polg in male infertiles
advertisement

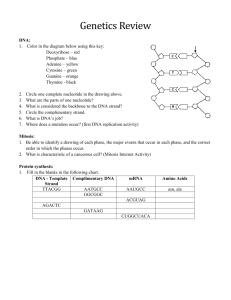
Supplement to Nature Genetics manuscript NG10059 Jacobs ON-LINE SUPPLEMENTARY INFORMATION A.T. Rovio et al., Mutations at the mitochondrial DNA polymerase (POLG) locus associated with male infertility ___________________________________________ NOTE THAT REFERENCES ARE NUMBERED AS IN THE MAIN TEXT, PLUS ADDITIONAL REFERENCES GIVEN HERE 1. Methods Patients, controls and ethical approval: Infertility for the purposes of this study is defined as lack of conception after at least 12 months of unprotected intercourse. Volunteers for the study, as authorized by the local ethical committee, were recruited from amongst infertile men attending a clinic in Oxford, and semen samples obtained by masturbation were stored frozen in liquid nitrogen for further study. Azoospermic individuals (approx. 20% of the total) were excluded, as were any for whom a clear, established etiology (hormonal, developmental, karyotypic or traumatic) could be found to account for their infertility. Semen was also collected from sperm donors, for use as fertile controls in the study. Seminal plasma was collected from similarly defined infertile males in Tampere, with ethical approval. Following ethical committee approval, 494 consecutive male patients attending the assisted conception (HARI) unit at the Rotunda Hospital, Dublin, for treatment with ICSI between July 1996 and June 1999 were studied. In all cases cytogenetic screening was carried out and 13 patients with an abnormal karyotype were excluded from the present study. The men ranged in age from 21 to 55 years (mean 35.3 years). All but 39 men provided at least one semen specimen, each after three days abstinence from sexual intercourse. Blood samples were provided by otherwise healthy volunteers amongst laboratory personnel and associates, who were not screened for fertility. Controls also included 270 unselected males from a previously studied birth cohort from England16. Semen analysis: Semen samples were analysed under the guidelines of the World Health Organisation17. Analyses carried out in Duesseldorf used strict criteria for evaluation of sperm morphology. DNA isolation: Blood DNA was isolated as described previously3. DNA was prepared from frozen sperm or seminal plasma as follows. An aliquot of 400 µl from each sample was micro-centrifuged at 13,000 gmax for 5 min and the pellets washed twice with PBS. Crude DNA was then extracted from the washed pellets using the proteinase K method described previously3. Prior to PCR, the DNA extracts were microcentrifuged for 15 s and 1 µl of clear lysate used as template. Other sperm and blood DNAs, prepared by similar or standard methods, were obtained from clinical sources in the various centres, along with clinical information and sperm analysis data, supplied anonymously. Oligonucleotides, PCR and fragment analysis: Fluorescent PCR analysis of POLG genotype was carried out as described previously3, using labelled primer mip-51 (Ref. 3), plus one downstream primer, either mip-31 (Ref. 3), mip-32 (Ref. 3) or mip-33 (CTCGTGCAGCCCTCTCGAGAGCAT), the latter generating a labelled PCR product of 176 bp from the common allele. Samples giving ambiguous or low signals were re-evaluated using a second downstream primer. Statistical analysis: Chi-squared testing was applied to determine whether the frequencies of different genotypes in infertile, control and fertile groups were significantly different. Posthoc analysis was based on standardized residuals. 2 2. Table A: POLG genotype of infertile men and control groups Phenotype Infertile malesc Total Homozygous numbera wild-typeb Heterozygousb ‘Homozygous’ mutantb 99 55 35 9 (56%) (35%) (9%) 0 80 18 (82%) (18%) 105 28 1 (78%) (21%) (1%) 196 70 4 (73%) (26%) (1%) 90 27 1 (76%) (23%) (1%) 391 125 6 (74.9%) (23.9%) (1.2%) 22.6% 1.7% Fertile malesc 98 Controls (mixed)d Controls (English, male)e 134 270 Controls (German, male) 118 All controls combinedf 522 Frequency expectationg 75.7% aExcluding a low proportion (approx. 15%) of infertile men from whom semen DNA failed to produce PCR products despite several repetitions of the analysis. We here define the ‘wild-type’ allele as the one carrying 10 CAG repeats. Heterozygotes b carry one copy of the wild-type and one other allele. ‘Homozygous’ mutants carry copies of either two different alleles (x/y) or a single (x/x) allele with a different number of repeats. 3 Percentages are quoted to the nearest whole number. cCombined data for 59 Finnish (6/59 homozygous mutant) and 40 English (3/40 homozygous mutant) infertile patients, compared with 65 Finnish and 33 English fertile males, P < 0.0001 (see statistical analysis in this supplement) dFinns plus ethnically mixed population, both genders, allele frequencies reported previously3. eMales fNote born in Hertfordshire 1920-1930, as studied previously16. that the 522 controls included in the population surveys were not scored for fertility, and are therefore likely to include some infertile males gHardy-Weinberg predictions in %, to 1 d.p., based on allele frequencies in the combined control groups (no selection based on fertility) of 0.87 for the wild-type allele and 0.13 for all mutant alleles combined. Observed genotypes in the control groups were close to these predictions. 3. Statistical analysis Two statistical tests were applied (Poisson analysis and chi-squared test). Using standard Poisson statistics (assuming a mean population frequency of the ‘homozygous mutant genotype’ of 1.7%), the probability of finding 9 or more such individuals out of a sample of 99 is 6 x 10–5. When fitting the model of homogeneous distributions using the chi-square statistic to the cross-tabulated data presented in Figure 1, the result was highly significant (P < 0.0001), i.e., the distributions were not homogeneous. The post-hoc analysis, based on the standardized residuals, which have a standardized normal distribution, showed that the reason for significance was the infertile group, where the homozygous wild-type class was significantly under-represented (z = –2.0) and the heterozygous and ‘homozygous mutant’ classes significantly over-represented (z = 2.1 and z = 4.8, respectively), when compared to 4 the control and the fertile groups. Between the last two groups there was no significant difference. 4. Additional clinical information for Table 1 Somewhat different criteria were applied in the collection of patients in the various centres participating in the study. The Scottish patients included a high proportion of azoospermic individuals and those with severe oligozoospermia (sperm concentration < 5 x 106/ml), whereas the German and Irish groups included many with only a mild abnormality of sperm concentration, motility and/or morphology. The Taiwanese group consisted of cases of ‘pure asthenozoospermia’, with sperm concentrations well into the normal range (generally >20 x 106/ml), whereas those from Australia included patients with various sperm abnormalities, plus 17 from whom testicular biopsies were taken for analysis but about whom no other clinical information was available. In the Table, data on Scottish and German patients (blood DNA) are combined because similar information was available for the two groups. Patients in this combined group with a known external cause for infertility were excluded from the analysis. Two additional mutant homozygotes were detected in the combined group, but are not included in the data shown: one Scottish individual for whom sperm data were unavailable, plus one German who also had Klinefelter syndrome. Data on the Irish patients (blood DNA) are presented separately, since information concerning other probable causes of infertility (affecting approximately 40% of the individuals studied) was not available on a case-by-case basis. As a result, the proportion of POLG mutants detected in this group is about half that seen in other groups of infertile men with comparable sperm counts. 5 5. Additional References 16. Poulton, J., Brown, M.S., Cooper, A., Marchington, D.R. & Phillips, D.I. Diabetologia 41, 5458 (1998) 17. World Health Organization. WHO laboratory manual for the examination of human semen and sperm-cervical mucus interaction. 4th ed., Cambridge University Press, Cambridge (1999). 6