Pituitary Hypothalamus (updated 2002)(2)
advertisement
(2)")
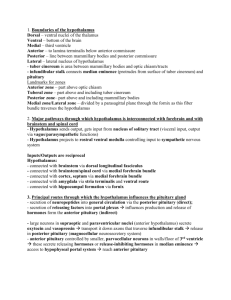
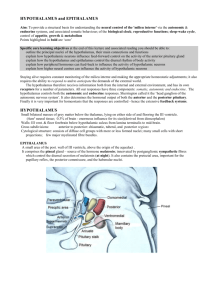
Pituitary & Hypothalamus Notes Compiled by Sid Dickson ~ with some modifications by Kira Armstrong ~ 9/7/02 ANATOMICAL AND CLINICAL REVIEW The pituitary and hypothalamus constitute a unique region of the nervous system. In addition to conventional synaptic transmission, both structures utilize soluble humoral factors as a major source of afferent and efferent information. The pituitary and hypothalamus form the link between the neural and endocrine systems The hypothalamus is the central regulator of homeostasis The hypothalamus interacts with and helps regulate “H.E.A.L.”: Homeostatic – hunger, thirst, sexual desire, sleep-wake cycles, etc. Endocrine – control of endocrine system via pituitary Autonomic control Limbic mechanisms (Chp. 18) Overall Anatomy of the Pituitary and Hypothalamus * Fig. 17.1 (p.738) depicts the embryological development of the anterior and posterior pituitary the hypothalamus is part of the diencephalon and it forms the walls and floor of the inferior portion of the third ventricle (recall the third ventricle is like two dinner plates placed together) it is separated from the thalamus by a shallow groove on the wall of the third ventricle called the hypothalamic sulcus on the ventral surface of the brain, portions of the hypothalamus can be visualized just posterior to the optic chiasm (the tuber cinereum, or “gray protuberance”, between the chiasm and mammilary bodies, and the mammilary bodies themselves which form the posterior portion of the hypothalamus) infundibulum (“funnel”) arises from tuber cinereum and continues inferiorly as the pituitary stalk the anterior portion of the infundibulum is called the median eminence, where hypothalamic neurons release regulating factors that are carried by portal vessels to the anterior pituitary the pituitary gland lies within the pituitary fossa, which is bounded by the anterior clinoid process and posterior clinoid process, which, together with parts of the sphenoid bone, form the sella turcica (“Turkish saddle”) the sella turcica is just above the sphenoid sinus, which allows the pituitary fossa to be accessed by a transphenoidal surgical approach (e.g., to resect pituitary tumors) within the pituitary fossa the pituitary is surrounded by dura the pituitary stalk communicates with the main cranial cavity through a round hole (in the middle of the diaphragma sella) the lateral walls of the pituitary fossa form the cavernous sinus given the location of the pituitary and other “sellar” and “suprasellar” structures just behind and inferior to the optic chiasm, tumors in this region can compress the optic chiasm causing visual problems, including bitemporal hemianopia (see KCC 11.2) SEE Fig. 17.2 (p.739) to familiarize yourself with the location of these structures; the pituitary fossa can be seen in Fig. 12.1, 12.3A; pp. 460, 465) THE FINE PRINT: Caveat emptor! These study materials have helped many people who have successfully completed the ABCN board certification process, but there is no guarantee that they will work for you. The notes’ authors, web site host, and everyone else involved in the creation and distribution of these study notes make no promises as to the complete accuracy of the material, and invite you to suggest changes. Pituitary and Hypothalamus ~ 2 ~ IMPORTANT HYPOTHALAMIC NUCLEI AND PATHWAYS Major Hypothalamic Nuclei The hypothalamic nuclei can be divided into four major regions, from anterior to posterior (Fig. 17.3) and into two different medial and lateral areas (Fig. 17.4) (pp.740-741) Fibers of the fornix pass through the hypothalamus on the way to the mammilary body, dividing the hypothalamus into a medial hypothalamic area and a lateral hypothalamic area Lateral hypothalamic area: lateral hypothalamic nucleus and several smaller nuclei Medial forebrain bundle: carries many connections to and from the hypothalamus, and between other regions Periventricular nucleus: thin layer of cells lying closes to third ventricle Preoptic area: embryologically “separate” from the hypothalamus, but functionally part of the hypothalamus Lateral preoptic nucleus and medial preoptic nucleus: rostral continuations of the lateral and medial hypothalamic areas, respectively Anterior to Posterior: Some neurons located in both the supraoptic and the paraventricular nuclei contain oxytocin or vasopressin and project to the posterior pituitary The suprachiasmatic nucleus (SCN) is the “master clock” for circadian rhythms; it receives inputs from retinal ganglion cells conveying information about day-night cycles The arcuate nucleus is one of the hypothalamic nuclei projecting to the median eminence to control the anterior pituitary. Hypothalamic Control of the Autonomic Nervous System descending autonomic fibers originate mainly from the paraventricular nucleus and project to the brain stem and spinal cord. inputs to the hypothalamus that regulate autonomic function come from numerous synaptic and humoral (chemical) sources. One important input source is the amygdala and other regions of the limbic cortex Hypothalamic-Limbic Pathways the subiculum of the hippocampal formation, a limbic structure, projects to the mammillary bodies of the hypothalamus via the fornix the mammillary bodies project via the mammillothalamic tract to the anterior thalamic nucleus, which in turn projects to limbic cortex in the cingulate gyrus. The amygdala has reciprocal connections with the hypothalamus via the strial terminalis and the ventral amygdalofugal pathway. These connections explain the relationship between emotional factors and autonomic responses. This is why your palms get sweaty and your stomach feels bad when you’re very nervous. The connection with homeostatic pathways include the immune system as well. This explains why depressed individuals may be more susceptible to infection Other Regionalized Functions of the Hypothalamus the lateral hypothalamus is important in increasing appetite; lesions to this area cause a decrease in body weight the medial hypothalamus, especially the ventromedial nucleus, appears to be important in inhibiting appetite, and medial hypothalamic lesions can cause obesity thirst appears to result from the activation of osmoreceptors in the anterior regions of the hypothalamus the anterior hypothalamus appears to detect increased body temperature and activates mechanisms of heat dissipation; anterior hypothalamus lesions can cause hyperthermia. The posterior hypothalamus functions to conserve heat. Sexual development and differentiation involves an interplay of neural and endocrine signals, many of which appear to be regulated by the hypothalamus THE FINE PRINT: Caveat emptor! These study materials have helped many people who have successfully completed the ABCN board certification process, but there is no guarantee that they will work for you. The notes’ authors, web site host, and everyone else involved in the creation and distribution of these study notes make no promises as to the complete accuracy of the material, and invite you to suggest changes. Pituitary and Hypothalamus ~ 3 ~ - Endocrine functions of the Pituitary and Hypothalamus the pituitary receives arterial blood from the inferior and superior hypophysial arteries, which are both branches of the internal carotid artery The anterior pituitary produces six important hormones: 1) adrenocoticotropic hormone (ACTH) stimulates the adrenal cortex to produce corticosteroid hormones, which are important for maintaining blood pressure, controlling electrolyte balance, and promoting glucose mobilization into the blood stream. 2) growth hormone (GH) causes the liver, kidneys, and other organs to produce insulin-like growth factors which promote increased growth of the long bones and other tissues 3) prolactin causes the mammillary glands to produce milk 4) thyroid-stimulating hormone (TSH) stimulates the thyroid gland to produce hormones (T4 and T3) which promote cellular metabolism 5) luteinizing hormone (LH) regulate ovarian hormones responsible for the menstrual cycle and oogenesis in females regulates testicular hormones and spermatogenesis in males 6) follicle-stimulating hormone (FSH) (same functions as LH) regulate ovarian hormones responsible for the menstrual cycle and oogenesis in females regulates testicular hormones and spermatogenesis in males The Posterior Pituitary produces: 1) oxytocin causes contractions of smooth muscle in the breast for milk letdown and contractions of the uterus during labor 2) vasopressin (antidiuretic hormone) participates in osmotic regulation by promoting water retention by the kidneys, allowing concentration of the urine Clinical Notes When a deficiency across all pituitary hormones occurs, this is called panhypopituitarism, which can be caused by several lesions or conditions of the pituitary and hypothalamic regions. On rare occasions, pituitary tumors can undergo spontaneous hemorrhage resulting in pituitary apoplexy. Patients with pituitary apoplexy present with sudden headache, meningeal signs, unilateral or bilateral cavernous sinus syndrome, visual loss, hypotension, and depressed level of consciousness. Pituitary adenoma The most common sellar or suprasellar region abnormality that causes endocrine disturbance, but other lesions in this region that can produce similar clinical symptoms include craniopharyngioma, aneurysms, meningioma, and other lesions. a) a slow-growing histologically benign tumor arising from cells in the anterior pituitary b) mean age of diagnosis is 40 years; some cases occasionally occur in adolescents or elderly c) the pituitary will often continue to secrete hormones, but at abnormally high levels, resulting in several endocrinological syndromes – even small pituitary tumors (e.g., <1mm) can cause significant endocrine abnormalities THE FINE PRINT: Caveat emptor! These study materials have helped many people who have successfully completed the ABCN board certification process, but there is no guarantee that they will work for you. The notes’ authors, web site host, and everyone else involved in the creation and distribution of these study notes make no promises as to the complete accuracy of the material, and invite you to suggest changes. Pituitary and Hypothalamus ~ 4 ~ d) some adenomas do not result in abnormal hormone secretion but rather grow large and thereby leading to hydrocephalus and brainstem compression which leads to headaches and/or visual disturbances (e.g., bitemporal hemianopia – characteristic sign) e) treatment options include medication, surgery, and radiotherapy f) if surgery is indicated, a transsphenoidal approach is usually taken (i.e., through the sphenoidal sinus, usually by means of pathway through the mouth and/or nose) g) prolactin secreting adenomas typically cause amenorrhea in women, hypogonadism in men, and galactorrhea, infertility, hair loss, decreased libido, and weight gain in both sexes. h) Growth hormone-secreting adenomas cause acromegaly, a slowly progressive overgrowth of bones and soft tissues – can lead to gigantism in adolescence. It can also lead to arthritis, infertility, hypertension and/or diabetes) i) ACTH-secreting adenomas cause Cushing’s disease which results in “cushingoid” appearance (round moonshaped facies and truncal obesity) and acne, hirsutism, purplish skin striae, thin-appearing skin, easy bruising, poor wound healing, hypertension, diabetes, edema, immunosuppression, osteoporosis, avascular necrosis of the femoral head, amenorrhea, decreased libido, myopathy, fatigue, and psychiatric disturbances including mania, psychosis, and depression. j) The dexamethasone suppression test is often used in diagnosis of adenomas. k) TSH-secreting adenomas are a rare cause of hyper- and hypothyroidism (which are more commonly caused by thyroid d/o’s like Grave’s disease and tumors) Diabetes insipidus (DI) a) production of large amounts of dilute urine b) can be caused by deficiency of ADH in neurogenic DI or by insensitivity of the kidneys to ADH in nephrogenic DI c) symptoms include severe thirst, polyuria, and polydipsia d) neurogenic DI (also called central DI) usually caused by neurosurgery, head trauma, or neoplastic lesions in the pituitary-hypothalamic region or in the third ventricle Hyperthyroidism symptoms include: nervousness, insomnia, weight loss, tremor, excessive sweating, poor temperature regulation, and frequent bowel movements thyroid opthalmopathy – inflammation of orbital tissues proximal muscle weakness, tremor, dyskinesias and dementia Hypothyroidism lethargy, weight gain, cold intolerance, hair loss, depression and constipation neuropathy, carpal tunnel, myalgia, ataxia and dementia when untreated in utero or infancy can lead to cretinism – MR, short stature, microcephaly THE FINE PRINT: Caveat emptor! These study materials have helped many people who have successfully completed the ABCN board certification process, but there is no guarantee that they will work for you. The notes’ authors, web site host, and everyone else involved in the creation and distribution of these study notes make no promises as to the complete accuracy of the material, and invite you to suggest changes.