Buteyko Breathing Program Registration Form
advertisement

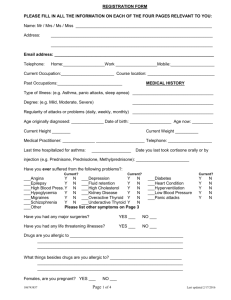
REGISTRATION FORM The information below is intended to assist the Educator to become familiar with your condition, your expectations of the program and your current medical symptoms. Although any information you complete is not intended to be shared with anyone but your Educator, you acknowledge that you provide it freely and voluntarily for its intended use. This program is not a medical therapy, nor should be used as a substitute for any medical treatment prescribed to you. If unsure, please consult your primary care physician. PLEASE FILL IN ALL THE INFORMATION ON EACH OF THE FOUR PAGES RELEVANT TO YOU: Name: Mr / Mrs / Ms / Miss ___________________________________________________________ Address: ______________________________________________________________________ ______________________________________________________________________ Email address: _____________________________________________________________________ Telephone: Home:__________________Work __________________Mobile:___________________ Current Occupation:_______________________ Course location: _____________________________ Past Occupations:____________________________ MEDICAL HISTORY Type of Illness: (e.g. Asthma, panic attacks, sleep apnea) ___________________________________ Degree: (e.g. Mild, Moderate, Severe) ___________________________________ Regularity of attacks or problems (daily, weekly, monthly) ___________________________________ Age originally diagnosed: ______________ Date of birth: __________________ Age now: _________ Current Height ________ Current Weight __________ Medical Practitioner: ______________ _____________________ Telephone: ___________________ Last time hospitalized for asthma: _________________ Date you last took cortisone orally or by injection (e.g. Prednisone, Prednisolone, Methylprednisone): _______________________ Have you ever suffered from the following problems?: Current? ___Angina Y ___Epilepsy Y ___High Blood Press. Y ___Hypoglycemia Y ___Migraines Y ___Schizophrenia Y ___Other N N N N N N Current? ___Depression ___Fluid retention ___High Cholesterol ___Kidney Disease ___Overactive Thyroid ___Underactive Thyroid Y Y Y Y Y Y N N N N N N Current? ___Diabetes ___Heart Condition ___Hyperventilation ___Low Blood Pressure ___Panic attacks Y Y Y Y Y N N N N N Please list other symptoms on Page 3 Have you had any major surgeries? YES ___ NO ___ Have you had any life threatening illnesses? YES ___ NO ___ Drugs are you allergic to _________________________________________________ _______________________________________________________________ _______________________________________________________________ What things besides drugs are you allergic to? _______________________________ _______________________________________________________________ _______________________________________________________________ Females, are you pregnant? YES ___ NO ___ COMPLETE THIS PAGE IF YOU HAVE ASTHMA, COPD NAME: _________________________ DATE: ____________ Please list all drugs you are currently taking, or have taken, in the past two months whether related to breathing difficulties or not. "Inhaler" Medication: Dosage Albuterol Alupent Atrovent Proair Number of puffs am pm Slow Release Relievers: Dosage Foradil Serevent Brovana Zyflo Number of puffs am pm Preventers: Inhaled Aerobid Asmanex Azmacort QVAR Flovent Intal Pulmicort Vanceril Number of puffs am pm Dosage Nebulizer Use: Dosage Dosage Number of puffs am pm Dosage Number of puffs am pm Dosage Number of tablets am pm Combivent Maxair Proventil Ventolin Xopenex Xolair Theophylline Symbicort Spiriva ADVAIR* Tablet Alvesco Medrol Prednisone Singulair Tilade Combined drugs: Symbicort ADVAIR* am pm Dosage am pm AccuNeb Xopenex Albuterol Atrovent Ventolin Duo Neb Nasal Spray Use: Dosage Astelin Rhinocort Nasocort Omnaris am pm Dosage am pm COMPLETE THIS PAGE WHETHER YOU HAVE ASTHMA OR NOT OTHER MEDICATION NOT RELATED TO ASTHMA: Medication Condition Dosage Do you or did you ever smoke? YES ___ If yes, how many packs per day?_____ AM PM Comments YES, have stopped ___ NO ___ If yes, how long? ____ If stopped, when did you stop smoking?___________ Please explain any surgeries: ____________________________________________________________________________ ____________________________________________________________________________ If you checked a life-threatening illness: How long ago was it? Sleep apnea/ snoring _____________________ Was it lung related? YES ___ NO ___ Have you had a sleep study? Yes ______ No ______ Was it kidney related? YES ___ NO ___ Date of test: ______________ Was it heart related? YES ___ NO ___ Results: __________________ Apneas noted: ____________ If you checked major surgeries: How long ago was it? _____________________ Oxygen saturation: _______% Was it lung related? YES ___ NO ___ CPAP pressure setting: ______ Was it kidney related? YES ___ NO ___ Are you using oxygen? Y What flow rate? N _______L/M Was it heart related? Do you have a blood disorder? YES ___ NO ___ YES ___ NO ___ If yes, which? ________________________ Have you been diagnosed with any chronic condition? YES ___ Are you experiencing chronic pain? YES ___ NO ___ If yes, which? __________ NO ___ If yes, where? ______________________ _______________________________________________________________________________________ COMPLETE THIS PAGE WHETHER YOU HAVE ASTHMA OR NOT SYMPTOMS SUFFERED PRIOR TO COMMENCING COURSE Please check your symptoms: 01( 02( 03( 04( 05( 06( 07( 08( 09( 10( 11( 12( 13( 14( 15( 16( 17( 18( 19( 20( 21( 22( 23( 24( 25( ) allergies ) anemia ) apathy ) asthma attacks ) bleeding veins ) breathing through mouth ) breathing without pause ) chest pains (not heart) ) constipation ) coughing ) deterioration of vision ) diarrhea ) dizziness ) dryness in mouth ) dryness of skin ) far sightedness ) fear of sultry air ) fear without reason ) flashes before eyes ) frequent deep breaths ) headaches ) impotence ) insomnia ) irritability ) lack of concentration Please list other symptoms 26( 27( 28( 29( 30( 31( 32( 33( 34( 35( 36( 37( 38( 39( 40( 41( 42( 43( 44( 45( 46( 47( 48( 49( 50( ) loss of feeling in limbs ) loss of hearing ) loss of libido ) loss of memory ) loss of smell ) mental fatigue ) muscle pains ) painful/irregular periods ) pains in heart region ) pains in bones ) physical exhaustion ) prone to colds and flu ) rhinitis ) ringing or buzzing in ears ) short temper ) shortness of breath ) shuddering in sleep ) snoring ) sudden chilling of limbs ) tightness around chest ) trembling and tic ) varicose veins ) weight gain ) weight loss ) other __________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ Please tell me about why you are attending the course and what you hope to gain from it: ____________________________________________________________________________ ____________________________________________________________________________ I understand that the Buteyko Breathing Reconditioning Program is a series of lectures and training. It does not constitute medical treatment. Furthermore, I, the undersigned, agree to only modify prescribed medication after consultation with a medical doctor. By signing below, I acknowledge that I have read and agree to the Terms of the Payment Agreement. I also agree and understand that by virtue of enrolling into this course, I will not become certified by the Buteyko Breathing Educators Association and should not use my knowledge to attempt to teach and educate others about this program, as one of the certified educators. Name: ___________________________________. Date: _________________ Signed: ______________________________________________ If client is under 18, a parent or guardian must sign this form