Developmental features of adolescence
Week 32 LOs
1. Review key developmental features of adolescence and describe the common
consequences of departures from normal developmental process with particular
reference to:
Cognitive development
Emotional development
Social development
Adolescence:
Early (11-14),
Middle (14-17) and
Late (17-20)
Biological onset is identified as puberty: girls 11 (range 8-13) and boys 13 (10-14) with the
development of primary and secondary sexual characteristics.
Early adolescence: A period of rapid change in physical growth.
Development of secondary sexual characteristics, major emotional and social changes.
Adolescent developmental tasks: Include distancing from parents, peer bonding, physical
acceptance of changes
Mid-adolescence:
Most pubertal changes have completed, focus is on establishing a personal identity.
Developmental tasks/Experimentation with:
o Relationships
o Behavior
o Activities
Peers become more important.
Independence and emancipation become major themes.
Sexual identity and confidence with sexuality established in this stage.
Late adolescence:
Developmental tasks: A period of future planning, testing identity in the form of further
education, vocations, emotional relationships, focused interests.
Chronic illness may delay educational opportunities, restrict choices of activities and
vocations.
The struggle for meaning and an integrated sense of identity is a key adolescent task.
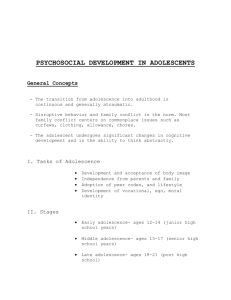
These have traditionally been divided into three domains:
EARLY
(11-14)
‘Am I Normal?’
Psychosocial Processes and Substages of Development
Emotional
Cognitive
Social
Adjustment to new
Concrete thinking
Increasing peer effect
body image
(acceptance)
MIDDLE
(15-17)
‘Who Am I?’
Emotional separation
from parents
Abstract thinking
verbal ability
school demands
LATE
(18-20)
‘Where am I going?’
Personal sense of
identity
Further development
of abstract thinking
Personal values
health risk
behaviour
Sexual peer interest
Early vocational plans
impulse control
Social autonomy
Vocational capability
Intimate relationships
Emotional Development:
This domain reflects the acceptance of the developing individual. This begins primitively with
the adjustment to new body image resulting from the initiation of puberty. Acceptance of new
body image generates the drive for emotional separation from parents which allows the
adolescent an individual sense of identity.
Consequences of deviation from normal developmental processes:
Parents (in proportion to their guilt) may increase control and protectiveness. Try to help
parents and child to separate care of illness from other contentions between them.
Illness and treatment can become the stage for adolescent rebellion, e.g., diabetes,
hemophilia, epilepsy.
Adolescents resent the necessity for dependence on adults.
Medical staff may treat the adolescent as he/she looks and inadvertently infantilize the
child. For example, in cystic fibrosis.
The normal bodily preoccupation and hypochrondriasis of adolescence are exaggerated by
illness.
Adolescents are often reluctant to participate in treatment that is disfiguring or emphasizes
deviation.
Extreme disability may actually make adjustment easier than moderate disability since it
removes the need to compete and allowances are made.
Early separation may lead to Separation anxiety causing agitation, irritability, tearfulness.
Unresponsive parents cause children to be more anxious and emotionally less mature.
Insecure attachment early in life causes low self-esteem, poor social relations, and
emotional vulnerability in adolescence or adulthood.
Cognitive Development:
Cognitive development is embracing the widening scope of intellectual activity with increased
awareness and capacity for insight. This is initiated with concrete thinking and progresses to
abstract thinking. Further development in this domain is the application and relevance of these
abstract values on life.
Consequences of deviation from normal developmental processes:
School absence and social isolation limit the development of cognitive functioning.
Late emancipation from parents can decrease the rate at which the person develops
capacity for insight.
Unresponsive parents or too early emancipation from parents may cause the person to
decide that cognitive development is not important.
Social Development:
The adolescent development is completed with the social domain. Early adolescents begin to
look away from their parents for acceptance. This is followed with increased risky behaviour (the
immortality of teenagers), peer sexual interest and early vocational plans. This domain
culminates in social autonomy, vocational capability and the beginning of intimate relationships.
Consequences of deviation from normal developmental processes:
Specific handicaps or disease may decrease the interactions with the wider community.
There is a tendency for medical personnel not to recognize sexuality in an ill adolescent and
to ignore or minimize the significance of flirting, crushes, need for privacy, etc.
School absence and social isolation limit peer group influence.
Late emancipation from parents can slow social development.
Hypochondriasis
A morbid concern about one's own health and exaggerated attention to any unusual bodily or
mental sensations; a delusion that one is suffering from some disease for which no physical
basis is evident.
2. Review key psychosocial adolescent milestones and describe how these may impact
on the assessment and management of the adolescent patient
Primary adolescent tasks are:
Achieving independence from parents: Initiated in early adolescence where teenagers
begin to look for acceptance away from the family unit, towards the peer group. This task is
finalised with the adolescent developing their individual image of self.
Adopting peer codes and lifestyles: With the detachment from parents, the adolescent
becomes more fixated on popularity with their peer group.
Reaching acceptance of ones own body image: This process of acceptance, initiated by
puberty, is the psychological development that results in the gradual acceptance of body
image.
Establishing sexual, vocational and moral identities: Through the above domains, the
adolescent should develop sexual, vocational and moral identities. This is obviously
influenced by the previously listed developmental tasks. E.g. A teenager not separated from
their parents will not be able to develop their own moral identity with their parents
continuing influence.
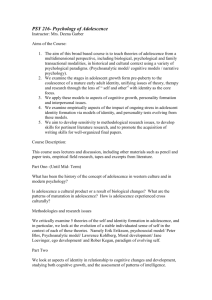
EARLY
(11-14)
‘Am I Normal?’
Psychosocial Processes and Substages of Development
Emotional
Cognitive
Social
Adjustment to new
Concrete thinking.
Increasing peer effect
body image.
(acceptance).
MIDDLE
(15-17)
‘Who Am I?’
Emotional separation
from parents.
Abstract thinking.
verbal ability.
school demands.
LATE
(18-20)
‘Where am I going?’
Personal sense of
identity.
Further development
of abstract thinking.
Personal values.
3. Describe normal pubertal development
See LO 1
4. Outline clinical Assessment of Pubertal Development
health risk
behaviour.
Sexual peer interest.
Early vocational plans.
impulse control.
Social autonomy.
Vocational capability.
Intimate
relationships.
What to look for:
Common variations of adolescent development (eg unequal breast size in girls,
gynaecomastia in boys)
Take note of physical changes and conditions related to pubertal growth and
development
Measure height, wt, BP
Use tanner charts
Allow the adolescent to indicate on the chart, stage of development (ie do not always
need to examine sensitive areas)
Provide feedback on your findings – be sensitive and straightforward in explaining what
findings mean
Check the adolescent’s understanding of your explanation and invite questions.
Reassure of normality where appropriate.
Tanner Scales for secondary sexual development
Puberty: (using Tanner scales)
Delayed if:
Males P1 > 15 yr G1 > 13.7 yr
Females P1 > 14 yr B1 > 13.7 yr
Precocious If:
Males G1 < 9.5 years
Females B2 or P2 < 8 years
P = pubic Hair
G = genital development
B = breasts.
Males
1. Preadolescent
2. Enlargement of testes and scrotum
3. Lengthening of penis
4. Increase in penis breadth, glans development and scrotal darkening
5. Adult: above plus pubic hair spread to medial surface of thighs
Females
Breasts
1. Preadolescent
2. breast bud (elevation of breasts and papilla)
3. enlargement of breast and areola 9no separation of contours)
4. areola and papilla project above breast level (secondary mound)
5. Adult: areola is recessed and papilla projects
Pubic hair
1. none
2. sparse growth, mainly over labia
3. darker, coarser, more curled hairs but sparse over the junction of the pubes
4. adult type but no hair spread to medial surface of thighs
5. adult: horizontal pattern and hair spread to medial thighs