Neuro- Rehab workstream
advertisement

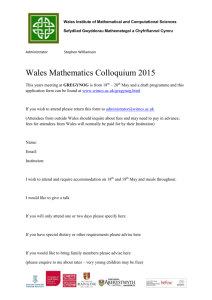
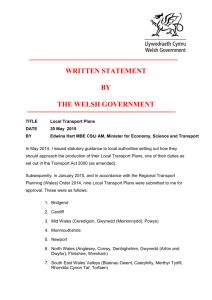
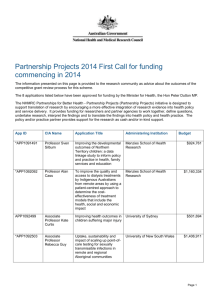
North Wales Neurosciences Review Implementation Neuro-Rehabilitation Workstream 1. Purpose The purpose of this report is to outline the preliminary work that has been conducted to date to develop the neuro-rehabilitation workstream of the North Wales neurosciences review. This has included a series of meetings with stakeholders to build understanding of the current neuro-rehabilitation care pathway, help define the key issues and explore perspectives on these issues. This has been used to inform the development of a project initiation document (PID). The PID describes how the schedule for this workstream will ensure the timescales for the overall neurosciences project are met. The phase 1 report on the current service will be delivered by March 31st 2009. The phase 2 report will be delivered by 30th April 2009 in line with the overall neurosciences review implementation schedule. 2. Gathering Intelligence In order to develop a robust project plan, a series of meetings have been held with stakeholders by the project lead and project manager, to gather information on the existing pattern of services, to identify key issues that need to be addressed in order to improve neuro rehabilitation services to implement the Steers review recommendations, and to develop the project plan. A series of meetings have been held with the following individuals and centres: Dr Carolyn Young, Walton Centre for Neurology and Neurosurgery Dr Colin Pinder, Clatterbridge Hospital Neuro-Rehabilitation Unit Dr Rudi Coetzer, North Wales Brain Injury Team Dr Matt Makin, Palliative Care Consultant Mr Kevin Thomas, MND Association Dr Bob Rafal, University of Bangor A meeting with the ‘Steers’ review team took place on 13th February and the opportunity was taken to understand the team’s thinking about the perceived needs for N Wales and models of future service provision that could be considered from England. A further meeting with Dr Anne Chamberlain (Steers Review Member) and clinical colleagues in Leeds has been organised for 6th March 2009. A number of individuals (appendix1) have been indentified with particular interest and expertise in this area of work and it is intended to hold 2 stakeholder meetings in March and April to sign off the Project plan, further develop current knowledge of services, needs and identify the gaps, and develop options for the development of services to meet the identified need. A final meeting is planned for July to agree the final report for submission to the Project group 1 3. Neurorehabilitation 3.1 Prevalence A study by Drs Elliston and Rodgers in 1996 identified 242 people at that time in N Wales who had suffered significant brain injury. (Representing only 25% of the expected number predicted from national rates) A study in 1997 by the All Wales Steering Group (Severe head injuries rehabilitation) estimated that there were some 1,000 survivors of brain trauma with long term disabilities living in the North Wales community. Bob Rafal (2002) estimated that from all three DGHs some 35-45 patients per annum could access an N Wales Rehabilitation Unit with lengths of stay in the range of 6 weeks to 3 months. 3.2 In Patient Care The Walton Centre provides a limited rehabilitation service for patients admitted and treated through to their service and provides a service for all types of acquired brain who can benefit from its service including trauma, tumour, infection, younger stroke patients and neurological conditions. The service is commissioned by HCW. Table 1 Contract value and activity Contract Value 2008/9 £18,946 Contract Baseline Activity 38 bed days 2007/8 2006/7 - 91 bed days 91 bed days Actual Activity 6 bed days to month 9 22 bed days - The Clatterbridge Hospital provides a service for referrals from North Wales Trusts and the Countess of Chester. The service is commissioned by Flintshire LHB on behalf on N Wales. Table 2 Contact Value and Activity Contract Value 2007/8 Contract Baseline Activity 13 patients / 938 bed days £390,884 Actual Activity 7 patients, 227 bed days For all Welsh patients discharged from the Clatterbridge service since 2001/2 (65 patients), average length of stay was 63 days (ranging from 7 days to 427 days). Further information is provided in appendix 2. 2 Criteria for admission for rehabilitation from Clatterbridge: be medically/surgically stable the WNRU consultant considers that, at the time of assessment a formal structured rehabilitation programme at WNRU has the potential to improve the patient's functioning. have specific goals for rehabilitation neurological conditions can include: brain injury from any cause e.g. trauma, infection, after neurosurgical intervention and other cerebrovascular event patients with multiple sclerosis and other demyelinating conditions patients with acute demyelinating polyneuropathy patients with intracranial tumours who are currently neurologically stable patient with spinal cord injury from medical cause In the three North Wales DGHs the following arrangements are in place for ABI patients; Wrexham Maelor Hospital-No dedicated rehabilitation beds for ABI. Patients admitted to 20 bed stroke rehabilitation ward for intermediate rehabilitation. Glan Clwyd Hospital-No dedicated ABI rehabilitation beds for ABI. Patients managed by orthopaedic service. Ysbyty Gwynedd-No dedicated ABI rehabilitation beds. Patients managed on Tegid ward by stroke rehabilitation team. A number of community hospitals have consultant beds and these are also used for continuing rehabilitation of ABI patients. Identifying patients admitted to the three DGHs is problematic and a search was undertaken of patients with the following diagnostic codes. Table 3 Diagnostic Codes for ABI Diagnosis Traumatic brain injury Intracerebral Haemorrhage Anoxic Brain Damage Meningitis ICD10 Code SO6.0 to SO6.9 I61.0 to I61.9: I62.0 to I62.9 G93.1 G00.0 to G00.9; G01; G02.8; G03.0 to G03.9 G04.0 to G04.9; G05.0 to G05.8 I67.1 I60.0 to I60.9 Encephalitis Cerebral Aneurysm Subarachnoid Haemorrhage The table in Appendix 3 shows patients admitted in 2007/8 to Wrexham Maelor, Ysbyty Glan Clwyd and Ysbyty Gwynedd with the above diagnoses and with a length of stay greater than 30 days. 3 The data indicates that there were 64 patients in total with a combined length of stay of 4299 bed days. On the assumption that all these patients would be appropriate for admission to an in-patient neuro-rehabilitation unit, this unit would require approximately 11 to 12 beds. Note that this analysis is preliminary only. Further work will be conducted to provide a more accurate estimate of need for neuro-rehabilitation. Some of the patients in this sample may not be appropriate for admission to a neurorehabilitation unit. It is also possible that some patients may be discharged to community hospitals prior to 30 days and thus not captured in this data. 3.3 Community Brain Injury Service The North Wales Brain Injury Service provides a multidisciplinary community based service of low intensity, long-term rehabilitation to individuals of any age with moderate to severe acquired (non-progressive) brain injuries including trauma, cerebro-vascular accidents, tumours, CNS infections and younger stroke patients. Table 4 New Referrals between 1st January 2008 and 31st December 2008 Total referrals received 174 Total appropriate referrals (accepted) 163 Total non-appropriate referrals (not accepted) Of the appropriate referrals: TBI referrals Non-TBI (e.g. stroke, tumour, infection) Not yet coded 11 59 70 34 Table 5 Staff Establishment (Feb 2009) Professional Group Neuropsychology Consultant Neuropsychologist (Head of Service) Neuropsychologists Psychology Clinical psychology trainees Assistant Psychologists Neurology Consultant Neurologists Neuropsychiatry Consultant Neuropsychiatrist Physiotherapy Physiotherapist Technical instructor Occupational Therapy Occupational Therapists OT students SLT SLT Social Worker Social Worker Social worker student 4 WTE 1 3 1 2 0.8 0.2 1 1 1.78 0 1 1 0 Medical Admin Registrars/Medical students Admin manager Admin and reception 1 1 1.6 3.4 Key Issues Identified The key neuro rehabilitation issues identified to date include: The need to map the current pathway for patients discharged from the Walton Centre many of whom are discharged to the care of DGHs rather than to a neuro-rehabilitation service able to meet their needs The need to map/describe the service provided by DGHs to acquired brain injury patients, to quantify this services in terms of patient case mix and resource The need for an agreed definitions set for key terminology relating to the neuro-rehabilitation pathway The need to develop a neuro-rehabilitation care pathway for North Wales, including the key interfaces with other services (e.g. neuropsychiatry, palliative care, acute care) Quantifying the need for neuro-rehabilitation, and capacity required to meet that need, is not straight forward. There is no specific code for neuro-rehabilitation. Patients are spread across many different locations within the DGHs. A triangulation approach is required that utilises diagnostic coding, academic research into incidence of ABI, and the views of clinicians to help verify estimates. Preliminary data is included above. 4. Palliative Care The work stream will focus on the needs of patients with ‘rapidly progressing neurological diseases’ and the interface with ‘neuro rehabilitation’. The main clinical condition in the above is Motor Neurone Disease (MND), Multiple Sclerosis (MS) and Parkinson’s disease (PD). Applying figures quoted in Jader (Jader, L. An Overview of Neurological Disorder in Wales. Neuroepidemiology 2007; 28: 65-78) for Wales to North Wales 2007 population estimates, it is estimated that there are at least 664 cases of multiple sclerosis, 40 cases of motor neurone disease and 1063 cases of Parkinson’s disease in North Wales. Tables and Figures Nos 1, 2 and 3 in Appendix 4 show average numbers of deaths per year in North Wales Counties and across Wales for these three diseases for the period 1996-2006. For MND diagnosis typically occurs at the Walton Centre for Neurology and Neurosurgery. 6 monthly neurology outpatient appointments continue at Walton unless patients seen at local DGHS by visiting Consultant. The Walton Centre has an established multidisciplinary clinic for newly diagnosed patients with MND providing assessment and advice following diagnosis, including Specialist Nurse, Physiotherapist, OT, S&LT, Welfare Rights and MND Association Regional Care Development Adviser. 5 An informal multidisciplinary team has been established in the former Conwy & Denbighshire NHS Trust area since 2006. Cases are discussed on a bimonthly basis, identifying future needs and timely, sensitive intervention. St David’s and St Kentigern’s hospices provide day care. In the former NE Wales Trust area the majority of patients with rapidly progressing MND are referred to Specialist Palliative Care Services. Nightingale House Hospice offers day care and out patient therapy assessments. Gaps in Current Service Provision include: Delays in diagnosis Fragmentation of services Duplication of referrals Assessment and provision of equipment Inequitable access to services (specialist advice and equipment) Respite and home care Communication between agencies Coordination and anticipatory care No Systematic care plan Following discussion with Dr Makin and Kevin Thomas it became clear that a detailed process mapping exercise to understand the journey for MND patients has been produced. The key opportunity for the workstream is to develop a pathway for patients with rapidly deteriorating neurological conditions and the interface with rehabilitation services. 5. Continuing Health Care Where patients have a ‘primary health need’ the NHS is responsible for funding their health care wherever it is met. There are a number of patients with acquired brain injuries that the NHS is funding their care in private institutions. An analysis of the number, costs and type is being prepared by the 6 N Wales LHBs. Conwy LHB funds placements at the following institutions: i) Hafod y Green – Nursing home providing long term care for Acquired Brain Injury clients. Currently 6 clients, 4 joint funded with CCBC. ii) Eithinog (Leonard Cheshire Disability) (Dual registration care home for Acquired Brain Injury clients). Currently 11 patients, 4 jointly funded with CCBC. Total Conwy LHB projected costs in 2008/9 £507,376. 6 6. Project Arrangements 6.1 Project Manager Luke Archard, Assistant Commissioner for Long Term Conditions and Neurosciences, Health Commission Wales, has been allocated a day a week by Health Commission Wales to provide project management support to Wyn Thomas, project lead. 6.2 Project Initiation Document A PID has been developed for the neuro-rehabilitation workstream. The document outlines specific objectives for the neuro-rehabilitation workstream as follows: To identify and acquire the key service data and information required to develop and evaluate a range of options for the organization and delivery of neuro-rehabilitation services for North Wales. To develop a long list of options for the organization and delivery of neuro-rehabilitation services for North Wales. To develop and apply a criteria for evaluating the long list of options in order to select a short list for full option appraisal. To conduct an option appraisal and to identify the most appropriate model for the provision of neuro-rehabilitation services for North Wales. Develop a pathway for the care of patients across North Wales with rapidly progressing neurological diseases e.g. motor neurone disease To identify the key issues relating to the interfaces between neurorehabilitation and other services, including acute care for head injured patients, neuro-psychiatry services, continuing care and palliative care, and to address these within the option appraisal. A series of meetings of the neuro-rehabilitation workstream Project Board will be held to direct the work. These meetings will be combined with workshops. The key actions to be achieved in each project meeting are set out below: Meeting 1 (March 2009) Key Actions Finalise and agree Project Initiation Document Agree Project Board ToR Agree work plan and timescales. Establish leads and terms of reference for project working groups to develop the products. 1st draft phase 1 report discussed. (To be signed off virtually by Project Board by March 31st). Hold workshop to identify current patient pathway and service gaps 7 Meeting 2 (Week beginning 13th April 2009) Meeting 3 (Week beginning 6th July 2009) Workshop to develop the long list of options for phase 2 report. Selection of short-list. (Phase 2 report completed following this meeting. Signed-off virtually by Project Board by 30 April 2009) Develop and agree criteria and weighting system for option appraisal to inform 3rd phase report Agree date and format of option appraisal workshop (to be held in June) Discuss and agree 3rd phase report (product 3) Discuss and agree costed implementation plan (product 4) 7. Appendices Attached are preliminary data and information to feed into the phase 1 report. Appendix 1 proposed project board membership Appendix 2 estimated number of patients with ABI admitted to North Wales DGHs in 2007/8. Implications for capacity of a neurorehabilitation unit for North Wales. Appendix 3 Data on patients discharged from Clatterbridge. Appendix 4 Data on MND, MS and PD patients across N Wales 8 Appendix 1 Proposed Board Members Name Wyn Thomas Dr Rudi Coetzer Dr Bob Rafael Iwan Bonds Dr Giles Harborne Dr Nigel Martin Iain Mitchell Pam Lewis Lowri Welnitschuk Angela Jones Ian Langfield Dr John Hindle Brian Pickles Helen Spellman Huw Thomas Professor Peter Madison Dr Martyn Bracewell Chris Jones Professor Carolyn Young Dr Colin Pinder Dr Jenny Thomas Dr David Abankwa Role in project Organisation Chair of Project Board and local commissioner Conwy LHB Expertise in neurorehabilitation and knowledge of current North Wales service Expertise in neurorehabilitation and knowledge of current North Wales service Financial oversight North Wales Trust University of Bangor NHS Trust Expert in neuro psychiatry and knowledge of current North Wales Trust North Wales service Palliative Care Nightingale House Hospice Expert in therapy services and knowledge of North North Wales Trust Wales Expert in therapy services and knowledge of North North West Wales NHS Trust Wales Continuing Care North West Wales NHS Trust Palliative Care North West Wales NHS Trust Service Group HCW Commissioner Expertise in rehabilitation North West Wales NHS Trust and Parkinson’s disease Planning expertise and links with Llandudno Hospital Conwy LHB project Voluntary sector expertise Leonard Cheshire Disability and head injury services Patient and Public N/A perspective Expertise in rheumatology NWW Trust and rehabilitation Expertise in neuro University of Bangor rehabilitation Patient and Public Conwy CHC perspective Independent expert in Walton Centre for Neurology and rehabilitation medicine Neurosurgery Independent expert in Clatterbridge Hospital, Wirral rehabilitation medicine NHS Trust Independent expert in Rookwood Hospital, Cardiff and rehabilitation medicine Vale NHS Trust Independent expert in Abertawe Bro-Morgannwg rehabilitation medicine University NHS Trust Kevin Thomas Patient perspective Luke Archard Project Management Support Welsh Neurological Alliance HCW 9 Position CEO Consultant Psychologist North Wales Brain Injury Service Professor of Clinical Neuroscience and Neuropsychology Management Accountant Chief of Staff (Mental Health Services) Asst medical Director Director of Therapy Services Head of Therapy Services Senior Nurse Senior Nurse Commissioner for Neurosciences Consultant Project Manager Llandudno Hospital Review Head of Acquired Brain Injury Division Retired CEO GHA Retired Consultant Rheumatologist Senior Lecturer Chief Officer Consultant in Rehabilitation medicine Consultant in Rehabilitation Medicine Consultant in Rehabilitation Medicine Consultant in Rehabilitation Medicine North Wales Care Development Officer Assistant Commissioner for Neurosciences Appendix 2 Admissions of Welsh Patients to Clatterbridge NRU 2001/2 to 2008/9 Year 2001-2 2002-3 2003-4 2004-5 2005-6 2006-7 2007-8 2008-9 Grand Total Admissions 1 11 10 13 8 10 3 14 70 Diagnoses of Welsh patients admitted to Clatterbridge NRU between 2001/2 and 2008 /9 Diagnosis Brain Stem Infarct Cerebellar infarct CVA/TBI GBS Hydrocephalus, syringomyelia Hypoxic Brain injury ICH ICH, Hydrocephalus, antiphospholipid syndrome Meningioma MS Peripheral Neuropathy Post. Fossa epidermoid cyst SAH Spinal cord Contusion Spinal cord infarct Spinal cord tumour Stroke TBI Not recorded Grand Total 10 Number of Patients 1 1 1 2 1 1 10 1 1 5 1 1 6 1 1 1 3 27 5 70 Appendix 3 Patients with an acquired head injury cared for in North Wales DGHs 2007/8 Site Name Wrexham Maelor Hospital Diagnosis Text LoS Patients 40 1 44 54 71 1 1 1 1 Acute disseminated encephalitis Acute disseminated encephalitis Total Cerebrovascular disease, unspecified Cerebrovascular disease, unspecified Total Intracerebral haemorrhage in cerebellum Intracerebral haemorrhage in cerebellum Total Intracerebral haemorrhage in hemisphere, sub cortical Intracerebral haemorrhage in hemisphere, sub cortical Total Intracerebral haemorrhage, intraventricular Intracerebral haemorrhage, intraventricular Total Intracerebral haemorrhage, unspecified Intracerebral haemorrhage, unspecified Total Other intracerebral haemorrhage Other intracerebral haemorrhage Total Other specified cerebrovascular diseases Other specified cerebrovascular diseases Total Subarachnoid haemorrhage from anterior communicating artery 11 3 142 1 1 39 55 1 1 2 118 1 1 32 44 47 55 70 71 80 165 1 1 1 1 1 1 1 1 34 58 8 1 1 2 35 43 1 1 2 35 69 1 1 Subarachnoid haemorrhage from anterior communicating artery Total Subarachnoid haemorrhage, unspecified Subarachnoid haemorrhage, unspecified Total Subdural haemorrhage (acute)(non traumatic) Subdural haemorrhage (acute)(non traumatic) Total Traumatic subarachnoid haemorrhage Traumatic subarachnoid haemorrhage Total Traumatic subdural haemorrhage 2 91 93 2 58 1 119 1 1 39 61 62 64 184 1 1 1 1 1 1 Traumatic subdural haemorrhage Total Total Ysbyty Glan Clwyd 1 1 5 2172 31 51 1 32 66 1 1 1 36 2 1 Cerebral aneurysm, non ruptured Cerebral aneurysm, non ruptured Total Cerebrovascular disease, unspecified Cerebrovascular disease, unspecified Total Diffuse brain injury Diffuse brain injury Total Encephalitis, myelitis and encephalomyelitis, unspecified Encephalitis, myelitis and encephalomyelitis, unspecified Total Focal brain injury Focal brain injury Total Intracerebral haemorrhage in hemisphere, sub cortical Intracerebral haemorrhage in hemisphere, sub cortical Total Intracerebral haemorrhage, unspecified 12 1 46 1 37 1 1 1 33 1 1 35 45 48 56 124 1 2 1 1 1 Intracerebral haemorrhage, unspecified Total Intracranial injury, unspecified Intracranial injury, unspecified Total Other intracranial injuries Other intracranial injuries Total Other specified cerebrovascular diseases Other specified cerebrovascular diseases Total Subarachnoid haemorrhage, unspecified Subarachnoid haemorrhage, unspecified Total Subdural haemorrhage (acute)(non traumatic) Subdural haemorrhage (acute)(non traumatic) Total Total Ysbyty Gwynedd 46 117 6 1 1 38 2 1 1 53 1 1 116 1 1 35 1 1 1014 19 128 1 69 128 1 1 1 Cerebrovascular disease, unspecified Cerebrovascular disease, unspecified Total Diffuse brain injury Diffuse brain injury Total Intracerebral haemorrhage in cerebellum Intracerebral haemorrhage in cerebellum Total Intracerebral haemorrhage in hemisphere, cortical Intracerebral haemorrhage in hemisphere, cortical Total Intracerebral haemorrhage, unspecified Intracerebral haemorrhage, unspecified Total Other intracerebral haemorrhage Other intracerebral haemorrhage Total Other specified cerebrovascular diseases Other specified cerebrovascular diseases Total 13 2 50 1 1 91 1 1 32 87 1 1 36 69 2 1 1 2 32 135 1 1 2 Subarachnoid haemorrhage from basilar artery Subarachnoid haemorrhage from basilar artery Total Subdural haemorrhage (acute)(non traumatic) Subdural haemorrhage (acute)(non traumatic) Total Traumatic subarachnoid haemorrhage 40 1 95 1 121 1 1 Traumatic subarachnoid haemorrhage Total Total Grand Total 14 1 1 1113 14 4299 64 Appendix 4 Table 1: Parkinson's disease mortality, European age-standardised rate (EASR) per 100,000 North Wales Local Authorities, all persons, 1996-2006 Average deaths per year Local Authority Isle of Anglesey Gwynedd Conwy Denbighshire Flintshire Wrexham Wales Crude rate per 100,000 EASR per 100,000 95% LCL 95% UCL Compared to Wales No sig. difference No sig. difference No sig. difference No sig. difference No sig. difference No sig. difference 5 11 13 7 8 8 7.1 9.2 11.6 8.0 5.2 6.3 3.3 4.1 4.1 3.3 3.1 3.5 2.5 3.4 3.4 2.6 2.5 2.8 4.6 5.1 5.0 4.3 4.0 4.4 205 7.0 3.6 3.5 3.8 Source: O NS (ADDE, MYE) Figure 1: Parkinson's disease mortality, European agestandardised rate (EASR) per 100,000, ranked North Wales Local Authorities, all persons, 1996-2006 Source: ONS (ADDE, MYE) 95% confidence intervals are shown around the EASR EASR 14 Crude rate 12 Rate per 100,000 Wales EASR = 3.6 10 8 6 4 2 Source: NPHS Table 2: 15 Gwynedd Conwy Wrexham Isle of Anglesey Denbighshire Flintshire 0 Multiple sclerosis mortality, European age-standardised rate (EASR) per 100,000 North Wales Local Authorities, all persons, 1996-2006 Average deaths per year Local Authority Isle of Anglesey Gwynedd Conwy Denbighshire Flintshire Wrexham Wales Crude rate per 100,000 EASR per 100,000 95% LCL 95% UCL Compared to Wales No sig. difference No sig. difference Sig. high No sig. difference No sig. difference No sig. difference 2 2 3 2 2 3 2.3 1.5 2.7 1.9 1.2 2.0 2.0 1.3 2.1 1.6 1.1 1.8 1.1 0.8 1.4 0.9 0.7 1.2 3.3 2.1 3.1 2.6 1.8 2.6 46 1.6 1.4 1.3 1.5 Source: O NS (ADDE, MYE) Figure 2: Multiple sclerosis mortality, European agestandardised rate (EASR) per 100,000, ranked North Wales Local Authorities, all persons, 1996-2006 Source: ONS (ADDE, MYE) 95% confidence intervals are shown around the EASR EASR 4.0 Crude rate 3.5 Rate per 100,000 3.0 2.5 Wales EASR = 1.4 2.0 1.5 1.0 0.5 Source: NPHS Table 3: 16 Conwy Isle of Anglesey Wrexham Denbighshire Gwynedd Flintshire 0.0 Motor neurone disease mortality, European age-standardised rate (EASR) per 100,000 North Wales Local Authorities, all persons, 1996-2006 Local Authority Average deaths per year Isle of Anglesey Gwynedd Conwy Denbighshire Flintshire Wrexham Wales Crude rate per 100,000 EASR per 100,000 95% LCL 95% UCL Compared to Wales No sig. difference No sig. difference Sig. high No sig. difference No sig. difference No sig. difference 2 3 5 2 4 4 3.2 2.6 4.8 2.2 2.5 3.0 2.0 1.9 2.8 1.5 2.0 2.4 1.3 1.3 2.1 0.9 1.4 1.7 3.3 2.7 3.9 2.4 2.8 3.3 79 2.7 2.0 1.8 2.1 Source: O NS (ADDE, MYE) Figure 3: Motor neurone disease mortality, European agestandardised rate (EASR) per 100,000, ranked North Wales Local Authorities, all persons, 1996-2006 Source: ONS (ADDE, MYE) 95% confidence intervals are shown around the EASR EASR 6 Crude rate 4 Wales EASR = 2.0 3 2 1 Source: NPHS 17 Conwy Wrexham Isle of Anglesey Flintshire Gwynedd 0 Denbighshire Rate per 100,000 5