the same level. Arms by the side of the body palms facing inward. The back is straight and stretched. Pelvis at the same level. Lower limbs ( hips and knees) straight. The feet are together at the same level. The toes are slightly apart (the angle between the feet not exceed 45 degree). -18- Positions derived from standing Stride Standing It is the most commonly used position assumed by the physical therapist during treatment of patients. - The same as standing but the feet are sideways pace apart and the base is therefore wide side to side giving good lateral stability. Walk Standing - The same as standing but the feet are a forward pace apart and the base is therefore wide from front to back giving good anteroposterior stability. -19- Range of Motion Exercise -20- RANGE OF MOTION EXERCISES Range of motion: Range of motion is the term that is used to describe the amount of movement that occur at each joint. Every joint in the body has a "normal" range of motion. Joints maintain their normal range of motion by being moved. It is therefore very important to move all your joints every day. Causes of decreased Range of Motion 1- Prolonged immobilization or bed rest. 2- Trauma to soft tissues, bones or other joint structures. 34567- Muscle weakness. Surgeries. Joint disease. Neuromuscular disease. Pain. Effect of Immobilization and Decreases Mobility Immobilization leads to decrease loading and stress on joints and soft tissues resulting in 123456- Joint stiffness and adhesion. Atrophy and weakness of the skeletal muscle. Decrease tensile strength of tendons and ligaments. Degeneration of articular surface. Adaptive shortening of the muscle and soft tissues. Osteoporotic changes of the bone. -21- All these complications lead to decrease ability of to perform the activities of daily living Range Of Motion Exercises Active Assisted ROM exercises Passive ROM exercises Active Free ROM exercises Joint Mobilization Stretching -22- Range of motion exercises: Range of motion exercises are also called "ROM" exercises. ROM exercises may be active or passive. Active ROM is done when a person can do the exercises by himself. Activeassisted ROM exercises are done by the person and a helper. Passive ROM exercises are done for a person by a helper. The helper does the ROM exercises because the person cannot do them by himself. Importance of ROM Exercises Range of motion (ROM) exercises are done to 1- Preserve and increase flexibility and mobility of the joints on which they are performed. 2- Prevent or at least slow down the freezing or adhesion of joints. 3- Reduce stiffness. -23- PASSIVE RANGE OF MOTION EXERCISES Definition: It is exercise in which movement is performed by an external force in the available pain free range of motion. The external force may be from the therapist, family member, or the patient or equipment. Passive ROM exercises are characterized by: No muscular activation by the patient Performed within the available ROM Applied by some external force No pain Importance of Passive ROM Exercises Passive ROM exercises are very important if you have to stay in bed or in a wheelchair. ROM exercises help keep joints and muscles as healthy as possible. Without these exercises, blood flow and flexibility (moving and bending) of the joints can decrease. Passive ROM exercises help keep joint areas flexible. Indications Passive exercises are indicated with the following conditions 1- when voluntary movements are impossible as when the subject is comatose, or when paralysis of the part. -24- 2- When Active movement may disrupt the healing process, as when there is acute inflammation of the joint or the surrounding tissue. 3- When active movement is too painful to perform, as after surgery and injury for 2 to 6 days according to the condition. Aims of Passive ROM Exercise Passive exercises are largely preventive in nature and are used to: 1- Maintain range of motion. 2- Maintain joint and connective tissue mobility. 3- Minimizes the effects of and the formation of 4567- contractures. Enhances synovial movement. Maintain mechanical elasticity of muscles. Assist circulation and vascular dynamics. Help maintain the patient’s awareness of movement. Points to remember Passive ROM exercises will NOT Build up muscles or make them stronger. Prevent muscle atrophy Increase strength or endurance Assist in circulation to the extent that active, voluntary muscle contraction will -25- Application of Passive Exercises Technical Principles Before performing passive exercises, some of the technical principles should be remembered 1- Place the patient in proper comfortable position with proper body alignment and stabilization to perform the exercise. 2- The therapist should be in a proper position and effective stance 3- Free the region from restrictive closes, linen, splints, and dressings 4- Drape and cover the patient as necessary. 5- Utilize the proper hand holds or grasps by the therapist. 6- Perform the exercise slowly, smoothly with rhythm within the available pain free range of motion without any force behind the range. 7- Do all ROM exercises smoothly and gently. Never force, jerk, or over-stretch a muscle. This can hurt the muscle or joint instead of helping. 8- Stop ROM exercises if the person feels pain. The exercises should never cause pain or go beyond the normal movement of that joint. 9- Repeat the exercise 5 to 10 repetitions according to the patient condition and response -26- Procedures Passive Exercises of the Upper limb Shoulder Flexion and Extension (Fig. 1) Patient Position: Supine lying Therapist Position : Stride standing beside the involved part at the level of the elbow. The therapist move his body weight over his legs to follow the movement Grasp: * Distal hand grasps the patient’s arm just under the elbow * Proximal hand, crossover and grasp the wrist and palm of the patient’s hands Motion: Lift the arm through the available range of motion of flexion and return to extension. Fig. (1): Shoulder flexion and Extension (A) initiating and (B) Completing shoulder flexion -27- Alternate Position: if the patient can not assume supine lying position the exercise could be performed from side lying. The proximal hand stabilize the scapula and the distal hand and forearm carry and support the weight of the patient’s upper limb. This position enable the therapist to perform shoulder hyperextension also (Fig. 2). Fig. (2): Shoulder flexion, extension and hyperextension. Shoulder Abduction and Adduction (Fig. 3) Patient Position: Supine lying. Therapist Position: Stride standing beside the involved part at the level of the elbow. The therapist should step back to allow the patient’s arm to move in full range of motion of abduction. Grasps: Proximal hand just under the elbow. Distal hand grasps the patient’s wrist and the palm, or shake hand with the patient’s hand. -28- Motion: The therapist bring the arm horizontally away from the body until 90 degree and then return with it again into adduction. Fig. (3): Shoulder abduction and adduction. Shoulder Internal and external Rotation (Fig. 4) Patient Position: supine lying with the affected arm shoulder flexed 90 degrees and elbow flexed 90 degrees, the forearm in neutral position so the palm face the patient. Therapist Position: Stride standing at the level of the elbow. Grasp: Proximal hand grasps patient’s wrist and hand with the index between the patient’s thumb and index and thumb and the rest of fingers on either sides of the patient’s wrist to stabilize it. Distal hand grasps the elbow under grasp. Motion: The therapist move the forearm towards the feet in internal rotation then towards the head in external rotation. -29- Fig. (4): Shoulder internal and external Rotation. Shoulder Horizontal Abduction and Adduction (Fig. 5) Patient Position: supine lying with the shoulder at the edge of the table, shoulder in abduction 90 degree and elbow either flexed or extended. Therapist Position: Stride standing at the shoulder level facing the patient. Grasp: As in flexion and extension. Motion: move the upper limb across the chest towards the other shoulder then return. -30- Fig. (5): Horizontal (A) abduction and (B) adduction of the shoulder. -31- Movements of the shoulder joint could be performed with elbow flexed if the limb is completely paralyzed or the patient is too obese and the weight of the limb is heavy for the therapist. Elbow Flexion and Extension (Fig. 6) Patient Position: Supine lying with the forearm supinated. Therapist Position: Stride standing at the level of the forearm. Grasp: Proximal hand grasp the wrist and hand of the patient. Distal hand holding under the elbow.. Motion: the elbow is bend into flexion then extended with the forearm in different position of supination, pronation and mid position. Fig. (6): Elbow flexion and extension. -32- Pronation and Supination (Fig. 7) Patient Position: Supine lying with elbow flexed 90 degrees. Therapist position: Stride standing at the level of the elbow Grasp: Proximal hand grasping the patient’s wrist, supporting the hand with the index finger and placing the thumb and the rest of the fingers on either sides of the wrist. Other grasp is by shake hand with the patient Distal hand holding the elbow in position with under grasp. Motion: roll the forearm into supination and pronation. Fig. (7): Supination and pronation. -33- Wrist joint Flexion, Extension, Radial Deviation and Ulnar Deviation (Fig. 8) Patient Position: Supine lying with elbow flexed 90 degrees and forearm in mid position. Therapist Position: Stride standing facing the patient at the level of the forearm. Grasp: Proximal hand stabilize the forearm just above the wrist joint. Distal hand hold patient’s hand. Motion: move the wrist in the four directions. To get full range of wrist allow fingers to move freely as you move the wrist. Fig. (8): Passive exercises for wrist joint. -34- Thumb and Fingers Passive Exercises( Fig. 9) Patient Position: Supine with elbow flexed 90 degrees. Therapist Position: Stride standing facing the patient. Grasp: There are many joints of the fingers (metacarpophalangeal and proximal and distal interphalangeal joints, so as a role always with one hand, stabilize proximal to the joint you want to move and then with the other hand move the distal segment of the joint. Passive Exercises of the Lower Limb Hip Flexion and Extension (Fig. 10) Patient Position: supine lying position. Therapist Position: Stride standing at the level of the patient’s knee joint facing the patient. Grasp: Proximal hand under the patient’s knee to support and lift the patient’s leg. Distal hand under the heel. Motion: the lower limb is taken into complete hip and knee flexion and as you flex the knee the therapist’s hand should slide to the side of the thigh to avoid limiting the range. At the end of the range the therapist’s hand may slide over the knee to reach full range. Then the therapist slides his hand under the knee to carry the weight of the lower limb and bring the lower limb back to extension of hip and knee. -35- Fig. (9): Passive Exercises of the thumb (A) and Fig. (10): Flexion and Extension of the hip. the fingers (B). Alternate Position: if the patient can not assume supine lying position the exercise could be performed from side lying. The proximal hand stabilize the pelvis and the distal hand and forearm carry and support the weight of the patient’s lower limb. This position also enable the therapist to perform hip hyperextension also (Fig. 11). -36- Fig. (11): Hip Flexion, Extension, and hyperextension from side lying Abduction and Adduction of the Hip (Fig. 12) Patient Position: Supine lying with the affected lower limb in neutral position and the other lower limb in slight abduction to permit full adduction of the affected limb. Therapist Position: Walk standing at the level of the patient’s knee. Grasp: Proximal hand under the patient’s knee to support the leg . Distal hand under the heel. Motion: move the limb into abduction away from the patient and towards you as you step back to allow full range. Then bring the lower limb into full adduction until in contact with the unaffected one. -37- Fig. (12): Abduction and adduction of the hip. Hip Internal and External Rotation with knee flexed (Fig. 13) Patient Position: Supine lying With hip and knee flexed 90 degrees Therapist Position: Stride standing at the level of the patient’s knee. Grasp: Proximal hand over the patient’s knee to support the knee in flexion. Distal hand and forearm carrying the patient’s lower leg. Motion: move the leg medial and lateral so the hip will rotate into internal and external rotation -38- Fig. (13): Hip Internal and External Rotation with knee flexed Hip Internal and External Rotation with Extended knee Patient Position: Supine lying Therapist Position: Stride standing at the level of the patient’s knee. Grasp: Proximal hand under the patient’s knee to support the knee. Distal hand under the ankle. Motion: roll the thigh inward and outward. Ankle Dorsi and Planter Flexion (Fig. 14) Patient Position: Supine lying Therapist Position: Stride standing at the level of the patient’s feet. -39- Grasp: Proximal hand just above ankle joint to stabilize the lower leg in dorsi flexion and in planter flexion the hand over the dorsum of the foot. Distal hand and forearm carrying the patient’s foot. Motion: move the foot up into dorsi flexion and pushing down into planer flexion. Fig. (14): Ankle Dorsi and Planter Flexion Subtalar Inversion and Eversion (Fig. 15) Patient Position: Supine lying Therapist Position: Stride standing at the level of the patient’s feet. Grasp: Proximal hand just above ankle joint to stabilize the lower leg. -40- Distal hand and forearm carrying the patient’s foot. The thumb medial and the fingers lateral to the joint on either side of the heel. Motion: turn the heel inward and outward. Fig. (15): Subtalar inversion (A) and eversion (B). -41- -42- -43- -44-