Nurse Residency Letter of Recommendation
advertisement

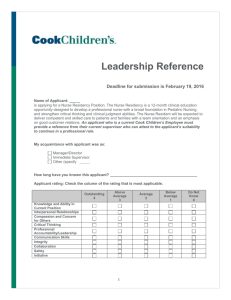
Letter of Recommendation The following statement indicates the applicant’s submitted signed response to the Letter of Recommendation Waiver. I waived my right to inspect the contents of this recommendation. I did not waive my right to inspect the contents of this recommendation. Deadline for submission is February 19, 2016 Name of Applicant: is applying for a Nurse Residency Position. The Nurse Residency is a 12-month clinical education opportunity designed to develop a professional nurse with a broad foundation in Pediatric Nursing, and strengthen critical thinking and clinical judgment abilities. The Nurse Resident will be expected to deliver competent and skilled care to patients and families with a team orientation and an emphasis on good customer relations. At least two letters of reference must be from persons who can attest to the applicant’s clinical knowledge and skill; one must be from a clinical faculty member knowledgeable about the candidate’s pediatric knowledge and clinical skill. If you cannot speak to the clinical knowledge and skill of this candidate, please do not complete a letter of recommendation. Please do not send via Google Docs. My acquaintance with applicant was as: Employer/Supervisor/Manager/Director Instructor/Professor School Advisor Other (specify) How long have you known this applicant? 1 Applicant rating: Check the column of the rating that is most applicable. Please be sure that you have selected one rating for each evaluation criteria. Incomplete letters of recommendation cannot be accepted. Please select one rating for each criteria Outstanding 4 Above Average 3 Average 2 Below Average 1 Do Not Know 0 1. Clinical Skill and Ability 2. Judgment and Common Sense 3. Compassion and Concern for Others 4. Critical Thinking 5. Professional Accountability/Leadership 6. Communication Skills 7. Integrity 8. Collaboration 9. Safety 10. Initiative What qualities or characteristics does the applicant have that would contribute to his/her success as a Nurse Resident? I would recommend this person for a nurse resident position. If no, please state concerns. Yes No Typed Name: ___________________________ Title: _______________________ (Submitting this form via your email address serves as an electronic signature.) Date: __________________________________ Daytime Phone Number: Please submit this form via e-mail to: (Please do not send via Google Docs) nurse.residency@cookchildrens.org 2 _______