Vitamin D in paediatric renal transplant recipients: interaction with

Vitamin D in paediatric renal transplant recipients: interaction with calcineurin inhibitors?
Agnieszka A Prytuła (1, 2), Antonia H Bouts (3), Martijn van Gorkom (1), Eiske Dorresteijn
(1), Karlien Cransberg (1)
(1) Pediatric Nephrology Department, Erasmus MC - Sophia Children’s Hospital, Rotterdam
(2) Pediatric Nephrology Department, University Hospital Ghent
(2) Pediatric Nephrology Department, Emma Children’s Hospital, Amsterdam
Corresponding author: A. Prytuła a.prytula@erasmusmc.nl
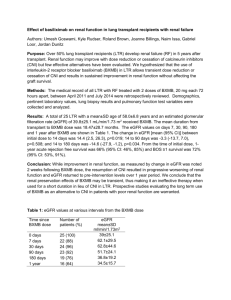
Objective: The use of calcineurin inhibitors (CNI) following renal transplantation is associated with bone disease, but its mechanism has not yet been elucidated. The aim of the study was to evaluate the 25(OH)D and 1,25(OH)
2
D levels in stable paediatric kidney transplant patients with emphasis on the interaction with CNI.
Methods: We included 62 renal transplant recipients in this retrospective cross-sectional study. Activated or nutritional vitamin D supplementation and CKD stages 4 -5 were exclusion criteria. The median time since transplantation was 16.5 months. The median eGFR was 67 ml/min/1.73m². Sixty one children were on CNI and 38 on corticosteroids. The control group included 32 pre-transplant children with CKD stages 1-3 and median eGFR 64 ml/min/1.73m².
Results: In the transplant group 56% children had low levels of 25(OH)D and 45% had hyperparathyroidism versus 53% and 53% respectively in the control group. Transplanted children had higher 1,25(OH)
2
D levels compared with pre-transplant children . The
1,25(OH)
2
D levels were exceptionally high in the first year post-transplant and correlated with the tacrolimus dose and inversely with the tacrolimus trough level and the dosenormalised tacrolimus level (DNTL). DNTL was a significant negative predictor of the
1,25(OH)
2
D levels (β=-0.54, P=0.01, CI95% -0.93— -0.14, R²=0.66).
Conclusion: In contrast with the low 25(OH)D levels, 1,25(OH)
2
D levels in post-transplant children were normal to high. High 1,25(OH)
2
D levels were associated with an increased
CNI metabolism as expressed by DNTL. The involvement of CYP3A4 in both CNI metabolism and intestinal catabolism of 1,25(OH)
2
D may help explain the mechanism behind
CNI-induced osteoporosis.