Clinical Leadership Structure Policy

CLINICAL LEADERSHIP STRUCTURE AND CLINICAL
LEADERSHIP ROLES
Version 4.1
Name of responsible (ratifying) committee DDNC
Date ratified
Document Manager (job title)
09.09.11
Medical Workforce Manager
Date issued
Review date
Electronic location
Related Procedural Documents
Key Words (to aid with searching)
09.09.2011
01 December 2015
Management & Reward Policies
SPA schedule
Leadership/Clinical/Management
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 1 of 25
CONTENTS
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 2 of 25
1. INTRODUCTION
1.1 The Trust requires clinical leadership at every level from Trust Board to specialty teams. We should therefore expect to see many doctors, nurses, and staff within the Allied Health
Professions (hitherto collectively referred to as ‘practitioners’), represented in formal leadership positions. To enable the Trust to achieve its objectives it must attract and develop practitioners to formulate and implement policies and to provide overall leadership to the clinical community.
1.2 The establishment of Clinical Service Centres (CSCs) is deemed to be a fundamental component of Service Line Management (SLM) and is consistent with a recognised need to strengthen clinical involvement and leadership in business decision making and delivery at every level. The implementation of SLM is a central part of the Trust’s organisational development strategy. SLM aims to create a culture of devolved autonomy and accountability to clinicians and managers, in order to deliver improved service quality and patient experience. By identifying specialist areas and managing them as distinct operational ‘business units’ (CSCs),
SLM enables an organisation to understand its performance and organise its services in a way that benefits patients and improves overall efficiency. A key aspect of SLM is that it enables clinicians to take the lead on service development and delivery
1.3
Apart from the Medical Director’s role, which may statutorily only be filled by a doctor, all other clinical leadership roles could potentially be filled by any practitioner. The fundamental requirement for a clinical leadership role is that the individual has the widespread support of senior practitioners within the relevant specialty/ Clinical Service Centre (CSC) for taking up the role, and is able to do so whilst continuing with some
‘frontline’ clinical practice.
1.4 The ultimate responsibility for the overall performance of the Trust lies with the Executive
Management Team (Directors) and Trust Board. However, the delivery of clinical care depends upon the CSC and Specialty teams. In addition, specialist groups will advise the Executive
Management Team on Trust-wide issues that impact the organisation, as a whole. These comprise, for example:
Senior Management Team
Heads of Service Forum
Clinical Directors’ Forum
Clinical Governance Team
Transformation Board
Service Planning Team
Strategic Learning and Development Group
These groups all require clinical input and representation.
1.5 The Chief Executive chairs the Senior Management Team (SMT) and the membership comprises the Executive Directors; Associate Medical Directors; Chiefs of Service (CoS);
Associate Medical Directors; General Managers; CSC Lead Nurses, and key corporate leads.
This is the Trust’s senior team and oversees the workings of the specialist groups and the
CSCs, thus enabling the Executive Directors to account to the Trust Board.
1.6The purpose of the Heads of Service ’ Forum is to act as a source of advice to the Executive
Management Team (EMT)/SMT on broad clinical and managerial issues; approve statements of strategic direction and develop policies and procedures to support that direction; enable clarity of corporate goals by enhancing communication between EMT and Clinical Leaders, and establish a forum for incorporating wider specialty perspectives in the overall decision-making process. Membership is as follows:
Medical Director (Chair)
Associate Medical Directors
Chief Executive
Chiefs of Service
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 3 of 25
Executive Directors
Director of Postgraduate Medical and Dental Education
1.7 The Trust’s Clinical Leadership structure is detailed at Appendix 1 .
2. PURPOSE
2.1 The purpose of this document is threefold:
to define the clinical leadership roles that exist within the Trust, the reporting structure and the
way in which individuals will be appointed to these posts;
to describe the core dimensions associated with clinical leadership roles and their
development;
to detail the level of additional remuneration, or ‘Management Responsibility Payments’, over
and above basic salary, that will be awarded to those clinical staff who undertake specific
management responsibilities associated with clinical leadership.
2.2 The Trust requires that all senior staff having managerial responsibilities will acknowledge, and abide by, a Managers’ Code of Conduct, as amended from time to time. This Code of Conduct applies to management practice and is supplementary to all professional codes of conduct.
3. DEFINITIONS
Clinical Leadership Roles and Reporting Structure
3.1 The clinical leadership roles and reporting structure aim to effectively support the establishment and sustainability of Clinical Service Centres (CSCs) and to ensure clinicians take a leading role in continuous and innovative service development and successful service delivery. The principal focus is to directly support the integrated clinical, operational, governance and fi nancial performance activities associated with the Trust’s CSCs.
3.2 While specific duties and responsibilities are assigned to each of the clinical leadership roles, all posts are expected to promote the highest standards of leadership in four key areas, namely:
Service Leadership
deliver service-specific strategies and objectives;
identify and prioritise opportunities to improve the delivery of excellent patient care;
effectively utilise the key drivers of financial performance;
deploy all resources effectively and economically, and promote an intolerance of waste.
People/Personal Leadership
provide inspirational leadership for people across professional boundaries;
effectively communicate with staff;
assist others to perform to their best ability;
ensure all staff are regularly and effectively appraised, and receive essential skills training.
Quality Leadership
demonstrate outstanding patient commitment, and promote patient safety;
demonstrate and demand a commitment to quality of care and outcomes;
continuously aim for self-development.
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 4 of 25
Collaborative Leadership
always act within the overall interests of the Trust;
effectively communicate and collaborate with other leaders within the Trust;
effectively engage with external partners.
3.3 A summary of the key dimensions associated with each of the four CSC clinical leadership roles is provided below. The clinical leadership reporting structure is detailed at Appendix 1 .
Contractual Provisions relating to Clinical Leadership Posts
The special terms and conditions relating to a particular clinical leadership post will be detailed in an Addendum to the individual’s main Contract of Employment. These terms and conditions are summarised as follows:
Clinical leadership posts are designated as part time roles
The combined hours associated with an individual’s clinical and managerial responsibilities
shall constitute a whole time appointment, for both contractual and pension purposes
Dependent upon the size and complexity of the CSC, Consultant medical staff who undertake the role of Chief of Service will be allocated between 2 and 4 Programmed
Activities (PAs) per week; 1.5 to 3 PAs from DCC, and 0.5 to 1 PA from SPA. All other senior clinicians undertaking this role must negotiate time away from their clinical activities equivalent to between 8 – 16 hours per week. See Appendix 3 for role description of CoS
In the case of Consultant medical staff appointed to Clinical Director roles, to accommodate the demands of the associated additional managerial responsibilities, individuals undertaking such roles will be required to use one PA of their weekly Supporting Professional Activity
(SPA) time and half a PA of Direct Clinical Care (DCC) commitment to undertake the role. All other senior clinicians who undertake the role of clinical director will need to adjust the amount of time spent on ‘frontline’ clinical activities, accordingly, and discuss this with their manager. This equates to approximately 6 hours per week
Consultant medical staff undertaking the role of clinical lead are required to use a PA of their
SPA per week. All other senior clinical staff must negotiate the time, equivalent to approximately four hours per week , with their manager
Individuals may be required to work such hours as are reasonable for the full performance of their duties. This may, from time to time involve working evenings, nights, weekends, bank, public, statutory or customary holidays, but this shall not be the norm
The salary associated with an individual’s combined clinical and management roles will be their current whole time salary (including any allowances and/or supplements), plus the designated additional Management Responsibility Payment. This combined salary will be paid in arrears in twelve equal monthly installments Current levels of additional Management
Responsibility Payments are detailed, where applicable, alongside each designated role in
Appendices 2-5
Additional Management Responsibility Payments are classed as pensionable earnings, and are subject to annual cost of living increases associated with basic salary,
Individuals are not entitled to payment for any overtime worked, in connection with their additional management responsibilities
Three months notice must be given by either side to terminate any of these leadership roles
The Trust Remuneration Committee will review all additional Management Responsibility
Payments annually. Outside of the annual review, the value of additional payments may be re-considered where, for example, the key activities and/or objectives associated with a particular role have significantly been revised. There is no contractual entitlement to any increase in this additional element of salary, but individuals will be formally notified of any such change
Where military personnel have a clinical leadership role that is remunerated, their management payment will be suspended for their period of military deployment and reinstated when they resume their management responsibilities. Whatever leadership role is undertaken, a suitable replacement must be established at least one month before
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 5 of 25
deployment to ensure proper handover. The management responsibility payment, where applicable, will be transferred to the interim appointee
Sabbaticals / Return to Work
Clearly clinical leadership roles may require changes in clinical job descriptions, role type or job plans. In order to support clinical leaders returning to full time clinical practice, a return to work or sabbatical process may be negotiated with the General or Clinical Manager
The individual’s contracted hours, prior to taking on the management role, will be protected if and when they cease to undertake the management role.
An individual returning to full time clinical practice must have an agreed job plan ready for the re-commencement of their duties that is commensurate to that of their colleagues.
4. DUTIES AND RESPONSIBILITIES
Designated Trust Clinical Leadership Roles and Associated Additional Management
Responsibility Payments
The current designated Trust clinical leadership roles are listed below, together with details relating to the recruitment and appointment procedures, and additional reward associated with each.
The appropriateness, and level, of all additional Management Responsibility Payments will be determined by the Medical Director and HR Director, prior to endorsement by the Trust
Remuneration Committee.
Medical Director
The Medical Director is the formal professional lead for medical staff within the Trust. The
Medical Director is a full voting member of the Trust Board and needs to have the confidence of board colleagues, in terms of managerial competence and strategic awareness, and the confidence of medical colleagues, in terms of professional leadership and clinical credibility.
The role could easily require full time commitment, but would normally be fulfilled by a practicing clinician. Other clinical staff will therefore take support roles in specific areas, and the Medical Director role will comprise a maximum of 10 Programmed Activities (PAs) and a minimum of 5 PAs.
Accountability is to the Chief Executive.
Recruitment will be through formal advertisement, application to the Chief Executive and an interview, which follows the guidelines for appointment of Executive Directors. The consultant body will be extensively engaged through the Chiefs of Service and Clinical Directors and via the formal involvement (though not veto) of the Doctors and Dentists Consultative and
Negotiating Committee.
Appointment will be for four years, with an option to extend by two years, up to a maximum of
10 years (with yearly reviews by the Chief Executive, which will include an assessment of the requirements detailed in 3.1). A replacement will be appointed one year prior to the end of the incumbent’s term. The Trust may choose to offer a permanent appointment to candidates making a definite career move.
The additional Management Responsibility Payment will be determined by the Trust Board, via the Trust Remuneration Committee.
Associate Medical Director
The Medical Director will, with the Chief Executive, appoint Associate Medical Directors to support him/her in the fulfilment of the role. The posts will carry some specific responsibilities of their own (e.g. Clinical Performance; External Relations Lead; Junior Doctors Hours Lead)
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 6 of 25
but will also deputise for and support the Medical Director across the full range of his / her responsibilities.
Associate Medical Directors are members of the Hospital Management Team and Heads of
Service Forum
Accountability is to the Medical Director.
Recruitment will be through internal advertisement and applications to the Medical Director.
Appointment will be made by a panel chaired by the Medical Director and including the
Director of Nursing, plus one other Executive Director, assisted by a Senior HR Manager.
Appointment will be for a three-year period, with an option to renew, but with a maximum term of 10 years.
To accommodate their additional management responsibilities, Associate Medical Directors will need to reduce their clinical commitments. This will be by agreement with the Medical
Director.
Associate Medical Directors will receive an additional Management Responsibility Payment of
£20k subject to assessment of experience and knowledge, and the complexity and range of responsibility associated with the role. However, if the AMD also hold a post as Chief of
Service, the remuneration will remain at £20k for the combined role.
Chief of Service (CoS)
A Clinical Service Centre is led by a Chief of Service, working with a General Manager, Lead
Nurse, Finance Manager, Workforce Manager and Business Intelligence Manager. This team is responsible for the delivery of its clinical services, through its service centre structures
CoS are members of the Hospital Management Team and the Heads of Service Forum
CoS will directly report to the Chief Operating Officer
Professional accountability is to the Medical Director
Recruitment will be through internal advert and applications made to the Medical Director.
Appointments will be made by a panel, chaired by the Chief Operating Officer, and including the Medical Director and the Director of Workforce, or a nominated deputy
Appointment will be for three years, with an option to extend up to a maximum of 9 years, but with yearly reviews by the Chief Operating Officer. A successor will be chosen one year before the three-year term is completed, to allow for effective succession planning
Dependent upon the size and complexity of the CSC, the CoS role will be allocated between
2 and 4 PAs per week. 1.5 – 3 from DCC and 0.5 – 1 PA from SPA
Chiefs of Service will normally receive an additional Management Responsibility Payment of
£15k per annum
If the CoS role is combined with the AMD role, remuneration will be up to a maximum of £20k
Clinical Director
A Clinical Director is responsible for leading an individual specialty, or an aggregation of several small specialties, within a Clinical Service Centre.
All Clinical Directors are members of the Clinical Directors’ Forum which meets bimonthly
CDs will directly report to the Chief Of Service
Professional accountability is to the Medical Director
Recruitment will be through internal advert and applications sent to the CSC Chief of Service.
Appointment will be made by a panel consisting of the Medical Director, plus or minus the
Chief of Service
Appointment will be for three years, with an option to extend, but with yearly reviews and a maximum term of 9 years. A successor will be chosen one year before the three-year term is complete
In the case of Consultant medical staff appointed to Clinical Director roles, to accommodate the demands of the associated additional managerial responsibilities, individuals undertaking such roles will be required to use one (PA) of their weekly Supporting Professional Activity
(SPA) time and half a PA of Direct Clinical Care (DCC) commitment to undertake the role. All other senior clinicians who undertake the role of clinical director will need to adjust the amount of time spent on ‘frontline’ clinical activities, accordingly, and discuss this with their manager. This equates to approximately 6 hours per week
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 7 of 25
Clinical Directors will receive an additional Management Responsibility Payment of up to
£5,000 per annum
Additional Clinical Leadership Roles
The Trust may elect to appoint individuals to Additional Clinical Leadership roles that will take the Trust lead for the delivery of a particular service. Such appointments will be made by agreement between the Chief Executive and Medical Director
Lead Clinicians
Practitioners may be appointed to Lead Clinician roles in the following areas:
Child Protection
Cancer Care
Research and Development
Postgraduate Medical and Dental Education
Large scale complex project management role for a time limited period
This list is not necessarily exhaustive, and the Trust may elect to establish other such additional clinical leadership roles, as required. They are professionally accountable to the
Medical Director and managerially accountable to an identified senior manager or Director as specified within the job description.
Practitioners undertaking Lead Clinician roles will receive an additional Management
Responsibility Payment of up to £15,000 per annum, subject to assessment of experience and knowledge, and the complexity and range of responsibility associated with the role.
Additional PAs would be negotiated depending upon specialty and requirement of posts.
Specialty Clinical Leads
The purpose of the Specialty Clinical Lead is to provide advice about, and assistance to, the
Clinical Director of the Specialty / CSC and the Management Team in the delivery and development of a high quality service by their respective specialty within the constraints of the allocated resources
These practitioners will be professionally accountable to the Chief of Service and managerially accountable to the General Manager
Practitioners undertaking Specialty Clinical Lead roles may receive an additional
Management Responsibility Payment of up to £2k per annum, but this is at the discretion of the CoS and dependent of the needs of the CSC. The majority of Clinical Lead roles are unremunerated
Clinical Leads will be expected to use one PA of their SPA / per week within their job plan to undertake this role. Senior clinicians who are not medical consultants will be expected to negotiate the equivalent of 4 hours time per week to execute this role
Review of Payments
The value of all additional Management Responsibility Payments will be reviewed, annually, by the Trust Remuneration Committee.
5. TRAINING REQUIREMENTS
Personal Support, Development and Succession Planning
5.1 Staff who are appointed to positions within the clinical leadership structure will bring with them a range of skills and experience that will be applicable to their role. However, it is recognised that a degree of training and development support will be needed to help individuals carry out their responsibilities effectively. This also reflects the Trust’s on-going commitment to encourage and support individuals in their personal career development, whilst ensuring that succession planning is effective. Therefore, the Trust will work closely with clinical leaders to
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 8 of 25
ensure their training and development needs are identified and met, through the use of both internal and external provision.
5.2 The Trust will work with Chiefs of Service to identify potential future leaders and to provide appropriate leadership development opportunities. In time, all members of the Trust who assume clinical leadership positions should already have benefited from the modular Clinical
Leadership Programme provided by the Trust, which covers many aspects of personal leadership and effectiveness, within the context of team working. This Programme is also open to any Clinical Leader who wishes to attend. The following are identified as key areas where training and development support will need to be provided (other areas may also be identified through individual appraisals and performance reviews, and personal experience):
People Management
Managing performance
Conducting performance reviews and appraisals
Providing effective feedback
Conflict resolution
Financial Management
Accounting for non-accountants
Budgetary management and control
General
Project management
Change management
Strategic awareness
6. REVIEW
This policy will be reviewed annually by the DDNC.
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 9 of 25
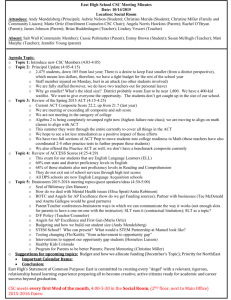
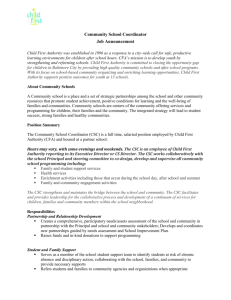
Appendix 1
Trust Clinical Leadership Structure
Chief Executive
Medical Director
Specialty
Clinical
Director(s) and/or
Specialty
Clinical
Leads(s)
Chief Operating Officer
CSC
Chief of Service
CSC
General Manager
Service Managers
Direct Reporting
Professional Accountability
Director of Nursing
CSC
Lead Nurse
CSC Support:
Workforce
Finance
Communications
Marketing
Business and
Performance
Intelligence
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 10 of 25
Appendix 2
Chief of Service Job Description
JOB DESCRIPTION
Job Title:
Status:
Reporting to:
Clinical Service Centre Chief of Service
Senior Clinician
Chief Operating Officer
Medical Director Professionally
Accountable to:
Clinical Service Centres
Clinical Service Centre s (CSCs) are the key units within which the Trust’s services are delivered to patients, with discrete resources used to meet a related set of patient needs.
Within the context of service-line management, the delivery of services via a portfolio of CSCs enables the devolution of ownership to the front line - where the capabilities, information, and patient relationships reside that enable the Trust to fulfill its overall business objectives.
Purpose, Scope and Authority
Reporting to the Chief Operating Officer, the purpose of the CSC Chief of Service role is to provide joint leadership and accountability for the integrated clinical, operational, and financial performance activities associated with the CSC. Specifically, the post holder is responsible for the effective and efficient deployment of medical workforce capacity and capability within the various specialties and departments that comprise the CSC.
Trust Key Dimensions
Portsmouth Hospitals NHS Trust delivers a full range of acute secondary services to a local population in excess of half a million, from a redeveloped hospital site providing world-class facilities. Other satellite units and clinics are provided within the region.
The Trust hosts the Wessex Renal and Transplant Unit, which serves a population of approximately two million, and provides a wide range of Cancer Services, both locally and beyond.
Annual turnover: c. £400 millions
Employees: c. 6,000 + full time equivalent, multi-disciplinary staff
Population served: c. 600,000
Clinical Service Centre Key Dimensions
Number of Service Lines:
Number of Sites from which services are based:
Total Operating Budget:
Total Staff Numbers (FTE):
(relating to named CSC)
(relating to named CSC)
(relating to named CSC)
(relating to named CSC)
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 11 of 25
Role Key Dimensions
Key Relationships and Partners Direct Reports
CSC Lead colleagues
Executive team
Medical and Clinical staff
Specialty Senior Nurses
External Agencies (e.g. GPs, PCTs, Social Services)
Specialty Clinical Directors
Time Commitment and Tenure
Dependent upon the size and complexity of the CSC, the CoS role will be allocated between 2 and 4 Programmed Activities (PAs) per week (1.5 to 3 PAs from DCC, and 0.5 to 1 PA from
SPA).
Normal tenure is three years, subject to satisfactory performance and annual review, with the option to renew for a further three years, thereafter, up to a maximum of 9 years.
Principal Duties and Responsibilities
Service Leadership
Deliver service-specific strategies and objectives:
In collaboration with CSC Lead colleagues, be responsible for developing, establishing and effectively communicating the overall strategic vision and key objectives for the CSC within the medical workforce.
Provide senior medical input for the development and implementation of an annual business plan that delivers the key business goals and objectives of the Unit.
Assist in developing and presenting business cases in support of the annual business plan.
Establish, implement and manage an effective process that ensures:
all senior medical staff undertake an annual review of their job plan (at team and individual level), such that medical workforce capacity and capability is fully aligned with activity and finance projections, and with the delivery of key business objectives;
Supporting Professional Activity (SPA) is appropriately planned, and allocated, such that it supports service delivery and business objectives, and meets the realistic expectations of individual clinicians;
outcomes associated with SPA are agreed and measured;
all senior medical staff undertake an annual appraisal, in accordance with Trust timescales.
Ensure that under-performance is recognised early, and appropriate and timely action is taken in response.
Identify and prioritise opportunities to improve the delivery of excellent patient care:
Regularly identify quantifiable opportunities for clinical staff to improve patient care and lead on their development and implementation.
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 12 of 25
Take a strategic view of opportunities, assisting with prioritising and deploying resources appropriately and effectively.
Effectively utilise the key drivers of financial performance:
Demonstrate and effectively communicate to the medical workforce a clear understanding of the key drivers of financial performance within the CSC, and identify the appropriate information required, in support.
Within a modern infrastructure and culture of transformational change, use the key drivers of financial performance to inform and support improvements in productivity within the medical workforce.
Promote organisational efficiency, demonstrate cost-effectiveness, and embed a culture of value for money and return on investment.
People/Personal Leadership
Provide inspirational leadership for people across professional boundaries:
Effectively mobilise the energy and commitment of the CSC clinical workforce.
Provide a clear vision and operating framework within which teams and individuals are able to succeed and flourish.
Actively encourage innovation and improvement from others.
Be an effective role model for others within the CSC, and beyond.
Assist others to perform to their best ability:
Provide leadership and absolute clarity of purpose for all direct reports.
Continuously challenge the status quo, and push for improved performance, at an individual level.
Take decisive and timely action to address areas of poor performance, under-achievement, and risk.
Assist in promoting and developing the culture of a learning organisation, that is fully committed to providing excellence in both health and customer care, and to providing continuous improvement.
CSC Shared Responsibilities
Collective responsibility with CSC General Manager, and CSC Clinical Lead colleagues:
Quality Leadership
Effectively prioritise patient safety:
Build and maintain outstanding working relationships with nursing teams and medical staff.
Ensure all complaints and SUIs are dealt with in a timely and thorough manner, and take appropriate preventative measures to mitigate recurrence.
Effectively utilise scorecard data and information to continuously improve patient safety.
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 13 of 25
Contribute to maintaining the highest standards of clinical and environmental hygiene to assure infection control standards and eliminate hospital-acquired infections.
Demonstrate commitment to quality of care and outcomes:
Drive innovation in clinical excellence.
Recognise and appropriately reward clinical excellence.
Utilise scorecard data and information provided on clinical performance to drive changes across service lines (at both team and individual levels).
Instigate improvements to clinical performance, on a continuous basis.
Proactively seek and utilise benchmarking data, and other internal/external resources, to improve clinical quality.
Demonstrate outstanding patient commitment:
Ensure the CSC is seen to place patients’ needs at the centre of its work.
Regularly engage with patients in the care of the Unit.
Take active responsibility for ensuring the patient experience is positive.
In the interests of delivering efficient patient pathways, consistent excellence in patient care, and the integration of services and promote effective pan-organisational working.
Continuously aim for self-development:
Regularly solicit feedback from others, and act upon that feedback.
Collaborative Leadership
Act within the overall interests of the Trust:
Fully engage with the strategy and key business objectives of the Trust, and ensure the strategy and objectives of the CSC are aligned with these.
Effectively balance the needs of the Unit with the needs of the Trust.
Understand the priorities of other CSCs and how these impact on own service lines.
Effectively communicate and collaborate with other leaders within the Trust:
Work effectively with other leaders to create a cohesive leadership team.
Create opportunities for service lines and CSCs to learn from one another.
Appropriately involve the executive team in CSC decisions.
Effectively engage with external partners:
Develop opportunities to work with partner organisations in the local economy to improve service levels and efficiency.
Initiate and regularly update communications with external partners.
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 14 of 25
Regularly solicit feedback from external partners, with respect to service line performance.
Organisational Expectations and Shared Corporate Responsibilities
In the course of their duties, and in the execution of their responsibilities, the post holder is expected to:
Significantly contribute to the successful overall performance of the Trust.
Act as an advocate for the Trust and its contribution to the Health Service arena, through the creation and maintenance of strong and effective partnerships and relationships with internal and external stakeholders.
Support and help develop the Trust culture of collaborative, flexible cross-team working and commitment to delivering high quality services and outcomes.
Set and maintain the highest personal and professional standards.
Manage own time to achieve results and develop and maintain effective working relationships with others.
Work with sensitivity and an understanding of the issues facing those working to deliver health services to the local and UK population.
Comply with the Corporate Governance structure, in keeping with the principles and standards set out by the Trust.
Maintain probity and manage Trust resources in a manner that represents appropriate use of public monies.
Be aware of and follow all Trust infection control guidelines and procedures relevant to their work, and participate in associated mandatory training and updates.
As a role model to other members of staff, follow consistently high standards of infection control practice, especially with reference to hand decontamination and adherence to the Trust dress code.
Maintain personal and professional development to meet the changing demands of the job, participate in appropriate training activities and encourage and support staff development and training.
Observe and promote the Trust’s policies and procedures, including those in respect of conduct, health and safety, and equality of opportunity.
Respect the confidentiality of all matters they may learn relating to their employment and other members of staff.
Respect the requirements of the Data Protection Act 1998.
Disclaimer: This job description does not purport to cover all aspects of the post holder’s duties, but is intended to be indicative of the main areas of responsibility.
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 15 of 25
Job Description Agreement
CSC Chief of Service (Post Holder):
Name (print): ………………………………………….
Signat ure: …………………………… Date: …….…
Medical Director:
Name (print): ………………………………………….
Signature: …………………………… Date: …….……
Chief Operating Officer:
Name (print): ………………………..……….
Signature: …………………………… Date: …….……
Annual Review Date:
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 16 of 25
Person Specification for Post of
Clinical Service Centre Chief of Service
Requirements
Qualifications
Essential:
Clinical qualification
Evidence of continuing professional development
Desirable:
MBA, or equivalent
Experience
Essential:
At least two years’ experience at senior clinical level
Leading and performance-managing teams and individuals
Desirable:
Proven successful track record in:
Supporting and sustaining transformational change within a complex organisation;
Translating business strategy into operational delivery;
Managing operating budgets and delivering financial surplus
.
Skills and Knowledge
Essential:
Ability to quickly establish effective working relationships and develop strong team working
Well developed interpersonal and facilitation skills, with ability to gain and maintain credibility with senior clinicians
Highly effective presentation skills and the ability to present well-reasoned and structured argument orally and in writing
Highly developed analytical skills
Proficiency in the use of ICT applications to support efficient work activity, including the analysis, interpretation and presentation of complex data
Ability to manage priorities in order to meet specific deadlines
Ability to hold direct and non direct reports to account
Desirable:
Detailed knowledge of Clinical Quality and Safety methodologies
Detailed knowledge of Clinical and Corporate Governance frameworks, legislation and best practice
Highly developed leadership skills
Detailed knowledge and understanding of clinical and corporate governance and risk management systems and processes
Measured By
Application, CV
Application, CV,
Assessment,
Interview
Application,
Assessment,
Interview
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 17 of 25
Personal Qualities
Tenacity: demonstrates high levels of self-belief, drive, enthusiasm and stamina to achieve goals and see things through
Ability to motivate, inspire and provide innovative solutions
Excellent judgment
Ability to achieve consistently good results in an inclusive and collaborative manner
Ability to work effectively in a complex and changing environment.
Ability to work under pressure to demanding timetables
Understands the need to deliver short-term priorities and achieve longterm goals (sense of balance)
High degree of political awareness
Displays innovative and lateral thinking
High degree of self-awareness
Ability to maintain confidence, at all times
High levels of personal integrity and loyalty
Ability to ‘broad scan’ to keep abreast of developments in the Health Care sector
Ability to deal with confidential issues in a professional and sensitive manner
Assessment,
Interview
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 18 of 25
Appendix 3
Clinical Leadership Roles – Clinical Director
The clinical leadership roles and reporting structure aim to effectively support the establishment and sustainability of Clinical Service Centres (CSCs) and to ensure clinicians take a leading role in continuous and innovative development and successful service delivery. The principal focus is to directly support the integrated clinical, operational, governance and financial performance associated with the Trust’s CSCs.
Purpose of the role
To provide direction, leadership and accountability in the overall management and performance of the specialty(s) within a Clinical Service Centre.
Accountability
Where the CD role is occupied by an individual who is a member of the medical workforce, they will be professionally accountable to the Director of Clinical Standards (Medical Director): otherwise, the post holder will be professionally accountable to their professional head of service.
The post holder will report to the CSC Chief of Service (CoS), to whom they are also accountable, with respect of their leadership role.
Responsibilities
The Clinical Director is to ensure;
The effective and safe delivery of patient services to the highest quality;
The highest standards of patient care and experience, and clinical outcomes;
High levels of staff motivation, contribution and performance;
The effective and efficient deployment of medical workforce capacity and capability;
Robust, effective and compliant governance arrangements are implemented and maintained;
Staff and other resources are secured, deployed and managed effectively;
Agreed financial performance objectives are met
On occasion, and within reason, CSC CDs will be expected to deputise for their CSC CoS.
All CSC CDs are members of the Clinical Director’s forum, and are expected to attend Forum meetings on a regular basis.
Recruitment
This will be through CSC internal advert and written applications to the CSC Chief of Service.
Appointment will be made by a panel consisting of the Medical Director plus or minus the Chief of Service.
Appointment
Appointment will be for three years, with an option to extend, but with yearly reviews and a maximum term of 9 years. A successor will be chosen 3 months prior to expiry of tenure.
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 19 of 25
The appointment can be terminated at any time by either the employer or the CD with three month’s notice on either side.
Time Allocation and Remuneration
In order to accommodate the demands of the leadership and management responsibilities associated with the role, sufficient time must be allocated within the post holder’s working week.
This allocation will be agreed between the post holder and their CoS, but, as a guide, it is anticipated that the equivalent of 1.5 PAs per week will be needed. At least one of these should be SPA.
However, where a doctor has less than 2.5 PAs of SPA allocated in their job plan or a CD is a non-medical appointment, time allocation must be locally negotiated by the CoS.
The additional remuneration associated with the role will be up to £5k per annum, depending on the needs of the CSC.
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 20 of 25
Appendix 4
Clinical Leadership Roles – Clinical Lead
The clinical leadership roles and reporting structure aim to effectively support the establishment and sustainability of Clinical Service Centres (CSCs) and to ensure clinicians take a leading role in continuous and innovative development and successful service delivery. The principal focus is to directly support the integrated clinical, operational, governance and financial performance associated with the Trust’s CSCs.
Purpose and Responsibilities of the Role
Working with the CSC Lead Nurse / Allied Health Professional (AHP) and Service Managers, the Specialty Clinical Lead will provide joint leadership for the clinical management and performance of the specialty for which they are responsible (accountability rests with the CSC
Clinical Director).
In particular, the post holder will;
Provide advice on service specific issues;
Be responsible for the effective and efficient deployment of medical workforce capacity and capability;
Be responsible for the setting of the clinical direction of the specialty in conjunction with the
CSC CD and CoS;
Be responsible for governance of the specialty
Accountability
Where the CL role is occupied by an individual who is a member of the medical workforce, they will be professionally accountable to the Medical Director: otherwise, the post holder will be professionally accountable to their professional head of service.
The post holder will report to the CSC Clinical Director, to whom they are also accountable, with respect of their leadership role.
Recruitment
This will be through CSC internal advert and written applications to the CSC Chief of Service.
Appointment will be made by a panel consisting of the CSC Chief of Service and either the
Lead Nurse or General Manager.
Appointment
Appointment will be for three years, with an option to extend, but with yearly reviews and a maximum term of 9 years. A successor will be chosen 3 months prior to expiry of tenure.
The appointment can be terminated at any time by either the employer or the CL with three month’s notice on either side.
Time Allocation and Remuneration
The time allocation will be agreed between the post holder and their CD or CoS, but, as a guide, it is expected that the equivalent of 1 PA per week will be needed which should be taken from the CL’s SPA allocation.
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 21 of 25
However, where a doctor has less than 2.5 PAs of SPA allocated in their job plan or a CL is a non-medical appointment, time allocation must be locally negotiated by the CoS.
There is typically no additional remuneration associated with the role, although some Chiefs of
Service may decide to reimburse Clinical Leads where they take on further responsibilities than those listed above.
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 22 of 25
Checklist for the Review and Ratification of Procedural Documents and
Consultation and Proposed Implementation Plan
To be completed by the author of the document and attached when the document is submitted for ratification: a blank template can be found on the Trust Intranet. Home page -> Policies -> Templates
CHECKLIST FOR REVIEW AND RATIFICATION
TITLE OF DOCUMENT BEING REVIEWED:
YES/NO
N/A
COMMENTS
1 Title
2
Is the title clear and unambiguous?
Will it enable easy searching/access/retrieval??
Is it clear whether the document is a policy, guideline, procedure, protocol or ICP?
Introduction
Yes
Yes
Yes
3
4
5
6
7
6
7
Are reasons for the development of the document clearly stated?
Content
Is there a standard front cover?
Is the document in the correct format?
Is the purpose of the document clear?
Is the scope clearly stated?
Does the scope include the paragraph relating to ability to comply, in the event of a infection outbreak, flu pandemic or any major incident?
Are there measurable standards or KPIs to support the monitoring of compliance with the effectiveness of the document?
Review Date
Is the review date identified?
Dissemination and Implementation
Is a completed proposed implementation plan attached?
Equality and Diversity
Is a completed Equality Impact Assessment attached?
Yes
Are the definitions clearly explained?
Are the roles and responsibilities clearly explained?
Does it fulfill the requirements of the relevant Risk Management
Standard? (see attached compliance statement)
Is it written in clear, unambiguous language?
Evidence Base
Yes
Yes
Yes
Yes
Is the type of evidence to support the document explicitly identified?
Are key references cited?
Yes
Yes
Are the references cited in full?
Are associated documents referenced?
Approval Route
Does the document identify which committee/group will approve it? Yes
Process to Monitor Compliance and Effectiveness
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes cont……
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 23 of 25
Checklist for the Review and Ratification of Procedural Documents and
Consultation and Proposed Implementation Plan
CONSULTATION AND PROPOSED IMPLEMENTATION PLAN
Date to ratification committee
Groups /committees / individuals involved in the development and consultation process
Is training required to support implementation?
If yes, outline plan to deliver training
Outline any additional activities to support implementation
No
DDNC
LNC
No n/a
Individual Approval
If, as the author, you are happy that the document complies with Trust policy, please sign below and send the document, with this paper, the Equality Impact Assessment and NHSLA checklist (if required) to the chair of the committee/group where it will be ratified. To aid distribution all documentation should be sent electronically wherever possible.
Name Nicola Heyworth Date May 2011
Signature
Committee / Group Approval
If the committee/group is happy to ratify this document, would the chair please sign below and send the policy together with this document, the Equality Impact Assessment, and NHSLA checklist (if required) and the relevant section of the minutes to the Trust Policies Officer. To aid distribution all documentation should be sent electronically wherever possible.
Name Date
Signature
If answers to any of the above questions is ‘no’, then please do not send it for ratification.
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 24 of 25
EQUALITY IMPACT ASSESSMENT
To be completed by the author of the document and attached when the document is submitted for ratification: a blank template can be found on the Trust Intranet. Home page -> Policies -> Templates
Title of document for assessment Clinical Leadership Structure Policy
Date of assessment May 2011
Job title of person responsible for assessment Medical Workforce Manager
Division/Service Corporate – HR & Workforce
Yes/No Comments
Does the document affect one group less or more favourably than another on the basis of:
Race
No
No
Gender (including transgender)
Religion or belief
Sexual orientation, including lesbian, gay and bisexual people
No
No
No
Age (for HR policies only)
Disability
– learning disabilities, physical disabilities, sensory impairment and mental health problems
No
No
Does this document affect an individual’s human rights?
If you have identified potential discrimination, are the exceptions valid, legal and/or justified?
No
If the answers to any of the above questions is ‘yes’ you will need to complete a full Equality Impact
Assessment (available from the Equality and Diversity website) or amend the policy such that only an disadvantage than can be justified is included. If you require any general advice please contact staff in the Equality and Diversity Department on 02392 288511
Clinical Leadership Structure Policy
Issued 09/09/2011 v4
Review date 01/12/2015
Page 25 of 25