Protocol for urine testing in ACH
advertisement

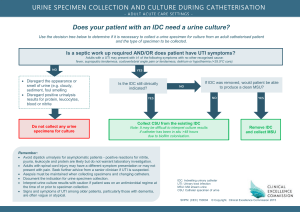
North East Valley Division of General Practice Aged Care GP Panels Initiative Sept 2005 Revised Jan 06, July 06 Residents of Aged Care Homes & Urine Testing Protocol Aged Care Home Guide Background The following protocol has been developed because of the high rate of testing of urine – both by dipstick, and by MSU and formal pathology – that occurs in the ACH setting. This leads to over-diagnosis of urinary tract infections (UTIs), unnecessary prescribing of antibiotics with no positive benefit and medication-related complications. There is excessive cost (tests, ACH staff and GP time, pathology services, medications) associated with all stages of the pathway and a contribution to the development of resistant organisms. The medical evidence does not support widespread testing (screening) of urine of residents in ACHs. This protocol is based on current evidence and reflects significant changes to traditional practice. Important points Residents in ACHs have high rates of bacteruria and pyuria without having UTIs. UTIs are also common in this group. Because of the high background rates of bacteruria and pyuria in the ACH setting, there is no place for routine urine testing (ie there is no place for screening of asymptomatic residents). There is no place for urine dipstick testing in the ACH setting due to lack of specificity of positive findings (nitrites and LE/leucocytes). A negative urine dipstick makes UTI less likely but does not definitely exclude a UTI. An MSU and formal pathology is the most useful test when UTI is clinically suspected, both to support the diagnosis and provide antibiotic sensitivities. A UTI is diagnosed by a combination of clinical signs and symptoms and positive MSU pathology (microscopy and culture). Odour or cloudiness alone is not indicative of UTI and no reason to test urine. Cloudy urine and bacteruria are expected in all patients with a urinary catheter. It is illegal to send an MSU to a laboratory without an order from a doctor. Because of the difficulty in establishing a definite diagnosis of UTI and the problem of increasing antimicrobial resistance, it is advisable to await the MSU result before commencing treatment if the clinical condition allows. Treatment should be guided by the clinical condition regardless of the pathology result. GP should be consulted urgently if the patient is significantly unwell. Fluid intake should be maintained particularly if UTI is suspected or confirmed. The evidence is not consistent regarding the use of cranberry juice to prevent recurrent UTIs. (It has been shown to reduce the rate of recurrence in young women with E.coli UTIs) If history of recurrent UTIs, GP may: o consider urinary retention and investigate with ultrasound o consider prophylactic antibiotics Careful continence management is the most useful preventive measure, especially avoiding prolonged exposure to faeces. The Urine Testing Protocol is based on current evidence & expert opinion. The NEVDGP is in the process of negotiating formal evaluation to establish whether or not implementation of the protocol can be endorsed as best practice in residential aged care. North East Valley Division of General Practice Aged Care GP Panels Initiative Sept 2005 Revised Jan 06, July 06 Flow chart for testing of urine in aged care homes Suspect a UTI when a patient has one or more of Dysuria Frequent passing of urine or urge to pass urine Bladder or renal pain Recent onset or worsening incontinence Also consider UTI if unexplained Fever; or Malaise; or Nausea and/or vomiting; or Confusion (change in mental state) But more likely to be UTI if specific UTI symptoms are present or if history of previous illness with UTI Needs clinical assessment by GP to exclude other possible diagnoses Notify GP Under direction from GP, ACH staff collect MSU and send for pathology If result confirms UTI, GP prescribes treatment to be administered by ACH staff or if clinical condition warrants, GP starts empirical antibiotic until MSU result available The Urine Testing Protocol is based on current evidence & expert opinion. The NEVDGP is in the process of negotiating formal evaluation to establish whether or not implementation of the protocol can be endorsed as best practice in residential aged care.