The Omega-3 Story
Nutritional Prevention of Preterm Birth and Other Adverse Pregnancy
Outcomes
James A. McGregor, MDCM*; Kenneth G. D. Allen, PhD†; Mary A. Harris, RD, PhD†;
Melanie Reece, PhD‡; Marsha Wheeler, MD*‡; Janice I. French, CNM*; John Morrison,
MD§
*University of Colorado School of Medicine, Department of Obstetrics and Gynecology, and ‡Denver
Health Medical Center, Department of Obstetrics and Gynecology, Denver, Colorado; †Colorado State
University, Department of Food Science and Human Nutrition, Fort Collins, Colorado; and §University of
Mississippi School of Medicine, Department of Obstetrics and Gynecology, Jackson, Mississippi
OBSTETRIC AND GYNECOLOGIC SURVEY 2001;56:S1-S13
[Click here for reference links. (64 references linked.)]
“Let food be thy medicine.”—Hippocrates.
Healthy intrauterine growth and development, appropriately timed parturition, and safe
birth continue to be critical determinants of each child’s chances of achieving their full
biological potential. Essential fatty acids (EFAs) and their metabolites are involved in the
synthesis of eicosanoids that play essential and multifaceted roles in human reproduction,
especially during pregnancy, parturition, and lactation. Fatty acid-derived prostaglandins
(PGs), hydroxyeicosatetraenoic molecules (HETE), leukotrienes (LTs), thromboxanes
(TXs), and prostacyclins (PIs) play well-documented “final common pathway” molecular
roles in both normal term labor as well as in preterm parturition (1). Abnormalities of
thromboxane and prostacyclin physiology also occur with preeclampsia, eclampsia, and
pregnancy-induced hypertension (PIH), which often require preterm delivery (2).
Docosahexaenoic acid (22:6 -3, DHA) and other EFA derivatives are important
components of the rapidly growing brain and retinal tissues of the perinate (3). DHA, a
long-chain omega-3 ( -3) fatty acid (LCPUFA) is expressed in breast milk, and breast-fed
and DHA-nutritionally supplemented children demonstrate improved performance on
various tests of brain and vision functioning (4). Ensuring maternal and perinatal
nutritional sufficiency during pregnancy and lactation is investigated increasingly as an
effective and inexpensive strategy for optimizing pregnancy and lactational outcome (5).
Informed families and providers are invested both in preventing the occurrence and
consequences of prematurity and inadequate uterine growth (6). Families and providers
are similarly interested in optimizing healthy growth and development of the fetus’
developing organs, especially brain, retina, and the cardiovascular system (7).
Preterm birth continues to cause neonatal morbidity and life time disabilities (8). Preterm
birth is associated with potentially immense direct and indirect costs, as well as
liabilities for care providers. Preterm birth is best understood as a syndrome caused by
numerous diseases such as intrauterine infection and inflammation, uterine over-distention
or intrauterine bleeding. Such causes of prematurity are best considered as “complex
diseases.” Complex diseases involve interactions between multiple bodily systems or
parameters including nutrition, immunity, coagulation, and the endocrine system. For
example, the fetus depends on maternal nutrients, such as EFAs, for multiple bodily
functions including eicosanoid metabolism as well as brain growth and retinal
development. Thus, if the mother is deficient in certain fatty acids, this deficiency tends to
be compounded in the fetus (9). Such complex disease processes are best dealt with using
primary prevention techniques—such as ensuring nutritional sufficiency, particularly -3
LCPUFA sufficiency, during pregnancy and lactation.
THE OMEGA-3 HYPOTHESIS
Reduced rates of low birth weight in fish-eating northern European populations (10)
continue in marked contrast with persistently higher rates of low birth weight in nonfishconsuming populations (11). These observations prompt examination of how aspects of
diet, such as the consumption of EFAs and their metabolites, may influence pregnancy.
Synthesis of -linolenic acid (18:3 -3, LnA) and linoleic acid (18:2 -6, LA) does not
occur in higher animals (12). These fatty acids are associated with well-defined deficiency
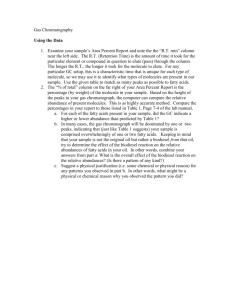
states (13, 14). Dietary LnA is the substrate (desaturase and elongation) for the -3
LCPUFAs, including DHA and eicosapentaenoic acid (20:5 -3, EPA) (15, 16) (Fig. 1).
LA is the precursor for arachidonic acid (AA), from which the potent -6 eicosanoids are
derived (17, 18). DHA, EPA, AA, and other LCPUFAs are not considered essential
because they can be synthesized in the liver from dietary LnA and LA (15). Importantly,
the same series of hepatic microsomal desaturase and elongation enzymes metabolize both
the -6 and -3 families of PUFAs in both fetal and adult liver (16, 17). As -6 fatty
acids predominate in both the adult and fetal diets, little DHA is ever produced from LnA
because of competitive inhibition. Therefore, preformed sources of -3 LCPUFA, such as
DHA and EPA are important in the maternal and infant diet.
Fig. 1. Biosynthesis of eicosanoids from EFAs, PG, LT, TX. Adapted
from Nair et al. (64).
Fatty acids are actively transported across the placenta where -3 fatty acids, including
DHA, as well as -6 fatty acids are extensively incorporated in the fetal tissues including
the placenta, erythrocytes, and neural tissues, especially neuronal myelin and retinal
photoreceptors (12, 18, 19). This so-called “placental biomagnification” occurs most
efficiently during the latter half of pregnancy.
Essential fatty acids in the maternal diet are among the most extensively studied dietary
factors influencing gestational length, fetal growth, and brain development (12, 14, 19–
22). It is suggested that early hominids and our human ancestors evolved consuming foods
with approximately equal proportions of -3 and -6 fatty acids (12, 23). This
observation leads to concern that contemporary diets provide 1) excess -6 fatty acids and
2) insufficient -3 fatty acids including DHA and EPA (23). It is suggested that these
imbalances could increase risks of preterm parturition, and possibly preeclampsia/PIH as
well as impair brain and retinal development in susceptible mothers and babies (23).
Preterm birth may impair newborn -3 EFA-related growth, development and neuronal
functioning, as most placental transport occurs in the second half of pregnancy (24, 25),
the preterm newborn liver possesses insufficient desaturase and elongation enzymes, and
breast milk or -3 LCPUFA supplementation may not be made available (25–30).
These connections between -3 LCPUFA and parturition have led to the hypothesis that
-3 LCPUFA insufficiency or -6 fatty acid excess can modulate gestational length. Both
animal and human studies suggest that diet-derived -3 LCPUFA are competitive with the
-6 fatty acid AA to alter production of the relatively more potent 2-series prostaglandin
(PGE2, PGE2 , and leukotrienes) (Table 1) (13). Animals with -6 fatty deficiency and
animals fed high levels of -3 fatty acids demonstrate reduced PG synthesis and increased
lengths of gestation (14). Consuming oily fish and dietary fish oils, which are rich in longchain -3 fatty acids, delays the onset of parturition and increases both the length of
gestation and birth weights in animal models (14). These effects are associated with
decreased PGE2 content of uterus, placenta, and fetal membranes (14). Clinical and
laboratory observations confirm that pregnant women and animal models who are
deficient in DHA suffer increased risks of a shortened gestation. Recent controlled trials
of DHA/EPA supplementation (fish or fish oil) are associated with reduced risks of
premature births in women who suffered a prior preterm birth and increased gestation
length and birth weight in women not selected as part of the control group (5).
Table 1. Nomenclature of important -3 and -6 fatty acids
This review will analyze contemporary knowledge regarding the roles of dietary DHA and
other -3 fatty acids in achieving successful pregnancy outcomes, including reducing
risks of prematurity. We propose that optimized maternal -3 LCPUFA status during
pregnancy and lactation, as well as before pregnancy and during the interconception
period, will be shown to enhance each mother’s chances of a healthy pregnancy and each
child’s chances of being well born.
PALEOBIOTIC NUTRITION
An extensive review by Broadhurst et al. (31) documents that early hominids as well as
Cro-Magnan man and our immediate preindustrial ancestors consumed -3 and -6 EFAs
in roughly equal proportions (1:1). Early hominids, as well as recently studied huntergather groups, have been shown to consume naturally varied diets commonly termed C-3
or C-4. These mixed diets consisted of wild foods available within grassy, forest, or shore
environments. Today’s postindustrial and industrial humans consume considerably greater
amounts of -6 EFAs, than did our ancestors. These -6 fatty acids are found in dairy and
meat products, fried or “fast” foods, vegetable oils, and commercially prepared baked
goods containing vegetable oils. Contemporary North Americans and Europeans consume
diets with estimated total -6 to -3 ratios of 10 to 25:1 (12, 31).
Estimates of prehistoric and preindustrial DHA consumption are approximately 200 to
1500 mg daily for a ratio of 4:1 to 1:1 -6 to -3 fatty acids (31). Most contemporary
Westerners consume less than 200 mg of DHA daily (23). These observations suggest that
modern diets are insufficient for DHA and other -3 fatty acids, at least in comparison
with our preindustrial ancestors.
ESSENTIAL FATTY ACID METABOLISM
Kinetic studies in liver microsomes and hepatocytes show that delta-6 ( 6) desaturase is
the rate-limiting enzyme system. Binding affinity for 6 desaturase is highest for LnA,
high for LA, and lowest for oleic acid (16). Consequently, relative abundance of the -3
progenitor linolenic acid tends to reduce -6 production of eicosanoids. Because of this
biochemical bottleneck at 6 desaturase, deficiencies of one or more essential fatty acids
can be detected by measuring downstream changes of 6 derivatives.
A common response seen in an -3 LCPUFA deficiency is a compensatory increase in 6 FAs, particularly docosapentaenoic acid (22:5 -6, DPA) and to a lesser extent, 22:4 6. Neural tissues of -3 FA-deficient animals demonstrate roughly a 45-fold increased in
the content of -6 DPA compared with controls (19, 20, 32). Faced with both -3 and 6 EFA deficiencies, -9 derivatives, especially eicosatrienoic acid (20:3 -9), are
increased.
Consumption of preformed -3 DHA and EPA as well as -6 AA is the surest way to
ensure adequate amounts of these FAs. Humans convert dietary LnA to both DHA and
eicosapentaenoic acid (20:5 -3), but the capacity for this conversion is limited. For
example, excess -6 fatty acids, particularly in the ratios described previously (10 to
20:1), limit the efficiency of this conversion. Nutritional enhancement of EFAs and
LCPUFAs are potentially powerful means to influence eicosanoid metabolism including
production of PGs, LTs, and TXs.
PROSTAGLANDIN BIOSYNTHESIS
The potent 2-series prostaglandins are synthesized from phospholipid-derived arachidonic
acid by prostaglandin H synthase (PGHS) or cyclooxygenase (COX) (Fig. 1). The
common intermediate of PG biosynthesis, PGH2, gives rise to a variety of prostaglandins
including PGE2 and PGF2 . Two forms of cyclooxygenase occur in tissues: constitutive
COX-1 and inducible COX-2 (33). Inducible COX-2 expression seems important in
sustaining the conversion of AA to PGs because rapid autoinactivation of the
cylcooxygenase pathway occurs as PGH2 is formed. COX-2 expression in rat uterus has
been shown to increase approximately 4-fold at the onset of parturition, while COX-1
expression remains constant. Inhibition of COX-2 expression powerfully inhibits
intrauterine prostaglandin production (34). Membrane -3 LCPUFAs give rise to the less
potent 3-series (trienoic) PGs. Omega-3 fatty acids tend to depress the synthesis of the
more potent 2-series PGs. This occurs presumably by preferential competition at the level
of PGHS, similar to the 6 desaturase “bottleneck, or simply by displacing AA from
membrane phospholipids. Because DHA preferentially displaces AA in cell phospholipid
membranes, DHA can significantly reduce production of -6 series PGs (Fig. 1).
PROSTAGLANDINS IN GESTATION AND PARTURITION
Prostaglandins and other eicosanoids derived from -3 and -6 fatty acids play essential
roles in both normal and pathologic gestation and parturition (1, 35, 36). Arachidonic acid
as well as PGE2 and PGF2 concentrations are elevated in the maternal circulation before
the onset of spontaneous labor (35). Exogenous administration of either PGE2 or PGF2
induces cervical ripening, myometrial contractions, and uterine emptying (37).
Furthermore, inhibitors of COX-1 and -2 inhibit labor (34). Amniotic fluid concentrations
of prostaglandins are lower in early and mid-pregnancy than at term (38, 39). Studies in
animals show that intrauterine tissues demonstrate increased PGHS activity during the
third trimester with rapid increases before parturition. In rabbit amnion, a 10- to 38-fold
increase in PG synthesis occurs from day 20 to 30 (term = 31 days), with the sharpest
increases occurring on days 29 and 30 (40). The dienoic PGs, PGE2 and PGF2 , as well
as the major metabolite of PGF2 (15-keto-13,14-dihydo-PGF2 ), are increased in
amniotic fluid during labor (41–43). Further, primary PG metabolites increase in the
maternal circulation during labor, adding to the overwhelming evidence that sharply
increased PG synthesis from -6 FA precursors occurs during parturition (41–43).
Maternal, fetal, and trophoblast tissues all metabolize EFAs to varying degrees.
Eicosanoid production from EFA precursors occurs in both maternal (uterus, decidua) and
fetal tissues (placenta, membranes). Tissue sample homogenates (amnion, chorion,
placental vessels, placenta, and myometrium) extracted both before and after labor, all
demonstrate capability for conversion of labeled AA into one or more PGs (44). PGHS
has been localized in amnion epithelium and the cytoplasm of fibroblast-like cells in
subepithelial amnion connective tissue. PGHS activity has also been identified in villous
cytotrophoblast, syncytiotrophoblast, and decidualized stroma (45, 46). PGE2 has been
identified in all gestational tissues and PGF2 is measurable in all but the amnion. The
prostacyclin metabolite, 6-keto-PGF1 , has been found in the myometrium, placental
vessels, amnion, and chorion (44). Although TX has been found in the placenta, placental
vessels, and myometrium, it is unclear whether these tissues synthesize TX or whether TX
is contributed by blood platelets. Comparisons of relative PG biosynthetic abilities among
gestational tissue show that myometrium demonstrates the greatest rate of AA to PG
conversion, whereas the placenta demonstrates the lowest. Amnion demonstrates the
highest capacity for PGE2 synthesis (40). Other eicosanoids including PIs and LTs also
play roles in gestation and parturition (40).
LEUKOTRIENES AND LIPOXYGENASE PRODUCTS IN PREGNANCY
Leukotrienes (LT) are noncyclized -6 and -3 metabolites containing three conjugated
double bonds. The role of LTs in inflammation, vascular permeability, and chemotaxis is
established. LT synthesis depends on 5-lipoxygenase and fatty acid substrates, including
AA and DHA (Fig. 1). A growing body of evidence suggests that arachidonic acid 5lipoxygenase products, particularly 5-HETE and LTC4, are important regulators of labor
onset (47). 5-HETE can induce uterine contractions and 5-HETE concentrations in
amniotic fluid increase 2- to 3-fold 1 week before labor in human pregnancy. Rhesus
monkeys treated with indomethacin, a cyclooxygenase inhibitor that reduces PG
production, give birth with only increases in amniotic fluid 5-HETE and LTC4, i.e.,
without increases in amniotic fluid PGF2 (47). These observations suggest that the 5lipoxygenase products of arachidonic acid, particularly 5-HETE and LTC4, are important
in the parturition process and challenge the primacy of PGs as molecular mediators of
labor (48). Correspondingly, 5-lipoxygenase products of -3 fatty acids are less potent
than those derived from -6 fatty acids. Each of the dienoic (potent) and trienoic (less
potent) eicosanoids demonstrates distinctive, but often overlapping or reinforcing
activities on reproductive tissues.
CERVIX AND MYOMETRIUM
Many EFA metabolite-mediated biochemical and biophysical changes occur in the cervix
in preparation for labor as well as during labor. The nonpregnant cervix is a firm, inelastic
structure compared with the soft and compliant cervix at delivery. Cervical ripening
involves dramatic changes in the configuration and concentration of cervical collagen
fibers, resulting in reduction in the tensile strength. At term, cervical collagen bundles are
fragmented and dispersed and collagen concentrations are decreased by 70% (49).
Prostaglandins and other eicosanoids are involved in: 1) the rate of cervical cellular
synthesis of collagenase and procollagenase, 2) concentrations of collagenase inhibitors
(anti-collagenase and 2-macroglobin), as well as 3) concentrations and activities of
collagenase activators (50). Within 6 hours of systemic or local PGE2 administration,
cervical collagenolysis begins concomitantly with increased myometrial activity (45). In
vitro studies on cervical smooth muscle demonstrate relaxation induced by PGE2 (49).
The 2-series eicosanoids leukotriene C4 and D4 have been associated with cervical
changes as well as uterine contractions even in the presence of suppressed levels of
PGF2 , during term and preterm labor (48).
Omega-6-derived eicosanoids mediate uterine concentrations by bringing about
intracellular release of calcium within myometrial cells. This leads to an increase in
intracellular cAMP, producing sequestration of calcium in the myometrial mitochondria
and sarcoplasmic reticulum (49). Additionally, PGs induce formation of gap junctions
between myometrial cells. Gap junction formation is critical for the efficient and rapid
spread of action potentials cell-to-cell within the uterus, with synchronized generation of
contractions in the entire myometrium.
EICOSANOIDS AND INFECTION DURING GESTATION
Intrauterine infections and chorioamnionitis are established causes of premature labor (36,
51). More potent inflammatory eicosanoid molecules derived from AA may heighten
intrauterine inflammatory responses and increase risks of preterm birth at relatively lower
thresholds of microbial contamination than would occur with the presence of less potent
-3-derived eicosanoids (52). Extrauterine infections in pregnancy can also alter cytokine
and eicosanoid metabolism, which can predispose to preterm parturition.
ANIMAL DIET SUPPLEMENT STUDIES
Animal studies have been performed to justify FA supplementation studies during human
pregnancy. Our group demonstrated both potential benefit and adverse effects of EFA/fish
oil supplementation in animals. Supplementation with high doses of 480 mg/day fish oil
(containing 200 mg of DHA) versus olive oil (control) from the day of mating until
delivery resulted in a 7-hour increase in the length of gestation in timed-mated pregnant
rates (54). However, dam weight at day 20 and pup weight was significantly reduced in
the high-dose fish oil-fed group. This effect is not seen with a lower dose of fish oil (200
mg/day) and may be because of inhibitory effects on EPA on perinatal growth. In a
second series with timed-mated rates that were surgically delivered on day 20 of gestation,
fish oil was found to selectively depress prostaglandin synthesis in amnion and uterine
homogenates and nonsignificantly depress PG synthesis in placenta. Treatment with fish
oil increased incorporation of DHA and EPA into placenta and uterus but not at the
expense of AA. Other animals, as well as human, studies suggest that diet-derived longchain -3 fatty acids act competitively with AA to alter production of LTs and 2-series
PGs during pregnancy (Table 2 and Table 3) (55, 56). In other studies, animals with -6
fatty acid deficiency and those fed high levels of -3 fatty acids have depressed PG
synthesis and increased lengths of gestation (58, 59).
Table 2. Selected observational studies of -3 and -6
fatty acids in pregnancy
Table 3. Selected controlled supplementation trials with
DHA/EPA or fish oil in pregnancy and/or lactation
HUMAN OBSERVATIONAL STUDIES
Investigations of maternal fatty acid status and PG production have been performed in
Colorado mothers (57–59). These studies will be detailed because our Colorado
population eats little or no fish and consume high amounts of -6 EFAs, in comparison
with fish-eating northern European populations (57). Our study women may be
representative of many modern women who consume few -3 EFAs, yet consume
increased amounts of -6 EFAs.
In a case-control, prospective study, 37 preterm and 34 control mother-baby dyads were
studied for multiple EFA-related parameters (58, 59). Fatty acid profiles (expressed as
percent of total fatty acids) were determined in both maternal and fetal red blood cells and
plasma, as well as placental tissues. Maternal plasma and erythrocyte AA was
dramatically higher in preterm mothers and babies than in controls sampled at comparable
gestational ages (34 weeks) and at delivery. Remarkably, maternal erythrocyte AA from
mothers delivering preterm showed a 278% increase in AA compared with controls at
delivery, and a 149% increase compared with undelivered controls at 34 weeks of
gestation.
Arachidonic acid levels were also increased in both total maternal plasma lipid and
phospholipids in preterm mothers. For maternal plasma total lipids, AA showed a 42%
increase in preterm mothers compared with controls at delivery and an 18% increase
compared with controls at 34 weeks of gestation. Thus, increased arachidonic acid in both
maternal erythrocytes and plasma total lipids was dramatic and consistent in preterm
mothers.
Correspondingly, we found markedly higher LA in maternal erythrocytes and modestly
higher LA in plasma total fatty acids in women delivering preterm. There was a
confirmatory 47% increase in LA compared with controls at 34 weeks of gestation. For
plasma total fatty acids there was a significant, but more modest (10%) enrichment of LA
in preterm samples. Our interpretation is that AA enrichment in preterm samples likely
reflects the diet consumed by these women—that is, a diet high in LA ( -6) fatty acids.
Women who delivered preterm also had evidence of reduced -3 levels. The sum of -3
LCPUFAs in maternal plasma phospholipids at delivery was significantly (34%) lower in
preterms than in controls at delivery. In maternal erythrocytes, the sum of -3 PUFAs was
significantly (22%) lower in preterms than in controls at delivery, although control
samples at 34 weeks of gestation were not different from preterms.
We found evidence of sustained -3 FA deficiency in mothers and babies who delivered
preterm. We noted elevated docosapentaenoic acid (22:5 -6, DPA) strongly suggestive
of dietary -3 fatty acid deficiency in preterm birth amniotic membranes (119% increase)
compared with controls at delivery. Preterm maternal erythrocyte membrane DPA was
950% higher than controls at delivery and 641% higher than controls at 34 weeks of
gestation. These increases in preterm maternal -6 DPA are strikingly large and support
the notion that a maternal diet high in -6 fatty acids and low in -3 fatty acids was
associated with preterm birth in this prospective study of non–fish-eating Colorado
women. Other observational studies are summarized in Table 2.
In Denmark, Olsen et al. (60, 61) have conducted the most extensive observational studies
focusing on -3 fatty acid consumption and gestational length and pregnancy
performance. Olsen et al. (61) conducted an observational study of 62 women in the Faroe
Islands and in 37 control women in Denmark. Faroe Island residents, who typically
consume large amount of -3-rich marine lipids, had significantly longer gestations and
gave birth to babies with significantly higher birth weights compared with women in
Denmark. For the women in Denmark, there was a significant positive relationship
between -3: -6 ratios of maternal erythrocytes and the length of gestation. A 20%
increase in erythrocyte -3: -6 ratio was associated with a significant 5.7-day increase in
pregnancy duration.
INTERVENTION STUDIES: FOTIP STUDY
Olsen and collaborators (5) recently published results of the Fish Oil Trials in Pregnancy
(FOTIP) study. This large European consortium study included four prophylactic trials of
232 women with prior preterm birth. Women were randomized to 2.7 gm/day of -3
LCPUFA (DHA/EPA) or an olive oil placebo, beginning at 20 weeks of gestation. Fish oil
supplements reduced risks of recurrent preterm birth from 33.3% to 21.3% (OR 0.54, 95%
CI 0.30–0.98). In the combined trial data, DHA/EPA supplement delayed spontaneous
delivery (P = .002). DHA/EPA supplement did not reduce risks of pregnancy-induced
hypertension or intrauterine growth restriction and did not reduce risks of prematurity in
twins. Other similar studies are summarized in Table 3. Previously in a large randomized
preliminary study, Olsen et al. (62) demonstrated a 4-day prolongation among pregnant
women consuming a fish-oil supplement (Pikasol) that provided 621 mg of DHA and 864
mg of EPA daily. Supplementation was commenced at the 30th week of gestation.
DHA ENHANCED FOODS
Enhanced foods are beginning to be evaluated as sources of DHA in pregnancy (63).
Borod and colleagues (63) conducted a small randomized, placebo-controlled, prospective
study using DHA-enhanced eggs (135 mg each egg) obtained from hens fed 1% DHA
from commercial microalgae sources. Fifty-three inner city women consumed either 4
eggs (group 1), 8 to 10 eggs (group 2), or DHA-enriched eggs (group 3) in the second half
of pregnancy. Regression analysis showed relationships between maternal DHA intake
and DHA in maternal and cord blood plasma and red blood cells. Consuming eggs in
group 1 provided about 16 mg of DHA per day, typical eggs in group 2 provided about 54
mg of DHA per day; in contrast, consuming the DHA-rich eggs provided pregnant women
200 mg of DHA per day. In this small study, high-DHA egg-fed mothers had fewer low
birth weight (0% vs. 13% group 1 and 26% group 2) and fewer preterm (6% vs. 25%
group 1 and 26% group 2) births and larger placentas (760 gm vs. 608 gm group 1 and
663 gm group 2) and fewer births delivered by cesarean.
POSSIBLE ADVERSE EFFECTS
Adverse effects in supplement studies seem limited to fish-oil dosing rather than
consumption of fish or DHA-enhanced eggs. Prolonged or difficult labor and excessive
bleeding times are observed in animals fed oils high in EPA and DHA (57). Importantly,
the study of pregnant women by Olsen et al. (62) receiving 2.7 gm fish oil per day (four
fish oil capsules providing 864 mg of EPA and 621 mg of DHA per day) did not show
increased rates of side effects during pregnancy, labor, or delivery. Olsen and colleagues
(62) reported a trend (P = .1) for increased maternal blood loss at birth for women
receiving fish oil (13.0% more than 500 ml) compared with those receiving olive oil
(8.8% more than 500 ml), or no oil supplementation (12.9% more than 500 ml). In typical
fish oils, EPA is the predominant -3 fatty acid. EPA is an inhibitor of platelet
aggregation because it is an effective substrate for cyclooxygenase and reduces TXA2
concentration (64). DHA is only a mild, indirect inhibitor of platelet aggregation (64).
Women taking fish oil report mild side effects such as belching and unpleasant taste more
often than those taking olive oil supplements (62). Women consuming fish or foods
enriched with DHA alone do not complain of eructation or unpleasant taste.
ADJUNCTIVE MECHANISMS BY WHICH EFAs INFLUENCE GESTATIONAL
LENGTH
As noted, possible mechanism(s) by which DHA and EFA sufficiency or supplementation
modify gestational length and other outcomes involve eicosanoid metabolism, but other
molecular mechanisms may also be involved, especially those involving cell signaling
systems.
Epidemiologic studies establishing reduced risks of cardiac death linked to -3 DHA and
EPA consumption in Eskimos have led to considerable progress in our understanding of
FA metabolism (64). Nair and co-workers (65) have reviewed extensively the DHAfocused animal experiments, epidemiological studies, and human intervention trials
regarding sudden cardiac death.
Mechanisms suggested for the DHA reduction of cardiac death include, direct effects on
membrane structure and fluidity through incorporation of fatty acids into membrane
phospholipids; direct effects of nonesterified fatty acids (perhaps released in myocytes
from phospholipid pools) on the myocardium; effects of these fatty acids on calcium
channels, and perhaps sodium and potassium channels; and incorporation into myocyte
phospholipid pools on the phosphatidylinositol (Ips) cell signaling system.
EFAs EXTINGUISH LABOR
Hypothesizing that -3 EFA metabolites may directly extinguish preterm labor
contractions, Baguma-Nibasheka et al. (68) and Ma et al. (69) infused a long-chain -3
fatty acid emulsion (20% DHA) in a sheep betamethasone-induced labor model. Two of
three infused ewes reverted from apparent labor to nonlabor—an effect never before
reported in glucocorticoid-induced labor in sheep. This novel study showed that LCPUFA
infusion suppressed uterine contractility by decreasing PGHS2 in RNA. The authors
suggested that LCPUFA administration decreased maternal plasma estradiol, which
promotes mRNA, PGHS2 and protein and thus, reduces prostaglandin production in
sheep.
PREECLAMPSIA, PIH, AND IUGR
There is biologic plausibility to the suggestion that LCPUFA may play roles in the
pathogenesis of preeclampsia, PIH, and IUGR, as well as in fetal and placental growth (2).
Prostacyclin is an -3-derived eicosanoid vasodilator and smooth muscle relaxer.
Conversely, -6-derived TX mediates vasoconstriction and coagulation. Sorenson (66)
has shown that fish oil (Pikasol) versus olive oil supplementation in pregnancy increased
thromboxane B2 and prostacyclin I3 (P < .001) in maternal blood while lowering
thromboxane B2 in fetal blood (P = .03). However, controlled supplementation trials do
not demonstrate reduction of clinical preeclampsia or IUGR (5, 67).
DHA STATUS IN PRETERM AND FULL-TERM INFANTS
Evidence of maternal and fetal EFA deficiencies (both -3 and -6) have been
documented in preterm birth (53). Crawford (53) observed a negative correlation between
the maternal serum phospholipid concentrations of Mead acid (20:3 -9), an indicator of
-6 deficiency, and low birth weight as well as low Apgar score 1 minute after birth in
neonates seeming normal. Levels of 22:5 -6, an indicator of -3 LCPUFA deficiency,
were also reported high in preterm neonates.
DHA is important for brain and retinal development and function. The DHA status of the
perinate is related to gestational age as well as maternal nutrition. Preterm infants are
deficient in DHA compared with full-term infants (25, 27). It is suggested that DHA
availability in children born preterm may be insufficient for optimal development of eye
and brain tissues (21). In full-term newborns, -3 fatty acid accretion rates in brain tissue
is reported to show a lag phase, suggesting that desaturation of parent EFAs may be
limited (25). This puts premature infants at an additional increased risk of DHA
deficiency because they suffer reduced time for intrauterine acquisition of DHA as well as
reduced newborn liver desaturase activity after birth.
Because of these concerns, it has been suggested that DHA supplementation may be
necessary for maximal neural development in preterm babies. Commercial formula
available in the U.S. for both preterm and term infants provides only LA and LnA;
whereas, breast milk can contain a range of fatty acids and chain elongation and
desaturation products, including gamma-linolenic acid (18:3 -6), dihomo-gammalinolenic acid (20:3 -6), AA, EPA, and DHA (28). DHA in erythrocyte membrane
phospholipids in both term and preterm infants is lower in formula-fed infants than in
breast-fed infants (28). Supplementation with DHA has been shown to increase membrane
phospholipid DHA and to improve visual function through retinal and occipital cortex
development (25, 29). Low-level supplementation with DHA (presumably balanced with
AA levels) improves growth in preterm infants (30).
In summary, two major perinatal factors contribute to DHA insufficiency in preterm
infants: 1) lack of DHA accretion during the last trimester of gestation, and 2) possibly
limited desaturase activity in the immature liver. Failure to furnish DHA-containing breast
milk may prolong and worsen DHA deficiency.
DHA AND OTHER OMEGA-3 FATTY ACIDS IN BREAST MILK
Boris, Jensen, Olsen, and colleagues (70) have shown that -3 supplementation in the
later half of pregnancy is associated with enhanced DHA and EPA concentrations in milk.
They also demonstrated that increased -3 EFA milk levels could be sustained in lactating
mothers who continued -3- enhanced food supplementation during lactation. Cherian
and Sim (71) demonstrated similar findings using DHA-enriched eggs.
DHA AND BRAIN AND RETINA DEVELOPMENT AND FUNCTIONING
Sufficient DHA maternal consumption during pregnancy and lactation is increasingly
considered important for perinatal and infant brain and retinal development and
functioning (21, 25, 26). DHA derived from transplacental transport, perinatal liver
production, lactation, and early infant feeding comprises 50% of brain myelin
phospholipid and 60% of retina phospholipid (21). Studies in the last decade demonstrate
that breast-fed or DHA-enhanced formula-fed children demonstrate improved eye
stimulus reaction times and other measures of central nervous systemic functioning
including tests of cognition and IQ (72–75).
Heightened -3 fatty acid consumption (fish or fish products) during pregnancy and
lactation has also been linked to reduced risks of cerebral palsy in a case-controlled study
of Greek mothers and children (76). Conversely, meat consumption was associated with
increased risks of cerebral palsy. The authors theorized that -3 eicosanoids offered
relative protection from periventricular leukomalacia (PVL) and prematurity.
DIABETES MELLITUS AND OMEGA-3 FATTY ACID CONSUMPTION IN
PREGNANCY
Information is accruing that -3 fatty acid sufficiency may play beneficial roles in the
prevention and treatment of diabetes mellitus. The suggestion that breast-feeding reduces
risks of insulin-dependent diabetes mellitus in children was first made in 1984 by BorchJohnson and Jonev (77). Breast-feeding has been shown to increase -3 LCPUFA content
within skeletal muscle and heightened insulin sensitivity (78). Devynck (79) subsequently
postulated that increased fluidity of cell membrane lipid bilayers associated with increased
-3 LCPUFA lipid content could explain decreased insulin resistance by allowing
increased exposure of insulin receptors. Alternatively, recent research shows that
increased dietary -3 FA consumption suppresses antigen processing and cytokine
production, which could mitigate immune destruction of islet cells (80, 81).
Case-control studies suggest that DHA sufficiency during pregnancy may be associated
with reduced diabetes mellitus in children and gestational diabetes in mothers. A large
population-based case-control study done by Stene and colleagues (82) evaluated cod liver
oil consumption during and after pregnancy along with multivitamin consumption in
Norwegian families with type 1 diabetes mellitus. Cod liver oil is traditionally consumed
among Norwegians primarily as a mean to supplement vitamin D consumption. Maternal
consumption of cod liver oil during pregnancy was associated with reduced risks of
childhood diabetes (OR 0.30, 95% CI, 0.12–0.75). Cod liver oil consumption during
infancy was not associated with reduced diabetes mellitus (OR 0.82, 95% CI, 0.70–2.16).
These observations suggest that -3 fatty acid and/or vitamin D supplement in pregnancy
is associated with reduced risk of early childhood diabetes mellitus. Wijendran and
colleagues (83) demonstrated reduced maternal blood DHA in women with gestational
diabetes. Olsen (9), Barker (84), and Sattar et al. (85) have postulated that in utero
LCPUFA insufficiency may herald cardiovascular disease in adult life.
OMEGA-3 FATTY ACID NUTRITION AND SUPPLEMENT SOURCES IN
PREGNANCY
Women who wish to enhance or supplement -3 fatty acid consumption during pregnancy
or lactation or in preparation for pregnancy have limited food choices. DHA and other
polyunsaturated long-chain fatty acid are most abundant in oily, dark-colored ocean fish,
including salmon, tuna, mackerel, and sardines. Shellfish and freshwater fish contain
fewer LCPUFAs. Some authorities suggest that pregnant women can eat up to three
servings a week of fish. Recent Environmental Protection Agency (EPA) warnings voice
concern about methyl mercury and polychlorinated biphenyls (PCBs) in pregnancy
(www.EPA.gov/OST/fishadvice). Several international organizations have also issued
similar warnings concerning fish consumption during pregnancy. Uncooked shellfish
should be avoided in pregnancy and lactation because of possible bacterial and viral
contamination. Local freshwater fish may contain lipid-soluble PCBs. Fish-oil
supplementation in doses of 4 gm/day (containing 2.4 gm of DHA/EPA) was used in all
the studies by Olsen et al. (5, 56, 60–62). Fish-oil supplements, theoretically, may contain
lipid-soluble methyl mercury (CH3Hg) as well as PCBs. Excess cod liver oil consumption,
theoretically, may mediate vitamin D teratogenicity (86–88). A viable nonfish option for
women who wish to avoid fish or for women who are vegetarians includes consumption
of microalgae produced by commercial fermentation processes. Oil produced from the
microalgae, Schizochytrium sp., contains up to 40% of total fatty acids as DHA. These
deep-ocean algae that are responsible for DHA in the ocean food chain are now grown
commercially (contamination free). These microalgae are now fed to food animals for
product enrichment or used to extract oils for dietary supplements. For example, hens fed
this marine microalgae will produce eggs containing 150 mg of DHA per egg. DHA from
microalgae also is used to fortify infant formula preparations in Europe and other
countries, but not in the United States. Recommended daily amounts of -3 fatty acids are
listed in Table 4. Women may choose to consume recommended daily amounts of -3
fatty acids not only during pregnancy or lactation, but also in preparation for pregnancy
and during interconceptional periods. Microalgae-derived sources for DHA are
appropriate for strict vegetarian women, as well as for women concerned about possible
mercury or PCB contamination.
Table 4. International organizations with established daily
recommended values for -3 fatty acids
CONCLUSION
We have reviewed evidence that -3 fatty acids, including DHA, play important roles in
pregnancy, parturition and lactation, as well as during perinatal and childhood
development. In evolutionary terms, -3 fatty acids, including DHA, were more
commonly consumed by our ancestors than by contemporary humans. Preindustrial diets
are estimated to have contained -6 and -3 fatty acids in ratios approximately 1:1.
Whereas in today’s western diet, consumption of -6 fatty acids exceeds consumption of
-3 fatty acids by 10 or 25:1.
Preterm birth continues to be the most common cause of perinatal mortality and morbidity
and excess costs. Of the many identified causes of preterm parturition, abnormal or
insufficient -3 fatty acids nutrition may play primary or intermediary roles by adversely
affecting prostaglandin and other eicosanoid metabolism. So called “complex diseases,”
such as preterm birth caused by infection/inflammation, may be amenable to
comprehensive primary prevention, which can include nutritional counseling and
subsequent dietary remediation. Daily consumption of over 200 mg of DHA has been
recommended. Increased consumption of -3 EFAs and preformed DHA is accomplished
by eating fish with dark oily flesh and marine oils, as well as breast milk and other DHAenhanced foods, including DHA-enhanced eggs (23). Deep-ocean algae represent the most
important source of DHA in ocean ecology (23). These algae are now commercially
grown and are incorporated into human foods, including eggs, by feed-ing algae directly
to food animals or extracting the DHA oil from algae for the direct fortification of foods.
Maternal DHA consumption during pregnancy and lactation continues to be studied
intensively as a means to improve pregnancy outcomes as well as to optimize perinatal
brain and retinal development. We speculate that ensuring fatty acid dietary sufficiency
during pregnancy and lactation will prove to be an effective prevention strategy for
optimizing pregnancy and lactation outcomes. Additional benefits may be possible by
ensuring sufficiency before pregnancy and during interconceptional periods. Expanded
studies are underway around the world examining potential benefits of -3 nutrition in
optimizing pregnancy, and perinatal and lactational outcomes.
References
[Click here for reference links. (64 references linked.)]
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
Norwitz ER, Robinson JW, Challis JRG. The control of labor. N Engl J Med 1999; 341: 660–
666.
Mills JS. Prostacyclin and thromboxane change predicting clinical onset of preeclampsia: A
multicenter prospective study. JAMA 1999; 282: 356–362.
Uauy R, Periano P, Hoffman D et al. Role of essential fatty acids in the function of the
developing nervous sytem. Lipids 1996; 31 (Suppl): S167–S176.
Willatts P, Forsyth JS. The role of long-chain polyunsaturated fatty acids in infant cognitive
development. Prostaglandin Leukot Essent Fatty Acids 2000; 63: 95–100.
Olsen SF, Secher NJ, Tabor A et al. Randomized clinical trials of fish oil supplementation in
high risk pregnancies. Fish Oil Trials in Pregnancy (FOTIP) team. Br J Obstet Gynaecol
2000; 107: 382–395.
Wood NS, Marlow N, Costeloe K et al. Neurologic and developmental disability after extreme
preterm birth. N Engl J Med 2000; 343: 378–384.
Crawford MA. Placental delivery of arachidonic and docosahexaenoic acids: implications for
the lipid nutrition of premature infants. Am J Clin Nutr 2000; 71: 275S–284S.
Lubcheno LC, Delivoria-Papadopoulos M, Searls D. Long-term follow up studies of
prematurely born infants. II. Influence of birth weight and gestational age on sequelae. J
Pediatr 1972; 80: 509–512.
Olsen SF. Further on the association between retarded foetal growth and adult
cardiovascular disease. Could low intakes of marine diet be a common cause? J Clin
Epidemiol 1994; 4: 565–569.
Committee to Study the Prevention of Low Birth Weight, Division of Health Promotion and
Disease, Institute of Medicine. Preventing low birth weight. Washington DC: National
Academy Press, 1985.
Anon. Division of Vital Statistics, Colorado Department of Health and Environment, Denver
CO, 1997.
Simopoulos AP. Omega-3 fatty acids in health and disease and in growth and development.
Am J Clin Nutr 1991; 54: 438–463.
Sinclair HM. The relative importance of essential fatty acids of the linoleic and linolenic acid
families. Prog Lipid Res 1981; 20: 897–899.
Tinoco J, Babcock R., Hincenbergs I et al. Linoleic acid deficiency: Changes in fatty acid
pattern in female and male rats raised on -linolenic acid deficient diet for two generations.
Lipids 1978; 13: 6–17.
Bernert JT, Sprecher H. Studies to determine the role rates of chain elongation and
desaturation play in regulating the unsaturated fatty acid composition of rat liver lipids.
Biochim Biophys Acta 1975; 398: 354–363.
Hagve TA, Christophersen BO. Linolenic acid desaturation and chain elongation and rapid
turnover of phospholipid (n-3) fatty acids in isolated rat liver cells. Biochim Biophys Acta
1983; 753: 339–349.
Christophersen BO, Hagve TA, Norseth J. Studies on the regulation of arachidonic acid
synthesis in isolated liver cells. Biochim Biophys Acta 1982; 712: 305–314.
Carman MA, Beare-Rogers JL. Influence of diet on (n-3) and (n-6) fatty acids in monkey
erythrocytes. Lipids 1988; 23: 501–503.
Neuringer M, Connor WE, Van Petten C et al. Dietary omega-3 fatty acid deficiency and
visual loss in infant rhesus monkeys. J Clin Invest 1984; 73: 272–276.
20. Neuringer M, Connor WE, Lin DS et al. Biochemical and functional effects of prenatal and
postnatal w3 fatty acid deficiency on retina and brain in rhesus monkeys. Proc Natl Acad Sci
USA 1986; 83: 4021–4025.
21. Neuringer M, Anderson GJ, Connor WE. The essentiality of n-3 fatty acids for the
development and function of the retina and brain. Annu Rev Nutr 1988; 8: 517–541.
22. VanHouwelingen AC, Foreman-van Drongelen MMHP, Nicolini U et al. Essential fatty acid
status of fetal plasma phospholipids: Similar to postnatal values obtained at comparable
gestational age. Early Hum Dev 1996; 46: 141–152.
23. Kris-Etherton PM, Taylor DS, Yu-Poth S et al. Polyunsaturated fatty acids in the food chain
in the United States. Am J Clin Nutr 2000; 71: 179S–188S.
24. Hornstra G, VanHouwelingen AC, Simonis M et al. Fatty acid composition of umbilical
arteries and veins: Possible implications for fetal EFA-status. Lipids 1989; 24: 511–517.
25. Clandinin MT, Chappell JE, Leong S et al. Intrauterine fatty acid accretion rates in human
brain: Implications for fatty acid requirements. Early Hum Dev 1980; 4: 121–130.
26. Hoffman DR, Birch EE, Birch DG et al. Effects of supplementation with w3 long-chain
polyunsaturated fatty acids on retinal and cortical development in premature infants. Am J
Clin Nutr 1993; 57 (Suppl): 807S–812S.
27. Clandinin MT, Chappell JE, Leong S et al. Extrauterine fatty acid accretion in brain:
Implications for fatty acid requirements. Early Hum Dev 1980; 4: 131–138.
28. Carlson SE, Rhodes PG, Ferguson MG. Docosahexaenoic acid status of preterm infants at
birth and following feeding with human milk or formula. Am J Clin Nutr 1986; 44: 798–804.
29. Carlson SE, Werlman SH, Rhodes PG, et al. Visual acuity development in healthy preterm
infants: Effect of marine oil supplementation. Am J Clin Nutr 1993; 58: 35–42.
30. Uauy R, Hoffman DR, Birch EE et al. Safety and efficacy of omega-3 fatty acids in the
nutrition of very low birth weight infants: Soy oil and marine oil supplementation of formula.
J Pediatr 1994; 124: 612–620.
31. Broadhurst CL, Cunnane SC, Crawford MA. Rift Valley Lake fish and shellfish provided
brain specific nutrition in early Homo. Br J Nutrition 1998; 79: 3–21.
32. Al MDM, VanHouwelingen AC, Hornstra G. Long-chain polyunsaturated fatty acids,
pregnancy, and pregnancy outcome. Am J Clin Nutr 2000; 71: 285S–291S.
33. Arslan A, Znigg HH. Regulation of COX-2 gene expression in rat uterus in vivo and in utero.
Prostaglandins 1996; 52: 463–481.
34. Sadovsky Y, Nelson DM, Muglia LJ et al. Effective dimunition of amniotic prostaglandin
production by selective inhibitors of cyclooxygenase type 2. Am J Obstet Gynecol 2000; 182:
370–376.
35. Karim SM. The role of prostaglandins in human parturition. Proc R Soc Med 1971; 64: 10–
12.
36. Gravett MG. Causes of preterm delivery. Semin Perinat 1984; 8: 246–257.
37. O’Brien WF, Knuppel RA, Cohen GR. Plasma prostaglandin metabolite levels after use of
prostaglandin E2 gel for cervical ripening. Am J Obstet Gynecol 1986; 155: 1037–1040.
38. Dray F, Frydman R. Primary prostaglandins in amniotic fluid in pregnancy and spontaneous
labor. Am J Obstet Gynecol 1976; 126: 13–19.
39. Hibbard BM, Sharma SC, Fitzpatrick RJ, et al. Prostaglandin F 2a concentrations in amniotic
fluid in late pregnancy. J Obstet Gynaecol Br Commonw 1974; 81: 35–38.
40. Elliot WJ, McLaughlin LL, Block MH et al. Arachidonic acid metabolism by rabbit fetal
membranes of various gestational ages. Prostaglandins 1984; 27: 27–36.
41. Keirse MJ, Mitchell MD, Turnbull AC. Changes in prostaglandin F and 13,14-dihydro-15keto prostaglandin F concentrations in amniotic fluid at the onset of and during labour. Br J
Obstet Gynaecol 1977; 84: 743–746.
42. Hillier K, Calder AA, Embrey MP. Concentrations of prostaglandin F 2a in amniotic fluid and
plasma in spontaneous and induced labours. J Obstet Gynaecol Br Commonw 1974; 81: 257–
263.
43. Green K, Bygdeman M, Toppozada M et al. The role of prostaglandin F2a in human
parturition. Endogenous plasma levels of 15-keto-13,14-dihydro-prostaglandin F2a during
labour. Am J Obstet Gynecol 1974; 120: 25–31.
44. Lundstrom V. The Uterus. Prostaglandins and their inhibitors in clinical obstetrics and
gynaecology. In: Bygdeman M, Berger GS et al., eds. Lancaster: MTP Press, 1986, pp 59–81.
45. Bryant-Greenwood GD, Rees MCP, Turnbull AC. Immunohistochemical localization of
relaxin, prolactin and prostaglandin synthase in human amnion, chorion, and decidua. J
Endocrinol 1987; 114: 491–496.
46. Price TM, Kauma SW, Curry TE et al. Immunohistochemical localization of prostaglandin
endoperoxide synthase in human fetal membranes and decidual. Bio Reprod 1989; 41: 701–
705.
47. Bleasdale JE, Johnson JM. Prostaglandins and human parturition: Regulation of arachidonic
acid mobilization. Perinat Med 1984; 5: 151–191.
48. Edwin SS, Roomero RJ, Munoz H et al. 5-Hydroxy-eicosatetraenoic acid and human
parturition. Prostaglandins 1996; 51: 403–412.
49. Huszar G, Naftolin F. The myometrium and uterine cervix in normal and preterm labor. N
Engl J Med 1984; 311: 571–581.
50. Uldbjerg N, Ulmsten U, Ekman G. The ripening of the human uterine cervix in terms of
connective tissue biochemistry. Clin Obstet Gynecol 1983; 26: 14–26.
51. Lopez Bernal A, Hansell DJ, Canete Soler RC et al. Prostaglandins, chorioamnionitis, and
preterm labor. Br J Obstet Gynaecol 1987; 94: 1156–1158.
52. Lopez Bernal A, Hansell DJ, Khong TY et al. Prostaglandin E production by the fetal
membranes in unexplained preterm labour and preterm labour associated with
chorioamnionitis. Br J Obstet Gynaecol 1989; 96: 1133–1139.
53. Crawford MD, Doule W, Drury P et al. n-6 and n-3 fatty acids during early human
development. J Intern Med 1989; 225 (Suppl): S159–S169.
54. Mathias MM, Tsai A, Harris MA et al. Oral administration of menhaden oil alters gestation
in rates. Polyunsaturated fatty acids and eicosanoids. In: Lands WFM, ed. Champaign, IL:
American Oil Chemists’ Society (AOCS) Press, 1987, pp 508–512.
55. Leaver HA, Lytton FD, Dyson H et al. The effect of dietary w3 and w6 polyunsaturated fatty
acids on gestation, parturition and prostaglandin E2 in the intrauterine tissues and the
kidney. Prog Lipid Res 1986; 25: 143.
56. Olsen SF, Hansen HS, Jensen B et al. Longer gestation in rats fed diet supplemented with (n3) fatty acids that in rats fed diet supplemented with (n-6) fatty acids. Sixth International
Conference on Prostaglandins and Related Compounds, Florence, Italy, June 3–6, 1986. Adv
Prostaglandin Thromboxane Leukot Res 1987; 17B: 89–93.
57. Harris MA, Reece MS, McGregor JA et al. Possible roles of maternal and perinatal longchain fatty acids in preterm birth. In: Huang Y-S, Sinclair AJ, eds. Lipids in Infant Nutrition.
Champaign, IL: American Oil Chemists’ Society (AOCS) Press, 1998, pp 1–18.
58. Reece MS, McGregor JA, Allen KGD et al. Prostaglandins in selected reproductive tissues in
preterm and full term gestations. Prostaglandin Leukot Essent Fatty Acids 1996; 55: 303–
307.
59. Reece MS, McGregor JA, Allen KGD et al. Maternal and perinatal long-chain fatty acids:
Possible roles in preterm birth. Am J Obstet Gynecol 1997; 176: 907–914.
60. Olsen SF, Hansen HS, Sorensen TI, Jensen B, Secher NJ, Sommer S, Knudsen LB. Intake of
marine fat, rich in (n-3) polyunsaturated fatty acids, may increase birthweight by prolonging
gestation. Lancet 1986; 2: 367–369.
61. Olsen SF, Hansen HS, Sommer S, Jensen B, Sorensen TIA, Secher NJ, Zachariassen P.
Gestational age in relation to marine n-3 fatty acids in maternal erythrocytes: A study in the
Faroe Islands and Denmark. Am J Obstet Gynecol 1991; 164: 1203–1209.
62. Olsen SF, Sorensen JD, Secher NJ, Hedegaard M, Henriksen TB, Hansen HS and Grant A.
Randomized controlled trial of effect of fish-oil supplementation on pregnancy duration.
Lancet 1992; 339: 1003–1007.
63. Borod E, Atkinson R, Barclay WR and Carlson SE. Effects of third trimester consumption of
eggs high in docosahexaenoic acid on docsocahexaenoic acid status and pregnancy. Lipids
1999; 34: S231.
64. Leaf A, Weber PL. Cardiovascular effects of n-3 fatty acids. N Engl J Med 1988; 318: 549–
557.
65. Nair SSD, Leitch JW, Falconer J et al. Prevention of cardiac arrhythmia by dietary (n-3)
polyunsaturated fatty acids and their mechanism of action. J Nutr 1997; 127: 383–393.
66. Sorenson JD. Effects of fish oil supplementation in the third trimester of pregnancy on
prostacyclin and thromboxane production. Am J Obstet Gynecol 1992; 168: 915–922.
67. Onwude JL. A randomized, double-blind, placebo-controlled trial of fish oil in high risk
pregnancy. Br J Obstet Gynaecol 1995; 102: 95–100.
68. Baguma-Nibasheka M, Brenna JT, Nathanielsz PW. Delay of preterm delivery in sheep by
omega-3 long-chain polyunsaturates. Biol Reprod 1999; 60: 698–701.
69. Ma XH, Wu WX, Brenna JT et al. Maternal administration of long-chain n-3
polyunsaturates to the pregnant ewe in late gestation results in specific inhibition of
prostaglandin in synthetase (PGHS)2, but not PGHS1 and oxytocin receptor in RNA in
myometrium during betamethasone induced labor. J Soc Gynecol Invest 2000; 7: 233–237.
70. Boris J, Jensen B, Olsen S et al. A randomized controlled trial of the effect of fish oil
supplement in late pregnancy and early lactation on the n-3 fatty acid content in human milk.
2001; In press.
71. Cherian G, Sim JS. Changes in the breast milk fatty acids and plasma lipids of nursing
mothers following consumption of n-3 polyunsaturated fatty acid enriched eggs. Nutrition
1996; 12: 8–12.
72. Lanting CI, Fidler V, Huisman M et al. Neurologic differences between 9-year-old children
fed breast milk or formula babies. Lancet 1994; 344: 1319–1322.
73. Willatts P, Forsyth JS, DiModugno MK et al. Effect of long-chain polyunsaturated fatty acids
in infant formula in problem solving at 10 months of age. Lancet 1998; 352: 688–691.
74. Jensen C, Fraley J, Kennard H. Effects of maternal docosahexaenoic acid (DHA)
supplemention on visual and neurodevelopmental function of breast-fed infants. J Pediatr
Gastroenterol Nutr 2000; 31 (Suppl): S136–S140.
75. Carlson SE, Werkman SH, Tolley EA. Effect of long-chain n-3 fatty acid supplementation on
visual acuity and growth of preterm infants with and without bronchopulmonary dysplasia.
Am J Clin Nutr 1996; 63: 687–697.
76. Petridou E, Koussouri M, Olsen J. Diet during pregnancy and the risk of cerebral palsy. Br J
Nutr 1998; 79: 407–412.
77. Borch-Johnson K, Jonev G. Relationship between breast-feeding and incidence rate of
insulin-dependent diabetes mellitus: A hypothesis. Lancet 1984; 11: 1083–1086.
78. Bauer LA, O’Connor J, Pan DA et al. The fatty acid composition of skeletal muscle
membrane phospholipid: Its relationship with the type of feeding and plasma glucose levels in
young children. Metabolism 1998; 47: 1-6–112.
79. Devynck MP. Do cell membrane dynamics participate in insulin resistance? Lancet 1995;
345: 336.
80. Hughes DA, Pinder AC. N-3 polyunsaturated fatty acids inhibit the antigen-presenting
function of human monocytes. Am J Clin Nutr 2000; 171 (Suppl): S357–S360.
81. Endroes S, Ghexbani R, Kelley VE. The effect of dietary supplementation with -3
polyunsaturated fatty acids on the synthesis of interleukin-1 and tumor necrosis factor by
mononuclear cells. N Engl J Med 1989; 320: 265–271.
82. Stene LV, Ulrickson J, Magnus P et al. Use of cod liver oil during pregnancy associated with
lower risk of type I diabetes in the offspring. Diabetologia 2000; 43: 1093–1098.
83. Wijendran V, Bondel RB, Couch SC et al. Maternal plasma phospholipid polyunsaturated
fatty acids in pregnancy with and without gestational diabetes mellitus: Relations with
maternal factors. Am J Nutr 1999; 70: 53–61.
84. Barker DJP. Fetal origins of coronary artery disease. BMJ 1995; 311: 171–174.
85. Sattar N, Berry C, Greer IA. Essential fatty acids in correlation to pregnancy complications
and fetal development. Br J Obstet Gynaecol 1998; 105: 1248–1255.
86. Rothman KI, Moore LL, Singer MR et al. Teratogenicity from high vitamin A intake. N Engl
J Med 1995; 333: 1369–1373.
87. Foreman-van Drongelan MMHD, Al MDM, VanHouwelingen AC et al. Comparison between
the essential fatty acid status of preterm and full term infants measured in umbilical vessel
walls. Early Hum Dev 1995; 42: 241–245.
88. Reddy S. The influence of maternal vegetarian diet on essential fatty acid status of the
newborn. Eur J Clin Nutr 1993; 48: 358–368.
Correspondence to: James A. McGregor, MDCM, 768 Bardin Drive, Durango, CO 81303. Email:
MC2@frontier.net.
Obstet Gynecol Surv 2001 May Part 2;56(5):S1-S13
Copyright © 2001 Lippincott Williams & Wilkins
All rights reserved