Supplementary Information (doc 180K)
advertisement
")
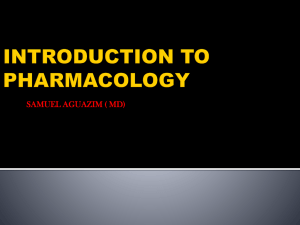
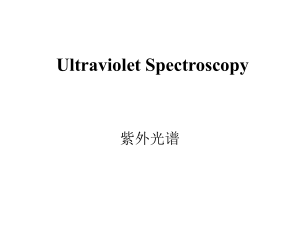
Supplementary Information A. Deriving the response curve for iron absorption from experimental data In this text we will describe how the functions for the control of iron (Fe) absorption and the erythropoiesis rate were parameterized based on experimental data from this study and recovery from blood donations. As discussed in the main text, the differential equations used for the model are: dx I absp(y) d y eryth(y) x e2 dt dy eryth(y) x d y e1 dt [1] [2] Where the variables x and y describe the amount of Fe bound to Hb and the amount of Fe in the rest of the body (“other body iron”, OBI), respectively. I is the daily Fe intake, d is the death rate ofRBCs, e2 is the time-averaged amount of Fe in Hb lost through menstruation and e1 represents other iron losses. absp(y) is the function describing the fraction of Fe absorbed based on Fe levels, and eryth(y) describes the rate of transfer of Fe from the OBI compartment to HB during erythropoiesis. The functions describing absp(y) and eryth(y), which will be described and justified in this text, are: a a0 amax amin , c a y 0 Ba ln max y c a a a 0 min 1 exp Ba h h0 hmax hmin , c h y 0 Bh ln max y c h h0 hmin 1 exp Bh absp(y) amin [3] eryth(y) hmin [4] Because iron excretion cannot be regulated, dietary iron (Fe) absorption is controlled in response to iron levels to ensure minimal changes in Hb levels with changing intake and other losses. Absorption is a percentage value that could theoretically vary between 0 and 100% (though in reality the range is much smaller). We have modeled this regulation by designing a steep response curve for the level of absorption based on Hb levels. This is a heuristic for the actual mechanisms involved. In reality, decreasing Fe input leads to decreased transferrin-bound Fe, which in turn leads to increased transferrin receptor levels, and signalling decreased hepcidin level and therefore increased Fe absorption. Direct modelling of these processes in a mouse system was done previously (Lao et al., 2006), which resulted in an inverse relationship between Fe levels and Fe absorption, with absorption increasing rapidly when Fe levels fall below normal levels, but levelling off at a minimum value of absorption for high Fe levels. Our heuristic response curve is very similar, except that we constrained Fe absorption to level off at a maximum value for low Fe levels, which we believe is more realistic. Supplementary Information It is necessary for the response curve for absorption versus Fe levels to be steep; that is, small decreases in Fe levels lead to large increases in absorption. Otherwise, it would not be possible to achieve the quick (~2 month) recovery after blood donation of ~10%, which is observed clinically. We can demonstrate this need for a sharp increase in absorption by considering the following calculation. Consider a “healthy” 55kg woman with a Hb of 13g.dL-1 (values justified in subsequent paragraph). With a plasma volume of 2.2 L (4% of total body mass), a hematocrit of 0.38 and using 1g Fe/ 285 g Hb, we get a total 1.62 g Fe in Hb (variable x). Since total body iron is the sum of iron in Hb and other body iron, it is given by T=x+y, and its rate of change is dT/dt=dx/dt + dy/dt =I absp(y)-(e1 + e2). When Hb decreases by about 10%, total body iron decreases by about 160 mg. With absorption staying at 3%, and a healthy intake of 55 mg.d-1 there would be no increase in Hb, since Fe balance is achieved. With a small increase in absorption, to say 4%, the rate of increase of total iron (I*absp(y)-(e1 + e2) ) would be 0.54 mg.d-1, so it would take around 300 days or 1 year for recovery. If absorption was 10% (half the maximum), then the rate of increase in iron is 3.8 mg.d-1, so it would take around 40 days for recovery. The latter is much closer to the 2 months that are observed. This means absorption must be quite high, even when Hb levels are close to recovering. This means the dose response curve must have a very sharp increase in absorption with small decreases in Hb levels This is consistent with earlier studies that have also shown that Fe absorption is extremely sensitive to changes in Fe status even in healthy non-anemic individuals (Kuhn et al 1968). The response curve for iron absorption versus iron levels was chosen to b a logistic function, constrained to have a minimum absorption of amin and a maximum of amax, and a value of a0 at a healthy Hb level of y0 (see Equation 3). The steepness of the response of Fe absorption to changes in Hb levels is given by the parameter Ba. Data on iron absorption percents and Hb levels was available for around 20 subjects, who all had a diet containing the same iron matrix. All subjects had Hb levels between 10 and 14. This population level data was used to derive a reasonable estimate for an individual’s dose-response curve for iron absorption. In the present study it appeared that there was a range of measurements at higher Hb levels where absorption was relatively low, and a range of lower Hb levels where there was much higher absorption, thought the variation between subjects was high. Since the trend in these data represents population level patterns it is not expected to be the same curve as a dose response curve for an individual. There is expected to be variation in the normal Hb set point between individuals, and so the curve may shift horizontally for different people. It may even have different maximums, minimums and slopes between individuals, though the shape of the curve should be very similar. For example, in the data it appears as though there is no change in average absorption for Hb levels between around 12 and 14. However, in an individual person there must be a constant decrease in absorption with increasing Hb. If this were not so, then if intake increased from the normal value and consequently iron levels rose, there would be no down-regulation of absorption and so Hb levels would continue to increase above healthy levels. This is not realistic. We interpreted this data as suggesting that people have Hb “set points”, where absorption is low, at Hb levels of between 12 and 14. Above this, we hypothesize that absorption slowly decreases to a minimal value, and below this, absorption sharply increases, and then increases less quickly at even lower Hb levels. Since between individuals’, “set points” are a bit different, and since the Supplementary Information slope of the absorption response at lower Hb levels is quite steep, this would result in the observed high level of inter-individual variation in absorption values for higher anemic Hb levels. We chose to use a “set point” Hb level of 13 g.dL-1 (y0), since this is generally a median observed value in healthy individuals, and set absorption to be 3% here (a0). We chose a minimum absorption fraction (amin) of 1% (the lowest frequently observed value, consistent with CITE) and a maximum (amax) of 20% (the highest value observed multiple times, consistent with CITE). With all these constraints specified, the slope of the response (Ba) was a free parameter that could be tuned to match the slope of the population level absorption patterns observed experimentally. To get an estimate for the slope, we measured the slope of the population level absorption data between Hb= 10.5 and 12 g/dL, and used this as the maximum slope of the response. Since the maximum slope of a curve defined by Equation 3 section is equal to (amaxamin)/(4*Ba), this was used to define the parameter Ba. The resulting function is shown in Figure 1 (a). It is important to note that these parameter values are specific for the diet considered in the absorption study, and that for other diets with different Fe bioavailability these values will have to be scaled. B. Deriving the response curve for the erythropoiesis rate Every day a fraction of OBI is moved to the Hb iron compartment during erythropoiesis. This fraction per day is called the erythropoiesis rate, and in steady state, the erythropoiesis rate is tuned so that RBC production balances with the destruction of RBCs. If the erythropoiesis rate remains constant, lower OBI levels will lead to decreased Hb production. Controlling iron absorption is one mechanism to maintain Hb levels, and another is control of the erythropoiesis rate. In response to decreased partial pressures of oxygen, the release of the erythropoietin is increased, which in turn increases the erythropoiesis rate. We have not modeled the intermediate steps, but have again used a heuristic logistic function to describe the relationship between Hb levels and the erythropoiesis rate (Equation 4). Explicit models of this regulatory pathway derive a more complicated function of this relationship (Mylrea and Abbrecht 1971), but it is approximately linear for much of the range and reaches a maximum at low Hb levels and a minimum at high Hb levels. We also modelled the increase in erythropoiesis as dependent on iron stores of the individual (OBI, x). It is necessary that this transfer depends on the OBI (x); otherwise a decrease in Fe levels would not result in lower Hb levels until Fe stores were completely depleted, which is unrealistic. Further, removal of 3.5 liters of blood by phlebotomy over 7 weeks in normal subjects resulted in increased erythropoiesis first and later led to a state of iron deficiency and decreased erythropoiesis (Finch et al 1950), while in those with low stores, erythropoiesis was severely reduced. The value at a healthy Hb level of 13 g/dL (y0) was taken as h0, and the constraints were a maximum value of 4*h0 and a minimum value of 0.7* h0 (Mylrea and Abbrecht 1971). In order to maintain Hb Fe and OBI levels of 1.62 g and 0.7 g in healthy individuals, the baseline Supplementary Information erythropoiesis rate (h0) was calculated as h0 = (d OBI + e1)/Fe(Hb) = (0.0055.d-1 1.62 g+ 0.00106 g.d-1 )/0.7 g = 0.014.d-1. The slope was tuned to match experimental results. See the section on parameters and function for the exact form of the logistic function used. The slope (Bh) was calibrated based on the time to recovery after a 10% blood loss. We simulated the time course of Hb levels for an otherwise healthy individual who donated 10% blood volume. The simulation started with the initial Hb concentration at 10% below steady state value, and simulating the return to steady state. During the entire simulation, Fe intake was constant at the ‘daily requirement’ value of 55 mg.day-1 defined in the Methods section (intake needed to achieve Fe balance in an inhibitory dietary matrix with a bioavailability of 3%). Even with the steep response for absorption derived from the data, given the maximum values of absorption, the recovery time (approximately 2 months) also requires a fewfold increase in erythropoiesis rates during recovery. We chose the minimum slope for the erythropoiesis curve (Bh) that resulted in at least 98% of healthy Hb values at 2 months following a 10% blood donation. The resulting curve is shown in Figure 1 (b). Figure 2 shows that with these final parameters, Hb levels return to close to normal (98% of normal) after approximately 2 months post donation, although OBI levels are still depleted at this time by about 5%, and take longer to return to normal values; in agreement with previous work (Franzone et al 1982). In response to the simulated blood donation and decreased Hb levels, absorption fraction and erythropoiesis rate are initially increased, but return to their baseline values as Hb levels recover. Supplementary Information Supplemental Figure 1: Logistic response curves for changes in (a) iron absorption fraction and (b) the erythropoiesis rate as a function of hemoglobin level. Supplemental Figure 2. Time course of (a) hemoglobin levels and other body iron levels and (b) iron absorption and erythropoiesis rate, after 10% depletion of hemoglobin. Supplementary Information References Finch S, Haskins D, Finch CA (1950). Iron metabolism; hematopoiesis following phlebotomy; iron as a limiting factor. J Clin Invest 29: 1078-1086. Franzone PC, Paganuzzi A, Stefanelli M (1982). A mathematical model of iron metabolism. J Math Biol 15: 173-201. Kuhn IN, Monsen ER, Cook JD, Finch CA (1968). Iron absorption in man. J Lab Clin Med 71: 715-721. Lao BJ, Kamei DT (2006). A compartmental model of iron regulation in the mouse. J Theor Biol 243: 542-554. Mylrea KC, Abbrecht PH (1971). Mathematical analysis and digital simulation of the control of erythropoiesis. J Theor Biol 33: 279-297.