Non-Small Cell Lung Fact Sheet
advertisement

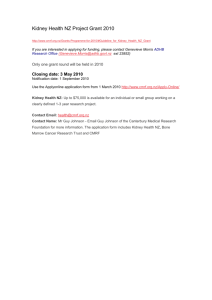
Kidney Cancer Fact Sheet What is Kidney Cancer? Kidney cancer is characterised by the uncontrolled growth of abnormal cells within the kidney or the immediately surrounding tissue. Renal cell cancer (RCC) is the most common form of kidney cancer, accounting for 85-90% of cases1 and can be further classified into four subtypes based on their appearance under a microscope. The most common subtype is ‘clear cell’ RCC which accounts for 80% of cases2. Other less common types include tumours of the papillary, chromophobe, or Bellini duct (collecting duct) cells3. Kidneys Tumour Renal pelvis Vena Cava (vein) Aorta (artery) Ureters Bladder Prevalence Kidney cancer represents approximately two percent of all cancers diagnosed worldwide4. According to recent global estimates, more than 200,000 patients were diagnosed with kidney cancer in 2002, and more than 100,000 people died from the disease4. The incidence of kidney cancer is considerably higher in developed countries than less developed countries4. Kidney cancer affects more men than women – approximately 62% of diagnoses and deaths occur in men4. Risk Factors The following factors may increase a person’s risk of developing kidney cancer: Age – the peak incidence of kidney cancer is among individuals aged between 50-70 years5. Smoking – kidney cancer is more common among smokers than among non-smokers6,7. Diet – there is some evidence that consumption of excessive quantities of meat, dairy 1 products, fat or protein may play a role in the development of kidney cancer8. Weight – individuals who are obese may have a more than two-fold increased risk of developing kidney cancer compared with those who are of normal weight9. Exposure to certain industrial chemicals such as arsenic and asbestos1,4. Diabetes, chronic kidney disease (and associated dialysis) or hypertension10. von Hippel-Lindau disease (VHL) – a rare inherited condition that leads to tumour or cyst formation throughout the body. Between 25-45% of VHL sufferers will develop RCC1. Symptoms Kidney cancer typically produces few, if any symptoms in the early stages and so unfortunately is often only detected when in advanced stages. When symptoms do arise they may include1: Blood in urine or abnormal urine colour. A persistent high temperature. Pain in the back, side or abdomen. Unintentional weight loss. Swelling of ankles or legs. Diagnosis There are a number of tests that may be used to diagnose kidney cancer that involve looking inside the kidneys. These include1,11: Intravenous urogram/pyelogram (IVU/IVP) – involves injecting a dye into a vein that passes through the kidneys so that any abnormalities of the urinary system can be detected by X-ray. Ultrasound – allows any growths inside the kidney to be seen. If initial tests show that kidney cancer is present, further examination may be necessary to ascertain the size and extent of cancer in the kidney and to see whether the disease has spread. These tests include Computed Tomography (CT) or Magnetic Resonance Imaging (MRI) scans and allow the cancer to be staged. Prognosis The outcome of treatment is often directly related to the staging of the cancer. If a diagnosis is made early in the disease, when the cancer has not spread, treatment can often be curative with surgical removal (nephrectomy) of part of, or the entire kidney. Unfortunately, because symptoms are rare in the early stages of kidney cancer, the majority of patients are diagnosed with advanced disease, when the prognosis is very poor: Approximately two thirds of patients with early stage kidney cancer that has not spread to other parts of the body can expect to live for more than 5 years after diagnosis12. In contrast, once metastasis has occurred and the cancer has spread into the lymph nodes, a patient has less than a 20% chance of surviving for longer than 5 years12. Once the cancer has spread to other distant organs patients usually have no greater than a 2 5% chance of surviving for longer than 5 years12. Treatment options Treatment options for patients with advanced kidney cancer are limited and therapy is usually employed with the view of controlling disease, improving the associated symptoms and ultimately increasing the quality of life for the patient. Treatment options available to patients with advanced disease include: Surgery – may slow the growth of kidney cancer but patients with advanced disease often do not benefit from surgery as the tumour has spread to too many places around the body. Chemotherapy, hormone therapy and radiation therapy – benefit a small number of patients but these therapies generally have very low efficacy against kidney cancer13. Cytokine therapy – the standard of care for patients with advanced kidney cancer. Immune mechanisms are thought to be important in the development of kidney tumours. Interferon (IFN)-alpha and interleukin are generally used to treat patients with advanced kidney cancer13. Novel treatment options Avastin® (bevacizumab) is an anti-angiogenic agent which blocks the activity of vascular endothelial growth factor (VEGF), a protein that stimulates the growth, survival, and repair of blood vessels. RCC is a highly vascularised tumour, meaning it has a lot of blood vessels14. By inhibiting angiogenesis, the growth of new blood vessels in and around a tumour, Avastin starves them of the blood supply that is critical to their growth and spread throughout the body, and through this the outcome for patients with RCC can be improved. Avastin, in combination with IFN, is clinically proven to extend survival in patients with advanced RCC. AVOREN The AVOREN study was a randomised, controlled, double-blind, phase III study that included 649 patients with advanced kidney cancer from 101 study sites across 18 countries. Study participants received treatment with either Avastin and IFN alpha-2a or placebo and IFN alpha-2a, the standard of care in patients with advanced kidney cancer. The results of the AVOREN trial showed that by adding Avastin to IFN: Progression free survival (PFS) was almost doubled from a median of 5.4 to 10.2 months Tumour response significantly increased from 12.8% with IFN alone to 31.4% when Avastin was added Dose-reduction of IFN did not appear to affect the efficacy of the combination with Avastin (based on PFS event free rates over time, as shown by a sub-group analysis) The study also showed a trend towards improved overall survival; however, these data are still 3 pending. No new or unexpected adverse events were observed. References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. Stewart BW and Kleihues P. World Cancer Report. IARC Press, Lyon, pp.183-7, 2003. Karumanchi, SA, et al. Renal cancer: molecular mechanisms and newer therapeutic options. Curr Opin Nephrol Hypertens, 2002; 11: 37-42. The National Comprehensive Cancer Network Practice Guidelines in Oncology – v1.2008. Kidney Cancer. September 2007. Parkin DM, Bray F, Ferlay J and Pisani P. Global cancer statistics 2002. CA Cancer J Clin, 2005; 55: 74-108. Board, et al. Anti-angiogenic therapy in the treatment of advanced renal cell cancer (2007). Cancer Treat Rev, 2007; 33: 1-8. Yuan, J-M et al. Tobacco use in relation to renal cell carcinoma. Cancer Epidemiol Biomarkers Prev, 1998; 7: 429-33. World Health Organization. IARC Monogr Eval Carcinog Risks Hum. Volume 83, 2002. Handa, K. and N. Kreiger. Diet patterns and the risk of renal cell carcinoma. Public Health Nutr, 2002; 6: 757-67. Yi Pan, et al. Obesity, High Energy Intake, Lack of Physical Activity, and the Risk of Kidney Cancer. Cancer Epidemiol Biomarkers Prev, 2006; 15: 2453-60. Chow, W.H., et al. Obesity, hypertension, and the risk of kidney cancer in men. N Engl J Med, 2000; 343: 1305-11 Cancerbackup. Further tests for kidney cancer (accessed 19 November 2007). http://www.cancerbackup.org.uk/Cancertype/Kidney/Causesdiagnosis/Furthertests. Medline Plus (accessed 8 November 2007) http://www.nlm.nih.gov/medlineplus/ency/article/000516.htm#Causes,%20incidence,%20and%20risk%20factors De Mulder, PHM. Targeted therapy in metastatic renal cell carcinoma. Ann Oncol, 2007; 18 (Supplement 9): ix98–ix102. Rini, BI. Vascular Endothelial Growth Factor Targeted Therapy in Renal Cell Carcinoma: Current Status and Future Directions. Clin Cancer Res 2007; 13: 1098-106. 4