")
Department of Human Services (DHS)
Division of Addiction Services (DAS)
Information Systems Management Unit (ISM)
Data Entry Form on Paper for
Norman G. Hoffmann, Ph.D. All rights reserved - 2001
No part of these materials may be adapted, photocopied or reproduced in any form. Such duplication is a violation
of copyright and constitutes unprofessional conduct.
LOCI-2R is to be used as an instrument for determination of Level of Care service for substance abuse patients
within NJSAMS Real-time Web Based Data System only.
NJSAMS Training and Demonstration Site
http://samsdev.rutgers.edu/samstraining/mainhome.htm
NJSAMS Real-time Data System (Do not use training or demo. purposes)
https://njsams.rutgers.edu/samsmain/mainhome.htm
If you have any questions please call customer service at:Phone: 609-292-3331; 609-943-5905; 609-292-1466 or Fax: 609-292-1045
Email: kyukyu.hlaing@dhs.state.nj.us or njsams.customerservice@dhs.state.nj.us
Updated: 01/01/2011
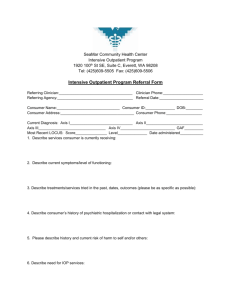
Name of the client: _____________________
Date of Evaluation: _____________________
Dependence
Substance
D1
D2
D3
D4
D5
Abuse
D6
D7
A1
A2
A3
A4
Abuse(A1..A4)
Alcohol
A1=Role Obligations
Marijuana-Hashish
A2=Hazardous Use
Cocaine
A3=Legal Problems
Opioids
A4=Social Problems
Amphetemine(or)
Methamphetamines
Sedatives/Hypnotic/
Anxiolytic
Dependence (D1..D7)
Hallucinogens
D1=Tolerance
PCP
D3=Excessive Use
Inhalants
D4=Desire/Attempts to stop
Poly/Unspecified
D5=Times pent using
Club Drugs
D6=Sacrificing activities to
use
Steroids
D7=Physical/Psychological
consequences
Tobacco
Other:specify
If the client is not diagnosed and the counselors/Clinicians want to see the client meets any criteria from
LOCI, check the box and click on “Continue LOCI” button.
1
DIMENSION 1: ACUTE INTOXICATION/WITHDRAWAL
PROCEED TO NEXT DIMENSION IF (a) OR (b):
____ a. There is no recent use; OR
____ b. No indication of acute intoxication or withdrawal problems.
LEVEL I-D – OUTPATIENT DETOXIFICATION
Status characterized by (a) and (b) and (c):
a. Minimal risk for severe withdrawal as evidenced by any of the following:
1. .CIWA-Ar < 8 after 8-24 hours of abstinence from alcohol; OR
2. Any recent use of sedative hypnotics was at therapeutic levels and not complicated by daily use of
a. alcohol or other drugs known to have a significant withdrawal syndrome; OR
3. withdrawing from therapeutic doses of sedative hypnotics, but no evidence of other active
a. alcohol/drug abuse or dependence, and withdrawal symptoms have responded to, or are likely to
b. respond to, substitute doses of sedative-hypnotics in the therapeutic range within 2 hours; OR
4. Injectable or smoked heroin has not been used daily for more than 2 weeks preceding admission or use
of opiates is near the therapeutically recommended level; OR
5. Gradual detoxification of opioid maintenance therapy, or treatment for mild withdrawal symptoms; OR
6. Stimulant withdrawal with some lethargy, agitation, paranoia, mild psychotic symptoms, or depression,
but impulse control is good; OR
7. Nicotine withdrawal requires nicotine replacement therapies or non-nicotine agents for symptomatic
treatment.
AND
b. Has withdrawal symptoms, but is at minimal risk for severe withdrawal syndrome and is likely to
complete detoxification and enter continued treatment or self-help recovery as evidence by (1) and
either(2) or (3):
1. Willing to accept recommendation for treatment; AND
2. Adequate understanding of ambulatory detox and has commitment to enter treatment; OR
3. Has adequate support services to ensure commitment to detox and ongoing treatment.
AND
c. Shows positive response to emotional support and comfort as evidenced by both (1) and (2):
1. Has decreased emotional symptoms by close of the initial treatment session; AND
2. Patient and/or support person have clear understanding of instructions for care and both the ability and
Resources to follow these instructions.
LEVEL II-D – AMBULATORY DETOXIFICATION WITH EXTENDED ON-SITE MONITORING
Status characterized by (a) and (b) and (c):
a. Moderate risk of severe withdrawal syndrome outside the program setting; AND
b. Free of severe physical and psychiatric complications and would safely respond to several hours of
monitoring, medication, and treatment as evidenced by any of the following:
1. CIWA-Ar score of 8 to 15; OR
2. Current withdrawal from sedative hypnotics without evidence of other active alcohol/drug abuse or
Dependence. Withdrawal symptoms, have responded to, or should respond to substitute doses of
Sedative-hypnotics in the therapeutic range within the observable hours of the program; OR
3. Used sedative-hypnotics in excess of therapeutic levels daily for at least 4 weeks, but risk of seizures,
hallucinations, or other complications during unobserved periods outside th e program assessed as
minimal. Close hourly monitoring is available if needed. There are no accompanying chronic mental or
physical disorders posing a danger during withdrawal; OR
4. Used sedative-hypnotics at or below therapeutic levels daily for at least 6 months, in combination with
daily alcohol use or regular use of another drug known to have its own dangerous withdrawal syndrome.
nonetheless, risk of seizures, hallucinations, dissociation or severe affective symptoms outside the program
2
is minimal; OR
5. Opiate abstinence syndrome( vital signs, physical discomfort, or craving) can be stabilized by the end of
each day’s monitoring , so that such symptoms can be managed at home with appropriate supervision; OR
6. Opiate withdrawal signs and symptoms are of such severity or instability that extended monitoring is
Required to determine the appropriate dosage; OR
7. Stimulant withdrawal with significant lethargy, agitation, paranoia, psychotic symptoms, or depression
Requiring extended outpatient monitoring to determine impulse control; OR
8. No additional biomedical problems. AND
c. Patient is likely to complete detoxification and enter continued treatment or self-help recovery as evidenced
by meeting(1) and either(2) or (3) or (4):
1. Patient or support persons clearly understand instructions for care and are able to follow instructions; AND
2. Has an adequate understanding of ambulatory detoxification and has expressed commitment or enter such
a program; OR
3. Has adequate support services to ensure commitment to completion of detoxification and ongoing
treatment or recovery; OR
4. Willing to accept a recommendation (e.g. attend outpatient sessions or self-help groups) for treatment once
Withdrawal has been managed.
LEVEL III.2-D - CLINICALLY MANAGED RESIDENTIAL DETOXIFICATION
Status characterized by both (a) and (b):
a. Not at risk for severe withdrawal, and moderate withdrawal is safely manageable at this level of surface as
evidenced by any of the following.
1. Intoxicated or is withdrawing from alcohol and CIWA-Ar less than 8 at admission, and monitoring is available to
assure that it remains below this level; OR
2. Opiate withdrawal signs and symptoms are distressing but do not require medication for reasonable withdrawal
discomfort, and patient is impulsive and lacks skills needed to prevent immediate continued drug use; OR
3. stimulant withdrawal – marked lethargy, hypersomnolence, paranoia or mild psychotic symptoms, and these are still
present beyond period of outpatient monitoring available in Level II-D
AND
b. Assessed as not requiring medication, but does require this level of service to complete detoxification and
enter into continued treatment or self-help recovery because of inadequate home supervision or support
structure as evidenced by meeting (1) or (2) or (3):
1. Lacks coping skills to deal with a recovery environment that is not supportive of detoxification and entry into
treatment; OR
2. Has a recent history of detoxification at less intensive levels of service marked by inability to complete
detoxification; OR
3. Recently has demonstrated an inability to complete detoxification at less intensive levels of service.
LEVEL III.7-D – MEDICALLY MONITORED INPATIENT DETOXIFICATION
Status characterized by either (a) or (b):
a. severe withdrawal risk that is manageable at this level of service as evidenced by any of the following:
1. CIWA-Ar score = 10 or greater by the end of the period of outpatient monitoring available in level II-D; OR
2. Daily use of sedative-hypnotics at more than therapeutic levels for more than 4 weeks and is unresponsive to
appropriate efforts to maintain dose at therapeutic levels; OR
3. daily use of sedatives above a therapeutic level for more than four weeks, plus daily alcohol use of regular use of
another drug known to pose a severe risk of withdrawal. Signs and symptoms of withdrawal are of moderate
severity, and cannot be stabilized by the end of the period of outpatient monitoring available at Level II-D; OR
4. Marked lethargy or hypersomnolence due to intoxication with alcohol or other drugs, and a history of severe
withdrawal, or the altered level of consciousness has not stabilized at the end of the period of outpatient monitoring
available at level II-D; OR
5. Daily use of injectable opiates for more than two weeks and a history of inability to complete withdrawal as an
outpatient or without medication at Level III.2-D; OR
6. Antagonist medication is to be used in withdrawal in a brief but intensive detoxification (as in multi-day
pharmacological induction onto naltrexone); OR
7. Marked lethargy, hypersomnolence, agitation, paranoia, depression or mild psychotic symptoms due to stimulant
withdrawal, and has poor impulse control and/or coping skills to prevent immediate continue drug use.
3
OR
__ b. This level of care is required to complete detoxification and enter into treatment or self-help recovery as evidenced
by any of
the following:
1. Requires medication and has a recent history of detoxification at a less intensive level of care, marked by inability to
complete detoxification. And enter into continuing addiction treatment, and continues to have insufficient skills or
supports to complete detoxification; OR
2. Has a recent history of detox at a less intensive level of care, marked by inability to complete detox. And enter into
continuing addiction treatment, and continues to have insufficient skills or supports to complete detox.; OR
3. Comorbid physical, emotional, behavioral or cognitive condition that increases clinical severity of the withdrawal and
complicates detox. Is manageable in a Level III.7-D setting.
LEVEL IV-D – MEDICALLY MANAGED INTENSIVE INPATIENT DETOXIFICATION.
Patient must meet (a) or (b);
a. Risk of severe withdrawal as evidence by any of the following:
1. Alcohol withdrawal and CIWA-Ar score is 10 or greater. The patient requires: monitoring more often than hourly;
intravenous medication or infusions; or close behavioral monitoring due to high levels of agitation, confusion or
extremes of vital signs; OR
2. Alcohol and sedative-hypnotic withdrawal with seizures, delirium tremens or severe, persistent hallucinations; OR
3. Daily sedative-hypnotic use at more than therapeutic levels for more than 4 weeks, and has accompanying acute
mental or physical disorder complicating withdrawal; OR
4. Daily sedative-hypnotic use for at least 6 months, in combination with daily alcohol use or regular use of another
mind-altering drug known to pose a severe withdrawal syndrome, and accompanying acute mental or physical
disorder complicating withdrawal; OR
5. Severe opiate withdrawal that has not been stabilized or managed at a less intensive level of service; OR
6. Antagonist medication is to be used in a rapid withdrawal ( as in pharmacological induction and resolution of opiate
withdrawal with naloxone in 6 Hours; OR
7. Stimulant intoxication or withdrawal requires psychiatric or medical monitoring more frequently than hourly because
of psychotic impulsive behavior or depressive suicidality; OR
8. Recent (within 24 hours) serious head trauma or loss of consciousness, with persistent mental status or
neurological changes resulting in need for at least close hourly observation; OR
9. Drug overdose or intoxication has compromised patient’s mental status, cardiac function, or vital signs or functions;
OR
10. Significant acute biomedical disorder poses substantial risk of serious or life-threatening consequences during
withdrawal; OR
11. Drug overdose compromises mental status, cardiac functioning, or other vital signs.
OR
b. requires medical support and comfort care in this level of care for either of the following reasons:
1. Detoxification regimen or response to the regimen requires monitoring or intervention more frequently than hourly;
OR
2. Detoxification or stabilization is required while patient is pregnant until she can be safely treated in a less intensive
level of care.
4
DIMENSION 2: BIOMEDICAL CONDITIONS/COMPLICATIONS
PROCEED TO NEXT DIMENSION IF:
There are no biomedical problems requiring attention.
GENERAL OUTPATIENT CRITERIA
(Levels I and II.1)
Status characterized by (a) and (b) and (c):
a. Any biomedical conditions are stable enough to permit outpatient treatment; AND
b. Biomedical problems will not interfere with treatment; AND
c. Biomedical problems do not warrant inpatient services.
LEVEL I- OUTPATIENT TREATMENT
Meets General outpatient criteria noted above plus:
Any clinical monitoring can be provided by this program with fewer than 9 hours of contact per week or through
concurrent arrangement for medical care.
LEVEL II.1 – INTENSIVE OUTPATIENT TREATMENT
Meets General Outpatient criteria noted above plus:
Any medical monitoring or management can be provided by this program with 9 or more hours of contact per week or
through concurrent arrangement for medical care.
LEVEL II.5 – PARTIAL HOSPITALIZATION
Status characterized by (a) and (b) and (c):
a. All biomedical conditions are stable enough to permit outpatient treatment; AND
b. Biomedical problems are severe enough to distract from recovery efforts but do not warrant inpatient
treatment; AND
c. Medical monitoring and/or medical management can be provided in the partial hospitalization environment
or through a concurrent arrangement for medical care.
LEVEL III.1 – CLINICALLY MANAGED LOW-INTENSITY RESIDENTIAL and
LEVEL III.3 – CLINICALLY MANAGED MEDIUM INTENSITY RESIDENTIAL TREATMENT
Status characterized by (a) or (b) or (c):
a.
All biomedical conditions are stable, any required medical or nurse monitoring or management can be
provided at this level of care and any prescribed medications are self-administered; OR
b.
Concurrent biomedical condition, though not severe enough to warrant inpatient treatment, will distract
from treatment or recovery efforts without medical monitoring provided by this program or through
established arrangement to provide necessary services; OR
c.
This is a biomedical-enhanced program that can address the biomedical condition and provide
necessary staff attention at this level of care.
LEVEL III.5 – CLINICALLY MANAGED HIGH-INTENSITY RESIDENTIAL TREATMENT
Status characterized by (a) or (b) or (c):
a. All biomedical conditions are stable, require less than 24-hour medical monitoring or management, and
any prescribed medications are self-administered; OR
b. Concurrent biomedical condition, though not severe enough to warrant inpatient treatment, will distract from
treatment or recovery efforts without medical monitoring provided by this program or through established
arrangement to provide necessary services; OR
c. This is a biomedical-enhanced program that can address the biomedical condition and provide necessary
staff attention at this level of care.
5
LEVEL III.7 - MEDICALLY MONITORED INTENSIVE INPATIENT
Status characterized by (a) or (b) or (c):
a. Interaction of biomedical condition and continued use creates imminent danger of serious damage to
physical health or concomitant biomedical conditions; OR
b. Biomedical complication(s) or illness requires 24-hour nursing and medical monitoring or active treatment,
but not the full resources of an acute care hospital; OR
c. This is a biomedical enhanced service that can address the biomedical problem requiring a degree of staff
attention that is not available in a non-enhanced program.
LEVEL IV – MEDICALLY MANAGED INPATIENT SERVICES
Status is characterized by any of the following:
a. Biomedical complications require medical management and skilled nursing care; OR
b. Concurrent biomedical illness or complicated pregnancy needs stabilization and daily medical management
with primary nursing interventions OR
c. Concurrent biomedical condition(s) in which continued use presents imminent danger to life or severe
danger to health(including pregnancy); OR
d. Recurrent or multiple seizures; OR
e. Disulfiram-alcohol reaction; OR
f. Life threatening symptomatology related to excessive use of alcohol or other drugs; OR
g. Alcohol or other drug use gravely complicating or exacerbating previously diagnosed medical conditions;
OR
h. Changes in medical status making abstinence imperative; OR
i. Stabilization of a medical condition allowing the patient to respond to addiction treatment; OR
j. Biomedical problems requiring 24-hour observation and evaluation.
6
DIMENSION 3: EMOTIONAL, BEHAVIORAL, OR COGNITIVE CONDITIONS
AND COMPLICATIONS
PROCEED TO NEXT DIMENSION IF (A) OR (B):
a. No indication of co-occurring mental health disorders; OR
b. Emotional, behavioral, or cognitive problems are very mild and do not require assessment,
services, monitoring, or management.
LEVEL 0.5 – EARLY INTERVENTION
Status characterized by:
Emotional, behavioral, or cognitive conditions/complications if any, are being addressed through appropriate mental
health services and do not interfere with therapeutic interventions.
LEVEL I –OUTPATIENT SERVICES
Status characterized by either (a) or (b) and both (c) and (d):
a. No symptoms of a co-occurring mental disorder; OR
b. Psychiatric symptoms are mild and mostly stable;
AND
c.
Mental status does not preclude ability to both:
1. Understand the materials presented; AND
2. Participate in the treatment planning and treatment process
AND
d. Poses no risk of harming self or others nor vulnerability to victimization by others.
LEVEL I-Dual Diagnosis Enhanced
Status characterized by either (a) or (b) and both (c) and (d):
a. The patient has a severe and persistent mental disorder; other motional, behavioral, or cognitive problems
or a substance-induced disorder; or
b. Although residing in a Level III.1 facility, a severe and persistent mental illness impairs ability to follow
through with mental health appointments or medication, without Level I services to augment the treatment
plan;
AND
c.
Mental functioning impairs ability to both:
a)
Understand the materials presented; AND
b) Participate in the treatment planning and treatment process AND
d. Assessed as not posing risk of harming self or others nor vulnerability to victimization by others.
LEVEL II.1 – INTENSIVE OUTPATIENT
Status characterized by either (a) or (b) or (c):
a) The patient’s abuse pf family members or significant others can be controlled through professional contact
exceeding 8 hours per week; OR
b) An emotional, behavioral or cognitive disorder requires intensive outpatient monitoring to minimize
distractions from his or her treatment or recovery; OR
c) Although residing in a Level III.1 facility, a severe and persistent mental illness impairs ability to follow
through with mental health appointments or medication, without intensive outpatient services to augment
the treatment plan.
7
LEVEL II.1 – Dual Diagnosis Enhances.
Status characterized by (a) or (b) or (c):
a) Diagnosed emotional, behavioral, or cognitive disorder requires management or stabilization due to
potential for distraction from treatment; OR
b) There is a mild risk of endangering self, others, or property; OR
c) A significant risk of victimization by another but safety should be maintained with 9 or more hours of contact
per week.
LEVEL II.5 – PARTIAL HOSPITALIZATION
Status characterized by (a) or (b):
a) A history of mild to moderate psychiatric decompensation on discontinuation of drugs of abuse indicates
need for monitoring at this frequency of contact to permit early intervention; OR
b) Contact with professional staff at this frequency and intensity is required for the patient to maintain
behavioral stability.
LEVEL II.5 – Dual Diagnosis Enhanced
Status characterized by (a) or (b) or (c):
a) Inability to maintain behavioral stability over a 48-hour period and requires mental health services for
stabilization; OR
b) A history of moderate psychiatric decompensation and such decompensation is currently observable; OR
c) At mild to moderate risk of endangering self, others, or property and is at imminent risk of relapse with
dangerous emotional, behavioral, or cognitive consequences in the absence of near daily contact with 20 or
more hours of structure services per week.
LEVEL III.1 – CLINICALLLY MANAGED LOW-INTENSITY RESIDENTIAL TREATMENT
Status characterized by (a) and any of (b) through (e)
a) Emotional stability and cognitive functioning are assesses as sufficiently stable to allow participation at this
level of care and benefit from treatment; AND
b) Psychiatric condition is stable and assessed as not posing a risk to self or others, but there is imminent
likelihood of relapse with dangerous consequences outside of a structure environment; OR
c) Symptoms and functional deficits are sufficiently severe that maintaining mental stability and/or abstinence
is unlikely unless treatment is provided in a residential setting; OR
d) Demonstrated inability to maintain stable behavior over a 24-hour period without the structure and support
of a residential setting; OR
e) Co-occurring emotional, behavioral, or cognitive conditions are being addressed concurrently through
appropriate psychiatric services.
LEVEL III.1 – Dual Diagnosis Enhanced
Status characterized by (a) and either (B) or (c):
a) Assessed as able to safely access the community for work education, and other community resources; AND
b) Requires monitoring of psychiatric symptoms concurrent with addiction treatment; OR
c) History suggests need for medication, monitoring, ongoing assessment of psychiatric symptoms, or
behavioral management techniques to prevent distractions from treatment efforts.
LEVEL III.3 – CLINICALLY MANAGED MEDIUM-INTENSITY RESIDENTIAL TREATMENT
Status characterized by (a) and one or more of (b) through (g)
a) Mental status is sufficiently stable to permit the patient ot participate in and benefit from the therapeutic
interventions provided at this level of care with its 24-hour structured environment; AND
b) Emotional, behavioral, or cognitive conditions significantly interfere with activities of daily living and
recovery; OR
c) Violent or disruptive behavior when intoxicated poses a danger to self or others; OR
d) Stress behaviors related to recent or threatened losses significantly impair activities of daily living so as to
require a secure environment to focus on the substance use and/or mental health problems; OR
e) Concomitant personality disorders are of such severity that the accompanying dysfunctional behaviors
require continuous structure interventions; OR
8
f)
Symptoms and functional deficits are assessed as sufficiently severe that maintaining mental stability
and/or abstinence in the home environment is unlikely; OR
g) Mild risk of endangering self, others, or property, and imminent danger of relapse with dangerous
emotional, behavioral, or cognitive consequences without 24-hour support and structure.
LEVEL III.3 – Dual Diagnosis Enhanced
Status characterized by (a) or (b) or (c) or (d):
a. The resident has an emotional, behavioral or cognitive disorder that requires active management; OR
b. Requires differential diagnosis and/or stabilization of psychiatric symptoms concurrent with addictions treatment;
OR
c. Cognitive deficits require that treatment is delivered at a slower pace and in a concrete or repetitive fashion; OR
d. The resident is assessed at a mild to moderate risk of behaviors endangering self, others, or property.
LEVEL III.5 – CLINICALLY MANAGED HIGH-INTENSITY RESIDENTIAL TREATMENT
Status characterized by (a) plus any of (b) through (f)
a) Mental status is sufficiently stable to permit the patient to participate in and benefit from treatment services
provided at this level of care; AND
b) The psychiatric condition is stabilizing, but despite best efforts, the persistent inability to control the use of
alcohol or other drugs and/or antisocial behaviors with attendant probability of harm to self or others without
the structure and 24-hour support afforded by this leel of care; OR
c) Demonstrates repeated inability to control impulses to use or to engage in antisocial behavior resulting in
danger of harm to self or others without the structure and 24-hour support afforded by this level of care; OR
d) Functional deficits are sufficiently severe that mental stability and/or abstinence cannot be maintained
without a residential setting; OR
e) Though pervasive, functional deficits are likely to respond to staff interventions that are primarily habilitative
in focus but do not require medical monitoring or management Or
f) Concomitant personality disorders are of such severity that accompanying dysfunctional behaviors require
continuous boundary-setting interventions.
LEVEL III.5 Dual Diagnosis Enhanced
Meets criteria for Level III.5 Dual Capable plus (a) or (b):
a. Psychiatric symptoms require active monitoring and interventions by mental health staff; OR
b. Behaviors and unpredictable losses of impulse control, pose a serious risk of harm to self or others without
active monitoring and containment in a 24-hour structured environment.
LEVEL III.7 – MEDICALLY MONITORED INTENSIVE INPATIENT SERVICE
Status characterized by any one of the following:
a. Psychiatric conditions unstable and interferes with abstinence and recovery to such a degree that the
patient needs a structured, 24-hour, medically monitored environment; OR
b. Stress behaviors related to recent or threatened losses, have impaired activities of daily living so as to
require a secure medically monitored environment; OR
c. Significant functional deficits that require ongoing psychiatric monitoring; OR
d. Moderate risk of behaviors endangering self, others, or property, and imminent danger of relapse with
dangerous emotional, behavioral, or cognitive consequences without the 24-hour medically monitored
support and structure; OR
e. Active intoxication, with resulting violent or disruptive behavior poses imminent danger to self or others; OR
f. Though disorders or cognitive limitations require stabilization but not medical management in a 224-hour
environment.
9
LEVEL III.7 – Dual Diagnosis Enhanced
Meets criteria for Level III.7 plus any of the following:
a. A history of moderate psychiatric decompensation on discontinuation of drugs of abuse, and such decompensation
is present; OR
b. Moderate to high risk endangering self, others, or property and imminent danger of relapse with dangerous
emotional, behavioral or cognitive consequences without the 24-hour setting and does not require one-on –one
suicide watch; OR
c. Severe depression, with suicidal impulses and a plan, but is able to reach out for help as needed in an intensive 24hour setting and does not require one-on-one suicide watch;
d. A co-occurring psychiatric disorder requires stabilization with psychotropic medications; OR
e. A severe co-occurring psychiatric disorder is marginally and tenuously stable and requires close management and
care available only in a program with integrated mental health and addiction treatment services to prevent
decompensation.
LEVEL IV – MEDICALLY MANAGED INPATIENT SERVICES
Status characterized by any of the following:
a. Emotional/behavioral complications of the patient’s addictive disorder require psychiatric management and skilled
nursing care; OR
b. A concurrent emotional, behavioral or cognitive disorder requires stabilization, daily medical management and
primary nursing interventions; OR
c. Uncontrolled behavior seriously endangers self or others; OR
d. The patient’s mental confusion and fluctuating orientation poses an imminent danger to self or others; OR
e. A serious emotional, behavioral, or cognitive disorder complicates the treatment of addiction and requires
differential diagnosis and medical management; OR
f. Extreme depression poses an imminent risk to his or her safety; OR
g. Impairments in cognitive functioning preclude the ability to manage activities of daily living and pose an imminent
risk to personal safety; OR
h. Continued alcohol and/or drug use has caused grave complications or exacerbation of a previously diagnosed
psychiatric, emotional, behavioral condition; OR
i. Altered mental status., with or without delirium as manifested by
1. Disorientation to self; OR
2. Alcoholic hallucinosis; OR
3. Toxic psychosis.
10
DIMENSION 4: READINESS TO CHANGE
LEVEL0.5 – EARLY INTERVENTION
Status characterized BY:
Willing to gain understanding of how current use may be harmful.
LEVEL I-OUTPATIENT SERVICES
Status characterized by (a) and any of (b) or (c) or (d);
a. Willing to participate in treatment planning and to attend all scheduled activities mutually agreed upon in the
treatment plan; AND
b. Acknowledges a substance-related and/or mental health problem and wants help to change; OR
c. Ambivalence about a substance-related and/or mental health problem requires monitoring and motivating strategies
but not a structured milieu; OR
d. Does not recognize the substance-related and/or mental health problem(s), but is invested in avoiding further
consequences.
LEVEL II.1 – INTENSIVE OUTPATIENT TREATMENT
Status characterized by (a) and either (b) or (c):
a. Willingness to participate in treatment and to explore awareness and readiness to change suggest that sufficiently
intensive treatment can be effective; AND
b. Structured therapy and programmatic milieu to promote treatment progress and recovery are required because
motivational interventions at a lower level of care have failed; OR
c. Perspective inhibits ability to make behavioral changes without repeated, structured, clinically directed motivational
interventions.
LEVEL II.1- Dual Diagnosis Enhanced
Meets criteria for admission to Level II.1 plus (a) or (b) or (c):
a. Reluctance regarding treatment and ambivalence about commitment to change a co-occurring mental health
problem; OR
b. Follow-through in treatment is poor or inconsistent due to the behavioral health problems so that treatment at a
lower level is neither succeeding nor feasible; OR
c. Awareness or commitment to change is so limited that an adequate level of functioning cannot be maintained
without intensive outpatient services that integrate mental health and addiction treatment services.
LEVEL II.5 – PARTIAL HOSPITILIZATION
Status characterized by (a) and either (bb) or (c):
a. Willingness to participate in treatment and sufficient readiness to change suggest that treatment of sufficient
intensity can be effective; AND
b. Structured therapy and services involving at least 20 hours per week are required because motivational
interventions at a lower level of care have failed; OR
c. Perspective and lack of impulse control inhibit ability to make behavioral changes without repeated, structured,
clinically directed motivational interventions.
LEVEL II.5 – Dual Diagnosis Enhanced
Meets criteria for admission to Level II.5 plus (a) or (b) or (c):
a. Manifests little awareness of co-occurring mental disorder; OR
b. Follow-Through in treatment is so poor or inconsistent due to emotional, cognitive, or behavioral problems that less
intensive services are not succeeding or feasible; OR
c. Requires more intensive engagement, community involvement, or case management services due to emotional,
cognitive, or behavioral problems than are available at a lower level program.
11
LEVEL III.1 – CLINICALLLY MANAGED LOW-INTENSITY RESIDENTIAL TREATMENT.
Status characterized by any of the following:
a. Acknowledge the existence of a psychiatric condition and/or substance use problem and is sufficiently ready and
cooperative enough to respond to low-intensity residential treatment; OR
b. due to early stage of readiness to change, needed engagement and motivational strategies can be provided via
Level III.1 plus augmentation by additional Level I or II serves; OR
c. A 24-hour structured milieu is required to promote treatment progress and recovery, because motivating
interventions have failed in the past and are assessed as not likely to succeed in the future in an outpatient setting;
OR
d. Impaired ability to make behavior changes without repeated, structured motivational interventions in a 24-hour
milieu.
LEVEL III.1 – Dual Diagnosis Enhanced
Meets criteria for Level III.1 plus any of the following:
a. Ambivalent regarding commitment to address a co-occurring mental health problem; OR
b. Lack of consistent follow-through with treatment due to emotional behavioral, or cognitive problem; OR
c. Minimal awareness of a problem, or being unaware of the need to change requiring active interventions with family,
significant others, and other external systems to create incentives and align incentives so as to promote
engagement in treatment.
LEVEL III.3 – CLINICALLY MANAGED MEDIUM-INTENSITY RESIDENTIAL TREATMENT
Status characterized by (a) and any of the following:
a. Treatment interventions available in a moderately intense residential setting can be expected to increase the
resident’s degree of readiness to change; AND
b. Limited readiness to change because the intensity and chronicity of the addictive disorder or cognitive limitations
preclude much awareness of the need for continued care, the existence of substance abuse/mental health
problem(s), or the need for treatment; OR
c. Marked difficulty understanding the relationship between substance use, addiction, mental health or life problems,
and impaired coping skills or level of functioning despite a history of serious consequences; OR
d. Continued substance use poses a danger of harm to self or others, but there is no demonstrated awareness of the
need to address the severity of addictions or psychiatric problems or the need for treatment; OR
e. Impaired ability to make behavior changes without repeated, structured, clinically directed intervention delivered in a
24-hour milieu.
LEVEL III.3 – Dual Diagnosis Enhanced
Meets criteria for Level III.3 plus (a) or (b):
a. a. Ambivalence in commitment to address a co-occurring mental health problem; OR
b. Inability to consistently follow through with treatment due to mental condition, or related lack of awareness of a
problem, or the need to change requires active interventions with family, significant others, and other external
systems to create and align incentives.
LEVEL III.5 – CLINICALLLY MANAGED HIGH-INTENSITY RESIDENTIAL TREATMENT.
Status characterized by (a) and any of (b) through (f):
a. Treatment interventions available in a structure 24-hour programmatic milieu can be expected to increase readiness
to change; AND
b. Manifests little awareness of the need for continuing care, the existence of a substance use or mental health
problem, or need for treatmentt; OR
c. Has marked difficulty understanding the relationship between substance use, addiction, mental health or life
problems, and impaired coping skills or level of functioning. Often blames others for problems; OR
d. Demonstrated opposition to addressing the severity of addiction or mental health problem(s); OR
e. Does not recognize the need for treatment even though continued substance use or inability to follow through with
mental health treatment poses a danger of harm to self or others; OR
f. Motivational interventions have failed at less intensive levels of care and are not likely to succeed at such lower
levels at this time; OR
12
g. Impaired ability to make behavior changes without repeated, structured, clinically directed motivational
interventions, delivered in a 24-hour milieu.
LEVEL III.5 – Dual Diagnosis Enhanced
Meets criteria for Level III.5 plus any of (a) through (d):
a.
b.
c.
d.
Reluctance to engage in activities necessary to address a co-occurring mental health problem; OR
Inconsistent follow-through with treatment for a mental problem; OR
Minimal awareness of co-occurring problem; OR
Requires active interventions with family, significant others, and other external systems to create leverage and align
incentives.
LEVEL III.7 – MEDICALLY MONITORED INTENSIVE INPATIENT TREATMENT
Status characterized by (a) or (b) or (c):
a. Despite serious consequences, does not accept or relate the addictive disorder to the problem severity; OR
b. Needs intensive motivating strategies, activities and processes available only in 24-hour structured, medically
monitored environment; OR
c. Need ongoing 24-hour psychiatric monitoring to follow through with the treatment regimen and to deal with issues
regarding compliance with psychiatric medications.
LEVEL III.7 – Dual Diagnosis Enhanced
Meets criteria for Level III.7 plus (a):
a. Lack of commitment to engage in activities necessary to address a co-occurring mental disorder.
LEVEL IV – MEDICALLY MANAGED INPATIENT TREATMENT
Problems in Dimension 4 are not sufficient for placement into Level IV.
13
DIMENSION 5: RELAPSE, CONTINUED USE, OR CONTINUED PROBLEM POTENTIAL
LEVEL 0.5 – EARLY INTERVENTION
Status characterized by (a) or (b):
a. Does not understand need to alter current use; OR
b. Needs to acquire skills to change.
LEVEL I -OUTPATIENT TREATMENT
Status characterized by:
Able to achieve or maintain abstinence or related treatment goals with support and therapeutic contact of less than 9
hour per week.
LEVEL I – Dual Diagnosis Enhanced
Meets criteria for Level 1 plus (a) or (b):
a. Support and therapeutic contact are required to deal with emotional or behavioral issues; OR
b. Instability requires outreach and support of assertive community treatment and intensive case management to
maintain mental health function.
LEVEL II.1 – INTENSIVE OUTPATIENT TREATMENT
Status characterized by (a) or (b) or (c):
a. Requires professional contact of 9 hours or more per week to terminate use or maintain abstinence; OR
b. An intensification of symptoms of the substance-related disorder at a lower level of care; OR
c. Level of functioning is deteriorating at lower level of care
LEVEL II.1 – Dual Diagnosis Enhanced
Meets criteria for Level II.1 plus (a) or (b):
a. Psychiatric symptoms pose a moderate risk of relapse to the alcohol, drug or psychiatric disorder – includes misuse
of medications; OR
b. Impaired recognition or ability to manage relapse issues due to emotional, cognitive, or behavioral problems
requiring fully integrated services.
LEVEL II.5 – PARTIAL HOSPITILIZATION
Status characterized by any of the following:
a. Treatment services consisting of at least 20 hours per week are judged necessary to provide sufficient intensity of
services to achieve or maintain abstinence; OR
b. Treatment at a less intensive level of care was insufficient to stabilize the patient’s condition; OR
c. Intensification of substance use disorder related symptoms and deterioration of functioning are occurring at a lower
level of care; OR
d. High risk of relapse or continued use without close outpatient monitoring and structured therapeutic services(e.g.
due to lack of awareness or inadequate coping)
LEVEL II.5 – Dual Diagnosis Enhanced
Meets criteria for Level II.5 plus any of the following:
a. Psychiatric symptoms pose a high risk of relapse to alcohol, drug use, or psychiatric de-compensation; OR
b. Impaired recognition or understanding of relapse issues and poor skills in coping with and interrupting mental
disorders; OR
c. Poor or inconsistent follow-through in treatment due to emotional, cognitive, or behavioral problems requires
integrated mental health and treatment services.
14
LEVEL III.1 – CLINICALLLY MANAGED LOW-INTENSITY RESIDENTIAL
Status characterized by any of the following:
a. Limited coping skills to address relapse triggers and urges and/or deteriorating mental functioning poses imminent
danger of relapse, with dangerous emotional, behavioral, or cognitive consequences without 24-hour structure; OR
b. Understands substance dependence and/or mental disorder but inability to consistently address either or both
poses risk of relapse without 24-hour structure; OR
c. Needs staff support to maintain engagement in recovery program wile transitioning to life in the community; OR
d. High risk of substance use or deteriorated mental functioning, with dangerous emotional, behavioral, or cognitive
consequences is addressed via Level II services plus close 24-hour support.
LEVEL III.1 – Dual Diagnosis Enhanced
Meets criteria for Level III.1 plus any of the following:
a. Psychiatric symptoms that pose a moderate risk of relapse to substance dependence or mental disorder; OR
b. Exhibits deteriorating functioning or ability apply skills without integrated mental health services; OR
c. Requires case management to coordinate the service necessary to manage medications or attain stabilization.
LEVEL III.3 – CLINICALLLY MANAGED MEDIUM-INTENSITY RESIDENTIAL TREATMENT.
Status characterized by any of the following:
a. Failure to recognize relapse triggers or the need for continuing care due to intensity or chronicity of addictive and/or
mental health disorder(s) or cognitive limitations poses dangerous consequences without 24-hour monitoring and
structure; OR
b. Cognitive impairment limits coping ability and requires that treatment be delivered at a slow pace, concretely and
repetitively, in a setting with 24-hour structure and support; OR
c. Intensification of symptoms and deteriorating functioning at a lower level of care despite amendments to the
treatment plan; OR
d. Despite active participation at a less intensive level of care, continued use or psychiatric deterioration poses
imminent dangerous consequences without close 24-hour monitoring and structured treatment.
LEVEL III.3 – Dual Diagnosis Enhanced
Meets criteria for Level III.3 plus any of the following:
a. Psychiatric symptoms pose a moderate risk of relapse to substance dependence or mental/psychiatric
decompensation with imminent serious consequences; OR
b. Cognitive deficits result in medication noncompliance or risk-taking behaviors requiring 24-hour structured services;
OR
c. Case management and collaboration across levels of care may be necessary to manage anti-craving, psychotropic,
or opioid maintenance medications; OR
d. Cognitive deficits or emotional issues(in preparation for transfer to a less intensive level of care, a different type of
service in the community, and/or reentry into the community) require case management and staff exploration of
supportive living environments.
LEVEL III.5 – CLINICALLLY MANAGED HIGH-INTENSITY RESIDENTIAL TREATMENT.
Status characterized by any of the following:
a. Failure to recognize relapse triggers and lack of commitment to continuing care despite the fact that continued use
poses an imminent danger of harm to self or others requires 24-hour monitoring and structured support; OR
b. Despite best efforts, the inability to control use and/or other behaviors with attendant probability of harm to self or
others requires 24-hour monitoring and structured support; OR
c. Psychiatric or addiction symptoms, such as drug craving, difficulty postponing immediate gratification, and other
drug seeking behaviors, poses and imminent danger of harm to self or others in the absence of 24-hour monitoring
and structured support; OR
d. A crisis situation poses imminent danger of relapse, with dangerous emotional, behavioral, or cognitive
consequences; OR
e. Despite active participation at a less intensive level of care, continued use and/or psychiatric decompensation pose
imminent dangerous consequences in the absence of close 24-hour monitoring and structured treatment
15
LEVEL III.5 – Dual Diagnosis Enhanced
Meets criteria for Level III.5 plus any of the following:
a. Psychiatric symptoms pose a moderate to high risk of relapse to substance dependence or mental disorder with
imminent serious consequences; OR
b. Behaviors pose a relapse risk as indicated by:
1. Criminal/antisocial behaviors; OR
2. Association with antisocial individuals/situations; OR
3. Inability to understand relapse risks posed by behaviors.
c. Case management and collaboration across levels of care may be necessary to manage anti-craving, psychotropic,
or opioid maintenance medications; OR
d. Preparation of the resident for transfer to less intensive level of care, a different type of service in the community,
and/or reentry into the community requires case management and transition arrangements to address emotional,
behavioral, or cognitive conditions.
LEVEL III.7 – MEDICALLY MONITORED INTENSIVE INPATIENT
Status characterized by any of the following:
a. Acute psychiatric or substance use crisis poses an imminent danger of harm to self or others in the absence of 24hour monitoring and structured support; OR
b. An escalation of relapse behaviors and/or reemergence of acute symptoms pose an imminent danger of harm to
self or others in the absence of monitoring and structured support found in a medically monitored setting; OR
c. The modality of treatment or protocols to address relapse(e.g., aversion therapy) require a medically monitored
program.
LEVEL III.7 – Dual Diagnosis Enhanced
Meets criteria for Level III.7 plus any of the following:
a. Psychiatric symptoms that pose a moderate to high risk of relapse to a substance dependence or mental disorder;
OR
b. Follow through with treatment is poor or inconsistent and his or her relapse problems are escalating due to
emotional, behavioral, or cognitive problems requiring integrated mental health and substance abuse services; OR
c. Suicidal ideation with a plan, but agrees to reach out for help and can be maintained at this level of care.
LEVEL IV – MEDICALLY MANAGED INPATIENT TREATMENT
Problems in Dimension 5 do not quality for Level IV services.
16
DIMENSION 6: RECOVERY ENVIRONMENT
LEVEL 0.5 – EARLY INTERVENTION
Status characterized by any of the following:
a.
b.
c.
d.
Social system is composed of persons whose substance use prevent them from meeting responsibilities; OR
Substance use/abuse by family members heighten risks for substance-related disorder; OR
Expressed values of significant other(s) concerning alcohol or other drugs create serious conflicts; OR
Significant other(s) encourages inappropriate use of alcohol or other drugs.
LEVEL I -OUTPATIENT TREATMENT
Status characterized by any one of the following:
a.
b.
c.
Psychosocial environment sufficiently supportive to make low-intensity outpatient treatment feasible; OR
inadequate support system but is sufficiently stable, motivated and willing to obtain a support system; OR
family/significant others are supportive but require professional assistance to address limit setting,
communication, or enabling to improve recovery prospects.
LEVEL I – Dual Diagnosis Enhanced
Meets criteria for Level I plus (a) or (b) or (c):
a. Inadequate primary or social support system and has mild emotional, behavioral, or cognitive impairment in ability
to, obtain a support system; OR
b. Family therapy or interventions are required for emotional behavioral, or related issued; OR
c. Access to intensive outreach and case management can address the following:
1. Severe and persistent mental disorder; AND
2. Inadequate family or social support; AND
3. Limited ability to establish adequate environment due to chronic impairment, but is not in imminent danger.
LEVEL II.1 – INTENSIVE OUTPATIENT TREATMENT
Status characterized by (a) or (b):
a. Given lack of resources and skill, continued exposure to current environment makes recovery unlikely without the
structure of a Level II.1 program of at least 9 hours of weekly services; OR
b. Recovery is jeopardized by any of the following:
1. Lack of appropriate social contact; OR
2. Few friends or peers do not use; OR
3. Lacks resources or skills to maintain an adequate level of social functioning without intensive outpatient
services.
LEVEL II.1 – Dual Diagnosis Enhanced
Meets criteria for Level II.1 plus (a) and (b):
a. Environment is not supportive of good mental functioning AND
b. Lacks resources and skills to deal with this.
LEVEL II.5 – PARTIAL HOSPITILIZATION
Status characterized by (a) or (b):
a. Lack of resources or skills necessary to maintain adequate functioning with continued exposure to the current
environment makes recovery unlikely without the structure of a II.5 program with at lease 20 hours per week of
outpatient services; OR
b. Requires relief from home environment for a greater part of the day than is provided by a less intensive level of
care to stay focused on recovery because family members and/or significant others:
1. Are not supportive of recovery goals; OR
2. Are passively opposed to treatment;
17
LEVEL II.5 – Dual Diagnosis Enhanced
Meets criteria for Level II.5 plus (a) or (b):
a. Environment is not supportive of good mental functioning; AND
b. Limited resources and skills require integrated services at this level of care to deal with the environment.
LEVEL III.1 – CLINICALLLY MANAGED LOW-INTENSITY RESIDENTIAL TREATMENT.
Status characterized by (a) and any of (b) through (f):
a. Able to cope for limited periods of time outside a 24-hour structure to pursue necessary activities; AND
b. Assessed as unable to achieve or maintain recovery due to moderately high environmental risk of physical, sexual,
or emotional abuse or substance use; OR
c. Requires 24-hour supportive setting due to any of the following:
1. Lacks appropriate social contact; OR
2. Significant social isolation and withdrawal; OR
3. Most friends regularly use alcohol/drugs; OR
d. Lives in an environment that is highly invested in alcohol or other drug use; OR
e. Continued exposure to the environment makes recovery unlikely in light of insufficient resources and skills to
maintain adequate functioning outside of a 24-hour supportive environment; OR
f. Danger of victimization by another.
LEVEL III.1 – Dual Diagnosis Enhanced
Meets criteria for Level III.1 and (a) plus (b) or (c) or (d):
a.
b.
c.
d.
Severe and persistent mental illness; AND
Mental condition precludes ability to benefit from skills training in the community environment; OR
Insufficient resources and skills to deal with an environment that is not supportive of good mental health; OR
Requires support and structure to achieve stabilization or prevent deterioration.
LEVEL III.3 – CLINICALLLY MANAGED MEDIUM-INTENSITY RESIDENTIAL TREATMENT.
Status characterized by (a) plus any of (b) through (f):
a. Unable to cope for even limited periods of time outside a structure 24-hour environment with staff monitoring; AND
b. Assessed as unable to achieve or maintain recovery due to environmental risk of physical, sexual, or emotional
abuse or substance use at a lower level of care; OR
c. Significant danger of victimization outside this level of care; OR
d. Social network includes regular users of alcohol or other drugs such that recovery goals are judged unattainable at
a less intensive level; OR
e. Living arrangement includes either of the following:
1. Lives with a person who is a regular user, abuser, or dealer, Or
2. Living environment is highly invested in use such that recovery goals are unattainable; OR
f. Vulnerability due to cognitive limitations posed danger of victimization by another.
LEVEL III.3 – Dual Diagnosis Enhanced
Meets criteria for Level III.3 and (a) plus (b) or (c) or (d):
a. Severe and persistent mental illness; AND
b. Mental condition precludes ability to benefit from skills training in the recovery environment; OR
c. Insufficient resources and sills to deal with an environment that is not supportive of good mental health without
assertive community treatment, intensive case management, or other support structures; OR
d. Requires support and structure of this level of care to achieve stabilization or prevent deterioration.
LEVEL III.5 – CLINICALLLY MANAGED HIGH-INTENSITY RESIDENTIAL TREATMENT.
Status is characterized by (a) plus (b) through (h):
a. Unable to cope for even limited periods of time outside a structured 24-hour environment with staff monitoring;
AND
b. Assessed as unable to achieve or maintain recovery due to risk of physical, sexual, or emotional abuse or
substance use at a lower level of care; OR
18
c. Social network includes regular users such that recovery goals are judged unattainable at a less intense level; OR
d. Significant danger of victimization outside this level of care; OR
e. Living arrangement includes either of the following:
1. Lives with a person who is a regular user, abuser, or dealer; OR
2. Living environment is highly invested in use so that recovery goals are unattainable; OR
f. social network is characterized by significant social isolation or withdrawal such that recovery goals are judged as
unachievable at less intensive level of care; OR
g. Living environment is characterized by criminal behavior and other antisocial norms and valuies.
h. Needs staff monitoring before transferring to alower level of service.
LEVEL III.5 – Dual Diagnosis Enhanced
Meets criteria for Level III.5 and (a) plus (b) or (c) or (d):
a. Severe and persistent mental illness; AND
b. Mental condition precludes ability to benefit from skills training in the recovery environment; OR
c. Insufficient resources and skills to deal with an environment that is not supportive of good mental health without
assertive community treatment, intensive case management, or other support structures; OR
d. Requires support and structure to achieve stabilization or prevent deterioration.
LEVEL III.7 – MEDICALLY MONITORED INPATIENT TREATMENT
Status characterized by (a) or (b) or (c):
a. Assessed as unable to achieve or maintain recovery at a less intensive level due to need for continuous medical
monitoring; OR
b. Family members or significant others are unsupportive or actively sabotaging treatment.
c. Unable to cope for even limited periods of time outside a structure, 24-hour environment with staff monitoring prior
to transferring to a less intensive level of services.
LEVEL III.7 – Dual Diagnosis Enhanced
Meets criteria for Level III.7 and (a) plus (b) or (c) or (d):
a.
b.
c.
d.
Severe and persistent mental illness; AND
Mental condition precludes ability to benefit from skills training in the community environment; OR
Insufficient resources and skills to deal with an environment that is not supportive of good mental health; OR
Requires support and structure to achieve stabilization or prevent deterioration.
LEVEL IV – MEDICALLY MANAGED INPATIENT TREATMENT
Problems on Dimension 6 do not qualify for Level IV services.
19
OPIOID MAINTENANCE THERAPY (OMT)
DIMENSION 1: ACUTE INTOXICATION/WITHDRAWAL
Status is characterized by any of the following:
a. Physician determines the individual has been physiologically dependent upon an opiate drug for at least a year,
and dependence is confirmed by physical signs; OR
b. The individual has been incarcerated or in a chronic care setting, but would have been eligible for OMT prior to
incarceration; OR
c. The program physician certifies that a female is pregnant and finds OMT medically justified; OR
d. Documented prior methadone treatment of 6 months or more and the program physician judges OMT to be
medically indicated.
DIMENSION 2: BIOMEDICAL CONDITIONS AND COMPLICATIONS
Status is characterized by any of the following:
a. Mets biomedical criteria for opioid dependence and requires outpatient medical monitoring; OR
b. Biomedical illness or pregnancy can be treated on an outpatient basis with minimal daily monitoring; OR
c. If present, biomedical problems can be monitored on a outpatient basis.
DIMENSION 3: EMOTIONAL, BEHAVIORAL, OR COGNITIVE CONDITIONS AND COMPLICATIONS
Status is characterized by any of the following
a. Problems, if present, are manageable in an outpatient structured environment; OR
b. Outpatient treatment is required for educe the risk of further deterioration; OR
c. Stable condition requires monitoring, management, or medication due to risk of distracting patient from treatment;
OR
d. Mild risk of harm to self or others can be managed safely in a structured outpatient environment; OR
e. Despite demonstrated stability, requires continued pharmacotherapy to prevent relapse to opiate use.
DIMENSION 4: READINESS TO CHANGE
Status is characterized by any of the following:
a. Requires structured therapy, pharmacotherapy, and programmatic milieu to promote progress and recovery; OR
b. Attributed problems to persons or external events, but resistance is low enough so that treatment may be effective
but requires clinically directed and repeated structured motivational interventions.
DIMENSION 5: RELAPSE, CONTINUED USE, OR CONTINUED PROBLEM POTENTIAL
Status is characterized by any of the following
a. Requires structured therapy, pharmacotherapy, and programmatic milieu due to physiologic craving or perceived
need for opiates; OR
b. Without provision of OMT, there is an intensification of addiction symptoms, high risk behaviors, or deteriorating
functioning despite revisions of treatment plan; OR
c. High risk for relapse without OMT due to lack of awareness of relapse triggers, difficulty in postponing gratification,
or ambivalence or resistance toward treatment.
DIMENSION 6: RECOVERY ENVIRONMENT
Status is characterized by any of the following:
a. Sufficiently supportive environment to make OMT feasible; OR
b. Family members and/or significant others are supportive but require professional assistance to improve likelihood or
success; OR
c. Does not have a positive social support system, but has demonstrated notification to obtain such support or an
appropriate living environment; OR
d. Has experienced traumatic events or has manifested the effects of emotional, behavioral, or cognitive problems in
the environment, but they are manageable on an outpatient basis.
20
")