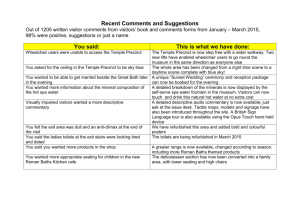
adult seating clinic referral form
advertisement

Regional Rehabilitation Outpatient Services Adult Wheelchair & Seating Clinic Hamilton Health Sciences Corporation, General Site Regional Rehabilitation Centre, 237 Barton St. East, Bldg. 2, Hamilton, ON L8L 2X2 Telephone: (905) 521-2100, Ext. 40806 Fax: (905) 521-2359 THIS PAGE TO BE COMPLETED BY PHYSICIAN CLIENT NAME____________________________________________PHONE_________________________ ADDRESS________________________________________________________________________________ ________________________________________________________POSTAL CODE____________________ DATE OF BIRTH ______/______/______HEALTH INSURANCE #__________________________________ D M Y RELEVANT DIAGNOSIS _________________________________ LENGTH OF TIME ________________ PERTINENT MEDICAL INFORMATION (include conditions, allergies & medications which may affect seating prescription)_________________________________________________________________________ __________________________________________________________________________________________ Current Medical Status_______________________________________________________________________ __________________________________________________________________________________________ Physician Name (please print): ________________________________________________________________ Address: _________________________________________________________Postal Code: ______________ Phone: ( )____________________________________Fax: ( )_______________________________ Physician Signature ________________________________________________ Date ____________________ Page 1 of 3 December 7, 2009 Regional Rehabilitation Outpatient Services Adult Wheelchair & Seating Clinic Name_________________________________________________Phone ________________________ Address______________________________________________________________________________ _______________________________________________________Postal Code____________________ Date of Birth ______/______/________ D M Y Health Card Number _______________________________ Version Code__________ Expiry Date_________________ Family Physician ___________________________________________Phone______________________ Do you have a Community Therapist? Yes No Therapist’s Name __________________________________ Agency ______________________________________ Phone _______________________ Yes Has there been any equipment trials recently completed ? Do you currently have a wheelchair? Manual Wheelchair Power Wheelchair Yes Model Model Do you have special seating in your wheelchair? Back Support Cushion Manual tilt/recline Other What are your current wheelchair/seating concerns? Pain/Comfort Posture/Sitting support Condition of current wheelchair Other Comments Page 2 of 3 December 7, 2009 No No Yes No Side Supports Tray Power tilt/recline Elevating legs Pressure area/Skin breakdown Mobility What are your goals for clinic involvement? New manual wheelchair Improved posture New back support Improved mobility Other (specify) Comments New power wheelchair Improved pressure reduction (manual/power tilt) New cushion Power of Attorney for Personal Care (if applicable) or Substitute Decision Maker Name Power of Attorney for Finances (if applicable) Relationship Name Phone Relationship Phone Vendor for wheelchairs and seating (see attached list) Vendor for custom seating Consent for Personal Information: I give consent to the Adult Wheelchair and Seating Clinic to collect information about me related to my need for wheelchair and seating/positioning. I understand that this information may be disclosed, as needed, to other members of the care team including, but not limited to, family doctor/referral source, vendor, Ministry of Health Assistive Devices Program (ADP). I understand that the collection and disclosure of information is within the guidelines as established by the Privacy Policy. _______________________________________________________________________________________ For use of Email Communication only: This section disregarded-email communication NOT appropriate OR I agree to allow personal and health information to be sent via email, even though I am aware it may not be secure. Yes No Pertinent information about me may be sent to the following : equipment supplier Family member Other: Signature Date If signature is other than client, please identify relationship This form must be completed in full before an appointment can be made Return to : Eleanor Walters, Intake Coordinator Hamilton Health Sciences Regional Rehabilitation Centre 237 Barton St. East, Bldg. 2, Hamilton, ON L8L 2X2 Phone: (905) 521-2100 Ext. 40806 Page 3 of 3 December 7, 2009 FAX: (905) 521-2359