The Impact of Early Intervention on Social/Emotional Development

1
The Impact of Early Intervention on
Social/Emotional Development in
Young Children Who Have Experienced
Trauma
Carol Noddings Eichinger, Lead Author
Edited by Elizabeth Wahl
“One crucial aspect of Part C is the requirement that early intervention program services develop an Individualized
Family Service Plan (IFSP). This plan, which is developed in collaboration with family members, guides the intervention process and contains information about the child, his or her family’s strengths and needs, and the services required to facilitate the child’s development and promote the family’s capacity to support the child’s progression. It acknowledges that families play an instrumental role in the optimal development of young children, and it focuses on the family rather than on the child. Providers are expected to enhance and preserve the caregiverchild relationship by coaching and supporting the primary caregivers rather that implementing one-onone activities with the child (Hauser-Cram & Howell, 2003; Wrightslaw, 2014).
In considering how to best serve children with developmental disabilities who have also experienced maltreatment, the National Symposium on Abuse and Neglect of Children with Disabilities emphasized the need for collaboration across all service sectors to enhance service effectiveness. As they noted, “there’s no one professional group that has all the wisdom associated with this problem” (National Symposium on Abuse and Neglect of Children with
Disabilities, 1995, p. 16). They highlighted the need for shared information and open communication across different service sectors, interdisciplinary teams that include experts on disabilities and child abuse, and integration of models from the varying service sectors.
Two types of legislation support interdisciplinary collaboration for children who have been maltreated: (a) the amendments to the Child Abuse Prevention and Treatment Act (CAPTA) of 2003 that are in the Keeping Children and Families Safe Act of 2003 (Pub. L. No. 108-136,117 Stat. 800, 2003, signed into Public Law 111-320 on
December 20, 2010); and (b) the IDEA 2004 reauthorization (Pub. L. No. 108-446, 118 Stat.2647, 2004, [Final regulations issued in September of 2011]). This legislation requires state early intervention and child welfare systems to develop coordinated procedures to guarantee that all children under the age of three who are involved in substantiated incidents of neglect or abuse are referred to Part C services (Casanueva, Cross & Ringeinsen, 2014;
Cohen, Cole & Szrom, 2011; Osofsky & Lieberman, 2011; Zero to Three Policy Center; 2006; Jones, 2009). According to Gilkerson et al. (2013) these two pieces of federal legislation command states to develop trauma-informed early intervention program services.”
(2014, C. Gosh Ippen, C.R. Noroña, & A.F. Lieberman , pp. 204-205)
Question: The Child Abuse Prevention and Treatment Act (CAPTA) requires coordinated procedures between state early intervention and child welfare systems when maltreatment is substantiated.
What capacity might early intervention offer children and families around social/emotional developmental concerns in early development, and how might better collaboration between various early childhood initiatives within a state enhance better outcomes for children?
Background
Neglect and toxic stress disrupt the developing brain architecture in young children (Lillas, Neurorelational Framework, 2015). Neurocognitive deficits have been reported in children who experienced early neglect, associated with prefrontal cortex white matter microstructure, which helps explain the cognitive deficits often associated with neglect. ( http://www.ncbi.nlm.nih.gov/pubmed/23480812
2013,Hanson JL, Adluru N, Chung MK, Alexander AL, Davidson RJ, Pollak SD.). Theodore Gaensbauer,
M.D. reminds us in his article Developmental and Therapeutic Aspects of Treating Infants and Toddlers
2
3
Who Have Witnessed Violence that trauma experienced early in life can have enduring developmental consequences. ( http://www.zerotothree.org/maltreatment/trauma/vol16-5p15.pdf
)
When there is a substantiated finding of child abuse or neglect, particularly with CAPTA referrals to early intervention programs, children are at risk for poor developmental outcomes. In 2013 in Wisconsin,
1512 children under the age of 3 were referred to Child Protective Services (CPS) due to maltreatment, as presented in the Wisconsin Child Abuse and Neglect Report disseminated by the Wisconsin
Department of Children and Families. http://dcf.wisconsin.gov/cwreview/reports/CAN/2013/2013CANReport.pdf
A report on child trends in Wisconsin reported that in 2013, just over 2,600 Wisconsin infants and toddlers were in foster care—a rate of 12.7 per 1,000 population, higher than in any of the previous 10 years. Rates for black and American Indian infants and toddlers were each five times as high as the 2013 rate for whites. Foster placements for these youngest children must be arranged, and monitored, with great care, so that they do not re-experience traumatic stress ( Wisconsin’s Infants & Toddlers , page 3). http://www.childtrends.org/wp-content/uploads/2015/04/2015-17WisconsinInfantsToddlers.pdf
In 2014, a Community of Practice (CoP) was formed of approximately 30 early interventionists from around the state of Wisconsin (see map, Appendix A) who were also graduates of the Infant, Early
Childhood and Family Mental Health Capstone Certificate Program at the University of Wisconsin-
Madison. The early intervention professionals represented the following disciplines, early childhood special education, physical therapy, social work, speech & language pathology, as well as state Part C leadership. Over the course of 2014-2015 the group considered the intersection of infant mental health practices with the IDEA Part C early intervention practices. Specific attention was paid to the assessment practices and intervention strategies for children who presented with social-emotional concerns and/or delays. Consideration of additional assessment practices was recommended within this group as a part of determination of eligibility for the early intervention when children present with social and emotional concerns. Possible assessment instruments to consider are listed in Appendix B, along with additional assessment resources.
Current Opportunities:
An Infant and Early Childhood Awareness & Action Day (Transforming Wisconsin’s Policies to Support
Infants, Young Children, and Families) was held on April 17, 2015 in Madison. The Infant/Toddler Policy
Workgroup involved in planning this event included members from the Wisconsin Alliance of Infant
Mental Health, Wisconsin Birth to 3 Program, YoungStar and other child care quality improvement initiatives, child welfare, home visiting, Wisconsin Head Start Association and Wisconsin’s Head Start
Collaboration Office, the Office of Children’s Mental Health and the Wisconsin Council on Children and
Families. Policy Priorities were crafted by this group, including specific attention to:
Effective Workforce
Universal Supports/Promotion
Secondary Supports/Intervention
Tertiary Supports/Treatment
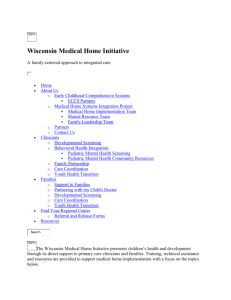
The Wisconsin Pyramid Model ( http://www.collaboratingpartners.com/social-emotional-competencesefel-pyramid.php
) offers a useful structure in consideration of the appropriate level of support as children enter into early intervention services. Though early intervention services might be considered to be at the top of the Pyramid as a Tier 3 Intensive Intervention, the Tier 1 Nurturing and Responsive
Relationship component is still the most critical. With many early intervention programs emphasizing the Primary Coach Approach to Teaming within Natural Environments the support of the relationship between the parent/caregiver and child becomes the focus for intervention. Concentration on the base of the pyramid around nurturing and responsive relationships becomes a foundation for assisting the children and families where dyadic relationship support is most integral aspect.
Red Tier 3 Intensive Interventions
Green Tier 2 Targeted Social-emotional Supports
Blue Tier 1 Nurturing and Responsive Relationships and High Quality Supportive
Environments
Yellow Foundation Effective Workforce
[Retrieved from: http://www.collaboratingpartners.com/documents/WISCONSIN_SEFEL_BROCHURE.pdf
April, 20015]
4
It would also be of interest to consider how early intervention programs focus on children presenting with a variety of social/emotional concerns, particularly those that might be influenced by traumatic events, might intersect with a state’s focus on trauma-informed care. One example is the Wisconsin
Department of Children (DCF) and Family’s Trauma Project. Some of the key project intentions around integrating trauma-specific interventions into a trauma-informed system of care include:
Introduce evidence-based trauma screening, assessment and treatment
Train parents & child welfare workers on childhood trauma
Create a more trauma-informed & responsive system of care
A number of counties have joined the Wisconsin Trauma Project during the last several years, including:
2012 –Kenosha, Barron, Burnett and St. Croix Tribe*
2013 –2014 La Crosse and Outagamie
2014 –2015 Grant, Lafayette, Crawford, Green, Iowa, Jackson, Polk, Rock, Walworth and Jefferson
An overview of that project description can be found at http://docs.legis.wisconsin.gov/raw/path/Committee%20Clerks%20Publications/2013-
14/LC%20Committees/LCC/Supporting%20Healthy%20Early%20Brain%20Development/Content/030%20-
%20September%209,%202014%20Meeting%2010:15%20a.m.%20412%20East/sep09presentation_dcf_trauma_project
5
Partnerships within communities around trauma care teams and multi -county mental health collaborations are important, as many counties begin to step into trauma-informed care practices across various systems that serve young children.
Partnership with Child Protective Services becomes especially important. In February of 2015, the
Center for IDEA Early Childhood Data Systems ( DaSy), worked with Alaska to publish a State Spotlight that came out of collaborative work between the CPS system and the early intervention system. It included important recommendations to improve timelines of CAPTA referrals and the capacity of early intervention providers to effectively serve children and families:
Child Welfare and Part C need to create a shared understanding of:
• which children and families should be referred and when;
• each system’s protocols and compliance requirements; and
• the responsibilities for both Child Welfare and Part C relative to the data transfer that enables Part C to locate eligible children and families.
To see the full report, access http://dasycenter.sri.com/downloads/DaSy_papers/AK_C_ChildWelfareDataSharing_FINAL_20150203_AccV4.pdf
Considerations from Implementation Science Research
As local early intervention programs consider children referred from CPS or other sources where social and emotional development is of primary concern, implementation science reminds us that special attention is needed to develop the organizational, leadership and competency required to consider additional knowledge and skills that will support both the assessment and intervention components.
For additional information related to implementation science, see The National Implementation
Research Network, FPG Child Development Institute, University of North Carolina, Chapel Hill
( http://nirn.fpg.unc.edu/ )
For this paper, the following questions are proposed related to Organizational, Leadership, and
Competency ‘drivers’ or influences that warrant both state system and local reflection.
Organizational
How do organizations assess the levels of knowledge, skill and attitudes of those involved?
What is the relationship with Child Protective Services (CPS) locally?
How are referrals made to the local early intervention program for children who have experienced substantiated abuse and neglect?
What information is provided? Does information include the CPS report that defines the experiences of the child and family that led to the removal of the child from the home, and the status of the child welfare case (custody, placement, TPR, foster/kinship care, etc)?
6
Is there continued communication between the CPS case worker and the early intervention program service coordinator and the primary coach serving the family?
Is there an endorsed Infant Mental Health Specialist (Level III) (http://test.wiaimh.org/) or a graduate with an infant mental health specialty, such as that provided by the
Wisconsin Infant, Early Childhood and Family Mental Health Capstone Certificate
Program, on the team?
How might the collaboration between CPS and the early intervention program be enhanced?
What training in social-emotional development and in trauma-informed care might be necessary for early interventionists, foster families, and biological families to understand the impact of trauma and the loss of family on the child? What is the early interventionist’s role in this? What is the CPS social worker’s role in this?
What might a study, such as the Wisconsin Adverse Childhood Experiences Study (ACES) offer to our understanding?
How might early intervention programs implement evaluation and assessment tools with sufficient sensitivity to detect delays in social-emotional development of young children?
How might documentation of atypical social-emotional development be addressed when an instrument does not indicate a % delay for the early intervention program eligibility and early intervention purposes?
Who are the other community partners who might assist the early intervention program team?
When might the early intervention program refer the family to a mental health clinician?
Are there local clinicians trained in infant mental health or Trauma-Informed
Child/Parent Psychotherapy (TI-CPP)?
Do local early intervention programs have access to funds for the Infant, Early Childhood and Family Mental Health Capstone Certificate or IMH Scholarships?
How might “missed visit” policies be re-evaluated to accommodate the impact trauma has and to allow the time it may take to build a relationship for families who need extra support to begin to trust?
How does the early intervention program address the potential of increased referrals, children found eligible, and the capacity to serve them if the child count increases substantially as a result of new practices and procedures?
How do local early intervention programs track their CAPTA referrals to monitor how many children are determined eligible for early intervention?
Could there be more regional support with Infant Mental Health consultants, similar to the Wisconsin Sound Beginnings CARES model in Wisconsin that is currently supporting early intervention program teams with individual consultation on children who are deaf and hard of hearing?
7
Does the state’s early intervention data reporting system, offer support with additional fields to allow clear ways to document these referrals and the access to services?
Leadership
How is the increased capacity of leaders supported?
Is the County Board aware of the link between trauma and developmental delays?
Does the supervisor of the local early intervention program have knowledge and/or familiarity with infant mental health research and practices?
Does the supervisor of the local early intervention program have a foundation, or knowledge of how to hold in mind the parallel process of supporting teamspractitioners-families-children? Does the supervisor value the ability to create a safe space within the agency for staff to reflect and process their work with families, and value the process as a mechanism for building competence when staff are experiencing complex emotions?
Does the supervisor of the local early intervention program endorse the relationshipbased work focusing on improvement of the dyad (family/child) interactions supporting the developmental progression of not only social and emotional well being, but language and cognitive development, adaptive skills, motor planning and sensory integration?
Does the supervisor of the local early intervention program support regular follow-up screening and/or assessment for CAPTA referrals that do not appear to meet eligibility criteria initially?
Competency
Is there an endorsed Infant Mental Health Specialist (Level III) (http://test.wiaimh.org/) or a graduate with an infant mental health specialty provided from a program such as the Wisconsin Infant, Early Childhood and Family Mental Health Capstone Certificate
Program on the local early intervention program team?
( http://www.psychiatry.wisc.edu/uwpInfant_about.html
)
Do early childhood special educators, speech pathologists, occupational therapists, physical therapists, and social workers have the knowledge and skill necessary to feel confident and competent in supporting the relationship/dyad around more nurturing connections/attachments that build the child’s capacity to use and understand language, to be curious and explore and learn?
Are staff trained to use and interpret tools that allow further screening and assessment of social-emotional development and also of parenting capacity and responsive relationships?
Who might be the Primary Coach, or provide support to the Primary Coach once eligibility is determined, to focus on the dyadic relationship?
8
Are staff comfortable with defining atypical development with description for the Early
Intervention Team Report or IFSP to document the concerns?
Is Reflective Supervision offered to the team to help recognize and manage the difficult emotions experienced by the early interventionists and uncertainty that some of these more complex cases entail?
Recommendations for Consideration:
1.
Predicate that social-emotional development including nurturing, responsive, safe relationships and environments is important and universal for ALL children’s optimal development and wellbeing and considered to be foundational for early intervention and lifelong learning.
2.
Ensure that all families in the early intervention program will have an opportunity to discuss parent-child relationships and their child’s social-emotional development as part of the intervention process. Information and support will be provided to the family in a way that respects and values the family’s culture and experiences.
3.
Additional assessment tools specific to social/emotional development and the dyadic relationship (see some samples in Appendix B) must be made available to the evaluation protocol when determining eligibility. A qualified team member skilled in the assessment of the social/emotional domain of development and/or infant mental health would be necessary to participate in the evaluation process.
4.
Discussion is recommended to explore the development of a protocol for use of additional tools both when a referral suggests concerns about social-emotional development prior to determination of eligibility and when a child is already receiving early intervention services but unique concerns about social-emotional development or parent-child relationships are observed by the family or practitioner.
5.
Intentional collaboration with the CPS system is essential. Some of the possibilities for exploration include:
Is there a potential to explore more intentional work with the biological family to enhance the competence and confidence of those parents if reunification is the goal?
How might the statewide early intervention programs work with CPS to promote therapeutic focus on building the relationship capacity between the biological parent and the child, rather than more discrete requirements such as parenting classes?
How might the statewide CPS programs and early intervention programs impact recidivism through trauma-informed care, examination of the inter-generational transmission of relationship difficulties, and attention to enhancing the dyadic relationship capacity between parent and child prior to reunification?
9
Should more attention be given in helping a child “make meaning” and have a more benevolent story of what has happened to the first family, when there is a termination of parental rights process?
What training in trauma-informed care, and in social-emotional development, might be necessary for foster families to understand the impact of both the trauma and the loss of family on the child? What is the early interventionist’s role in this? What is the CPS social worker’s role in this?
6.
Consideration is necessary on assessment of the quality of the dyadic relationship between parent and child, administered by qualified professionals (preferably with an infant mental health expertise). Some examples of tools to consider could include:
The Parent/Child Early Relational Assessment (PCERA) http://epm.sagepub.com/content/59/5/821.short
The Piccolo, for assessing quality of the parent-child interaction http://products.brookespublishing.com/PICCOLO-Provider-Starter-Kit-P679.aspx
7.
Guidance to local early intervention teams may need to be provided on beginning conversations with families about the use of tools that inform practitioners about potential challenges in behavior, attachment, or the relationship.
8.
In selection of appropriate tools for assessing social-emotional development:
When considering selection of screening and assessment tools: i.
Training required for use of the tool, and qualifications of examiners ii.
When a screening might suggest more comprehensive evaluation by a mental health practitioner.
When conducting developmental assessments with infants and young children, especially social-emotional development and functioning, this should be done in the context of the parent-child relationship.
Use of video replay of parent-child interaction to engage the parent in assessing their relationship with their child and looking together at the meaning of the child's behavior/delays or disability to the parent and for collaborative goal setting.
9.
In examining possible reasons children might demonstrate some concern about social-emotional development that could result in atypical development, a few possible phrases to consider are below:
Social-emotional development concerns impacting overall development resulting from….
Effects on child from history of trauma
10
Traumatic experiences leading to….(dysregulation, withdrawal, regression in communication or other skills, attachment concerns….etc. for examples)
Intense or prolonged periods of distress, depressed affect in caregiver/child (depression, apathy, withdrawal, sadness, constricted range of affect)
Child’s aggressive, negative, ignoring, or unresponsive behaviors due to challenges from reduced parental responsivity
Attachment concerns or lack of connectedness or turning towards for comfort between parent and child
Child reaction to loss of significant caregiver and separation anxiety
Child’s difficulties with self regulation and the ability to calm and recover from distress
Child’s difficulties related to sleep
Challenges to dyadic relationship with caregiver (negative attitude towards child, lack of positive affect in interactions, tone of voice in interactions with child) impacting child’s development
Child’s body-based and sensory regulation challenges connected with trauma history
Anxiety and anxious mood in both caregiver and child
Child’s ongoing Irritable/frustrated/angry mood
10.
Additional considerations include these questions:
How to best equip staff for holding relationships with great respect and empathy, and having the confidence and competence during conversations with families by… o Acknowledging that trauma has happened when a history of trauma is evident o Helping the family understand the event and full experience o Putting words to the “unspeakable” o Making meaning of the trauma with the child, with the parent, for ourselves o Assisting the child and family in finding safety and re-establishing the “protective shield”
How to manage vicarious trauma and understanding that o “Not talking about the elephant in the room”…… is more traumatic for both the family and for the practitioner o Knowledge of the trauma helps ensure trauma-informed care o Asking about a family’s trauma can help prevent the vicarious trauma for the practitioner
Early intervention programs have the opportunity to offer supports to children and families facing social/emotional developmental concerns. Enhanced collaboration between various early childhood initiatives within a state have the potential to enhance better outcomes for children. A number of
considerations are necessary for systemic improvements:
1.
Further integration of trauma-informed practices, infant mental health practices, and early intervention services.
2.
Additional training in assessment practices and intervention strategies for children who presented with social-emotional concerns and/or delays.
3.
More intentional teaming between CPS social workers and early intervention teams.
4.
Deeper supports to the dyadic relationship between the parent/caregiver and child.
5.
Coordination with a trauma-informed psychotherapist when a mental health referral is indicated, particularly one trained in Trauma Informed Child-Parent Psychotherapy (TI-CPP).
Additional Resources
Adverse Childhood Experiences in Wisconsin http://wichildrenstrustfund.org/files/WisconsinACEs.pdf
C. Gosh Ippen, C.R. Noroña, & A.F. Lieberman (2014) Clinical Considerations for Conducting Child-Parent
Psychotherapy with Young Children with Developmental Disabilities Who Have Experienced Trauma
Pragmatic Case Studies in Psychotherapy, http://pcsp.libraries.rutgers.edu
Volume 10, Module 3, Article 2, pp. 196-211, 11-07-14 [copyright by authors]
Godoy, L., Carter, A.S., Clark, R. (2008) Social-emotional development assessment. In M. Haith and J.
Benson (Eds.), Encyclopedia of Infant and Early Childhood Development. Oxford, UK: Elsevier Ltd.
Hanson JL, Adluru N, Chung MK, Alexander AL, Davidson RJ, Pollak SD. (2013) Early Neglect Is Associated
With Alterations in White Matter Integrity and Cognitive Functioning . Child Development. 84(5):1566-
78.
Hauser-Cram, P., & Howell, A. (2003). The development of young children with disabilities and the families: Implications for policies and programs (pp. 259-271). In M. Lerner, F. Jacobs & D. Wertlieb
(Eds.). Handbook of applied developmental science: Promoting positive child, adolescent, and family development through research, policies, and programs. Volume 1. Thousand Oaks: CA.
Howe, D. (2006). Disabled children, maltreatment, and attachment. British Journal of Social Work, 36,
743-760.Jones, L. (2009). Making hope a reality: Early Intervention for infants and toddler with disabilities. Washington, DC: Zero to Three Policy Center.
Indicators for Social-emotional Development in Early Childhood; A Guide for Local Stakeholders http://www.nccp.org/publications/pub_901.html
11
Slade, A. & Sadler, L.S. (2013). Minding the Baby: Complex trauma and home visiting. International
Journal of Birth and Parenting Education, 1, 50-53.
The National Child Traumatic Stress Network: http://www.nctsnet.org/sites/default/files/assets/pdfs/helping_young_children_heal_crisis.pdf http://www.nctsnet.org/sites/default/files/assets/pdfs/nctsn_earlychildhoodtrauma_08-2010final.pdf
Wrightslaw Special Education Law and Advocacy (2014). Early intervention (part C of IDEA). Retrieved from http://www.wrightslaw.com/info/ei.index.htm
ZERO TO THREE. (2005). Diagnostic classification of mental health and developmental disorders of infancy and early childhood (rev.). Washington, DC: Author.
Importance of assessing young child's development within the context of the parent-child relationship-
Clark, R., Paulson, A., & Conlin, S. (1993). Assessment of developmental status and parent-infant relationships: The therapeutic process of evaluation. In C.H. Zeanah (Ed.), Handbook of infant mental
health (pp. 191-209). New York: Guilford Press.
Parent-Child Relationship and Interaction assessments-
Clark, R., Tluczek, A., & Gallagher, K. (2004). Assessment of parent-child early relational disturbances. In
R. Del Carmen & A. Carter (Eds.), Handbook of Infant, Toddler, and Preschool Mental Health Assessment
(pp. 25-59). Oxford: Oxford University Press.
12
Appendix A
Wisconsin Infant Mental Health Fellows
In Early Intervention
Western Region
Douglas County
Kathleen Ronchi
Jackson County
Anita Leis
Lacrosse County
Tara Opelt
Susan Fossen
Washburn County
LeAnn Johnson
Southern Region
Columbia County
Bonnie Erickson
Sarah Kravick, LMFT
Dane County
Yvonne Hiebert
Lynn Phillips
Sara Tortomasi (also Rock)
Bridgette M. White
Sauk County
Cindy Schick
Waisman Center
Carol Noddings Eichinger
Elizabeth Wahl
13
Northeastern Region
Calument County
Kathleen Stock
Fond du Lac County
Heather Reilley
Marquette County
Jenny Rieson
Washara County
Sherri Nichols
Winnebago County
Kristen Baumann
Southeastern Region
Jefferson County
Elizabeth Boucher
Milwaukee County
Jennifer McBride
Maria Salcido
Sarah Wittmann
Christine Wittwer
Ozaukee
Cynthia Michalak
Walworth County
Sarah Greene
Washington County
Amy Burmeister
Michael Hoffman
Ashley Smith
Cassi Drury
Waukesha County
Amanda Smith
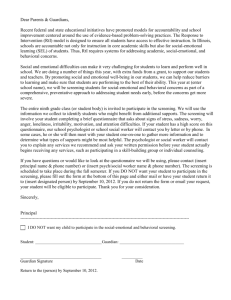
Appendix B
Title
Ages and
Stages
Questionnair e-Social-
Emotional
(ASQ-SE)
Greenspan
Social-
Emotional
Growth
Chart
Brief
Infant/Toddl er
Social-
Emotional
Assessment
(BITSEA)
Social-
Emotional
Assessment
Measure
(SEAM)
Vineland
Social-
Emotional
Early
Childhood
Scales
Achenbach:
Child
Behavior
Checklist
Screening or
Assessment
Screening
Brief Description
Self-regulation, compliance, communication, adaptive behaviors, autonomy, affect, and interaction with people
Screening and
Assessment
(when used with the
Bayley III)
Monitor the milestones of social-emotional development in infants and very young children. Based on Greenspan’s stages of social-emotional development
Screening
Assessment Social-emotional development and parenting strengths and needs
Assessment There are three scales—
Interpersonal Relationships,
Play and Leisure Time, and
Coping Skills—and the Social-
Emotional Composite
Devereux
Early
Childhood
Assessment for Infants and Toddlers
(DECA-I/T)
Screening and
Assessment
Based on a Resilience Model, provides information about child’s Initiative,
Attachment/Relationships, and
Self Regulation
Assessment
System
Assesses:
Problems, Disabilities,
Parent/Respondent Concerns ,
Best things about the Child
Age
Range
3 to 66 months
0-42 months
Areas assessed are problem and competence, including activity, anxiety, and emotionality.
12 to 36 months
2 to 66 months
Birth to 5 years, 11 months
Language
English and
Spanish
English
English,
Spanish,
French,
Hebrew, and Dutch
English and
Spanish
Parent report forms available in
English and
Spanish
Administered By Website
Parents; home visitors; other providers; requires a
6th grade reading level. Professionals score the questionnaires.
Parents; home visitors, other providers
Parent and Childcare
Provider forms
Early interventionists, early childhood teachers, Head Start and Early head Start
Professionals, home visitors, parent educators
Interviewer assisted parent report. Level B tool. http://www.brookesp
ublishing.com/resourc e-center/screeningandassessment/asq/asqse/ http://www.pearsoncli
nical.com/childhood/p roducts/100000214/gr eenspan-socialemotional-growthchart.html#tab-faq http://www.pearsoncli
nical.com/childhood/p roducts/100000150/br ief-infant-toddlersocial-emotionalassessmentbitsea.html
http://www.brookesp
ublishing.com/resourc e-center/screeningandassessment/seam/
Parent/Caregiver forms, scored by professional http://www.pearsoncli
nical.com/education/p roducts/100000283/vi neland-socialemotional-earlychildhood-scalesvineland-seec.html
https://www.kaplanco
.com/product/16139/ deca-i-t-kit
Infant form 1 to
18 months,
Toddler
English and
Spanish form 18 to 36 months
½-5 Years Multicultur al Option
Parent and/or caregiver completed. http://www.aseba.org
14
Temperamen t Atypical
Behavior
Scale (TABS)
Screening Areas screened are temperament, attention and activity, attachment and social behavior, neurobehavioral state, sleeping, play, vocal and oral behavior, senses and movement, and self stimulatory behavior.
11-71 months
English
Only
Problems
Disabilities
Parent/Respondent
Concerns
Best things about the
Child http://www.brookesp
ublishing.com/store/b ooks/bagnatotabs/index.htm
Individual
Growth and
Development
Indicators
(IGDIs)
Screening and
Assessment
Multi-Domain, Authentic
Assessment, includes scaled indicators for
Communication, Movement,
Social, Problem Solving, Parent-
Child Interaction
Birth to
36 months
English People trained and certified at various levels of administration and interpretation.
Other Resources for Social/Emotional Screening and Assessment:
http://products.brook
espublishing.com/Usin g-IGDIs-P231.aspx
Helping Young Children Succeed; Strategies to Promote Early Childhood Social and Emotional
Development
http://main.zerotothree.org/site/DocServer/helping_young_children_succeed_final.pdf?docID=1725
Developmental and Social-Emotional Screening Instruments for Use in Pediatric Primary Care for Infants and Young Children
http://www.childrenshealthfund.org/sites/default/files/dev-and-mental-health-primary-care-screeningtools.pdf
Developmental Screening and Assessment Instruments with an Emphasis on Social and
Emotional Development for Young Children Ages Birth through Five http://www.nectac.org/~pdfs/pubs/screening.pdf
15