C-01 : membranoproliferative glomerulopathy
F- 08 : infectious complications
H- 14 : infectious complications
Hepatitis C Virus Infection and Kidney Transplantation in 2014:
What's New?
S. Baid-Agrawal1,*, M. Pascual2, D. Moradpour3, R. Somasundaram4 and M. Muche4
Article first published online: 4 AUG 2014
DOI: 10.1111/ajt.12835
American Journal of Transplantation Volume 14, Issue 10, pages 2206–2220, October
2014
ABSTRACT
Chronic hepatitis C virus (HCV) infection remains an important health problem, which is
associated with deleterious consequences in kidney transplant recipients. Besides hepatic
complications, several extrahepatic complications contribute to reduced patient and allograft
survival in HCV-infected kidney recipients. However, HCV infection should not be considered
as a contraindication for kidney transplantation because patient survival is better with
transplantation than on dialysis. Treatment of HCV infection is currently interferon-alpha
(IFN-α) based, which has been associated with higher renal allograft rejection rates.
Therefore, antiviral treatment before transplantation is preferable. As in the nontransplant
setting, IFN-free treatment regimens, because of their greater efficacy and reduced toxicity,
currently represent promising and attractive therapeutic options after kidney transplantation
as well. However, clinical trials will be required to closely evaluate these regimens in kidney
recipients. There is also a need for prospective controlled studies to determine the optimal
immunosuppressive regimens after transplantation in HCV-infected recipients. Combined
kidney and liver transplantation is required in patients with advanced liver cirrhosis. However,
in patients with cleared HCV infection and early cirrhosis without portal hypertension, kidney
transplantation alone may be considered. There is some agreement about the use of HCVpositive donors in HCV-infected recipients, although data regarding posttransplant survival
rates are controversial.
COMMENTS
The prevalence of HCV infection in kidney transplant recipients is significantly higher than in
the general population, and it is associated with increased morbidity and mortality. In spite of
recent therapeutic advances, the management of HCV infection continues to be a challenge.
This review will summarize our current understanding of the epidemiology and diagnosis,
natural history and outcome, as well as management of HCV infection in kidney transplant
recipients, with an emphasis on recent advances in interferon (IFN)-free treatment regimens.
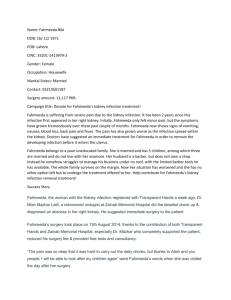
Algorithm for screening for HCV in patients on hemodialysis. EIA, enzyme-linked
immunoassays; HCV, hepatitis C virus; NAT, nucleic acid amplification test; RIBA,
recombinant immunoblot assay.
Progress in the treatment of chronic hepatitis C. DAA, direct-acting antiviral; IFN-alpha,
interferon-alpha; PEG-IFN-α, pegylated interferon-alpha; 1st-gen PI, first-generation protease
inhibitor; RBV, ribavirin; SVR, sustained virological response.
Pr. Jacques CHANARD
Professor of Nephrology
 0
0