Introduction - Harvard University Department of Physics
advertisement

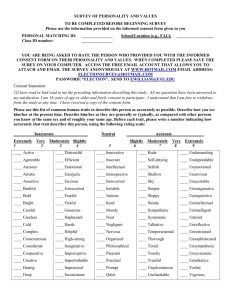
Proposal to switch from explicit consent to presumed consent organ donation legislation in Massachusetts Sarah Harland-Logan and Josh Feng Introduction The organ shortage: looking at the numbers Over 94 000 people are currently awaiting an organ transplant in the United Statesi; one of these people will die every ninety minutesii. While the number of deceased donors has increased substantially in recent yearsiii, the waiting list nonetheless increased by approximately 45% between 1995 and 2004iv. And as the waiting list increases in size, the average amount of time that organ transplant candidates spend on this list correspondingly increases. Between 1995 and 2001, the median time spent on the waiting list prior to receiving a kidney transplant (by far the common organ transplantv) increased from 918 to 1176 daysvi. In short, the supply of organs for transplant—the vast majority of which are obtained from deceased donors, though a few organs can also be obtained from living donors—is falling far short of the demand for these organsvii. This shortfall is particularly tragic in light of the fact that every year, thousands of people who could have become organ donors after their death, do not; since each organ donor yields 2.8 organs on average, several thousand people die unnecessarily on the waiting list each year. It is clear that the current system for organ donation and transplantation in this country is broken, and that the search for a more effective system should be a national priority. In order to determine what new approaches we might take to address the problem of organ shortages, we need to understand how the current system works—and why, in the end, it doesn’t. The current system The current system for procuring organs for transplant in the United States is based on two principles: first, that organ donation is beneficial to society and so should be encouraged and promoted; second, that organ donation must be a free choice on the part of the individual, and that the individual’s right to make this decision for him- or herself outweighs in this case the individual’s obligation to act in the interest of society. Any attempt to alter or to replace the current system must respect these two fundamental principles. Current legislation exists at both the federal and the state level to uphold these two principles. We summarize below the pieces of legislation that are crucial to an understanding of how the current system works. At the Federal Level (1) Title 42 Section 274 establishes the Organ Procurement and Transplantation Network (OPTN), “the national organization that coordinates, implements, and monitors the organ transplantation system as a whole”viii. The United Network of Organ Sharing (UNOS) administers the OPTN and collects its dataix. (2) Title 42 Section 273 lists the guidelines to qualify as an Organ Procurement Organization (OPO)x. OPOs are the “local or regional organizations responsible for retrieving organs and notifying potential recipientsxi; there are fifty-eight OPOs in the United States, the jurisdictions of which generally correspond loosely with state boundariesxii. (3) Title 42 Section 274e prohibits a market in organs.xiii At the State Level (1) All fifty states and the District of Columbia have adopted the 1968 Uniform Anatomical Gift Act, which states principally that: any person at least eighteen years of age and competent to make informed decisions can consent to the removal upon his or her death of his or her organs for donation; consent may take the form of a will or of any document, signed by the deceased and witnessed by two other people, giving express consent to the removal of his or her organs for donation after death; the deceased’s next of kin can also consent to donate his or her organs in the absence of any statement indicating that the deceased did not with to be an organ donor. (2) Twenty-four states, not including Massachusetts, subsequently adopted the 1987 Uniform Anatomical Gift Act, which states principally: that the procurement staff do not require the consent of the next of kin in order to remove organs from a person who has given his or her consent; and that witnesses are not required to validate a written statement that one wishes to become an organ donor upon one’s death. (3) All fifty states issue driver’s licenses on which the individual can state his or intent to become an organ donor.xiv Explicit, First-Person, and Family Consent A key feature of current organ donation law in the United States is explicit, firstperson consent: the only way to become an organ donor is to give explicit consent to having one’s body used in this way after death. Every state allows the individual to give his or her explicit consent in several different ways; in Massachusetts, one can give express consent through each of the following: “an organ and tissue donor card, inclusion in a donor registry, a statement attached to or imprinted on a driver's license or an identification card issued by the registrar of motor vehicles, a will or other writing”xv. Massachusetts is one of only three states, however, where explicit, first-person consent is necessary but not sufficient to become an organ donor. The family of the deceased must be informed prior to organ removal, whether or not the deceased has given his or her express consent. Organ removal cannot proceed if the family objectsxvi. Presumed consent: A better choice Over twenty countries have enacted presumed consent legislation in response to the shortage of organs for transplantxvii. In essence, “presumed consent” means changing the “default setting” for organ donation from non-donor to donor: instead of having to “opt in” to become an organ donor by giving explicit consent to this effect, every potential donor is presumed to have given consent unless he or she has “opted out” by expressly stating that he or she does not wish to be a donor. There are two distinct versions of presumed consent, “hard” and “soft”. In hard presumed consent, the procurement team can remove the deceased’s organs without the family’s consent, whereas in “soft” presumed consent, the family’s consent is required in order for donation to proceedxviii. Countries that have implemented presumed consent legislation have been able substantially to reduce their organ transplant waiting listsxix, and so have saved many thousands of lives. Presumed consent legislation, when properly implemented, strikes a balance far superior to that of the current system between protecting the autonomy and dignity of the individual, and saving lives that today are lost needlessly. In addition, presumed consent is relatively inexpensive to implement. Below, we consider the evidence that presumed consent is indeed responsible for the comparatively high organ donation rates of the countries that have implemented it, and demonstrate that a switch to presumed consent legislation in this country does in fact have the potential substantially to reduce the waiting list and therefore to save thousands of lives each year. We also address the most common practical, legal, and ethical arguments invoked against presumed consent and show how the objections raised by each of these arguments are either ill-founded or removable through particular approaches to implementing presumed consent legislation. Recommendation In light of this analysis, we recommend that individual states take the challenging but worthwhile step of switching from express consent to the hardest form of presumed consent that is currently feasible. Specifically, we recommend that Massachusetts implement soft presumed consent—with the goal of eventually switching to hard presumed consent—in such a way that: the public is aware of the change in legislation and understands what the change entails; provided that it is easy for an individual to opt out, and there are several different ways to do so; and that in general the new presumed consent law is as closely parallel to the current explicit consent law as is possible. It is time for Massachusetts to take this admittedly challenging but vital step. What presumed consent is not Many of the most common objections to presumed consent stem from misconceptions about what presumed consent actually is. Presumed consent is often confused in the public discourse with organ conscription and with the system that goes by the initially bewildering name of “mandatory choice.” Here we differentiate presumed consent from each of these approaches to organ donation. Organ conscription Organ conscription is a term used by scholars to refer to organ donation policies that require every person in the population (or within a certain subset of the population) who is eligible to donate his or her organs after death to do so. Conscription implies that the government has property rights over the individual’s body, and so can use individuals’ bodies in any way it sees fit; human organs become a national resource that the distribution of which is overseen by the government. Many scholars refer to China’s policy of removing organs from deceased political prisoners as organ conscription. Presumed consent is not in any way related to organ conscription. Consent, whether explicit or presumed, is not required or even relevant in an organ conscription system; in presumed consent, the individual maintains the right to decide what happens to his or her body after death, and the state has no right of any kind to any individual’s organs. The only way in which presumed consent differs from express consent is that consent can be implicit; consent is still an absolute requirement for organ removal to proceed. As a result, individuals are free to opt out—to choose not to be organ donors— in a presumed consent system; there is no such option in organ conscription.xx Mandatory Choice A mandatory choice law would require every person to specify whether or not he or she wishes to be an organ donor. As a result, there is no “default setting” for organ donation, and consent is not presumed. Mandatory choice resembles presumed consent only in that consent is indeed required for organ donation. Proponents of mandatory choice argue: (1) that it promotes individual freedom by ensuring that individuals will think about organ donation and make a decision based on this reflection; and (2) that many people who would not otherwise have signed up to be donors, when forced actively to choose, would decide after consideration of the societal benefits of organ donation to become donors. Opponents argue, however: (1) that while mandated choice “would force people to speak autonomously for themselves”, “it would do so by imposing a novel legal obligation upon individuals backed by the force of the state”xxi; and (2) that mandatory choice would “create a new class of explicit non-donors” without simultaneously shifting the societal norm concerning donation to “donor” as opposed to “non-donor” (as is the case in presumed consent), and thus it is possible that mandatory choice could in fact undermine the end it seeks to attain: an increased supply of organs for transplantxxii. Below, we respond to the major arguments that have been made against presumed consent per se. Why here, why now? Effect of Presumed Consent Legislation on Organ Donation Rate In a recent study done by Abadie and Gayxxiii, it is estimated that presumed consent legislation increases organ donations by roughly 26%. This result, however, does not come without qualifiers, which affect donation rates both positively and negatively. We will analyze the study in great detail, to discover where the number comes from. A direct analysis of average donation rate in the two systems yields no statistically significant difference between the two types of systems (explicit consent and presumed consent). Furthermore, if we exclude the outlier Spain, the difference drops from 16% to 10%. (Spain is often considered an outlier, because its unique donation system and significantly higher donation rates skew the difference in donation rates between the two different systems.) These results seem to support some claims that there is only a statistical difference between the two systems when the outlier is included. The results discussed so far, however, do not take into account other factors that affect organ donation rates. Intuitively, we must take average results, factor in the conditions specific to each country, and then ascertain the pure effect of a change to presumed consent legislation. The following table from Abadie and Gay attempts to quantify the effects of the characteristics of a specific country on organ donations: Table 1: Factors affecting organ donation rate (Abadie and Gay) Entire sample Presumed consent countries Explicit consent countries Difference (S.E.) (1) (2) (3) ((2) − (3)) 3.10 (1.99) −5,697 (3731) −651 (399) .5925** (.1663) −.6452** (.1576) .4638** (.1523) Presumed consent country .5634 [.4971] Cadaveric donors (per million population) GDP per capita (constant 1995 USD) Health expenditures per capita (constant 1995 USD) Catholic country Common law MVA and CVD deaths (per thousand population) 15.94 [5.35] 22366 [9768] 1930 [970] .4413 [.4977] .2817 [.4509] 1.2123 [.4374] 17.29 [6.01] 19879 [11241] 1634 [946] .7000 [.4602] 0 [0] 1.4156 [.4570] 14.19 [3.72] 25576 [6161] 2285 [880] .1075 [.3114] .6452 [.4811] .9518 [.2217] Number of countries 22 13 10 Number of observations 213 120 93 Notes: Standard deviations in brackets. Standard errors in parentheses are clustered by country. The number of countries with explicit and presumed consent laws do not sum to the total number of countries in the sample because one of the countries in the sample (Sweden) changed legislation during the sample period. ** Indicates statistical significance at the 5% level. Using these differences, we can then attempt to hypothesize the pure effect of a change to presumed consent legislation in the USA. The table below shows analyses of several data series, with trials 3 through 8 accounting for a set of attributes. Trials 2 and 8 normalize for the aforementioned outlier Spain. Only trials 3 through 8 (starred) yielded statistically significant results. The average result is around the 26% increase mentioned earlier. This proves that the prevailing notion of presumed consent having little effect is statistically misleading once other factors that affect organ donation rates are accounted for: Table 2: pure effect of implementing presumed consent in US (Abadie and Gay) Trial Increase in organ donation rate upon imlementationof presumed consent. 1 2 3 4 5 6 7 8 .1559 (.1352) .1027 (.1316) .2615** (.1206) .2577** (.1233) .2839** (.1294) .2562** (.1386) .3111** (.1238) .2493** (.1164) (Mean, (Standard Deviation)) (** indicates statistical significance.) Mathematical Models of Organ Donationxxiv Model of total people on the waiting list: X n : Waiting list people in year n. p : probability someone goes on p : probability someone on wait list passes away in a given year p d : probability that any person donates A : Number of people eligible to donate k : Fraction of population eligible to donate Model: X n 1 X n p A p X n p d kA Which reduces to: X n 1 (1 p ) X n ( p kp d ) A Assuming constant coefficients, the solution to this recursively defined function is a degree n polynomial (1 p ) n , with an extra term to account for the inhomogeneous changes in population over time (although we could well characterize population as a function of n also). Since p is not significant compared to 1, the polynomial term is almost constant. The inhomogeneous term would then represent the change from year to year. Therefore, the effective increase would be very close to a constant progression. The assumption of constant coefficients, however, is an oversimplification of current and future trends in these coefficients: p : Medical advances have allowed previously ineligible people to go on the waitlist for a transplant, so as n increases, there will be an increase in this coefficient. p : This coefficient should actually be an increasing function of the total number on the waitlist, but that would not have a significant effect on stunting the increase in numbers. It would, however, signal an increase in the number of deaths of people on the waiting list increases. p d : This is the product of people who are willing to donate times the number of people who fall into the pool of decedents (assuming that there is no correlation between the two events). This number will change under different organ donation systems. A : Population growth will shrink the increase if kpd p , but will increase the gap if kpd p . An increase in p d would curb shortage in organs. Linear Extrapolationxxv Rather than a model with many different factors, we can use a simple linear extrapolation of past waiting list numbers to estimate future numbers. Despite ignoring the theoretical non-linearity presented above, the projections paint a very bleak picture of the future of the organ donation system. Using the graph below, we can represent waiting list patient numbers as a function of the year: X (t ) 5600 (T 1992) 28500 Therefore, there will be approximately 168,500 people on the waitlist ten years from now, 224,500 people twenty years from now, and an astounding 392,500 people on the waitlist half a century from now. Figure 1: Waiting list, 1992-2002 Model of Explicit Consent vs. Presumed Consent Now, we turn to the theoretical benefits of switching to a Presumed Consent system from an Explicit Consent system to determine a rationale for a pure effect of a change in legal system. The following models are inspired by similar ones presented by Abadie and Gay.xxvi Simple Model Here, we assume here that the patient’s indication is the final say in whether he or she donates, and that cost subtracts from utility, which as we will discuss later, is not the case. Let ud be the utility gained from donating, and un be the utility derived from not donating. Finally, let A= ud - un. We will assume that A is distributed normally around some value for the people who do fall into a decedent state. Let C be the total cost of registering as an organ donor. This includes mental costs suffered through contemplation of death and also time and registration costs. Medical literature suggests that mental costs far outweigh any material costs[Abadie]. In countries under an explicit consent system, people will only register if A>C, because the increase in utility from donating would have to be greater than the costs involved with the process. In countries under a presumed consent system, people will stay donors as long as A>-C. People do not have to take the hit unless they believe strongly against organ donation. Therefore, they could avoid the very negative A by paying a less negative C. In our proposed system, the cost C will be minimized, so that people who receive positive utility from donation can do so without suffering a cost C, and people who receive negative utility from donating can opt out without any significant losses. The process of minimizing the mental and physical cost C will be discussed later. This leads to the conclusion that changing the system cannot lead to a worse yield of donated organs. In fact, if the distribution is around 0, then this difference is very large. Figure 2: The change in donations is the area under the curve between the vertical lines. The difference between the purple and light blue regions in the diagram above represents the different increases depending on the mean of the distribution. A distribution around a positive mean will reduce the effect of switching legal systems. We must also not ignore the impact of a switch in systems on the mean around which the mean is distributed. A change to presumed consent will lead to a cultural change in willingness to donate, positively shifting the distribution. If the distribution was initially around a negative mean, then this will contribute more organs, on top of the ones caused by the cost effect, if the shift is between 0 and 2x, where x is the magnitude of the initial mean. However, if the mean was distributed around a non-negative mean, then the cultural shift would detract from the increase due to costs, as shown in the diagram above. Complex Model of Organ Donation In most of the countries currently under a presumed consent system, the assumption that the donor has the final word is flawed. Most hospitals still require family consent before a decadent donates organs. Therefore, opting in or opting out is only a signaling device to the family about his or her value of A, the difference of utilities. This then opens up the possibility that the family would decide correctly without the signaling. Model Assumptions: There are two actors, a potential donor and his or her family. Both act to maximize the utility of the potential donor. Explicit consent If a decedent has registered to be a donor, then the family will follow his or her decision. If a decedent has not registered: The family, however, has imperfect information on the value of A (the difference in utilities defined above). Therefore, the value the family receives is equal to A+e, where e is distributed around a mean of zero. Therefore, the expected utility of the unregistered donor is: p(A+e<C) * un + p(A+e>C) * ud (Note: p(X) denotes the probability of X being true.) This is expected utility is weighed against the utility derived from signaling: ud – C. Rearranging terms, and noticing that the two probabilities sum to 1, we can determine the condition upon which a person does register: p(A+e<C) * A > C Presumed consent If a decedent has indicated unwillingness to donate, then the family will follow his or her decision. If a decedent has not indicated unwillingness: The family has imperfect information on the value of A. It once again receives a value of A+e. Therefore, the expected utility of the donor is: p(A+e<-C) * un + p(A+e>-C) * ud This is weighed against the utility of signaling: un – C Rearranging, people will choose not to indicate if: p(A+e>-C) * A > -C Comparing these two results, we notice that we have worked in the position of the distribution of A into the number of registered donors. We also notice that fewer people choose to signal in the explicit consent system, because the cost of signaling is not worth canceling out the probability that the family does not correctly determine the patient’s utility values. Therefore, a switch to presumed consent would have a greater effect than the one predicted by the simple model. Additionally, if the cost for opting out is close to 0, the number of people who do not wish to donate but do not opt out is negligible (see below also). Projected Effect of Presumed Consent Legislation on National Waiting List, United States Now we will project the effect on the organ transplant waitlist a change to presumed consent would have. Here, we will assume that there will be an increase of 26% to the organ donation ratexxvii on top of the current 35-43% donation rate in the United Statesxxviii. Additionally, we will use the estimate of 0.0028 as the probability that a person at age 30 will eventually fall into a decedent statexxix. Furthermore, we will make an approximation that this probability is spread evenly over each year until age 50, when a person becomes ineligible to donate. Finally, we will hold the US Population at 300 million, and attempt to estimate the number of eligible people in each given year. According to the CIA Factbookxxx, the percentage of people between 15 and 64 of age is 67.2% of the overall population. Add to this the fact that the median age is 35, and we can estimate the number of eligible people in the population as 70% of this number. Finally, we assume that the US population is a constant 300 million. This comes out to around half the population being eligible. The effect of the change on the waiting list increase will be equal, according to our model, the change in pd times the overall population. This change will equal the probability that someone falls into a decedent state, times 26% of the current donation rate, multiplied by the overall population between ages 30-50. This change comes out to about 2,200 people per year. The graph below illustrates that, despite the significant reduction in the increment, there is still a long road to eliminating the organ transplant waitlist. The pink points represent the waiting list numbers under a presumed consent system, while the dark blue points represent numbers under explicit consent. Table 3: Waiting list extrapolations Years from now 10 20 50 Explicit consent 168,500 224,500 392,500 Presumed consent 146,500 180,500 282,500 Figure 3: Waiting list extrapolations People on Waitlist Effects of PC 500000 400000 300000 200000 100000 0 2000 2020 2040 2060 2080 2100 Year Massachusetts: Prior Success with the Massachusetts Organ Donation Initiativexxxi In 2000, the state of Massachusetts launched a coordinated organ donation initiative to improve organ donation rates. At a meeting in May 1999, the Massachusetts Department of Health, hospital CEOs, and representatives from the New England Organ Bank met to discuss a means of improving organ donation rates. They agreed that organ donation campaigns had already raised public awareness and support, and that the main obstacle to reaching higher rates was family consent. Eventually, they reached a plan that involved cooperation amongst the three parties that would lead to higher donation rates. The plan had one main focus: to give sound advice to families of decedent patients at the most opportune time. First, the request for donation would be separated from the announcement of brain death. Second, trained staff from the Organ Bank instead of hospital workers would be the key players in making the donation requests. Finally, hospitals would exert greater effort to arrange a consultation during the window of possible donation (31). Initially, hospitals were wary of allowing Organ Bank staff to take over requesting, but eventually they became cooperative (33). From the table below (32), we can see that the conversion rate, the number of donors over the number eligible, rose about 35% during the initiative. There were also significant increases in referral rate (the number of families consulted over total number of families) and consent rate (the percentage of willing families after consultation). The Massachusetts organ donation initiative also had nationwide ramifications. The US Department of Health and Human Services released a report delineating measures that would improve the efficiency of the organ donation system. Many of these measures cited the improvement in organ donation rates under the Massachusetts initiative (34). The initiative also led to the implementation of Institute for Healthcare Improvement’s Rapid Replication project in several hundred medical centers across the country (34). Despite complications in sustaining the initiative, such as September 11th and the anthrax outbreak, Massachusetts has clearly been a leader and instigator in a national quest to improve organ donation rates and to quell the rapid increase in the number of people on the transplant waitlist. As a leader in the US organ donation system, Massachusetts should carefully consider the implementation of a presumed consent donation system, which should have a significant and positive impact on the organ donation system in Massachusetts. Figure 4: Effect of the Massachusetts Organ Donation Initiativexxxii We have shown that presumed consent has substantially increased the rate of organ donation in countries that have implemented it, and has the potential to be similarly successful in the United States; and that Massachusetts, through the Massachusetts Organ Donation Initiative, has established itself as a national leader in organ donation policy. We will now address the major practical, ethical and legal arguments offered against presumed consent. Response to Major Arguments against Presumed Consent Practical Argument: Presumed consent may work well in other countries, but the American public simply would not support it. Approximately 30% of respondents polled for the 2005 National Survey of Organ Donation (conducted by [cite]) indicated that they would choose to “opt out” and register as non-donors should the United States switch to a presumed consent system; 63.1% indicated that they would choose to remain organ donors; and 5.9% indicated that they did not knowxxxiii. The current conversion rate (the number of actual organ donors divided by the number of potential organ donors) in the United States is 42%[Keely— insert rest of citation]. These data suggest that, if slightly over 30% of the American population did indeed opt out under a hypothetical national system of soft presumed consent the population of organ donors might not significantly increase and could actually decline, given that a substantial proportion of families continue to choose not to donate. Response 1: The available data are not conclusive; an alternate source of data suggests that the public would in fact support presumed consent. In 2003, Goldstein and Johnson, of the Center for Decision Sciences at Columbia University, conducted an internet survey in 2003 in which participants answered three different versions of the same question: each question asked whether or not participants would choose to be organ donors given a hypothetical situation, but the circumstances under which they were asked to make this decision were different for each of the three versions. In the first version, “participants were told to assume that they had just moved to a new state where the default was not to be an organ donor” (in other words, a state using the current express consent system); in the second version, participants were told to assume that they had moved to a state using an opt-out system of organ donation (presumed consent); and in the third version, participants were told to assume that there was no default in place (mandatory choice)xxxiv. 42% of participants given the express consent version indicated that they would choose to donate, while 82% of participants given the presumed consent version and 79% of participants given the mandatory choice version indicated that they would choose to donate. These results contradict the National Survey of Organ Donation results, suggesting that a much higher percentage of the public might support presumed consent. Response 2: Public resistance to presumed consent would be minimized through an extensive education campaign. A striking feature of the above survey is that the presumed consent question did not use the term “presumed consent,” which has acquired negative connotations due to public confusion of presumed consent and with mandatory consentxxxv; perhaps some of the discrepancy between the results of this survey and the results of the National Survey of Organ Donation could be explained simply by the different phrasing of the two presumed consent questions. Goldstein and Johnson’s results imply that most people would choose to be organ donors in a presumed consent system, given that they understand what presumed consent actually entails. Therefore, an extensive public education campaign would be essential to the implementation of presumed consent, not only because it is morally imperative that people be aware of such a profound and personal change in legislation, but also because public education is likely to increase donation rates. Since approximately 85% of Americans approve, in principle, of organ donation, it seems likely that the majority of Americans simply don’t bother to become organ donors under the express consent system; therefore, removing this obstacle to donation by making donation the “no-action default”xxxvi, combined with extensive public education to inform the public of this change and to dispel misconceptions about presumed consent, should eventually result in a presumed consent rate approaching 85%. Response 3: In the end, the only way to determine if American citizens would support presumed consent legislation is to implement such legislation. No matter how many opinion polls we conduct, there is only one way to find out if American citizens will actually accept presumed consent legislation, and that is to implement such legislation in one or more states. Presumed consent has been highly successful in many countries, and clearly has the potential—given an extensive public education campaign—to be a viable policy option in America; but we will never learn if this option could indeed save thousands of lives here, as it does elsewhere, unless at least one state implements presumed consent. We recommend that Massachusetts build on its previous success as an innovator in organ donation policy by enacting presumed consent legislation. Ethical Argument A: Presumed consent undermines individual liberty, a key American value. Since presumed consent by definition assumes that the individual can give consent without doing so explicitly, one common objection to presumed consent is that it downplays or subverts the autonomy of the individualxxxvii. Response 1: Presumed consent does not limit the individual’s ability to make a free choice, since: the same set of choices is available to the individual under express consent and presumed consent; neither choice requires the exertion of unreasonable effort; the public will be educated about the presumed consent system. This objection can be mitigated by implementing presumed consent in the following manner: (1) Any signed and witnessed statement is acceptable in Massachusetts for the purpose of giving express consent to donate one’s organs. Therefore, under presumed consent, any signed and witnessed statement expressly denying consent to be an organ donor should be acceptable for the purpose of opting outxxxviii. (2) Massachusetts currently operates an electronic organ donor registry[find citation]; therefore, upon the enactment of presumed consent legislation, Massachusetts should replace the donor registry with a non-donor registry. (3) The state currently issues donor cards along with driver’s licenses, and provides specially marked license plates to drivers who choose to be organ donors, in order to facilitate the carrying out of their wishes in the event of their death in a motor vehicle accidentxxxix; therefore, under presumed consent, the state should issue non-donor cards along with driver’s licenses, and provide specially marked license plates to drivers who choose not to be organ donors. (4) Funeral directors are currently required to provide information about organ donation to potential clientsxl; therefore, funeral directors should still be required to provide these resources in a presumed consent system. In short, presumed consent should be implemented so that this legislation would mirror existing legislation as closely as possible. And, as previously stated, the switch to presumed consent would need to be accompanied by an extensive public education campaign. Implementing presumed consent in this manner would ensure that the individual is: aware of the choice to be made—whether or not to be an organ donor (this is the same choice that the individual makes in the context of the current express consent system); aware that the no-action default is being an organ donor; aware of the actions that he or she can take to opt out; and easily able to carry out these actions. Therefore, presumed consent need not in any way restrict the individual freedom of choice that is present in the express consent system. It is also reassuring to note that Goldstein and Johnson found that most people chose to remain organ donors under presumed consent in a situation where opting out required no more effort than staying in (both required the participant simply to click a mouse)xli. In practice, of course, opting out will always be slightly harder than remaining “in”, but Goldstein and Johnson’s finding suggests that the ethically necessary step of making it as easy as possible to opt out will not substantially compromise the practical success of presumed consent legislation. Response 2: Presumed consent not only preserves individual liberty, it promotes another core American value, altruism. Presumed consent legislation assumes that people will choose to act altruistically—to give their organs after death to strangers who desperately need these organs—unless they specify that for whatever reason they do not wish to act altruistically. Presumed consent legislation therefore promotes this core American value while preserving the core American value of individualism. Ethical Argument B: Organs will inevitably be removed from some people who did not wish to be donors but failed, for whatever reason, to opt out. Response 1: An extensive education campaign will reduce this risk. Response 2: Providing several means of becoming a non-donor, and specifically of adding one’s name to the state-wide non-donor registry, will reduce this risk. Response 3: More people’s wishes will be respected under presumed consent than are respected under the current system (and as a result, under presumed consent the burden to exert effort to express one’s wishes falls to the minority). Since 85% of the population supports organ donationxlii, it is clear that enacting presumed consent would serve the interest of the majority in that the no-action default would be in accordance with the wishes of the majority; the burden of action would fall to the minority who do not wish to be organ donors. Therefore, there is a higher probability that an individual’s wishes will be disrespected by failing to remove their organs in the explicit consent system than that an individual’s wishes will be disrespected by removing their organs in the presumed consent system. Response 4: While it is true that removal and non-removal of organs contrary to one’s wishes are not morally equivalent actions, the moral evil of occasional removal of organs against one’s wishes under presumed consent is outweighed by the moral evil of allowing people needlessly to suffer and die under the express consent system. It is inevitable that, under presumed consent legislation, an individual’s organs would occasionally be removed against his or her will, no matter how many precautions were taken against this event. While every such occurrence would indeed be highly unfortunate, it is not merely unfortunate but tragic that several of the approximately seventeen people who will die todayxliii on the UNOS waiting list will die unnecessarily. Each of these events represents a moral evil that society must attempt to abolish or at least to reduce; but the magnitude of the moral evil currently resulting from the explicit consent system far outweighs the magnitude of the moral evil that would result from the presumed consent system, assuming that presumed consent is implemented as specified above. Therefore, presumed consent is the ethically preferable option. Response 5: Initial implementation of soft presumed consent will initially reduce this risk. As we noted above, Massachusetts is one of only three states that do not have a first-person consent law, which means that every potential donor’s family must consent to donation, even when the potential donor has expressly given his or her consent. Since the family currently plays a crucial role in organ donation in Massachusetts, this state is ideally positioned in this regard to implement soft presumed consent, the form of presumed consent where the family’s consent is required to remove organs from individuals presumed to have consented to organ donation. The main purpose of soft presumed consent is to ensure that the family is given the opportunity to consider if the potential donor had any objections to becoming a donor that he or she expressed to the family, but for some reason did not opt out. Implementation of soft presumed consent will therefore reduce the risk that organs will accidentally be removed from individuals against their wishes. However, implementing soft presumed consent is unlikely to increase the number of organ donors as dramatically as would hard presumed consent, since American families agree to donate their loved one’s organs approximately half the time they are askedxliv, soft presumed consent would result in a system where fewer—but certainly not zero—waiting list patients die while a willing donor’s organs go to waste. Family consent rates would likely increase under a soft presumed consent system, since the family of each prospective donor (who has not opted out) could—and should—be approached as the family of a consenting donor, and not simply as the family of an eligible donor whose wishes are unknown. Soft presumed consent (when properly implemented, as explained above) therefore represents a moral improvement over the current system, but seems unlikely to reduce the number of unnecessary deaths on the waiting list as much as could hard presumed consent. For this reason, we recommend that Massachusetts begin by implementing soft presumed consent—the less effective form, but the form that more closely parallels the current legislature, and that includes the additional check-and-balance of family consent—but eventually switch to hard presumed consent, once the soft presumed consent system has been perfected and public support of presumed consent has sufficiently increased. Inevitably, a higher percentage of the population of eligible donors would have their organs removed against their (unexpressed) wishes under a hard presumed consent system than under even a soft presumed consent system—but we believe, as explained above, that the resulting moral harm done by implementing hard presumed consent (with all the precautionary measures previously described) is insignificant compared to the moral harm done by not switching to hard presumed consent as soon as feasible, and thus allowing people to die unnecessarily. Ethical Argument C: Disenfranchised people will be exploited under presumed consent, since it is unlikely that they will be aware either of the presumed consent legislation itself or of the available options should they wish not to donate. Response 1: Disenfranchised people are unlikely to be affected by this legislation, due to their probable circumstances of death. A potential organ donor is typically an individual whose death was determined by neurological criteria; in other words, the potential donor has a pulse but no brain activity (i.e., is brain-dead)[find citation]. An individual whose death is determined in this way is typically a young, healthy person who suffered an intracranial hemorrhage due to head trauma (sustained, for example, in a motor vehicle accident), or an aneurysm. Increasingly, potential organ donors can also be people whose deaths are determined by cardiovascular criteria, meaning that they no do not have a pulse; these potential donors are typically somewhat older people who suffered a heart attack or stroke and arrived at the hospital promptly (since human organs can survive for only 3-5 minutes without oxygen[find citation]). Individuals who are so disenfranchised that, not only do they not possess a motor vehicle, but they do not even have access to the educational resources described above, are unlikely upon their death to fall into either of these categories of organ donor. Practically speaking, then, presumed consent legislation would not have any bearing on the vast majority of these people. Response 2: Massachusetts law currently permits the state to use the bodies of disenfranchised people without their consent; therefore, disenfranchised people would be exploited both absolutely and comparatively less under presumed consent than they are today. Chapter 113 Section 1 of the General Laws of Massachusetts General Law states that: Upon the written application of the dean or other officer of any medical school established by law in the commonwealth, the penal institutions commissioner of Boston, the trustees and superintendent of the Tewksbury hospital or other public institution supported in whole or part at the public expense [this phrase implies that this section is very old] . . . in this chapter called the authorities, shall permit such dean or other officer to take, within three days after death, the body of any person, required to be buried at the public expense, who died in any institution under the control of such authorities, to be used within the commonwealth for the promotion of anatomical science. . . .xlv Chapter 113 Section 8 states that, if the hospital cannot locate any family or guardians of a potential organ donor, than the decision to donate or not falls to “any other person authorized or under obligation to dispose of the body”xlvi, and thus in the end to the state. These sections of Chapter 113 are not presumed-consent legislation: the deceased’s consent to these uses of his or her body is not required either explicitly or implicitly. Both these statutes simply declare that the state has property rights over the bodies for the disposal of which it is responsible—in other words, over the bodies of utterly disenfranchised people. Therefore, these laws resemble not presumed consent but organ conscription. In light of these laws, presumed consent legislation would be beneficial to disenfranchised people in two ways. First, it is conceivable that the extensive public education campaign might reach some of these people, who would then be able to act on their wish not to become an organ donor if they so desired. The above legislation, by contrast, is not known to exist by the general population, never mind the people to whom it is relevant. Second, presumed consent would make disenfranchised people equal in the eyes of the law to the rest of the population, since their consent would be presumed—and therefore required, albeit implicitly—along with that of everyone else. The wishes of disenfranchised people would be given the same weight as the wishes of the more fortunate. Ethical Argument D: Soft presumed consent (the form initially to be implemented) would add another burden to grieving families, who would have to attempt to determine whether their deceased relative’s presumed consent actually represents his or her wishes. Response: On the contrary, presumed consent would provide families with more guidance than they currently receive, thus easing the burden of decision-making for these families. Case One: The deceased expressly specified that he or she wishes not to donate. Massachusetts lacks a first-person consent law, presumably so that the family can choose not to donate if they are aware of any objections to becoming a donor that the individual registered subsequent to giving his or her express consent to donate. The absence of a first-person consent law indicates that Massachusetts law recognizes that removal of organs against the deceased’s wishes is morally worse than failing to remove organs when the deceased wished to be a donor. Therefore, should Massachusetts enact presumed consent legislation, this legislation should state that a potential donor’s choice to opt out is legally binding and cannot be overridden by the person’s family. In this situation, then, the family is spared the burden of choice that currently falls to the family of every person who explicitly consents to donation. Case Two: The deceased is presumed to have consented to organ donation. Under soft presumed consent legislation, the consent of the potential donor’s family is required for organ donation to proceed. However, the family would now be approached from a particular standpoint—as the family of an intended donor—and it is assumed that organ procurement will proceed unless the family knows of an unregistered objection to donation on the part of the deceased. It is clear in this situation that donation is the expected outcome, whereas there is no expected outcome for potential donors who did not give explicit consent to donate in the current system. (It seems likely also that approaching the family as the family of a donor would substantially increase the family consent rate.) We note also that any argument against soft presumed consent based on the claim that adding to the potential donor’s family’s decision-making burden is a moral harm and should be avoided, by implication favors a hard presumed consent system, where the decision-making burden is placed entirely on the individual and removed from the grieving family. Legal Argument: There is no legal precedent for presumed consent in Massachusetts. Response: While there is no legal precedent for presumed consent in the context of organ donation, the idea of presumed consent is not entirely foreign to medical practice in Massachusetts. Massachusetts law exempts emergency medical services personnel from liability for any injury sustained by patients who are resuscitated by these personnelxlvii. Therefore, there is precedent in Massachusetts law for suspending the common-law definition of assault as physical contact without explicit permission, and instead presuming the consent to engage in (often violent) physical contact, in order to save a life. Of course, there is one obvious and crucial difference between this form of presumed consent and presumed consent in organ donation: EMS personnel resuscitate patients in the attempt to save the patients’ lives; while doctors removing organs under presumed consent legislation would be doing so in order to save other people’s lives. However, this form of presumed consent legislation establishes a precedent for the validity of presumed consent in medical practice in Massachusetts. Conclusion It is time for Massachusetts to take the lead in American organ donation policy, by implementing soft presumed consent legislation as soon as possible. ~~~~~ Improve/correct: 1. Endnotes: (i) Retrieve and/or check a few references; (ii) Improve/correct formatting; (iii) Eliminate any unnecessary citations (e.g., multiple citations of same source within one paragraph that deals exclusively with that one source); (iv) Less exclusive reliance on a few sources? 2. Math: My partner did the “Why Here, Why Now?” section of the paper. I don’t currently have the background to properly check my partner’s math; I will find someone who can help me with this, make any necessary additions or changes, and then rewrite some of his prose to improve clarity. Extend/include: 1. Scope of the project: an improved version of this draft will be submitted to the Commissioner for Public Health in Massachusetts. For the conference, I intend to broaden the scope of this paper to address the actions best taken by individual states as well as by other countries whose legal systems are based on Common Law (e.g., Canada, Britain). 2. Economic feasibility of presumed consent: implementation would be expensive, but Spain has actually saved money with PC because kidney transplants cost less than years of dialysis (and the government pays for both—as in the United States, under Medicare). I will investigate the economic feasibility and potential benefit of PC in the US. 3. Legal analysis: I intend to speak to a professor at HLS, in order to extend/clarify/correct (if necessary) the legal argument in this paper—precedents, federal vs. state-level PC legislation, likelihood that the Supreme Court would uphold PC legislation, etc. 4. Happy to take other suggestions! ~~~~~ i “Data: Waiting List Candidates.” UNOS.com. 2007. UNOS. 3 Dec. 2006. <www.UNOS.com> Satel, Sally. “Death’s Waiting List.” New York Times 15 May 2006. iii Howard, David. “Producing Organ Donors: The Current System and Prospects for Reform.” The Journal of Economic Perspectives: forthcoming. iv Childress, James F. and Liverman, Catharyn T., ed. Organ Donation: Opportunities for Action. Washington, D.C.: The National Academies Press, 2006. v Satel. vi “Scientific Registry of Transplant Recipients.” June 22, 2006. ustransplant.org. <http://www.ustransplant.org> vii Cohen, Eric and Crowe, Sam. “Organ Transplant Policies and Policy Reforms.” Staff Discussion Paper: The President’s Council on Bioethics. Sept. 2006. viii Cohen. ix “About OPTN.” OPTN.com. 2007. OPTN. 3 Dec. 2006. <http://www.opten.org/optn> x Cohen. xi Cohen. xii “What is an OPO?” 11 May 2000. TransWeb.org. 18 Dec. 2006. <http://www.transweb.org/reference/maps/opo_image_map/usopomap.htm> xiii Cohen. xiv Cohen. xv Massachusetts General Law (through Sept. 30 2006): Chapter 113, Section 7. xvi Cohen??? xvii Abadie, Alberto and Sebastien Gay. “The impact of presumed consent legislation on cadaveric organ donation: A cross-country study.” Journal of Health Economics 25 (2006): 599-620. xviii Childress. xix Abadie. xx Cohen. xxi Cohen. xxii Cohen. xxiii Abadie. xxiv Summarized from Abadie. xxv Abadie xxvi Inspired by Abadie. xxvii Abadie. xxviii Koh, Howard et al. “A Statewide Public Health Approach to Improving Organ Donation.” American Journal of Public Health 97.1 (2007): 30-36. xxix Howard. xxx “United States.” CIA - The World Factbook. 19 Dec 2006. CIA. 17 Jan 2007 <https://www.cia.gov/cia/publications/factbook/geos/us.html>. xxxi Koh. xxxii Koh. xxxiii Childress. xxxiv Goldstein, Daniel and Johnson, Eric J. “Do Defaults Save Lives?” Science 302.5649 (2003): 1338-9 xxxv Gundle, Kenneth. “Presumed Consent: An International Comparison and Possibilities for Change in the United States.” Cambridge Quarterly of Healthcare Ethics 14.1 (2005): 113-8 xxxvi Goldstein. xxxvii Cohen. xxxviii MA Gen. Law 113.7 xxxix Massachusetts General Law (through Sept. 30 2006): Chapter 90, Section 8d. xl Massachusetts General Law (through Sept. 30 2006): Chapter 112, Section 84c. xli Goldstein. ii xlii Goldstein. Gundle. xliv Satel. xlv Massachusetts General Law (through Sept. 30 2006): Chapter 113, Section 1. xlvi Massachusetts General Law (through Sept. 30 2006): Chapter 113, Section 8. xlvii Massachusetts General Law (through Sept. 30 2006): Chapter 111c, Section 21. xliii