pregnant liver
advertisement

Liver, thyroid and neurological disorders in pregnancy
سهيلة.د
Cholecystitis
Cholecystitis occurs rarely during pregnancy (0.3%) because the gallbladder and biliary
duct smooth muscle are relaxed by progesterone.
cholecystectomy can be performed in the second trimester, the fetal loss rate probably is
not increased.
Laparoscopic cholecystectomy in pregnancy is widely accepted. after 20 weeks' gestation,
it should be performed with special care to avoid injury to the uterus.
In the third trimester, surgical intervention can cause preterm delivery.
Intrahepatic Cholestasis of Pregnancy
Intrahepatic cholestasis of pregnancy is a condition characterized by accumulation of bile
acids in the liver with subsequent accumulation in the plasma, causing pruritis. It is similar
to the cholestasis that occasionally occurs during combined oral contraceptive therapy.
Estrogens are considered to play a role in its etiology, probably by slowing the enzymes
involved in bile transport.
The cardinal clinical findings: is total body itching involving the palms and soles.
differential diagnoses: are
1. hepatitis,
2. biliary tract disease,
3. acute fatty liver of pregnancy (AFLP)
4. and the {hemolysis, elevated liver enzymes, low platelet count (HELLP)
syndrome}.
Investigations:
increased levels of alkaline phosphatase, bilirubin, and serum bile acids
(chenodeoxycholic acid, deoxycholic acid, cholic acid).
Aspartate transaminase (AST) and alanine transaminase (ALT) levels may be mildly
elevated.
Patients may be symptomatic weeks before the diagnostic laboratory abnormalities are
noted.
Treatment:
Symptomatic treatment of pruritus with
1- antihistamines such as diphenhydramine is useful.
2- Ursodeoxycholic acid inhibit absorption of toxic bile acids and increase their biliary
excretion and so normalizes bile acids, improves liver function tests, and relieves
pruritus.
3- Oral steroids also have been used to relieve symptoms.
4- Symptoms resolve postpartum.
Complications:
1- intrahepatic cholestasis of pregnancy is associated with fetal death,
2- spontaneous preterm birth,
3- and postpartum hemorrhage.
The etiology is unclear, may be due to the fetal toxicity of bile acids. different
strategies for assessment of fetal wellbeing have been proposed: biophysical profile
twice per week starting at the time of diagnosis is suggested, amniocentesis at 35–36
weeks, delivery at 37–38 weeks
Acute Fatty Liver of Pregnancy (AFLP)
Acute fatty liver of pregnancy is a rare complication (1 in 5000 to 1 in 13,000) that occurs
in the third trimester. Early recognition and termination of the pregnancy (delivery) and
extensive supportive therapy have reduced the mortality rate to approximately 5–10%.
Recurrence in subsequent pregnancies is rare and appears limited to women with abnormal
fatty acid transport and metabolism pathway.
Symptoms and signs:
include nausea and vomiting, malaise, epigastric pain, and jaundice. AFLP should be
suspected in any patient who presents with new-onset nausea and malaise in the third
trimester until the results of liver and chemistry panels are available.
Investigations:
elevated AST and ALT levels (up to 7 times normal),
markedly elevated bilirubin level,
prolonged prothrombin time.
Hypoglycemia,
Thrombocytopenia,
Hypofibrinogenemia
Elevated serum creatinine level
Complications:
1- Acute renal failure,
2- DIC,
3- encephalopathy,
4- and sepsis can be severe.
Management:
The principles of management are supportive care and prompt delivery. Glucose 50%,
blood products, broad-spectrum antibiotic coverage, and pulmonary support are critical.
Importantly, the total bilirubin level may continue to rise for up to 10 days after delivery
which is part of the natural history of recovering AFLP
HELLP Syndrome: a complication of PET.
Viral Hepatitis
Viral hepatitis complicates 0.2% of all pregnancies. Hepatitis may be caused by numerous
viruses, drugs, or toxic chemicals; and the clinical manifestations of all forms are similar.
The development of specific serologic markers has improved the accuracy of the
diagnosis. The most common viral agents causing hepatitis in pregnancy are hepatitis A
virus, hepatitis B virus, hepatitis C (formerly termed non-A, non-B hepatitis virus),
hepatitis E, Hepatitis D (Delta).
Hepatitis A
The primary mode of transmission is the fecal/oral route.
Excretion of the virus in stool normally begins approximately 2 weeks prior to the onset of
clinical symptoms and is complete within 3 weeks following onset of clinical symptoms.
No carrier state exists for the virus. Both blood and stool are infectious during the (2-6)
week incubation period.
Perinatal transmission does not occur.
Hepatitis B
Hepatitis B is blood borne double stranded DNA virus. It is usually transmitted by
inoculation of infected blood or blood products, or sexual contact. The virus is contained
in most body secretions.
Approximately 5–10% of people infected with hepatitis B virus become chronic carriers of
the virus.
The incubation period of hepatitis B is 6 weeks to 6 months.
The hepatitis B surface antigen (HBsAg), usually measured in blood. The presence of
HBsAg is the first manifestation of viral infection; it usually appears before clinical
evidence of the disease and lasts throughout the infection. Persistence of HBsAg after the
acute phase of hepatitis usually is associated with clinical and laboratory evidence of
chronic hepatitis.
The hepatitis B core antibody (HBcAb) is produced against the core of the largest viral
particle. HBcAb occurs with acute hepatitis B infection at the onset of clinical illness.
Hepatitis B e antigen (HBeAg) is found only when HBsAg is present.
Pregnant women who are HBeAg-positive in the third trimester
frequently transmit this infection to the offspring (80–90%) in the
absence of immunoprophylaxis, whereas those who are negative
rarely infect their offspring.
Hepatitis C
Up to 85% of infected individuals become chronic carriers.
The incubation period usually is 7–8 weeks. The course of infection is similar to that of
hepatitis B.
Hepatitis C antibody is present in approximately 90% of patients.
Investigations:
PCR for hepatitis C RNA and Hepatitis C antibody.
Vertical transmission occurs in 5–8% of infected pregnancies.
Hepatitis D
Hepatitis D virus is an RNA virus that is smaller than all other known RNA viruses. The
agent can cause infection only when HBsAg positive. Hepatitis D is isolated in up to 50%
of cases of fulminant hepatitis B infection. Hepatitis D antigen (HDAg) and hepatitis D
antibody (HDAb) are serologic markers for the disease.
Hepatitis E
Hepatitis E is transmitted via the oral/fecal route. Hepatitis E, it is endemic in several
developing countries. The disease is self-limited and does not result in a chronic carrier
state.
Pregnant patients who are acutely infected have a 15% risk of
fulminant liver failure with a 5% mortality rate.
Clinical Findings
The clinical picture of hepatitis is highly variable. Most patients have asymptomatic
infection, but a few may present with fulminating disease and die within a few days. The
clinical features of hepatitis A and B are similar, although hepatitis B is more insidious
and have an acute or a chronic course. Fulminant hepatic failure is very rare with hepatitis
A but occurs in approximately 1% of patients infected with hepatitis B.
Frequent symptoms include:
General malaise, myalgia, fatigue, anorexia, nausea and vomiting, right upper quadrant
pain, and low-grade fever. Mild hepatomegaly and/or splenomegaly occur in 5–10% of
affected patients and lymphadenopathy in 5%.
Investigations:
Leucopenia, and mild proteinuria and bilirubinuria occur early in the course of the disease.
The levels of AST, ALT, bilirubin, and alkaline phosphatase usually are elevated.
PT and PTT may be prolonged with severe liver involvement.
Definitive diagnosis is made using serologic markers—anti-HA IgM, HBsAg, HC PCR,
anti-HBc IgM, HD PCR, anti-HE IgM. Liver biopsy, which should be avoided during
pregnancy.
The differential diagnosis of viral hepatitis:
should include viruses A, B, C, and D; Epstein-Barr virus; cholestasis; preeclampsia;
AFLP; toxoplasmosis, other agents, rubella, cytomegalovirus, and herpes simplex
(TORCH) infections; secondary syphilis; autoimmune; and toxic or drug-induced
hepatitis. Additionally, intrahepatic or extrahepatic bile duct obstruction should be
included.
Treatment
Immunoglobulin prophylaxis should be given to pregnant women
within 2 weeks of exposure to hepatitis A.
Two hepatitis A vaccines using inactivated virus are available and can
be used during pregnancy.
All pregnant women should routinely be tested for HBsAg during an
early prenatal visit in each pregnancy and Hepatitis B vaccine should
be administered to an HBsAg-negative woman.
Hepatitis B Ig can be given to patients who are parenterally or
sexually exposed to blood or secretions from hepatitis B–infected
individuals.
Interferon and ribavirin therapy improves the prognosis for chronic
active hepatitis (C in particular), but both drugs are relatively
contraindicated during pregnancy.
In symptomatic case:
Bed rest should be instituted during the acute phase of illness, if
nausea, vomiting, or anorexia is prominent, intravenous hydration
and general supportive measures are instituted. All hepatotoxic agents
should be avoided.
Antepartum fetal assessment should be instituted in the third trimester
because of the increased risks for premature delivery and stillbirth.
During labour: Fetal scalp electrode and FBS should be avoided to
prevent vertical transmission. There is no evidence of the advantage
of delivery by C/S over vaginal delivery in preventing perinatal
infection of the baby.
Passive immunization by Ig in the 1st 24 hours for the newborn of
woman with high infectivity, and active immunization of the newborn
is 85–95% effective in preventing perinatal transmission of hepatitis B
virus. Neonates infected at birth have a>90% chance of becoming
chronic carriers.
Breastfeeding is not contraindicated with hepatitis B if the infant has
been immunized.
Complications & Prognosis:
The maternal course of viral hepatitis is generally unaltered by pregnancy, except in
hepatitis E the pregnant woman has 15% risk of fulminant hepatic failure and 5% risk of
mortality.
prematurity may be increased in viral hepatritis.
Liver transplant and pregnancy:
Pregnancy in women with liver transplants has been reported and, in general, has an
uncomplicated prenatal and delivery course. Treatment with immunosuppressants and
corticosteroids is generally well tolerated in pregnancy.
Chronic liver disease and pregnancy:
Severe hepatic impairment is associated with infertility. Liver disease may decompensate
with pregnancy, and pregnancy should be discouraged in women with severe impairment
of liver function.
If there are portal hypertension and oesophageal varices there is increased risk of bleeding
in the 2nd and 3rd trimesters.
Thyroid disorders in pregnancy
Thyroid disease is the commonest endocrine disorder in pregnant women.
THYROID FUNCTION IN NORMAL PREGNANCY
Thyroid volume increases by approximately 30% during pregnancy and this return to
normal over a 12-week period postpartum. In early pregnancy (hCG) may suppress
thyroid-stimulating hormone (TSH) because they share a common α-subunit.
Thyroid-binding globulin concentrations double during pregnancy by the effect of
estrogen on the liver. Overall, free plasma (T3) and thyroxine (T4) concentrations remain
at the same levels as outside pregnancy (although total levels are raised) and most
pregnant women are euthyroid. Free T4 may fall in late gestation.
(T4)and (T3) return to normal within 4 weeks post-partum.
The fetus cannot synthesize (T4)and (T3) until the 10th week of gestation, and it is
therefore dependent upon transplacental transfer of the maternal hormone.
In areas of relative iodide deficiency maternal hypothyroxinaemia and goiter may
develope.
1- HYPOTHYROIDISM
Overt hypothyroidism causes subfertility, and the presence of thyroid autoantibodies, even
if the mother is euthyroid, is associated with an increased risk of miscarriage
Hypothyroidism affects approximately 1% of pregnant women and the most common
cause is iodine deficiency. Providing thyroxine replacement therapy is adequate,
hypothyroidism is not associated with an adverse pregnancy outcome for the mother or
fetus.
In poorly controlled hypothyroidism and a variety of adverse outcomes, which may
include congenital hypothyroidism and cretinism of the offspring, fetal growth restriction,
maternal hypertension, placental abruption, premature delivery, and post-partum
haemorrhage. Severe hypothyroidism affects the subsequent intelligence of the offspring
of affected mothers.
Women with hypothyroidism should be given thyroxine replacement at a dose that
ensures a FT4 at the upper normal range appropriate for each trimester of pregnancy
{Thyroid function in normal pregnancy}
2- HYPERTHYROIDISM
Hyperthyroidism affects 1 in 500 pregnant women.
Causes:
90% of hyperthyroid patients have Graves’ disease, other less common causes are: toxic
nodule, hashimoto's thyroiditis, multinodular goiter, hyperemesis gravidarum, and
trophoblastic disease (very rare).
Graves’ disease is caused by TSH receptor stimulating antibodies.
{The disease is usually present before pregnancy and may remit during the
latter trimesters therefore treatment may need to be reduced or stopped.
In the post-partum period the disease may require treatment with the same or
higher doses of antithyroid medication}.
Management:
Most of the patients are treated as an outpatient, except in severe uncontrolled cases
where hospitalization is considered.
Treatment during pregnancy is almost always consisting of antithyroid drugs
like: propylthiouracil, or carbimazole to inhibit thyroid hormone synthesis. There is no
evidence that either drug is associated with congenital abnormalities.
However, a greater proportion of carbimazole enters breast milk, and therefore
propylthiouracil is usually the drug of choice if a woman is diagnosed as having
hyperthyroidism for the first time during pregnancy.
Propylthiouracil and carbimazole both cross the placenta; However, fetal hypothyroidism
is rarely seen.
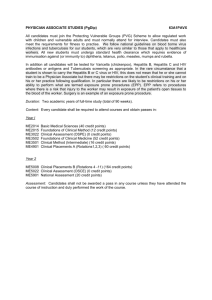
TSH receptor stimulating antibodies also cross the placenta and may influence the fetal
and neonatal thyroid status as shown in the figure below.
Fetal wellbeing should be assessed well by serial U/S to assess fetal growth.
Radioactive iodine is an option of treatment but contraindicated during pregnancy
because it affect the fetal thyroid and lead to fetal hypothyroidism.
Complications:
Women with well-treated disease rarely have maternal complications of pregnancy. Poorly
controlled hyperthyroidism is associated with several pregnancy complications, including
1) maternal thyrotoxic crisis (triggered by stress of labor),
2) miscarriage,
3) gestational hypertension,
4) pre-eclampsia, and
5) anemia.
Fetal complications: include intrauterine growth restriction, prematurity, fetal and
neonatal hyperthyroidism, goiter, and still birth.
Fetal and neonatal effects of transplacental passage of TSH receptor stimulating antibodies
3- POST-PARTUM THYROIDITIS:
Post-partum thyroiditis is associated with the presence of thyroid antiperoxidase
antibodies. Incidence 2-5% of all women. It is characterized by an initial (hyperthyroid
phase) that occurs 4-8 weeks post-partum, followed by a (hypothyroid phase), which
usually resolves within few weeks to few months after delivery.
The hypothyroidism may require treatment with thyroxine, but treatment should be
stopped after 1 year as the condition resolves. The likelihood of developing subsequent
hypothyroidism is 5%, and for this reason affected women should have their thyroid
function checked regularly.
Neurological conditions
Serious manifestations of neurological disease are fortunately rare in pregnancy, though
cerebral haemorrhage remains a significant cause of maternal death. Epilepsy and
migraine are common causes of morbidity.
Epilepsy
Women of childbearing age who suffer from epilepsy and are on maintenance therapy
must have their treatment reviewed and monotherapy is recommended if at all possible.
Antiepileptic drugs can cause teratogenicity and folic acid 5 mg daily is generally
prescribed in view of the relative folate deficiency of many mothers on antiepileptic
therapy. It is important that control of seizures is achieved to minimize maternal morbidity
(fits can be fatal) and patients must be monitored during pregnancy to ensure that dose
adjustments are made as appropriate. Sodium valproate is the major cause for concern in
the second and third trimesters in the light of data suggesting increased educational needs
in children exposed in utero.
All patients should receive anomaly ultrasound assessment to exclude specific
abnormalities associated with their medication. These are specifically orofacial clefts,
neural tube defects and craniofacial dysmorphism. Vitamin K is recommended to be given
from 36 weeks onwards to prevent neonatal bleeding disorders. Epileptic seizures may
occur during labour and as such may confuse the diagnostic situation that includes
eclampsia. Epileptic seizures should be treated in these circumstances as they would be
normally and may be reduced with the use of epidural anaesthesia. Post-partum drug doses
may need to be adjusted if doses have been increased during pregnancy. Specific advice
must be given to epileptic women about childcare, for example, not bathing the baby on
their own, and patient organizations offer information leaflets for patients, which are
invaluable .
Migraine
Headaches are a common problem in pregnancy and migraine sufferers may find their
symptoms worsen during the first trimester. Many patients may be using ergot alkaloids to
treat migraine prior to the onset of pregnancy and they must be advised not to use these
during pregnancy. Migraines may improve considerably in the second and third trimesters
but in patients in whom continuing problems exist, the strategies that are employed for
prophylaxis are low-dose aspirin, paracetamol and codeine as pain relief and propranolol if
attacks continue to be troublesome despite these measures.